
Abstract
Maintaining skeletal muscle mass is important for improving muscle strength and function. Hence, maximizing lean body mass (LBM) is the primary goal for both elite athletes and fitness enthusiasts. The use of amino acids as dietary supplements is widespread among athletes and physically active individuals. Extensive literature analysis reveals that branched-chain amino acids (BCAA), creatine, glutamine and β-alanine may be beneficial in regulating skeletal muscle metabolism, enhancing LBM and mitigating exercise-induced muscle damage. This review details the mechanisms of these amino acids, offering insights into their efficacy as supplements. Recommended dosage and potential side effects are then outlined to aid athletes in making informed choices and safeguard their health. Lastly, limitations within the current literature are addressed, highlighting opportunities for future research.
Similar content being viewed by others

Introduction
Amino acids are the building blocks for all life forms. There are 21 amino acids that make up human tissue proteins, with selenocysteine now included in the list and utilized for synthesizing proteins and essential molecules that fulfill significant physiological functions related to nutrition, sensory perception, and biological regulation [1,2,3]. These amino acids can be classified into essential amino acids (EAA, incapable of endogenous synthesis and must be obtained through dietary intake) and non-essential amino acids (NEAA, synthesized within the cell) [4]. Furthermore, under specific circumstances such as physical activity, lactation, trauma, and illness, certain NEAA may experience heightened utilization rates, thereby being referred to as conditionally essential amino acids (CEAA), when their demand exceeds the synthesis capacity [5]. Thus, amino acids, particularly EAA or CEAA, are commonly consumed as nutritional supplements by athletes across all levels of sports participation and individuals engaged in regular and moderate physical activity.
Participation in physical activity is a cornerstone of a healthy lifestyle and represents an excellent, cost-effective means to enhance overall well-being. However, engaging in physical activity can result in immediate decreases in muscle strength and the development of exercise-induced muscle damage, characterized by symptoms such as muscle swelling, stiffness, and discomfort [6, 7]. Skeletal muscles, which constitute approximately 45–55% of total body weight, are crucial for performance, locomotion [8]. Muscle metabolism is contingent upon the intricate equilibrium between muscle protein synthesis (MPS) and muscle protein breakdown (MPB). A surplus of MPS over MPB leads to a net positive protein balance, facilitating muscle growth, whereas the opposite scenario leads to muscle atrophy [9]. Maintaining a favorable net muscle protein balance, achieved by elevating MPS or reducing MPB, is paramount to improve function and strength. For example, dietary constraints, such as energy restriction, can curtail the rate of MPS, leading to a negative net protein balance and consequent lean body mass (LBM) loss, underscoring the potential importance of protein or amino acid supplementation to counteract negative net protein balance during dietary energy limitations [10,11,12].
A comprehensive analysis of the available literature reveals that supplementation with BCAA, creatine, glutamine, and β-Alanine has shown promise in increasing LBM, enhancing muscle strength and functionality. Although creatine, glutamine, and β-Alanine may modulate MPS and MPB indirectly, their additional effects are vital for sustaining muscle metabolism and mitigating muscle damage and fatigue. For example, creatine acts as a cellular energy buffer, maintains mitochondrial integrity, increases phosphocreatine (PCr) availability and mitigates oxidative damage [13]; glutamine acts as a nitrogen transporter, is a precursor of nucleotide bases and the antioxidant glutathione, and it regulates acid-base balance [14]; β-Alanine is a precursor for carnosine (β-alanyl-L-histidine) synthesis, which is involved in pH-buffering, calcium regulation, and endogenous antioxidant activity [15]. Hence, this review primarily focuses on elucidating the mechanisms of action, recommended dosages and potential side effects associated with these amino acid supplements in disease-free populations. The following sections offer valuable insights into amino acid supplementation for athletes and those engaged in regular moderate-vigorous physical activity to enable informed decision-making. Furthermore, this review addresses the existing gaps in the literature, emphasizing the imperative need for further research.
Branched-chain amino acids (BCAA)
BCAA refers to a class of amino acids characterized by their aliphatic side chains, including three specific amino acids: leucine, isoleucine and valine [16]. Structurally, the BCAA exhibit a high degree of hydrophobicity compared to other proteogenic amino acids, a property critical for preserving the maturity and stability of folded proteins [17]. The three amino acids found in the BCAA group are categorized as EAA, indicating that they cannot be endogenously synthesized in the human body and must be obtained through dietary sources to support vital physiological functions [4]. In contrast to other amino acids primarily metabolized in the liver, BCAA are absorbed and catabolized within skeletal muscle [18, 19]. This distinctive characteristic is crucial for the pivotal roles of BCAA in MPS and post-exercise muscle recovery [19]. Given the recognition of BCAA as a key regulator in MPS, these amino acids have become widely popular as nutritional supplements for individuals engaged in physical activity.
The potential mechanism of BCAA in regulating skeletal muscle metabolism
BCAA are integral to the regulation of skeletal muscle protein metabolism, through a complex network of intracellular signaling pathways. The mammalian target of rapamycin (mTOR) signaling pathway is a key driver of protein synthesis with eukaryotic translation initiation factor 4E (eIF4E) binding protein 1 (4E-BP1) and S6 kinase 1 (S6K1) playing key roles as phosphorylated substrates of mTOR complex 1 (mTORC1) [20,21,22,23,24,25]. These proteins regulate mRNA translation initiation and elongation, ultimately facilitating protein synthesis [24, 26]. Stress response proteins called Sestrins, including Sestrin1, Sestrin2 and Sestrin3, function as upstream negative regulators of mTORC1. The Sestrins have been shown to interact with GTPase-activating protein toward rags 2 (GATOR2), leading to the inhibition of mTORC1 activity [27]. The interaction between intracellular Sestrins and GATOR2 depends on amino acid availability. In vivo studies have demonstrated specific binding sites for leucine within Sestrin1 and Sestrin2, but not Sestrin3, and ingestion of leucine can thereby activate mTORC1 through these signaling pathways [28,29,30]. Further investigation is required to elucidate the precise mechanism by which leucine binding to Sestrin1/2 disrupts their interaction with GATOR2.
In addition to the role of Sestrins, research indicates that leucyl tRNA synthetase (LRS) functions as a sensor for leucine, activating the mTORC1 pathway. Specifically, LRS serves as a GTPase-activating protein (GAP) for RagD GTPase, prompting its transition from the inactive GTP-bound form (RagDGTP) to the active GDP-bound state (RagDGDP). Rag GTPases are known to be pivotal mediators in the amino acid-responsive mTORC1 pathway. Leucine induces the translocation of mTORC1 to the lysosome, where GTP-bound RagB-containing Rag heterodimers interact with mTORC1, leading to the activation of mTORC1 [31,32,33].
β-hydroxy-β-methylbutyrate (HMB), a metabolite derived from leucine, represents approximately 5–10% of leucine metabolism within the body [34]. Numerous studies support that HMB can stimulate MPS while simultaneously reducing MPB [35,36,37,38,39]. Mechanistically, HMB activates the mTORC1 pathway by enhancing AKT phosphorylation, which subsequently inactivates the tuberous sclerosis complex 2 (TSC2) [40, 41]. The TSC1-TSC2 complex acts as a negative regulator of mTORC1, with TSC2 serving as a GTPase-activating protein (GAP) for the small Ras-related GTPase Rheb, while TSC1 aids in stabilizing and safeguarding TSC2 from degradation [24]. The activated GTP-bound form of Rheb directly interacts with mTORC1 or enhances substrate recognition by mTORC1, thereby activating the mTORC1 pathway [23]. Additionally, increased AKT phosphorylation induces the phosphorylation of Forkhead box O 1 (FOXO1) and decreases nuclear FOXO1 levels, ultimately leading to the downregulation of muscle atrophy-related muscle RING-finger protein-1 (MURF1), thus mitigating MPB [41, 42].
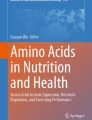
In summary, leucine activates the mTORC1 pathway through various mechanisms (Fig. 1), including the disruption of the Sestrin1/2-GATOR2 complex, the activation of LRS and the dephosphorylation of AKT facilitated by its metabolite, HMB.

The mechanisms of amino acids involvement in skeletal muscle cell metabolism. Leucine activates the mTORC1 pathway through the Sestrin1/2-GATOR2, LRS, or the dephosphorylation of AKT by its metabolite, HMB. Creatine upregulates IGF-1 and MRFs expression, activates satellite cells, and mitigates mitochondrial damage. Glutamine may activate AKT signaling pathways, mitigate mitochondrial damage and activate HSP-70. β-alanine is is a rate-limiting reactant in the synthesis of carnosine. Carnosine act as an intracellular pH buffer, metal-ion chelator, and regulator of calcium release and calcium sensitivity
Dosage recommendations and adverse effects
Utilizing the indicator amino acid oxidation (IAAO) method, the recommended total intake of BCAA for adults is 0.144 g/kg/day, with specific leucine, isoleucine, and valine intake at 0.055 g/kg/day, 0.042 g/kg/day, and 0.047 g/kg/day, respectively [43]. Furthermore, the recent study conducted by the European Prospective Investigation into Cancer and Nutrition (EPIC) indicates that, on average, adults consume 5.6 g of leucine, 3.2 g of isoleucine and 3.8 g of valine daily, with leucine being the most consumed EAA [44].
Leucine is recognized as a most potent and widely used amino acid supplement, due to its central role as the primary driver of MPS. Multiple studies have suggested that supplementation with low doses of protein or EAA enriched with leucine result in greater MPS stimulation compared to the consumption of 20–40 g of whey protein [45,46,47,48]. For example, the ingestion of just 3 g of EAA enriched with 1.2 g of leucine can elicit MPS to a level equivalent to that achieved by consuming 20 g of whey protein in older women, both at rest and following exercise [47]. In addition, D J Wilkinson et al. have reported that supplementation with 3 g of leucine in isolation can induce maximal MPS stimulation [46].
There is a debate that the consumption of leucine in isolation may be more efficacious for MPS than BCAA supplementation due to leucine’s competition with other neutral amino acids for transport into muscle cells, potentially limiting its unique impact on MPS [49]. However, supplementation with leucine alone can result in decreased concentrations of isoleucine and valine in both plasma and muscle [50,51,52]. This occurrence is attributed to ketoisocaproate, a product of leucine transamination, which enhances BCKA dehydrogenase activity in muscles, liver, and adipose tissues [50,51,52,53]. Therefore, the potential limitation of MPS induced by leucine intake alone due to the bioavailability of isoleucine and valine underscores the necessity for rigorously controlled double-blind trials to thoroughly assess and contrast the impact of leucine in isolation versus BCAA supplementation on MPS in individuals, both in sedentary conditions and during physical activity.
Although HMB can stimulate MPS and reduce MPB, several systematic reviews and meta-analyses have shown that HMB supplementation does not increase or prevent loss of muscle mass [35, 54,55,56]. Furthermore, HMB supplementation did not enhance the increases in muscle mass and strength resulting from resistance training [35].
The analysis of data from the International Council on Amino Acid Science has resulted in the determination of a tolerable upper intake level for leucine. The recommended limit for leucine supplementation is set at 0.5 g/kg/day for adults and 0.43 g/kg/day for elderly men over 70 years of age, corresponding to daily intakes of 35 g and 30 g, respectively, for a 70 kg individual [2, 57, 58]. Exceeding these established values can lead to elevated blood ammonia levels primarily as a result of the rapid transamination rates [2]. This heightened transamination activity is attributed to the higherKm values (Michaelis-Menten constant) of BCAA aminotransferases compared to tissue BCAA, being two to four times greater [19].
Limitations and future research opportunities
Based on existing research, the efficacy of leucine supplementation in maintaining protein balance over extended periods remains inconclusive [59,60,61]. Consequently, future research is necessary to evaluate the impact of prolonged BCAA or leucine supplementation on muscle anabolism, taking into account factors such as age, type of training, and duration.
BCAA are commonly included in a variety of supplements, including whey protein. However, current evidence does not support BCAA or leucine supplementation for muscle hypertrophy in individuals who meet daily protein intake recommendations (≥ 1.6 g/kg/day) for exercise, suggest that supplementation with BCAA may increase muscle mass in individuals who cannot guarantee sufficient protein intake [62,63,64,65]. Moberg et al. reported that the hierarchy of anabolic stimulation for whole intact proteins is as follows: EAA > BCAA > leucine alone, with the condition that sufficient leucine is present [66]. As such, the potential benefits of BCAA supplementation for athletes, including enhanced muscle function, reduced muscle soreness and delayed fatigue, should be approached with caution and warrant further investigations.
Creatine
Creatine is one of the most widely used nutritional supplements among both elite and amateur athletes [67, 68]. Under typical circumstances, an average individual requires approximately 2 g of creatine per day to offset daily losses, which equates to roughly 1.7% of the total creatine content in the body [69]. Creatine is sourced from two origins: one is endogenous synthesis (about 1 g, approximately half of the daily requirement) in the pancreas, liver and kidneys from methionine, glycine and arginine metabolism. The other source is exogenous from food like beef and seafood [70]. The average total creatine storage capacity in the human body is about 120 g, with the majority (95%) located in skeletal muscles and the remaining 5% distributed among the brain, kidneys, liver, and testes [71]. In skeletal muscle tissue, creatine is found in two primary forms: approximately 33% exists as the unbound free form, while the remaining 67% binds to phosphate molecules released from adenosine triphosphate (ATP)to form PCr. PCr, with the assistance of creatine kinase (CK), facilitates the transfer of phosphate to adenosine diphosphate (ADP) to regenerate ATP [71, 72]. Consequently, creatine operates as an energy regulator by promoting the recycling of ATP, exerting significant influence on muscle recovery, improving LBM, and enhancing strength [73].
As is well known, creatine supplementation enhances resistance training adaptations [68, 74, 75]. Studies have shown that skeletal muscle contraction stimulates intramyocellular uptake of creatine, and that a combination of creatine supplementation and resistance training may maximize its accretion [76]. As results, creatine supplementation combined with resistance training increases LBM and muscle strength [75, 77,78,79,80]. However, there is no evidence to suggest that creatine supplementation independent of resistance training can increase muscle strength.
The potential mechanism of creatine in regulating skeletal muscle metabolism
Creatine may regulate skeletal muscle metabolism through several pathways.Firstly, it may accelerate MPS by upregulating insulin-like growth factor-1 (IGF-1) levels and enhancing the release of IGF-1 from muscle cells [81, 82]. IGF-1 functions as a ligand, binding to IGF receptors on the cell membrane and subsequently activating signaling pathways, including the AKT/mTOR pathways, which promote cell growth and proliferation [83]. For instance, in a double-blind cross-over study involving high-intensity resistance exercise following five days of creatine supplementation, researchers observed a 30% increase in IGF mRNA expression in resting muscle, which leads to elevated phosphorylation levels of 4E-BP1, and enhancing MPS [81]. Secondly, creatine supplementation upregulates mRNA and protein expression of myogenic regulatory factors (MRFs), such as myogenin and MRF-4 [84]. These MRFs play pivotal roles in the activation, proliferation, and differentiation of satellite cells (skeletal muscle resident stem cells), which are crucial for the repair and regeneration of muscle fibers [71]. Satellite cells, located between the sarcolemma and the basal lamina of muscle fibers, fuse with the muscle fiber membrane upon activation, passing through the sarcolemma and differentiating into myonuclei, ultimately boosting muscle fiber protein synthesis [85]. In a study, the administration of creatine subsequent to resistance training was found to increase satellite cell numbers and myonuclei concentration in human skeletal muscle fibers, thereby facilitating muscle fiber hypertrophy [86].
Several studies indicate that creatine supplementation diminishes urinary 3-methylhistidine (3-MH, a global marker of protein breakdown) and leucine oxidation (a marker of MPB), implying a potential reduction of protein catabolism [87, 88] Mechanistically, the regulation of MPB by creatine may be attributed to its ability to attenuate mitochondrial damage. It is well-established that the aging process and physical activity can negatively impact mitochondrial function, resulting in compromised respiratory chain activity and generated reactive oxygen species (ROS) [89, 90]. ROS can accelerate muscle fatigue and damage by impairing calcium sensitivity and altering cell membrane permeability [90, 91]. Creatine reduces ROS, which mitigates mitochondrial damage, thereby protect against muscle damage and MPB [92]. The effects may arise from creatine’s direct antioxidant properties or its role in enhancing cell membrane stability and cellular energy production [13].
Taken together, existing research suggests potential mechanisms by which creatine may augment MPS and diminish MPB (Fig. 1), such as the upregulation of IGF-1 and MRFs expression, activation of satellite cells, and mitigation of mitochondrial damage. However, the precise mechanism by which creatine regulates skeletal muscle metabolism remains to be further determined.
Dosage recommendations and adverse effects
As previously mentioned, research has shown that creatine supplementation can improve exercise performance, muscle strength and muscle mass, especially in aging individuals [74, 75]. Due to the inadequate endogenous synthesis of creatine in the body, exogenous supplementation is often necessary to optimize anabolism in the majority of individuals [70]. In order to sustain proper levels of creatine in muscle tissue, it is advised to consume 1–3 g of creatine daily through dietary sources, a recommendation that especially important for vegetarians, who typically have lower muscle creatine stores and may experience benefits from creatine supplementation [93, 94]. Wallimann and colleagues recommend the inclusion of 3 g/day of exogenous creatine in individuals’ diets to promote overall health, particularly with advancing age [95]. Due to the benefits creatine provides, such as enhancing acute exercise capacity and training adaptations, elite athletes are frequently advised to utilize creatine supplementation as an ergogenic aid to optimize their training results [68].
After a saturation period, creatine supplementation can enhance high-intensity performance and strength/power by 5–15%, correlating with the degree of increase in muscle PCr levels [96]. The most rapid and effective approach to achieve creatine saturation entails the consumption of 20 g/day (or 0.3 g/kg/day) of creatine, administered in four 5 g doses, over a period of 5–7 days. Subsequently, a dose of 3–5 g/day (or 0.03 g kg/day) is advised for the maintenance of elevated muscle creatine stores [76, 97]. Studies indicate that a daily intake of 5–10 g of creatine is necessary for larger athletes to sustain increased creatine [96, 98, 99]. It is generally observed that heightened muscle creatine levels will return to baseline within 4–6 weeks after supplementation cessation [99, 100]. While, there is a lack of empirical evidence, it is unlikely that muscle creatine levels would fall below baseline levels post-supplementation discontinuation, indicating that prolonged exogenous creatine use does not inhibit the body’s inherent creatine synthesis capacity [101, 102].
Since the early 1990s, creatine monohydrate extensively researched and continues to be the predominant form of creatine supplementation [67]. Various newer forms of creatine, such as creatine dipeptides, creatine salts, and creatine complexes with other nutrients, have emerged in the market, claiming superior efficacy, safety, and bioavailability compared to creatine monohydrate [103]. Nevertheless, none of these alternative forms of creatine demonstrate the exceptional absorption rate of creatine monohydrate, which is estimated to be around 99% [104]. Various forms of creatine have a lower content per gram in comparison to creatine monohydrate, which boasts a creatine content of 87.9%, suggesting that creatine monohydrate may offer superior bioavailability [105]. Despite its limited solubility, creatine monohydrate powder demonstrates stability and resistance to degradation into creatinine even under prolonged storage and elevated temperatures [105]. Consequently, creatine monohydrate powder continues to be the favored option, prompting the need for additional research to formulate a stable and efficacious liquid form of creatine supplementation.
The prevalence of creatine use in sports and exercise, has prompted inquiries into potential side effects linked to its supplementation. Available studies have indicated that creatine supplementation, at doses ranging from 0.3 to 0.8 g/kg/day for up to 5 years, poses no adverse health risks, regardless age [68]. While anecdotal reports have suggested potential side effects like water retention, muscle cramping, dehydration, and kidney dysfunction. However, multiple studies have shown that creatine supplementation is not associated with increased instances of muscle cramping or dehydration [106,107,108,109,110,111]. Publications by the International Society of Sports Nutrition in 2007 and 2017 consistently confirm the efficacy and safety of creatine monohydrate [68, 104, 112, 113].
In summary, when administered at recommended dosages, creatine supplementation is deemed safe and advantageous for individuals spanning a wide range of demographics, including both healthy individuals and those with medical conditions across various age brackets from infancy to old age.
Limitations and future research opportunities
Several studies have indicated that the concurrent consumption of creatine with carbohydrates or a combination of carbohydrates and protein can improve creatine absorption [114, 115]. However, when compared to the use of creatine in isolation, this combined approach only marginally elevates muscle creatine levels and does not impact exercise performance or training adaptations significantly [68]. The potential effects of this combined method on muscle mass are still inconclusive, and existing evidence does not support its recommendation as a viable strategy.
In comparison to resistance exercise, creatine supplementation may not exert a substantial influence on continuous, prolonged, steady-state moderate intensity endurance exercise, but may be beneficial in higher intensity activities [70, 116, 117]. Further research is warranted to explore the effects of creatine supplementation on diverse endurance modalities.
Several reports have demonstrated enhancements in muscle mass, strength and performance in various female populations with creatine supplementation, including young, elderly, and post-menopausal women [118, 119]. However, females may be less responsive to exogenously creatine supplementation due to the presence of the higher baseline intramuscular concentrations in their muscles [120,121,122]. The optimal dosage of creatine supplementation for females compared to males remains uncertain.
Glutamine
Glutamine is a non-essential amino acid predominantly biosynthesized in skeletal muscles, with a smaller fraction originating from organs such as the lungs, brain, liver and adipose tissues [123, 124]. During the biosynthesis of glutamine within skeletal muscle, BCAA undergo deamination, transferring amino groups to α-ketoglutaric acid to produce glutamic acid. Subsequently, glutamic acid combines with ammonia to form glutamine through the catalytic activity of glutamine synthetase [123]. Glutamine is one of the most abundant amino acids found in human tissues and organs, comprising 80% of free amino acids in skeletal muscles and 20% in plasma [125].
Functionally, glutamine plays a vital role as a nitrogen transporter, aiding in the transfer of nitrogen generated in tissues to the kidneys for excretion, including the nitrogen released by skeletal muscles, with more than 80% of it being transported through glutamine [126, 127]. Glutamine serves as a critical source of ammonia necessary for the kidneys to regulate acid-base balance, while also serving as an energy source for various cell types such as epithelial cells, fibroblasts, and immune cells [128, 129]. Additionally, it is a precursor for the biosynthesis of proteins, amino acids, nucleotides, and glucose [130]. Research indicates that approximately 30–35% of the nitrogen resulting from protein degradation exists in the form of glutamine, underscoring its fundamental role in protein structure [131].
Notably, levels of glutamine in both blood and skeletal muscle decline rapidly during different forms of physical activity (e.g., resistance training and exhaustive exercise) [132,133,134]. These findings underscore that the potential inadequacy of endogenous glutamine synthesis in meeting the needs of athletes and individuals with specific medical conditions. Consequently, glutamine is recognized as a CEAA, that plays a role in immune system function, intestinal health, and overall protein balance [135, 136].
Several research has been reported that glutamine supplementation can improve MPS, decrease MPB, expedite wound healing, and mitigate muscle damage in animal models [137,138,139,140,141,142,143,144,145,146]. For example, increasing glutamine from 0.67 to 5.0 mM led to a 66% increase in MPS in rat skeletal muscle, even without insulin. In the presence of insulin, protein synthesis was boosted by 80% [137]. Their findings also revealed that the addition of 15 mM glutamine significantly reduced net protein loss and MPB compared to levels observed in the absence of glutamine [147]. Additionally, glutamine supplementation has been shown to stimulate protein synthesis and inhibit protein degradation in the mucosal cells of the small intestine [148, 149]. However, there remains a contentious discourse surrounding the impact of glutamine on MPS and MPB in human subjects. While some studies indicate that glutamine supplementation does not significant influence LBM and body composition, others have found a positive association between muscle glutamine levels and MPS in humans, implying a potential role for glutamine in muscle protein metabolism [150,151,152,153,154]. Further investigation is needed to elucidate the potential role of glutamine in regulating muscle protein turnover in humans.
The potential mechanism of glutamine in regulating skeletal muscle metabolism
According to existing research, glutamine may enhances net muscle mass through several mechanisms: (I) Glutamine may activates the AKT/mTOR signaling pathway through upregulation levels of AKT, mTOR and 4E-BP1 and downregulation ubiquitin ligases atrogin-1 (MAFbx) and MuRF-1 [155, 156]. (II) Glutamine directly stimulates glycogen synthesis through the activation of glycogen synthase, thereby facilitating energy production for MPS [154, 157, 158]. (III) Glutamine functions as the main nitrogen transporter in the body, thereby mitigating the buildup of harmful ammonia and its byproducts within muscle tissues [159, 160]. The presence of ammonia and its metabolites has been shown to interfere with enzyme activity, ion permeability, and the NAD+/NADH ratio in cells [161]. (IV) Glutamine stimulates the upregulation of heat shock proteins (HSP), specifically HSP70, via the processes of O-glycosylation and phosphorylation of transcription factors heat-shock factor 1 (HSF-1) and specificity protein 1 (Sp1) [162, 163]. HSP70 acts as a molecular chaperone, regulating protein folding, ubiquitin degradation pathways, and subcellular protein localization, thereby safeguarding against cell damage [164, 165].
Glutamine is recognized as an indirect antioxidant due to its role in glutathione synthesis, which aids in the elimination of ROS and shields against muscle damage [145]. Thus, it may regulate muscle plasticity, prevent muscle damage and promote muscle recovery [146, 166, 167].
Collectively, glutamine may increase MPS and reduce MPB through various potential mechanisms (Fig. 1), including the activation of AKT signaling pathways, stimulation of glycogen synthesis, up-regulation of the HSP family expression, glutathione synthesis, and reduction of ammonia and its metabolite accumulation. However, most studies on glutamine are based on animal models, and translating these findings to human trials may not be straightforward. Further investigation is needed to better understand the precise mechanisms of glutamine in skeletal muscle in humans.
Dosage recommendations and adverse effects
Given the current uncertain evidence of glutamine in muscle protein metabolism, body composition, and athlete performance, well-controlled clinical trials are needed to elucidate definitive guidelines for the supplementation of glutamine. The recommended daily intake of glutamine from dietary protein for a 70 kg individual is 3–6 g, while supplementation doses during exercise can range from 2 g to 40 g per day (0.05–0.6/kg/day) [14, 49, 125]. A review by Novak et al. showed that 0.2 g/kg/day of glutamine is the minimum concentration required for detectable clinical results [168]. It is worth noting that low plasma glutamine levels have been positively correlated with certain types of exercise, particularly those that are prolonged or exhaustive activities, indicating potential benefits of glutamine supplementation for individuals engaging in very strenuous exercise [132,133,134]. For instance, glutamine supplementation (10 g/day for 30 days) improved knee muscle power, strength, glycemic regulation, and plasma redox balance in elderly women aged 60–80 who were physically active [169].
It is essential to note that around 70% of orally administered glutamine undergoes degradation in the small intestine, resulting in only approximately 30% entering the bloodstream [5, 170]. To improve the bioavailability of glutamine and mitigate its instability, L-alanyl-L-glutamine, a dipeptide comprising glutamine and alanine, has been employed in lieu of free glutamine among athletes. Further research indicates that L-alanyl-L-glutamine (0.2 g/kg/day) exhibits superior stability and efficacy in elevating plasma and muscle glutamine levels, thereby promoting MPS in comparison to free glutamine [171, 172].
Glutamine is widely regarded as safe and well-tolerated for healthy individuals at recommended doses [14]. Research indicates that even higher glutamine supplementation levels, as high as 50–60 g/day or 0.65 g/kg/day for the short-term were safe and did not result in adverse events in hospital patients [173, 174]. Therefore, the safe upper intake level of glutamate in healthy individuals still needs further investigation.
Limitations and future research opportunities
Given the decline in plasma glutamine levels during prolonged or intense physical exertion, glutamine supplementation may offer advantages for individuals engaging in strenuous exercise. In addition, glutamine has a unique property of rapid turnover rate, indicating that its role in cellular metabolism cannot be underestimated. Nonetheless, the instability of free glutamine and its substantial degradation by the small intestine present obstacles, making the dipeptide form, L-alanyl-L-glutamine, may be as a more feasible option in commercial supplementation products. Therefore, future research, particularly in the form of rigorous clinical trials such as double-blind studies, is essential to validate the efficacy of glutamine in humans and further elucidate its intricate mechanisms of action.
β-alanine
β-alanine is an ergogenic aid favored by athletes for its potential to enhance performance. This non-essential β-amino acid, distinct in being one of the naturally occurring endogenous β-amino acids in both humans and animals, is synthesized through three main pathways [175,176,177]. First, it can be produced through the decarboxylation of L-aspartate, a reaction catalyzed by aspartate decarboxylase, which is secreted by gastrointestinal microbes. Secondly, β-alanine can emerge as a byproduct of the reaction between L-alanine and pyruvate, facilitated by β-alanine-pyruvate transaminase. Lastly, it is also generated through the decarboxylation and deamination of uracil, which involves three enzymes: dihydropyrimidine dehydrogenase, dihydropyrimidinase, and 3-Ureidopropionase.
Although β-alanine does not directly participate in synthesizing proteins or enzymes, it is physiologically significant holds. Its importance is primarily attributed to its role in the synthesis of carnosine (β-alanyl-L-histidine). This dipeptide is formed in muscle through a reaction between β-alanine and L-histidine, catalyzed by carnosine synthase with the involvement of ATP [178]. Carnosine, synthesized in this manner, is distributed throughout various organs, including the muscles, the brain, and the central nervous system [179]. Muscle carnosine serves multiple functions, including acting as an intracellular pH buffer, chelating metal ions, inhibiting glycation, and functioning as an antioxidant [180].
The potential mechanism of β-alanine in regulating skeletal muscle metabolism
According to recent research, the supplementation of β-alanine has been shown to enhance performance, improve muscle function and decrease fatigue during exercise [181, 182]. β-alanine is essential in exercise due to its role as a rate-limiting reactant in the synthesis of carnosine, and exogenous supplementation of β-alanine effectively elevate muscle carnosine concentrations [183,184,185].
The mechanisms underlying the action of carnosine encompasses several important aspects (Fig. 1). Firstly, carnosine functions as a pH buffer, mitigating the accumulation of lactate during physical activity and thereby mitigating acidosis and its negative impact on exercise performance and fatigue [186,187,188]. Secondly, carnosine demonstrates antioxidant properties through mechanisms that are both metal-ion-independent and metal-ion-dependent, providing protection against exercise-induced ROS damage [189,190,191]. Furthermore, carnosine has a high affinity for binding to the imidazole group of carnosine, facilitating its rapid oxidation and resulting in a decrease in levels of ROS in the presence of copper [15, 192]. Thirdly, carnosine functions as a protective agent against the formation of advanced lipoxidation end-products (ALEs) and advanced glycoxidation end-products (AGEs) by inhibiting protein carbonylation and glycoxidation [193,194,195,196].This protective mechanism primarily involves the prevention of lipid or glucose oxidation and the generation of reactive carbonyl species (RCS), thereby safeguarding cells from potential damage [15, 197, 198]. Lastly, carnosine serves as a modulator of calcium release and calcium sensitivity, playing a role in the regulation of muscle excitation and contraction coupling, ultimately improving muscle function [199, 200].
In summary, the primary function of β-alanine is to synthesize carnosine, which may regulate skeletal muscle metabolism by acting as intracellular pH buffer metal-ion chelator, and regulator of calcium release and calcium sensitivity (Fig. 1). These multifaceted mechanisms underscore the significance of carnosine as a beneficial component in improving exercise performance and muscle function.
Dosage recommendations and adverse effects
Since β-alanine is the rate limiting precursor for carnosine synthesis, it is necessary to consume 1–3 g of β-alanine daily through dietary sources [49]. In the context of athletes and sportsmen, the recommended dosage range for β-alanine supplementation is 3.2–6.4 g/day (0.04–0.08 g/kg/day, for an 80 kg individual) [201,202,203]. Numerous studies consistently demonstrate that supplementing with 4–6.4 g of β-alanine per day for a period of 4–10 weeks can lead to a significant increase in muscle carnosine content ranging from 40–100% [187, 204]. According to Harris et al., an increase of 40% in muscle carnosine levels is associated with a 4% enhancement in overall muscle buffering capacity and a 7% improvement in buffering capacity specifically in type II muscle fibers [185].
The most recent recommendation by Sport Integrity Australia (SIA) suggests initiating β-alanine supplementation at a dosage of 3.2 g/day for 8 weeks or 6.4 g/day for 4 weeks, followed by a maintenance dose of 1.2 g/day [205]. In this sense, supplementation of 1.2 g/day β-alanine has been demonstrated to be the optimal dose for sustaining muscle carnosine levels at 30–50% above pre-supplementation levels [206]. A meta-analysis revealed that the duration of exercise significantly influences the efficacy of β-alanine supplementation. Specifically, exercise periods lasting between 0.5 and 10 min are likely to yield the greatest benefits [182]. Moreover, when compared to the supplementation of β-alanine alone, the combined supplementation of β-alanine and sodium bicarbonate has been shown to produce the most significant effect [182].
A meta-analysis assessing the comprehensive risk of toxicity concluded that β-alanine supplementation (6.4 g/day for 24 weeks) poses no adverse effects in healthy individuals [203, 207]. Additionally, recent studies have shown that supplementation with 12 g/day of β-alanine has no side effects in the short term (7 or 14 days) [208, 209]. However, the establishment of a safe upper intake level for β-alanine remains a subject requiring further investigation.
Limitations and future research opportunities
Research has found that direct supplementation of carnosine does not produce the equivalent outcomes as β-alanine due to the swift degradation of carnosine by serum carnosinase into β-alanine and histidine upon ingestion, diminishing its efficacy [15, 210]. Consequently, the development of carnosine analogs that are resistant to degradation by carnosinase represents a significant challenge for future research. In addition, supplementing histidine in isolation did not significantly increase the level of muscle carnosine [211]. However, prolonged β-alanine supplementation may diminish the available pool of free histidine in muscles or plasma, suggesting that the co-supplementation of histidine and β-alanine may be a promising strategy for increasing carnosine levels [211].
Furthermore, research indicates that females naturally possess lower levels of intramuscular carnosine than males, with their carnosine content potentially increasing at a faster rate following β-alanine consumption [212, 213]. This finding suggests that females may exhibit different responses to β-alanine administration. However, there is a lack of research regarding the impact of β-alanine on female athletes. It remains to be determined whether females may require different β-alanine supplementation regimens in comparison to males and how β-alanine influences female body composition and muscle functions in relation to its ergogenic properties.
Conclusions and perspectives
Amino acids are widely used dietary supplements by individuals engaged in sports training and physical activity. This review outlines the effectiveness, recommended dosage, potential adverse effects (Table 1) and mechanisms (Fig. 1) of specific amino acids, including BCAA, creatine, glutamine and β-alanine, in regulating skeletal muscle metabolism. Significantly, existing evidence indicates that supplementation with these amino acids at prescribed doses is typically safe for healthy adults. Further research is necessary to investigate the adaptive responses and potential adverse effects linked to high-dose and prolonged amino acid supplementation. Furthermore, this review discusses the existing gaps in current literature. Future studies should to elucidate the impacts and optimal dosage schedules of amino acids across various demographic groups, considering variables such as sex, age, type and duration of physical activity, as well as specific physiological conditions like pregnancy, lactation, and hepatic or renal disorders. In conclusion, this review offers valuable insights for elite athletes and fitness enthusiasts, providing recommendations on the selection and utilization of specific amino acids in dietary supplementation to promote the maintenance and improvement of skeletal muscle mass.
Data availability
No datasets were generated or analysed during the current study.
References
Chung CZ, Krahn N. The selenocysteine toolbox: a guide to studying the 21st amino acid. Arch Biochem Biophys. 2022;730:109421.
Elango R. Tolerable Upper Intake Level for individual amino acids in humans: a narrative review of recent clinical studies. Adv Nutr. 2023;14:885–94.
Elango R, Laviano A. Protein and amino acids: key players in modulating health and disease. Curr Opin Clin Nutr Metab Care. 2017;20:69–70.
Hou Y, Yin Y, Wu G. Dietary essentiality of nutritionally non-essential amino acids for animals and humans. Exp Biol Med (Maywood). 2015;240:997–1007.
Wu G. Amino acids: metabolism, functions, and nutrition. Amino Acids. 2009;37:1–17.
Howatson G, van Someren KA. The prevention and treatment of exercise-induced muscle damage. Sports Med. 2008;38:483–503.
Owens DJ, Twist C, Cobley JN, Howatson G, Close GL. Exercise-induced muscle damage: what is it, what causes it and what are the nutritional solutions? Eur J Sport Sci. 2019;19:71–85.
Hector AJ, Phillips SM. Protein recommendations for weight loss in Elite athletes: a focus on body composition and performance. Int J Sport Nutr Exerc Metab. 2018;28:170–7.
Rasmussen BB, Phillips SM. Contractile and nutritional regulation of human muscle growth. Exerc Sport Sci Rev. 2003;31:127–31.
Pasiakos SM, Cao JJ, Margolis LM, Sauter ER, Whigham LD, McClung JP, Rood JC, Carbone JW, Combs GF Jr., Young AJ. Effects of high-protein diets on fat-free mass and muscle protein synthesis following weight loss: a randomized controlled trial. FASEB J. 2013;27:3837–47.
Areta JL, Burke LM, Camera DM, West DW, Crawshay S, Moore DR, Stellingwerff T, Phillips SM, Hawley JA, Coffey VG. Reduced resting skeletal muscle protein synthesis is rescued by resistance exercise and protein ingestion following short-term energy deficit. Am J Physiol Endocrinol Metab. 2014;306:E989–997.
Hector AJ, Marcotte GR, Churchward-Venne TA, Murphy CH, Breen L, von Allmen M, Baker SK, Phillips SM. Whey protein supplementation preserves postprandial myofibrillar protein synthesis during short-term energy restriction in overweight and obese adults. J Nutr. 2015;145:246–52.
Arazi H, Eghbali E, Suzuki K. Creatine Supplementation, Physical Exercise and oxidative stress markers: a review of the mechanisms and Effectiveness. Nutrients 2021, 13.
Gleeson M. Dosing and efficacy of glutamine supplementation in human exercise and sport training. J Nutr. 2008;138:S2045–9.
Boldyrev AA, Aldini G, Derave W. Physiology and pathophysiology of carnosine. Physiol Rev. 2013;93:1803–45.
Neinast M, Murashige D, Arany Z. Branched chain amino acids. Annu Rev Physiol. 2019;81:139–64.
Brosnan JT, Brosnan ME. Branched-chain amino acids: enzyme and substrate regulation. J Nutr. 2006;136:S207–11.
Foure A, Bendahan D. Is branched-chain amino acids supplementation an efficient nutritional strategy to alleviate skeletal muscle damage? A systematic review. Nutrients 2017, 9.
Harper AE, Miller RH, Block KP. Branched-chain amino acid metabolism. Annu Rev Nutr. 1984;4:409–54.
Atherton PJ, Smith K, Etheridge T, Rankin D, Rennie MJ. Distinct anabolic signalling responses to amino acids in C2C12 skeletal muscle cells. Amino Acids. 2010;38:1533–9.
Matthews DE. Observations of branched-chain amino acid administration in humans. J Nutr. 2005;135:S1580–4.
Rieu I, Balage M, Sornet C, Giraudet C, Pujos E, Grizard J, Mosoni L, Dardevet D. Leucine supplementation improves muscle protein synthesis in elderly men independently of hyperaminoacidaemia. J Physiol. 2006;575:305–15.
Caron E, Ghosh S, Matsuoka Y, Ashton-Beaucage D, Therrien M, Lemieux S, Perreault C, Roux PP, Kitano H. A comprehensive map of the mTOR signaling network. Mol Syst Biol. 2010;6:453.
Laplante M, Sabatini DM. mTOR signaling in growth control and disease. Cell. 2012;149:274–93.
Kimball SR, Jefferson LS. Signaling pathways and molecular mechanisms through which branched-chain amino acids mediate translational control of protein synthesis. J Nutr. 2006;136:S227–31.
Cao Y, Liu S, Liu K, Abbasi IHR, Cai C, Yao J. Molecular mechanisms relating to amino acid regulation of protein synthesis. Nutr Res Rev. 2019;32:183–91.
Glaviano A, Foo ASC, Lam HY, Yap KCH, Jacot W, Jones RH, Eng H, Nair MG, Makvandi P, Geoerger B, et al. PI3K/AKT/mTOR signaling transduction pathway and targeted therapies in cancer. Mol Cancer. 2023;22:138.
Chantranupong L, Wolfson RL, Orozco JM, Saxton RA, Scaria SM, Bar-Peled L, Spooner E, Isasa M, Gygi SP, Sabatini DM. The sestrins interact with GATOR2 to negatively regulate the amino-acid-sensing pathway upstream of mTORC1. Cell Rep. 2014;9:1–8.
Wolfson RL, Chantranupong L, Saxton RA, Shen K, Scaria SM, Cantor JR, Sabatini DM. Sestrin2 is a leucine sensor for the mTORC1 pathway. Science. 2016;351:43–8.
Xu D, Shimkus KL, Lacko HA, Kutzler L, Jefferson LS, Kimball SR. Evidence for a role for Sestrin1 in mediating leucine-induced activation of mTORC1 in skeletal muscle. Am J Physiol Endocrinol Metab. 2019;316:E817–28.
Yoon MS, Son K, Arauz E, Han JM, Kim S, Chen J. Leucyl-tRNA synthetase activates Vps34 in amino acid-sensing mTORC1 signaling. Cell Rep. 2016;16:1510–7.
Han JM, Jeong SJ, Park MC, Kim G, Kwon NH, Kim HK, Ha SH, Ryu SH, Kim S. Leucyl-tRNA synthetase is an intracellular leucine sensor for the mTORC1-signaling pathway. Cell. 2012;149:410–24.
Lee M, Kim JH, Yoon I, Lee C, Fallahi Sichani M, Kang JS, Kang J, Guo M, Lee KY, Han G, et al. Coordination of the leucine-sensing rag GTPase cycle by leucyl-tRNA synthetase in the mTORC1 signaling pathway. Proc Natl Acad Sci U S A. 2018;115:E5279–88.
Espina S, Sanz-Paris A, Bernal-Monterde V, Casas-Deza D, Arbones-Mainar JM. Role of branched-chain amino acids and their derivative beta-hydroxy-beta-methylbutyrate in liver cirrhosis. J Clin Med 2022, 11.
Phillips SM, Lau KJ, D’Souza AC, Nunes EA. An umbrella review of systematic reviews of beta-hydroxy-beta-methyl butyrate supplementation in ageing and clinical practice. J Cachexia Sarcopenia Muscle. 2022;13:2265–75.
Baier S, Johannsen D, Abumrad N, Rathmacher JA, Nissen S, Flakoll P. Year-long changes in protein metabolism in elderly men and women supplemented with a nutrition cocktail of beta-hydroxy-beta-methylbutyrate (HMB), L-arginine, and L-lysine. JPEN J Parenter Enter Nutr. 2009;33:71–82.
Cruz-Jentoft AJ. Beta-hydroxy-Beta-methyl butyrate (HMB): from Experimental Data to Clinical evidence in Sarcopenia. Curr Protein Pept Sci. 2018;19:668–72.
Din USU, Brook MS, Selby A, Quinlan J, Boereboom C, Abdulla H, Franchi M, Narici MV, Phillips BE, Williams JW, et al. A double-blind placebo controlled trial into the impacts of HMB supplementation and exercise on free-living muscle protein synthesis, muscle mass and function, in older adults. Clin Nutr. 2019;38:2071–8.
Flakoll P, Sharp R, Baier S, Levenhagen D, Carr C, Nissen S. Effect of beta-hydroxy-beta-methylbutyrate, arginine, and lysine supplementation on strength, functionality, body composition, and protein metabolism in elderly women. Nutrition. 2004;20:445–51.
Holecek M. Beta-hydroxy-beta-methylbutyrate supplementation and skeletal muscle in healthy and muscle-wasting conditions. J Cachexia Sarcopenia Muscle. 2017;8:529–41.
Kimura K, Cheng XW, Inoue A, Hu L, Koike T, Kuzuya M. beta-hydroxy-beta-methylbutyrate facilitates PI3K/Akt-dependent mammalian target of rapamycin and FoxO1/3a phosphorylations and alleviates tumor necrosis factor alpha/interferon gamma-induced MuRF-1 expression in C2C12 cells. Nutr Res. 2014;34:368–74.
Vasques J, Guerreiro CS, Sousa J, Pinto M, Cortez-Pinto H. Nutritional support in cirrhotic patients with Sarcopenia. Clin Nutr ESPEN. 2019;33:12–7.
Elango R, Ball RO, Pencharz PB. Recent advances in determining protein and amino acid requirements in humans. Br J Nutr. 2012;108(Suppl 2):S22–30.
Iguacel I, Perez-Cornago A, Schmidt JA, Van Puyvelde H, Travis R, Casagrande C, Nicolas G, Riboli E, Weiderpass E, Ardanaz E, et al. Evaluation of protein and amino acid intake estimates from the EPIC dietary questionnaires and 24-h dietary recalls using different food composition databases. Nutr Metab Cardiovasc Dis. 2022;32:80–9.
Churchward-Venne TA, Burd NA, Mitchell CJ, West DW, Philp A, Marcotte GR, Baker SK, Baar K, Phillips SM. Supplementation of a suboptimal protein dose with leucine or essential amino acids: effects on myofibrillar protein synthesis at rest and following resistance exercise in men. J Physiol. 2012;590:2751–65.
Wilkinson DJ, Hossain T, Hill DS, Phillips BE, Crossland H, Williams J, Loughna P, Churchward-Venne TA, Breen L, Phillips SM, et al. Effects of leucine and its metabolite beta-hydroxy-beta-methylbutyrate on human skeletal muscle protein metabolism. J Physiol. 2013;591:2911–23.
Bukhari SS, Phillips BE, Wilkinson DJ, Limb MC, Rankin D, Mitchell WK, Kobayashi H, Greenhaff PL, Smith K, Atherton PJ. Intake of low-dose leucine-rich essential amino acids stimulates muscle anabolism equivalently to bolus whey protein in older women at rest and after exercise. Am J Physiol Endocrinol Metab. 2015;308:E1056–1065.
Atherton PJ, Kumar V, Selby AL, Rankin D, Hildebrandt W, Phillips BE, Williams JP, Hiscock N, Smith K. Enriching a protein drink with leucine augments muscle protein synthesis after resistance exercise in young and older men. Clin Nutr. 2017;36:888–95.
Holecek M. Side effects of amino acid supplements. Physiol Res. 2022;71:29–45.
Block KP, Harper AE. Valine metabolism in vivo: effects of high dietary levels of leucine and isoleucine. Metabolism. 1984;33:559–66.
Holecek M, Siman P, Vodenicarovova M, Kandar R. Alterations in protein and amino acid metabolism in rats fed a branched-chain amino acid- or leucine-enriched diet during postprandial and postabsorptive states. Nutr Metab (Lond). 2016;13:12.
May RC, Piepenbrock N, Kelly RA, Mitch WE. Leucine-induced amino acid antagonism in rats: muscle valine metabolism and growth impairment. J Nutr. 1991;121:293–301.
Aftring RP, Block KP, Buse MG. Leucine and isoleucine activate skeletal muscle branched-chain alpha-keto acid dehydrogenase in vivo. Am J Physiol. 1986;250:E599–604.
Holland BM, Roberts BM, Krieger JW, Schoenfeld BJ. Does HMB enhance body composition in athletes? A systematic review and Meta-analysis. J Strength Cond Res. 2022;36:585–92.
Jakubowski JS, Nunes EA, Teixeira FJ, Vescio V, Morton RW, Banfield L, Phillips SM. Supplementation with the leucine metabolite beta-hydroxy-beta-methylbutyrate (HMB) does not improve Resistance Exercise-Induced changes in body composition or strength in young subjects: a systematic review and Meta-analysis. Nutrients 2020, 12.
Sanchez-Martinez J, Santos-Lozano A, Garcia-Hermoso A, Sadarangani KP, Cristi-Montero C. Effects of beta-hydroxy-beta-methylbutyrate supplementation on strength and body composition in trained and competitive athletes: a meta-analysis of randomized controlled trials. J Sci Med Sport. 2018;21:727–35.
Elango R, Chapman K, Rafii M, Ball RO, Pencharz PB. Determination of the tolerable upper intake level of leucine in acute dietary studies in young men. Am J Clin Nutr. 2012;96:759–67.
Rasmussen B, Gilbert E, Turki A, Madden K, Elango R. Determination of the safety of leucine supplementation in healthy elderly men. Amino Acids. 2016;48:1707–16.
Koopman R, Verdijk LB, Beelen M, Gorselink M, Kruseman AN, Wagenmakers AJ, Kuipers H, van Loon LJ. Co-ingestion of leucine with protein does not further augment post-exercise muscle protein synthesis rates in elderly men. Br J Nutr. 2008;99:571–80.
Verhoeven S, Vanschoonbeek K, Verdijk LB, Koopman R, Wodzig WK, Dendale P, van Loon LJ. Long-term leucine supplementation does not increase muscle mass or strength in healthy elderly men. Am J Clin Nutr. 2009;89:1468–75.
Leenders M, Verdijk LB, van der Hoeven L, van Kranenburg J, Hartgens F, Wodzig WK, Saris WH, van Loon LJ. Prolonged leucine supplementation does not augment muscle mass or affect glycemic control in elderly type 2 diabetic men. J Nutr. 2011;141:1070–6.
Aguiar AF, Grala AP, da Silva RA, Soares-Caldeira LF, Pacagnelli FL, Ribeiro AS, da Silva DK, de Andrade WB, Balvedi MCW. Free leucine supplementation during an 8-week resistance training program does not increase muscle mass and strength in untrained young adult subjects. Amino Acids. 2017;49:1255–62.
IT DEA, Gualano B, Hevia-Larrain V, Neves-Junior J, Cajueiro M, Jardim F, Gomes RL, Artioli GG, Phillips SM, Campos-Ferraz P, Roschel H. Leucine supplementation has no further effect on training-induced muscle adaptations. Med Sci Sports Exerc. 2020;52:1809–14.
Mobley CB, Mumford PW, McCarthy JJ, Miller ME, Young KC, Martin JS, Beck DT, Lockwood CM, Roberts MD. Whey protein-derived exosomes increase protein synthesis and hypertrophy in C(2-)C(12) myotubes. J Dairy Sci. 2017;100:48–64.
Plotkin DL, Delcastillo K, Van Every DW, Tipton KD, Aragon AA, Schoenfeld BJ. Isolated leucine and branched-chain amino acid supplementation for enhancing muscular strength and hypertrophy: a narrative review. Int J Sport Nutr Exerc Metab. 2021;31:292–301.
Moberg M, Apro W, Ekblom B, van Hall G, Holmberg HC, Blomstrand E. Activation of mTORC1 by leucine is potentiated by branched-chain amino acids and even more so by essential amino acids following resistance exercise. Am J Physiol Cell Physiol. 2016;310:C874–884.
Kerksick CM, Wilborn CD, Roberts MD, Smith-Ryan A, Kleiner SM, Jager R, Collins R, Cooke M, Davis JN, Galvan E, et al. ISSN exercise & sports nutrition review update: research & recommendations. J Int Soc Sports Nutr. 2018;15:38.
Kreider RB, Kalman DS, Antonio J, Ziegenfuss TN, Wildman R, Collins R, Candow DG, Kleiner SM, Almada AL, Lopez HL. International Society of Sports Nutrition position stand: safety and efficacy of creatine supplementation in exercise, sport, and medicine. J Int Soc Sports Nutr. 2017;14:18.
Brosnan JT, da Silva RP, Brosnan ME. The metabolic burden of creatine synthesis. Amino Acids. 2011;40:1325–31.
Forbes SC, Candow DG, Neto JHF, Kennedy MD, Forbes JL, Machado M, Bustillo E, Gomez-Lopez J, Zapata A, Antonio J. Creatine supplementation and endurance performance: surges and sprints to win the race. J Int Soc Sports Nutr. 2023;20:2204071.
Candow DG, Forbes SC, Chilibeck PD, Cornish SM, Antonio J, Kreider RB. Variables influencing the effectiveness of Creatine Supplementation as a therapeutic intervention for Sarcopenia. Front Nutr. 2019;6:124.
Wyss M, Kaddurah-Daouk R. Creatine and creatinine metabolism. Physiol Rev. 2000;80:1107–213.
Turnagol HH, Kosar SN, Guzel Y, Aktitiz S, Atakan MM. Nutritional Considerations for Injury Prevention and Recovery in Combat sports. Nutrients 2021, 14.
Delpino FM, Figueiredo LM, Forbes SC, Candow DG, Santos HO. Influence of age, sex, and type of exercise on the efficacy of creatine supplementation on lean body mass: a systematic review and meta-analysis of randomized clinical trials. Nutrition 2022, 103–4:111791.
Forbes SC, Candow DG, Ostojic SM, Roberts MD, Chilibeck PD. Meta-analysis examining the importance of Creatine Ingestion strategies on lean tissue Mass and Strength in older adults. Nutrients 2021, 13.
Harris RC, Soderlund K, Hultman E. Elevation of creatine in resting and exercised muscle of normal subjects by creatine supplementation. Clin Sci (Lond). 1992;83:367–74.
Branch JD. Effect of creatine supplementation on body composition and performance: a meta-analysis. Int J Sport Nutr Exerc Metab. 2003;13:198–226.
Chilibeck PD, Kaviani M, Candow DG, Zello GA. Effect of creatine supplementation during resistance training on lean tissue mass and muscular strength in older adults: a meta-analysis. Open Access J Sports Med. 2017;8:213–26.
Devries MC, Phillips SM. Creatine supplementation during resistance training in older adults-a meta-analysis. Med Sci Sports Exerc. 2014;46:1194–203.
Rawson ES, Volek JS. Effects of creatine supplementation and resistance training on muscle strength and weightlifting performance. J Strength Cond Res. 2003;17:822–31.
Deldicque L, Louis M, Theisen D, Nielens H, Dehoux M, Thissen JP, Rennie MJ, Francaux M. Increased IGF mRNA in human skeletal muscle after creatine supplementation. Med Sci Sports Exerc. 2005;37:731–6.
Candow DG, Forbes SC, Chilibeck PD, Cornish SM, Antonio J, Kreider RB. Effectiveness of Creatine Supplementation on Aging muscle and bone: Focus on Falls Prevention and Inflammation. J Clin Med 2019, 8.
Brown LA, Perry RA Jr., Haynie WS, Lee DE, Rosa-Caldwell ME, Brown JL, Greene NP, Wolchok JC, Washington TA. Moderators of skeletal muscle maintenance are compromised in sarcopenic obese mice. Mech Ageing Dev. 2021;194:111404.
Willoughby DS, Rosene JM. Effects of oral creatine and resistance training on myogenic regulatory factor expression. Med Sci Sports Exerc. 2003;35:923–9.
Kao M, Columbus DA, Suryawan A, Steinhoff-Wagner J, Hernandez-Garcia A, Nguyen HV, Fiorotto ML, Davis TA. Enteral beta-hydroxy-beta-methylbutyrate supplementation increases protein synthesis in skeletal muscle of neonatal pigs. Am J Physiol Endocrinol Metab. 2016;310:E1072–1084.
Olsen S, Aagaard P, Kadi F, Tufekovic G, Verney J, Olesen JL, Suetta C, Kjaer M. Creatine supplementation augments the increase in satellite cell and myonuclei number in human skeletal muscle induced by strength training. J Physiol. 2006;573:525–34.
Candow DG, Little JP, Chilibeck PD, Abeysekara S, Zello GA, Kazachkov M, Cornish SM, Yu PH. Low-dose creatine combined with protein during resistance training in older men. Med Sci Sports Exerc. 2008;40:1645–52.
Johannsmeyer S, Candow DG, Brahms CM, Michel D, Zello GA. Effect of creatine supplementation and drop-set resistance training in untrained aging adults. Exp Gerontol. 2016;83:112–9.
Suzuki K, Tominaga T, Ruhee RT, Ma S. Characterization and modulation of systemic inflammatory response to Exhaustive Exercise in relation to oxidative stress. Antioxid (Basel) 2020, 9.
Johnston AP, De Lisio M, Parise G. Resistance training, Sarcopenia, and the mitochondrial theory of aging. Appl Physiol Nutr Metab. 2008;33:191–9.
Moopanar TR, Allen DG. Reactive oxygen species reduce myofibrillar Ca2 + sensitivity in fatiguing mouse skeletal muscle at 37 degrees C. J Physiol. 2005;564:189–99.
Sestili P, Martinelli C, Colombo E, Barbieri E, Potenza L, Sartini S, Fimognari C. Creatine as an antioxidant. Amino Acids. 2011;40:1385–96.
Brosnan ME, Brosnan JT. The role of dietary creatine. Amino Acids. 2016;48:1785–91.
Benton D, Donohoe R. The influence of creatine supplementation on the cognitive functioning of vegetarians and omnivores. Br J Nutr. 2011;105:1100–5.
Wallimann T, Tokarska-Schlattner M, Schlattner U. The creatine kinase system and pleiotropic effects of creatine. Amino Acids. 2011;40:1271–96.
Kreider RB. Effects of creatine supplementation on performance and training adaptations. Mol Cell Biochem. 2003;244:89–94.
Hultman E, Soderlund K, Timmons JA, Cederblad G, Greenhaff PL. Muscle creatine loading in men. J Appl Physiol (1985). 1996;81:232–7.
Casey A, Constantin-Teodosiu D, Howell S, Hultman E, Greenhaff PL. Creatine ingestion favorably affects performance and muscle metabolism during maximal exercise in humans. Am J Physiol. 1996;271:E31–37.
Greenhaff PL, Casey A, Short AH, Harris R, Soderlund K, Hultman E. Influence of oral creatine supplementation of muscle torque during repeated bouts of maximal voluntary exercise in man. Clin Sci (Lond). 1993;84:565–71.
Vandenberghe K, Goris M, Van Hecke P, Van Leemputte M, Vangerven L, Hespel P. Long-term creatine intake is beneficial to muscle performance during resistance training. J Appl Physiol (1985). 1997;83:2055–63.
Kim HJ, Kim CK, Carpentier A, Poortmans JR. Studies on the safety of creatine supplementation. Amino Acids. 2011;40:1409–18.
Kreider RB, Melton C, Rasmussen CJ, Greenwood M, Lancaster S, Cantler EC, Milnor P, Almada AL. Long-term creatine supplementation does not significantly affect clinical markers of health in athletes. Mol Cell Biochem. 2003;244:95–104.
Kreider RB, Jager R, Purpura M. Bioavailability, Efficacy, Safety, and Regulatory Status of Creatine and Related compounds: a critical review. Nutrients 2022, 14.
Antonio J, Candow DG, Forbes SC, Gualano B, Jagim AR, Kreider RB, Rawson ES, Smith-Ryan AE, VanDusseldorp TA, Willoughby DS, Ziegenfuss TN. Common questions and misconceptions about creatine supplementation: what does the scientific evidence really show? J Int Soc Sports Nutr. 2021;18:13.
Jager R, Purpura M, Shao A, Inoue T, Kreider RB. Analysis of the efficacy, safety, and regulatory status of novel forms of creatine. Amino Acids. 2011;40:1369–83.
Greenwood M, Kreider RB, Melton C, Rasmussen C, Lancaster S, Cantler E, Milnor P, Almada A. Creatine supplementation during college football training does not increase the incidence of cramping or injury. Mol Cell Biochem. 2003;244:83–8.
Greenwood M, Kreider RB, Greenwood L, Byars A. Cramping and Injury Incidence in Collegiate Football players are reduced by Creatine Supplementation. J Athl Train. 2003;38:216–9.
Watson G, Casa DJ, Fiala KA, Hile A, Roti MW, Healey JC, Armstrong LE, Maresh CM. Creatine use and exercise heat tolerance in dehydrated men. J Athl Train. 2006;41:18–29.
Rosene JM, Matthews TD, McBride KJ, Galla A, Haun M, McDonald K, Gagne N, Lea J, Kasen J, Farias C. The effects of creatine supplementation on thermoregulation and isokinetic muscular performance following acute (3-day) supplementation. J Sports Med Phys Fit. 2015;55:1488–96.
Lopez RM, Casa DJ, McDermott BP, Ganio MS, Armstrong LE, Maresh CM. Does creatine supplementation hinder exercise heat tolerance or hydration status? A systematic review with meta-analyses. J Athl Train. 2009;44:215–23.
Kozmik Z, Swamynathan SK, Ruzickova J, Jonasova K, Paces V, Vlcek C, Piatigorsky J. Cubozoan crystallins: evidence for convergent evolution of pax regulatory sequences. Evol Dev. 2008;10:52–61.
Geller AI, Shehab N, Weidle NJ, Lovegrove MC, Wolpert BJ, Timbo BB, Mozersky RP, Budnitz DS. Emergency Department visits for adverse events related to Dietary supplements. N Engl J Med. 2015;373:1531–40.
Buford TW, Kreider RB, Stout JR, Greenwood M, Campbell B, Spano M, Ziegenfuss T, Lopez H, Landis J, Antonio J. International Society of Sports Nutrition position stand: creatine supplementation and exercise. J Int Soc Sports Nutr. 2007;4:6.
Green AL, Hultman E, Macdonald IA, Sewell DA, Greenhaff PL. Carbohydrate ingestion augments skeletal muscle creatine accumulation during creatine supplementation in humans. Am J Physiol. 1996;271:E821–826.
Steenge GR, Simpson EJ, Greenhaff PL. Protein- and carbohydrate-induced augmentation of whole body creatine retention in humans. J Appl Physiol (1985). 2000;89:1165–71.
Anomasiri W, Sanguanrungsirikul S, Saichandee P. Low dose creatine supplementation enhances sprint phase of 400 meters swimming performance. J Med Assoc Thai. 2004;87(Suppl 2):S228–232.
Rossiter HB, Cannell ER, Jakeman PM. The effect of oral creatine supplementation on the 1000-m performance of competitive rowers. J Sports Sci. 1996;14:175–9.
Cox G, Mujika I, Tumilty D, Burke L. Acute creatine supplementation and performance during a field test simulating match play in elite female soccer players. Int J Sport Nutr Exerc Metab. 2002;12:33–46.
Aguiar AF, Januario RS, Junior RP, Gerage AM, Pina FL, do Nascimento MA, Padovani CR, Cyrino ES. Long-term creatine supplementation improves muscular performance during resistance training in older women. Eur J Appl Physiol. 2013;113:987–96.
Smith-Ryan AE, Cabre HE, Eckerson JM, Candow DG. Creatine Supplementation in Women’s Health: A Lifespan Perspective. Nutrients 2021, 13.
Forbes SC, Sletten N, Durrer C, Myette-Cote E, Candow D, Little JP. Creatine Monohydrate Supplementation does not augment fitness, performance, or body composition adaptations in response to four weeks of high-intensity interval training in Young females. Int J Sport Nutr Exerc Metab. 2017;27:285–92.
Kalhan SC, Gruca L, Marczewski S, Bennett C, Kummitha C. Whole body creatine and protein kinetics in healthy men and women: effects of creatine and amino acid supplementation. Amino Acids. 2016;48:677–87.
Wagenmakers AJ. Amino acid metabolism, muscular fatigue and muscle wasting. Speculations on adaptations at high altitude. Int J Sports Med. 1992;13(Suppl 1):S110–113.
Cordova-Martinez A, Caballero-Garcia A, Bello HJ, Perez-Valdecantos D, Roche E. Effect of glutamine supplementation on muscular damage biomarkers in professional basketball players. Nutrients 2021, 13.
Master PBZ, Macedo RCO. Effects of dietary supplementation in sport and exercise: a review of evidence on milk proteins and amino acids. Crit Rev Food Sci Nutr. 2021;61:1225–39.
van Hall G, Saris WH, Wagenmakers AJ. Effect of carbohydrate supplementation on plasma glutamine during prolonged exercise and recovery. Int J Sports Med. 1998;19:82–6.
Watford M. Glutamine metabolism and function in relation to proline synthesis and the safety of glutamine and proline supplementation. J Nutr. 2008;138:S2003–7.
Xi P, Jiang Z, Zheng C, Lin Y, Wu G. Regulation of protein metabolism by glutamine: implications for nutrition and health. Front Biosci (Landmark Ed). 2011;16:578–97.
Karakoulas KA, Vasilakos D, Grosomanidis V, Thomareis O, Goudas LC, Giala MM. Effects of pneumoperitoneum and LPS-induced endotoxemia on cerebral perfusion pressure in pigs. J Neurosurg Anesthesiol. 2006;18:194–9.
Smith RJ. Glutamine metabolism and its physiologic importance. JPEN J Parenter Enter Nutr. 1990;14:S40–4.
Wagenmakers AJ. Protein and amino acid metabolism in human muscle. Adv Exp Med Biol. 1998;441:307–19.
Brodan V, Kuhn E, Pechar J, Tomkova D. Changes of free amino acids in plasma of healthy subjects induced by physical exercise. Eur J Appl Physiol Occup Physiol. 1976;35:69–77.
Ziegler TR, Szeszycki EE, Estivariz CF, Puckett AB, Leader LM. Glutamine: from basic science to clinical applications. Nutrition. 1996;12:S68–70.
Holecek M, Sispera L. Glutamine deficiency in extracellular fluid exerts adverse effects on protein and amino acid metabolism in skeletal muscle of healthy, laparotomized, and septic rats. Amino Acids. 2014;46:1377–84.
Hardy G, Hardy IJ. Can glutamine enable the critically ill to cope better with infection? JPEN J Parenter Enter Nutr. 2008;32:489–91.
Stehle P, Zander J, Mertes N, Albers S, Puchstein C, Lawin P, Furst P. Effect of parenteral glutamine peptide supplements on muscle glutamine loss and nitrogen balance after major surgery. Lancet. 1989;1:231–3.
MacLennan PA, Brown RA, Rennie MJ. A positive relationship between protein synthetic rate and intracellular glutamine concentration in perfused rat skeletal muscle. FEBS Lett. 1987;215:187–91.
Davenport MT, Dickson JA, Johnson MR, Chamberland S. Total synthesis of Clavatadine B. J Nat Prod. 2019;82:3191–5.
Davis MV. Evolving concepts regarding hiatal hernia and gastroesophageal reflux. Ann Thorac Surg. 1969;7:120–33.
Legault Z, Bagnall N, Kimmerly DS. The influence of oral L-Glutamine supplementation on muscle strength recovery and soreness following unilateral knee extension eccentric Exercise. Int J Sport Nutr Exerc Metab. 2015;25:417–26.
Arribas-Lopez E, Zand N, Ojo O, Snowden MJ, Kochhar T. The effect of amino acids on Wound Healing: a systematic review and Meta-analysis on arginine and glutamine. Nutrients 2021, 13.
Cruzat VF, Rogero MM, Tirapegui J. Effects of supplementation with free glutamine and the dipeptide alanyl-glutamine on parameters of muscle damage and inflammation in rats submitted to prolonged exercise. Cell Biochem Funct. 2010;28:24–30.
Cruzat VF, Tirapegui J. Effects of oral supplementation with glutamine and alanyl-glutamine on glutamine, glutamate, and glutathione status in trained rats and subjected to long-duration exercise. Nutrition. 2009;25:428–35.
Eckel S, Sushkov AO, Lamoreaux SK. Limit on the electron electric dipole moment using paramagnetic ferroelectric Eu0.5Ba0.5TiO3. Phys Rev Lett. 2012;109:193003.
Leite JS, Raizel R, Hypolito TM, Rosa TD, Cruzat VF, Tirapegui J. l-glutamine and l-alanine supplementation increase glutamine-glutathione axis and muscle HSP-27 in rats trained using a progressive high-intensity resistance exercise. Appl Physiol Nutr Metab. 2016;41:842–9.
Petry ER, Cruzat VF, Heck TG, Leite JS, Homem de Bittencourt PI Jr., Tirapegui J. Alanyl-glutamine and glutamine plus alanine supplements improve skeletal redox status in trained rats: involvement of heat shock protein pathways. Life Sci. 2014;94:130–6.
Munoz-Torres M, Diaz J, Escobar-Jimenez F, Gonzalez-Calvin G, Vara C, Ruiz Requena ME, Vara R, Morales I. Measurement of parathyrin in blood from thyroid veins: two radioimmunoassays compared in patients with primary hyperparathyroidism. Clin Chem. 1988;34:2148–50.
Curi R, Lagranha CJ, Doi SQ, Sellitti DF, Procopio J, Pithon-Curi TC, Corless M, Newsholme P. Molecular mechanisms of glutamine action. J Cell Physiol. 2005;204:392–401.
Coeffier M, Claeyssens S, Hecketsweiler B, Lavoinne A, Ducrotte P, Dechelotte P. Enteral glutamine stimulates protein synthesis and decreases ubiquitin mRNA level in human gut mucosa. Am J Physiol Gastrointest Liver Physiol. 2003;285:G266–273.
Candow DG, Chilibeck PD, Burke DG, Davison KS, Smith-Palmer T. Effect of glutamine supplementation combined with resistance training in young adults. Eur J Appl Physiol. 2001;86:142–9.
Finn KJ, Lund R, Rosene-Treadwell M. Glutamine supplementation did not benefit athletes during short-term weight reduction. J Sports Sci Med. 2003;2:163–8.
Ramezani Ahmadi A, Rayyani E, Bahreini M, Mansoori A. The effect of glutamine supplementation on athletic performance, body composition, and immune function: a systematic review and a meta-analysis of clinical trials. Clin Nutr. 2019;38:1076–91.
Rennie MJ, Edwards RH, Krywawych S, Davies CT, Halliday D, Waterlow JC, Millward DJ. Effect of exercise on protein turnover in man. Clin Sci (Lond). 1981;61:627–39.
Coqueiro AY, Rogero MM, Tirapegui J. Glutamine as an anti-fatigue amino acid in sports Nutrition. Nutrients 2019, 11.
Marc Rhoads J, Wu G. Glutamine, arginine, and leucine signaling in the intestine. Amino Acids. 2009;37:111–22.
Lambertucci AC, Lambertucci RH, Hirabara SM, Curi R, Moriscot AS, Alba-Loureiro TC, Guimaraes-Ferreira L, Levada-Pires AC, Vasconcelos DA, Sellitti DF, Pithon-Curi TC. Glutamine supplementation stimulates protein-synthetic and inhibits protein-degradative signaling pathways in skeletal muscle of diabetic rats. PLoS ONE. 2012;7:e50390.
Varnier M, Leese GP, Thompson J, Rennie MJ. Stimulatory effect of glutamine on glycogen accumulation in human skeletal muscle. Am J Physiol. 1995;269:E309–315.
Bowtell JL, Gelly K, Jackman ML, Patel A, Simeoni M, Rennie MJ. Effect of oral glutamine on whole body carbohydrate storage during recovery from exhaustive exercise. J Appl Physiol (1985). 1999;86:1770–7.
Bassini-Cameron A, Monteiro A, Gomes A, Werneck-de-Castro JP, Cameron L. Glutamine protects against increases in blood ammonia in football players in an exercise intensity-dependent way. Br J Sports Med. 2008;42:260–6.
Coqueiro AY, Raizel R, Bonvini A, Hypolito T, Godois ADM, Pereira JRR, Garcia ABO, Lara RSB, Rogero MM, Tirapegui J. Effects of Glutamine and Alanine Supplementation on Central Fatigue Markers in Rats Submitted to Resistance Training. Nutrients 2018, 10.
Meneguello MO, Mendonca JR, Lancha AH Jr., Costa Rosa LF. Effect of arginine, ornithine and citrulline supplementation upon performance and metabolism of trained rats. Cell Biochem Funct. 2003;21:85–91.
Singleton KD, Wischmeyer PE. Glutamine induces heat shock protein expression via O-glycosylation and phosphorylation of HSF-1 and Sp1. JPEN J Parenter Enter Nutr. 2008;32:371–6.
Wischmeyer PE. Glutamine and heat shock protein expression. Nutrition. 2002;18:225–8.
Senf SM. Skeletal muscle heat shock protein 70: diverse functions and therapeutic potential for wasting disorders. Front Physiol. 2013;4:330.
Raizel R, Leite JS, Hypolito TM, Coqueiro AY, Newsholme P, Cruzat VF, Tirapegui J. Determination of the anti-inflammatory and cytoprotective effects of l-glutamine and l-alanine, or dipeptide, supplementation in rats submitted to resistance exercise. Br J Nutr. 2016;116:470–9.
Milne KJ, Noble EG. Response of the myocardium to exercise: sex-specific regulation of hsp70. Med Sci Sports Exerc. 2008;40:655–63.
Senf SM, Howard TM, Ahn B, Ferreira LF, Judge AR. Loss of the inducible Hsp70 delays the inflammatory response to skeletal muscle injury and severely impairs muscle regeneration. PLoS ONE. 2013;8:e62687.
Novak F, Heyland DK, Avenell A, Drover JW, Su X. Glutamine supplementation in serious illness: a systematic review of the evidence. Crit Care Med. 2002;30:2022–9.
Amirato GR, Borges JO, Marques DL, Santos JMB, Santos CAF, Andrade MS, Furtado GE, Rossi M, Luis LN, Zambonatto RF et al. L-Glutamine supplementation enhances strength and power of knee muscles and improves glycemia control and plasma redox balance in exercising Elderly women. Nutrients 2021, 13.
Castell LM, Poortmans JR, Newsholme EA. Does glutamine have a role in reducing infections in athletes? Eur J Appl Physiol Occup Physiol. 1996;73:488–90.
Hoffman JR, Williams DR, Emerson NS, Hoffman MW, Wells AJ, McVeigh DM, McCormack WP, Mangine GT, Gonzalez AM, Fragala MS. L-alanyl-L-glutamine ingestion maintains performance during a competitive basketball game. J Int Soc Sports Nutr. 2012;9:4.
Rogero MM, Tirapegui J, Pedrosa RG, Castro IA, Pires IS. Effect of alanyl-glutamine supplementation on plasma and tissue glutamine concentrations in rats submitted to exhaustive exercise. Nutrition. 2006;22:564–71.
Garlick PJ. Assessment of the safety of glutamine and other amino acids. J Nutr. 2001;131:S2556–61.
Ward E, Picton S, Reid U, Thomas D, Gardener C, Smith M, Henderson M, Holden V, Kinsey S, Lewis I, Allgar V. Oral glutamine in paediatric oncology patients: a dose finding study. Eur J Clin Nutr. 2003;57:31–6.
Cronan JE Jr. Beta-alanine synthesis in Escherichia coli. J Bacteriol. 1980;141:1291–7.
Hayaishi O, Nishizuka Y, Tatibana M, Takeshita M, Kuno S. Enzymatic studies on the metabolism of beta-alanine. J Biol Chem. 1961;236:781–90.
Tiedje KE, Stevens K, Barnes S, Weaver DF. Beta-alanine as a small molecule neurotransmitter. Neurochem Int. 2010;57:177–88.
Bakardjiev A, Bauer K. Transport of beta-alanine and biosynthesis of carnosine by skeletal muscle cells in primary culture. Eur J Biochem. 1994;225:617–23.
Gallant S, Semyonova M, Yuneva M. Carnosine as a potential anti-senescence drug. Biochem (Mosc). 2000;65:866–8.
Thomas DT, Erdman KA, Burke LM. Position of the Academy of Nutrition and Dietetics, dietitians of Canada, and the American College of Sports Medicine: Nutrition and athletic performance. J Acad Nutr Diet. 2016;116:501–28.
Furst T, Massaro A, Miller C, Williams BT, LaMacchia ZM, Horvath PJ. beta-alanine supplementation increased physical performance and improved executive function following endurance exercise in middle aged individuals. J Int Soc Sports Nutr. 2018;15:32.
Saunders B, Elliott-Sale K, Artioli GG, Swinton PA, Dolan E, Roschel H, Sale C, Gualano B. beta-alanine supplementation to improve exercise capacity and performance: a systematic review and meta-analysis. Br J Sports Med. 2017;51:658–69.
Bex T, Chung W, Baguet A, Stegen S, Stautemas J, Achten E, Derave W. Muscle carnosine loading by beta-alanine supplementation is more pronounced in trained vs. untrained muscles. J Appl Physiol (1985). 2014;116:204–9.
Culbertson JY, Kreider RB, Greenwood M, Cooke M. Effects of beta-alanine on muscle carnosine and exercise performance: a review of the current literature. Nutrients. 2010;2:75–98.
Harris RC, Tallon MJ, Dunnett M, Boobis L, Coakley J, Kim HJ, Fallowfield JL, Hill CA, Sale C, Wise JA. The absorption of orally supplied beta-alanine and its effect on muscle carnosine synthesis in human vastus lateralis. Amino Acids. 2006;30:279–89.
Blancquaert L, Everaert I, Derave W. Beta-alanine supplementation, muscle carnosine and exercise performance. Curr Opin Clin Nutr Metab Care. 2015;18:63–70.
Hill CA, Harris RC, Kim HJ, Harris BD, Sale C, Boobis LH, Kim CK, Wise JA. Influence of beta-alanine supplementation on skeletal muscle carnosine concentrations and high intensity cycling capacity. Amino Acids. 2007;32:225–33.
Hobson RM, Saunders B, Ball G, Harris RC, Sale C. Effects of beta-alanine supplementation on exercise performance: a meta-analysis. Amino Acids. 2012;43:25–37.
Klebanov GI, Teselkin Yu O, Babenkova IV, Popov IN, Levin G, Tyulina OV, Boldyrev AA, Vladimirov Yu A. Evidence for a direct interaction of superoxide anion radical with carnosine. Biochem Mol Biol Int. 1997;43:99–106.
Pavlov AR, Revina AA, Dupin AM, Boldyrev AA, Yaropolov AI. The mechanism of interaction of carnosine with superoxide radicals in water solutions. Biochim Biophys Acta. 1993;1157:304–12.
Tamba M, Torreggiani A. A pulse radiolysis study of carnosine in aqueous solution. Int J Radiat Biol. 1998;74:333–40.
Tamba M, Torreggiani A. Hydroxyl radical scavenging by carnosine and cu(II)-carnosine complexes: a pulse-radiolysis and spectroscopic study. Int J Radiat Biol. 1999;75:1177–88.
Aldini G, Facino RM, Beretta G, Carini M. Carnosine and related dipeptides as quenchers of reactive carbonyl species: from structural studies to therapeutic perspectives. BioFactors. 2005;24:77–87.
Nagai R, Murray DB, Metz TO, Baynes JW. Chelation: a fundamental mechanism of action of AGE inhibitors, AGE breakers, and other inhibitors of diabetes complications. Diabetes. 2012;61:549–59.
Seidler NW, Yeargans GS, Morgan TG. Carnosine disaggregates glycated alpha-crystallin: an in vitro study. Arch Biochem Biophys. 2004;427:110–5.
Zhou S, Decker EA. Ability of carnosine and other skeletal muscle components to quench unsaturated aldehydic lipid oxidation products. J Agric Food Chem. 1999;47:51–5.
Alhamdani MS, Al-Kassir AH, Abbas FK, Jaleel NA, Al-Taee MF. Antiglycation and antioxidant effect of carnosine against glucose degradation products in peritoneal mesothelial cells. Nephron Clin Pract. 2007;107:c26–34.
Peterszegi G, Molinari J, Ravelojaona V, Robert L. Effect of advanced glycation end-products on cell proliferation and cell death. Pathol Biol (Paris). 2006;54:396–404.
Dutka TL, Lamb GD. Effect of carnosine on excitation-contraction coupling in mechanically-skinned rat skeletal muscle. J Muscle Res Cell Motil. 2004;25:203–13.
Dutka TL, Lamboley CR, McKenna MJ, Murphy RM, Lamb GD. Effects of carnosine on contractile apparatus ca(2)(+) sensitivity and sarcoplasmic reticulum ca(2)(+) release in human skeletal muscle fibers. J Appl Physiol (1985). 2012;112:728–36.
de Andrade Kratz C, de Salles Painelli V, de Andrade Nemezio KM, da Silva RP, Franchini E, Zagatto AM, Gualano B, Artioli GG. Beta-alanine supplementation enhances judo-related performance in highly-trained athletes. J Sci Med Sport. 2017;20:403–8.
de Camargo JBB, Brigatto FA, Zaroni RS, Germano MD, Souza D, Bacurau RF, Marchetti PH, Braz TV, Aoki MS, Lopes CR. Does beta-alanine supplementation enhance adaptations to resistance training? A randomized, placebo-controlled, double-blind study. Biol Sport. 2023;40:217–24.
Saunders B, Franchi M, de Oliveira LF, da Eira Silva V, da Silva RP, de Salles Painelli V, Costa LAR, Sale C, Harris RC, Roschel H, et al. 24-Week beta-alanine ingestion does not affect muscle taurine or clinical blood parameters in healthy males. Eur J Nutr. 2020;59:57–65.
Baguet A, Reyngoudt H, Pottier A, Everaert I, Callens S, Achten E, Derave W. Carnosine loading and washout in human skeletal muscles. J Appl Physiol (1985). 2009;106:837–42.
Fernandez-Lazaro D, Fiandor EM, Garcia JF, Busto N, Santamaria-Pelaez M, Gutierrez-Abejon E, Roche E, Mielgo-Ayuso J. beta-alanine supplementation in Combat sports: evaluation of sports Performance, Perception, and Anthropometric Parameters and Biochemical Markers-A Systematic Review of clinical trials. Nutrients 2023, 15.
Naderi A, de Oliveira EP, Ziegenfuss TN, Willems MT. Timing, optimal dose and intake duration of Dietary supplements with evidence-based Use in sports Nutrition. J Exerc Nutr Biochem. 2016;20:1–12.
Dolan E, Swinton PA, Painelli VS, Stephens Hemingway B, Mazzolani B, Infante Smaira F, Saunders B, Artioli GG. Gualano B: a systematic risk Assessment and Meta-Analysis on the use of oral beta-alanine supplementation. Adv Nutr. 2019;10:452–63.
Church DD, Hoffman JR, Varanoske AN, Wang R, Baker KM, La Monica MB, Beyer KS, Dodd SJ, Oliveira LP, Harris RC, et al. Comparison of two beta-alanine dosing protocols on muscle carnosine elevations. J Am Coll Nutr. 2017;36:608–16.
Hoffman JR, Gepner Y, Hoffman MW, Zelicha H, Shapira S, Ostfeld I. Effect of High-Dose, short-duration beta-alanine supplementation on circulating IL-10 concentrations during intense military training. J Strength Cond Res. 2018;32:2978–81.
Park YJ, Volpe SL, Decker EA. Quantitation of carnosine in humans plasma after dietary consumption of beef. J Agric Food Chem. 2005;53:4736–9.
Blancquaert L, Everaert I, Missinne M, Baguet A, Stegen S, Volkaert A, Petrovic M, Vervaet C, Achten E, M DEM, et al. Effects of histidine and beta-alanine supplementation on human muscle Carnosine Storage. Med Sci Sports Exerc. 2017;49:602–9.
Everaert I, Mooyaart A, Baguet A, Zutinic A, Baelde H, Achten E, Taes Y, De Heer E, Derave W. Vegetarianism, female gender and increasing age, but not CNDP1 genotype, are associated with reduced muscle carnosine levels in humans. Amino Acids. 2011;40:1221–9.
Stegen S, Bex T, Vervaet C, Vanhee L, Achten E, Derave W. beta-alanine dose for maintaining moderately elevated muscle carnosine levels. Med Sci Sports Exerc. 2014;46:1426–32.
Funding
This study was supported by The Project of the Jilin Province Sports Bureau (202308).
Author information
Authors and Affiliations
Contributions
JL and GL wrote the main manuscript text and JL, GL and ZL read, edited and approved the manuscript. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Ethical approval and consent to participate
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Li, G., Li, Z. & Liu, J. Amino acids regulating skeletal muscle metabolism: mechanisms of action, physical training dosage recommendations and adverse effects. Nutr Metab (Lond) 21, 41 (2024). https://doi.org/10.1186/s12986-024-00820-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12986-024-00820-0