
Abstract
Background
SARS-CoV-2, the pathogen of COVID-19, is a worldwide threat to human health and causes a long-term burden on the cardiovascular system. Individuals with pre-existing cardiovascular diseases are at higher risk for SARS-CoV-2 infection and tend to have a worse prognosis. However, the relevance and pathogenic mechanisms between COVID-19 and cardiovascular diseases are not yet completely comprehended.
Methods
Common differentially expressed genes (DEGs) were obtained in datasets of human induced pluripotent stem cell-derived cardiomyocytes (hiPSC-CMs) infected with SARS-CoV-2 and myocardial tissues from heart failure patients. Further GO and KEGG pathway analysis, protein–protein interaction (PPI) network construction, hub genes identification, immune microenvironment analysis, and drug candidate predication were performed. Then, an isoproterenol-stimulated myocardial hypertrophy cell model and a transverse aortic constriction-induced mouse heart failure model were employed to validate the expression of hub genes.
Results
A total of 315 up-regulated and 78 down-regulated common DEGs were identified. Functional enrichment analysis revealed mitochondrial metabolic disorders and extensive immune inflammation as the most prominent shared features of COVID-19 and cardiovascular diseases. Then, hub DEGs, as well as hub immune-related and mitochondria-related DEGs, were screened. Additionally, nine potential therapeutic agents for COVID-19-related cardiovascular diseases were proposed. Furthermore, the expression patterns of most of the hub genes related to cardiovascular diseases in the validation dataset along with cellular and mouse myocardial damage models, were consistent with the findings of bioinformatics analysis.
Conclusions
The study unveiled the molecular networks and signaling pathways connecting COVID-19 and cardiovascular diseases, which may provide novel targets for intervention of COVID-19-related cardiovascular diseases.
Similar content being viewed by others


Background
The coronavirus disease 2019 (COVID-19), caused by the severe acute respiratory syndrome-coronavirus 2 (SARS-CoV-2) infection, has resulted in a global pandemic. In hospitalized COVID-19 patients, acute clinical cardiovascular manifestations are prevalent, including myocarditis, arrhythmias, myocardial ischemia, cardiogenic shock, and acute heart failure [1]. Furthermore, at least 10% of COVID-19 survivors develop persistent symptoms for more than three months following their initial infection, a condition recognized as “long COVID”. Cardiovascular indications, such as hypotonia, palpitations, tachycardia, and chest pain, are the most commonly documented [2, 3]. Additionally, up to one-third of COVID-19 inpatients present with a history of cardiovascular diseases [1]. Coexisting cardiac diseases are usually related to increased rates of infection, thromboembolism, and mortality [1, 4]. Even after the acute infection phase, individuals with a history of heart failure are at 2–4 times greater risk of heart failure exacerbation and death [4,5,6,7]. Due to their considerable power in exacerbating the severity of COVID-19-related diseases, both the acute and long-term impact of COVID-19 on cardiovascular system remain a major concern.
During the acute phase of COVID-19, both direct and indirect mechanisms have been proposed to contribute to cardiovascular injury. SARS-CoV-2 infection is initiated by binding of the receptor binding domain (RBD) of Spike surface protein to the angiotensin-converting enzyme 2 (ACE2) receptor, which is a crucial component of the renin–angiotensin–aldosterone system (RAAS) involved in regulating blood pressure and electrolyte balance [8,9,10]. ACE2 is highly expressed in alveolar epithelial cells and small intestinal epithelial cells, which aligns with the potential transmission pathway of SARS-CoV-2 [11]. ACE2 is also widely present in vascular endothelial cells and smooth muscle cells of various organs, including the heart, creating conditions for SARS-CoV-2 to directly infect cardiac tissues and cause acute myocardial injury and myocarditis [11]. Analysis of autopsy cases demonstrated the presence of SARS-CoV-2 in the myocardial tissues of COVID-19 patients, and in vitro cellular infection experiments confirmed the susceptibility of cardiomyocytes to SARS-CoV-2 [12,13,14]. Patients with different cardiac etiologies have been found to exhibit an increased expression of ACE2 in cardiac tissues, which may enhance the risk of SARS-CoV-2 infection [15, 16]. After receptor binding, the Spike protein must be cleaved by the host transmembrane protease serine 2 (TMPRSS2) to initiate membrane fusion [17]. A variety of cell-surface molecules and cellular proteases may also be involved in SARS-CoV-2 invasion [17,18,19,20]. The basal expression levels of these viral entry-associated receptors or co-factors may be a crucial determinant of SARS-CoV-2 cellular tropism; however, the correlation between their expression levels in cardiovascular disease patients and susceptibility to COVID-19 is largely unknown.
Indirect injury is mainly mediated by systemic inflammation, hypoxic injury, RAAS dysregulation, and a mismatch between myocardial supply and demand [21, 22]. While the mechanism of sustained cardiac injury after acute illness remains poorly understood. It has been postulated that the mechanisms involved in long COVID may be the consequences of physical harm to the cardiovascular system and modified physiological conditions that occurs during the acute phase of COVID-19, encompassing dysregulation of the immune system, persistent damage following inflammation, complications following critical illness, and continuous underlying viral infection [23, 24]. In addition, individuals with SARS-CoV-2 infection usually present with a multi-organ disease syndrome. The interactions between heart and other organs, such as heart-brain axis (HBA) dysfunction, may exacerbate the prognosis of patients with COVID-19 [25]. SARS-CoV-2 interferes with HBA, thereby compromising overall HBA homeostasis and leading to multiorgan complications, including arrhythmias, acute myocardial infarction, and stress cardiomyopathy [25]. It is also worth noting that the emergence of new variants of SARS-CoV-2, particularly mutations in the Spike protein, and the development of vaccines have caused changes in virulence and transmissibility of the virus [26, 27]. For example, compared with earlier Delta variant, the Omicron BA.1 subvariant was strongly attenuated in human cardiomyocyte, whereas the BA.5 subvariant showed increased replication ability [14]. Therefore, the severity of cardiac injury caused by different SARS-CoV-2 variants may vary. Although possible mechanisms for SARS-CoV-2-induced cardiac involvement have been proposed, the underlying molecular mechanisms between COVID-19 and cardiovascular diseases are not yet fully understood. A more comprehensive understanding of the interplay and molecular crosstalk between these two conditions will assist in formulating novel intervention strategies during the COVID-19 pandemic.
Integration and analysis of data through bioinformatics tools allows for more accurate prediction of the molecular pathogenesis of diseases and accelerates precision medicine. To uncover the pathogenesis of COVID-19-related cardiovascular disorders, the common differentially expressed genes of the two diseases were obtained from public databases. Based on this, the shared profiles of genes, molecular networks, and signaling pathways of COVID-19 and cardiovascular diseases were revealed, and potential therapeutic agents were predicted.
Methods
Data collection and processing
The second-generation high-throughput sequencing data and microarray data for illnesses were obtained from the National Center for Biotechnology Information (NCBI) Gene Expression Omnibus (GEO) datasets (http://www.ncbi.nlm.nih.gov/geo/). The GSE156754 dataset investigates the susceptibility and response of human induced pluripotent stem cell-derived cardiomyocytes (hiPSC-CMs) to SARS-CoV-2 infection, containing an infection group and a mock group, each with 3 samples [28]. The dataset GSE84796 investigates gene expression in heart failure, containing transcriptome profiles of human left ventricular free wall samples obtained from 10 end-stage heart failure patients and 7 organ donors (characteristics of clinical information of this heart failure dataset can be found in Additional file 1: Table S1) [29]. The GSE57338 dataset, containing microarray data of left ventricle samples from 177 patients with failing hearts and 136 healthy controls, was selected as a validation set for verification of the hub DEGs [30]. Datasets were accessed from GEO using the R package “GEO query” [31]. Differentially expressed genes (DEGs) from each dataset were obtained with the R package “limma”, and P-value < 0.05 and log2|fold change (FC)|> 1 were set as the criteria for identifying DEGs. Namely, genes meeting the criteria, P-value < 0.05 and FC > 2 in comparison with control, were characterized as up-regulated DEGs, whereas genes with P-value < 0.05 and FC < -2 compared with the control were considered to be down-regulated DEGs. Resulting DEGs were visualized by volcano plot using the online website (https://www.xiantaozi.com/). The common DEGs between the GSE156754 and GSE84796 datasets were obtained and visualized with the R packages “VennDiagram” and “ggplot2”.
GO and KEGG enrichment analysis
To explore the shared pathogenesis between COVID-19 and cardiovascular diseases, Gene Ontology (GO) analysis, including biological process, molecular function, and cellular component, as well as Kyoto Encyclopedia of Genes and Genomes (KEGG) pathway enrichment analysis, were performed through the web-based platform DAVID (https://david.ncifcrf.gov/home.jsp) with homo sapiens genes as a background. The P-values obtained from DAVID’s analyses were adjusted for multiple testing using Benjamini’s correction, and a threshold value of 0.05 was applied. Redundant GO terms were then eliminated by REVIGO (http://revigo.irb.hr/) based on semantic similarity. The threshold for allowed similarity in REVIGO was set to “Medium (0.7)”, and the semantic similarity measure “SimRel” was chosen. The results of GO and KEGG enrichment analyses were visualized using web service Hiplot Pro (https://hiplot.com.cn/), a comprehensive web service for biomedical data analysis and visualization.
Network analysis and hub genes identification
The common DEGs were used to construct the protein‒protein interaction (PPI) network using the STRING database (https://string-db.org/), with a minimum required interaction score set to medium confidence (0.4) [32], and the results were visualized using Cytoscape (v3.8.2). Hub genes and vital networks were identified using the plugins CytoHubba and MCODE in Cytoscape. Furthermore, the GeneMANIA database (https://genemania.org/) was utilized to analyze gene network of the hub genes [33].
Identification of immune-related DEGs (ImmuneDEGs)
Immune-related genes were obtained from the ImmPort database (https://www.immport.org). ImmuneDEGs were selected and visualized by taking the intersection of the common DEGs and the immune-related genes using the R packages “VennDiagram” and “ggplot2”.
Identification of mitochondria-related DEGs (MitoDEGs)
Mitochondrial genes were obtained from the mitochondrial protein database MitoCarta 3.0 (https://www.broadinstitute.org/mitocarta/mitocarta30-inventory-Mammalian-mitochondrial-proteins-and-pathways) [34]. MitoDEGs, which refer to nuclear genes coding proteins with mitochondrial location in this study, were obtained and visualized by taking the intersection of the common DEGs and the mitochondrial genes using the R packages “VennDiagram” and “ggplot2”.
Immune infiltration analysis
The web-based platform CIBERSORTx (https://cibersortx.stanford.edu/) was used to estimate the expression of 22 immune cells in each sample in the heart failure cohort. Subsequently, spearman correlation analysis was performed to assess the interrelationship among the immune cells.
Obtainment of potential key genes for cardiovascular diseases
The Comparative Toxicogenomics Database (CTD, http://ctdbase.org/) provides data on interfaces between chemicals, genetic products, biological outcomes, and diseases and contributes to the study of potential mechanisms of pharmaceutical action and disease-related environmental exposures [35]. Using the CTD database, the associations between hub genes and the risk of the onset of cardiovascular diseases, heart diseases, and vascular diseases were analyzed.
Identification of drug candidates
The Connectivity Map (CMap, https://clue.io/), which reveals connections among pharmaceuticals, genes, and diseases [36], was utilized to screen for drug candidates. To identify potential therapeutic agents, hub DEGs were uploaded to the CMap database. According to the score, the top 3 candidate drugs (containing some drugs with the same rating) were selected as candidate drugs for the treatment of cardiac injury associated with SARS-CoV-2 infection.
Cell culture and drug treatment
The H9c2 cells, derived from embryonic rat myocardial tissue, were used in this study to induce hypertrophy [37,38,39]. H9c2 cells (GNR 5) were obtained from the Shanghai Institutes for Biological Sciences, Chinese Academy of Sciences (Shanghai, China). The cells were cultured in 24-well plates at 37 ℃ in a humidified environment with 5% CO2 using Dulbecco’s modified Eagle’s medium (DMEM) supplemented with 10% fetal bovine serum (FBS; Gibco, Cat#10099–141) and 1% penicillin/streptomycin (Yeasen, Cat#60162ES76). To induce cardiomyocyte hypertrophic injury, H9c2 cells were treated with β-adrenergic agonist, isoproterenol (ISO), as described previously [40,41,42]. Briefly, cells were cultured with serum-free DMEM medium for 12 h and then exposed to 10, 30, and 60 μM ISO (MCE, Cat#HY-B0468) or vehicle (dimethyl sulfoxide, DMSO) for 24 h. The collected cells were subjected to qPCR analysis.
Models of transverse aortic constriction
The animal procedure was performed in accordance with the Guide for the Care and Use of Laboratory Animals published by the US National Institutes of Health (NIH Publication No. 85–23). All experimental procedures were approved by the Animal Use Subcommittee at Soochow University, China. C57BL/6 male mice (8‒10 weeks) were purchased from JOINN Laboratories (Suzhou, China) and were used in all experiments. A mouse model of heart failure was established by transverse aortic constriction (TAC) surgery for 8 weeks, as previously described [43]. Mice were anesthetized with 2% isoflurane and incubated under controlled respiration cycled at 125‒150 breaths per minute and a tidal volume of 0.1‒0.3 mL. With the mouse supine, the aortic arch was fully exposed via the left thoracotomy. A 26G syringe needle was placed between the brachiocephalic artery and the left common carotid artery, which was followed by the ligation with a 7–0 thin thread to constrict the aortic arch to 0.44 mm in diameter. After the ligation, the syringe needle was removed immediately. Mice in the sham group underwent the same surgery without constriction of the aortic arch. All animals were given sterile saline of 1 mL containing buprenorphine and penicillin subcutaneously for half an hour prior to TAC surgery and then at 12 h intervals as appropriate.
Echocardiography
All animals were anaesthetized with inhaled 1–2% isoflurane and imaged on a warm platform via a 40 MHz linear array transducer attached to a preclinical ultrasound system (Vevo 2100, FUJIFILM Visual Sonics, Canada) with a nominal in-plane spatial resolution of 40 μm (axial) × 80 μm (lateral) as previously described [44]. Changes of ejection fraction (EF), fractional shortening (FS), left ventricular anterior wall dimension at end-diastole (LVAW;d), left ventricular anterior wall dimension at end-systole (LVAW;s), left ventricle end diastolic inner diameter (LVID;d), left ventricle end systolic inner diameter (LVID;s), left ventricle posterior wall thickness at end-diastole (LVPW;d), left ventricle posterior wall thickness at end-systole, (LVPW;s), left ventricular diastolic volume (LV Vol;d), and left ventricular systolic volume (LV Vol;s) were determined.
RNA extraction and qPCR
RNA isolation and qPCR were performed to analyze the mRNA expression in cells and mice failing heart tissues. Total mRNA was extracted using TRIzol (Invitrogen, Cat#15596018), followed by reverse transcription into cDNA using TaKaRa PrimeScript RT reagent Kit with gDNA Eraser (Takara, Cat#047A) according to the manufacturer’s instructions. The PCR amplifications were quantified using TaKaRa TB Green Premix Ex Taq (Takara, Cat#420A) on the StepOnePlus Real-Time PCR System (Applied Biosystems). The relative mRNA levels were calculated using the 2−∆∆Ct method with Glyceraldehyde-3-phosphate dehydrogenase (GAPDH) or β-Actin as a control for standardization. The primer sequences for qPCR were clarified in Additional file 1: Table S2.
Histological analysis
Hearts tissues were collected and fixed in 10% formalin, followed by embedded in paraffin and sectioned at 5 µm intervals following standard protocol as described previously [45]. After processing, haematoxylin and eosin (H&E) staining were performed according to standard procedures. Cardiomyocyte cross-sectional areas and collagen deposition of heart sections were determined as we previously described [44, 46].
Malondialdehyde (MDA) assay
The relative MDA concentration in heart tissue homogenate was assessed using a Lipid Peroxidation (MDA) Assay Kit (Solarbio, Cat#BC0025) according to the manufacturer’s instructions.
Caspase-3 activity
Caspase-3 activity in cardiac tissues was measured using a Caspase-3 Fluorescence Assay Kit (Biomol Research Laboratories, Inc., Plymouth, PA, USA) following the manufacturer’s instructions.
Statistical analysis
Statistical analysis was performed using the bioinformatics tools mentioned above, R Studio software V4.2.1 and GraphPad Prism 6.0. The Student's t-test was utilized to assess the statistical significance between the two groups when the data conformed to a normal distribution. Results were considered statistically significant at *P < 0.05, **P < 0.01, ***P < 0.001, and ****P < 0.0001.
Results
Identification of common DEGs between COVID-19 and cardiovascular diseases
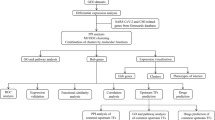
The workflow diagram of this study is shown in Fig. 1. To study the interaction and crosstalk between COVID-19 and cardiovascular diseases, we downloaded and analyzed the GSE156754 and GSE84796 datasets from the GEO database. Genes meeting the criteria, P-value < 0.05 and fold change (FC) > 2 in comparison with control, were characterized as up-regulated DEGs, whereas genes with P-value < 0.05 and FC < -2 compared with the control were considered to be down-regulated DEGs. The GSE156754 dataset was applied for the identification of DEGs in SARS-CoV-2 infected cardiomyocytes. A total of 11,720 DEGs were identified, of which 7900 genes were up-regulated and 3820 genes were down-regulated (Fig. 2A). Using the GSE84796 heart failure dataset, 1421 DEGs were obtained, of which 953 genes were up-regulated and 468 genes were down-regulated (Fig. 2B). Among these DEGs, 315 common up-regulated genes and 78 common down-regulated genes were screened by the intersection of DEGs from the SARS-CoV-2 infection and heart failure datasets (Fig. 2C, D).

Study flowchart. Two categories of samples (SARS-CoV-2 infected hiPSC-CMs and heart failure samples) were collected from the GSE156754 dataset and GSE84796 dataset, respectively. The common differentially expressed genes (DEGs) of both datasets were identified. GO enrichment analysis, KEGG pathway analysis, protein–protein interaction (PPI) network construction, hub genes identification, immune infiltration analysis, drug candidate prediction, and experimental validation were performed on the common DEGs. hiPSC-CMs, human induced pluripotent stem cell-derived cardiomyocytes

The common differentially expressed genes between SARS-CoV-2 infection and cardiovascular diseases. Volcano plot of DEGs in the SARS-CoV-2-related GSE156754 dataset (A) and cardiovascular diseases-related GSE84796 dataset (B). Red dots represent up-regulated DEGs, blue dots represent down-regulated DEGs, and gray dots represent genes that were not significantly different between the two groups. Common up-regulated (C) and down-regulated (D) DEGs in the GSE156754 dataset (blue) and GSE84796 dataset (red) were represented by venn diagrams. E–S Expression of potential receptors or co-factors for SARS-CoV-2 entry in the cardiovascular diseases-related GSE84796 dataset. See also Supplementary methods in Additional file 1 for more information on these factors. CVD, cardiovascular disease. *P < 0.05; ***P < 0.001; ****P < 0.0001; ns, no significance
Certain receptors or co-factors for SARS-CoV-2 invasion were up-regulated in individuals with cardiovascular diseases
The invasion of cells by SARS-CoV-2 is contingent upon the binding of Spike protein to receptors on the cell membrane and cleavage of Spike by cellular proteases, and the expression level of such receptors or proteases can signify the entry and dissemination of viruses as well as the clinical manifestations. To explore the distribution of receptors and entry-related co-factors for SARS-CoV-2, as well as host proteins predicted to interact with the Spike protein based on structural analysis [17,18,19,20] in individuals with cardiovascular diseases, we investigated their expression levels in myocardial tissues of heart failure patients and healthy controls (Fig. 2E–S and Additional file 1: Fig. S1. Detailed information for these factors can be found in Additional file 1: Methods). In myocardial tissues afflicted with heart failure, the expression of ACE2, the most crucial receptor for SARS-CoV-2, was significantly increased. Moreover, three other factors that have been reported to be involved in the entry of SARS-CoV-2, namely sialic acid binding Ig like lectin 1 (SIGLEC1), C-type lectin domain containing 10A (CLEC10A), and mannose receptor C-type 1 (MRC1), were also elevated. SIGLEC1 is reported to mediate the attachment of SARS-CoV-2 to antigen-presenting cells [47]. CLEC10A interacts with the Spike protein of SARS-CoV-2, and this interaction leads to a marked pro-inflammatory response in myeloid cells, which directly correlates with the severity of COVID-19 [48]. MRC1 is highly expressed in dendritic cells, monocytes and macrophages, and has a strong affinity for the SARS-CoV-2 Spike protein [49]. In addition, the expression of several genes showed a tendency of upregulation, although there was no significant difference. For instance, von willebrand factor (VWF), a marker of vascular endothelial cell phenotype, is recently found to regulate ACE2 expression in vascular endothelial cells, and may be involved in susceptibility to cardiac infections associated with the degree of oxidative stress [50]. These results suggest that patients with pre-existing cardiovascular diseases over-expressed certain receptors or co-factors for SARS-CoV-2, which may heighten the susceptibility of cardiac tissue to the virus and lead to a worse prognosis.
GO and KEGG enrichment analysis
To reveal the underlying molecular mechanisms of SARS-CoV-2 infection-related cardiac injury, we performed GO enrichment and KEGG pathway analyses on the common DEGs. In biological process (BP), these common up-regulated genes were primarily responsible for inflammatory response, innate immune response, transmembrane receptor protein tyrosine kinase signaling pathway, cell surface receptor signaling pathway, peptidyl-tyrosine phosphorylation, positive regulation of T cell proliferation, cytokine-mediated signaling pathway, T cell receptor signaling pathway, calcium ion transport, and calcium-mediated signaling. In cellular component (CC), these common up-regulated genes mostly distributed in lipid bilayer membranes, such as plasma membrane, immunological synapse, phagocytic cup, receptor complex, membrane raft, and lysosome. In molecular function (MF), these common up-regulated genes were mainly involved in transmembrane signaling receptor activity, non-membrane spanning protein tyrosine kinase activity, cytokine receptor activity, protein tyrosine kinase activity, T cell receptor binding, protein serine/threonine/tyrosine kinase activity, signaling receptor binding, phosphotyrosine residue binding, chemokine activity, and carbohydrate binding (Fig. 3A). KEGG analysis showed that these common up-regulated genes were involved in B cell receptor signaling pathway, hematopoietic cell lineage, Th17 cell differentiation, Th1 and Th2 cell differentiation, osteoclast differentiation, viral protein interaction with cytokine and cytokine receptor, cytokine-cytokine receptor interaction, chemokine signaling pathway, primary immunodeficiency, and NF-κB signaling pathway (Fig. 3C). These results suggest that inflammatory response and immune activation play a crucial role in the progression of COVID-19 and cardiovascular diseases.

Gene Ontology and pathway enrichment analysis. GO (A) and KEGG enrichment analysis (C) of the 315 common up-regulated genes identified in SARS-CoV-2 infection and cardiovascular diseases. GO (B) and KEGG enrichment analysis (D) of the 78 common down-regulated genes identified in SARS-CoV-2 infection and cardiovascular diseases. BP, biological process; CC, cellular component; MF, molecular function
For these common down-regulated genes, among the biological process, DEGs were mainly enriched in cardiac muscle hypertrophy in response to stress, small GTPase mediated signal transduction, mitochondrial electron transport, NADH to ubiquinone, positive regulation of potassium ion export across plasma membrane, positive regulation of transcription, DNA-templated, mitochondrial ATP synthesis coupled proton transport, regulation of centrosome cycle, aerobic respiration, regulation of high voltage-gated calcium channel activity, and endocardial cushion formation. In cellular component, these common down-regulated genes were mostly localized in spindle midzone, focal adhesion, mitochondria, longitudinal sarcoplasmic reticulum, and so forth. In molecular function, these common down-regulated genes were primarily concentrated in protein binding, GTP binding, calmodulin binding, protein kinase binding, GTPase activity, identical protein binding, and calcium ion binding (Fig. 3B). In terms of the KEGG pathway, the common down-regulated genes were enriched in pathways of non-alcoholic fatty liver disease, cGMP-PKG signaling pathway, diabetic cardiomyopathy, thermogenesis, oxidative phosphorylation, vascular smooth muscle contraction, retrograde endocannabinoid signaling, adrenergic signaling in cardiomyocytes, axon guidance, and metabolic pathways (Fig. 3D). These results showed that mitochondrial dysfunction, metabolic dysregulation, and cytokinesis failure play a crucial role in the progression of COVID-19 and cardiovascular diseases. In addition, these functional enrichment analyses also indicated that SARS-CoV-2 infection had an impact on pathways associated with the heart, such as diabetic cardiomyopathy and adrenergic signaling in cardiomyocytes.
Protein‒protein interaction network analysis and hub genes identification
The 393 common DEGs were uploaded into STRING to construct the PPI network, and the generated file was imported into Cytoscape for visualization (Fig. 4A). The MCODE plugin was used to recognize key clusters, and a significant module consisting of 15 nodes and 72 edges was identified, as depicted in Fig. 4B. The genes involved in the module were IL10RA, TLR7, CD1C, CCL5, CCL3, CXCL10, CCR5, IRF4, CSF1R, MRC1, CXCL9, KLRB1, CD3E, SIGLEC1, and NCF4. Then, using the CytoHubba plugin based on four algorithms, 11 genes (PTPRC, CD19, ITGAX, GZMB, IL10RA, TLR7, CSF1R, CCR7, CCR5, ITGAL, and IL2RB) were identified as hub genes and considered the core targets of COVID-19 and cardiovascular diseases (Fig. 4C and Table 1). A gene network was further constructed using GeneMANIA. Gene functional annotation revealed that these hub genes are all associated with innate immune and inflammatory response, primarily involved in leukocyte mediated cytotoxicity, response to interleukin-2, receptor signaling pathway, lymphocyte proliferation, regulation of inflammation, and chemokine production (Fig. 4D).

Protein‒protein interaction (PPI) network analysis and hub genes identification. A PPI network for common DEGs that are shared by SARS-CoV-2 infection and cardiovascular diseases. Red nodes represent up-regulated DEGs, and blue nodes represent down-regulated DEGs. The size of the node responds to its degree in the network. The thickness of the edges is related to the strength of the interaction. B A key cluster with 15 genes was further chosen by MCODE plugin in Cytoscape. C The 11 hub genes identified according to four algorithms (MCC, MNC, degree, and EPC) of CytoHubba plugin in Cytoscape (see also Table 1). D The gene network and functional analysis of hub genes were generated using GeneMANIA. The inner circle stands for hub genes, and the outer circle refers to the corresponding reciprocal genes. Colors of nodes represent gene function annotations, which refer to GO terms enriched among the genes in the network displayed by GeneMANIA. Colors of edges represent interaction based on co-expression, physical interactions, co-localization, shared protein domain, or predicted interaction
In addition, as the functional enrichment results above suggested, immune activation and mitochondrial dysfunction were closely associated with the course of both diseases. Therefore, we conducted further scrutiny of the correlation between genes related to immunity or mitochondria. Immune-related genes were searched from the ImmPort database, and genes overlapping with common DEGs were selected as ImmuneDEGs. Totally, 74 ImmuneDEGs (67 up-regulated and 7 down-regulated) were obtained (Fig. 5A). Then, 10 hub ImmuneDEGs were identified using CytoHubba, including PTPRC, IL10RA, TLR7, CCL5, CCL3, CXCL9, CD19, CD1C, CSF1R, and GZMB, most of which were also identified as the aforementioned hub genes. These hub ImmuneDEGs were further imported into GeneMANIA to construct a gene network (Fig. 5C). IL10RA has immune receptor activity [51]. CCL5, CCL3, and CXCL9 are chemokines with cytokine activity and are involved in the cellular response to chemokine. In addition, these hub ImmuneDEGs are mainly enriched in biological processes such as regulation of ERK1 and ERK2 cascade, lymphocyte mediated immunity, regulation of inflammatory response, and calcium ion transport.

Network and functional analysis of ImmuneDEGs and MitoDEGs. Venn diagram showing 74 ImmuneDEGs (A) and 14 MitoDEGs (B). ImmuneDEGs and MitoDEGs were submitted to the STRING database and 10 hub ImmuneDEGs and 7 hub MitoDEGs were identified using the CytoHubba plugin in Cytoscape. Then, the 10 hub ImmuneDEGs (C) and 7 hub MitoDEGs (D) were uploaded in the GeneMANIA database for the further gene network analysis. The inner circle stands for hub genes, and the outer circle refers to the corresponding reciprocal genes. Colors of nodes represent gene function annotations, which refer to GO terms enriched among the genes in the network displayed by GeneMANIA. Colors of edges represent interaction based on co-expression, shared protein domain, co-localization, physical interactions, pathway, or predicted interaction. ImmuneDEGs, immune-related DEGs; MitoDEGs, mitochondria-related DEGs
Similarly, mitochondria-associated genes, mainly referring to nuclear genes coding proteins with mitochondrial location, were accessed from the MitoCarta3.0 database, and genes that were overlapping with shared DEGs were chosen as MitoDEGs. After intersection with the common DEGs, 14 genes (3 up-regulated and 11 down-regulated) were selected as MitoDEGs (Fig. 5B). These genes were then subjected to CytoHubba analysis, which highlighted 7 hub MitoDEGs, namely NDUFAB1, NDUFA6, NDUFV3, MRPS12, MRPL12, CYCS, and COQ5. Hub MitoDEGs were then used to construct a gene network via GeneMANIA (Fig. 5D). These hub MitoDEGs are mainly localized to mitochondrial protein complex, such as NDUFAB1, NDUFA6 and NDUFV3 are members of the NADH dehydrogenase complex with NADH dehydrogenase activity [52, 53]. In terms of biological processes, NDUFAB1, NDUFA6, NDUFV3, and CYCS are involved in mitochondrial ATP synthesis coupled electron transport, and COQ5 is involved in quinone biosynthesis process [54].
Immune cell infiltration in cardiovascular diseases
Considering the vital role of immune activation in COVID-19-related cardiovascular diseases, we conducted a detailed analysis of the immune microenvironment in the cardiac tissue of patients with cardiovascular diseases. Using the CIBERSORTx algorithm, we examined the infiltration of 22 different kinds of immune cells and compared them between the cardiovascular diseases group and the control group. Our findings showed that there were significant differences in the myocardial infiltration of 11 immune cell types between the two groups. Specifically, CD8 + T cells, activated memory CD4 + T cells, Tregs, γδT cells, monocytes, and M1 macrophages were much more abundant in the cardiovascular diseases group, whereas naive B cells, resting memory CD4 + T cells, follicular helper T cells, activated dendritic cells, and activated mast cells were more abundant in the control group (Fig. 6A, B). Further analysis also revealed various correlations among infiltrating immune cells (Fig. 6C).

Immune infiltration analysis. A Immune cell infiltration analysis in the cardiovascular diseases-related GSE84796 dataset. B Stacked bar chart showing the percentage of immune cells in each sample. C Heat map showing the correlation between immune cells. *P < 0.05; **P < 0.01; ***P < 0.001; ns, no significance
Prediction of candidate drugs for COVID-19-related cardiovascular diseases
To anticipate efficacious agents for the therapy of COVID-19-related cardiovascular diseases, the 11 hub DEGs were submitted to the cMAP database. The results of drug candidates were generated based on the absolute enrichment score (Table 2). The analysis showed that actarit, raltegravir, epigallocatechin, doxylamine, lidocaine, tetrabenazine, escitalopram, desoxypeganine, and valproic-acid were the top 9 candidate drugs. These drugs represent the potential drugs for COVID-19-related cardiovascular diseases.
Experimental validation of hub genes
To strengthen the clinical relevance of hub DEGs, we conducted an analysis on the association between hub genes and clinical features. The CTD database was utilized to forecast the links between hub DEGs and cardiovascular, heart, and vascular diseases. The results demonstrated that CSF1R, CCR5, ITGAL, IL10RA, and ITGAX had the highest association with cardiovascular diseases, and CSF1R, CCR5, TLR7, ITGAL, and CCR7 showed the highest correlation with heart diseases, while CSF1R, CCR5, ITGAL, PTPRC, and CCR7 showed the highest correlation with vascular diseases (Fig. 7A). To verify the expression of the top 10 cardiovascular diseases-related hub genes shown in Fig. 7A, we analyzed the GSE57338 dataset to assess their expression in heart failure patients. The results revealed that most of the genes, including PTPRC, ITGAX, GZMB, TLR7, CSF1R, CCR7, ITGAL, and IL2RB, exhibited significantly elevated expression levels in failing hearts as compared to non-failing hearts (Fig. 7B–K).

Relationship between hub genes and cardiovascular diseases and validation of hub genes in heart failure patients. A Analysis of the relationship between hub genes and cardiovascular diseases, heart diseases, and vascular diseases based on the CTD database. B–K Expression of hub genes in the validation set GSE57338. *P < 0.05; **P < 0.01; ***P < 0.001; ****P < 0.0001
Subsequently, isoproterenol (ISO)-stimulated cardiomyocyte hypertrophic injury in H9c2 cells and a transverse aortic constriction-induced heart failure model in mice were used to further verify the expression of hub genes [37,38,39]. First, different concentrations of ISO were used to establish an in vitro cell model using H9c2 cells. The results showed that, treatment of H9c2 cells with 60 μM ISO for 24 h induced a significant up-regulation of the expression of cardiac hypertrophy markers, atrial natriuretic peptide (ANP) and myosin heavy chain β (β-MHC), and had no significant effect on cell viability (Additional file 1: Fig. S2). Additionally, in ISO-treated H9c2 cells, the mRNA levels of Ccr5, Csf1r, Ccr7, and Il2rb were also remarkably raised (Fig. 8A). The remaining genes were difficult to detect, probably due to their low expression in H9c2 cells. Similarly, in ISO-stimulated hiPSC-CMs, which exhibits an arrhythmic phenotype [55, 56], mRNA expression levels of CCR5, CSF1R, TLR7, IL2RB, and IGTAX were upregulated (Additional file 1: Fig. S3).

Experimental verification of the expression of hub genes in cardiac injury. A H9c2 cells treated with DMSO or 60 μM isoproterenol for 24 h were performed to analyze mRNA expression levels of hub genes. Values represent means ± SD (n = 3 biologically independent samples). B–Q Characterization of physiological and cardiac features of transverse aortic constriction (TAC) induced heart failure and confirmation of hub genes expression. Heart failure was induced by TAC at a 0.44 mm diameter for 8 weeks. Cardiac function (B and C) was determined in the heart. Hearts were collected and processed for anatomical and histologic analysis. Heart weight/body weight (D) and heart weight/tibia length (E). F Representative image of whole heart, and histological picture of H&E staining, Sirius red staining, and fluorescence-conjugated wheat germ agglutinin (WGA) staining for heart. Bars, 50 μm. Quantification for collagen deposition (G) and cardiomyocyte cross-sectional areas (H). I The levels of malondialdehyde (MDA) in heart lysates. J Apoptosis was determined based on caspase-3 activity. K The expression levels of mRNA of hub genes were confirmed in sham and TAC mice. Values represent means ± SD (n = 4 mice). L–Q Correlations between Ccr5, Csf1r, and Tlr7 mRNA expression levels and cardiac functional parameters. R denotes the correlation coefficient between the variables and P denotes the statistical P-value between the variables, which were obtained by Pearson correlation analysis. All qPCR graphs show gene expression normalized to Glyceraldehyde-3-phosphate dehydrogenase (Gapdh). *P < 0.05; **P < 0.01; ns, no significance
In 8-week TAC mice, echocardiographic measurement demonstrated that ejection fraction and fractional shortening were decreased in TAC mice (Fig. 8B, C and Additional file 1: Table S3). In line with this, histological and anatomical analyses revealed that TAC mice exhibited noticeable changes associated with myocardial hypertrophy and fibrosis. These changes included increased inflammatory cell infiltration, collagen deposition, enlarged cross-sectional areas of cardiomyocytes, and enlargement of the heart size (Fig. 8D–H). Accordingly, analysis of gene expression demonstrated upregulation of mRNA levels related to myocardial hypertrophy (ANP and β-MHC) and fibrosis (Col3a1) in the hearts of TAC mice compared to the sham group (Additional file 1: Fig. S4). In addition, myocardial oxidative stress and apoptosis were further evaluated. The results showed increased production of MDA, the lipid peroxidation marker, and elevated caspase-3 activity, in the heart tissues of TAC mice (Fig. 8I, J). Taken together, these results demonstrate that TAC surgery induces hypertrophy and heart failure in mice. As shown in Fig. 8K, mRNA levels of three candidate genes (Ccr5, Csf1r, and Tlr7) were significantly increased in heart failure mice. Meanwhile, the remaining hub genes, while not displaying statistical significance, exhibited a discernible trend of increased expression in heart failure mice. Then, the relationship between the above three hub genes (Ccr5, Csf1r, and Tlr7) and cardiac function was further investigated. The expression of Ccr5 was significantly negatively correlated with EF% (R = − 0.921; P = 0.001) and FS% (R = − 0.928; P < 0.001); while the expression of Csf1r and Tlr7 was slightly negatively correlated with EF% and FS% (Fig. 8L–Q). These findings suggest that the up-regulated expression of Ccr5, Csf1r, and Tlr7 in the myocardial tissues is related to the decline of cardiac function in heart failure mice.
Discussion
During the COVID-19 pandemic, it has been recognized that SARS-CoV-2 infection can induce serious or even fatal cardiac complications [1, 57]. Moreover, patients with pre-existing cardiovascular diseases have poorer outcomes after developing COVID-19 [1, 4]. However, there is limited research on the shared molecular mechanisms between COVID-19 and cardiovascular diseases. In the present study, we identified 315 common up-regulated DEGs and 78 common down-regulated DEGs between COVID-19 and cardiovascular diseases. Functional enrichment analysis showed that mitochondrial dysfunction, metabolic abnormality, immune activation, and inflammatory response were the most important features of COVID-19 and cardiovascular diseases. In addition, enrichment of cardiovascular-related pathways, such as diabetic cardiomyopathy, adrenergic signaling in cardiomyocytes, and vascular smooth muscle contraction, may reflect the occurrence of cardiovascular injury in COVID-19 patients. Representative aspects of the interplays between COVID-19 and cardiovascular diseases highlighted in this study are further discussed below.
The mitochondrion plays a vital role in the maintenance of intracellular homeostasis. Mitochondria are responsible for a series of essential cellular processes, for instance, ATP synthesis, anabolism and catabolism, fatty acid oxidation, calcium ion storage, modulation of innate immune signaling and inflammatory response, and regulation of cell death [58]. Our results reveal that genes associated with energy metabolism in mitochondria are down-regulated predominantly in both COVID-19 and cardiovascular diseases. These findings are consistent with results from multiple actual infection systems or patients. For instance, patients with COVID-19 exhibit notable mitochondrial dysfunction as well as metabolic disturbances marked by an upsurge in glycolysis in peripheral blood mononuclear cells (PBMCs) [59]. SARS-CoV-2 can also cause transcriptional downregulation of the mitochondrial respiratory chain complex and ATP synthesis in hiPSC-CMs [60]. Our and these previous studies demonstrate that mitochondrial dysfunction and metabolic alteration are involved in COVID-19. Mitochondrial metabolic abnormalities have also been shown to play a critical role in various cardiovascular disorders [61]. Under physiological conditions, cardiomyocytes critically depend on fatty acid-driven oxidative phosphorylation for ATP synthesis [62]. In a variety of cardiomyopathies, cardiomyocytes are accompanied by ATP exhaustion and increase of reactive oxygen species (ROS), which may directly compromise myocardial function [63]. In general, the increase in ROS and the consumption of ATP appears to be associated with impaired homeostasis of certain metabolites and co-factors that are beneficial for proper mitochondrial function, as well as impairment of mitochondrial dynamics and abnormal restructuring of mitochondrial and mitochondrial membrane structures [64]. Thus, mitochondria and mitochondrial proteins are a promising set of pharmacological targets for the search of new molecular targets and drugs to combat cardiovascular diseases [64, 65].
In addition to regulating energy metabolism, maintaining intracellular Ca2+ homeostasis is also a core function of mitochondria. According to the outcomes of our GO analysis, disturbances in Ca2+ homeostasis are present in both diseases, as evidenced by the enrichment of DEGs in calcium ion transport, calcium-mediated signaling, and calcium channel activity. Calcium ion acts as an intracellular messenger and regulator of numerous cellular processes and is central to overall cardiac activity [66]. For example, Ca2+ flux is crucial for cardiomyocytes and vascular smooth muscle cells because both cardiac and arterial contractions rely on instantaneous changes in cellular Ca2+ concentrations [66]. SARS-CoV-2-encoded E and ORF3a proteins function as viroporins, which form Ca2+ channels at the mitochondria-ER contact sites within infected cells [67, 68]. The resultant alteration in intracellular Ca2+ homeostasis subsequently triggers the inflammatory cascade, leading to a cytokine storm and tissue injury. Extensive and unreversible mitochondrial dysfunction, culminating in altered permeability of the mitochondrial membrane, has a pivotal role in mitochondrial-regulated cell death, including apoptosis, regulatory necrosis, and pyroptosis [69]. The irreversible death of damaged cells is an essential trigger for the development of cardiovascular diseases, including atherosclerosis, myocardial infarction, and heart failure.
In addition, mitochondria serve as an important innate immune antiviral platform by housing the mitochondrial antiviral signaling protein (MAVS) to act as a central hub for antiviral signaling [70]. Viral components may be involved in the regulation of mitochondrial function through interactions with proteins with mitochondrial localization. For example, a recent study based on a computational approach predicting the interaction of Spike protein and ACE2-related proteins found that Spike protein may interact with neurolysin (NLN) and thimet oligopeptidase (THOP1), which have high structural similarity to ACE2 and have mitochondrial localization [18]. NLN and THOP1 are closely-related zinc metallopeptidases, NLN plays a crucial role in the assembly of respiratory chain supercomplexes [71], and both NLN and THOP1 play key physiological functions in the regulation of energy metabolism [72]. Interestingly, the mRNA expression level of THOP1 were downregulated in cardiac tissues from heart failure patients, which could be related to impaired cardiac energy metabolism in heart failure individuals (Additional file 1: Fig. S1B). The potential interaction between Spike protein and these proteins, which are localized in mitochondria and play a role in regulating energy metabolism, offers insights into how SARS-CoV-2 causes damage to cardiac tissue by disrupting mitochondrial function. The shared cardiac mitochondrial dysfunction and metabolic profile of COVID-19 and cardiac diseases imply that SARS-CoV-2 infection may potentially contribute to worsening clinical symptoms of cardiovascular diseases.
Mitochondria and immune system are inextricably interrelated, and mitochondrial function is crucial for modulating the immune response and resolution during recovery after cardiac injury [73, 74]. Innate immunity serves as the first barrier against viruses, while an imbalanced immune system can also trigger life-threatening inflammatory responses. Reduced innate antiviral defenses and “cytokine storm” are thought to be the pathological mechanisms of COVID-19 and the sequelae of the circulatory system in COVID-19, with monocytes and macrophages being the primary contributors [75, 76]. Evidence from clinical studies indicates that the severity of COVID-19 is positively associated with chemokine and inflammatory cytokine levels in the plasma of patients, such as TNF-α, IL-1β, IL-6, CCL2, CCL8, and CXCL9 [76, 77]. Additionally, long COVID patients experience persistent immunological dysfunction, including absence of naive T and B cells and high levels of inflammatory mediators in their plasma, even 8 months after infection [24, 78]. Chronic inflammatory disorders are also risk factors associated with a variety of cardiovascular diseases [79, 80]. For example, pro-inflammatory response driven by TLR signaling is a critical mechanism in the pathogenesis of atherosclerosis [81]. As atherosclerosis progresses, inflammation and immune responses promote instability of the arterial lesions, which leads to lethal consequences such as myocardial infarction. In this study, analysis of the immune microenvironment revealed an increase of monocytes and M1 macrophages and a reduction of naive B cells in myocardial tissues from individuals with cardiovascular diseases, exhibiting an immune cell fraction profile similar to that of COVID-19. Since inflammation is an important player in both COVID-19 and cardiovascular diseases, we hypothesize that abnormal activation of the immune system and excessive systemic inflammatory response, rather than a direct cell-killing effect caused by SARS-CoV-2 infection, may be triggers for cardiac involvement.
Additionally, the hub genes associated with the common pathogenesis of COVID-19 and cardiovascular diseases identified in this study, namely PTPRC, ITGAX, GZMB, IL10RA, TLR7, CSF1R, CCR7, CCR5, ITGAL, and IL2RB, are all associated with innate immune and inflammatory responses. Integrin signaling has been shown to regulate endothelial phenotype, leukocyte homing, and smooth muscle fibro proliferative remodeling, thereby contributing to the development of cardiovascular diseases [82]. The discovery of ITGAX and ITGAL, members of the integrin family, suggests that these integrin regulatory mechanisms may be the pathway by which SARS-CoV-2 drives its adverse effects on the cardiovascular system. Colony-stimulating factor 1 receptor (CSF1R) is important for proliferation, differentiation and survival of mononuclear phagocytes and has been identified as a key gene in COVID-19-related cardiovascular diseases [83, 84]. The PTPRC gene, which encodes the protein tyrosine phosphatase receptor type C, is critical for regulating antigen receptor signaling in T and B cells. PTPRC is revealed as a new biomarker for SARS-COV-2 pathogenesis through the analysis of various transcriptomic datasets from COVID-19 patients [85]. Toll-like receptor 7 (TLR7), a member of the toll-like receptor family, has an essential role in pathogen recognition and immune system activation. SARS-CoV-2 can be recognized by TLR7 and activate the MyD88-dependent NF-κB pathway, resulting in elevated production of pro‐inflammatory cytokines [86, 87]. Additionally, TLR7 activation has been linked to the acceleration of cardiovascular pathology [88]. GZMB encodes a serine protease, which is crucial for cytotoxic T lymphocyte-mediated cell death. SARS-CoV-2 infection triggers a strong cytotoxic T-cell immune response [89]. Similarly, our immune infiltration analysis showed significant activation of CD8 + T cells in the cardiac tissues of heart failure patients (Fig. 6). GZMB also plays a role in matrix remodeling and cardiac fibrosis [90]. The interleukin 10 (IL-10) receptor, IL10RA, mediates the immunosuppressive signal of the anti-inflammatory cytokine, IL-10, which limits excessive tissue disruption caused by inflammation [51]. The elevation of IL-10 receptors in COVID-19 and cardiovascular diseases appears to be a mechanism by which the body regulates pathological consequences caused by inflammatory response. IL2RB, a receptor for IL-2, is involved in T cell-mediated immune responses and plays a fundamental role in the development of coronary artery disease [91]. Chemokines and chemokine receptors play a great function in controlling the degree of immune cell infiltration. The higher expression levels of CCR5, CCR7 and their ligands are associated with the development and progression of cardiovascular diseases, such as atherosclerosis [92]. These results further strengthen the potential role of the hub genes we identified in the pathogenesis of COVID-19-related cardiovascular diseases.
Since the pandemic, the development of vaccines against SARS-CoV-2 has progressed rapidly, and approved vaccines, mainly including inactivated, mRNA, protein subunit, and adenoviral vector vaccines, have been highly effective in preventing COVID-19, particularly severe disease [26, 93]. However, as the protective effect of vaccines diminishes due to viral variants, the passage of time since vaccination, and waning immunity [26, 27], there remains an urgent need for new antiviral therapies to combat the pandemics. Currently, several antiviral drugs, such as paxlovid, immunomodulatory drugs, and anti-SARS-CoV-2 neutralizing monoclonal antibodies (i.e., bamlanivimab, etesevimab, sotrovimab, casirivimab, and imdevimab, which block infection of target cells while invoking phagocytosis and elimination of the virus), have been proposed as potential treatments for COVID-19 [94,95,96]. Despite the promise of these agents, their high cost renders them impractical for large-scale implementation. Moreover, the multiple complications accompanying SARS-CoV-2 infection limit the currently available options, and the safety of drug administration needs to be considered more thoroughly. Thus, a comprehensive analysis of the common pathogenesis between COVID-19 and cardiovascular diseases may yield valuable insights for future personalized treatments for specific populations. Here, we propose potential drugs that may be used to treat COVID-19-associated cardiac injury. For example, epigallocatechin, a compound in green tea, has been reported to have anti-SARS-CoV-2 and cardioprotective efficacy [97, 98]. Epigallocatechin may exert protective effect on mitochondrial function by preventing mitochondrial ROS induced by SARS-CoV-2 or cardiovascular disease via its broad antioxidant activity [97, 98]. Lidocaine, a local anesthetic agent, has been approved for the treatment of cardiac arrhythmias owing to its remarkable anti-inflammatory properties. Recent research has revealed that lidocaine effectively modulates the inflammatory response induced by the SARS-CoV-2 infection [99]. Actaris, an anti-rheumatic drug, is employed to rectify immunological disorders through immunomodulation [100]. Raltegravir acts as an inhibitor of HIV-1 integrase [101]. The aforementioned drugs exert their effects by modulating immune response, inflammation, or mitochondrial function, which are also common pathological manifestations of COVID-19 and cardiovascular diseases, and additional validations are necessary to further investigate their potential applications. These findings suggest a deeper understanding of the shared molecular pathogenic mechanisms between COVID-19 and cardiovascular diseases could be strategically useful in developing therapeutic targets in the treatment of cardiac injury associated with SARS-CoV-2 infection.
However, there are limitations to this study due to data and sample restrictions. Specifically, the investigation relied on data obtained solely from virus-infected cardiomyocytes or patients with heart failure, rather than those with both conditions. And we were unable to acquire cardiac tissue samples from patients with COVID-19 and cardiovascular diseases to confirm the expression of key genes. Given the limitations, it is necessary to collect more information on patients with cardiac injury associated with SARS-CoV-2 infection and explore the relationship between viral infection and the occurrence of cardiac involvement in the future.
Conclusions
This study is critical for understanding SARS-CoV-2-host interactions, the mechanisms underlying SARS-CoV-2-induced cardiac injury, and the factors contributing to poorer outcomes in COVID-19 patients with pre-existing cardiovascular diseases. These key genes identified in this study, particularly immune-inflammation and mitochondrial metabolism-related genes, along with the signaling pathways they control, may guide the clinical management of COVID-19 patients and facilitate the development of new and effective therapeutic strategies.
Availability of data and materials
The datasets (GSE156754, GSE84796, and GSE57338) analyzed in this study can be found in NCBI Gene Expression Omnibus (GEO).
Abbreviations
- SARS-CoV-2:
-
Severe acute respiratory syndrome coronavirus 2
- COVID-19:
-
Coronavirus disease 2019
- hiPSC-CMs:
-
Human induced pluripotent stem cell-derived cardiomyocytes
- DEGs:
-
Differentially expressed genes
- ACE2:
-
Angiotensin-converting enzyme 2
- FC:
-
Fold change
- GO:
-
Gene Ontology
- KEGG:
-
Kyoto Encyclopedia of Genes and Genomes
- PPI:
-
Protein–protein interaction
- NCBI:
-
National Center for Biotechnology Information
- GEO:
-
Gene Expression Omnibus
- ISO:
-
Isoproterenol
- TAC:
-
Transverse aortic constriction
- FS:
-
Fraction shortening
- EF:
-
Ejection fraction
- qPCR:
-
Quantitative real-time polymerase chain reaction
- GAPDH:
-
Glyceraldehyde-3-phosphate dehydrogenase
- BP:
-
Biological process
- CC:
-
Cellular component
- MF:
-
Molecular function
- IL10RA:
-
Interleukin 10 receptor subunit alpha
- TLR7:
-
Toll like receptor 7
- CCR5:
-
C–C motif chemokine receptor 5
- CSF1R:
-
Colony stimulating factor 1 receptor
- SIGLEC1:
-
Sialic acid binding Ig like lectin 1
- CLEC10A:
-
C-type lectin domain containing 10A
- MRC1:
-
Mannose receptor C-type 1
- VWF:
-
Von willebrand factor
- PTPRC:
-
Protein tyrosine phosphatase receptor type C
- ITGAX:
-
Integrin subunit alpha X
- GZMB:
-
Granzyme B
- CCR7:
-
C–C motif chemokine receptor 7
- ITGAL:
-
Integrin subunit alpha L
- IL2RB:
-
Interleukin 2 receptor subunit beta
- ANP:
-
Atrial natriuretic peptide
- β-MHC:
-
β-Myosin heavy chain
References
Chung MK, Zidar DA, Bristow MR, Cameron SJ, Chan T, Harding CV 3rd, Kwon DH, Singh T, Tilton JC, Tsai EJ, et al. COVID-19 and cardiovascular disease: from bench to bedside. Circ Res. 2021;128:1214–36.
Gyongyosi M, Alcaide P, Asselbergs FW, Brundel B, Camici GG, Martins PDC, Ferdinandy P, Fontana M, Girao H, Gnecchi M, et al. Long COVID and the cardiovascular system-elucidating causes and cellular mechanisms in order to develop targeted diagnostic and therapeutic strategies: a joint Scientific Statement of the ESC Working Groups on Cellular Biology of the Heart and Myocardial and Pericardial Diseases. Cardiovasc Res. 2023;119:336–56.
Davis HE, McCorkell L, Vogel JM, Topol EJ. Long COVID: major findings, mechanisms and recommendations. Nat Rev Microbiol. 2023;21:133–46.
Alvarez-Garcia J, Lee S, Gupta A, Cagliostro M, Joshi AA, Rivas-Lasarte M, Contreras J, Mitter SS, LaRocca G, Tlachi P, et al. Prognostic impact of prior heart failure in patients hospitalized with COVID-19. J Am Coll Cardiol. 2020;76:2334–48.
Ayoubkhani D, Khunti K, Nafilyan V, Maddox T, Humberstone B, Diamond I, Banerjee A. Post-covid syndrome in individuals admitted to hospital with covid-19: retrospective cohort study. BMJ. 2021;372: n693.
Bader F, Manla Y, Atallah B, Starling RC. Heart failure and COVID-19. Heart Fail Rev. 2021;26:1–10.
Chatrath N, Kaza N, Pabari PA, Fox K, Mayet J, Barton C, Cole GD, Plymen CM. The effect of concomitant COVID-19 infection on outcomes in patients hospitalized with heart failure. ESC Heart Fail. 2020;7:4443–7.
Pierri CL. SARS-CoV-2 spike protein: flexibility as a new target for fighting infection. Signal Transduct Target Ther. 2020;5:254.
Turonova B, Sikora M, Schurmann C, Hagen WJH, Welsch S, Blanc FEC, von Bulow S, Gecht M, Bagola K, Horner C, et al. In situ structural analysis of SARS-CoV-2 spike reveals flexibility mediated by three hinges. Science. 2020;370:203–8.
Bian J, Li Z. Angiotensin-converting enzyme 2 (ACE2): SARS-CoV-2 receptor and RAS modulator. Acta Pharm Sin B. 2021;11:1–12.
Bourgonje AR, Abdulle AE, Timens W, Hillebrands JL, Navis GJ, Gordijn SJ, Bolling MC, Dijkstra G, Voors AA, Osterhaus AD, et al. Angiotensin-converting enzyme 2 (ACE2), SARS-CoV-2 and the pathophysiology of coronavirus disease 2019 (COVID-19). J Pathol. 2020;251:228–48.
Lindner D, Fitzek A, Brauninger H, Aleshcheva G, Edler C, Meissner K, Scherschel K, Kirchhof P, Escher F, Schultheiss HP, et al. Association of cardiac infection with SARS-CoV-2 in confirmed COVID-19 autopsy cases. JAMA Cardiol. 2020;5:1281–5.
Kawakami R, Sakamoto A, Kawai K, Gianatti A, Pellegrini D, Nasr A, Kutys B, Guo L, Cornelissen A, Mori M, et al. Pathological evidence for SARS-CoV-2 as a cause of myocarditis: JACC review topic of the week. J Am Coll Cardiol. 2021;77:314–25.
Nchioua R, Diofano F, Noettger S, von Maltitz P, Stenger S, Zech F, Munch J, Sparrer KMJ, Just S, Kirchhoff F. Strong attenuation of SARS-CoV-2 Omicron BA.1 and increased replication of the BA.5 subvariant in human cardiomyocytes. Signal Transduct Target Ther. 2022;7:395.
Nicin L, Abplanalp WT, Mellentin H, Kattih B, Tombor L, John D, Schmitto JD, Heineke J, Emrich F, Arsalan M, et al. Cell type-specific expression of the putative SARS-CoV-2 receptor ACE2 in human hearts. Eur Heart J. 2020;41:1804–6.
Chen C, Wang J, Liu YM, Hu J. Single-cell analysis of adult human heart across healthy and cardiovascular disease patients reveals the cellular landscape underlying SARS-CoV-2 invasion of myocardial tissue through ACE2. J Transl Med. 2023;21:358.
Singh M, Bansal V, Feschotte C. A single-cell RNA expression map of human coronavirus entry factors. Cell Rep. 2020;32: 108175.
Tragni V, Preziusi F, Laera L, Onofrio A, Mercurio I, Todisco S, Volpicella M, De Grassi A, Pierri CL. Modeling SARS-CoV-2 spike/ACE2 protein-protein interactions for predicting the binding affinity of new spike variants for ACE2, and novel ACE2 structurally related human protein targets, for COVID-19 handling in the 3PM context. EPMA J. 2022;13:149–75.
Radzikowska U, Ding M, Tan G, Zhakparov D, Peng Y, Wawrzyniak P, Wang M, Li S, Morita H, Altunbulakli C, et al. Distribution of ACE2, CD147, CD26, and other SARS-CoV-2 associated molecules in tissues and immune cells in health and in asthma, COPD, obesity, hypertension, and COVID-19 risk factors. Allergy. 2020;75:2829–45.
Lim S, Zhang M, Chang TL. ACE2-independent alternative receptors for SARS-CoV-2. Viruses. 2022;14:2535.
Elseidy SA, Awad AK, Vorla M, Fatima A, Elbadawy MA, Mandal D, Mohamad T. Cardiovascular complications in the Post-Acute COVID-19 syndrome (PACS). Int J Cardiol Heart Vasc. 2022;40: 101012.
Sewanan LR, Clerkin KJ, Tucker NR, Tsai EJ. How does COVID-19 affect the heart? Curr Cardiol Rep. 2023;25:171–84.
Peluso MJ, Lu S, Tang AF, Durstenfeld MS, Ho HE, Goldberg SA, Forman CA, Munter SE, Hoh R, Tai V, et al. Markers of immune activation and inflammation in individuals with postacute sequelae of severe acute respiratory syndrome coronavirus 2 infection. J Infect Dis. 2021;224:1839–48.
Phetsouphanh C, Darley DR, Wilson DB, Howe A, Munier CML, Patel SK, Juno JA, Burrell LM, Kent SJ, Dore GJ, et al. Immunological dysfunction persists for 8 months following initial mild-to-moderate SARS-CoV-2 infection. Nat Immunol. 2022;23:210–6.
Lionetti V, Bollini S, Coppini R, Gerbino A, Ghigo A, Iaccarino G, Madonna R, Mangiacapra F, Miragoli M, Moccia F, et al. Understanding the heart-brain axis response in COVID-19 patients: A suggestive perspective for therapeutic development. Pharmacol Res. 2021;168: 105581.
Tregoning JS, Flight KE, Higham SL, Wang Z, Pierce BF. Progress of the COVID-19 vaccine effort: viruses, vaccines and variants versus efficacy, effectiveness and escape. Nat Rev Immunol. 2021;21:626–36.
Lipsitch M, Krammer F, Regev-Yochay G, Lustig Y, Balicer RD. SARS-CoV-2 breakthrough infections in vaccinated individuals: measurement, causes and impact. Nat Rev Immunol. 2022;22:57–65.
Perez-Bermejo JA, Kang S, Rockwood SJ, Simoneau CR, Joy DA, Silva AC, Ramadoss GN, Flanigan WR, Fozouni P, Li H, et al. SARS-CoV-2 infection of human iPSC-derived cardiac cells reflects cytopathic features in hearts of patients with COVID-19. Sci Transl Med. 2021;13:eabf7872.
Laugier L, Frade AF, Ferreira FM, Baron MA, Teixeira PC, Cabantous S, Ferreira LRP, Louis L, Rigaud VOC, Gaiotto FA, et al. Whole-genome cardiac DNA methylation fingerprint and gene expression analysis provide new insights in the pathogenesis of chronic chagas disease cardiomyopathy. Clin Infect Dis. 2017;65:1103–11.
Liu Y, Morley M, Brandimarto J, Hannenhalli S, Hu Y, Ashley EA, Tang WH, Moravec CS, Margulies KB, Cappola TP, et al. RNA-Seq identifies novel myocardial gene expression signatures of heart failure. Genomics. 2015;105:83–9.
Davis S, Meltzer PS. GEOquery: a bridge between the gene expression omnibus (GEO) and bioconductor. Bioinformatics. 2007;23:1846–7.
Szklarczyk D, Kirsch R, Koutrouli M, Nastou K, Mehryary F, Hachilif R, Gable AL, Fang T, Doncheva NT, Pyysalo S, et al. The STRING database in 2023: protein-protein association networks and functional enrichment analyses for any sequenced genome of interest. Nucleic Acids Res. 2023;51:D638–46.
Franz M, Rodriguez H, Lopes C, Zuberi K, Montojo J, Bader GD, Morris Q. GeneMANIA update 2018. Nucleic Acids Res. 2018;46:W60–4.
Rath S, Sharma R, Gupta R, Ast T, Chan C, Durham TJ, Goodman RP, Grabarek Z, Haas ME, Hung WHW, et al. MitoCarta3.0: an updated mitochondrial proteome now with sub-organelle localization and pathway annotations. Nucleic Acids Res. 2021;49:D1541–7.
Davis AP, Wiegers TC, Johnson RJ, Sciaky D, Wiegers J, Mattingly CJ. Comparative toxicogenomics database (CTD): update 2023. Nucleic Acids Res. 2023;51:D1257–62.
Lamb J, Crawford ED, Peck D, Modell JW, Blat IC, Wrobel MJ, Lerner J, Brunet JP, Subramanian A, Ross KN, et al. The connectivity map: using gene-expression signatures to connect small molecules, genes, and disease. Science. 2006;313:1929–35.
Verma SK, Krishnamurthy P, Barefield D, Singh N, Gupta R, Lambers E, Thal M, Mackie A, Hoxha E, Ramirez V, et al. Interleukin-10 treatment attenuates pressure overload-induced hypertrophic remodeling and improves heart function via signal transducers and activators of transcription 3-dependent inhibition of nuclear factor-kappaB. Circulation. 2012;126:418–29.
Klein M, Schermuly RT, Ellinghaus P, Milting H, Riedl B, Nikolova S, Pullamsetti SS, Weissmann N, Dony E, Savai R, et al. Combined tyrosine and serine/threonine kinase inhibition by sorafenib prevents progression of experimental pulmonary hypertension and myocardial remodeling. Circulation. 2008;118:2081–90.
Zhang N, Zhang Y, Qian H, Wu S, Cao L, Sun Y. Selective targeting of ubiquitination and degradation of PARP1 by E3 ubiquitin ligase WWP2 regulates isoproterenol-induced cardiac remodeling. Cell Death Differ. 2020;27:2605–19.
Tse MM, Aboutabl ME, Althurwi HN, Elshenawy OH, Abdelhamid G, El-Kadi AO. Cytochrome P450 epoxygenase metabolite, 14,15-EET, protects against isoproterenol-induced cellular hypertrophy in H9c2 rat cell line. Vascul Pharmacol. 2013;58:363–73.
Sudheesh AP, Mohan N, Francis N, Laishram RS, Anderson RA. Star-PAP controlled alternative polyadenylation coupled poly(A) tail length regulates protein expression in hypertrophic heart. Nucleic Acids Res. 2019;47:10771–87.
Kumari S, Katare PB, Elancheran R, Nizami HL, Paramesha B, Arava S, Sarma PP, Kumar R, Mahajan D, Kumar Y, et al. Musa balbisiana fruit rich in polyphenols attenuates isoproterenol-induced cardiac hypertrophy in rats via inhibition of inflammation and oxidative stress. Oxid Med Cell Longev. 2020;2020:7147498.
deAlmeida AC, van Oort RJ, Wehrens XH. Transverse aortic constriction in mice. J Vis Exp. 2010;38:e1729.
Cao T, Ni R, Ding W, Ji X, Li L, Liao G, Lu Y, Fan GC, Zhang Z, Peng T. MLKL-mediated necroptosis is a target for cardiac protection in mouse models of type-1 diabetes. Cardiovasc Diabetol. 2022;21:165.
Zheng D, Cao T, Zhang LL, Fan GC, Qiu J, Peng TQ. Targeted inhibition of calpain in mitochondria alleviates oxidative stress-induced myocardial injury. Acta Pharmacol Sin. 2021;42:909–20.
Cao T, Fan S, Zheng D, Wang G, Yu Y, Chen R, Song LS, Fan GC, Zhang Z, Peng T. Increased calpain-1 in mitochondria induces dilated heart failure in mice: role of mitochondrial superoxide anion. Basic Res Cardiol. 2019;114:17.
Perez-Zsolt D, Munoz-Basagoiti J, Rodon J, Elosua-Bayes M, Raich-Regue D, Risco C, Sachse M, Pino M, Gumber S, Paiardini M, et al. SARS-CoV-2 interaction with Siglec-1 mediates trans-infection by dendritic cells. Cell Mol Immunol. 2021;18:2676–8.
Lu Q, Liu J, Zhao S, Gomez Castro MF, Laurent-Rolle M, Dong J, Ran X, Damani-Yokota P, Tang H, Karakousi T, et al. SARS-CoV-2 exacerbates proinflammatory responses in myeloid cells through C-type lectin receptors and Tweety family member 2. Immunity. 2021;54(1304–1319): e1309.
Gao C, Zeng J, Jia N, Stavenhagen K, Matsumoto Y, Zhang H, Li J, Hume AJ, Muhlberger E, van Die I, et al. SARS-CoV-2 spike protein interacts with multiple innate immune receptors. BioRxiv. 2020. https://doi.org/10.1101/2020.07.29.227462.
Furini G, De Carli A, Fonnesu R, Spezia PG, Scebba F, Pistello M, Lai M, Lionetti V. Gene silencing of endothelial von Willebrand factor reduces the susceptibility of human endothelial cells to SARS-CoV-2 infection. FEBS J. 2023;290:4300–15.
Moore KW, de Waal MR, Coffman RL, O’Garra A. Interleukin-10 and the interleukin-10 receptor. Annu Rev Immunol. 2001;19:683–765.
Trisolini L, Gambacorta N, Gorgoglione R, Montaruli M, Laera L, Colella F, Volpicella M, De Grassi A, Pierri CL. FAD/NADH dependent oxidoreductases: from different amino acid sequences to similar protein shapes for playing an ancient function. J Clin Med. 2019;8:2117.
Padavannil A, Ayala-Hernandez MG, Castellanos-Silva EA, Letts JA. The mysterious multitude: structural perspective on the accessory subunits of respiratory complex I. Front Mol Biosci. 2021;8: 798353.
De Grassi A, Lanave C, Saccone C. Evolution of ATP synthase subunit c and cytochrome c gene families in selected Metazoan classes. Gene. 2006;371:224–33.
Knollmann BC. Induced pluripotent stem cell-derived cardiomyocytes: boutique science or valuable arrhythmia model? Circ Res. 2013;112(969–976):discussion 976.
Bezzerides VJ, Caballero A, Wang S, Ai Y, Hylind RJ, Lu F, Heims-Waldron DA, Chambers KD, Zhang D, Abrams DJ, Pu WT. Gene therapy for catecholaminergic polymorphic ventricular tachycardia by inhibition of Ca(2+)/calmodulin-dependent kinase II. Circulation. 2019;140:405–19.
Raman B, Bluemke DA, Luscher TF, Neubauer S. Long COVID: post-acute sequelae of COVID-19 with a cardiovascular focus. Eur Heart J. 2022;43:1157–72.
Galluzzi L, Kepp O, Trojel-Hansen C, Kroemer G. Mitochondrial control of cellular life, stress, and death. Circ Res. 2012;111:1198–207.
Ajaz S, McPhail MJ, Singh KK, Mujib S, Trovato FM, Napoli S, Agarwal K. Mitochondrial metabolic manipulation by SARS-CoV-2 in peripheral blood mononuclear cells of patients with COVID-19. Am J Physiol Cell Physiol. 2021;320:C57–65.
Shen Y, Chen M, Gu W, Wan J, Cheng Z, Shen K, Zhang W, He J, Wang Y, Deng X. The molecular mechanism of cardiac injury in SARS-CoV-2 infection: focus on mitochondrial dysfunction. J Infect Public Health. 2023;16:746–53.
Bonora M, Wieckowski MR, Sinclair DA, Kroemer G, Pinton P, Galluzzi L. Targeting mitochondria for cardiovascular disorders: therapeutic potential and obstacles. Nat Rev Cardiol. 2019;16:33–55.
Schulze PC, Drosatos K, Goldberg IJ. Lipid Use and Misuse by the Heart. Circ Res. 2016;118:1736–51.
Lai L, Leone TC, Keller MP, Martin OJ, Broman AT, Nigro J, Kapoor K, Koves TR, Stevens R, Ilkayeva OR, et al. Energy metabolic reprogramming in the hypertrophied and early stage failing heart: a multisystems approach. Circ Heart Fail. 2014;7:1022–31.
Todisco S, Musio B, Pesce V, Cavalluzzi MM, Petrosillo G, La Piana G, Sgobba MN, Schlosserova N, Cafferati Beltrame L, Di Lorenzo R, et al. Targeting mitochondrial impairment for the treatment of cardiovascular diseases: from hypertension to ischemia-reperfusion injury, searching for new pharmacological targets. Biochem Pharmacol. 2023;208: 115405.
Tragni V, Primiano G, Tummolo A, Cafferati Beltrame L, La Piana G, Sgobba MN, Cavalluzzi MM, Paterno G, Gorgoglione R, Volpicella M, et al. Personalized medicine in mitochondrial health and disease: molecular basis of therapeutic approaches based on nutritional supplements and their analogs. Molecules. 2022;27:3494.
Lopez-Crisosto C, Pennanen C, Vasquez-Trincado C, Morales PE, Bravo-Sagua R, Quest AFG, Chiong M, Lavandero S. Sarcoplasmic reticulum-mitochondria communication in cardiovascular pathophysiology. Nat Rev Cardiol. 2017;14:342–60.
Poggio E, Vallese F, Hartel AJW, Morgenstern TJ, Kanner SA, Rauh O, Giamogante F, Barazzuol L, Shepard KL, Colecraft HM, et al. Perturbation of the host cell Ca(2+) homeostasis and ER-mitochondria contact sites by the SARS-CoV-2 structural proteins E and M. Cell Death Dis. 2023;14:297.
Breitinger U, Farag NS, Sticht H, Breitinger HG. Viroporins: Structure, function, and their role in the life cycle of SARS-CoV-2. Int J Biochem Cell Biol. 2022;145: 106185.
Galluzzi L, Kepp O, Kroemer G. Mitochondrial regulation of cell death: a phylogenetically conserved control. Microb Cell. 2016;3:101–8.
Tiku V, Tan MW, Dikic I. Mitochondrial functions in infection and immunity. Trends Cell Biol. 2020;30:263–75.
Mirali S, Botham A, Voisin V, Xu C, St-Germain J, Sharon D, Hoff FW, Qiu Y, Hurren R, Gronda M, et al. The mitochondrial peptidase, neurolysin, regulates respiratory chain supercomplex formation and is necessary for AML viability. Sci Transl Med. 2020;12:eaaz8264.
Ferro ES, Gewehr MCF, Navon A. Thimet oligopeptidase biochemical and biological significances: past, present, and future directions. Biomolecules. 2020;10:1229.
Makowski L, Chaib M, Rathmell JC. Immunometabolism: from basic mechanisms to translation. Immunol Rev. 2020;295:5–14.
Marchi S, Guilbaud E, Tait SWG, Yamazaki T, Galluzzi L. Mitochondrial control of inflammation. Nat Rev Immunol. 2023;23:159–73.
Ramasamy S, Subbian S. Critical determinants of cytokine storm and type I interferon response in COVID-19 pathogenesis. Clin Microbiol Rev. 2021;34:10–128.
Blanco-Melo D, Nilsson-Payant BE, Liu WC, Uhl S, Hoagland D, Moller R, Jordan TX, Oishi K, Panis M, Sachs D, et al. Imbalanced host response to SARS-CoV-2 drives development of COVID-19. Cell. 2020;181(1036–1045): e1039.
Hadjadj J, Yatim N, Barnabei L, Corneau A, Boussier J, Smith N, Pere H, Charbit B, Bondet V, Chenevier-Gobeaux C, et al. Impaired type I interferon activity and inflammatory responses in severe COVID-19 patients. Science. 2020;369:718–24.
Gedda MR, Danaher P, Shao L, Ongkeko M, Chen L, Dinh A, Thioye Sall M, Reddy OL, Bailey C, Wahba A, et al. Longitudinal transcriptional analysis of peripheral blood leukocytes in COVID-19 convalescent donors. J Transl Med. 2022;20:587.
Cai J, Xu M, Zhang X, Li H. Innate immune signaling in nonalcoholic fatty liver disease and cardiovascular diseases. Annu Rev Pathol. 2019;14:153–84.
Steven S, Frenis K, Oelze M, Kalinovic S, Kuntic M, Bayo Jimenez MT, Vujacic-Mirski K, Helmstadter J, Kroller-Schon S, Munzel T, Daiber A. Vascular inflammation and oxidative stress: major triggers for cardiovascular disease. Oxid Med Cell Longev. 2019;2019:7092151.
Goulopoulou S, McCarthy CG, Webb RC. Toll-like receptors in the vascular system: sensing the dangers within. Pharmacol Rev. 2016;68:142–67.
Finney AC, Stokes KY, Pattillo CB, Orr AW. Integrin signaling in atherosclerosis. Cell Mol Life Sci. 2017;74:2263–82.
Chitu V, Stanley ER. Regulation of embryonic and postnatal development by the CSF-1 receptor. Curr Top Dev Biol. 2017;123:229–75.
Fu Y, Zhang J, Xu L, Zhang H, Ma S, Gao Y, Jiang Y. Developing a novel immune-related seven-gene signature and immune infiltration pattern in patients with COVID-19 and cardiovascular disease. J Cardiovasc Dev Dis. 2022;9:450.
Lawal B, Kuo YC, Rachmawati Sumitra M, Wu ATH, Huang HS. Identification of a novel immune-inflammatory signature of COVID-19 infections, and evaluation of pharmacokinetics and therapeutic potential of RXn-02, a novel small-molecule derivative of quinolone. Comput Biol Med. 2022;148: 105814.
Manik M, Singh RK. Role of toll-like receptors in modulation of cytokine storm signaling in SARS-CoV-2-induced COVID-19. J Med Virol. 2022;94:869–77.
Karki R, Kanneganti TD. Innate immunity, cytokine storm, and inflammatory cell death in COVID-19. J Transl Med. 2022;20:542.
Elshikha AS, Teng XY, Kanda N, Li W, Choi SC, Abboud G, Terrell M, Fredenburg K, Morel L. TLR7 activation accelerates cardiovascular pathology in a mouse model of lupus. Front Immunol. 2022;13: 914468.
Notarbartolo S, Ranzani V, Bandera A, Gruarin P, Bevilacqua V, Putignano AR, Gobbini A, Galeota E, Manara C, Bombaci M, et al. Integrated longitudinal immunophenotypic, transcriptional and repertoire analyses delineate immune responses in COVID-19 patients. Sci Immunol. 2021;6:eabg5021.
Shen Y, Cheng F, Sharma M, Merkulova Y, Raithatha SA, Parkinson LG, Zhao H, Westendorf K, Bohunek L, Bozin T, et al. Granzyme B deficiency protects against angiotensin II-induced cardiac fibrosis. Am J Pathol. 2016;186:87–100.
Chen X, Wang X, Zhang Z, Chen Y, Wang C. Role of IL-9, IL-2RA, and IL-2RB genetic polymorphisms in coronary heart disease. Herz. 2021;46:558–66.
Li J, Ley K. Lymphocyte migration into atherosclerotic plaque. Arterioscler Thromb Vasc Biol. 2015;35:40–9.
Li M, Wang H, Tian L, Pang Z, Yang Q, Huang T, Fan J, Song L, Tong Y, Fan H. COVID-19 vaccine development: milestones, lessons and prospects. Signal Transduct Target Ther. 2022;7:146.
Yuan Y, Jiao B, Qu L, Yang D, Liu R. The development of COVID-19 treatment. Front Immunol. 2023;14:1125246.
Drozdzal S, Rosik J, Lechowicz K, Machaj F, Szostak B, Przybycinski J, Lorzadeh S, Kotfis K, Ghavami S, Los MJ. An update on drugs with therapeutic potential for SARS-CoV-2 (COVID-19) treatment. Drug Resist Updat. 2021;59: 100794.
Desikan R, Padmanabhan P, Kierzek AM, van der Graaf PH. Mechanistic models of COVID-19: insights into disease progression, vaccines, and therapeutics. Int J Antimicrob Agents. 2022;60: 106606.
Zhang Z, Zhang X, Bi K, He Y, Yan W, Yang CS, Zhang J. Potential protective mechanisms of green tea polyphenol EGCG against COVID-19. Trends Food Sci Technol. 2021;114:11–24.
Yang CS, Zhang J. Studies on the prevention of cancer and cardiometabolic diseases by tea: issues on mechanisms, effective doses, and toxicities. J Agric Food Chem. 2019;67:5446–56.
Elizagaray ML, Mazitelli I, Pontoriero A, Baumeister E, Docena G, Raimondi C, Correger E, Rumbo M. Lidocaine reinforces the anti-inflammatory action of dexamethasone on myeloid and epithelial cells activated by inflammatory cytokines or SARS-CoV-2 infection. Biomed J. 2023;46:81–92.
Li Y, Pan H, Duan H, Chen J, Zhu Z, Fan J, Li P, Yang X, Pan W. Double-layered osmotic pump controlled release tablets of actarit: in vitro and in vivo evaluation. Asian J Pharm Sci. 2019;14:340–8.
Deeks ED. Raltegravir once-daily tablet: a review in HIV-1 infection. Drugs. 2017;77:1789–95.
Acknowledgements
We thank the databases and software mentioned above for providing us with data and analysis tools.
Funding
This work was supported by the National Natural Science Foundation of China (No. 92168203), Jiangsu Cardiovascular Medicine Innovation Center (CXZX202210), and Science Foundation of the First Affiliated Hospital of Soochow University (BXQN202223).
Author information
Authors and Affiliations
Contributions
SD and TC conceived, designed, and performed the analysis, and wrote the manuscript. HS, XZ, WG, HL, and LW performed experiments and analyzed data. HS, HH, and YY contributed to data acquisition. YC and FH contributed with analysis tools and reviewed the analysis principles. YC and WY reviewed data and the manuscript. ZS conceptualized the study, supervised the research and revised the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The animal procedure in this study were approved by the Animal Use Subcommittee at Soochow University, China.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Figure S1.
Expression of host proteins predicted to interact with SARS-CoV-2 Spike protein based on structural analysis in the cardiovascular diseases-related GSE84796 dataset. Figure S2. Effect of isoproterenol (ISO) on H9c2 cells. Figure S3. Experimental verification of hub genes expression in isoproterenol induced hiPSC-CMs. Figure S4. Expression of cardiac hypertrophy and fibrosis markers in heart tissues of TAC mice. Table S1. Characteristics of heart tissue samples from heart failure dataset used in this study. Table S2. Primers used in this study. Table S3. Parameters of cardiac functions in two groups of mice.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Dai, S., Cao, T., Shen, H. et al. Landscape of molecular crosstalk between SARS-CoV-2 infection and cardiovascular diseases: emphasis on mitochondrial dysfunction and immune-inflammation. J Transl Med 21, 915 (2023). https://doi.org/10.1186/s12967-023-04787-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12967-023-04787-z