
Abstract
Background
Peripheral nerve injuries and central neurologic conditions can result in extensive disabilities. In cases with unilateral impairment, assessing the asymmetry between the upper extremity has been used to assess outcomes of treatment and severity of injury. A wide variety of validated and novel tests and sensors have been utilized to determine the upper extremity asymmetry. The purpose of this article is to review the literature and define the current state of the art for describing upper extremity asymmetry in patients with peripheral nerve injuries or central neurologic conditions.
Method
An electronic literature search of PubMed, Scopus, Web of Science, OVID was performed for publications between 2000 to 2022. Eligibility criteria were subjects with neurological conditions/injuries who were analyzed for dissimilarities in use between the upper extremities. Data related to study population, target condition/injury, types of tests performed, sensors used, real-world data collection, outcome measures of interest, and results of the study were extracted. Sackett’s Level of Evidence was used to judge the quality of the articles.
Results
Of the 7281 unique articles, 112 articles met the inclusion criteria for the review. Eight target conditions/injuries were identified (Brachial Plexus Injury, Cerebral Palsy, Multiple Sclerosis, Parkinson’s Disease, Peripheral Nerve Injury, Spinal Cord Injury, Schizophrenia, and stroke). The tests performed were classified into thirteen categories based on the nature of the test and data collected. The general results related to upper extremity asymmetry were listed for all the reviewed articles. Stroke was the most studied condition, followed by cerebral palsy, with kinematics and strength measurement tests being the most frequently used tests. Studies with a level of evidence level II and III increased between 2000 and 2021. The use of real-world evidence-based data, and objective data collection tests also increased in the same period.
Conclusion
Adequately powered randomized controlled trials should be used to study upper extremity asymmetry. Neurological conditions other than stroke should be studied further. Upper extremity asymmetry should be measured using objective outcome measures like motion tracking and activity monitoring in the patient’s daily living environment.
Similar content being viewed by others

Introduction
It is estimated that 795,000 people suffer a stroke in the United States yearly of which 70% are first time strokes [1]. Between 2015 and 2018, 7.6 million people suffered a stroke [2]. Cerebral Palsy (CP) affects more than 17 million people worldwide [3,4,5,6]. Each year, about 60,000 Americans are diagnosed with Parkinson’s disease (PD) [7]. In 2020, the number of known cases of Multiple Sclerosis (MS) increased to 2.8 million worldwide [8]. Amyotrophic Lateral Sclerosis (ALS) affected about 12,187 people in the United States between 2010 and 2011 [9].
Traumatic injuries resulting in peripheral nerve injury (PNI) (including brachial plexus injury (BPI)) and spinal cord injury (SCI) cause extensive disabilities in the upper extremity (UE). Motor vehicle accidents (MVA) are the predominant cause of PNI, where 5% of all MVAs result in a form of PNI [10]. About 8% of PNI patients have a BPI [11]. Adult traumatic BPI results in severe impairment following penetrating wounds, falls, and MVA or other high-energy trauma. Young male adults comprise a majority among patients with a BPI [12]. MVAs and falls are a leading cause of SCI. 38.1% of all SCI were caused by MVAs and 53% by falls between 2010 and 2014 [13]. The United States has an estimated annual SCI incidence of 17,000 [14]. The National Spinal Cord Injury Statistical Center estimated 282,000 people were living with a SCI in 2016 [15].
Conditions/injuries affecting the nervous system can be debilitating. Stroke victims suffer paretic limbs [16] and is the third-leading cause of disability [17]. CP accounts for most of the lifelong neurological disabilities [3,4,5,6]. Bimanual coordination impairments were found in children with CP [18,19,20]. BPI predominately affects young and otherwise healthy men resulting in paralytic upper extremities [21]. Patients with MS display reduced gross or fine motor capabilities, in addition to slowness, clumsiness, and dysmetria [22,23,24], while patients with PD displayed a deficit in inhibitory control [25,26,27,28,29,30]. Many of the UE PNI patients, despite rehabilitative efforts, never achieve satisfactory motor recovery [31,32,33,34]. All of these neurological conditions/injuries can affect the patient’s ability to perform daily tasks with their affected UE.
A wide range of outcome measures have been described in the literature as well as clinical practice to quantify the disabilities of the UE. These measures involve tests and surveys on dexterity, strength, pain, disability, amount of activity, etc. When the neurological condition/injury is unilateral, the differences in the outcome measures between the ipsilateral and contralateral sides can be used to gauge the patient’s recovery or the progression of the condition. Such a comparison between the affected and the unaffected sides is beneficial and provides patient specific, real-world evidence (RWE) [35] based data and information. Real world evidence is a combination of data collected outside of a traditional clinical setting. Asymmetry measures can either be subjective or objective, measured in a clinical setting or in the patient’s daily living environment. Clinical surveys to measure outcomes are either too extensive or too limited in scope, are completed without supervision and is time intensive for patients with a relatively high rate of failure to complete. This emphasizes the importance to understand the benefits and shortcomings of each type of test in relation to the treatment population.
Previous reviews have explored wearable systems [36,37,38], fine and gross motor tests [39], and various functional evaluation techniques [40] for UE assessment and rehabilitation. No currently available review or article explores the state of the art in assessing UE asymmetry caused by nerve injuries or central neurologic conditions. Hence, it is necessary to investigate the available literature and identify the present gaps in knowledge and redirect research focus onto such gaps.
The purpose of this review is to document the various tests/techniques/sensors used in clinical practice to assess UE asymmetry in a population with neurological conditions/injuries. This work was undertaken with the following goals:
-
1.
Report trends in studies published from 2000 to 2022.
-
2.
Classify the most widely used tests/techniques/sensors to assess UE asymmetry.
-
3.
Classify the most widely studied neurological conditions/injuries.
-
4.
Analyze the frequency of RWE based approaches compared to in-clinic approaches.
Methods
The PRISMA-ScR guidelines for reporting scoping reviews were followed [41, 42]. The project was registered with the Open Science Framework (https://doi.org/10.17605/OSF.IO/8PFUW). A protocol was created and followed for the review (https://osf.io/bk3at).
Literature search
Initial searches were performed on 1/26/2023 in PubMed, Scopus, and Web of Science. Date limits were set from 1/1/2000 forward. A follow-up search of multiple databases was performed on April 18, 2023. Results were also limited to 1/1/2000 forward. Databases for the follow up search were Ovid MEDLINE(R) (1946 + including epub ahead of print, in-process, and other nonindexed citations), Ovid Embase (1974 +), Ovid Cochrane Central Register of Controlled Trials (1991 +), Ovid Cochrane Database of Systematic Reviews (2005 +), and Scopus via Elsevier (1970 +). The initial search was performed by the study investigator SGB. The expanded and updated search strategies were designed and conducted by a medical librarian with input from the study investigators (SGB, AYS, KRK). The searched articles were limited to a publishing date between 1/1/2000 to 12/31/2022. Controlled vocabulary supplemented with keywords was used for this search. The actual strategies for each search that lists all search terms and how they are combined is available in the Table 1. Results included journal articles and peer reviewed conference proceedings in the English language and articles with available English translation. Duplicates were identified and removed from the main list using Endnote X9 (Clarivate, Philadelphia, PA).
Eligibility criteria
A thorough review of the literature was performed based on the following criteria.
Inclusion criteria:
-
The study involved analysis of the dissimilarities in activity between the upper extremities (right vs. left) and included any assessment method to analyze this dissimilarity.
-
The study involved subjects with neurological conditions/injuries.
Exclusion criteria:
-
The article was a systematic review, a case study, or a book chapter.
-
The study included only unimpaired subjects (No treatment group).
-
The study involved analysis of the UE during indirect periodic tasks (e.g., gait, etc.).
-
The article did not focus on the asymmetry between the upper extremities (e.g., device design and validation articles).
-
The study was performed on newborns or infants.
-
The article explored the UE activity via mathematical modelling.
Selection process
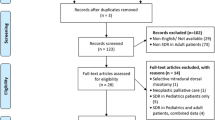
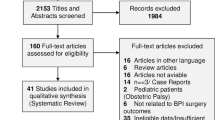
The selection process included several steps (Fig. 1). Database search results (publication years 2000 forward) were checked for duplicates. These unique articles were then screened using their abstracts for relevance to the review topic. Full texts for the screened articles were accessed online. The articles that could not be retrieved (for any reason) were disregarded from the review. The retrieved articles were assessed and selected based on the eligibility criteria. Several systematic review articles [36,37,38,39] related to the current review topic were identified during the search. The references listed in these review articles were screened and the process described above was performed on these references to check for eligibility.

PRISMA flowchart for the literature search and exclusions. “n” is the number of articles in each given step
Data extraction
Selected articles were reviewed and the following data were extracted as per the protocol: study population, target condition/injury, types of tests performed, sensors used, real-world data collection as described in [35], outcome measures, and study results. Statistical significance was recorded. Data collected was classified as either objective, subjective, or a mixture of both. The search and mark functionality were used on pdf reader applications such as Adobe acrobat reader DC v2022.001.20142 (Adobe, San Jose, CA, USA) and Notability v11.3.1 (Ginger Labs, San Francisco, CA, USA). The extracted data were charted in an excel sheet (Excel, Microsoft 365 apps for enterprise, version 2211, Microsoft corporations, Redmond, WA, USA), and the counts were plotted using R version 4.2.0.
Critical appraisal
A modified Sackett’s Level of Evidence (LoE) [43] was used to judge the quality of the studies based on the information provided in the articles. Level I indicated the study was a randomized controlled trial (RCT), Level II were cohort studies, Level III were case-controlled studies, and Level IV were poorly designed case-controlled studies. The LoE value indicating quality of the articles decreased from Level I to IV.
All the above steps were performed by SGB under the supervision of AYS and KRK.
Results
Selection of sources
From a total of 7281 unique articles, 112 met the specified criteria and were included in this review. Details of the exclusions performed are listed in Fig. 1. Review articles or case studies [36,37,38,39, 44,45,46,47,48,49,50,51,52,53] and studies without a treatment population (conducted exclusively on healthy subjects) [54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105] were excluded. Eleven articles studied UE asymmetry during indirect periodic movements (e.g., gait, etc.) [106,107,108,109,110,111,112,113,114,115,116,117,118,119,120,121]. Some excluded studies were designed to assess a specific device’s design [122,123,124,125], focused on mathematical modelling and analysis of the asymmetries [111, 126,127,128,129,130], or did not study the UE asymmetry resulting from any specific neurological condition (e.g., [131,132,133,134,135,136,137,138,139,140,141,142,143,144,145,146,147,148,149,150,151]). Articles focused on the reliability or validity of methods were also excluded [152,153,154,155,156,157,158,159,160,161,162,163]. Exclusions were also performed due to the subject population studied (Amputees [164, 165], and newborns/toddlers [166,167,168,169,170,171]). The study population, objectives and significant results from the reviewed articles are listed in Table 2.
The selected articles concentrated on BPI, CP, MS, PD, PNI, SCI, Schizophrenia (SCZ), and stroke. It is important to note that even though SCZ is not a nervous system lesion or injury, it is a neurological disorder and presents with upper extremity behavioral asymmetry. Stroke was the most prominent condition (63 articles) followed by CP (27 articles). PNI, and SCZ were the least studied conditions/injuries (1 article each) (Fig. 2a).

Number of articles divided by a target condition/injury, b level of evidence, c type of study, and d publication year (n = number of articles)
Critical appraisal of sources
The reviewed articles had a higher proportion of Level III and IV of evidence (44 and 35 counts respectively). Five articles were at Level I evidence, and 28 articles contained Level II evidence (Fig. 2b and Table 2). The number of Level II and III articles increased over the years (Fig. 2d), with the increase being concentrated over 2018 to 2021. 93 articles performed data collection in a clinical setting, while 19 articles collected complete or partial RWE (Fig. 2c). An upward trend was seen in the number of articles published over the years, with the highest number of articles published in 2020 and 2021 (11 articles each) (Fig. 2d).
Extracted data
The tests and sensors used in the selected studies were divided into thirteen categories based on the type of test and data collected (Table 3). SGB divided the tests into respective categories based on each test’s description (as stated in databases such as the Shirley Ryan Ability Lab rehabilitation measure database) and data collected. Kinematics tests were the most common types of tests performed (37 instances) followed by strength measures (36 instances). Motion reflex test was the least common type of test used (1 instance) (Fig. 3c). The articles contained 153 instances of objective tests, 48 instances of subjective tests, and 11 instances of mixed data type tests (Table 3). Objective data collection increased between 2000 to 2021 (from 6 to 18instances) (Fig. 3a). Stroke had the highest number of objective tests (105 instances) and subjective tests (25 instances), followed by CP (34 and 12 instances, respectively) (Fig. 3b). All activity monitoring, electromyography, kinematic, and motion reflex tests collected objective data, while amount of use, handedness, quality of life, and spasticity tests collected subjective data. Some disability tests of fine motor skills or strength collected mixed data. Strength measures were the most popular outcome measures for stroke (28 instances) followed by fine motor tests (20 instances), activity monitoring (19 instances) and disability measures (18 instances). Gross motor tests were used primarily on the CP treatment groups (15 instances).

Heat map distribution of the tests performed in the selected articles by target condition/injury and test categories; Number of articles divided by a publication year, b target condition/injury, c test categories
Most of the articles reviewed performed tests and collected data in the clinic (93 articles). Articles on stroke as the target condition saw most of the real-world data collection (16 articles) (Fig. 4a). Studies using RWE based tests had a higher treatment group population (median: 20) compared to studies using in-clinic tests (median: 16) (Fig. 4b). The number of studies utilizing real-world data increased between 2000 and 2021 with only 1 out of 6 articles in 2000 compared to 5 out of 11 articles in 2021 containing some form of RWE (Fig. 4c).

Distribution of the data collection method for a target condition/injury, b treatment group population vs. type of study, and c publication year (n = number of articles)
Discussion
Summary of evidence
The evolution of the science for assessing UE asymmetry secondary to neurological conditions/injuries from 2000 to 2022 was reviewed. Most articles were Level III or IV of evidence. Stroke and CP were the most studied conditions. Tests collecting data on the kinematics and strength were widely used. RWE based testing and objective data collection increased between 2000 and 2021.
Stroke and CP were the most common conditions studied. Although CP and the other neurological conditions affect the patient chronically, stroke resulted in the most deaths, while also causing chronic paralysis in the patients who survived. Research funding allocated to stroke by the National Institute of Health (NIH) has seen a rise of 51% between 2008 and 2021, $296 million to $447 million respectively [283]. Within the same period, funding for CP increased by 7% ($28 to $30 million), PD by 67% ($152 to $254 million), SCI by 26% ($80 to $101 million). The funding for MS and SCZ reduced by 25% ($169 to $126 million) and 2% ($249 to $242 million) respectively [283]. No data was found for BPI and PNI. The neurological conditions other than stroke and PD are underfunded and under-studied. Hence, it is recommended that future research endeavors focus on a more diverse patient population affected by neurological conditions/injuries.
A higher proportion of the studies reviewed were case-controlled or poor cohort/ case-controlled studies (LoE Level III and IV). The quality of a study is largely dependent on its design. It is widely accepted that RCTs (LoE Level I) are the “gold standard”, but there are certain disadvantages associated with them (e.g., expensive to conduct, monitoring biases, quality is dependent on degree of randomization, etc.) [284]. Due to these disadvantages, cohort studies (LoE Level II) are often preferred. Case–control studies are retrospective (LoE Level III), hence do not explore the incidence of the outcome. Case–control studies also have many shortcomings as discussed by Lewallen et. al. [285]. Hence, future studies on UE asymmetry should be designed as either a RCT or a cohort study (LoE Levels I or II).
Most of the tests performed in the articles collected objective data. Qualitative tests often require less personnel training to collect, are less time consuming, and do not require expensive equipment or sensors. However, they often depend on a skilled observer or a dedicated patient to report the outcome based on a set guideline. The subjective data collected is dependent on perception or feeling at the time of the test. They also require skilled observers and if not attentive, they may inadvertently induce bias. Objective data provides a more unambiguous and unbiased representation of outcome. The use of objective data for quantifying UE asymmetry increased between 2000 and 2022, and further studies are necessary to determine their applicability and reproducibility.
The reviewed articles extensively employed tests to capture the kinematics of patients across all studied conditions and injuries. Among the various methods used for studying the subject's kinematics, Optical Motion Capture (OMC) stood out as the most prominent. According to an article that reviewed the state of the art in human motion tracking, Optoelectronic measurement systems (also known as OMC systems) were found to be more accurate than other systems, but they relied on proper calibration [286]. In contrast, Electromagnetic motion tracking systems were less accurate than OMC. They exhibited greater susceptibility to electromagnetic noise and had a lower sampling rate [286]. On the other hand, Inertial Measurement Units (IMUs) gained significance as a wireless and marker less motion tracking technology in recent years. IMU-based systems offered advantages such as being lightweight, cost-effective, and portable. However, there were certain concerns related to angle calculation that needs careful consideration [287]. Therefore, selecting the appropriate motion tracking system became crucial and depended on the specific use-case at hand.
Force transducers, primarily handheld dynamometers, were the dominant type of test used, appearing in 33 instances. As Mendoza et al. highlighted, handheld dynamometry (HHD) offered an efficient, objective, sensitive, and cost-effective method for quantifying strength [288]. Nevertheless, recent literature indicates that HHD is prone to intertester variability, meaning that different testers may produce varying results when using the same device [289]. Additionally, the reliability of HHD is influenced by the strength of the tester, particularly when assessing larger muscle groups. This aspect must be considered while interpreting the results obtained through HHD measurements.
Activity monitoring tests were one of the popular forms of outcome measure applied. Hollis et. al. supported the use of accelerometry by stating that it “…is not contaminated by learning and practice effects that may occur with repeated administration of standard measures.” [238]. When used to measure limb use asymmetry, accelerometry has been well correlated with standard clinical assessments [174, 290]. De Lucena et. al. stated “If quality of movement during daily life is an outcome important to people with a stroke, perhaps kinematic analysis of accelerometry provides a window to assess it.” [232]. Lakhani et. al. suggested the use of accelerometry in conjunction with other outcome measures to predict impairment in individuals with chronic stroke [250]. Toba et. al. emphasized the importance of the method used to analyze the actigraphy data [276]. Hence, when used appropriately, activity monitors have the potential to become a valid outcome measure in clinical practice.
Studies adopting RWE based outcome measures have increased in the recent years. Rehabilitation of patients with neurological conditions/injuries aims at improving the use of the affected UE in daily living tasks [233]. Webber et. al. noted that “…collection of real world data places minimal burden on subjects and provides quantitative arm usage information previously inaccessible to clinicians.” [174]. Similar observations were made by other articles [240, 252, 278]. The U.S. Food and Drug Administration (FDA) emphasized the importance of real world data and real world evidence to supplement clinical data in medical device clearance and best practices development [291]. RWE based approaches provide a better understanding of the patient’s condition in their day-to-day life as opposed to data collection in a research/clinical setting [35]. Pau et. al. pointed out the shortcoming of in-clinic tests, stating “…clinical tests capture only limited information about individuals’ actual upper limb dysfunction…” [201]. John Doyle stated “Real-world patients are fundamentally different than clinical trial patients.”, hence supporting the use of RWE in medical device testing [292]. All these testimonies recommend RWE and data be used in prognostic, diagnostic, and rehabilitative care of patients. There are number of limitations associated with RWE as stated by Kim et. al. (need for experts for data analysis, high possibility of bias, lack of standardization, etc.) [293]. RWE based tests often require an extended period of data collection. These limitations make it difficult to maintain a large subject size. All studies reviewed had a statistically significant result but might have been underpowered since a power analysis was not provided. Hence, it is recommended that a power analysis be performed for RWE based studies and the population size be large enough to ensure reliable statistical analyses.
Limitations
There are limitations inherent to retrospective, scoping reviews. Only articles published within the range of 2000 and 2022 were considered for the review. Articles were selected from a list of articles only published in English (including English language translations). Hence, there is a possibility of missing the knowledge from publications in other languages. The software used for identifying the duplicate articles in the master list was trusted and the results were not cross referenced. There is a chance that some articles could have been overlooked due to the terms used for the electronic search. Hence, the search involved using multiple synonyms to reduce the risk of data loss. This review focused on multiple conditions and injuries. The quality assessment tools used for these conditions/injuries, though similar, still have some differences. We used the LoE to judge all the articles to facilitate a fair comparison. Systematic reviews, case studies, and book chapters were excluded from our review.
Conclusions
The discussed limitations notwithstanding, this review demonstrated the following:
-
More randomized controlled trials or cohort studies (LoE I or II) are needed in studies on UE asymmetry to improve the level of evidence being reported.
-
Real-world outcome measures should be collected more frequently.
-
Objective outcome measures should be given more importance.
-
UE asymmetry for neurological conditions other than stroke need to be studied.
-
Adequate power analysis must be performed to ensure reliable analyses.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- 3D:
-
Three dimensional
- AAUT:
-
Actual amount of use test
- ActM:
-
Activity monitoring
- ADL:
-
Activities of daily living
- AHA:
-
Assisting hand assessment
- AI:
-
Asymmetry index
- ALS:
-
Amyotrophic lateral sclerosis
- AoU:
-
Amount of use
- AoUT:
-
Amount of use tests
- AR2_24:
-
Asymmetry rate index for the 24-hour period
- ARAT:
-
Action reaction arm test
- BBT:
-
Box and block test
- BPI:
-
Brachial plexus injury
- CP:
-
Cerebral palsy
- CST:
-
Corticospinal tract
- DBS:
-
Deep brain stimulation
- DM:
-
Disability measures
- EA:
-
Error augmentation
- EDSS:
-
Expanded disability status scale
- EMG:
-
Electro myography
- FGMT:
-
Fine and gross motor tests
- FMA:
-
Fugl-Meyer assessment
- FMT:
-
Fine motor tests
- GMT:
-
Gross motor tests
- HABIT:
-
Hand–arm bimanual intensive therapy
- HCP:
-
Hemiparetic cerebral palsy
- HT:
-
Handedness tests
- KT:
-
Kinematics tests
- LHD:
-
Left hemisphere damage
- LoE:
-
Sackett’s level of evidence
- MACS:
-
Manual ability classification system
- MAL:
-
Motor activity log
- MCID:
-
Minimal clinically important difference
- MN:
-
Motor neglect
- mRS:
-
Modified Rankin scale
- MRT:
-
Motion reflex test
- MS:
-
Multiple sclerosis
- MWF:
-
Myelin water fraction
- NHPT:
-
Nine-hole peg test
- NIHSS:
-
National Institute of Health Stroke Scale
- PD:
-
Parkinson's disease
- PMT:
-
Peg moving task
- PNI:
-
Peripheral nerve injury
- QOL:
-
Quality of life surveys
- RCT:
-
Randomized controlled trial
- RHD:
-
Right hemisphere damage
- RWE:
-
Real world evidence
- SCI:
-
Spinal cord injury
- SCZ:
-
Schizophrenia
- SD:
-
Standard deviation
- SM:
-
Strength measures
- ST:
-
Spasticity tests
- UE:
-
Upper extremity
- USCP:
-
Unilateral spastic cerebral palsy
- VR:
-
Virtual reality
References
Tsao CW, Aday AW, Almarzooq ZI, Alonso A, Beaton AZ, Bittencourt MS, et al. Heart disease and stroke statistics—2022 update: a report from the American Heart Association. Circulation. 2022;145(8):e153–639.
Virani SS, Alonso A, Aparicio HJ, Benjamin EJ, Bittencourt MS, Callaway CW, et al. Heart disease and stroke statistics—2021 update: a report from the American Heart Association. Circulation. 2021;143(8):e254–743.
Dunbar M, Mineyko A, Hill M, Hodge J, Floer A, Kirton A. Population based birth prevalence of disease-specific perinatal stroke. Pediatrics. 2020. https://doi.org/10.1542/peds.2020-013201.
Kirton A, Deveber G. Life after perinatal stroke. Stroke. 2013;44(11):3265–71.
Kirton A, deVeber G. Paediatric stroke: pressing issues and promising directions. Lancet Neurol. 2015;14(1):92–102.
Oskoui M, Coutinho F, Dykeman J, Jette N, Pringsheim T. An update on the prevalence of cerebral palsy: a systematic review and meta-analysis. Dev Med Child Neurol. 2013;55(6):509–19.
Marras C, Beck J, Bower J, Roberts E, Ritz B, Ross G, et al. Prevalence of Parkinson’s disease across North America. NPJ Parkinson’s Dis. 2018;4(1):1–7.
Walton C, King R, Rechtman L, Kaye W, Leray E, Marrie RA, et al. Rising prevalence of multiple sclerosis worldwide: insights from the Atlas of MS. Mult Scler J. 2020;26(14):1816–21.
Talbott EO, Malek AM, Lacomis D. The epidemiology of amyotrophic lateral sclerosis. Handb Clin Neurol. 2016;138:225–38.
Noble J, Munro CA, Prasad VS, Midha R. Analysis of upper and lower extremity peripheral nerve injuries in a population of patients with multiple injuries. J Trauma Acute Care Surg. 1998;45(1):116–22.
Bekelis K, Missios S, Spinner RJ. Falls and peripheral nerve injuries: an age-dependent relationship. J Neurosurg. 2015;123(5):1223–9.
Faglioni W, Siqueira MG, Martins RS, Heise CO, Foroni L. The epidemiology of adult traumatic brachial plexus lesions in a large metropolis. Acta Neurochir. 2014;156(5):1025–8.
Chen Y, He Y, DeVivo MJ. Changing demographics and injury profile of new traumatic spinal cord injuries in the United States, 1972–2014. Arch Phys Med Rehabil. 2016;97(10):1610–9.
Yue JK, Hemmerle DD, Winkler EA, Thomas LH, Fernandez XD, Kyritsis N, et al. Clinical implementation of novel spinal cord perfusion pressure protocol in acute traumatic spinal cord injury at US level I trauma center: TRACK-SCI Study. World Neurosurg. 2020;133:e391–6.
Center NSCIS. Facts and figures at a glance. Birmingham, AL: University of Alabama at Birmingham. 2016;10.
Desrosiers J, Rochette A, Noreau L, Bourbonnais D, Bravo G, Bourget A. Long-term changes in participation after stroke. Top Stroke Rehabil. 2006;13(4):86–96.
Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2095–128.
Hung Y-C, Charles J, Gordon AM. Bimanual coordination during a goal-directed task in children with hemiplegic cerebral palsy. Dev Med Child Neurol. 2004;46(11):746–53.
Utley A, Steenbergen B, Sugden D. The influence of object size on discrete bimanual co-ordination in children with hemiplegic cerebral palsy. Disabil Rehabil. 2004;26(10):603–13.
Charles J, Gordon AM. Development of hand–arm bimanual intensive training (HABIT) for improving bimanual coordination in children with hemiplegic cerebral palsy. Dev Med Child Neurol. 2006;48(11):931–6.
Sakellariou VI, Badilas NK, Mazis GA, Stavropoulos NA, Kotoulas HK, Kyriakopoulos S, et al. Brachial plexus injuries in adults: evaluation and diagnostic approach. Int Sch Res Not. 2014. https://doi.org/10.1155/2014/726103.
Bertoni R, Lamers I, Chen CC, Feys P, Cattaneo D. Unilateral and bilateral upper limb dysfunction at body functions, activity and participation levels in people with multiple sclerosis. Mult Scler J. 2015;21(12):1566–74.
Holper L, Coenen M, Weise A, Stucki G, Cieza A, Kesselring J. Characterization of functioning in multiple sclerosis using the ICF. J Neurol. 2010;257(1):103–13.
Kraft GH, Amtmann D, Bennett SE, Finlayson M, Sutliff MH, Tullman M, et al. Assessment of upper extremity function in multiple sclerosis: review and opinion. Postgrad Med. 2014;126(5):102–8.
Gauggel S, Rieger M, Feghoff T. Inhibition of ongoing responses in patients with Parkinson’s disease. J Neurol Neurosurg Psychiatry. 2004;75(4):539–44.
Mancini C, Modugno N, Santilli M, Pavone L, Grillea G, Morace R, et al. Unilateral stimulation of subthalamic nucleus does not affect inhibitory control. Front Neurol. 2019;9:1149.
Mirabella G, Fragola M, Giannini G, Modugno N, Lakens D. Inhibitory control is not lateralized in Parkinson’s patients. Neuropsychologia. 2017;102:177–89.
Mirabella G, Iaconelli S, Romanelli P, Modugno N, Lena F, Manfredi M, et al. Deep brain stimulation of subthalamic nuclei affects arm response inhibition in Parkinson’s patients. Cereb Cortex. 2012;22(5):1124–32.
Obeso I, Wilkinson L, Jahanshahi M. Levodopa medication does not influence motor inhibition or conflict resolution in a conditional stop-signal task in Parkinson’s disease. Exp Brain Res. 2011;213(4):435–45.
Wylie SA, van Wouwe NC, Godfrey SG, Bissett PG, Logan GD, Kanoff KE, et al. Dopaminergic medication shifts the balance between going and stopping in Parkinson’s disease. Neuropsychologia. 2018;109:262–9.
Brattain K. Analysis of the peripheral nerve repair market in the United States. Magellan Med Technol Consult Inc Minneap. 2014.
Dyck PJ, Boes CJ, Mulder D, Millikan C, Windebank AJ, Dyck PJB, et al. History of standard scoring, notation, and summation of neuromuscular signs. A current survey and recommendation. J Peripher Nerv Syst. 2005;10(2):158–73.
He B, Zhu Z, Zhu Q, Zhou X, Zheng C, Li P, et al. Factors predicting sensory and motor recovery after the repair of upper limb peripheral nerve injuries. Neural Regen Res. 2014;9(6):661.
Kouyoumdjian JA, Graça CR, Ferreira VF. Peripheral nerve injuries: aretrospective survey of 1124 cases. Neurol India. 2017;65(3):551.
Sherman RE, Anderson SA, Dal Pan GJ, Gray GW, Gross T, Hunter NL, et al. Real-world evidence—what is it and what can it tell us. N Engl J Med. 2016;375(23):2293–7.
Wang Q, Markopoulos P, Yu B, Chen W, Timmermans A. Interactive wearable systems for upper body rehabilitation: a systematic review. J Neuroeng Rehabil. 2017;14(1):1–21.
Gebruers N, Vanroy C, Truijen S, Engelborghs S, De Deyn PP. Monitoring of physical activity after stroke: a systematic review of accelerometry-based measures. Arch Phys Med Rehabil. 2010;91(2):288–97.
Braito I, Maselli M, Sgandurra G, Inguaggiato E, Beani E, Cecchi F, et al. Assessment of upper limb use in children with typical development and neurodevelopmental disorders by inertial sensors: a systematic review. J Neuroeng Rehabil. 2018;15(1):1–18.
Kim RK, Kang N. Bimanual coordination functions between paretic and nonparetic arms: a systematic review and meta-analysis. J Stroke Cerebrovasc Dis. 2020;29(2): 104544.
Webber CM, Shin AY, Kaufman KR. Assessment of upper extremity function. J Hand Surg. 2019;44(7):600–5.
Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–73.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Int J Surg. 2021;88: 105906.
Paci M, Cigna C, Baccini M, Rinaldi LA. Types of article published in physiotherapy journals: a quantitative analysis. Physiother Res Int. 2009;14(4):203–12.
Schalow G, Vaher I, Jaigma P. Overreaching in coordination dynamics therapy in an athlete with a spinal cord injury. Electromyogr Clin Neurophysiol. 2008;48(2):83–95.
Kantak S, Jax S, Wittenberg G. Bimanual coordination: a missing piece of arm rehabilitation after stroke. Restor Neurol Neurosci. 2017;35(4):347–64.
Van De Oliveira MC, Demartino AM, Rodrigues LC, Gomes RP, Michaelsen SM. The activity assessment instruments of the upper limbs do contemplate the most accomplished tasks at home by people with hemiparesis? Braz J Occup Ther. 2018;26(4):809–27.
David A, Subash T, Varadhan SKM, Melendez-Calderon A, Balasubramanian S. A framework for sensor-based assessment of upper-limb functioning in hemiparesis. Front Hum Neurosci. 2021;15: 667509.
Arya K, Pandian S. Interlimb neural coupling: implications for poststroke hemiparesis. Ann Phys Rehabil Med. 2014;57(9–10):696–713.
Torrey M. therapeutic implementation of a custom dynamic elbow brace for children with neonatal brachial plexus palsy: a case report. Pediatr Phys Ther. 2021;33(1):E23–7.
Chin TY, Duncan JA, Johnstone BR, Graham HK. Management of the upper limb in cerebral palsy. J Pediatr Orthopaed B. 2005;14(6):389–404.
Ward AB. A literature review of the pathophysiology and onset of post-stroke spasticity. Eur J Neurol. 2012;19(1):21–7.
Bornheim S, Thibaut A, Beaudart C, Maquet P, Croisier J-L, Kaux J-F. Evaluating the effects of tDCS in stroke patients using functional outcomes: a systematic review. Disabil Rehabil. 2022;44(1):13–23.
Navarro-López V, Vázquez DF, Molina-Rueda F, Gómez AC, Prados PG, del Valle-Gratacos M, et al. Arm-swing kinematics in Parkinson’s disease: a systematic review and meta-analysis. Gait Posture. 2022. https://doi.org/10.1016/j.gaitpost.2022.08.017.
Bailey RR, Lang CE. Upper extremity activity in adults: referent values using accelerometry. J Rehabil Res Dev. 2014;50(9):1213.
Carpes FP, Geremia JM, Karolczak APB, Diefenthaeler F, Vaz MA. Preference and torque asymmetry for elbow joint. Motriz Revista Educacao Fisica. 2012;18(2):319–26.
Kwon JC, Cohen ML, Williamson J, Burtis B, Heilman KM. Bimanual-vertical hand movements. J Int Neuropsychol Soc. 2011;17(4):732–9.
Wylde MJ, Callaway AJ, Williams JM, Yap J, Leow S, Yong LC. Limb specific training magnitude and asymmetry measurement to discriminate between athletes with and without unilateral or bilateral lower limb injury history. Phys Ther Sport. 2022;56:76–83.
Bhullar A, Kang N, Idica J, Christou EA, Cauraugh JH. Increased visual information gain improves bimanual force coordination. Neurosci Lett. 2015;608:23–7.
Walker EH, Perreault EJ. Arm dominance affects feedforward strategy more than feedback sensitivity during a postural task. Exp Brain Res. 2015;233:2001–11.
Akpinar S, Sainburg RL, Kirazci S, Przybyla A. Motor asymmetry in elite fencers. J Mot Behav. 2015;47(4):302–11.
Kolber MJ, Hanney WJ, Cheatham SW, Salamh PA, Masaracchio M, Liu X. Shoulder joint and muscle characteristics among weight-training participants with and without impingement syndrome. J Strength Cond Res. 2017;31(4):1024–32.
Rincón D, Valderrama JA, Castaño-Pino YJ, Montilla L, Muñoz B, Orozco JL, et al., editors. Wearable system to measure asymmetry by sensing arms swing. 2019 IEEE international conference on E-health networking, application & services (HealthCom); 2019: IEEE.
Bagesteiro LB, Lima KO, Wang J. Interlimb differences in visuomotor and dynamic adaptation during targeted reaching in children. Hum Mov Sci. 2021;77: 102788.
Schaefer SY. Preserved motor asymmetry in late adulthood: is measuring chronological age enough? Neuroscience. 2015;294:51–9.
Cochet H, Centelles L, Jover M, Plachta S, Vauclair J. Hand preferences in preschool children: Reaching, pointing and symbolic gestures. Laterality Asymmetries Body Brain Cogn. 2015;20(4):501–16.
Córdova Bulens D, Crevecoeur F, Thonnard J-L, Lefèvre P. Optimal use of limb mechanics distributes control during bimanual tasks. J Neurophysiol. 2018;119(3):921–32.
Datta S, Karmakar CK, Yan B, Palaniswami M. Novel measures of similarity and asymmetry in upper limb activities for identifying hemiparetic severity in stroke survivors. IEEE J Biomed Health Inform. 2020;25(6):1964–74.
Gutnik B, Nicholson J, Nash D. A new conceptual model of asymmetry in motor performance for bidimensional fast-oscillating movements in selected variants of performance. Percept Mot Skills. 2000;91(1):155–87.
Lang CE, Waddell KJ, Klaesner JW, Bland MD. A method for quantifying upper limb performance in daily life using accelerometers. JoVE J Vis Exp. 2017;122: e55673.
Martin BJ, Adamo DE, editors. Contribution of sensory and motor components to motor control asymmetries: an analytical model approach. 2011 Annual International Conference of the IEEE Engineering in Medicine and Biology Society; 2011: IEEE.
Morouço PG, Marinho DA, Fernandes RJ, Marques MC. Quantification of upper limb kinetic asymmetries in front crawl swimming. Hum Mov Sci. 2015;40:185–92.
Przybyla A, Haaland KY, Bagesteiro LB, Sainburg RL. Motor asymmetry reduction in older adults. Neurosci Lett. 2011;489(2):99–104.
Sainburg RL, Schaefer SY, Yadav V. Lateralized motor control processes determine asymmetry of interlimb transfer. Neuroscience. 2016;334:26–38.
Serrien DJ, Sovijärvi-Spapé MM. Hemispheric asymmetries and the control of motor sequences. Behav Brain Res. 2015;283:30–6.
Teo W-P, Rodrigues JP, Mastaglia FL, Thickbroom GW. Changes in corticomotor excitability and inhibition after exercise are influenced by hand dominance and motor demand. Neuroscience. 2012;210:110–7.
Webber CM, Shin AY, Kaufman KR. Effects of elbow immobilization on upper extremity activity. Clin Biomech. 2020;80: 105106.
Ballanger B, Boulinguez P. EMG as a key tool to assess motor lateralization and hand reaction time asymmetries. J Neurosci Methods. 2009;179(1):85–9.
Bardo A, Kivell TL, Town K, Donati G, Ballieux H, Stamate C, et al. Get a grip: variation in human hand grip strength and implications for human evolution. Symmetry. 2021;13(7):1142.
Coley B, Jolles BM, Farron A, Aminian K. Arm position during daily activity. Gait Posture. 2008;28(4):581–7.
Graves LE, Ridgers ND, Stratton G. The contribution of upper limb and total body movement to adolescents’ energy expenditure whilst playing Nintendo Wii. Eur J Appl Physiol. 2008;104:617–23.
Kaneko M, Yamashita Y, Inomoto O, Iramina K. Soft neurological signs in childhood by measurement of arm movements using acceleration and angular velocity sensors. Sensors. 2015;15(10):25793–808.
Kim J, Song C. Postural difference between the interventions reflecting the concept of mirror therapy in healthy subjects. Brain Sci. 2021;11(12):1567.
Kons RL, Dal Pupo J, Gheller RG, Costa FE, Rodrigues MM, Bishop C, et al. Effects of successive judo matches on interlimb asymmetry and bilateral deficit. Phys Ther Sport. 2021;47:15–22.
Kuhtz-Buschbeck J, Brockmann K, Gilster R, Koch A, Stolze H. Asymmetry of arm-swing not related to handedness. Gait Posture. 2008;27(3):447–54.
Mahoney SJ, Hackney KJ, Jurivich DA, Dahl LJ, Johnson C, McGrath R. Handgrip strength asymmetry is associated with limitations in individual basic self-care tasks. J Appl Gerontol. 2022;41(2):450–4.
McGrath R, Vincent BM, Jurivich DA, Hackney KJ, Tomkinson GR, Dahl LJ, et al. Handgrip strength asymmetry and weakness together are associated with functional disability in aging Americans. J Gerontol Ser A. 2021;76(2):291–6.
Mirifar A, Cross-Villasana F, Beckmann J, Ehrlenspiel F. Effects of the unilateral dynamic handgrip on resting cortical activity levels: a replication and extension. Int J Psychophysiol. 2020;156:40–8.
Natale V. Circadian motor asymmetries in humans. Neurosci Lett. 2002;320(1–2):102–4.
Natale V, Lehnkering H, Siegmund R. Handedness and circadian motor asymmetries in humans: preliminary findings. Physiol Behav. 2010;100(4):322–6.
Sun C, Chu K, Miao Q, Li P, Zhong W, Qi S, et al. Bilateral asymmetry of hand force production in dynamic physically-coupled tasks. IEEE J Biomed Health Inform. 2021;26(4):1826–34.
Tzourio-Mazoyer N, Labache L, Zago L, Hesling I, Mazoyer B. Neural support of manual preference revealed by BOLD variations during right and left finger-tapping in a sample of 287 healthy adults balanced for handedness. Laterality. 2021;26(4):398–420.
Castro-Luna G, Jiménez-Rodríguez D. Relative and absolute reliability of a motor assessment system using KINECT® camera. Int J Environ Res Public Health. 2020;17(16):5807.
Chieffi S, Villano I, Iavarone A, Messina A, Monda V, Viggiano A, et al. Manual asymmetry for temporal and spatial parameters in sensorimotor synchronization. Exp Brain Res. 2017;235:1511–8.
Doustan M, Namazizadeh M, Sheikh M, Naghdi N. Evaluation of learning of asymmetrical bimanual tasks and transfer to converse pattern: load, temporal and spatial asymmetry of hand movements. Acta Gymnica. 2019;49(3):115–24.
Faria I, Diniz A, Barreiros J. Manual asymmetries in bimanual isochronous tapping tasks in children. Acta Physiol (Oxf). 2017;172:41–8.
Flindall JW, Doan JB, Gonzalez CL. Manual asymmetries in the kinematics of a reach-to-grasp action. Laterality Asymmetries Body Brain Cogn. 2014;19(4):489–507.
Ghacibeh GA, Mirpuri R, Drago V, Jeong Y, Heilman KM, Triggs WJ. Ipsilateral motor activation during unimanual and bimanual motor tasks. Clin Neurophysiol. 2007;118(2):325–32.
Gueugnon M, Torre K, Mottet D, Bonnetblanc F. Asymmetries of bilateral isometric force matching with movement intention and unilateral fatigue. Exp Brain Res. 2014;232:1699–706.
Haemi J, Jaehyun P. Comparative analyses of the dominant and non-dominant upper limbs during the abduction and adduction motions. Iran J Public Health. 2019;48(10):1768.
Jee H. Feasibility of a set of wrist-worn novice devices for dual motion comparison of the upper limbs during lateral raise motions. J Exerc Rehabil. 2019;15(4):531.
Main JC, Carey DP. One hand or the other? Effector selection biases in right and left handers. Neuropsychologia. 2014;64:300–9.
Rabuffetti M, Meriggi P, Pagliari C, Bartolomeo P, Ferrarin M. Differential actigraphy for monitoring asymmetry in upper limb motor activities. Physiol Meas. 2016;37(10):1798.
Sebastjan A, Skrzek A, Ignasiak Z, Sławińska T. Age-related changes in hand dominance and functional asymmetry in older adults. PLoS ONE. 2017;12(5): e0177845.
Summers JJ, Davis AS, Byblow WD. The acquisition of bimanual coordination is mediated by anisotropic coupling between the hands. Hum Mov Sci. 2002;21(5–6):699–721.
Teixeira LA, Caminha LQ. Intermanual transfer of force control is modulated by asymmetry of muscular strength. Exp Brain Res. 2003;149:312–9.
Lundh D, Coleman S, Riad J. Movement deviation and asymmetry assessment with three dimensional gait analysis of both upper-and lower extremity results in four different clinical relevant subgroups in unilateral cerebral palsy. Clin Biomech. 2014;29(4):381–6.
Jee H. Kinematic comparisons of increased exercise repetitions and intensities on the dominant and non-dominant upper limbs for prevention of dyskinesia. Iran J Public Health. 2020;49(10):1878–84.
Rincón D, Valderrama J, González MC, Muñoz B, Orozco J, Montilla L, et al. Wristbands containing accelerometers for objective arm swing analysis in patients with Parkinson’s disease. Sensors. 2020;20(15):4339.
Koh S-B, Park Y-M, Kim M-J, Kim W-S. Influences of elbow, shoulder, trunk motion and temporospatial parameters on arm swing asymmetry of Parkinson’s disease during walking. Hum Mov Sci. 2019;68: 102527.
Angelico F, Freslier M, Romkes J, Brunner R, Schmid S. Upper extremity motion during gait in adolescents with structural leg length discrepancy—an exploratory study. Gait Posture. 2017;53:115–20.
Andersson SA, Danielsson A, Ohlsson F, Wipenmyr J, Alt MM. Arm impairment and walking speed explain real-life activity of the affected arm and leg after stroke. J Rehabil Med. 2021;53(6): jrm00210.
Ferraris C, Amprimo G, Masi G, Vismara L, Cremascoli R, Sinagra S, et al. Evaluation of arm swing features and asymmetry during gait in Parkinson’s disease using the azure kinect sensor. Sensors. 2022. https://doi.org/10.3390/s22166282.
Gomez NG, Foreman KB, Hunt M, Merryweather AS. Upper-extremity kinematics and interlimb movement correlation in persons with Parkinson disease on irregular terrain, cross-slope, and under dual-task condition. Heliyon. 2022. https://doi.org/10.1016/j.heliyon.2022.e11223.
Dai J, Wu F, Li J, Yu M, Liao C, Shou Y. Surface electromyography analysis of mirror movements under unilateral movement in stroke patients: a retrospective study. Front Hum Neurosci. 2022. https://doi.org/10.3389/fnhum.2022.1079596.
Murphy A, Andersson S, Danielsson A, Wipenmyr J, Ohlsson F. Comparison of accelerometer-based arm, leg and trunk activity at weekdays and weekends during subacute inpatient rehabilitation after stroke. J Rehabil Med. 2019;51(6):426–33.
Plate A, Sedunko D, Pelykh O, Schlick C, Ilmberger J, Bötzel K. Normative data for arm swing asymmetry: how (a) symmetrical are we? Gait Posture. 2015;41(1):13–8.
Huang X, Mahoney JM, Lewis MM, Du G, Piazza SJ, Cusumano JP. Both coordination and symmetry of arm swing are reduced in Parkinson’s disease. Gait Posture. 2012;35(3):373–7.
Roggendorf J, Chen S, Baudrexel S, Van De Loo S, Seifried C, Hilker R. Arm swing asymmetry in Parkinson’s disease measured with ultrasound based motion analysis during treadmill gait. Gait Posture. 2012;35(1):116–20.
Uswatte G, Foo WL, Olmstead H, Lopez K, Holand A, Simms LB. Ambulatory monitoring of arm movement using accelerometry: an objective measure of upper-extremity rehabilitation in persons with chronic stroke. Arch Phys Med Rehabil. 2005;86(7):1498–501.
Le Moing A-G, Seferian AM, Moraux A, Annoussamy M, Dorveaux E, Gasnier E, et al. A movement monitor based on magneto-inertial sensors for non-ambulant patients with Duchenne muscular dystrophy: a pilot study in controlled environment. PLoS ONE. 2016;11(6): e0156696.
Mollineda RA, Chía D, Fernandez-Beltran R, Ortells J. Arm swing asymmetry measurement from 2D gait videos. Electronics. 2021;10(21):2602.
Markopoulos P, Timmermans AA, Beursgens L, Van Donselaar R, Seelen HA, editors. Us' em: the user-centered design of a device for motivating stroke patients to use their impaired arm-hand in daily life activities. 2011 Annual International Conference of the IEEE Engineering in Medicine and Biology Society; 2011: IEEE.
Okahashi S, Sakamoto K, Hashiya F, Kumasaka K, Yamaguchi T, Seiyama A, et al. Development of an electric pegboard (e-Peg) for hand dexterity improvement and cognitive rehabilitation: a preliminary study. Adv Biomed Eng. 2023;12:81–90.
Luster EL, McDaniel T, Fakhri B, Davis J, Goldberg M, Bala S, et al., editors. Vibrotactile cueing using wearable computers for overcoming learned non-use in chronic stroke. 2013 7th International Conference on Pervasive Computing Technologies for Healthcare and Workshops; 2013: IEEE.
Mohan A, Knutson JS, Cunningham DA, Widina M, O’Laughlin K, Arora T, et al. Contralaterally controlled functional electrical stimulation combined with brain stimulation for severe upper limb hemiplegia-study protocol for a randomized controlled trial. Front Neurol. 2022. https://doi.org/10.3389/fneur.2022.869733.
Hurd WJ, Morrow MM, Kaufman KR. Tri-axial accelerometer analysis techniques for evaluating functional use of the extremities. J Electromyogr Kinesiol. 2013;23(4):924–9.
Begliomini C, Sartori L, Miotto D, Stramare R, Motta R, Castiello U. Exploring manual asymmetries during grasping: a dynamic causal modeling approach. Front Psychol. 2015;6:167.
Sekaran SN, Reid SL, Chin AW, Ndiaye S, Licari MK. Catch! Movement kinematics of two-handed catching in boys with developmental coordination disorder. Gait Posture. 2012;36(1):27–32.
Ofir-Geva S, Meilijson I, Frenkel-Toledo S, Soroker N. Use of multi-perturbation Shapley analysis in lesion studies of functional networks: the case of upper limb paresis. Hum Brain Mapp. 2022. https://doi.org/10.1002/hbm.26105.
Padilla-Magaña JF, Peña-Pitarch E. Classification models of action research arm test activities in post-stroke patients based on human hand motion. Sensors (Basel). 2022. https://doi.org/10.3390/s22239078.
Almeida QJ, Wishart LR, Lee TD. Disruptive influences of a cued voluntary shift on coordinated movement in Parkinson’s disease. Neuropsychologia. 2003;41(4):442–52.
Platz T, Bock S, Prass K. Reduced skilfulness of arm motor behaviour among motor stroke patients with good clinical recovery: does it indicate reduced automaticity? Can it be improved by unilateral or bilateral training? A kinematic motion analysis study. Neuropsychologia. 2001;39(7):687–98.
Nawge S, Karthikbabu S. Does bimanual task training benefit manual ability and hand function of children with bilateral spastic cerebral palsy? J Pediatr Rehabil Med. 2023;16(1):49–57.
Brandao MB, Coster WJ, Figueiredo PRP, Amaral MF, Gordon AM, Mancini MC. Assisting hand use and self-care bimanual performance of children with unilateral spastic cerebral palsy. Dev Med Child Neurol. 2023;65(3):385–92.
Volman MJM, Wijnroks A, Vermeer A. Effect of task context on reaching performance in children with spastic hemiparesis. Clin Rehabil. 2002;16(6):684–92.
Volman MJM, Wijnroks A, Vermeer A. Bimanual circle drawing in children with spastic hemiparesis: effect of coupling modes on the performance of the impaired and unimpaired arms. Acta Psychol (Amst). 2002;110(2–3):339–56.
Lee J-S, Choi IJ, Shin MJ, Yoon J-A, Ko SH, Shin YB. Bone age in unilateral spastic cerebral palsy: is there a correlation with hand function and limb length? J Pediatr Endocrinol Metab. 2017;30(3):337–41.
Datta S, Karmakar CK, Rao AS, Yan B, Palaniswami M. Automated scoring of hemiparesis in acute stroke from measures of upper limb co-ordination using wearable accelerometry. IEEE Trans Neural Syst Rehabil Eng. 2020;28(4):805–16.
Gebruers N, Truijen S, Engelborghs S, DeDeyn PP. Predictive value of upper-limb accelerometry in acute stroke with hemiparesis. J Rehabil Res Dev. 2013;50(8):1099–106.
Tamas G, Szirmai I, Palvolgyi L, Takats A, Kamondi A. Impairment of post-movement beta synchronisation in parkinson’s disease is related to laterality of tremor. Clin Neurophysiol. 2003;114(4):614–23.
Verleger R, Adam S, Rose M, Vollmer C, Wauschkuhn B, Kompf D. Control of hand movements after striatocapsular stroke: high-resolution temporal analysis of the function of ipsilateral activation. Clin Neurophysiol. 2003;114(8):1468–76.
Graziadio S, Tomasevic L, Assenza G, Tecchio F, Eyre JA. The myth of the “unaffected” side after unilateral stroke: is reorganisation of the non-infarcted corticospinal system to re-establish balance the price for recovery? Exp Neurol. 2012;238(2):168–75.
Amano S, Umeji A, Uchita A, Hashimoto Y, Takebayashi T, Kanata Y, et al. Reliability of remote evaluation for the Fugl-Meyer assessment and the action research arm test in hemiparetic patients after stroke. TOP. 2018;25(6):432–7.
Amer M, Hubert G, Sullivan SJ, Herbison P, Franz EA, Hammond-Tooke GD. Reliability and diagnostic characteristics of clinical tests of upper limb motor function. J Clin Neurosci. 2012;19(9):1246–51.
Arwert H, Schut S, Boiten J, Vliet Vlieland T, Meesters J. Patient reported outcomes of hand function three years after stroke. TOP. 2018;25(1):13–9.
Fattapposta F, Pierelli F, Traversa G, My F, Mostarda M, D’Alessio C, et al. Preprogramming and control activity of bimanual self-paced motor task in Parkinson’s disease. Clin Neurophysiol. 2000;111(5):873–83.
Lidman GRM, Nachemson AK, Peny-Dahlstrand MB, Himmelmann KME. Long-term effects of repeated botulinum neurotoxin A, bimanual training, and splinting in young children with cerebral palsy. Dev Med Child Neurol. 2020;62(2):252–8.
van den Berg C, Beek PJ, Wagenaar RC, van Wieringen PC. Coordination disorders in patients with Parkinson’s disease: a study of paced rhythmic forearm movements. Exp Brain Res. 2000;134(2):174–86.
Sleimen-Malkoun R, Temprado J-J, Berton E. A dynamic systems approach to bimanual coordination in stroke: implications for rehabilitation and research. Medicina (Kaunas). 2010;46(6):374–81.
Liao W-W, Wu C-Y, Hsieh Y-W, Lin K-C, Chang W-Y. Effects of robot-assisted upper limb rehabilitation on daily function and real-world arm activity in patients with chronic stroke: a randomized controlled trial. Clin Rehabil. 2012;26(2):111–20.
Dewald JP, Beer RF. Abnormal joint torque patterns in the paretic upper limb of subjects with hemiparesis. Muscle Nerve. 2001;24(2):273–83.
Louwers A, Krumlinde-Sundholm L, Boeschoten K, Beelen A. Reliability of the Assisting Hand Assessment in adolescents. Dev Med Child Neurol. 2017;59(9):926–32.
Chae J, Labatia I, Yang G. Upper limb motor function in hemiparesis: concurrent validity of the arm motor ability test. Am J Phys Med Rehabil. 2003;82(1):1–8.
Dawe J, Yang JF, Fehlings D, Likitlersuang J, Rumney P, Zariffa J, et al. Validating accelerometry as a measure of arm movement for children with hemiplegic cerebral palsy. Phys Ther. 2019;99(6):721–9.
Gianutsos JG, Cohen JM, Batavia M. Test-retest reliability in performance of persons with hemiparesis tracking by means of compatibly displayed myoelectric feedback derived from upper limb muscles. Percept Mot Skills. 2004;98(1):19–30.
Turk R, Notley SV, Pickering RM, Simpson DM, Wright PA, Burridge JH. Reliability and sensitivity of a wrist rig to measure motor control and spasticity in poststroke hemiplegia. Neurorehabil Neural Repair. 2008;22(6):684–96.
Ovacik U, Tarakci E, Gungor F, Menengic KN, Leblebici G, Acar ZO, et al. The minnesota manual dexterity test as a bimanual performance measure in people with multiple sclerosis. Mult Scler Relat Disord. 2022;64: 103943.
Elvrum A-KG, Johansen GO, Vik T, Krumlinde-Sundholm L. External validity of the Both Hands Assessment for evaluating bimanual performance in children with bilateral cerebral palsy. Dev Med Child Neurol. 2022;64(5):586–92.
Decraene L, Feys H, Klingels K, Basu A, Ortibus E, Simon-Martinez C, et al. Tyneside Pegboard Test for unimanual and bimanual dexterity in unilateral cerebral palsy: association with sensorimotor impairment. Dev Med Child Neurol. 2021;63(7):874–82.
Lee HJ, Kim SK, Park H, Kim HB, Jeon HS, Jung YJ, et al. Clinicians’ tendencies to under-rate Parkinsonian tremors in the less affected hand. PLoS ONE. 2015;10(6): e0131703.
Scharoun SM, Bryden PJ, Sage MD, Almeida QJ, Roy EA. The influence of Parkinson’s disease motor symptom asymmetry on hand performance: an examination of the grooved pegboard task. Parkinson’s Dis. 2015;2015: 307474.
Burgess A, Boyd RN, Chatfield MD, Ziviani J, Sakzewski L. Hand function in 8- to 12-year-old children with bilateral cerebral palsy and interpretability of the both hands assessment. Phys Occup Ther Pediatr. 2021;41(4):358–71.
Pan Y-CP, Goodwin B, Sabelhaus E, Peters KM, Bjornson KF, Pham KLD, et al. Feasibility of using acceleration-derived jerk to quantify bimanual arm use. J Neuroeng Rehabil. 2020;17(1):44.
Frey S, Motawar B, Buchanan K, Kaufman C, Stevens P, Cirstea C, et al. Greater and more natural use of the upper limbs during everyday life by former amputees versus prosthesis users. Neurorehabil Neural Repair. 2022. https://doi.org/10.1177/15459683211062889.
Carey SL, Highsmith MJ, Maitland ME, Dubey RV. Compensatory movements of transradial prosthesis users during common tasks. Clin Biomech. 2008;23(9):1128–35.
Pascal A, Govaert P, Ortibus E, Naulaers G, Lars A, Fjørtoft T, et al. Motor outcome after perinatal stroke and early prediction of unilateral spastic cerebral palsy. Eur J Paediatr Neurol. 2020;29:54–61.
Aktas D, Eren B, Kenis-Coskun O, Karadag-Saygi E. Function in unaffected arms of children with obstetric brachial plexus palsy. Eur J Paediatr Neurol. 2018;22(4):610–4.
Mazzarella J, McNally M, Chaudhari AM, Pan X, Heathcock JC. Differences in coordination and timing of pre-reaching upper extremity movements may be an indicator of cerebral palsy in infants with stroke: a preliminary investigation. Clin Biomech. 2020;73:181–8.
Bahm J. Upper limb multifactorial movement analysis in brachial plexus birth injury. J Brach Plexus Peripher Nerve Injury. 2016. https://doi.org/10.1055/s-0036-1579762.
Agranovich OE, Oreshkov AB, Mikiashvili EF. Treatment approach to shoulder internal rotation deformity in children with obstetric brachial plexus palsy. Pediatr Traumatol Orthopaed Reconstr Surg. 2018;6(2):22–8.
Strohrmann C, Labruyère R, Gerber CN, van Hedel HJ, Arnrich B, Tröster G. Monitoring motor capacity changes of children during rehabilitation using body-worn sensors. J Neuroeng Rehabil. 2013;10:1–16.
Duff SV, Dayanidhi S, Kozin SH. Asymmetrical shoulder kinematics in children with brachial plexus birth palsy. Clin Biomech. 2007;22(6):630–8.
Nazarahari M, Chan KM, Rouhani H. A novel instrumented shoulder functional test using wearable sensors in patients with brachial plexus injury. J Shoulder Elbow Surg. 2021;30(8):e493–502.
Webber CM, Shin AY, Kaufman KR. Upper extremity function in the free living environment of adults with traumatic brachial plexus injuries. J Electromyogr Kinesiol. 2019. https://doi.org/10.1016/j.jelekin.2019.05.013.
Beani E, Maselli M, Sicola E, Perazza S, Cecchi F, Dario P, et al. Actigraph assessment for measuring upper limb activity in unilateral cerebral palsy. J Neuroeng Rehabil. 2019;16(1):1–8.
Dellatolas G, Nunes Filho G, Souza L, Nunes LG, Braga LW. Manual skill, hand skill asymmetry, and neuropsychological test performance in schoolchildren with spastic cerebral palsy. Laterality. 2005;10(2):161–82.
Friel KM, Kuo HC, Carmel JB, Rowny SB, Gordon AM. Improvements in hand function after intensive bimanual training are not associated with corticospinal tract dysgenesis in children with unilateral cerebral palsy. Exp Brain Res. 2014;232(6):2001–9.
Gaillard F, Cretual A, Cordillet S, Le Cornec C, Gonthier C, Bouvier B, et al. Kinematic motion abnormalities and bimanual performance in children with unilateral cerebral palsy. Dev Med Child Neurol. 2018;60(8):839–45.
Gordon AM, Schneider JA, Chinnan A, Charles JR. Efficacy of a hand–arm bimanual intensive therapy (HABIT) in children with hemiplegic cerebral palsy: a randomized control trial. Dev Med Child Neurol. 2007;49(11):830–8.
Hoyt CR, Brown SK, Sherman SK, Wood-Smith M, Van AN, Ortega M, et al. Using accelerometry for measurement of motor behavior in children: relationship of real-world movement to standardized evaluation. Res Dev Disabil. 2020;96: 103546.
Huang H-H, Ellis TD, Wagenaar RC, Fetters L. Effect of body-scaled information on reaching in children with hemiplegic cerebral palsy: a pilot study. Pediatr. 2014;26(1):28–37.
Hung YC, Zeng W. Accuracy constraints improve symmetric bimanual coordination for children with and without unilateral cerebral palsy. Dev Neurorehabil. 2020;23(3):176–84.
Kara OK, Yardimci BN, Livanelioglu A, Soylu AR. Examination of touch-coordinate errors of adolescents with unilateral spastic cerebral palsy at an aiming-tapping task. J Back Musculoskelet Rehabil. 2020;33(1):81–9.
Klevberg GL, Elvrum A-KG, Zucknick M, Elkjaer S, Ostensjo S, Krumlinde-Sundholm L, et al. Development of bimanual performance in young children with cerebral palsy. Dev Med Child Neurol. 2018;60(5):490–7.
Langan J, Doyle ST, Hurvitz EA, Brown SH. Influence of task on interlimb coordination in adults with cerebral palsy. Arch Phys Med Rehabil. 2010;91(10):1571–6.
McCall JV, Hu X, Kamper DG. Exploring kinetic and kinematic finger individuation capability in children with hemiplegic cerebral palsy. Percept Mot Skills. 2023;130(2):732–49.
Mutalib SA, Mace M, Burdet E. Bimanual coordination during a physically coupled task in unilateral spastic cerebral palsy children. J NeuroEng Rehabil. 2019. https://doi.org/10.1186/s12984-018-0454-z.
Ricken AXC, Savelsbergh GJP, Bennett SJ. Interception of moving objects while walking in children with spastic hemiparetic cerebral palsy. Disabil Rehabil. 2007;29(1):69–77.
Shum LC, Valdes BA, Hodges NJ, Van Der Loos HFM. Error augmentation in immersive virtual reality for bimanual upper-limb rehabilitation in individuals with and without hemiplegic cerebral palsy. IEEE Trans Neural Syst Rehabil Eng. 2020;28(2):541–9.
Smits-Engelsman BC, Rameckers EA, Duysens J. Muscle force generation and force control of finger movements in children with spastic hemiplegia during isometric tasks. Dev Med Child Neurol. 2005;47(5):337–42.
Steenbergen B, Thiel EV, Hulstijn W, Meulenbroek RGJ. The coordination of reaching and grasping in spastic hemiparesis. Hum Mov Sci. 2000;19(1):75–105.
Steenbergen B, Meulenbroek RGJ, Rosenbaum DA. Constraints on grip selection in hemiparetic cerebral palsy: effects of lesional side, end-point accuracy, and context. Brain Res Cogn Brain Res. 2004;19(2):145–59.
Steenbergen B, Charles J, Gordon AM. Fingertip force control during bimanual object lifting in hemiplegic cerebral palsy. Exp Brain Res. 2008;186(2):191–201.
Tomhave WA, Van Heest AE, Bagley A, James MA. Affected and contralateral hand strength and dexterity measures in children with hemiplegic cerebral palsy. J Hand Surg [Am]. 2015;40(5):900–7.
van Roon D, Steenbergen B, Hulstijn W. Reciprocal tapping in spastic hemiparesis. Clin Rehabil. 2000;14(6):592–600.
Van Thiel E, Meulenbroek RG, Hulstijn W, Steenbergen B. Kinematics of fast hemiparetic aiming movements toward stationary and moving targets. Exp Brain Res. 2000;132(2):230–42.
Van Thiel E, Steenbergen B. Shoulder and hand displacements during hitting, reaching, and grasping movements in hemiparetic cerebral palsy. Mot Control. 2001;5(2):166–82.
Verrel J, Bekkering H, Steenbergen B. Eye-hand coordination during manual object transport with the affected and less affected hand in adolescents with hemiparetic cerebral palsy. Exp Brain Res. 2008;187(1):107–16.
Volman MJM. Spatial coupling in children with hemiplegic cerebral palsy during bimanual circle and line drawing. Mot Control. 2005;9(4):395–416.
Xu K, Mai J, He L, Yan X, Chen Y. Surface electromyography of wrist flexors and extensors in children with hemiplegic cerebral palsy. PM R. 2015;7(3):270–5.
Pau M, Leban B, Deidda M, Porta M, Coghe G, Cattaneo D, et al. Use of wrist-worn accelerometers to quantify bilateral upper limb activity and asymmetry under free-living conditions in people with multiple sclerosis. Mult Scler Relat Disord. 2021;53: 103081.
Severijns D, Lemmens M, Thoelen R, Feys P. Motor fatigability after low-intensity hand grip exercises in persons with multiple sclerosis. Mult Scler Relat Disord. 2016;10:7–13.
Solaro C, Grange E, Di Giovanni R, Cattaneo D, Bertoni R, Prosperini L, et al. Nine Hole Peg Test asymmetry in refining upper limb assessment in multiple sclerosis. Mult Scler Relat Disord. 2020;45: 102422.
Unluer NO, Ozkan T, Yasa ME, Ates Y, Anlar O. An investigation of upper extremity function in patients with multiple sclerosis, and its relation with shoulder position sense and disability level. Somatosens Mot Res. 2019;36(3):189–94.
Di Caprio V, Modugno N, Mancini C, Olivola E, Mirabella G. Early-stage Parkinson’s patients show selective impairment in reactive but not proactive inhibition. Mov Disord. 2020;35(3):409–18.
Amano S, Hong SL, Sage JI, Torres EB. Behavioral inflexibility and motor dedifferentiation in persons with Parkinson’s disease: bilateral coordination deficits during a unimanual reaching task. Neurosci Lett. 2015;585:82–7.
Gorniak SL, McIntyre CC, Alberts JL. Bimanual force coordination in Parkinson’s disease patients with bilateral subthalamic deep brain stimulation. PLoS ONE. 2013. https://doi.org/10.1016/j.parkreldis.2007.11.014.
Ham JH, Lee JJ, Kim JS, Lee PH, Sohn YH. Is dominant-side onset associated with a better motor compensation in Parkinson’s disease? Mov Disord. 2015;30(14):1921–5.
Jackson GM, Jackson SR, Hindle JV. The control of bimanual reach-to-grasp movements in hemiparkinsonian patients. Exp Brain Res. 2000;132(3):390–8.
Louie S, Koop MM, Frenklach A, Bronte-Stewart H. Quantitative lateralized measures of bradykinesia at different stages of Parkinson’s disease: the role of the less affected side. Mov Disord. 2009;24(13):1991–7.
Schaefer LV, Loffler N, Klein J, Bittmann FN. Mechanomyography and acceleration show interlimb asymmetries in Parkinson patients without tremor compared to controls during a unilateral motor task. Sci. 2021;11(1):2631.
Stegemoller E, Zaman A, MacKinnon CD, Tillman MD, Hass CJ, Okun MS. Laterality of repetitive finger movement performance and clinical features of Parkinson’s disease. Hum Mov Sci. 2016;49:116–23.
Yang ZY, Ni JD, Long Z, Kuang LT, Tao SB. Unusual presentation of congenital radioulnar synostosis with osteoporosis, fragility fracture and nonunion: a case report and review of literature. World J Clin Cases. 2020;8(8):1538–46.
Philip BA, Thompson MR, Baune NA, Hyde M, Mackinnon SE. Failure to compensate: patients with nerve injury use their injured dominant hand, even when their nondominant is more dexterous. Arch Physical Med Rehabil. 2021. https://doi.org/10.1016/j.apmr.2021.10.010.
Bondi M, Kalsi-Ryan S, Delparte JJ, Burns AS. Differences in sensorimotor and functional recovery between the dominant and non-dominant upper extremity following cervical spinal cord injury. Spinal Cord. 2022;60(5):422–7.
Britten L, Coats R, Ichiyama R, Raza W, Jamil F, Astill S. Bimanual reach to grasp movements after cervical spinal cord injury. PLoS ONE [Electronic Resource]. 2017;12(4): e0175457.
Calabro FJ, Perez MA. Bilateral reach-to-grasp movement asymmetries after human spinal cord injury. J Neurophysiol. 2016;115(1):157–67.
Lei Y, Perez MA. Phase-dependent deficits during reach-to-grasp after human spinal cord injury. J Neurophysiol. 2018;119(1):251–61.
Lisi G, Nico D, Ribolsi M, Niolu C, Lacquaniti F, Siracusano A, et al. Asymmetries in initiation of aiming movements in schizophrenia. Neuropsychologia. 2018;109:200–7.
Akremi H, Higgins J, Aissaoui R, Nadeau S. Bilateral motor coordination during upper limb symmetric pushing movements at two levels of force resistance in healthy and post-stroke individuals. Hum Mov Sci. 2022;81: 102913.
Hmaied Assadi S, Barel H, Dudkiewicz I, Gross-Nevo RF, Rand D. Less-affected hand function is associated with independence in daily living: a longitudinal study poststroke. Stroke. 2022;53(3):939–46.
Bailey RR, Klaesner JW, Lang CE. Quantifying real-world upper-limb activity in nondisabled adults and adults with chronic stroke. Neurorehabil Neural Repair. 2015;29(10):969–78.
Bailey RR, Birkenmeier RL, Lang CE. Real-world affected upper limb activity in chronic stroke: an examination of potential modifying factors. TOP. 2015;22(1):26–33.
Basilio ML, Samora GAR, Pereira DAG, Parreira VF, Ada L, Teixeira-Salmela LF. Upper limb energy demand during unilateral arm crank submaximal exercise testing in individuals with chronic stroke. Arch Phys Med Rehabil. 2021;102(9):1755–63.
Bertrand AM, Mercier C, Shun PLW, Bourbonnais D, Desrosiers J. Effects of weakness on symmetrical bilateral grip force exertion in subjects with hemiparesis. J Neurophysiol. 2004;91(4):1579–85.
Biryukova EV, Kondur AA, Kotov SV, Turbina LG, Bobrov PD. Paretic and non-paretic arm motor deficit and recovery as a function of lesion lateralization and paresis severity: a biomechanical study. Hum Physiol. 2022;48(6):667–79.
Buxbaum LJ, Permaul P. Hand-centered attentional and motor asymmetries in unilateral neglect. Neuropsychologia. 2001;39(7):653–64.
Cai NHM, Drogos J, Dewald JPA, Gurari N. Individuals with hemiparetic stroke accurately match torques they generate about each elbow joint. Front Neurosci. 2019. https://doi.org/10.3389/fnins.2019.01293.
Calautti C, Jones PS, Persaud N, Guincestre JY, Naccarato M, Warburton EA, et al. Quantification of index tapping regularity after stroke with tri-axial accelerometry. Brain Res Bull. 2006;70(1):1–7.
Chae J, Yang G, Park BK, Labatia I. Muscle weakness and cocontraction in upper limb hemiparesis: relationship to motor impairment and physical disability. Neurorehabil Neural Repair. 2002;16(3):241–8.
Dash A, Dutta A, Lahiri U. Quantification of grip strength with complexity analysis of surface electromyogram for hemiplegic post-stroke patients. NeuroRehabilitation. 2019;45(1):45–56.
de Lucena DS, Stoller O, Rowe JB, Chan V, Reinkensmeyer DJ, editors. Wearable sensing for rehabilitation after stroke: bimanual jerk asymmetry encodes unique information about the variability of upper extremity recovery. 2017 International Conference on Rehabilitation Robotics (ICORR); 2017: IEEE.
de Niet M, Bussmann JB, Ribbers GM, Stam HJ. The stroke upper-limb activity monitor: its sensitivity to measure hemiplegic upper-limb activity during daily life. Arch Phys Med Rehabil. 2007;88(9):1121–6.
Gebruers N, Truijen S, Engelborghs S, Nagels G, Brouns R, De Deyn P. Actigraphic measurement of motor deficits in acute ischemic stroke. Cerebrovasc Dis. 2008;26(5):533–40.
Gosser SM, Rice MS. Efficiency of unimanual and bimanual reach in persons with and without stroke. TOP. 2015;22(1):56–62.
Gurari N, Drogos JM, Dewald JPA. Individuals with chronic hemiparetic stroke can correctly match forearm positions within a single arm. Clin Neurophysiol. 2017;128(1):18–30.
Harris JE, Eng JJ. Individuals with the dominant hand affected following stroke demonstrate less impairment than those with the nondominant hand affected. Neurorehabil Neural Repair. 2006;20(3):380–9.
Hollis A, Cole L, Zewdie E, Metzler MJ, Kirton A. Bilateral actigraphic quantification of upper extremity movement in hemiparetic children with perinatal stroke: a case control study. J Neuroeng Rehabil. 2021;18(1):1–10.
Hu XL, Tong KY, Li L. The mechanomyography of persons after stroke during isometric voluntary contractions. J Electromyogr Kinesiol. 2007;17(4):473–83.
Iacovelli C, Caliandro P, Rabuffetti M, Padua L, Simbolotti C, Reale G, et al. Actigraphic measurement of the upper limbs movements in acute stroke patients. J Neuroeng Rehabil. 2019;16(1):1–10.
Johnson BP, Westlake KP. Chronic poststroke deficits in gross and fine motor control of the ipsilesional upper limb. Am J Phys Med Rehabil. 2021;100(4):345–8.
Johnson T, Ridgeway G, Luchmee D, Jacob J, Kantak S. Bimanual coordination during reach-to-grasp actions is sensitive to task goal with distinctions between left- and right-hemispheric stroke. Exp Brain Res. 2022;240(9):2359–73.
Kang N, Cauraugh JH. Bimanual force variability and chronic stroke: asymmetrical hand control. PLoS ONE [Electronic Resource]. 2014;9(7): e101817.
Kang N, Cauraugh JH. Bilateral synergy as an index of force coordination in chronic stroke. Exp Brain Res. 2017;235(5):1501–9.
Kantak S, McGrath R, Zahedi N. Goal conceptualization and symmetry of arm movements affect bimanual coordination in individuals after stroke. Neurosci Lett. 2016;626:86–93.
Kantak SS, Zahedi N, McGrath RL. Task-dependent bimanual coordination after stroke: relationship with sensorimotor impairments. Arch Phys Med Rehabil. 2016;97(5):798–806.
Kim Y, Kim W-S, Koh K, Yoon B, Damiano DL, Shim JK. Deficits in motor abilities for multi-finger force control in hemiparetic stroke survivors. Exp Brain Res. 2016;234(8):2391–402.
Koesler IBM, Dafotakis M, Ameli M, Fink GR, Nowak DA. Electrical somatosensory stimulation improves movement kinematics of the affected hand following stroke. J Neurol Neurosurg Psychiatry. 2009;80(6):614–9.
Lai C-H, Sung W-H, Chiang S-L, Lu L-H, Lin C-H, Tung Y-C, et al. Bimanual coordination deficits in hands following stroke and their relationship with motor and functional performance. J Neuroeng Rehabil. 2019;16(1):101.
Lakhani B, Hayward KS, Boyd LA. Hemispheric asymmetry in myelin after stroke is related to motor impairment and function. NeuroImage Clin. 2017;14:344–53.
Lang CE, Edwards DF, Birkenmeier RL, Dromerick AW. Estimating minimal clinically important differences of upper-extremity measures early after stroke. Arch Phys Med Rehabil. 2008;89(9):1693–700.
Lang CE, Wagner JM, Edwards DF, Dromerick AW. Upper extremity use in people with hemiparesis in the first few weeks after stroke. J Neurol Phys Ther. 2007;31(2):56–63.
Lodha N, Misra G, Coombes SA, Christou EA, Cauraugh JH. Increased force variability in chronic stroke: contributions of force modulation below 1 Hz. PLoS ONE [Electronic Resource]. 2013;8(12): e83468.
Lee JP, Chen S, Tsai CT, Chung HC, Chang WD, Galeoto G. Characteristics associated with the differential activity of nondominant and dominant affected hands in patients with poststroke right hemiparesis. Occup Therapy Int. 2020. https://doi.org/10.1155/2020/2387378.
Lewis GN, Byblow WD. Bimanual coordination dynamics in poststroke hemiparetics. J Mot Behav. 2004;36(2):174–88.
Li S, Latash ML, Yue GH, Siemionow V, Sahgal V. The effects of stroke and age on finger interaction in multi-finger force production tasks. Clin Neurophysiol. 2003;114(9):1646–55.
Lodha N, Patten C, Coombes SA, Cauraugh JH. Bimanual force control strategies in chronic stroke: Finger extension versus power grip. Neuropsychologia. 2012;50(11):2536–45.
Lodha N, Coombes SA, Cauraugh JH. Bimanual isometric force control: asymmetry and coordination evidence post stroke. Clin Neurophysiol. 2012;123(4):787–95.
Maenza C, Good DC, Winstein CJ, Wagstaff DA, Sainburg RL. Functional deficits in the less-impaired arm of stroke survivors depend on hemisphere of damage and extent of paretic arm impairment. Neurorehabil Neural Repair. 2020;34(1):39–50.
McCrea PH, Eng JJ, Hodgson AJ. Time and magnitude of torque generation is impaired in both arms following stroke. Muscle Nerve. 2003;28(1):46–53.
Metrot J, Mottet D, Hauret I, van Dokkum L, Bonnin-Koang H-Y, Torre K, et al. Changes in bimanual coordination during the first 6 weeks after moderate hemiparetic stroke. Neurorehabil Neural Repair. 2013;27(3):251–9.
Morris JH, Van Wijck F. Responses of the less affected arm to bilateral upper limb task training in early rehabilitation after stroke: a randomized controlled trial. Arch Phys Med Rehabil. 2012;93(7):1129–37.
Noskin O, Krakauer JW, Lazar RM, Festa JR, Handy C, O’Brien KA, et al. Ipsilateral motor dysfunction from unilateral stroke: implications for the functional neuroanatomy of hemiparesis. J Neurol Neurosurg Psychiatry. 2008;79(4):401–6.
Olczak A, Truszczynska-Baszak A. Motor coordination and grip strength of the dominant and non-dominant affected upper limb depending on the body position-an observational study of patients after ischemic stroke. Brain sci. 2022;12(2):26.
Patel P, Lodha N. Dynamic bimanual force control in chronic stroke: contribution of non-paretic and paretic hands. Exp Brain Res. 2019;237(8):2123–33.
Pohl PS, Luchies CW, Stoker-Yates J, Duncan PW. Upper extremity control in adults post stroke with mild residual impairment. Neurorehabil Neural Repair. 2000;14(1):33–41.
Pollet AK, Patel P, Lodha N. Does the contribution of the paretic hand to bimanual tasks change with grip strength capacity following stroke? Neuropsychologia. 2022;168: 108186.
Prados-Roman E, Cabrera-Martos I, Lopez-Lopez L, Rodriguez-Torres J, Torres-Sanchez I, Ortiz-Rubio A, et al. Deficits underlying handgrip performance in mildly affected chronic stroke persons. TOP. 2021;28(3):190–7.
Reale G, Giovannini S, Iacovelli C, Castiglia SF, Picerno P, Zauli A, et al. Actigraphic measurement of the upper limbs for the prediction of ischemic stroke prognosis: an observational study. Sensors. 2021;21(7):2479.
Rinehart JK, Singleton RD, Adair JC, Sadek JR, Haaland KY. Arm use after left or right hemiparesis is influenced by hand preference. Stroke. 2009;40(2):545–50.
Rose D, Winstein C. The co-ordination of bimanual rapid aiming movements following stroke. Clin Rehabil. 2005;19(4):452–62.
Rose DK, Winstein CJ. Temporal coupling is more robust than spatial coupling: an investigation of interlimb coordination after stroke. J Mot Behav. 2013;45(4):313–24.
Siekierka-Kleiser E, Kleiser R, Wohlschläger A, Freund H-J, Seitz R. Quantitative assessment of recovery from motor hemineglect in acute stroke patients. Cerebrovasc Dis. 2006;21(5–6):307–14.
Soares AV, Borges Júnior NG, Domenech SC, Loch MSG. Deficits in upper limbs after stroke: Influences of functional hemispheric asymmetries. Revista Neurociencias. 2015;23(2):260–6.
Song R, Tong KY. EMG and kinematic analysis of sensorimotor control for patients after stroke using cyclic voluntary movement with visual feedback. J Neuroeng Rehabil. 2013;10:18.
Toba MN, Pagliari C, Rabuffetti M, Nighoghossian N, Rode G, Cotton F, et al. Quantitative assessment of motor neglect. Stroke. 2021;52(5):1618–27.
Uswatte G, Miltner WH, Foo B, Varma M, Moran S, Taub E. Objective measurement of functional upper-extremity movement using accelerometer recordings transformed with a threshold filter. Stroke. 2000;31(3):662–7.
Uswatte G, Giuliani C, Winstein C, Zeringue A, Hobbs L, Wolf SL. Validity of accelerometry for monitoring real-world arm activity in patients with subacute stroke: evidence from the extremity constraint-induced therapy evaluation trial. Arch Phys Med Rehabil. 2006;87(10):1340–5.
Varghese R, Kutch JJ, Schweighofer N, Winstein CJ. The probability of choosing both hands depends on an interaction between motor capacity and limb-specific control in chronic stroke. Exp Brain Res. 2020;238(11):2569–79.
McCombe Waller S, Harris-Love M, Liu W, Whitall J. Temporal coordination of the arms during bilateral simultaneous and sequential movements in patients with chronic hemiparesis. Exp Brain Res. 2006;168(3):450–4.
Whitford M, Schearer E, Rowlett M. Effects of in home high dose accelerometer-based feedback on perceived and actual use in participants chronic post-stroke. Physiotherapy Theory Pract. 2018. https://doi.org/10.1080/09593985.2018.1493759.
Yang C-L, Liu J, Simpson LA, Menon C, Eng JJ. Real-world functional grasping activity in individuals with stroke and healthy controls using a novel wearable wrist sensor. Neurorehabil Neural Repair. 2021;35(10):929–37.
Estimates of Funding for Various Research, Condition, and Disease Categories (RCDC): National Institutes of Health (NIH); 2022. https://report.nih.gov/funding/categorical-spending#/.
Saturni S, Bellini F, Braido F, Paggiaro P, Sanduzzi A, Scichilone N, et al. Randomized controlled trials and real life studies. Approaches and methodologies: a clinical point of view. Pulm Pharmacol Ther. 2014;27(2):129–38.
Lewallen S, Courtright P. Epidemiology in practice: case-control studies. Community Eye Health. 1998;11(28):57.
Van der Kruk E, Reijne MM. Accuracy of human motion capture systems for sport applications; state-of-the-art review. Eur J Sport Sci. 2018;18(6):806–19.
Ribeiro NF, Santos CP, editors. Inertial measurement units: A brief state of the art on gait analysis. 2017 IEEE 5th Portuguese Meeting on Bioengineering (ENBENG); 2017: IEEE.
Mendoza M, Miller RG. Muscle Strength, Assessment of. 2003.
Clarke M, Mhuircheartaigh NDA, Walsh G, Walsh J, Meldrum D. Intra-tester and inter-tester reliability of the MicroFET 3 hand-held dynamometer. Physiotherapy Pract Res. 2011;32(1):13–8.
Noorkõiv M, Rodgers H, Price CI. Accelerometer measurement of upper extremity movement after stroke: a systematic review of clinical studies. J Neuroeng Rehabil. 2014;11(1):1–11.
Food U, Administration D. Use of real-world evidence to support regulatory decision-making for medical devices. Guidance for Industry and Food and Drug Administration Staff Washington, DC: FDA. 2017.
Shore C, Gee AW, Kahn B, Forstag EH, National Academies of Sciences E, Medicine, editors. Barriers and disincentives to the use of real-world evidence and real-world data. Examining the impact of real-world evidence on medical product development: Proceedings of a Workshop Series; 2019: National Academies Press (US).
Kim H-S, Lee S, Kim JH. Real-world evidence versus randomized controlled trial: clinical research based on electronic medical records. J Korean Med Sci. 2018. https://doi.org/10.3346/jkms.2018.33.e213.
Acknowledgements
The authors would like to thank Leslie Hassett (Mayo Clinic Libraries, Mayo Clinic, Rochester, MN, U.S.A.) for helping us with the followup literature search.
Funding
Funding for this work was provided from the Department of Defense grant W81XWH-20–1-0923, a generous grant from a Mayo Clinic benefactor who wishes to remain anonymous, and by the generosity of W. Hall Wendel, Jr.
Author information
Authors and Affiliations
Contributions
SGB performed the initial searches, selected the articles, extracted the data, and wrote the initial drafts of the manuscript. AYS and KRK guided the review process. All the authors were involved in writing and reviewing the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable. The current article reviews published studies.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Bhat, S.G., Shin, A.Y. & Kaufman, K.R. Upper extremity asymmetry due to nerve injuries or central neurologic conditions: a scoping review. J NeuroEngineering Rehabil 20, 151 (2023). https://doi.org/10.1186/s12984-023-01277-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12984-023-01277-7