
Abstract
Molecular epidemiology evidence indicates racial and ethnic differences in the aggressiveness and survival of breast cancer. Hispanics/Latinas (H/Ls) and non-Hispanic Black women (NHB) are at higher risk of breast cancer (BC)-related death relative to non-Hispanic white (NHW) women in part because they are diagnosed with hormone receptor-negative (HR) subtype and at higher stages. Since the cell cycle is one of the most commonly deregulated cellular processes in cancer, we propose that the mitotic kinases TTK (or Mps1), TBK1, and Nek2 could be novel targets to prevent breast cancer progression among NHBs and H/Ls. In this study, we calculated levels of TTK, p-TBK1, epithelial (E-cadherin), mesenchymal (Vimentin), and proliferation (Ki67) markers through immunohistochemical (IHC) staining of breast cancer tissue microarrays (TMAs) that includes samples from 6 regions in the Southeast of the United States and Puerto Rico -regions enriched with NHB and H/L breast cancer patients. IHC analysis showed that TTK, Ki67, and Vimentin were significantly expressed in triple-negative (TNBC) tumors relative to other subtypes, while E-cadherin showed decreased expression. TTK correlated with all of the clinical variables but p-TBK1 did not correlate with any of them. TCGA analysis revealed that the mRNA levels of multiple mitotic kinases, including TTK, Nek2, Plk1, Bub1, and Aurora kinases A and B, and transcription factors that are known to control the expression of these kinases (e.g. FoxM1 and E2F1-3) were upregulated in NHBs versus NHWs and correlated with higher aneuploidy indexes in NHB, suggesting that these mitotic kinases may be future novel targets for breast cancer treatment in NHB women.
Similar content being viewed by others
Introduction
Breast cancer is the most commonly diagnosed cancer worldwide, representing 12% of all new annual cancer cases globally [1]. In America, breast cancer is the most commonly diagnosed cancer among women, and in the United States (US), it is the second leading cause of all cancer mortality among women, after lung cancer. Molecular epidemiology studies provide evidence for racial/ethnic differences in the aggressiveness and survival of breast cancer patients revealing that non-Hispanic black (NHB) women and Hispanic/Latino women (H/L) have poorer outcomes and survival compared with non-Hispanic White (NHW) women [2,3,4,5,6]. H/L women from the Caribbean (C-H/L: from Puerto Rico, Dominican Republic, and Cuba) have higher incidences [7, 8] and poorer survival outcomes than other H/L [9, 10]. Thus, compelling evidence demonstrates the disparities among NHB and H/L who are more likely to be diagnosed at later stages (stages II-IV) compared with NHW women [4, 11,12,13,14,15,16]. NHB and H/L also have a higher probability of being diagnosed with triple-negative breast cancer (TNBC), a subtype that lacks hormone receptors and for which there are no effective biological treatments. H/L and NHB women with TNBC have significantly poorer 5 year survival outcomes than NHW women with TNBC [17]. While TNBC and socioeconomic status independently contribute to poor outcomes in H/L and NHB women with breast cancer, worse survival rates occur even after adjusting for socioeconomic status, estrogen receptor (ER) and progesterone receptor (PR) status, and access to health care [4]. This is supported by observations that NHB women have higher mortality rates than NHW women, even when detected with the Luminal (ER + PR + and Her2 + or –) subtypes, which have the best prognostic outcomes of any breast cancer subtype [18,19,20]. The same trend is seen in black H/L women with breast cancer, who have lower survival percentages than their white counterparts [21]. Thus, novel therapeutic strategies are needed to reduce the high mortality rates of H/L and NHB women with advanced breast cancer. Elucidating the expression patterns of centrosome-associated mitotic kinases in specific racial/ethnic groups and therapies against these kinases has the potential to greatly improve the survival outcomes of H/L and NHB women with breast tumors.
Over the past decade, many studies have shown a direct role of protein kinase dysregulation (through protein overexpression or mutations) in several human diseases including cancer [22]. Kinases are common drug targets for cancer treatment [23], and therapies against mitotic kinases are an emerging strategy against cancer [24]. TTK is a kinase that initiates the spindle assembly checkpoint (SAC), a mechanism that prevents the missegregation of chromosomes by ensuring the attachment of kinetochores to the spindle at metaphase [25,26,27]. TTK recruits several regulators of the SAC, including KNL1, MAD1, and BUB1 kinases into centromeres, and is an essential protein in cancer cells [28]. TBK1, an IKK (IκB Kinase)-related kinase that mediates inflammatory responses [29] and that is involved in the stabilization of microtubules [30] is also an important regulator of the SAC in breast and lung cancer [31]. NIMA-related kinase 2 (Nek2) triggers centrosome separation at the G2 phase and the SAC [32,33,34]. When dysregulated these kinases modulate rates of centrosome amplification-driven chromosome instability (CA/CIN) [30, 35,36,37,38,39,40,41], which is an abnormal process that promotes tumor initiation and cell invasion [42,43,44]. Therefore, chemical inhibitors against these kinases prevent the further generation of CA/CIN but also lead to massive chromosome losses that result in cell death [24, 45,46,47].
Recent publications from our laboratory and others have found that centrosome-associated mitotic kinases are involved in early intermediate steps to metastasis, including cell migration and invasion (reviewed in [24, 48]. Our group has demonstrated that the pharmacological or genomic silencing of TTK suppressed the epithelial-to-mesenchymal transition (EMT) and invasion of mesenchymal, TNBC cells through different mechanisms including the induction of the transcription factor KLF5, the induction of mi-RNA (miR) 200, the decreased expression of the EMT-associated miR-21, and the suppression of TGF-β-induced SMAD-3 phosphorylation [49]. We also demonstrated that Nek2 drives the EMT of TNBC cell lines by regulating EMT markers including E-cadherin, and Vimentin, as well as the EMT transcription factors Slug and Zeb1 [35]. To further explore these findings, here we present data on the expression of TTK, Nek2, and TBK1 mRNA in different ethnic and racial groups. In addition, we present data on expression levels of TTK and TBK1 and how that correlates with EMT markers including E-cadherin and Vimentin, using a novel set of tissue microarrays (TMAs) with invasive ductal carcinoma (IDC) breast tissue samples from NHB, C-H/L, and NHW women from Southeast USA and Puerto Rico. These TMAs were previously designed and constructed as part of an effort between Ponce Health Sciences University-Ponce Research Institute and Moffitt Cancer Center with the purpose to study drivers of breast cancers in different ethnic and racial populations [50]. Thus, our findings will provide novel knowledge related to future strategies for therapeutic intervention in NHBs and H/Ls with advanced stages of breast cancer.
Materials and methods
Ethics and consent statement
The protocol for this study was classified as exempt by the Institutional Review Board from the Ponce Health Sciences University (Human subjects assurance number FWA00000345) and approved under protocol number 160115-HS.
Bioinformatic analysis of gene expression
Gene expression in breast tumors was done using cBIOPORTAL [51, 52] analyses by using either the METABRIC or the TCGA databases. Overexpression is defined as a z-score threshold ± 2.0 of gene expression in tumors relative to diploid samples. Filters were applied, including subtype (both databases), race, and ethnicity (only available in TCGA). Data was downloaded onto Excell and analyzed using statistics (below).
Patient cohorts from the breast cancer tissue microarray (TMA)
For this study, we used formalin-fixed, paraffin-embedded TMAs from the National Cancer Institute (NCI) Minority Biospecimen/Biobanking Geographic Management Program for region 3 (BMaP-3), now BMaP region 2. The TMA includes breast cancer samples characterized pathologically by hematoxylin/eosin (H&E) and immuno-histochemically with antibodies recognizing ER, PR, and Her2 [50]. The breast cancer samples were collected in a de-identified fashion by six academic centers (Moffitt Cancer Center, Emory Winship Cancer Center, Ponce Health Sciences University, Tulane University, the University of Alabama at Birmingham, and the University of Mississippi Medical Center) serving the Southeast of the United States and Puerto Rico. Samples are from patients older than 18 years of age and primary, invasive ductal carcinomas (no metastasis). The subtypes included in the array are TNBC (Her2-ER-PR-), Luminal (Her2 − ER + PR + or Her2 + ER + PR +), and Her2 + (Her2 + ER-PR-). The TMA includes breast cancer tissues from 147 NHB, 168 H/L, and 112 NHW women subtyped into TNBC (n = 85), Her2 + (n = 26), and Luminal (n = 119). Survival outcomes or genotyping for determining genetic ancestry were not allowed for samples from some of the institutions. Some archival samples were not subtyped with ER, PR, or Her2. Another major limitation is that the TMA does not contain enough patients from different ethnicities and races to make statistically sound conclusions about expression within pathological subtypes in specific races (e.g. NHB vs. NHW) or ethnicities (non-H/L vs. H/L). A sample size of at least 100 tumors per ethnic/racial category or subtype would be needed to achieve an 85% power to detect the difference (50% versus 20%) using Fisher exact test and a two-sided 5% Type I error. A minor technical limitation is that very rarely were cores lifted and were lost during the staining procedure and thus the number of samples for each marker for each race and ethnicity slightly varies.
Immunohistochemistry and scoring
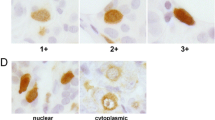
Tissue slides were de-paraffinized in xylene and rehydrated in 100%, 95%, 80%, and 75% ethanol followed by a distilled H2O wash. Endogenous peroxidase was blocked with 3% hydrogen peroxide for 15 min at room temperature. Incubation of 40 min for antigen retrieval was done using a citrate antigen retrieval solution that was preheated to 95 ℃ and then allowed to cool down for 20 min. Tissues were then incubated in primary antibody for TTK (1:100) (Cell Signal #5469S), E-cadherin (1:300) (Cell Signal #3195S), Vimentin (1:200) (Cell Signal #5741S), and Ki67 (1:200) (Cell Signal #9449S) (or PBS for negative controls) overnight at 4–8 ℃ in a sealed humid chamber. Tissues were then incubated with a biotin-conjugated secondary antibody solution for 30 min in the humid chamber. The secondary antibody was included in the Super Sensitive Link Label IHC kit (Cat. No. LP000-ULE, BioGenex, Fremont, CA); this same kit was used in subsequent steps for signal development following the manufacturer’s instructions. For slide mounting, tissues were dehydrated with 85%, 90%, 95%, and 100% ethanol and lastly incubated in xylene, oven-dried at 37 ℃ for 30 min, and sealed with permanent mounting medium and coverslips. Slides that were used for pathology analyses were counterstained with hematoxylin–eosin. Immuno-stained slides were independently and blindly scored for the number of positive cells by the board-certified pathologist Dr. Marilin Rosa. The whole tumor area was scored to account for tumor heterogeneity with at least four 40X visual fields per core counted. Pathologists used a 0 to 5 scoring system, in which a score of 0 meant 0% positive cells per 40X visual field, and 1, 2, 3, 4, and 5 meant less than 1%, 1–10%, 11–33%, 34–66%, and 67–100% positive cells per 40X visual field, respectively. TMA slides were digitally imaged with a Leica Aperio AT2 slide scanner where additional scoring was conducted using the Aperio’s Positive Pixel Count algorithm by Mr. Joseph Johnson at the Moffitt Cancer Center’s Imaging Core. No data points or subjects were excluded from our analyses.
Statistical analysis
Descriptive statistics for TTK or TBK1 cohort were done using compareGroups r package. For all categorical variables frequency (percentage) is presented. The associations between categorical clinic variables and each biomarker score were evaluated using the Chi-square test when each biomarker score was treated as the categorical variable while using the Kruskal–Wallis test when the score was treated as the continuous variable. Bioinformatic statistical analysis of TCGA and/or METABRIC datasets from the cBioportal was done using a T-test (2-tails, unequal variance).
Results
The expression of centrosome-mitotic kinase mRNAs co-occurs with epithelial-to-mesenchymal markers
We assessed the expression of TTK and TBK1 mRNAs using the METABRIC database, using the cBioPortal for Cancer Genomics, an open-access resource for multidimensional cancer genomics datasets analysis tool [51,52,53]. METABRIC determined global gene expression in over 2000 patients using RNA seq; this database subtyped breast tumors into molecular subtypes (Luminal A or B, Her2 + , Basal, and Normal-like) using PAM50 analysis. The analysis was done using Luminal A breast cancer as the baseline since it is the molecular subtype with the best prognosis [19]. In contrast, basal breast cancers (over 70% of which are TN, or Her2-ER-PR-) have the worst prognosis. A previous publication from our laboratory using the same database showed significant overexpression of Nek2 in Claudin Low, Luminal B, Her2 + , and Basal relative to Luminal A breast cancers [35]. In addition, we have published that the overexpression of Nek2 or TTK mRNA is associated with poor overall- and relapse-free survival of breast cancer patients [36]. TBK1 mRNA is significantly overexpressed in Luminal B breast cancers and significantly underexpressed in basal breast cancers (Fig. 1A). TTK mRNA is significantly overexpressed in Claudin-Low, Luminal B, Her2 + , and basal breast cancers (Fig. 1B).

TBK1 and TTK are overexpressed in different breast cancer subtypes. METABRIC (RNA seq Z values) analysis of mRNA expression of TBK1 and TTK by breast cancer molecular subtype classification. cBioPortal analyses of mRNA expression of TBK1 and TTK mitotic kinases in lobular and ductal breast cancer subtypes determined by PAM50 molecular subtyping, n = 2509. A z-score threshold ± 2.0 was used for optimal results. Significance was addressed with ANOVA
Next, we examined the gene expression of TTK and TBK1 mRNAs in different subtypes of breast cancers using TCGA (n = 996 breast cancers) [54] and METABRIC (n = 1904 breast cancers), Table 1. This analysis found more frequent upregulation of TTK in basal breast cancers (31.6% in TCGA and 32.2% in METABRIC) than in other subtypes. TBK1 was overexpressed in some basal breast cancer patients (2.3% in TCGA and 2% in METABRIC), and downregulated in other basal breast cancer patients (5.3% in TCGA and 12% in METABRIC). Notably, TBK1 is overexpressed in 26.7% of TCGA breast cancers that do not fall within the molecular classifications, or that failed to classify. The differences between data obtained through METABRIC and TCGA may include technical differences in performing the assays (for example, METABRIC data was obtained using Agilent microarray platforms and TCGA used RNA seq), as well as because they sample different populations (METABRIC includes population from the United Kingdom and Canada, while TCGA includes population from the United States of America).
The expression of centrosome-mitotic kinase mRNAs is elevated in non-Hispanic black women with breast cancer
We examined the TCGA dataset to understand the differences in the mRNA expression of Nek2 (Fig. 2A), TTK (Fig. 2B), and TBK1 (Fig. 2C) in NHW (n = 743), NHB (n = 187), and H/L (n = 39) populations with breast cancer based on their self-reported race and ethnicity. This analysis revealed that there were significant differences in the expression of the three kinases between NHB versus NHW, with Nek2 and TTK being overexpressed and TBK1 underexpressed in NHB (Fig. 2A–C). However, the H/L versus NHW differences were not significant, perhaps due to the limited sample size (n = 39), and it is known that TCGA did not recruit sufficient numbers of ethnic and racial minorities with breast cancer [57]. Therefore, we calculated the power to detect differences (G*Power 3.1), estimated based on the observed NHB versus NHW results for three kinases. Assuming an alpha level of 0.015 (three kinases), and differences observed in Nek2 (NHW observed mean: 16.53, sd: 1.99; NHB observed mean: 17.30, sd = 1.48), yielded an effect size of 0.4. This corresponds to 99% power to detect a difference between NHB and NHW populations. Using the sample size for H/L (n = 39) with the same parameters yields a power of 49.9% suggesting that the H/L cohort in TCGA is too small to adequately assess these differences. To achieve 90% power would require 98 H/L samples. A similar TCGA analysis done with ancestry [58] revealed that the expression of Nek2 and TTK is elevated in subjects with over 50% African ancestry (Fig. 2D, E). On the other hand, TBK1 is overexpressed in patients with 50% African ancestry or less (Fig. 2F).

The mRNA expression of mitotic kinases in different racial and ethnic groups. Expression patterns of Nek2, TTK, and TBK1 in breast cancer patients from TCGA (A–C). A z-score threshold ± 2.0 was used for optimal results. P-values were calculated using a pairwise ANOVA t-test and a Dunn analysis for the Kruskal–Wallis Test. The results for the three kinases resulted in P < 2.96e-06 to 7.3e-08 (***). Expression of Nek2, TTK, and TBK1 as a function of ancestry. P-values were calculated using the Kruskal–Wallis Test.
We also performed a TCGA expression analysis of mRNA levels by self-reported race, ethnicity, and subtype (Table 2). This analysis has some rigor limitations due to the limited sample size. Nevertheless, this indicated that TTK and Nek2 are overexpressed in NHB women, and TBK1 in NHW, when all breast cancers are taken into consideration; this result closely follows the ancestry data presented in Fig. 2. TTK and TBK1 are significantly overexpressed in NHW women with basal breast cancers, and TTK in basal and Luminal A breast cancers from H/L women. TTK and Nek2 are significantly overexpressed in NHB women with breast cancers that do not fall within any specific molecular classification, or that failed to classify (other). The results indicate that there are racial, ethnic and subtype-specific patterns of mRNA expression of the centrosome-mitotic kinases TTK, Nek2, and TBK1.
A side-by-side comparison of mRNA levels of several mitotic regulators was done by race, using the TCGA database (Additional file 1: Fig. S1). This analysis indicates that the mRNA levels of multiple mitotic regulators, including TTK, Nek2, PLK1, Cyclin B1, BUB1, Aurora kinases A and B, and NDC80 (also known as HEC1) are elevated in breast cancers in NHB women. When analyzed by subtype, PLK1 and Aurora kinase B are significantly elevated in TNBC from NHB women, while TTK and TBK1 are significantly elevated in NHW women with TNBC. NHW women with Her2 + breast tumors significantly overexpress TTK, TBK1, Nek2, BUB1, and SGOI. The most common breast cancer subtype is Luminal A; NHB women with Luminal A breast cancers significantly overexpress PLK1, AURKB, and NDC80, while TBK1 is significantly overexpressed in Luminal A breast cancers from NHW women. AURKB is overexpressed in Luminal B breast cancers in NHB women. All mitotic regulators analyzed except TBK1 are significantly overexpressed in breast cancers that do not fall under a traditional subtype, or that failed to classify.
In addition, several transcription factors, including FOXM1, E2F1, E2F2, and E2F3, and c-Myc are known to regulate the expression of key cell cycle regulators. Therefore, we performed the same analysis as above and determined that all are significantly overexpressed in breast cancers in NHB women (Additional file 1: Fig. S2). E2F1 and c-Myc are overexpressed in basal breast cancers from NHB women, FoxM1 in Her2 + breast cancers from NHW women, FoxM1, E2F1 and E2F2 in Luminal A breast cancers from NHB women. Similarly to the patterns of expression of mitotic kinases in breast cancers that do not fall under traditional classification (or that failed to classify) FOXM1, E2F1, E2F2, E2F3, and c-Myc are overexpressed in that subtype.
Saavedra and Chellappan’s labs have demonstrated that the silencing of Nek2, TTK, or TBK1 can individually modulate rates of centrosome amplification-driven chromosome instability and aneuploidy [35, 39, 41, 59, 60]. Therefore, we performed TCGA analysis of the average aneuploidy index (0 representing no aneuploidy, and 35 maximal aneuploidy) in NHB, NHW, H/L, and Non-H/L to determine if it is significantly higher in particular subtypes, race or ethnicity and if these indexes correlate with the mRNA expression of mitotic kinases. The average aneuploidy index is significantly higher in NHB relative to NHW women in all breast cancer subtypes (Table 3). There were no differences between H/L and Non-H/L in any of the subtypes, perhaps due to the small sample size of H/L women recruited to TCGA. Notably, dysregulated levels of all mitotic kinases, including Nek2 and TTK mRNAs presented in Table 2 and Additional file 1: Figure S1 correlate with increased aneuploidy in all breast cancer subtypes but only dysregulated expression of PLK1 and AURKB correlate with higher aneuploidy indexes in NHB women with basal breast cancers. This suggests that mitotic kinase overexpression may in part contribute to the overall higher aneuploidy indexes in NHB women.
TTK expression correlates with EMT and proliferation biomarkers
The expression of several surrogate markers of poor prognosis, including TTK, TBK1, E-cadherin (low levels associated with EMT), Vimentin (high levels in mesenchymal states), and Ki67 (proliferation marker) was assessed through immunohistochemical (IHC) staining of TMAs from the NCI BMaP-3 region (now BMaP region 2) (Fig. 3A). Nek2 and pH3 IHCs were done, but the pathologist determined that the staining was not consistent between slides. This TMA is unique since it is the first microarray that contained a similar number of breast cancer patients from different ethnic and racial groups; patient characteristics, including average age, ethnicity, race, and country of origin have been published [50]. Results indicate that TTK, Ki67, and Vimentin are significantly expressed in the TNBC subtype (Fig. 3B). These results are consistent with the nature of TNBC, which has high mitotic indexes and is overrepresented among metastatic breast cancers [61, 62].

A breast cancer tissue microarray showing TTK correlates with EMT and proliferation biomarkers in different breast cancer pathological subtypes. A. Representative IHC images using several surrogate markers of breast cancer (40X). The scale = 50 microns. Mean Allred scores of the indicated proteins related to pathological subtypes B. p-TBK1 levels were assessed in TNBC patients from the USA. P-values were derived from the Kruskal–Wallis Test
Correlation of biomarker scores with clinical variables within the breast cancer cohort
Allred's score [63] from the TMA results for the five biomarkers TTK, TBK1, Vimentin, E-cadherin, and Ki67 were categorized as non-expression (Allred score = 0) and expression (Allred score > 0). Comparisons were done using Chi-squared tests (or Fisher’s exact test if the expected frequencies are < 5). We evaluated associations of the TTK cohort with different variables including race (NHB compared to NHW), ethnicity (Non-H/L vs. H/L), race and ethnicity (NHB, NHW, and H/L), ER, PR, Her2, and mean score of the other biomarkers (Vimentin, E-cadherin, and Ki67), Table 4. TTK expression is significantly elevated in NHW relative to NHB, in non-Hispanics (NHW and NHB) relative to H/L, and NHW relative to NHB and H/L. In addition, TTK expression is more highly overexpressed in TNBC, Her2 + , and Other subtypes relative to Luminal (ER + PR +) subtypes. TTK expression correlates with higher expression of Vimentin, E-cadherin, and Ki67.
Next, we analyzed the Vimentin score with the clinical variables (Additional file 1: Table S1). The expression of Vimentin is significantly elevated in NHW patients relative to NHB patients, and NHW relative to NHB and H/L breast cancer patients. Vimentin levels are higher in TNBC relative to other breast cancer subtypes. Vimentin levels also correlated with TTK and Ki67 expression, and it was inversely correlated with the expression of E-cadherin.
Analysis of the correlation of E-cadherin with the clinical variables (Additional file 1: Table S2) does not show a correlation between E-cadherin with race. The analysis showed that E-cadherin levels are significantly higher in non-H/L relative to H/L, and in NHB and NHW when compared to H/L. There are no significant differences in the levels of E-cadherin between different breast cancer subtypes or with proliferation markers. There is a significant correlation between high E-cadherin expression with TTK expression, and it is inversely correlated with the expression of vimentin. When we analyzed the Ki67 score with the clinical variables (Additional file 1: Table S3) the expression of Ki67 is significantly higher in NHW relative to NHB, in non-H/L relative to H/L, and NHW relative to NHB and H/L. Ki-67 levels are higher in TNBC relative to other subtypes. Ki-67 significantly correlates with high TTK and Vimentin expression. We did not find a correlation with E-cadherin (P = 0.705).
We then analyzed a smaller cohort of TNBC patients from Moffitt Cancer Center (N = 129) for the expression of TTK, active (p-TBK1), Ki-67, Vimentin, and E-cadherin in NHB and NHW patients. In this smaller cohort of patients, TTK levels do not correlate with markers of EMT or proliferation (Additional file 1: Table S4). As the results presented above for a larger cohort, TTK overexpression is higher in NHW relative to NHB patients. There are no correlations between p-TBK1 expression and proliferation, or EMT markers (Table 5). Elevated Vimentin, E-cadherin, or Ki-67 levels do not correlate with levels of other surrogate markers of prognosis in this smaller cohort (Additional file 1: Tables S5, S6, S7).
Discussion
Besides their role in regulating centrosome homeostasis and mitosis, centrosome-associated mitotic kinases can drive cancer progression. Several of these kinases, including Nek2 and TTK, can drive early intermediates to metastasis, including the epithelial-to-mesenchymal transition, cell migration, and cell invasion [24, 35, 49]. Polo-like kinases and Aurora kinases showed efficacy in recent clinical trials; however, these drugs also appear to have limited efficacy in solid tumors as single agents [64,65,66,67] perhaps due to overlapping roles of mitotic kinases during mitosis [45]. Thus, mitotic-based therapies are currently been refined, and small molecule inhibitors against several centrosome and mitotic regulators are currently in clinical trials, including a phase II trial with the inhibitor ENMD-2076, which is specific against the Aurora kinase A and angiogenesis kinases, against metastatic, triple-negative breast cancers [68]. That clinical trial found that the clinical benefit rate (patients that achieved partial, complete responses or stable disease) was 16.7% in 6 months after commencing treatment, and 27.8% in 4 months after commencing treatment; the most common side effects were hypertension, fatigue, diarrhea, and nausea. None of these patients achieved complete responses. Another phase II clinical trial that focused on breast cancer patients utilized the Aurora kinase A inhibitor Alisertib along with Paclitaxel compared to Paclitaxel alone [69]. The 22 month progression-free survival was significantly reduced when Alisertib was added to Paclitaxel, while the differences in overall survival were non-significant. However, the addition of Alisertib enhanced grade 3 or 4 adverse effects, including neutropenia, sepsis, anemia, diarrhea, and stomatitis or oral mucositis. When considering the TNBC cohort only, the addition of Paclitaxel and Alisertib significantly reduced progression-free survival, while a trend toward significance was observed in overall survival (P = 0.09). Results from TTK clinical trials have recently been published, and some adverse effects (severe anemia, fatigue, and neutropenia at the highest doses) were reported with combined treatments with TTK inhibitor S81694 [70], or with Paclitaxel and TTK inhibitor BAY1217389 [71] in patients with diverse solid tumors. The results are encouraging since 32–34% of patients achieved stable disease. However, > 3 neutropenia was attributed to increases in TTK inhibitor. These results suggest that these inhibitors must be used in combination with other drugs that include microtubule agents. Some TBK1 inhibitors are FDA approved for inflammatory diseases (e.g. Amlexanox) and derivatives are been tested pre-clinically as anticancer agents [29, 72,73,74]. Our previous work shows that co-inhibiting the mitotic kinases TTK and TBK1 may represent a more effective way of suppressing mitotic markers such as Cyclin B expression, the phosphorylation of the mitotic markers Aurora kinases A, B, and C, pH3, and cell viability relative to the single inhibition of either kinase [31].
In the present study, we evaluated mRNA expression patterns of the mitotic kinases Nek2, Mps1/TTK, and TBK1, as well as the expression and association of these proteins with biomarkers of proliferation (Ki67) and EMT (E-cadherin and Vimentin) by using a novel breast cancer TMA. Besides its role in the cell cycle and SAC, TTK is overexpressed and correlates with advanced stages in several cancer types such as NSCLC [75, 76], prostate [77], colon [78], and breast [49, 79, 80] cancers. Previous studies analyzing TTK expression from breast cancer biopsies for each of the main breast cancer subtypes including TNBC, Her2, Luminal A, and Luminal B found that TTK overexpression was specific for the TNBC subtype [79].
NIMA-related kinase 2 (Nek2) is understudied in cancer compared with other cell cycle regulators. However, Nek2 is overexpressed in many cancers, including those of the liver, lungs, pancreas, glioma, colon, prostate, and breast [81,82,83,84,85,86,87]. Nek2 overexpression has been described as a prognostic biomarker for disease progression and patient survival in different cancer types, including breast cancer [87,88,89]. TTK and Nek2 (along with VRK1, MASTL, SRPK1, CDC7, AURKA, PLK1, AURKB, CHEK1, CDC2, BUB1, MELK, PBK, BUBB1, and PLK4) belong to a 16-kinase mRNA signature that can identify basal breast cancers and a subset of poor-prognosis Luminal patients [90]. In this study, Nek2 also showed a high overall expression in samples from breast cancer patients, which is consistent with our previous studies, as well as other studies highlighting elevated Nek2 gene expression in breast cancer, including the TNBC subtype [35, 91]. Despite the general overexpression of Nek2 and TTK shown in breast cancer, no clear information exists on whether this is a general or specific pattern related to the genetic context of patients. Limited evidence regarding the contribution of ancestry and mitotic kinase gene expression exists. A meta-analysis conducted by Wang et al. 2019, identified Nek2 as a worse prognostic predictor in solid cancers for Asians [87]. NHB and H/L are typically more severely affected by breast cancer disparities when compared with NHW [4, 92,93,94]. In the present study, we demonstrate that NHB had the highest gene expression for the Nek2 and TTK mRNAs, as well as the mRNAs of other mitotic regulators, including PLK1, CCNB1, BUB1, AURKA, AURKB, and NDC80 (also known as HEC1), while NHW had the higher levels of TBK1. When we analyzed the gene expression of these kinases by subtype, TTK mRNA is more highly overexpressed in basal breast cancers from NHW and H/L patients, and Luminal A patients from H/L. However, it is known that TNBCs have a higher prevalence in NHB and H/L compared to NHW and that more studies with proportional subtype representation are needed. PLK1 and AURKB are more highly overexpressed in basal breast cancers from NHB. All the mitotic regulators above, including Nek2 and TTK, are also overexpressed in non-classified breast tumors. No explanation was given for this unclassified group in the original TCGA manuscript [54]; this group could also represent tumors that failed to classify due to technical reasons. The overexpression of Nek2 and TTK also correlates with the higher aneuploidy indexes in NHB women. On the other hand, TBK1 mRNA was significantly overexpressed in all breast tumors from NHW patients, and in NHW patients with basal, and Luminal A subtypes. However, when protein levels of TTK, and TBK1 are analyzed by immunohistochemistry, the patterns of expression differ when compared to their mRNA levels. For example, while levels of TTK mRNA were higher in NHB and H/L women, its protein levels were significantly elevated in NHW women and non-H/L relative to H/L. This may be due to post-transcriptional mechanisms that may lead to changes in the protein stability of these kinases. It may also be due to the mRNAs and the protein samples originating from different cohorts (the mRNA from TCGA and the protein samples from the Puerto Rico Biobank). Future studies will be conducted using a new generation TMA where the tumor samples will also be RNA and DNA seq, so the data will exactly match. We have shown that the overexpression of E2Fs alters the protein stability of several mitotic regulators, including Cyclin B1, SgoI, and BubR1 [36] and similar mechanisms may also govern the stability of TTK and TBK1. Nevertheless, our data revealed important associations between TTK expression and subtypes that associate with a poorer prognosis, including TNBC and Her2 + breast cancers. TTK overexpression also correlated with surrogate markers of poor prognosis, including EMT (higher Vimentin levels) and with a higher proliferation index. There were also correlations of Vimentin overexpression with breast cancers in NHW women, with the TNBC subtype and with Ki67, and an inverse correlation with E-cadherin. The major difference between H/L and non-H/L was the lower levels of E-cadherin marker in H/L relative to NHB and NHW women. Regarding Ki67, it was higher in NHW women and non-H/L; H/L women had the lowest proliferation index. These results may have clinical implications since they suggest that EMT in H/L may occur through different mechanisms relative to non-H/L women since E-cadherin levels are significantly higher in the former. The lower levels of Ki67 in H/L may also be of clinical significance since high proliferation indexes are highly correlated to better responses to docetaxel-based chemotherapy in ER + breast cancer patients [95].
A possible mechanism involved in the regulation of the targets described in this study could be the Forkhead box protein M1 (FOXM1), a member of the FOX family of transcription factors that plays a key role in the G2/M phase of the cell cycle, controlling proliferation and genomic stability [96,97,98]. TCGA analysis showed a significant increase in the relative expression of FOXM1 in All, Luminal A, and unclassified (or that failed to classify) breast cancers for NHB, and a significant increase of relative expression in Her2 for NHW (Additional file 1: Fig. S1). Among the cell cycle genes regulated by FOXM1 are Plk1, Cyclin B2, CENPF, and Nek2. Thus, future studies through this transcription factor can establish specific molecular mechanisms of action for these mitotic kinases. Another potential mechanism (non-mutually exclusive with FoxM1 dysregulation) is that the E2Fs may also contribute to the dysregulation of mitotic regulation in NHB women. Our work has shown that Nek2 and Plk4 mRNAs are directly regulated by the E2F activators [38], while others have shown that Aurora Kinase A is a transcriptional target of E2F [99]; likewise, PLK1 is an E2F target [100].
Given the significant disparities in breast cancer patients, centrosome-associated mitotic kinases could be important targets to be evaluated in the context of genetic differences and their related significant health disparities in breast cancer.
Conclusions
In summary, we established different correlations of centrosome-associated mitotic kinases with biomarkers from the EMT in a novel breast cancer TMA with tumor samples derived from women with different ethnic backgrounds including NHB, NHW, and C-H/L. Thus, our results showed high expression of TTK, Ki67, and Vimentin in TN tumors, while low expression of E-cadherin. TTK, but not TBK1, showed significant correlations with all the clinical variables measured. On the other hand, TCGA dataset analysis revealed that the mRNA levels of several centrosome-mitotic kinases were significantly higher in NHB versus NHW women. However, the H/L results were not significant due to the limited sample size. Thus, TTK and Nek2 may be future potential targets for TNBC treatment in NHB and H/L populations.
Availability of data and materials
All the data generated as part of this study are included in this published article and its Additional files.
References
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 Countries. CA Cancer J Clin. 2021;71(3):209–49.
Iqbal J, Ginsburg O, Rochon PA, Sun P, Narod SA. Differences in breast cancer stage at diagnosis and cancer-specific survival by race and ethnicity in the United States. JAMA. 2015;313(2):165–73.
Ooi SL, Martinez ME, Li CI. Disparities in breast cancer characteristics and outcomes by race/ethnicity. Breast Cancer Res Treat. 2011;127(3):729–38.
Akinyemiju T, Moore JX, Ojesina AI, Waterbor JW, Altekruse SF. Racial disparities in individual breast cancer outcomes by hormone-receptor subtype, area-level socio-economic status and healthcare resources. Breast Cancer Res Treat. 2016;157(3):575–86.
Lund MJ, Trivers KF, Porter PL, Coates RJ, Leyland-Jones B, Brawley OW, et al. Race and triple negative threats to breast cancer survival: a population-based study in Atlanta. GA Breast Cancer Res Treat. 2009;113(2):357–70.
Lund MJ, Butler EN, Bumpers HL, Okoli J, Rizzo M, Hatchett N, et al. High prevalence of triple-negative tumors in an urban cancer center. Cancer. 2008;113(3):608–15.
Pinheiro PS, Sherman RL, Trapido EJ, Fleming LE, Huang Y, Gomez-Marin O, et al. Cancer incidence in first generation U.S. Hispanics: cubans, mexicans, puerto ricans, and new latinos. Cancer Epidemiol Biomarkers Prev. 2009;18(8):2162–9.
Banegas MP, Leng M, Graubard BI, Morales LS. The risk of developing invasive breast cancer in hispanic women: a look across Hispanic subgroups. Cancer. 2013;119(7):1373–80.
Pinheiro PS, Callahan KE, Siegel RL, Jin H, Morris CR, Trapido EJ, et al. Cancer mortality in Hispanic ethnic groups. Cancer Epidemiol Biomarkers Prev. 2017;26(3):376–82.
Martinez Tyson D, Medina-Ramirez P, Flores AM, Siegel R, Aguado LC. Unpacking hispanic ethnicity-cancer mortality differentials among Hispanic subgroups in the United States, 2004–2014. Front Public Health. 2018;6:219.
Hines LM, Risendal B, Byers T, Mengshol S, Lowery J, Singh M. Ethnic disparities in breast tumor phenotypic subtypes in Hispanic and non-Hispanic white women. J Womens Health. 2011;20(10):1543–50.
Howlader N, Altekruse SF, Li CI, Chen VW, Clarke CA, Ries LA, et al. US incidence of breast cancer subtypes defined by joint hormone receptor and HER2 status. J Natl Cancer Inst. 2014;106:5.
Banegas MP, Li CI. Breast cancer characteristics and outcomes among Hispanic black and hispanic white women. Breast Cancer Res Treat. 2012;134(3):1297–304.
Sineshaw HM, Gaudet M, Ward EM, Flanders WD, Desantis C, Lin CC, et al. Association of race/ethnicity, socioeconomic status, and breast cancer subtypes in the national cancer data base (2010–2011). Breast Cancer Res Treat. 2014;145(3):753–63.
Chen L, Li CI. Racial disparities in breast cancer diagnosis and treatment by hormone receptor and HER2 status. Cancer Epidemiol Biomarkers Prev. 2015;24(11):1666–72.
Huo D, Ikpatt F, Khramtsov A, Dangou JM, Nanda R, Dignam J, et al. Population differences in breast cancer: survey in indigenous African women reveals over-representation of triple-negative breast cancer. J Clin Oncol. 2009;27(27):4515–21.
Jusino S, Rivera-Rivera Y, Chardon-Colon C, Ruiz-Justiz AJ, Velez-Velazquez J, Isidro A, et al. E2F3 drives the epithelial-to-mesenchymal transition, cell invasion, and metastasis in breast cancer. Exp Biol Med. 2021. https://doi.org/10.1177/15353702211035693.
D’Arcy M, Fleming J, Robinson WR, Kirk EL, Perou CM, Troester MA. Race-associated biological differences among luminal a breast tumors. Breast Cancer Res Treat. 2015;152(2):437–48.
Sorlie T, Perou CM, Tibshirani R, Aas T, Geisler S, Johnsen H, et al. Gene expression patterns of breast carcinomas distinguish tumor subclasses with clinical implications. Proc Natl Acad Sci USA. 2001;98(19):10869–74.
Warner ET, Tamimi RM, Hughes ME, Ottesen RA, Wong YN, Edge SB, et al. Racial and ethnic differences in breast cancer survival: mediating effect of tumor characteristics and sociodemographic and treatment factors. J Clin Oncol. 2015;33(20):2254–61.
Goel N, Yadegarynia S, Lubarsky M, Choi S, Kelly K, Balise R, et al. Racial and ethnic disparities in breast cancer survival: emergence of a clinically distinct hispanic black population. Ann Surg. 2021;274(3):e269–75.
Garcia-Aranda M, Redondo M. Protein kinase targets in breast cancer. Int J Mol Sci. 2017;18:12.
Shah NP, Tran C, Lee FY, Chen P, Norris D, Sawyers CL. Overriding imatinib resistance with a novel ABL kinase inhibitor. Science. 2004;305(5682):399–401.
Colon-Marrero S, Jusino S, Rivera-Rivera Y, Saavedra HI. Mitotic kinases as drivers of the epithelial-to-mesenchymal transition and as therapeutic targets against breast cancers. Exp Biol Med. 2021. https://doi.org/10.1177/1535370221991094.
Marques S, Fonseca J, Silva PM, Bousbaa H. Targeting the spindle assembly checkpoint for breast cancer treatment. Curr Cancer Drug Targets. 2015;15(4):272–81.
Wang Y, Jin F, Higgins R, McKnight K. The current view for the silencing of the spindle assembly checkpoint. Cell Cycle. 2014;13(11):1694–701.
Tanaka K, Hirota T. Chromosome segregation machinery and cancer. Cancer Sci. 2009;100(7):1158–65.
Pachis ST, Kops G. Leader of the SAC: molecular mechanisms of Mps1/TTK regulation in mitosis. Open Biol. 2018;8:8.
Antonia RJ, Hagan RS, Baldwin AS. Expanding the view of Ikk: new substrates and new biology. Trends Cell Biol. 2021;31(3):166–78.
Pillai S, Nguyen J, Johnson J, Haura E, Coppola D, Chellappan S. Tank binding kinase 1 is a centrosome-associated kinase necessary for microtubule dynamics and mitosis. Nat Commun. 2015;6:10072.
Maan M, Agrawal NJ, Padmanabhan J, Leitzinger CC, Rivera-Rivera Y, Saavedra HI, et al. Tank binding kinase 1 modulates spindle assembly checkpoint components to regulate mitosis in breast and lung cancer cells. Biochim Biophys Acta Mol Cell Res. 2021;1868(3):118929.
Faragher AJ, Fry AM. Nek2A kinase stimulates centrosome disjunction and is required for formation of bipolar mitotic spindles. Mol Biol Cell. 2003;14(7):2876–89.
Fry AM, Mayor T, Meraldi P, Stierhof YD, Tanaka K, Nigg EA. C-Nap1, a novel centrosomal coiled-coil protein and candidate substrate of the cell cycle-regulated protein kinase Nek2. J Cell Biol. 1998;141(7):1563–74.
Liu Q, Hirohashi Y, Du X, Greene MI, Wang Q. Nek2 targets the mitotic checkpoint proteins Mad2 and Cdc20: a mechanism for aneuploidy in cancer. Exp Mol Pathol. 2010;88(2):225–33.
Rivera-Rivera Y, Marina M, Jusino S, Lee M, Velazquez JV, Chardon-Colon C, et al. The Nek2 centrosome-mitotic kinase contributes to the mesenchymal state, cell invasion, and migration of triple-negative breast cancer cells. Sci Rep. 2021;11(1):9016.
Lee M, Rivera-Rivera Y, Moreno CS, Saavedra HI. The E2F activators control multiple mitotic regulators and maintain genomic integrity through Sgo1 and BubR1. Oncotarget. 2017;8(44):77649–72.
Lee M, Oprea-Ilies G, Saavedra HI. Silencing of E2F3 suppresses tumor growth of Her2+ breast cancer cells by restricting mitosis. Oncotarget. 2015. https://doi.org/10.1863/oncotarget.5686.
Lee MY, Moreno CS, Saavedra HI. E2F activators signal and maintain centrosome amplification in breast cancer cells. Mol Cell Biol. 2014;34(14):2581–99.
Harrison Pitner MK, Saavedra HI. Cdk4 and nek2 signal binucleation and centrosome amplification in a her2+ breast cancer model. PLoS ONE. 2013;8(6):e65971.
Adon AM, Zeng X, Harrison MK, Sannem S, Kiyokawa H, Kaldis P, et al. Cdk2 and Cdk4 regulate the centrosome cycle and are critical mediators of centrosome amplification in p53-null cells. Mol Cell Biol. 2010;30(3):694–710.
Zeng X, Shaikh FY, Harrison MK, Adon AM, Trimboli AJ, Carroll KA, et al. The ras oncogene signals centrosome amplification in mammary epithelial cells through cyclin D1/Cdk4 and Nek2. Oncogene. 2010;29(36):5103–12.
Levine MS, Bakker B, Boeckx B, Moyett J, Lu J, Vitre B, et al. Centrosome amplification is sufficient to promote spontaneous tumorigenesis in mammals. Dev Cell. 2017;40(3):313–22.
Weaver BA, Silk AD, Cleveland DW. Low rates of aneuploidy promote tumorigenesis while high rates of aneuploidy cause cell death and tumor suppression. Cell Oncol. 2008;30(5):453.
Godinho SA, Picone R, Burute M, Dagher R, Su Y, Leung CT, et al. Oncogene-like induction of cellular invasion from centrosome amplification. Nature. 2014. https://doi.org/10.1038/nature13277.
Henriques AC, Ribeiro D, Pedrosa J, Sarmento B, Silva PMA, Bousbaa H. Mitosis inhibitors in anticancer therapy: when blocking the exit becomes a solution. Cancer Lett. 2019;440–441:64–81.
Dominguez-Brauer C, Thu KL, Mason JM, Blaser H, Bray MR, Mak TW. Targeting mitosis in cancer: emerging strategies. Mol Cell. 2015;60(4):524–36.
Rivera-Rivera Y, Saavedra HI. Centrosome—a promising anti-cancer target. Biologics. 2016;10:167–76.
Jusino S, Saavedra HI. Role of E2Fs and mitotic regulators controlled by E2Fs in the epithelial to mesenchymal transition. Exp Biol Med. 2019. https://doi.org/10.1177/1535370219881360.
King JL, Zhang B, Li Y, Li KP, Ni JJ, Saavedra HI, et al. TTK promotes mesenchymal signaling via multiple mechanisms in triple negative breast cancer. Oncogenesis. 2018;7(9):69.
Seijo E, Lima D, Iriabho E, Almeida J, Monico J, Echeverri M, et al. Construction and validation of a multi-institutional tissue microarray of invasive ductal carcinoma from racially and ethnically diverse populations. Cancer Control. 2016;23(4):383–9.
Gao J, Aksoy BA, Dogrusoz U, Dresdner G, Gross B, Sumer SO, et al. Integrative analysis of complex cancer genomics and clinical profiles using the cBioPortal. Sci Signal. 2013;6:269.
Cerami E, Gao J, Dogrusoz U, Gross BE, Sumer SO, Aksoy BA, et al. The cBio cancer genomics portal: an open platform for exploring multidimensional cancer genomics data. Cancer Discov. 2012;2(5):401–4.
Curtis C, Shah SP, Chin SF, Turashvili G, Rueda OM, Dunning MJ, et al. The genomic and transcriptomic architecture of 2000 breast tumours reveals novel subgroups. Nature. 2012;486(7403):346–52.
Cancer Genome Atlas N. Comprehensive molecular portraits of human breast tumours. Nature. 2012;490(7418):61–70.
Nielsen TO, Parker JS, Leung S, Voduc D, Ebbert M, Vickery T, et al. A comparison of PAM50 intrinsic subtyping with immunohistochemistry and clinical prognostic factors in tamoxifen-treated estrogen receptor-positive breast cancer. Clin Cancer Res. 2010;16(21):5222–32.
Korde LA, Lusa L, McShane L, Lebowitz PF, Lukes L, Camphausen K, et al. Gene expression pathway analysis to predict response to neoadjuvant docetaxel and capecitabine for breast cancer. Breast Cancer Res Treat. 2010;119(3):685–99.
Spratt DE, Chan T, Waldron L, Speers C, Feng FY, Ogunwobi OO, et al. Racial/ethnic disparities in genomic sequencing. JAMA Oncol. 2016;2(8):1070–4.
Carrot-Zhang J, Chambwe N, Damrauer JS, Knijnenburg TA, Robertson AG, Yau C, et al. Comprehensive analysis of genetic ancestry and its molecular correlates in cancer. Cancer Cell. 2020;37(5):639–54.
Maan M, Agrawal NJ, Padmanabhan J, Leitzinger CC, Rivera-Rivera Y, Saavedra HI, et al. Tank binding kinase 1 modulates spindle assembly checkpoint components to regulate mitosis in breast and lung cancer cells. Biochim Biophys Acta Mol Cell Res. 2020. https://doi.org/10.1016/j.bbamcr.2020.
Lee MY, Marina M, King JL, Saavedra HI. Differential expression of centrosome regulators in Her2+ breast cancer cells versus non-tumorigenic MCF10A cells. Cell Div. 2014;9:3.
Kumar P, Aggarwal R. An overview of triple-negative breast cancer. Arch Gynecol Obstet. 2016;293(2):247–69.
Anders CK, Zagar TM, Carey LA. The management of early-stage and metastatic triple-negative breast cancer: a review. Hematol Oncol Clin North Am. 2013;27(4):737–49.
Allred DC, Harvey JM, Berardo M, Clark GM. Prognostic and predictive factors in breast cancer by immunohistochemical analysis. Mod Pathol. 1998;11(2):155–68.
Traynor AM, Hewitt M, Liu G, Flaherty KT, Clark J, Freedman SJ, et al. Phase I dose escalation study of MK-0457, a novel aurora kinase inhibitor, in adult patients with advanced solid tumors. Cancer Chemother Pharmacol. 2011;67(2):305–14.
Steeghs N, Eskens FA, Gelderblom H, Verweij J, Nortier JW, Ouwerkerk J, et al. Phase I pharmacokinetic and pharmacodynamic study of the aurora kinase inhibitor danusertib in patients with advanced or metastatic solid tumors. J Clin Oncol. 2009;27(30):5094–101.
Hofheinz RD, Al-Batran SE, Hochhaus A, Jager E, Reichardt VL, Fritsch H, et al. An open-label, phase I study of the polo-like kinase-1 inhibitor, BI 2536, in patients with advanced solid tumors. Clin Cancer Res. 2010;16(18):4666–74.
Bavetsias V, Linardopoulos S. Aurora kinase inhibitors: current status and outlook. Front Oncol. 2015;5:278.
Diamond JR, Eckhardt SG, Pitts TM, van Bokhoven A, Aisner D, Gustafson DL, et al. A phase II clinical trial of the aurora and angiogenic kinase inhibitor ENMD-2076 for previously treated, advanced, or metastatic triple-negative breast cancer. Breast Cancer Res. 2018;20(1):82.
O’Shaughnessy J, McIntyre K, Wilks S, Ma L, Block M, Andorsky D, et al. Efficacy and safety of weekly paclitaxel with or without oral alisertib in patients with metastatic breast cancer: a randomized clinical trial. JAMA Netw Open. 2021;4(4):e214103.
Schoffski P, Awada A, de la Bigne AM, Felloussi Z, Burbridge M, Cantero F, et al. First-in-man, first-in-class phase I study with the monopolar spindle 1 kinase inhibitor S81694 administered intravenously in adult patients with advanced, metastatic solid tumours. Eur J Cancer. 2022;169:135–45.
Atrafi F, Boix O, Subbiah V, Diamond JR, Chawla SP, Tolcher AW, et al. A phase I study of an MPS1 inhibitor (BAY 1217389) in combination with paclitaxel using a novel randomized continual reassessment method for dose escalation. Clin Cancer Res. 2021;27(23):6366–75.
Xiang S, Song S, Tang H, Smaill JB, Wang A, Xie H, et al. TANK-binding kinase 1 (TBK1): an emerging therapeutic target for drug discovery. Drug Discov Today. 2021. https://doi.org/10.1016/j.drudis.2021.
Thomson DW, Bergamini G. Recent progress in small molecule TBK1 inhibitors: a patent review (2015–2020). Expert Opin Ther Pat. 2021. https://doi.org/10.1080/13543776.2021.
Revach OY, Liu S, Jenkins RW. Targeting TANK-binding kinase 1 (TBK1) in cancer. Expert Opin Ther Targets. 2020;24(11):1065–78.
Chen X, Yu C, Gao J, Zhu H, Cui B, Zhang T, et al. A novel USP9X substrate TTK contributes to tumorigenesis in non-small-cell lung cancer. Theranostics. 2018;8(9):2348–60.
Chen J, Wu R, Xuan Y, Jiang M, Zeng Y. Bioinformatics analysis and experimental validation of TTK as a biomarker for prognosis in non-small cell lung cancer. Biosci Rep. 2020;40:10.
Chen S, Wang J, Wang L, Peng H, Xiao L, Li C, et al. Silencing TTK expression inhibits the proliferation and progression of prostate cancer. Exp Cell Res. 2019;385(1):111669.
Ling Y, Zhang X, Bai Y, Li P, Wei C, Song T, et al. Overexpression of Mps1 in colon cancer cells attenuates the spindle assembly checkpoint and increases aneuploidy. Biochem Biophys Res Commun. 2014;450(4):1690–5.
Maire V, Baldeyron C, Richardson M, Tesson B, Vincent-Salomon A, Gravier E, et al. TTK/hMPS1 is an attractive therapeutic target for triple-negative breast cancer. PLoS ONE. 2013;8(5):e63712.
Yuan B, Xu Y, Woo JH, Wang Y, Bae YK, Yoon DS, et al. Increased expression of mitotic checkpoint genes in breast cancer cells with chromosomal instability. Clin Cancer Res. 2006;12(2):405–10.
Wubetu GY, Morine Y, Teraoku H, Yoshikawa M, Ishikawa D, Yamada S, et al. High NEK2 expression is a predictor of tumor recurrence in hepatocellular carcinoma patients after hepatectomy. Anticancer Res. 2016;36(2):757–62.
Zhong X, Guan X, Liu W, Zhang L. Aberrant expression of NEK2 and its clinical significance in non-small cell lung cancer. Oncol Lett. 2014;8(4):1470–6.
Ning Z, Wang A, Liang J, Liu J, Zhou T, Yan Q, et al. Abnormal expression of Nek2 in pancreatic ductal adenocarcinoma: a novel marker for prognosis. Int J Clin Exp Pathol. 2014;7(5):2462–9.
Liu H, Liu B, Hou X, Pang B, Guo P, Jiang W, et al. Overexpression of NIMA-related kinase 2 is associated with poor prognoses in malignant glioma. J Neurooncol. 2017;132(3):409–17.
Cappello P, Blaser H, Gorrini C, Lin DC, Elia AJ, Wakeham A, et al. Role of Nek2 on centrosome duplication and aneuploidy in breast cancer cells. Oncogene. 2014;33(18):2375–84.
Zhang FB, Du Y, Tian Y, Ji ZG, Yang PQ. MiR-1299 functions as a tumor suppressor to inhibit the proliferation and metastasis of prostate cancer by targeting NEK2. Eur Rev Med Pharmacol Sci. 2019;23(2):530–8.
Wang X, Chen K, Liu H, Huang Z, Chen X, Yin L. Prognostic significance of NEK2 in human solid tumors: a systematic review and meta-analysis. Biosci Rep. 2019;39:1.
Lu L, Zhai X, Yuan R. Clinical significance and prognostic value of Nek2 protein expression in colon cancer. Int J Clin Exp Pathol. 2015;8(11):15467–73.
Marina M, Saavedra HI. Nek2 and Plk4: prognostic markers, drivers of breast tumorigenesis and drug resistance. Front Biosci. 2014;19:352–65.
Finetti P, Cervera N, Charafe-Jauffret E, Chabannon C, Charpin C, Chaffanet M, et al. Sixteen-kinase gene expression identifies luminal breast cancers with poor prognosis. Cancer Res. 2008;68(3):767–76.
Roberts MS, Sahni JM, Schrock MS, Piemonte KM, Weber-Bonk KL, Seachrist DD, et al. LIN9 and NEK2 are core regulators of mitotic fidelity that can be therapeutically targeted to overcome taxane resistance. Cancer Res. 2020;80(8):1693–706.
Danforth DN Jr. Disparities in breast cancer outcomes between caucasian and African American women: a model for describing the relationship of biological and nonbiological factors. Breast Cancer Res. 2013;15(3):208.
Dietze EC, Sistrunk C, Miranda-Carboni G, O’Regan R, Seewaldt VL. Triple-negative breast cancer in African-American women: disparities versus biology. Nat Rev Cancer. 2015;15(4):248–54.
Newman LA, Jenkins B, Chen Y, Oppong JK, Adjei E, Jibril AS, et al. Hereditary susceptibility for triple negative breast cancer associated with western sub-saharan African ancestry: results from an international surgical breast cancer collaborative. Ann Surg. 2019;270(3):484–92.
Penault-Llorca F, Andre F, Sagan C, Lacroix-Triki M, Denoux Y, Verriele V, et al. Ki67 expression and docetaxel efficacy in patients with estrogen receptor-positive breast cancer. J Clin Oncol. 2009;27(17):2809–15.
Costa RH. FoxM1 dances with mitosis. Nat Cell Biol. 2005;7(2):108–10.
Laoukili J, Kooistra MR, Bras A, Kauw J, Kerkhoven RM, Morrison A, et al. FoxM1 is required for execution of the mitotic programme and chromosome stability. Nat Cell Biol. 2005;7(2):126–36.
Wonsey DR, Follettie MT. Loss of the forkhead transcription factor FoxM1 causes centrosome amplification and mitotic catastrophe. Cancer Res. 2005;65(12):5181–9.
He L, Yang H, Ma Y, Pledger WJ, Cress WD, Cheng JQ. Identification of aurora-a as a direct target of E2F3 during G2/M cell cycle progression. J Biol Chem. 2008;283(45):31012–20.
Tategu M, Nakagawa H, Sasaki K, Yamauchi R, Sekimachi S, Suita Y, et al. Transcriptional regulation of human polo-like kinases and early mitotic inhibitor. J Genet Genomics. 2008;35(4):215–24.
Funding
This work has been supported in part by the Analytic Microscopy Core Facility at the H. Lee Moffitt Cancer Center & Research Institute, an NCI-designated Comprehensive Cancer Center (P30-CA076292), R01CA266046, PSM-U54-CA163071/MCC-U54-CA163068 (support from the Admin Core, Puerto Rico Biobank and the Quantitative Sciences Core), 2U54MD007587 (PRCTRC), 1U54GM133807-01A1 (Hispanic Alliance for Clinical and Translational Research), G12MD007579 (RCMI), and the Puerto Rico Science, Technology and Research. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Author information
Authors and Affiliations
Contributions
YRR, GV, and NJ conducted experiments and performed data normalization analyses; ANM provided input in experimental protocol, writing, and editing of the manuscript; JOJ obtained and organized the Aperio software data and provided input in the overall methodology and analysis; YRR wrote the manuscript; JL, D-TC, and SE performed statistical analyses; MR performed the pathological analysis; JD helped to obtain clinical data, provided input, and edited the manuscript; SPC and HIS provided overall experimental design and edited the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Immunostaining breast cancer tissue samples were done under the IRB protocol 160115-HS. De-identified data and biospecimens were obtained from the U56/U56’s Puerto Rico Biobank from previously consented patients through the IRB protocol 080121-IF.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1
: Figure S1. Average expression of mitotic kinases and regulators by breast cancer subtypes in NHBs and NHWs using the TCGA database. P-values were done by T-test (2-tails and unequal variance). The * (p≤0.05) refers to significance in NHB (relative to NHW) and the # (p≤0.05) refers to significance in NHW (relative to NHB). Figure S2. Average expression of FoxM1, E2Fs, and Myc transcription factors by breast cancer subtypes in NHB and NHW using the TCGA database. P-values were done by T-test (2-tails, unequal variance). The * refers to significance in NHBs (relative to NHW, p≤0.05) and the # refers to significance in NHWs (relative to NHB, p≤0.05). Table S1. The association of Vimentin score with the clinical variables in the total cohort. Table S2. The association of E-cadherin score with the clinical variables in the total cohort. Table S3. The association of Ki67 score with the clinical variables in the total cohort. Table S4. The association of TTK score with the clinical variables in the Moffitt Cancer Center’s TNBC cohort. Table S5. The association of Vimentin score with the clinical variables in the Moffitt Cancer Center’s TNBC cohort. Table S6. The association of E-cadherin score with the clinical variables in the Moffitt Cancer Center’s TNBC cohort. Table S7. The association of Ki67 score with the clinical variables in the Moffitt Cancer Center’s TNBC cohort.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Rivera-Rivera, Y., Vargas, G., Jaiswal, N. et al. Ethnic and racial-specific differences in levels of centrosome-associated mitotic kinases, proliferative and epithelial-to-mesenchymal markers in breast cancers. Cell Div 17, 6 (2022). https://doi.org/10.1186/s13008-022-00082-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13008-022-00082-3