
Abstract
Background
The most common endocrine and metabolic disorders in premenopausal women is polycystic ovary syndrome (PCOS), characterized by hyperandrogenism, chronic anovulation, and/or ultrasound evidence of small ovarian cysts. Obesity and insulin resistance are also the main factors influencing the clinical manifestations of this syndrome. Alzheimer’s disease (AD) is the most typical progressive neurodegenerative disorder of the brain, and recent studies suggest a relationship between endocrinal dysregulation and neuronal loss during AD pathology.
Aim
This study aimed to evaluate the common risk factors for Alzheimer’s and PCOS based on previous studies. Knowing the common risk factors and eliminating them may prevent neurodegenerative Alzheimer’s disease in the future.
Method
In this narrative review, international databases, including Google Scholar, Scopus, PubMed, and the Web of Science, were searched to retrieve the relevant studies. The relevant studies’ summaries were categorized to discuss the possible pathways that may explain the association between Alzheimer’s and PCOS signs/symptoms and complications.
Results
According to our research, the factors involved in Alzheimer’s and PCOS disorders may share some common risk factors. In patients with PCOS, increased LH to FSH ratio, decreased vitamin D, insulin resistance, and obesity are some of the most important factors that may increase the risk of Alzheimer’s disease.
Plain English summary
Polycystic ovary syndrome is a disorder of the female reproductive system that can be caused by hormonal disorders. The disease is detected by an ultrasound of the ovaries with small ovarian cysts. Obesity and insulin resistance are among the factors that can affect the clinical symptoms of this disease. Obesity due to high-fat consumption can affect cognitive functions with age. Alzheimer’s is the most common disease associated with disorders in brain cells; a link between hormonal disorders and Alzheimer’s has recently been reported. We conducted a review of reports and articles published in connection with polycystic ovary syndrome and neurodegenerative disorders in reputable scientific databases. Studies have shown that the factors involved in polycystic ovary syndrome and Alzheimer’s disease may indicate that both diseases have common risk factors. It may be linked to the symptoms and/or complications of Alzheimer’s disease and polycystic ovary syndrome. Future preclinical studies are needed to closely examine the mechanisms associated with polycystic ovary syndrome and the association with Alzheimer’s. The novelty of our study is from the fact that the PCOS may be to some extent considered as a cause (exposure) among others of AD’s (outcome) and the association might be confounded by some or all the risk factors assessed in this review. The nature of the method—the narrative review—is relatively subjective (in the determination of which studies to include, the way the studies are analyzed, and the conclusions drawn) and hence may not help mitigate bias.
Similar content being viewed by others


Introduction
Polycystic ovary syndrome (PCOS) is a heterogeneous group of disorders with metabolic and endocrine disorders that affect 8–10% of women of reproductive age [1]. PCOS often shows a wide range of metabolic changes, such as insulin resistance (IR), blood lipids, obesity, inflammation, increased oxidative stress, and hormonal changes [2]. The exact cause of PCOS is not known, but genetic and environmental factors appear to be involved. Recent studies have shown that hyperandrogenism (HA) and IR are the main causes and primary features of PCOS. Furthermore, these factors can influence the onset and progression of PCOS [3].
IR directly or indirectly enhances androgen synthesis and secretion; hyperandrogenism stimulates the breakdown of visceral adipose tissue, leading to an increase in free fatty acids, which intensifies IR levels. Eventually, this can create a vicious cycle between hyperandrogenemia and IR in PCOS and lead to development and progression [4]. Insulin also affects central nervous system (CNS) function by playing a role in regulating energy homeostasis, central action on peripheral glucose metabolism, learning, memory, cognition, and survival of brain neurons in adults [5]. Therefore, any disturbance in insulin metabolism in the CNS may have adverse effects on brain function and cognitive activity [6].
Alzheimer’s disease (AD) is an irreversible and progressive disorder with neuronal destruction characterized by behavioral changes and cognitive function loss in the elderly. AD accounts for 60 to 80% of dementia cases [7]. Approximately 46 million people have dementia globally, and this number is projected to increase to 131.5 million by 2050 [8]. Common symptoms include short-term memory loss, cognitive impairment, and inability to perform tasks in daily life [9]. Definitive diagnosis of the disease is usually made only after postmortem examination in which the histopathological examination of senile plaques and neurofibrillary tangles tau can be diagnosed. However, today there are research institutes that can diagnose amyloid and tau burden in living patients, and thus this historical paradigm has challenged the definitive diagnosis of the disease [10].
Intracellular inclusions of tau protein in the form of neurofibrillary tangles and extracellular plaque formation by the accumulation of the amyloid beta-peptide (Aβ) derived from the β-amyloid precursor protein (APP) are two primary pathological lesions in the brains of Alzheimer’s patients [11]. Neurosteroids and sex steroids have been suggested as one reason for reducing the pathology of AD. Alzheimer’s is more common in women than men, and estrogen depletion is generally associated with an increased risk of AD [12]. The age-related decrease in brain levels of testosterone in men and 17β-estradiol (E2) in women during menopause has been associated with a greater risk of developing AD [12].
Loss of neurons and synapses leads to atrophy of the cortex and subcortical areas [13]. Neurodegeneration in AD is associated with unregulated lipid and carbohydrate metabolism, cytokine-mediated inflammation, increased oxidative and cellular stress, ongoing cell death, and vascular destruction [14]. These factors are also present in type 2 diabetes, metabolic syndrome, and non-alcoholic fatty liver disease and support the notion that insulin-resistant diseases are all related and could have the same origins, and may be managed by similar if not identical therapeutic strategies.
Evidence suggests that, in addition to hormonal disorders and obesity, vitamin deficiencies and sleep disorders are also risk factors for this disease [15].
There is no effective treatment to prevent or slow the progression of AD. But in this context, it should also be emphasized that factors considered protective, such as physical exercise, diet, and cognitive stimuli should be strongly and widely encouraged [16].
Because Alzheimer’s patients have risk factors similar to those of PCOS, such as insulin resistance, vitamin D deficiency, sexual hormonal changes, inflammation, and sleep disorders, it may be hypothesized that PCOS may increase the risk of Alzheimer’s disease. This narrative review aimed to summarize the possible pathways that may explain the association between Alzheimer’s and PCOS.
Methods
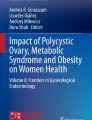
A comprehensive search of Google Scholar, Scopus, PubMed, and the Web of Science (until February 01, 2021) was conducted during this review. Search parameters, MeSH indexing terms, included polycystic ovary syndrome, PCOS, vitamin D, obesity, sex hormones, androgens, estrogens, progesterone, insulin resistance, sleep apnea, memory, Alzheimer disease, and dementia. All original and review studies in English based on the keywords searched in the database mentioned above, studies on humans and animal models, and published from 1973 to 2021 were included in our study. Non-English studies, conference abstracts, chapters of books, letters to the editor, and ex vivo studies were excluded. At the last screening among articles that had met the inclusion criteria, those which repeatedly stated the scientific facts were removed, and those with more up-to-date topics were selected. In addition, in all cases, common pathways leading to Alzheimer’s disease and PCOS were considered. A total of 2876 articles from four databases were identified, and 118 studies that had inclusion criteria were subjected to careful review (Fig. 1).

The flow diagram of study selection for the present literature review on the poly cystic ovary syndrome (PCOS), and Alzheimer’s disease
Results
Hypothalamic–pituitary–gonadal axis and estrogen
The hypothalamic–pituitary–gonadal (HPG) plays an essential role in regulating various activities, and an impaired HPG axis can cause polycystic ovary syndrome; sex hormone levels are regulated by the HPG [17, 18]. Deregulation in the HPG axis leads to menopause in women and andropause in men [19].
HPG axis hormone receptors (including steroid hormones, human chorionic gonadotropin, LH, and GnRH) are concentrated in the limbic system, especially hippocampal pyramidal neurons, and are involved in regulating the growth, structure, and function of the adult brain. These sections are very sensitive to AD pathology [20,21,22].
Estrogen receptors (ERs) by activating brain-derived neurotrophic factor (BDNF) have an essential effect on AD, and a significant reduction in postmenopausal estrogen may increase the risk of Alzheimer’s [23, 24]. Decreased sex gland hormones and increased gonadotropins such as LH are involved in cognitive dysfunction in aging and the pathogenesis of age-related disorders such as AD. This is especially important for women, who are twice as likely to develop postmenopausal AD [25]. The estrogen receptor network is one of the significant regulatory systems in the brain; under its influence, the brain responds to the ovarian-neural estrogen axis at appropriate intervals to regulate its energy metabolism [26]. The Hippocampus, Prefrontal cortex, amygdala, and posterior cingulate cortex of the brain regions with substantial estrogen receptors are essential for learning and memory [27].
Because estrogen’s protective effect on the brain is known, estrogen loss during menopause can partly lead to impaired brain metabolism and mitochondrial dysfunction in AD [28]. In this regard, several studies have shown a strong association between decreased estrogen levels during menopause and AD development [11, 29]. Studies using estradiol as the physiological form of estrogen have also shown that estrogen stabilizes or improves cognition in women with AD [30]. Estrogen modulates neurogenesis by modulating learning and memory in the hippocampus in various species, from rodents to primates [31].
Due to the significant role of hormones in memory and cognition, in addition to clinical and epidemiological studies of estrogen and androgens in AD, it is necessary to study other hormones involved in the HPG axis.
Hypothalamic–pituitary–gonadal axis dysfunction
The ratio of luteinizing hormone (LH) to follicle-stimulating hormone (FSH) (LH/FSH ratio) in women with PCOS is significantly higher than in normal women of the same age [32], and increasing this ratio is a powerful indicator of PCOS [33]. In these patients, the increase in LH secretion may be due to a defective hypothalamic–pituitary–ovarian axis [34]. LH is a gonadotropin secreted by the anterior pituitary gland that binds to luteinizing hormone receptors (LHR) and is found in the tissues of the gonad and non-gonad [35]. In patients with PCOS, by increasing LH, the ovarian theca cells produce excess androgens, and low FSH contributes to impaired folliculogenesis and ovulation [3]. Interestingly, IR and hyperinsulinemia, which are prominent PCOS features, stimulate LH secretion from the pituitary gland (thus increasing the LH/FSH ratio) and increase androgen production in ovarian follicular cells [36]. LH in the ovaries and testes stimulates the production of gonadal hormones, including estrogens and androgens [37]. An increase in LH increases androstenedione’s production is converted to testosterone by 17β reductase in thecal cells and released into the blood [38]. Androstenedione can also be converted to estradiol by the FSH-dependent aromatase enzyme in ovarian granulosa cells [39].
Because in PCOS, LH levels are high compared to FSH, androstenedione accumulates in the ovaries. In the early stages, androstenedione causes the follicles to grow; however, the persistence of high levels promotes the growth of most follicles as they mature, so ovulation does not lead to the accumulation of antral follicles, and the ovary becomes polycystic [40]. Increased LH levels compared to FSH in PCOS cause more conversion of androstenedione to testosterone, leading to hirsutism [41].
LH increases with age in both men and women. This hormone may be the main hormone in cognitive dysfunction and AD [42]. In this regard, the evidence in epidemiological studies supports the increase of LH in exacerbating the age-related cognitive decline in men and women [42]. There is an inverse relationship between LH and memory, and most studies show a correlation between serum LH concentration and amyloid-beta plasma accumulation and deposition [43]. Elevated LH levels are involved in Aβ metabolism and accumulation and are associated with an increased risk of AD [20]. Some studies suggest a link between LH and BDNF in the hippocampus, and these studies suggest that estrogen-increasing and LH-lowering treatments may both require BDNF signaling to improve spatial memory [44]. While most studies have shown that LH increases BDNF levels in gonadal tissue, some studies have shown that LH decreases BDNF levels in the CNS [44]. Genetic defects in the amyloid beta-AD pathway may increase GnRH and LH, which in turn may have a spiral effect on AD neurotoxicity.
There is not much research on the possible effects of FSH in this area, although one study found that there was a correlation between higher cognitive function in older women and increased FSH levels [45]. However, as mentioned earlier, LH has the most significant effect on the hippocampus, and more research is needed.
Insulin resistance (IR)
Insulin resistance is a pathological condition in which cells fail to respond to normal circulating insulin levels, so insulin cannot provide average glucose and lipid homeostasis [46]. IR and hyperinsulinemia play a major role in the cause of PCOS, and 50% to 70% of these patients are presented with IR [47]. IR is an essential regulator of androgen synthesis and IR resistance is common in some diseases, such as PCOS, AD, Parkinson’s diseases, and several cancers [3, 48,49,50].
Insulin is a major trophic factor in brain development [51] and, insulin irregularity and IR are other features of endocrine changes in the pathology of AD that may play a role in disease progression [52]. As a result, patients with impaired insulin metabolism may be at a higher risk of developing Alzheimer’s disease [5]. Women with PCOS are more prone to a wide range of complications from metabolic disorders, so the question is whether PCOS can make women more susceptible to AD?
Metabolic diseases impair brain health and cognitive function [53], and insulin signaling affects the hippocampus’s molecular cascades of flexibility, learning, and memory [54]. Insulin has a wide range of effects on the CNS and regulates critical processes such as energy homeostasis, endocrine reproduction, learning, memory, and neuronal survival in adults [5]. Insulin regulates neural proliferation, apoptosis, and synaptic transmission, and has pleiotropic effects on neurons [55]. There is a mechanical link between Aβ metabolism and insulin resistance. It has been shown that in advanced AD cases, the higher the Aβ level, the more insulin receptors are removed from the cell surface [52]. Studies have shown that IR or deficiency impairs learning and memory, so that insulin administration improves working memory and cognition and increases Aβ42 clearance in the brain [56].
Alzheimer’s disease should be considered as a degenerative metabolic disease due to brain insulin resistance and deficiency. Impaired insulin signaling can involve many essential abnormalities in AD, including neuroinflammation [57]. Neuroinflammation exacerbates IR, neurotoxicity, and cell death due to oxidation, gliosis, and toxicity of Aβ42 means that the association between IR and neuroinflammation is very close [57].
Inflammation and obesity
PCOS women are at higher risk for impaired fat metabolism. Abdominal obesity in PCOS patients is related to IR, hyperandrogenism, regular ovulation, and inflammation [40, 41]. On the other hand, central obesity exacerbates endocrine and metabolic disorders in PCOS [58]. Obesity is associated with an increase in inflammatory factors; including interleukins and peptides associated with the calcitonin gene, and it can upregulate ovarian androgen production [59]. Inflammatory genes, such as interleukin-1 beta (IL-1β), IL-8, leukemia inhibitory factor (LIF), NOS2, and prostaglandin-endoperoxide synthase 2 (PTGS2), are over-expressed in granulosa cells (GCs) of PCOS patients, indicating inflammation of the ovarian GC responses [60]. TNFα, as a proinflammatory agent, may exacerbate the development of IR in PCOS women [3].
Neuro-inflammation is a primary and consistent feature in many neurodegenerative diseases, including AD [61]. Overweight people and diabetics are at higher risk for cognitive impairment and dementia [45], and by comparing obese and thin patients of the same age, obese patients show a higher degree of hyperandrogenism. Some studies have also shown that free fatty acids promote the development of amyloid fibers and tau in vitro [62], and therefore, obesity is associated with mild cognitive impairment and changes in the structure and function of the hippocampus [63, 64]. Free fatty acids contribute to Alzheimer’s pathology by causing inflammation, enhancing Aβ deposition, and inhibiting clearance of Aβ [65].
Increased expression of proinflammatory cytokines in the vicinity of Aβ42 plaques indicates that neuroinflammation is an essential mediator of AD neuro-degradation [66].
Also, neuro-inflammation promotes neuronal injury and cholinergic dysfunction [67]. In this regard, epidemiological studies have shown that people who take chronic anti-inflammatory drugs or antioxidants have a lower risk of developing cognitive impairment and AD [68]. Increased systemic inflammation is thought to cause changes in the microglia, resulting in inflammation in the CNS, and may increase the risk of cognitive aging and Alzheimer’s disease [69].
Because sleep disorders have essential effects on inflammatory biology, inflammation may be a biologically acceptable pathway and a link between sleep disorders and the risk of Alzheimer’s disease [70].
Obstructive sleep apnea (OSA)
Obstructive sleep apnea (OSA) is characterized by partial or total obstruction of the upper airways and recurrence during sleep that leads to intermittent hypoxemia, of which obesity is a pillar of its physical pathology [71]. Obese women with PCOS are more likely to develop obstructive sleep apnea than healthy women [72, 73].
Studies show that androgens affect sleep patterns and lead to OSA development [74, 75]. As a result, women with PCOS have higher respiratory sleep levels, which may be associated with increased androgen levels associated with the syndrome [71]. Due to hormonal disorders, the prevalence of OSA is higher in women with PCOS compared with women without PCOS [76]. A wide range of hormonal and metabolic abnormalities in PCOS is also associated with people's hormonal profiles with OSA [77]. The increasing prevalence of obstructive sleep apnea in PCOS patients is associated with an increase in androgens or a decrease in estrogens and an increase in visceral adiposity [78]. Studies have shown that higher levels of testosterone in PCOS patients are related to OSA [79]. This is why sleep disorders in patients with PCOS are twice as common as in ordinary people [80]. Hyperandrogenism, IR, and low estrogen and progesterone levels with PCOS have all been suggested to cause OSA in PCOS patients [81]. IR is associated with irregular sleep breathing [3]. Progesterone increases respiratory pressure and the muscles’ function that dilates the upper airway [82]. This is why hormone therapy in postmenopausal women can be a protective factor against obstructive sleep apnea syndrome.
Evidence suggests that sleep disorders may lead to cognitive decline by increasing β-amyloid load, which increases the risk of dementia in AD [15]. On the other hand, respiratory disorders during sleep increase the risk of dementia and AD [83]. In humans, the concentration of β-amyloid in CSF fluctuates and increases during the day and decreases at night, and sleep deprivation or insomnia can affect the pattern of secretion [84].
Animal studies show that sleep increases clearance of soluble β-amyloid, and sleep–wake activity disorders interfere with eliminating potentially neurotoxic waste products, such as β-amyloid, which accumulate during the waking period [85, 86]. Evidence suggests that depression is a risk factor for cognitive decline and dementia and that sleep disorders and insomnia can be risk factors for depression and recurrence of depression [87, 88]. As a result, it can be said that there is usually a two-way relationship between sleep disorders and depression, also between sleep disorders and dementia.
Sleep is recognized as an essential modulator of several aspects of endocrine function, making it challenging to elucidate the relationship between these factors [76]. However, there is no evidence that treatment for sleep disorders prevents cognitive decline or dementia.
Vitamin D
Over the past 25 years, vitamin D has been recognized as a serious candidate for the nervous system’s development and functioning and a treatment option for several neurological pathologies [89].
Researchers have recently shown that vitamin D deficiency is common in PCOS and that vitamin D levels are associated with reproductive ability, metabolic changes, and mental health in PCOS patients [90]. In this regard, Krul-Poel et al. showed that women with PCOS and infertility have lower serum levels of 25 (OH) D than the fertile control group [91].
Vitamin D deficiency in PCOS may lead to IR [38], so vitamin D concentration is negatively correlated with IR parameters and body fat mass. Also, treatment with vitamin D improves the metabolism of IR and lipids, improving the metabolic disorders of PCOS patients [90].
Vitamin D increases the maturation of adipose cells, activates enzymes involved in lipid and carbohydrate metabolism, and increases adipose tissue [92].
Vitamin D levels are inversely related to serum androgen levels. Vitamin D administration lowers serum androgen and anti-Müllerian hormone (AMH) levels and reduces endometrial thickness; this reduction in androgen levels in PCOS patients improves the menstrual cycle folliculogenesis [90].
Studies show that vitamin D deficiency is associated with the onset of the first symptoms of AD and can contribute to the onset of dementia. However, interventional studies did not improve cognitive function after administering vitamin D supplementation [89]. Vitamin D plays an essential role in metabolic pathways, including calcium homeostasis, the insulin pathway, and the synthesis of sex hormones, all of which are affected by PCOS [93].
The main reason for taking vitamin D supplementation in PCOS women is its role in suppressing proinflammatory cytokines, glucose metabolism, increasing insulin receptor expression, plus synthesis and secretion of insulin [94]. Vitamin D deficiency is associated with many human diseases, especially age-related diseases, such as AD, cardiovascular disease, cancer, type II diabetes, multiple sclerosis, and various inflammatory disorders [95]. The progression of dementia and non-communicable diseases such as AD is a major public health problem. One of the direct causes of neuronal loss and decreased recognition of Aβ accumulation is associated with increased inflammatory responses in the brain [96]. Vitamin D deficiency is a growing problem and plays a significant role in the cytotoxicity of amyloid plaques, which affect a significant portion of the population in many countries [97]. Vitamin D is involved in genomic and non-genomic effects on calcium homeostasis, neurotransmission, oxidative stress, Aβ and Tau accumulation, vascularization, and inflammation; all of these pathways can be impaired in AD [98]. In addition to calcium homeostasis, vitamin D has numerous functions in the nervous system, including regulating the production of neurotrophic factors, neurotransmitter secretion, oxidative stress mechanisms, modulating the immune system, and is currently known as an effective immune modulator [89]. It also has the potential to regulate the inflammatory status in AD pathology [89].
Hyperandrogenism
Androgens belong to the family of steroid hormones and hyperandrogenism is one of the main clinical manifestations of PCOS [99]. Androgens include testosterone, androstenedione (A4), dihydrotestosterone (DHT), dehydroepiandrosterone (DHEA), and dehydroepiandrosterone sulfate (DHEAS) [100]. Serum levels of various androgens in PCOS patients are constantly increasing compared to healthy individuals [101]. Approximately 75% of PCOS patients having hyperandrogenism, and more than 80% having abnormally free testosterone levels [102]. This may be due to oxidative stress and hyperinsulinemia, which stimulate theca-interstitial cell proliferation and androgen production [103, 104]. Studies have shown that exposure of female fetuses to androgen overload in all models causes PCOS characteristics [105].
On the other hand, androgens may help reduce the process of AD, and decreased levels of gonadal hormones, especially estrogens and androgens, are commonly associated with the onset of AD [42]. Some studies have shown that androgens’ administration improves cognitive function [59]; androgen administration reduces the expression of inflammatory factor IL-1β, so reduces nerve death in the hippocampus [106].
Sex hormone-binding globulin (SHBG) is a sex steroid produced in the hepatic cells, and its low production may be involved in the pathogenesis of PCOS [107]. SHBG has a slight tendency to bind estradiol and a high affinity for testosterone [108]. The biological activity of androgens is also determined by free testosterone, and therefore investigation of SHBG levels is essential in assessing hyperandrogenism [107]; in PCOS patients, one of the reasons for low serum SHBG levels is hyperandrogenemia [109]. SHBG binds to free androgens and lowers free androgen levels, then reducing hyperandrogenism and IR [109]. SHBG levels increase in AD patients and lower serum levels of bioactive sex steroids [21].
Discussion
The HPG axis plays an important role in the pathophysiology of PCOS, which is one of the most common endocrine and metabolic disorders [110]. Hormones, especially gonadal hormones, widely affect the function and stability of the central nervous system [111]. Also, cognitive function may depend on the level of sex steroids and gonadotropins, including HPG-based dysfunction [21].
This study investigated some common factors such as IR, inflammation, sleep apnea, vitamin D deficiency, LH/FSH ratio, and sex hormones that may play a role in the association between AD and PCOS.
Four phenotypes have been defined for PCOS (According to Rotterdam criteria), including complete PCOS with hyperandrogenism, ovulation disorder, and polycystic ovaries; PCOS with hyperandrogenism and ovulation disorders; PCOS with hyperandrogenism and polycystic ovaries; PCOS associated with ovulatory and polycystic ovary disorders [112]. Studies have shown that the incidence of the disease among PCOS patients is significantly different based on ethnicity, phenotype, and morbidity. It seems that the component of hyperandrogenism is the most important determining factor in the pathophysiology of PCOS among other factors and also this factor is the main predictor of metabolic disorders observed in the disease [113]. It is important to note that the major determinants of the pathophysiology of PCOS may not necessarily be the determinants of the vulnerability of these patients to neurodegenerative Alzheimer’s disease. Evidence-based studies should be performed to determine which phenotype of PCOS leads to Alzheimer’s disease.
Obesity and IR, which are also seen in PCOS patients, may increase the risk of cognitive decline and neurodegenerative diseases [53]. On the other hand, due to the increased levels of androgens in PCOS patients, we expect cognitive activity to increase in these patients. However, oral contraceptive pills (OCPs) are drugs prescribed to women with PCOS as a first-line treatment to reduce androgen overexpression and regulate menstrual cycles [114]. Because OCPs reduce androgens, they can have adverse effects on memory and cognition. Also, drugs such as Metformin, which reverses IR, are associated with increased SHBG levels in women with PCOS [115]. As mentioned above, SHBG levels also increase in patients with AD. The use of these drugs may increase the symptoms of AD by increasing the level of SHBG. Contradictory results have been reported on the effects of metformin on central nervous system function and pathology. Some studies have shown increased neurogenesis, improved spatial learning, and decreased cognitive impairment, but others have shown negative consequences such as the increased risk of AD. Cognitive dysfunction has been shown to impair neuronal viability in the AD mouse model. There is also evidence that metformin reduces the activity of acetylcholinesterase (AChE), which is responsible for the breakdown of acetylcholine (Ach), a neurotransmitter involved in learning and memory. Therefore, the effect of metformin on Alzheimer’s disease is multifaceted [116, 117]. Although more research is needed, controlling SHBG levels may keep endogenous estrogens and androgens bioactive and improve cognition. Due to the variety of actions of estrogen, LH, and testosterone, combination hormone therapy may be more effective in preventing AD. Of course, the negative effects of hormone therapy in different reproductive periods of women before and after menopause should not be ignored [118].
Studies in this area are not adequate, so more animal research and studies in human research such as case–control studies may also help to give more insights into the potential association between PCOS and AD.
Conclusion
In general, the results of our study identified the following highlights:
-
Accumulation of amyloid-beta and tau proteins is a prominent feature of Alzheimer’s disease pathology. Increased levels of LH to FSH are involved in the metabolism and accumulation of Aβ and reduce BDNF in the brain.
-
Calcium signaling by vitamin D in neurons is crucial for neurotransmission and maintenance of synaptic plasticity and LTP.
-
Insulin signaling also affects hippocampal plasticity, learning, and memory.
-
Free fatty acids increase inflammation by causing Aβ deposition and resulting in nerve damage.
-
In patients with PCOS, increased LH to FSH ratio, decreased vitamin D, insulin resistance, and obesity are some of the most important factors that may increase the risk of Alzheimer’s disease.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
Abbreviations
- PCOS:
-
Polycystic ovary syndrome
- AD:
-
Alzheimer disease
- IR:
-
Insulin resistance
- HA:
-
Hyperandrogenism
- CNS:
-
The central nervous system
- Aβ:
-
Amyloid beta-peptide
- APP:
-
Amyloid precursor protein
- HPG:
-
Hypothalamic–pituitary–gonadal
- ERs:
-
Estrogen receptors
- BDNF:
-
Brain-derived neurotrophic factor
- GnRH:
-
Gonadotropin-releasing hormone
- IL-1β:
-
Interleukin-1 beta
- PTGS2:
-
Prostaglandin-endoperoxide synthase 2
- LIF:
-
Leukemia inhibitory factor
- TNFα:
-
Tumor necrosis factor-alpha
- OSA:
-
Obstructive sleep apnea
- AMH:
-
Anti-Müllerian hormone
- LH:
-
Luteinizing hormone
- FSH:
-
Follicle-stimulating hormone
- LHR:
-
Luteinizing hormone receptors
- DHT:
-
Dihydrotestosterone
- DHEAs:
-
Dehydroepiandrosterone sulfate
- OCPs:
-
Oral contraceptive pills
- SHBG:
-
Sex hormone-binding globulin
References
Spinedi E, Cardinali DP. The polycystic ovary syndrome and the metabolic syndrome: a possible chronobiotic-cytoprotective adjuvant therapy. Int J Endocrinol. 2018. https://doi.org/10.1155/2018/1349868.
González F. Inflammation in polycystic ovary syndrome: underpinning of insulin resistance and ovarian dysfunction. Steroids. 2012;77(4):300–5.
Wang J, Wu D, Guo H, Li M. Hyperandrogenemia and insulin resistance: The chief culprit of polycystic ovary syndrome. Life Sci. 2019;236:116940.
He FF, Li YM. Role of gut microbiota in the development of insulin resistance and the mechanism underlying polycystic ovary syndrome: a review. J Ovarian Res. 2020;13(1):73.
Sabayan B, Foroughinia F, Borhani Haghighi A, Mowla A. Are women with polycystic ovary syndrome (PCOS) at higher risk for development of Alzheimer disease? Alzheimer Dis Assoc Disord. 2007;21(3):265.
Barber TM, Kyrou I, Randeva HS, Weickert MO. Mechanisms of insulin resistance at the crossroad of obesity with associated metabolic abnormalities and cognitive dysfunction. Int J Mol Sci. 2021;22(2):546.
Tang M, Taghibiglou C. The mechanisms of action of curcumin in Alzheimer’s disease. J Alzheimers Dis. 2017;58(4):1003–16.
Wimo A, Guerchet M, Ali GC, Wu YT, Prina AM, Winblad B, et al. The worldwide costs of dementia 2015 and comparisons with 2010. Alzheimers Dement. 2017;13(1):1–7.
Burns A, Iliffe S. Alzheimer’s disease. BMJ. 2009;338:b158.
Caselli RJ, Beach TG, Knopman DS, Graff-Radford NR, editors. Alzheimer disease: scientific breakthroughs and translational challenges. In: Mayo Clinic Proceedings; Elsevier. 2017.
Li R, Cui J, Shen Y. Brain sex matters: estrogen in cognition and Alzheimer’s disease. Mol Cell Endocrinol. 2014;389(1–2):13–21.
Akwa Y. Steroids and Alzheimer’s disease: changes associated with pathology and therapeutic potential. Int J Mol Sci. 2020;21(13):4812.
Du AT, Schuff N, Kramer JH, Rosen HJ, Gorno-Tempini ML, Rankin K, et al. Different regional patterns of cortical thinning in Alzheimer’s disease and frontotemporal dementia. Brain. 2007;130(Pt 4):1159–66.
Nunomura A, Perry G. RNA and oxidative stress in Alzheimer’s disease: focus on microRNAs. Oxid Med Cell Longev. 2020;2020:2638130.
Irwin MR, Vitiello MV. Implications of sleep disturbance and inflammation for Alzheimer’s disease dementia. Lancet Neurol. 2019;18(3):296–306.
Silva MVF, Loures CdMG, Alves LCV, de Souza LC, Borges KBG, das Graças Carvalho M. Alzheimer’s disease: risk factors and potentially protective measures. J Biomed Sci. 2019;26(1):1–11.
Arao Y, Hamilton KJ, Wu S-P, Tsai M-J, DeMayo FJ, Korach KS. Dysregulation of hypothalamic-pituitary estrogen receptor α-mediated signaling causes episodic LH secretion and cystic ovary. FASEB J. 2019;33(6):7375–86.
Wang F, Zhang ZH, Xiao KZ, Wang ZC. Roles of hypothalamic-pituitary-adrenal axis and hypothalamus-pituitary-ovary axis in the abnormal endocrine functions in patients with polycystic ovary syndrome. Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 2017;39(5):699–704.
Atwood CS, Bowen RL. The reproductive-cell cycle theory of aging: an update. Exp Gerontol. 2011;46(2–3):100–7.
Ahmad MH, Fatima M, Mondal AC. Role of hypothalamic-pituitary-adrenal axis, hypothalamic-pituitary-gonadal axis and insulin signaling in the pathophysiology of Alzheimer’s disease. Neuropsychobiology. 2019;77(4):197–205.
Blair JA, McGee H, Bhatta S, Palm R, Casadesus G. Hypothalamic-pituitary-gonadal axis involvement in learning and memory and Alzheimer’s disease: more than “just” estrogen. Front Endocrinol (Lausanne). 2015;6:45.
Zhang G, Li J, Purkayastha S, Tang Y, Zhang H, Yin Y, et al. Hypothalamic programming of systemic ageing involving IKK-β, NF-κB and GnRH. Nature. 2013;497(7448):211–6.
Simpkins JW, Perez E, Wang X, Yang S, Wen Y, Singh M. The potential for estrogens in preventing Alzheimer’s disease and vascular dementia. Ther Adv Neurol Disord. 2009;2(1):31–49.
Henderson VW. Alzheimer’s disease: review of hormone therapy trials and implications for treatment and prevention after menopause. J Steroid Biochem Mol Biol. 2014;142:99–106.
Bhatta S, Blair JA, Casadesus G. Luteinizing hormone involvement in aging female cognition: not all is estrogen loss. Front Endocrinol (Lausanne). 2018;9:544.
Brinton RD, Yao J, Yin F, Mack WJ, Cadenas E. Perimenopause as a neurological transition state. Nat Rev Endocrinol. 2015;11(7):393–405.
McEwen BS, Akama KT, Spencer-Segal JL, Milner TA, Waters EM. Estrogen effects on the brain: actions beyond the hypothalamus via novel mechanisms. Behav Neurosci. 2012;126(1):4–16.
Long J, He P, Shen Y, Li R. New evidence of mitochondria dysfunction in the female Alzheimer’s disease brain: deficiency of estrogen receptor-β. J Alzheimers Dis. 2012;30(3):545–58.
Lan YL, Zhao J, Li S. Update on the neuroprotective effect of estrogen receptor alpha against Alzheimer’s disease. J Alzheimers Dis. 2015;43(4):1137–48.
Wharton W, Baker LD, Gleason CE, Dowling M, Barnet JH, Johnson S, et al. Short-term hormone therapy with transdermal estradiol improves cognition for postmenopausal women with Alzheimer’s disease: results of a randomized controlled trial. J Alzheimers Dis. 2011;26(3):495–505.
Galea LA, Wainwright SR, Roes MM, Duarte-Guterman P, Chow C, Hamson DK. Sex, hormones and neurogenesis in the hippocampus: hormonal modulation of neurogenesis and potential functional implications. J Neuroendocrinol. 2013;25(11):1039–61.
Malini NA, Roy GK. Evaluation of different ranges of LH:FSH ratios in polycystic ovarian syndrome (PCOS)—Clinical based case control study. Gen Comp Endocrinol. 2018;260:51–7.
Bothou A, Koutlaki N, Iatrakis G, Mastorakos G, Tsikouras P, Liberis V, et al. ANTIMÜLLERIAN HORMONE AS INDICATOR OF OVARIAN DYSFUNCTION. Acta Endocrinol (Buchar). 2017;13(2):237–45.
Balen A. The pathophysiology of polycystic ovary syndrome: trying to understand PCOS and its endocrinology. Best Pract Res Clin Obstet Gynaecol. 2004;18(5):685–706.
Braunstein GD, Vaitukaitis JL, Carbone PP, Ross GT. Ectopic production of human chorionic gonadotrophin by neoplasms. Ann Intern Med. 1973;78(1):39–45.
Laganà AS, Rossetti P, Buscema M, La Vignera S, Condorelli RA, Gullo G, et al. Metabolism and ovarian function in PCOS women: a therapeutic approach with inositols. Int J Endocrinol. 2016;2016:6306410.
Kazmi SRH, Can AS. Luteinizing hormone deficiency. In: StatPearls. Treasure Island: StatPearls Publishing LLC.; 2020.
Nna VU, Bakar ABA, Ahmad A, Mohamed M. Down-regulation of steroidogenesis-related genes and its accompanying fertility decline in streptozotocin-induced diabetic male rats: ameliorative effect of metformin. Andrology. 2019;7(1):110–23.
Keskin FE, Özkaya HM, Ortaç M, Salabaş E, Kadıoğlu A, Kadıoğlu P. Sexual function in women with Cushing’s syndrome: a controlled study. Turk J Urol. 2018;44(4):287–93.
Khattak M, Sultana N, Usman R, Khattak U, Zafar U, Salman H. Luteinizing hormone to follicle stimulating hormone ratio in patients with polycystic ovary syndrome. J Ayub Med Coll Abbottabad. 2020;32(2):255–8.
Kaur R, Kaur T, Kaur A. Genetic association study from North India to analyze association of CYP19A1 and CYP17A1 with polycystic ovary syndrome. J Assist Reprod Genet. 2018;35(6):1123–9.
Burnham VL, Thornton JE. Luteinizing hormone as a key player in the cognitive decline of Alzheimer’s disease. Horm Behav. 2015;76:48–56.
Verdile G, Laws SM, Henley D, Ames D, Bush AI, Ellis KA, et al. Associations between gonadotropins, testosterone and β amyloid in men at risk of Alzheimer’s disease. Mol Psychiatry. 2014;19(1):69–75.
Bohm-Levine N, Goldberg AR, Mariani M, Frankfurt M, Thornton J. Reducing luteinizing hormone levels after ovariectomy improves spatial memory: possible role of brain-derived neurotrophic factor. Horm Behav. 2020;118:104590.
Rodrigues MA, Verdile G, Foster JK, Hogervorst E, Joesbury K, Dhaliwal S, et al. Gonadotropins and cognition in older women. J Alzheimers Dis. 2008;13(3):267–74.
Lebovitz HE. Insulin resistance—a common link between type 2 diabetes and cardiovascular disease. Diabetes Obes Metab. 2006;8(3):237–49.
Legro RS, Castracane VD, Kauffman RP. Detecting insulin resistance in polycystic ovary syndrome: purposes and pitfalls. Obstet Gynecol Surv. 2004;59(2):141–54.
Mastorakos G, Lambrinoudaki I, Creatsas G. Polycystic ovary syndrome in adolescents: current and future treatment options. Paediatr Drugs. 2006;8(5):311–8.
Prudente S, Trischitta V. The TRIB3 Q84R polymorphism, insulin resistance and related metabolic alterations. Biochem Soc Trans. 2015;43(5):1108–11.
Zhang Y, Hu M, Jia W, Liu G, Zhang J, Wang B, et al. Hyperandrogenism and insulin resistance modulate gravid uterine and placental ferroptosis in PCOS-like rats. J Endocrinol. 2020;246(3):247–63.
Sousa-Nunes R, Yee LL, Gould AP. Fat cells reactivate quiescent neuroblasts via TOR and glial insulin relays in Drosophila. Nature. 2011;471(7339):508–12.
Gómez JM. Growth hormone and insulin-like growth factor-I as an endocrine axis in Alzheimer’s disease. Endocr Metab Immune Disord Drug Targets. 2008;8(2):143–51.
Fusco S, Spinelli M, Cocco S, Ripoli C, Mastrodonato A, Natale F, et al. Maternal insulin resistance multigenerationally impairs synaptic plasticity and memory via gametic mechanisms. Nat Commun. 2019;10(1):4799.
Spinelli M, Fusco S, Grassi C. Brain insulin resistance and hippocampal plasticity: mechanisms and biomarkers of cognitive decline. Front Neurosci. 2019;13:788.
Plum L, Belgardt BF, Brüning JC. Central insulin action in energy and glucose homeostasis. J Clin Invest. 2006;116(7):1761–6.
de la Monte SM, Tong M, Bowling N, Moskal P. si-RNA inhibition of brain insulin or insulin-like growth factor receptors causes developmental cerebellar abnormalities: relevance to fetal alcohol spectrum disorder. Mol Brain. 2011;4:13.
de la Monte SM. Insulin resistance and neurodegeneration: progress towards the development of new therapeutics for alzheimer’s disease. Drugs. 2017;77(1):47–65.
Kałużna M, Człapka-Matyasik M, Wachowiak-Ochmańska K, Moczko J, Kaczmarek J, Janicki A, et al. Effect of central obesity and hyperandrogenism on selected inflammatory markers in patients with PCOS: a WHtR-matched case-control study. J Clin Med. 2020;9(9):3024.
Zhang J, Bao Y, Zhou X, Zheng L. Polycystic ovary syndrome and mitochondrial dysfunction. Reprod Biol Endocrinol. 2019;17(1):67.
Schmidt J, Weijdegård B, Mikkelsen AL, Lindenberg S, Nilsson L, Brännström M. Differential expression of inflammation-related genes in the ovarian stroma and granulosa cells of PCOS women. Mol Hum Reprod. 2014;20(1):49–58.
Webers A, Heneka MT, Gleeson PA. The role of innate immune responses and neuroinflammation in amyloid accumulation and progression of Alzheimer’s disease. Immunol Cell Biol. 2020;98(1):28–41.
Axen KV, Dikeakos A, Sclafani A. High dietary fat promotes syndrome X in nonobese rats. J Nutr. 2003;133(7):2244–9.
O’Brien PD, Hinder LM, Callaghan BC, Feldman EL. Neurological consequences of obesity. Lancet Neurol. 2017;16(6):465–77.
López S, Bermúdez B, Pacheco YM, Villar J, Abia R, Muriana FJ. Distinctive postprandial modulation of beta cell function and insulin sensitivity by dietary fats: monounsaturated compared with saturated fatty acids. Am J Clin Nutr. 2008;88(3):638–44.
Cholerton B, Baker LD, Craft S. Insulin, cognition, and dementia. Eur J Pharmacol. 2013;719(1–3):170–9.
Dandrea MR, Reiser PA, Gumula NA, Hertzog BM, Andrade-Gordon P. Application of triple immunohistochemistry to characterize amyloid plaque-associated inflammation in brains with Alzheimer’s disease. Biotech Histochem. 2001;76(2):97–106.
Giovannini MG, Scali C, Prosperi C, Bellucci A, Vannucchi MG, Rosi S, et al. Beta-amyloid-induced inflammation and cholinergic hypofunction in the rat brain in vivo: involvement of the p38MAPK pathway. Neurobiol Dis. 2002;11(2):257–74.
Standridge JB. Pharmacotherapeutic approaches to the prevention of Alzheimer’s disease. Am J Geriatr Pharmacother. 2004;2(2):119–32.
Wood H. Dementia: peripheral inflammation could be a prodromal indicator of dementia. Nat Rev Neurol. 2018;14(3):127.
Spira AP, Chen-Edinboro LP, Wu MN, Yaffe K. Impact of sleep on the risk of cognitive decline and dementia. Curr Opin Psychiatry. 2014;27(6):478–83.
Hachul H, Polesel DN, Tock L, Carneiro G, Pereira AZ, Zanella MT, et al. Sleep disorders in polycystic ovary syndrome: influence of obesity and hyperandrogenism. Rev Assoc Med Bras (1992). 2019;65(3):375–83.
Kumarendran B, Sumilo D, O’Reilly MW, Toulis KA, Gokhale KM, Wijeyaratne CN, et al. Increased risk of obstructive sleep apnoea in women with polycystic ovary syndrome: a population-based cohort study. Eur J Endocrinol. 2019;180(4):265–72.
Fogel RB, Malhotra A, Pillar G, Pittman SD, Dunaif A, White DP. Increased prevalence of obstructive sleep apnea syndrome in obese women with polycystic ovary syndrome. J Clin Endocrinol Metab. 2001;86(3):1175–80.
Andersen ML, Alvarenga TF, Mazaro-Costa R, Hachul HC, Tufik S. The association of testosterone, sleep, and sexual function in men and women. Brain Res. 2011;1416:80–104.
Behan M, Wenninger JM. Sex steroidal hormones and respiratory control. Respir Physiol Neurobiol. 2008;164(1–2):213–21.
Leproult R, Van Cauter E. Role of sleep and sleep loss in hormonal release and metabolism. Endocr Dev. 2010;17:11–21.
Tock L, Carneiro G, Togeiro SM, Hachul H, Pereira AZ, Tufik S, et al. Obstructive sleep apnea predisposes to nonalcoholic fatty liver disease in patients with polycystic ovary syndrome. Endocr Pract. 2014;20(3):244–51.
Tasali E, Van Cauter E, Ehrmann DA. Polycystic ovary syndrome and obstructive sleep apnea. Sleep Med Clin. 2008;3(1):37–46.
Mokhlesi B, Scoccia B, Mazzone T, Sam S. Risk of obstructive sleep apnea in obese and nonobese women with polycystic ovary syndrome and healthy reproductively normal women. Fertil Steril. 2012;97(3):786–91.
Spinedi E, Cardinali DP. The polycystic ovary syndrome and the metabolic syndrome: a possible chronobiotic-cytoprotective adjuvant therapy. Int J Endocrinol. 2018;2018:1349868.
Sam S, Ehrmann DA. Pathogenesis and consequences of disordered sleep in PCOS. Clin Med Insights Reprod Health. 2019;13:1179558119871269.
Marcouiller F, Boukari R, Laouafa S, Lavoie R, Joseph V. The nuclear progesterone receptor reduces post-sigh apneas during sleep and increases the ventilatory response to hypercapnia in adult female mice. PLoS ONE. 2014;9(6):e100421.
Shi L, Chen SJ, Ma MY, Bao YP, Han Y, Wang YM, et al. Sleep disturbances increase the risk of dementia: a systematic review and meta-analysis. Sleep Med Rev. 2018;40:4–16.
Kang JE, Lim MM, Bateman RJ, Lee JJ, Smyth LP, Cirrito JR, et al. Amyloid-beta dynamics are regulated by orexin and the sleep-wake cycle. Science. 2009;326(5955):1005–7.
Xie L, Kang H, Xu Q, Chen MJ, Liao Y, Thiyagarajan M, et al. Sleep drives metabolite clearance from the adult brain. Science. 2013;342(6156):373–7.
Aalling NN, Nedergaard M, DiNuzzo M. Cerebral metabolic changes during sleep. Curr Neurol Neurosci Rep. 2018;18(9):57.
Bao YP, Han Y, Ma J, Wang RJ, Shi L, Wang TY, et al. Cooccurrence and bidirectional prediction of sleep disturbances and depression in older adults: meta-analysis and systematic review. Neurosci Biobehav Rev. 2017;75:257–73.
Mourao RJ, Mansur G, Malloy-Diniz LF, Castro Costa E, Diniz BS. Depressive symptoms increase the risk of progression to dementia in subjects with mild cognitive impairment: systematic review and meta-analysis. Int J Geriatr Psychiatry. 2016;31(8):905–11.
Landel V, Annweiler C, Millet P, Morello M, Féron F, Vitamin D. Cognition and Alzheimer’s disease: the therapeutic benefit is in the D-tails. J Alzheimers Dis. 2016;53(2):419–44.
Mu Y, Cheng D, Yin TL, Yang J. Vitamin D and polycystic ovary syndrome: a narrative review. Reprod Sci. 2020. https://doi.org/10.1007/s43032-020-00369-2.
Krul-Poel YHM, Koenders PP, Steegers-Theunissen RP, Ten Boekel E, Wee MMT, Louwers Y, et al. Vitamin D and metabolic disturbances in polycystic ovary syndrome (PCOS): a cross-sectional study. PLoS ONE. 2018;13(12):e0204748.
Wikiera B, Zubkiewicz-Kucharska A, Nocoń-Bohusz J, Noczyńska A. Metabolic disorders in polycystic ovary syndrome. Pediatr Endocrinol Diabetes Metab. 2017;23(4):204–8.
Karadağ C, Yoldemir T, Yavuz DG. Effects of vitamin D supplementation on insulin sensitivity and androgen levels in vitamin-D-deficient polycystic ovary syndrome patients. J Obstet Gynaecol Res. 2018;44(2):270–7.
Angellotti E, D’Alessio D, Dawson-Hughes B, Nelson J, Cohen RM, Gastaldelli A, et al. Vitamin D supplementation in patients with type 2 diabetes: the vitamin D for established type 2 diabetes (DDM2) study. J Endocr Soc. 2018;2(4):310–21.
Pines A. Vitamin D and health issues-questioned benefits. Climacteric. 2014;17(6):657–9.
Zhang F, Jiang L. Neuroinflammation in Alzheimer’s disease. Neuropsychiatr Dis Treat. 2015;11:243–56.
Littlejohns TJ, Henley WE, Lang IA, Annweiler C, Beauchet O, Chaves PH, et al. Vitamin D and the risk of dementia and Alzheimer disease. Neurology. 2014;83(10):920–8.
Landel V, Annweiler C, Millet P, Morello M, Féron F, Vitamin D. Cognition and Alzheimer’s disease: the therapeutic benefit is in the D-tails. J Alzheimer’s Dis JAD. 2016;53(2):419–44.
Lim JJ, Lima PDA, Salehi R, Lee DR, Tsang BK. Regulation of androgen receptor signaling by ubiquitination during folliculogenesis and its possible dysregulation in polycystic ovarian syndrome. Sci Rep. 2017;7(1):10272.
Zeng X, Xie YJ, Liu YT, Long SL, Mo ZC. Polycystic ovarian syndrome: correlation between hyperandrogenism, insulin resistance and obesity. Clin Chim Acta. 2020;502:214–21.
Palomba S, Falbo A, Chiossi G, Muscogiuri G, Fornaciari E, Orio F, et al. Lipid profile in nonobese pregnant women with polycystic ovary syndrome: a prospective controlled clinical study. Steroids. 2014;88:36–43.
Huang A, Brennan K, Azziz R. Prevalence of hyperandrogenemia in the polycystic ovary syndrome diagnosed by the National Institutes of Health 1990 criteria. Fertil Steril. 2010;93(6):1938–41.
Moran L, Teede H. Metabolic features of the reproductive phenotypes of polycystic ovary syndrome. Hum Reprod Update. 2009;15(4):477–88.
Kodaman PH, Duleba AJ. HMG-CoA reductase inhibitors: do they have potential in the treatment of polycystic ovary syndrome? Drugs. 2008;68(13):1771–85.
Walters KA. Androgens in polycystic ovary syndrome: lessons from experimental models. Curr Opin Endocrinol Diabetes Obes. 2016;23(3):257–63.
Yao PL, Zhuo S, Mei H, Chen XF, Li N, Zhu TF, et al. Androgen alleviates neurotoxicity of β-amyloid peptide (Aβ) by promoting microglial clearance of Aβ and inhibiting microglial inflammatory response to Aβ. CNS Neurosci Ther. 2017;23(11):855–65.
Qu X, Donnelly R. Sex hormone-binding globulin (SHBG) as an early biomarker and therapeutic target in polycystic ovary syndrome. Int J Mol Sci. 2020;21(21):8191.
Dunn JF, Nisula BC, Rodbard D. Transport of steroid hormones: binding of 21 endogenous steroids to both testosterone-binding globulin and corticosteroid-binding globulin in human plasma. J Clin Endocrinol Metab. 1981;53(1):58–68.
Zhu JL, Chen Z, Feng WJ, Long SL, Mo ZC. Sex hormone-binding globulin and polycystic ovary syndrome. Clin Chim Acta. 2019;499:142–8.
Valkenburg O, Uitterlinden AG, Piersma D, Hofman A, Themmen AP, de Jong FH, et al. Genetic polymorphisms of GnRH and gonadotrophic hormone receptors affect the phenotype of polycystic ovary syndrome. Hum Reprod. 2009;24(8):2014–22.
Marshall KM. Introduction to the interaction between gonadal steroids and the central nervous system. Curr Top Behav Neurosci. 2011;8:1–13.
Lizneva D, Suturina L, Walker W, Brakta S, Gavrilova-Jordan L, Azziz R. Criteria, prevalence, and phenotypes of polycystic ovary syndrome. Fertil Steril. 2016;106(1):6–15.
Engmann L, Jin S, Sun F, Legro RS, Polotsky AJ, Hansen KR, et al. Racial and ethnic differences in the polycystic ovary syndrome metabolic phenotype. Am J Obstet Gynecol. 2017;216(5):493.e1–e13.
Costello MF, Misso ML, Balen A, Boyle J, Devoto L, Garad RM, et al. Evidence summaries and recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome: assessment and treatment of infertility. Hum Reprod Open. 2019;2019(1):hoy021.
Pasquali R, Gambineri A, Biscotti D, Vicennati V, Gagliardi L, Colitta D, et al. Effect of long-term treatment with metformin added to hypocaloric diet on body composition, fat distribution, and androgen and insulin levels in abdominally obese women with and without the polycystic ovary syndrome. J Clin Endocrinol Metab. 2000;85(8):2767–74.
Markowicz-Piasecka M, Sikora J, Szydłowska A, Skupień A, Mikiciuk-Olasik E, Huttunen KM. Metformin—a future therapy for neurodegenerative diseases. Pharm Res. 2017;34(12):2614–27.
Thangthaeng N, Rutledge M, Wong JM, Vann PH, Forster MJ, Sumien N. Metformin impairs spatial memory and visual acuity in old male mice. Aging Dis. 2017;8(1):17.
Hill DA, Crider M, Hill SR. Hormone therapy and other treatments for symptoms of menopause. Am Fam Physician. 2016;94(11):884–9.
Acknowledgements
Not applicable.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author information
Authors and Affiliations
Contributions
NS: Concepts, design, definition of intellectual content, research studies, manuscript preparation, manuscript editing, manuscript review, data acquisition; HS: Concepts, design, definition of intellectual content, research studies, manuscript preparation, manuscript editing, manuscript review, data acquisition; NER: Literature search, manuscript preparation, manuscript editing, manuscript review; ES: Literature search, data acquisition, manuscript preparation, manuscript review, NR Manuscript editing, manuscript review, data acquisition, manuscript review. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethical considerations
Unethical issues (including plagiarism, informed consent, misconduct, data fabrication, and/or forgery, duplication and/or submission, redundancy, etc.) have been investigated by the authors.
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Sarahian, N., Sarvazad, H., Sajadi, E. et al. Investigation of common risk factors between polycystic ovary syndrome and Alzheimer’s disease: a narrative review. Reprod Health 18, 156 (2021). https://doi.org/10.1186/s12978-021-01203-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12978-021-01203-x