
Abstract
Immunotherapy, including immunostimulation and immunosuppression, has seen significant development in the last 10 years. Immunostimulation has been verified as effective in anti-cancer treatment, while immunosuppression is used in the treatment of autoimmune disease and inflammation. Currently, with the update of newly-invented simplified isolation methods and the findings of potent triggered immune responses, extracellular vesicle-based immunotherapy is very eye-catching. However, the research on three main types of extracellular vesicles, exosomes, microvesicles and apoptotic bodies, needs to be more balanced. These three subtypes share a certain level of similarity, and at the same time, they have their own properties caused by the different methods of biogensis. Herein, we summarized respectively the status of immunotherapy based on each kind of vesicle and discuss the possible involved mechanisms. In conclusion, we highlighted that the effect of the apoptotic body is clear and strong. Apoptotic bodies have an excellent potential in immunosuppressive and anti-inflammatory therapies .
Similar content being viewed by others


Introduction
Immunotherapy is divided into immunostimulation and immunosuppression according to the type of disease. Immunostimulation, also called immunostimulatory therapy, has shown excellent potential in treating cancer [1] and has also been explored in treating some viral infections [1]. Immunostumulation’s representative product is the PD-1 inhibitor to treat tumours. Targeting the suppression of the immune system is the aim of immunosuppressive/ immunomodulatory therapy. Immunomodulation is also widely used in anti-inflammatory treatment. This therapy is effective under several conditions: (i) after organ and/or tissue transplantation (graft-vs-host disease, GvHD); (ii) in autoimmunity; (iii) when it overreacts to allergens.
Extracellular vesicles (EVs) are widely studied. Types of EVs include exosomes, microvesicles (MVs) and apoptotic bodies (ApoBs) [2,3,4,5,6]. All three subtypes have therapeutic potential as they act as important messengers in physiological and pathological conditions. EVs all potentially and purposefully target immune cells to mediate immunotherapy.
As one of the smallest types of EVs, exosomes range approximately from 30 to 150 nm [7,8,9]. Due to their therapeutic properties and delivery potential, exosomes have become an absolute research hotspot in the last decade (Fig. 1). Exosomes are small-sized particles formed during double invagination of the plasma membrane and the generation of intracellular multivesicular bodies (MVBs) wrapping intraluminal vesicles [10,11,12]. After MVB fuses with the plasma membrane, intraluminal vesicles are finally released through exocytosis as exosomes [12] (Fig. 2). Their small size (~ 50 nm) was considered to allow a higher cellular uptake than larger-size EVs in thermodynamic models and several experimental studies [7, 13, 14]. Although, its surface membrane protein CD47 can bind to SIRP-α to block phagocytosis by the immune cells [15, 16]. CD47 exempts the phagocyte system and enables them to target other immunocytes. Especially after modification/engineering, their target capacity can be significantly enhanced. Several studies have enabled exosomes to be involved in the phagocytes system. Artificial CD47 knock-out [17] and CD47/SIRP-α competitive occupancy [18] are two effective methods to allow exosomes to be phagocytosed.

The number of publications about the three types of vesicles in the recent decade. The data was acquired by searching each vesicular name as “topic” in the webofscience.com. This figure was generated by GraphPad Software (9.0.0)

Biogenesis of three kinds of vesicles. Exosomes form by undergoing intracellular multivesicular bodies pathway. Microvesicles (MVs) are shed by outward blebbing of the plasma membrane. Apoptotic bodies (ApoBs) are produced by apoptotic cells. The process begins with condensation of the nuclear chromatin, followed by membrane blebbing, progressing to the disintegration of the cellular content into distinct membrane-enclosed vesicles
Microvesicles (MVs) are vesicles (0.1–1.0 μm) shed by outward blebbing of the plasma membrane [26] (Fig. 2). MVs shared similar properties with exosomes. MVs and exosomes are often merged and referred to as small EV (sEV). Both MVs and exosomes are multi-targeting. MVs and exosomes can target multiple cells depending on their parental cells. MVs also express vesicular CD47 [34, 35], they are speculated to escape phagocytosis in vivo and have a prolonged circulation time.
Depending on the different cell sources, MVs and exosomes can promote immunostimulation or immunosuppression. For example, MVs from tumours can present tumour antigens to the antigen-presenting cells (APCs) to mediate immunostimulation [36, 37], while mesenchymal stromal cell (MSC)-derived exosomes are immunomodulatory. MSC-exosomes have been shown to immunomodulate in many autoimmune diseases including, GvHD [38], rheumatoid arthritis [39] and multiple sclerosis [40].
Compared to exosomes and microvesicles, the enthusiasm to study ApoBs is lower (Fig. 1). However ApoBs have very similar properties to exosomes except for their larger size (50–5000 nm) [28]. They are produced by apoptotic cells. Apoptosis begins with the condensation of the nuclear chromatin, followed by membrane blebbing, progressing to the disintegration of the cellular content into distinct membrane-enclosed vesicles termed ApoBs or apoptosomes [29, 32] (Fig. 2). Like MVs and exosomes, ApoBs also strongly affect recipient cells, which are professional phagocytes and nonprofessional neighbouring cells [41]. But unlike MVs and exosomes, ApoBs’ target cells are less variable. Among all the recipient cells, the main target cells are macrophages, dendritic cells (DCs) and other neighbouring cells. Both macrophages and DCs play an important role in modulating the immune system. After phagocytosing ApoBs, macrophages are inclined to polarize to anti-inflammatory M2 phenotype [42] while, tumour-derived ApoBs induce DCs to pro-inflammatory mature phenotype [43].
Overall, exosomes, MVs and ApoBs have a similar lipid bilayer membrane and carry a gene andprotein cargo. Also, all of them are released by cells but through different pathways. They all can deliver their cargo or loaded drug to recipient cells and elicit a therapeutic effect. But in recent years, the enthusiasm to study ApoBs has been low despite their potent effect on immune cells. In this review, we stated the status of immunotherapy meditated by these three vesicles and with a specific interest in the the effect of ApoBs. The possible involved mechanism which causes the difference was also analyzed.
Comparison of immunotherapy
Immunotherapy mediated by exosomes
Exosomes’ recipient cells vary depending on the derivation. Homing effect to target their parental cells, ligand-receptor binding-mediated targeting and macrophage-dependent clearance are three major theories of exosome targeting. (1) The homing effect refers to the exosomes ability to home to their cells type of origin, for example, tumour-exosomes target and alter tumour cell in tumour mircoenviroment [44, 45]. (2) Ligand-receptor binding also called active targeting. Active targeting is where a targeting moiety, such as a ligand or an antibody, is introduced onto the exosomes to target tissues with specific upregulated proteins in comparison to the surrounding cells [46,47,48]. (3) Macrophage clearance is that exosomes are primarily cleared via phagocytosis and endocytosis by macrophages in the mononuclear phagocyte system (MPS) [49, 50]. These three targeting methods are compatible, and multiple mechanisms are often used together to design exosome treatment strategies.
Immunostimulation mediated by exosomes
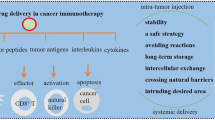
The most typical immunostimulation model induced by exosomes is tumour immunotherapy elicited by tumour-derived exosomes. Regarded as a very potential tumour vaccine, exosomes carry sufficient antigens from their parent cells. After being presented by APCs or directly recognized by T-cell receptors [51], an immunostimulatory cascade reaction is initiated and thus leads to a beneficial pro-inflammatory anti-tumour effect [52].
However, the binding of exosomal surface CD47 and SIRP-α causes a “don’t eat me” signal [15, 53], enabling exosome’ immune escape from MPS. The low-efficient phagocytosis, resulting in less antigen-presenting, is a challenge of tumoral exosome immunostimulatory therapy. Through the blocking of CD47, the phagocytosis of exosomes by MPS increases but whether this loss of CD47 results in a stronger immunostimulatory reaction remains unknown.
To overcome this low-efficient phagocytosis obstacle, there are three main strategies.
-
(1)
In vitro incubating antigen-carried exosomes with DCs. It is verified that DCs are able to uptake exosomes in a simpler in vitro environment than in more complex in vivo environments [54]. In this paper, breast cancer cell E0771-derived exosomes were reported to contain immunomodulatory molecules such as HSP70, HSP90, MHC I and MHC II. After incubating with exosomes in vitro, mice dendritic cell DC2.4 cells increase the proliferation and migration abilities, accompanied by the upregulation of CD40 (a marker of mature DC). These DCs-treated tumour-bearing mice exhibited decreased tumour growth and sufficient T-cell infiltration [54]. Importantly, in another research paper, exosome-incubated DCs can induce stronger stimulatory reactions and anti-tumour effects than tumour lysate-incubated DCs [55], demonstrating the sufficiency and high efficiency of antigens carried by exosomes.
-
(2)
Using dying tumour cell-derived exosomes. DCs fail to recognize live tumour cells and cease to become activated, but DCs can be activated by antigens from apoptotic tumour cells. Thus, Zhou et al. prepared a dying tumour cell-derived exosomes to stimulate the immune system [56]. Although they did not quantify the apoptotic exosomal CD47, the uptake efficiency of apoptotic vesicles was very high, and the immunostimulation was also successfully triggered. The relevant mechanism of apoptotic vesicles likely involved the exposed phosphatidylserine, similar to ApoBs. This mechanism will be discussed in a later chapter.
-
(3)
Antigens, adjuvant or other therapeutic agent co-delivery. Generally, this co-delivery method is to strengthen immunostimulation. The research above using apoptotic cell-derived exosomes [56] also involves adjuvant and siRNA to enhance the therapeutic effect. Zhou et al. used MART-1 to expand T-cell-related responses and CCL22 siRNA to impede CCR4/CCL22 axis between Tregs and DCs. Commonly used adjuvant includes CpG DNA [57] and α-galactosylceramide [55].
Regarding, CD47-targeting strategy, exosomes can be utilized to block tumoral CD47 binding with MPS SIRPα, and thus leading to improved phagocytosis. This immunostimulation was caused by exosomes indirectly because exosomes are not regarded as the presented antigen. For example, by transfecting SIRPα plasmid DNA, SIRPα-expressed exosomes display an excellent affinity to CD47-naturally-overexpressed cancer HT29 cells. Due to the binding of tumoral CD47-exosomal SIRPα, macrophages cannot recognize tumoral CD47 “don’t eat me” signals and phagocytose more tumour cells. This will also enable intensive T-cell infiltration and thus reduce the volume of the tumour in vivo [16].
Except for tumour-derived cells/exosomes, M1 macrophage-derived exosomes are studied to enhance immunostimulation as M1 is a commonly-considered pro-inflammatory cell phenotype. Mice M1 macrophage cell RAW264.7-derived exosomes are reported to be able to increase M0 RAW264.7 releasing pro-inflammatory cytokines, while M2 RAW264.7-derived exosomes cannot. Exomsome treated M0 RAW264.7 secreted cytokines induce murine breast cancer cells 4T1 apoptosis [58].
Immunosupression mediated by exosomes
The previous paragraph introduced a lot of tumour-derived exosomes that cause immune stimulation. In fact, most of the tumour-derived exosomes naturally induce immunosuppression functions and are a very important component of the immunosuppressive tumour microenvironment [59,60,61]. These exosomes, especially PD-L1-expressing tumour exosomes, are produced in autologous tumour tissue and benefit tumour progression [62,63,64]. Autologous tumoral and PD-L1-carried exosomes contribute to immunosuppression and impede anti-PD-1 therapy [65] via inducing tumour-specific CD8 + T cell exhaustion [66] and suppression [67] and thus reducing immune infiltration. Blocking these immunosuppressive exosomes is a good strategy to overcome the low response of PD-L1 therapy. Using Macitentan to inhibit these autologous tumoral EVs secretion, the binding to PD-1 and PD-L1 decreases and thus enhancing the CD8 + T cell-mediated tumour killing and anti-PD-L1 therapy [68].
MSC have antigen-presenting properties [69]. This property is relevant to immunomodulation and immune tolerance [70,71,72]. Effecting similarly with their parental cells, MSC-exosomes are also reported to involve antigen-presenting pathways, which can induce more Tregs in the presence of DCs than absence [73]. This demonstrated that MSC-exosomes might present the relevant antigens to DCs, but not directly affect T cells. However, MSC-exosomes antigen presenting mechanism of action is currently lacking explanation. Despite the lack of explanation, the immunomodulatory effect of MSC-exosomes is widely verified. They can expand Tregs [73], polarize M2 macrophage [74] and inhibit T cell proliferation [75]. MSC-exosomes have potential in various autoimmunity diseases, including graft-versus-host disease [38, 76], rheumatoid arthritis [39, 77] and uveitis [78, 79].
Immunotherapy mediated by MVs
MVs function similarly to exosomes. These two vesicles are often amalgamated and referred to as small EVs. Some studies compared the proteomics between exosomes and MVs [80, 81] to reveal the difference. It is likely that MVs carry more kinds of proteins than exosomes, possibly due to their larger size [82, 83]. MVs are more similar to their parental cells with more comparable protein categories than exosomes [83]. Although there are differences between these two particles, the conclusion is that both can reflect the state and function of their parental cells. No studies have shown a significant difference in function between these two particles. Additionally, MVs also express CD47 [34, 35] to enable extended circulation times and multi-targeting properties. In this review, we speculate MV and exosomes function similarly.
In the case of similar effects, tumour and MSC-derived MVs were also widely studied. Like their exosomes, tumour-derived MVs can induce mature DCs in vitro and cause an anti-tumour immunostimulatory response [37]. MSC-derived MVs are immunomodulatory and have demonstrated the ability to modulate inflammatory responses [84, 85]. Apart from tumour and MSC-MVs other immunotherapies of different MVs are also interesting. In the aspect of immunostimulation, activated CD4 + effector cells are immunostimulatory. Their MVs target microvascular endothelial cells. Proteomic analysis showed these inflammation-related cell-derived MVs were enriched with proteins involved in pro-inflammatory processes. CD4 + MVs have been shown to inhibit endothelial wound healing and induce endothelial cell apoptosis [86]. The activated T cell-derived MVs are also proven to deliver gene signal miR-4443 to the mast cell, leading to their activation in the T cell-mediated inflammation [87]. These facts further demonstrate MVs function similarly to their parental cells.
Immunotherapy mediated by ApoBs
Unlike the multi-targeting of exosomes, ApoBs are eliminated by two main kinds of cells. The first is a “professional phagocyte” such as a macrophage and immature DC. The other is “nonprofessional neighbouring cells” such as the neighbouring tumour cells. More importantly, the lack of CD47 enables rapid clearance and is fewer off-target effects. Therefore, compared with EVs, the most potent advantage of ApoBs is a clear target cell (Fig. 3).

Three major pathways to clear apoptotic bodies. The clearance via macrophages and dendritic cells (DCs) can be used in immunotherapy
Anti-inflammatory and immunosuppressive: phagocyted by macrophages and inducing M2 phenotype
Macrophages are a category of white blood cell that engulfs and digests substances which do not have proteins specific to healthy cells on their surface. Macrophages are crucial in the initiation, maintenance, and resolution of inflammation. It is macrophages that eliminate ApoBs.
Furthermore, macrophages can induce host defense and inflammatory response or suppress these functions via phenotyping conversion [88,89,90,91]. The authors speculated that ApoBs or apoptotic cells contained “dead” and “injured” signals. The macrophages phagocyte ApoBs and initiate a negative feedback loop, in other words, marcophages differentiate into anti-inflammatory/ regeneration-facilitating M2 phenotype. Among all the ApoBs in mediating M2 macrophage, MSC-derived ApopBs are the most studied.
Recently, it has been reported that MSC undergo apoptosis before eliciting their functioning in vivo [92]. Then apoptotic MSCs and their efferocytosis-induced inflammatory pathways in alveolar macrophages mediate immunomodulation and reduce disease severity of autoimmunity [93]. The immunomodulatory potency of apoptotic MSCs is even higher than alive MSCs [94]. These findings likely reveal that apoptosis is the most immunomodulatory status of MSC. The eventual outcome of apoptosis is ApoBs production. This may predict the strong immunomodulation of MSC-derived ApoBs. In other words, MSC-ApoBs have the potential to be a more direct therapeutic agent than MSC itself. In addition, ApoBs are more in line with the concept of cell-free therapy, its immunogenicity is lower than MSC in theory. In all, MSC-ApoBs deserve a greater focus, equal to that of other EVs.
There have been some studies focusing on the immunomodulatory property of MSC-derived ApoBs via the mediation of macrophages. Liu et al. verified that MSC-ApoBs facilitate cutaneous wound healing by polarizing M2 macrophages [42]. Also, to induce M2 phenotype, Zheng et al. utilized MSC-ApoBs (apoptotic vesicles) to treat type 2 diabetes. They also showed efferocytosis of ApoBs can induce macrophages to reprogram transcriptionally in vitro and inhibit the infiltration and activation of diseased liver macrophages in vivo [95].
Pro-inflammatory: phagocyted by DCs
As mentioned above, macrophage phagocytosing results in an anti-inflammation response. This responses can switch to a pro-inflammatory status when the phagocytic cells become DCs. It has been widely reported in the establishment of apoptotic tumour cell-phagocytosed DCs for immunotherapy [96,97,98,99,100]. DCs that acquired antigens from apoptotic tumour cells are able to induce major histocompatibility complex (MHC) class I-restricted cytotoxic T cells and anti-tumor immunity [98]. This work inspired us to examine the role of ApoBs-phagocytosed DCs.
DCs, which load myeloma cell-derived ApoBs, can induce myeloma-specific T cells, leading to the activation of myeloma-reactive allogeneic T lymphocytes that produce IFN-γ [101]. Meanwhile, allogenic DCs from healthy donors, pulsed with leukemic cell-derived ApoBs, is a feasible and safe treatment for chronic lymphocytic leukaemia patients [43]. More importantly, compared with the lysate and the RNA from tumour cells, the ApoBs can induce a stronger autologous T-cell response in chronic lymphocytic leukaemia. In this clinical trial, ApoB-loaded DCs induce stronger T-cell responses with higher expression of IL-2 and IFN-γ [102]. This demonstrates ApoBs can induce better immunostimulatory DCs than tumour lysate. However, these ApoB-activated DC studies are slightly dated and have been completed more than ten years ago. Their method and technology to characterize ApoBs are limited. This is a clear limitation of these studies.
Compared to the macrophage-ApoBs strategy, the DC-involved ApoB study preferentially incubates ApoBs with DCs in vitro before injecting DC in vivo, while the ApoBs-macrophage strategy enables direct in-vivo fusion. We speculated this may account for (1) macrophage is the major population of tissue-resident mononuclear phagocytes [103]; (2) the increased phagocytosis capacity of macrophages [104]; (3) ApoBs are inclined to be phagocytosed by macrophages because of exposed phosphatidylserine (PS) [105]. If ApoBs can be accurately delivered to DC, infusing them in vitro prior to injection is unnecessary and the immunosuppression of tumour microenvironment will be greatly improved.
Phagocyted by neighbouring cells
The third way of phagocytosing ApoBs is through neighbouring cells. If the professional phagocyte is not abundant at the apoptosis site, nonprofessional neighbours usually clear ApoBs during development [106]. However, this phagocytosis does not directly connect to the immune response. In this neighbouring cell-phagocytosing mechanism, ApoBs mainly play a role in promoting cell growth and proliferation [107,108,109,110]. It is possible that macrophages and DCs can also grow or divide rapidly after phagocytosis of ApoBs.
Modifiable (engineered) properties
Because exosomes, MVs and ApoBs all have a similar lipid bilayer membrane and a loading-feasible core, the modifiable property is shared by all these particles. In the above paragraph, we discussed some modified vesicles that illustrate a strengthened immunotherapy function. In brief, this modification can be separated into vesicle-core cargo loading, membrane modification and membrane fusion engineering (Fig. 4).

Commonly-used methods to modify the vesicles
Firstly, natural loading is the most commonly utilized way to enhance the therapeutic efficacy on the basis that vesicles already load the natural therapeutical genes and proteins. Artificially loaded cargo implies altering the cargo by a variety of non-organic procedures and includes alterations to the genes and proteins. For example, 4T1 tumour cell-derived exosomes loaded miR-142, miR-155 or Let-7i respectively by electroporation [111]. Each kind of microRNA-loading enhances the effect on DC maturation and thus mediates an immunostimulatory response. On the contrary, monocytic THP-1 cell-derived exosomes loading miR-146a or miR494 exhibit an enhanced inhibitory effect on DC maturation [112]. These two studies sufficiently demonstrate the importance of vesicle cargo. These mircoRNA’s immunostimulatory or immunosuppressive effect needs to be verified in advance, and loading into exosomes amplifies their effect. As for protein delivery, ovalbumin is often loaded in the nanoparticle to mediate allergen-specific tolerance in the ovalbumin-induced allergic inflammation model. In an ovalbumin-caused allergic rhinitis mice model, exosomes play an important role as a messenger. Exosomes simultaneously deliver allergens (ovalbumin) and CpG DNA, an adjuvant that can induce a Th1 immune response, for the treatment of allergic rhinitis. Ovalbumin was expressed in the exosomes by transfecting ovalbumin plasmid DNA into cells. Ovalbumin-loaded exosomes were delivered to the mice’s nasopharynx-associated lymphoid tissue and were primarily absorbed by the DCs via intranasal administration. Intranasally administering ovalbumin-loaded exosomes increased ovalbumin-specific IgG antibody titers in vivo thus ameliorated the disease [113].
Beside genes and proteins, chemical drugs are also very popular to load into the vesicle. Due to their small molecular size, they are easy to load into EVs. For example, to reduce the associated multiple serious adverse effects of systematic dexamethasone (DEX) therapy and achieve an accurate delivery to inflamed kidney, DEX was encapsulated into macrophage-derived MVs, because macrophage-derived EV can interact with inflamed endothelium through exosomal adhesion molecules. Macrophage-derived MVs deliver DEX into the kidney and suppress renal fibrosis and inflammation without glucocorticoid adverse effects [114].
Secondly, membrane modification usually conjugates proteins or adaptors on the vesicle membrane. The conjugated protein (adaptor) has a high affinity to the specific protein. and it lead to an accurate delivery. For example, glioblastoma EVs, modified with a high-affinity ligand LewisY by insertion, can target DC-specific intercellular adhesion molecule-3-grabbing non-integrin. This therfore potentiates EVs as anti-cancer immunotherapy [115].
In terms of membrane fusion, liposome membrane is often used to incorporate with vesicular membrane because of they share a similar bilayer structure. Liposome membranes are commonly used to enhance further the modifiable property of natural vesicles [116]. For example, Kang et al. fused liposomes with EVs to form hybrid vesicles. They further extrude these hybrid vesicles with superparamagnetic ferroferric oxide nanoparticles to achieve magnetism and then insert 1,2-distearoyl-sn-glycero-3-phosphoethanolamine-N-[dibenzocyclooctyl(polyethylene glycol) (DSPE-PEG-DBCO).The DBCO-combined nanoparticle can capture circulating melanoma cells by azide-DBCO recognition. Than the captured melanoma cells can be enriched by magnetism [117]. Generally, the EV membrane in this research plays a role in camouflage to escape the recognition by MPS. And liposome fusion is used to further conferred magnetism and lipid insertion. Seldom can EVs be modified complexly and directly like this.
Involved mechanisms causing macrophagic post-phagocytic anti-inflammation of ApoBs
As demonstrated above, compared with the multi-target properties of MVs and exosomes, ApoBs’ target is much simpler, which tends to be uptake by the phagocyte system. This review summarized three main involved mechanisms of the target tendency.
Different size: it is possible that larger ApoBs are more easily to be phagocyted by macrophages
Exosomes’ size is controversial. For decades, there has not been any accurate range for them, which is mainly because of the different methods for isolating and determining their size. It is now widely supported that exosomes are the smallest population of EVs. The size is approximately 30–150 nm [6, 9].
In this review, we exemplify liposomes, an analogy with EVs, to demonstrate the size-dependent property of EVs. Nowadays, on the one hand, direct evidence of EVs’ size-related superiority is lacking evidence. Liposomes and EVs both have a phospholipid bilayer membrane structure [118]. They were usually compared in functions.
The small size is of advantage. First of all, a smaller size signifies high oral bioavailability. (Although there is little to no oral EV immunotherapy, milk-derived EV has been studied for oral administration [119].) Ong et al. [120] used griseofulvin as a model drug encapsulated by different sizes of liposomes. Smaller liposomes’ (≤ 400 nm) bioavailability was higher by approximately three times compared to larger liposomes (≥ 400 nm). Meanwhile, the smaller size also signifies improved stability, Farooq et al. [121] modified liposomes with D-α-tocopheryl polyethylene glycol 1000 succinate (TPGS) to generate TPGS-liposomes of smaller sizes. As a result, after 7 days at 4 °C, the size increment of the TPGS-liposome was less than the common liposome. And after 28 days, the modified smaller liposome still could keep higher encapsulation efficiency than the large more, common liposome.
Compared to exosomes, ApoBs have a wider range, which spans from 50 to 1000 nm. It is mainly because ApoBsares lysed from apoptotic cells. So its size is uneven. According to the current literature most of ApoBs are about 1 μm [30]. The Large size may represent targeting macrophages because phagocytosis is regarded as the uptake of particles larger than 0.5 μm [122]. This theory was also proven in recent years. For example, 1000 nm-liposomes could deliver the drug to rat alveolar macrophages better than smaller liposomes [123]. Only liposomes larger than 600 nm can lead to mononuclear phagocytes secreting IL-2 to induce the Th1 immune response [124].
Different surface molecules: ApoBs have “eat-me” signatures
Apoptotic cells and ApoBs are inclined to be phagocyted by macrophages. They can be recognized by a variety of receptors on the surface of macrophages that can bind to apoptotic surface ligands and phagocytosis is initiated. Apoptotic cell surfaces are characterized by decreased “don’t eat me” molecules such as CD47 [125, 126] and CD31 [127,128,129], and overexpressed “eat-me” signals, such as cell-surface calreticulin and exposed phosphatidylserine (Table 1; Fig. 5). These alterations trigger phagocytosis via macrophages, which then drives polarization to M2 phenotypes and anti-inflammatory signalling (Table 2).

The molecules involved in the phagocytosis of ABs by macrophages
Among these signals, the exposed PS is the most widely-studied “eat-me” signal [94]. When apoptosis occurs, PS will move from the inner leaflet of the plasma membrane to the outer leaflet. By binding to the surface of phagocytes, after phagocyte recognition and engulfment, anti-inflammatory signaling is triggered within these phagocytes.
By utilizing PS-mediated “eat-me” signal, there are several ApoB-inspired nanoparticles prepared: (1) Utilizing macrophage’s affinity to PS, Liu et al. [137] synthesized ApoB-mimicking nanoparticles. This nanoparticle could externalize its inner PS triggered by overexpressed matrix metalloproteinase 2 (MMP2) in the tumour site. Once phagocytosed by macrophages, it releases cytotoxic drugs to kill the macrophages and then damage the tumour microenvironment. (2) Using PS, Kraynak et al. [138] mimicked ApoBs by presenting it in the context of a generic stromal cell membrane from 3T3 fibroblasts. The PS-supplemented particle is anti-inflammatory without the use of any other drugs. Moreover, they verified PS incorporation not only improves relative uptake by macrophages but also polarizes the marcophages to their M2 phenotype.
Aside from for PS, calreticulin (CRT), localized normally in the endoplasmic reticulum lumen, is also transferred to the outer cell membrane where, along with PS, facilitates phagocytosis [139].
The possible essence of phagocyted ApoBs: anti-inflammation
As mentioned above, EVs play a similar role to their parental cells. In this situation, ApoBs to some degree, function more similarly to their apoptotic parental cells rather than live cells. Apoptotic cells in vivo are more on the anti-inflammatory side. Apoptosis, which occurs every day, is regarded as an important way to maintain homeostasis [140, 141]. Apoptosis is also known as a significant death pathway and can trigger new cell development. Contrary to apoptosis, histiocytosis is characterized as pro-inflammatory [142,143,144,145].
In the above chapter, DCs phagocyte ApoBs and then trigger the immunostimulatory response. However, this reaction needs to be intervened in vitro. In other words, naturally occurring apoptosis and phagocytosis triggers anti-inflammation responses. The phagocytosis process of apoptotic material also promotes intrinsic mechanisms such as tissue growth and remodeling, regeneration and resolution of injury and inflammation.
In terms of the apoptosis-involved anti-inflammatory mechanism, at first, apoptosis, especially caspase-dependent apoptosis, is an immunologically silent form of cell death [146]. Caspases regulates inflammation by acting on two opposing functions. By catalyzing pro-inflammatory cytokine production, “inflammatory” caspases trigger inflammation [147]. On the contrary, “apoptotic” caspases safeguard against the triggering of inflammation by imposing a cell-death form that withholds the release of alarmins by dying cells and dictates the generation of anti-inflammatory mediators [148]. A recent study also demonstrated the inducible caspase-9-mediated apoptotic MSC exhibited stronger immunosuppressive properties than conventional MSC in vitro [149]. Besides, anti-inflammatory caspase, exposed-PS, a typical signal on the surface of the apoptotic cells, is a global immunosuppressive [150] and anti-inflammatory [151] molecule. PS-dependent ingestion of apoptotic cells promotes macrophage-secreting TGF-β1 and the resolution of inflammation [152, 153]. Also, in tumours, PS released from tumour apoptotic cells polarizes M2-like macrophage via the PSR-STAT3-JMJD3 axis [135]. Based on this strong polarized effect by PS, in recent years, there have been studies using PS liposomes to induce the M2 macrophage phenotype [154,155,156].
In addition, the post-phagocytosis mechanism of the apoptotic cells has also been summarized as (1) Nuclear receptors actively inhibit the formation of pro-inflammatory cytokines; and (2) Macrophages respond to the uptake of apoptotic cells/ ApoBs by releasing anti-inflammatory cytokines [146].
Conclusion
To conclude exosomes, MVs and ApoBs have similar structures and modifiable properties. The effect of exosomes and MVs vary more, ranging from immunostimulation to immunosuppression, depending on the parental cell. But ApoBs in vivo mainly exert immunosuppressive functions. It is very clear that ApoBs target professional and non-professional phagocytes. Based on their immunosuppressive and anti-inflammatory properties, ApoBs are likely to have big potential in treating autoimmunity and inflammation.
Abbreviations
- ApoB:
-
Apoptotic body
- APC:
-
Antigen-presenting cell
- CRT:
-
Calreticulin
- EV:
-
Extracellular vesicle
- DC:
-
Dendritic cell
- DEX:
-
Dexamethasone
- GVHD:
-
Graft-vs-host disease
- MMP2:
-
Matrix metalloproteinase 2
- MHC:
-
Major histocompatibility complex
- MSC:
-
Mesenchymal stromal cell
- MV:
-
Microvesicle
- MPS:
-
Mononuclear phagocyte system
- MVB:
-
Multivesicular body
- PS:
-
Phosphatidylserine
References
Hegde NR, et al. Immunotherapy of viral infections. Immunotherapy. 2009;1(4):691–711. https://doi.org/10.2217/imt.09.26.
Xie M, et al. Immunoregulatory effects of stem cell-derived extracellular vesicles on immune cells. Front Immunol. 2020. https://doi.org/10.3389/fimmu.2020.00013.
Debs S, et al. Interplay of extracellular vesicles and other players in cerebral malaria pathogenesis. Biochim Biophys Acta-General Subj. 2019;1863(2):325–31. https://doi.org/10.1016/j.bbagen.2018.10.012.
Wu KR, et al. Extracellular vesicles as emerging targets in cancer: recent development from bench to bedside. Biochim Biophys Acta-Rev Cancer. 2017;1868(2):538–63. https://doi.org/10.1016/j.bbcan.2017.10.001.
Sun HY, et al. Extracellular vesicles in the development of cancer therapeutics. Int J Mol Sci. 2020. https://doi.org/10.3390/ijms21176097.
Thery C, et al. Minimal information for studies of extracellular vesicles 2018 (MISEV2018): a position statement of the International Society for Extracellular vesicles and update of the MISEV2014 guidelines. J Extracell Vesicles. 2018;7(1):1535750. https://doi.org/10.1080/20013078.2018.1535750.
Caponnetto F, et al. Size-dependent cellular uptake of exosomes. Nanomedicine. 2017;13(3):1011–20. https://doi.org/10.1016/j.nano.2016.12.009.
Hoshino A, et al. Extracellular vesicle and particle biomarkers define multiple human cancers. Cell. 2020;182(4):1044. https://doi.org/10.1016/j.cell.2020.07.009.
Sidhom K, Obi PO, Saleem A. A review of exosomal isolation methods: is size exclusion chromatography the best option? Int J Mol Sci. 2020;21(18): 6466. https://doi.org/10.3390/ijms21186466.
Qiu P, et al. Exosome: the regulator of the immune system in sepsis. Front Pharmacol. 2021;12:12. https://doi.org/10.3389/fphar.2021.671164.
Villarroya-Beltri C, et al. ISGylation controls exosome secretion by promoting lysosomal degradation of MVB proteins. Nat Commun. 2016;7:7. https://doi.org/10.1038/ncomms13588.
Perrin P, et al. Retrofusion of intralumenal MVB membranes parallels viral infection and coexists with exosome release. Curr Biol. 2021;31(17):3884. https://doi.org/10.1016/j.cub.2021.06.022.
Hoshyar N, et al. The effect of nanoparticle size on in vivo pharmacokinetics and cellular interaction. Nanomedicine. 2016;11(6):673–92. https://doi.org/10.2217/nnm.16.5.
Yeh YT, et al. Rapid size-based isolation of extracellular vesicles by three-dimensional carbon nanotube arrays. ACS Appl Mater Interfaces. 2020;12(11):13134–9. https://doi.org/10.1021/acsami.9b20990.
Chao MP, Weissman IL, Majeti R. The CD47-SIRPalpha pathway in cancer immune evasion and potential therapeutic implications. Curr Opin Immunol. 2012;24(2):225–32. https://doi.org/10.1016/j.coi.2012.01.010.
Koh E, et al. Exosome-SIRPalpha, a CD47 blockade increases cancer cell phagocytosis. Biomaterials. 2017;121:121–9. https://doi.org/10.1016/j.biomaterials.2017.01.004.
Kamerkar S, et al. Exosomes facilitate therapeutic targeting of oncogenic KRAS in pancreatic cancer. Nature. 2017;546(7659):498–503. https://doi.org/10.1038/nature22341.
Jiang ZX, et al. Targeting CD47 for cancer immunotherapy. J Hematol Oncol. 2021. https://doi.org/10.1186/s13045-021-01197-w.
Tschuschke M, et al. Inclusion biogenesis, methods of isolation and clinical application of human cellular exosomes. J Clin Med. 2020;9(2): 436. https://doi.org/10.3390/jcm9020436.
Crivelli SM, et al. Function of ceramide transfer protein for biogenesis and sphingolipid composition of extracellular vesicles. J Extracell Vesicles. 2022. https://doi.org/10.1002/jev2.12233.
van Niel G, et al. The tetraspanin CD63 regulates ESCRT-Independent and -dependent endosomal sorting during melanogenesis. Dev Cell. 2011;21(4):708–21. https://doi.org/10.1016/j.devcel.2011.08.019.
Suarez H, et al. CD9 inhibition reveals a functional connection of extracellular vesicle secretion with mitophagy in melanoma cells. J Extracell Vesicles. 2021. https://doi.org/10.1002/jev2.12082.
Crenshaw BJ, et al. Alcohol modulates the biogenesis and composition of microglia-derived exosomes. Biology-Basel. 2019. https://doi.org/10.3390/biology8020025.
Jia XN, et al. The role of viral proteins in the regulation of exosomes biogenesis. Front Cell Infect Microbiol. 2021. https://doi.org/10.3389/fcimb.2021.671625.
Li SP, et al. Exosomal cargo-loading and synthetic exosome-mimics as potential therapeutic tools. Acta Pharmacol Sin. 2018;39(4):542–51. https://doi.org/10.1038/aps.2017.178.
Stahl AL, et al. Exosomes and microvesicles in normal physiology, pathophysiology, and renal diseases. Pediatr Nephrol. 2019;34(1):11–30. https://doi.org/10.1007/s00467-017-3816-z.
Teng F, Fussenegger M. Shedding light on extracellular vesicle biogenesis and bioengineering. Adv Sci (Weinh). 2020;8(1):2003505. https://doi.org/10.1002/advs.202003505.
Kakarla R, et al. Apoptotic cell-derived exosomes: messages from dying cells. Exp Mol Mede. 2020;52(1):1–6. https://doi.org/10.1038/s12276-019-0362-8.
Battistelli M, Falcieri E. Apoptotic bodies: particular extracellular vesicles involved in intercellular communication. Biology (Basel). 2020. https://doi.org/10.3390/biology9010021.
Serrano-Heras G, et al. Isolation and quantification of blood apoptotic bodies, a non-invasive tool to evaluate apoptosis in patients with ischemic stroke and neurodegenerative diseases. Biol Proced Online. 2020. https://doi.org/10.1186/s12575-020-00130-8.
Poon IKH, et al. Moving beyond size and phosphatidylserine exposure: evidence for a diversity of apoptotic cell-derived extracellular vesicles in vitro. J Extracell Vesicles. 2019;8(1):1608786. https://doi.org/10.1080/20013078.2019.1608786.
Akers JC, et al. Biogenesis of extracellular vesicles (EV): exosomes, microvesicles, retrovirus-like vesicles, and apoptotic bodies. J Neurooncol. 2013;113(1):1–11. https://doi.org/10.1007/s11060-013-1084-8.
Jiang L, et al. Determining the contents and cell origins of apoptotic bodies by flow cytometry. Sci Rep. 2017;7:7. https://doi.org/10.1038/s41598-017-14305-z.
Kim HS, et al. Proteomic analysis of microvesicles derived from human mesenchymal stem cells. J Proteome Res. 2012;11(2):839–49. https://doi.org/10.1021/pr200682z.
Stachurska A, et al. Selected CD molecules and the phagocytosis of microvesicles released from erythrocytes ex vivo. Vox Sang. 2019;114(6):576–87. https://doi.org/10.1111/vox.12819.
Battisti F, et al. Tumor-derived microvesicles modulate antigen cross-processing via reactive oxygen species-mediated alkalinization of phagosomal compartment in dendritic cells. Front Immunol. 2017;8:8. https://doi.org/10.3389/fimmu.2017.01179.
Dionisi M, et al. Tumor-derived microvesicles enhance cross-processing ability of clinical Grade dendritic cells. Front Immunol. 2018;9:9. https://doi.org/10.3389/fimmu.2018.02481.
Li KL, et al. Exosomes released from human bone marrow-derived mesenchymal stem cell attenuate acute graft-versus-host disease after allogeneic hematopoietic stem cell transplantation in mice. Front Cell Dev Biol. 2021. https://doi.org/10.3389/fcell.2021.617589.
Tian XH, et al. Gingival mesenchymal stem cell-derived exosomes are immunosuppressive in preventing collagen-induced arthritis. J Cell Mol Med. 2022;26(3):693–708. https://doi.org/10.1111/jcmm.17086.
Riazifar M, et al. Stem cell-derived exosomes as nanotherapeutics for autoimmune and neurodegenerative disorders. ACS Nano. 2019;13(6):6670–88. https://doi.org/10.1021/acsnano.9b01004.
Arandjelovic S, Ravichandran KS. Phagocytosis of apoptotic cells in homeostasis. Nat Immunol. 2015;16(9):907–17. https://doi.org/10.1038/ni.3253.
Liu J, et al. Apoptotic bodies derived from mesenchymal stem cells promote cutaneous wound healing via regulating the functions of macrophages. Stem Cell Res Ther. 2020;11(1):507. https://doi.org/10.1186/s13287-020-02014-w.
Hus I, et al. Allogeneic dendritic cells pulsed with tumor lysates or apoptotic bodies as immunotherapy for patients with early-stage B-cell chronic lymphocytic leukemia. Leukemia. 2005;19(9):1621–7. https://doi.org/10.1038/sj.leu.2403860.
Qiao L, et al. Tumor cell-derived exosomes home to their cells of origin and can be used as trojan horses to deliver cancer drugs. Theranostics. 2020;10(8):3474–87. https://doi.org/10.7150/thno.39434.
Li Y-J, et al. Gemcitabine loaded autologous exosomes for effective and safe chemotherapy of pancreatic cancer. Acta Biomater. 2019. https://doi.org/10.1016/j.actbio.2019.10.022.
Wang J, et al. The use of RGD-engineered exosomes for enhanced targeting ability and synergistic therapy toward angiogenesis. Nanoscale. 2017;9(40):15598–605. https://doi.org/10.1039/c7nr04425a.
Liang YJ, et al. Engineering exosomes for targeted drug delivery. Theranostics. 2021;11(7):3183–95. https://doi.org/10.7150/thno.52570.
Clemons TD, et al. Distinction between active and passive targeting of nanoparticles dictate their overall therapeutic efficacy. Langmuir. 2018;34(50):15343–9. https://doi.org/10.1021/acs.langmuir.8b02946.
Matsumoto A, et al. Role of phosphatidylserine-derived negative surface charges in the recognition and uptake of intravenously injected b16bl6-derived exosomes by macrophages. J Pharm Sci. 2017;106(1):168–75. https://doi.org/10.1016/j.xphs.2016.07.022.
Matsumoto A, et al. Blood concentrations of small extracellular vesicles are determined by a balance between abundant secretion and rapid clearance. J Extracell Vesicles. 2020. https://doi.org/10.1080/20013078.2019.1696517.
Hiltbrunner S, et al. Exosomal cancer immunotherapy is independent of MHC molecules on exosomes. Oncotarget. 2016;7(25):38707–17. https://doi.org/10.18632/oncotarget.9585.
Tang QS, et al. Tumor-derived exosomes in the cancer immune microenvironment and cancer immunotherapy. Cancer Lett. 2022. https://doi.org/10.1016/j.canlet.2022.215823.
Wang Y, et al. Intravenous delivery of siRNA targeting CD47 effectively inhibits melanoma tumor growth and lung metastasis. Mol Ther. 2013;21(10):1919–29. https://doi.org/10.1038/mt.2013.135.
Piao YJ, et al. Application of immunotherapy based on dendritic cells stimulated by tumor cell-derived exosomes in a syngeneic breast tumor mouse model. Biochem Biophys Rep. 2021. https://doi.org/10.1016/j.bbrep.2021.101136.
Liu H, et al. Co-delivery of tumor-derived exosomes with alpha-galactosylceramide on dendritic cell-based immunotherapy for glioblastoma. Cancer Lett. 2017;411:182–90. https://doi.org/10.1016/j.canlet.2017.09.022.
Zhou WX, et al. Exosomes derived from immunogenically dying tumor cells as a versatile tool for vaccination against pancreatic cancer. Biomaterials. 2022. https://doi.org/10.1016/j.biomaterials.2021.121306.
Morishita M, et al. Exosome-based tumor antigens-adjuvant co-delivery utilizing genetically engineered tumor cell-derived exosomes with immunostimulatory CpG DNA. Biomaterials. 2016;111:55–65. https://doi.org/10.1016/j.biomaterials.2016.09.031.
Wang P, et al. Exosomes from M1-polarized macrophages enhance paclitaxel antitumor activity by activating macrophages-mediated inflammation. Theranostics. 2019;9(6):1714–27. https://doi.org/10.7150/thno.30716.
Yang EL, et al. Exosome-mediated metabolic reprogramming: the emerging role in tumor microenvironment remodeling and its influence on cancer progression. Signal Transduct Target Therapy. 2020. https://doi.org/10.1038/s41392-020-00359-5.
da Costa VR, et al. Exosomes in the tumor microenvironment: from biology to clinical applications. Cells. 2021;10(10): 2617. https://doi.org/10.3390/cells10102617.
Jiang ZM, et al. Cancer derived exosomes induce macrophages immunosuppressive polarization to promote bladder cancer progression. Cell Commun Signal. 2021. https://doi.org/10.1186/s12964-021-00768-1.
Li CL, et al. Clinical significance of PD-L1 expression in serum-derived exosomes in NSCLC patients. J Transl Med. 2019. https://doi.org/10.1186/s12967-019-2101-2.
Cordonnier M, et al. Tracking the evolution of circulating exosomal-PD-L1 to monitor melanoma patients. J Extracell Vesicles. 2020. https://doi.org/10.1080/20013078.2019.1710899.
Fan YB, et al. Exosomal PD-L1 retains immunosuppressive activity and is associated with gastric cancer prognosis. Ann Surg Oncol. 2019;26(11):3745–55. https://doi.org/10.1245/s10434-019-07431-7.
Chen G, et al. Exosomal PD-L1 contributes to immunosuppression and is associated with anti-PD-1 response. Nature. 2018;560(7718):382–6. https://doi.org/10.1038/s41586-018-0392-8.
Chen J, et al. PDL1-positive exosomes suppress antitumor immunity by inducing tumor-specific CD8(+) T cell exhaustion during metastasis. Cancer Sci. 2021;112(9):3437–54. https://doi.org/10.1111/cas.15033.
Maybruck BT, et al. Tumor-derived exosomes induce CD8(+) T cell suppressors. J Immunother Cancer. 2017. https://doi.org/10.1186/s40425-017-0269-7.
Lee CH, et al. Macitentan improves antitumor immune responses by inhibiting the secretion of tumor-derived extracellular vesicle PD-L1. Theranostics. 2022;12(5):1971–87. https://doi.org/10.7150/thno.68864.
Chan JL, et al. Antigen-presenting property of mesenchymal stem cells occurs during a narrow window at low levels of interferon-gamma. Blood. 2006;107(12):4817–24. https://doi.org/10.1182/blood-2006-01-0057.
Duffy MM, et al. Mesenchymal stem cell effects on T-cell effector pathways. Stem Cell Res Ther. 2011;2:2. https://doi.org/10.1186/scrt75.
Klyushnenkova E, et al. T cell responses to allogeneic human mesenchymal stem cells: immunogenicity, tolerance, and suppression. J Biomed Sci. 2005;12(1):47–57. https://doi.org/10.1007/s11373-004-8183-7.
Nauta AJ, et al. Donor-derived mesenchymal stem cells are immunogenic in an allogeneic host and stimulate donor graft rejection in a nonmyeloablative setting. Blood. 2006;108(6):2114–20. https://doi.org/10.1182/blood-2005-11-011650.
Zhang B, et al. Mesenchymal stromal cell exosome-enhanced regulatory T-cell production through an antigen-presenting cell-mediated pathway. Cytotherapy. 2018;20(5):687–96. https://doi.org/10.1016/j.jcyt.2018.02.372.
He XN, et al. MSC-derived exosome promotes M2 polarization and enhances cutaneous wound healing. Stem Cells Int. 2019. https://doi.org/10.1155/2019/7132708.
Lee S, et al. Mesenchymal stem cell-derived exosomes suppress proliferation of T cells by inducing cell cycle arrest through p27kip1/Cdk2 signaling. Immunol Lett. 2020;225:16–22. https://doi.org/10.1016/j.imlet.2020.06.006.
Fujii S, et al. Graft-versus-host disease amelioration by human bone marrow mesenchymal stromal/stem cell-derived extracellular vesicles is associated with peripheral preservation of naive T cell populations. Stem Cells. 2018;36(3):434–45. https://doi.org/10.1002/stem.2759.
Cosenza S, et al. Mesenchymal stem cells-derived exosomes are more immunosuppressive than microparticles in inflammatory arthritis. Theranostics. 2018;8(5):1399–410. https://doi.org/10.7150/thno.21072.
Li YT, et al. Effect of small extracellular vesicles derived from IL-10-overexpressing mesenchymal stem cells on experimental autoimmune uveitis. Stem Cell Res Ther. 2022. https://doi.org/10.1186/s13287-022-02780-9.
Li H, et al. Therapeutic effect of rapamycin-loaded small extracellular vesicles derived from mesenchymal stem cells on experimental autoimmune uveitis. Front Immunol. 2022;13:13. https://doi.org/10.3389/fimmu.2022.864956.
Sun Y, et al. Comparative proteomic analysis of exosomes and microvesicles in human saliva for lung cancer. J Proteome Res. 2018;17(3):1101–7. https://doi.org/10.1021/acs.jproteome.7b00770.
Pedersen S, et al. Circulating microvesicles and exosomes in small cell lung cancer by quantitative proteomics. Clin Proteom. 2022. https://doi.org/10.1186/s12014-021-09339-5.
Palmisano G, et al. Characterization of membrane-shed microvesicles from cytokine-stimulated beta-cells using proteomics strategies. Mol Cell Proteom. 2012;11(8):230–43.
Mohammadi MR, et al. Isolation and characterization of microvesicles from mesenchymal stem cells. Methods. 2020;177:50–7. https://doi.org/10.1016/j.ymeth.2019.10.010.
Wu XQ, et al. Micro-vesicles derived from human Wharton’s jelly mesenchymal stromal cells mitigate renal ischemia-reperfusion injury in rats after cardiac death renal transplantation. J Cell Biochem. 2018;119(2):1879–88. https://doi.org/10.1002/jcb.26348.
Du T, et al. Microvesicles derived from human umbilical cord mesenchyme promote M2 macrophage polarization and ameliorate renal fibrosis following partial nephrectomy via hepatocyte growth factor. Hum Cell. 2021;34(4):1103–13. https://doi.org/10.1007/s13577-021-00525-z.
Vdovenko D, et al. Microvesicles released from activated CD4(+) T cells alter microvascular endothelial cell function. Eur J Clin Invest. 2022. https://doi.org/10.1111/eci.13769.
Shefler I, et al. MicroRNA-4443 regulates mast cell activation by T cell-derived microvesicles. J Allergy Clin Immunol. 2018;141(6):2132. https://doi.org/10.1016/j.jaci.2017.06.045.
Muller L, et al. Immunomodulatory properties of mesenchymal stromal cells: an update. Front Cell Dev Biol. 2021;9: 637725. https://doi.org/10.3389/fcell.2021.637725.
Lichtnekert J, et al. Changes in macrophage phenotype as the immune response evolves. Curr Opin Pharmacol. 2013;13(4):555–64. https://doi.org/10.1016/j.coph.2013.05.013.
Mosser DM, Hamidzadeh K, Goncalves R. Macrophages and the maintenance of homeostasis. Cell Mol Immunol. 2021;18(3):579–87. https://doi.org/10.1038/s41423-020-00541-3.
Ma C, et al. The contribution of macrophages to systemic lupus erythematosus. Clin Immunol. 2019;207:1–9. https://doi.org/10.1016/j.clim.2019.06.009.
Galleu A, et al. Apoptosis in mesenchymal stromal cells induces in vivo recipient-mediated immunomodulation. Sci Transl Med. 2017;9(416): eaam7828. https://doi.org/10.1126/scitranslmed.aam7828.
Pang SHM, et al. Mesenchymal stromal cell apoptosis is required for their therapeutic function. Nat Commun. 2021;12(1):6495. https://doi.org/10.1038/s41467-021-26834-3.
He X, et al. Spontaneous apoptosis of cells in therapeutic stem cell preparation exert immunomodulatory effects through release of phosphatidylserine. Signal Transduct Target Ther. 2021;6(1):270. https://doi.org/10.1038/s41392-021-00688-z.
Zheng C, et al. Apoptotic vesicles restore liver macrophage homeostasis to counteract type 2 diabetes. J Extracell Vesicles. 2021;10(7):e12109. https://doi.org/10.1002/jev2.12109.
Kokhaei P, et al. Dendritic cells loaded with apoptotic tumour cells induce a stronger T-cell response than dendritic cell-tumour hybrids in B-CLL. Leukemia. 2003;17(5):894–9. https://doi.org/10.1038/sj.leu.2402913.
Ebstein F, et al. Cytotoxic T cell responses against mesothelioma by apoptotic cell-pulsed dendritic cells. Am J Respir Crit Care Med. 2004;169(12):1322–30. https://doi.org/10.1164/rccm.200312-1683OC.
Chen Z, et al. Efficient antitumor immunity derived from maturation of dendritic cells that had phagocytosed apoptotic/necrotic tumor cells. Int J Cancer. 2001;93(4):539–48. https://doi.org/10.1002/ijc.1365.
Delirezh N, et al. Autologous dendritic cells loaded with apoptotic tumor cells induce T cell-mediated immune responses against breast cancer in vitro. Cell Immunol. 2009;257(1–2):23–31. https://doi.org/10.1016/j.cellimm.2009.02.002.
Parameswaran S, et al. Enhanced protective immunity derived from dendritic cells with phagocytosis of CD40 ligand transgene-engineered apoptotic tumor cells via increased dendritic cell maturation. Tumori J. 2015;101(6):637–43. https://doi.org/10.5301/tj.5000297.
Ocadlikova D, et al. Generation of myeloma-specific T cells using dendritic cells loaded with MUC1-and hTERT- drived nonapeptides or myeloma cell apoptotic bodies. Neoplasma. 2010;57(5):455–64. https://doi.org/10.4149/neo_2010_05_455.
Kokhaei P, et al. Apoptotic tumor cells are superior to tumor cell lysate, and tumor cell RNA in induction of autologous T cell response in B-CLL. Leukemia. 2004;18(11):1810–5. https://doi.org/10.1038/sj.leu.2403517.
Hirayama D, Iida T, Nakase H. The phagocytic function of macrophage-enforcing Innate immunity and tissue homeostasis. Int J Mol Sci. 2018. https://doi.org/10.3390/ijms19010092.
Kiama SG, et al. Evaluation of phagocytic activity in human monocyte-derived dendritic cells. J Aerosol Med Depos Clear Eff Lung. 2001;14(3):289–99. https://doi.org/10.1089/089426801316970240.
Budai Z, et al. Macrophages engulf apoptotic and primary necrotic thymocytes through similar phosphatidylserine-dependent mechanisms. Febs Open Bio. 2019;9(3):446–56. https://doi.org/10.1002/2211-5463.12584.
Shklover J, Levy-Adam F, Kurant E. Apoptotic cell clearance in development. Curr Top Dev Biol. 2015;114:297–334. https://doi.org/10.1016/bs.ctdb.2015.07.024.
Golpon HA, et al. Life after corpse engulfment: phagocytosis of apoptotic cells leads to VEGF secretion and cell growth. Faseb J. 2004;18(12):1716. https://doi.org/10.1096/fj.04-1853fje.
Cerri PS. Osteoblasts engulf apoptotic bodies during alveolar bone formation in the rat maxilla Anatomical Record Part a-Discoveries in Molecular Cellular and Evolutionary Biology. 2005;286A(1):833–40. https://doi.org/10.1002/ar.a.20220.
Brock CK, et al. Stem cell proliferation is induced by apoptotic bodies from dying cells during epithelial tissue maintenance. Nat Commun. 2019;10:10. https://doi.org/10.1038/s41467-019-09010-6.
Ryoo HD, Gorenc T, Steller H. Apoptotic cells can induce compensatory cell proliferation through the JNK and the wingless signaling pathways. Dev Cell. 2004;7(4):491–501. https://doi.org/10.1016/j.devcel.2004.08.019.
Taghikhani A, et al. microRNA modified tumor-derived exosomes as novel tools for maturation of dendritic cells. J Cell Physiol. 2019;234(6):9417–27. https://doi.org/10.1002/jcp.27626.
Czernek L, Peczek L, Duchler M. Small extracellular vesicles loaded with immunosuppressive miRNAs leads to an inhibition of dendritic cell maturation. Arch Immunol Ther Exp. 2022. https://doi.org/10.1007/s00005-022-00664-7.
Liu W, et al. Development of allergic rhinitis immunotherapy using antigen-loaded small extracellular vesicles. J Controlled Release. 2022;345:433–42. https://doi.org/10.1016/j.jconrel.2022.03.016.
Tang TT, et al. Employing macrophage-derived microvesicle for kidney-targeted delivery of Dexamethasone: an efficient therapeutic strategy against renal inflammation and fibrosis. Theranostics. 2019;9(16):4740–55. https://doi.org/10.7150/thno.33520.
Dusoswa SA, et al. Glycan modification of glioblastoma-derived extracellular vesicles enhances receptor-mediated targeting of dendritic cells. J Extracell Vesicles. 2019. https://doi.org/10.1080/20013078.2019.1648995.
Zhang W, et al. Engineered cancer-derived small extracellular vesicle-liposome hybrid delivery system for targeted treatment of breast cancer. ACS Appl Mater Interfaces. 2023;15(13):16420–33. https://doi.org/10.1021/acsami.2c22749.
Kang K et al. Hybrid Extracellular vesicles-liposomes camouflaged magnetic vesicles cooperating with bioorthogonal click chemistry for high-efficient melanoma circulating tumor cells enrichment. Adv Healthc Mater. 2023.https://doi.org/10.1002/adhm.202202825.
Wang J, Zhu MT, Nie GJ. Biomembrane-based nanostructures for cancer targeting and therapy: from synthetic liposomes to natural biomembranes and membrane-vesicles. Adv Drug Deliv Rev. 2021. https://doi.org/10.1016/j.addr.2021.113974.
Tong L, et al. Oral administration of bovine milk-derived extracellular vesicles alters the gut microbiota and enhances intestinal immunity in mice. Mol Nutr Food Res. 2020;64(8):e1901251. https://doi.org/10.1002/mnfr.201901251.
Ong SGM, et al. Influence of the encapsulation efficiency and size of liposome on the oral bioavailability of griseofulvin-loaded liposomes. Pharmaceutics. 2016. https://doi.org/10.3390/pharmaceutics8030025.
Farooq MA, et al. Enhanced cellular uptake and cytotoxicity of vorinostat through encapsulation in TPGS-modified liposomes. Colloids Surf B-Biointerfaces. 2021. https://doi.org/10.1016/j.colsurfb.2020.111523.
Aderem A, Underhill DM. Mechanisms of phagocytosis in macrophages. Annu Rev Immunol. 1999;17:593–623. https://doi.org/10.1146/annurev.immunol.17.1.593.
Chono S, et al. Influence of particle size on drug delivery to rat alveolar macrophages following pulmonary administration of ciprofloxacin incorporated into liposomes. J Drug Target. 2006;14(8):557–66. https://doi.org/10.1080/10611860600834375.
Matsuoka Y, et al. Importance of particle size of oligomannose-coated liposomes for induction of Th1 immunity. Int Immunopharmacol. 2021. doi: 10.1016/j.intimp.2021.108068.
Krysko DV, Ravichandran KS, Vandenabeele P. Macrophages regulate the clearance of living cells by calreticulin. Nat Commun. 2018;9: 9. https://doi.org/10.1038/s41467-018-06807-9.
Lv Z, et al. Loss of cell surface CD47 clustering formation and binding avidity to SIRPalpha facilitate apoptotic cell clearance by Macrophages. J Immunol. 2015;195(2):661–71. https://doi.org/10.4049/jimmunol.1401719.
Brown S, et al. Apoptosis disables CD31-mediated cell detachment from phagocytes promoting binding and engulfment. Nature. 2002;418(6894):200–3. https://doi.org/10.1038/nature00811.
Migneault F, et al. Apoptotic exosome-like vesicles regulate endothelial gene expression, inflammatory signaling, and function through the NF-kappa B signaling pathway. Sci Rep. 2020. https://doi.org/10.1038/s41598-020-69548-0.
Park SY, Kim IS. Engulfment signals and the phagocytic machinery for apoptotic cell clearance. Exp Mol Med. 2017. https://doi.org/10.1038/emm.2017.52.
Shimizu A, et al. Exosomal CD47 plays an essential role in immune evasion in ovarian cancer. Mol Cancer Res. 2021;19(9):1583–95. https://doi.org/10.1158/1541-7786.mcr-20-0956.
Kibria G, et al. A rapid, automated surface protein profiling of single circulating exosomes in human blood. Sci Rep. 2016;6: 36502. https://doi.org/10.1038/srep36502.
Jiaa GH, Sowers JR. Targeting endothelial exosomes for the prevention of cardiovascular disease. Biochim Biophys Acta-Mol Basis Dis. 2020. https://doi.org/10.1016/j.bbadis.2020.165833.
Buono L, et al. Mesenchymal stem cell-derived extracellular vesicles protect human corneal endothelial cells from endoplasmic reticulum stress-mediated apoptosis. Int J Mol Sci. 2021;22(9): 4930. https://doi.org/10.3390/ijms22094930.
Lehner GF, et al. Hemofiltration induces generation of leukocyte-derived CD31+/CD41-microvesicles in sepsis. Ann Intensiv Care. 2017. https://doi.org/10.1186/s13613-017-0312-3.
Liang X, et al. Phosphatidylserine released from apoptotic cells in tumor induces M2-like macrophage polarization through the PSR-STAT3-JMJD3 axis. Cancer Commun (Lond). 2022;42(3):205–22. https://doi.org/10.1002/cac2.12272.
Lemke G. How macrophages deal with death. Nat Rev Immunol. 2019;19(9):539–49. https://doi.org/10.1038/s41577-019-0167-y.
Liu Y, et al. Targeting tumor-associated macrophages by MMP2-sensitive apoptotic body-mimicking nanoparticles. ACS Appl Mater Interfaces. 2020;12(47):52402–14. https://doi.org/10.1021/acsami.0c15983.
Kraynak CA, Yan DJ, Suggs LJ. Modulating inflammatory macrophages with an apoptotic body-inspired nanoparticle. Acta Biomater. 2020;108:250–60. https://doi.org/10.1016/j.actbio.2020.03.041.
Schcolnik-Cabrera A, et al. Calreticulin in phagocytosis and cancer: opposite roles in immune response outcomes. Apoptosis. 2019;24(3–4):245–55. https://doi.org/10.1007/s10495-019-01532-0.
Trzeciak A, Wang YT, Perry JSA. First we eat, then we do everything else: the dynamic metabolic regulation of efferocytosis. Cell Metabol. 2021;33(11):2126–41. https://doi.org/10.1016/j.cmet.2021.08.001.
Gregory CD, Pound JD. Microenvironmental influences of apoptosis in vivo and in vitro. Apoptosis. 2010;15(9):1029–49. https://doi.org/10.1007/s10495-010-0485-9.
Biavasco R, et al. Oncogene-induced senescence in hematopoietic progenitors features myeloid restricted hematopoiesis, chronic inflammation and histiocytosis. Nat Commun. 2021;12(1): 4559. https://doi.org/10.1038/s41467-021-24876-1.
van Nieuwenhuijze AE, et al. Transgenic expression of GM-CSF in T cells causes disseminated histiocytosis. Am J Pathol. 2014;184(1):184–99. https://doi.org/10.1016/j.ajpath.2013.09.014.
Takedomi H, Akutagawa T, Esaki M. Crystal-storing histiocytosis of the rectum possibly associated with chronic mucosal inflammation by ulcerative colitis. Dig Endosc. 2023. https://doi.org/10.1111/den.14526.
Lin JD, et al. Detection of immune microenvironment changes and immune-related regulators in langerhans cell histiocytosis bone metastasis. Biomed Res Int. 2023. https://doi.org/10.1155/2023/1447435.
Szondy Z, et al. Anti-inflammatory mechanisms triggered by apoptotic cells during their clearance. Front Immunol. 2017;8:8. https://doi.org/10.3389/fimmu.2017.00909.
Yuan YY, et al. Inflammatory caspase-related pyroptosis: mechanism, regulation and therapeutic potential for inflammatory bowel disease. Gastroenterol Rep. 2018;6(3):167–76. https://doi.org/10.1093/gastro/goy011.
Wallach D, et al. Anti-inflammatory functions of the “apoptotic” caspases clearance of dying cells in healthy and diseased immune systems. Ann NY Acad Sci. 2010;1209:17–22. https://doi.org/10.1111/j.1749-6632.2010.05742.x.
Romecin PA, et al. Robust in vitro and in vivo immunosuppressive and anti-inflammatory properties of inducible Caspase-9-mediated apoptotic mesenchymal stromal/stem cell. Stem Cells Transl Med. 2022;11(1):88–96. https://doi.org/10.1093/stcltm/szab007.
Birge RB, et al. Phosphatidylserine is a global immunosuppressive signal in efferocytosis, infectious disease, and cancer. Cell Death Differ. 2016;23(6):962–78. https://doi.org/10.1038/cdd.2016.11.
Reutelingsperger CP, van Heerde WL. Annexin V, the regulator of phosphatidylserine-catalyzed inflammation and coagulation during apoptosis. Cell Mol Life Sci. 1997;53(6):527–32. https://doi.org/10.1007/s000180050067.
Huynh MLN, Fadok VA, Henson PM. Phosphatidylserine-dependent ingestion of apoptotic cells promotes TGF-beta 1 secretion and the resolution of inflammation. J Clin Invest. 2002;109(1):41–50. https://doi.org/10.1172/jci200211638.
Otsuka M, Biological, et al. Phosphatidylserine-specific receptor contributes to TGF-beta production in macrophages through a MAP kinase, ERK. Pharm Bull. 2005;28(9):1707–10. https://doi.org/10.1248/bpb.28.1707.
Wu LL, et al. Effects of RGD-grafted phosphatidylserine-containing liposomes on the polarization of macrophages and bone tissue regeneration. Biomaterials. 2021. https://doi.org/10.1016/j.biomaterials.2021.121239.
Quan HX, et al. Modulation of the anti-inflammatory effects of phosphatidylserine-containing liposomes by PEGylation. J Biomed Mater Res Part A. 2017;105(5):1479–86. https://doi.org/10.1002/jbm.a.35981.
Wu Y, et al. An apoptotic body-biomimic liposome in situ upregulates anti-inflammatory macrophages for stabilization of atherosclerotic plaques. J Control Release. 2019;316:236–49. https://doi.org/10.1016/j.jconrel.2019.10.043.
Acknowledgements
Jiemin Wang acknowledges the financial support from the China Scholarship Council (202006370067). Figures 2, 3, 4 and 5 were created by biorender.com. In the end, the authors acknowledge the suggestions gotten from MD536 Advanced and Applied Immunology course. This course is organized by Prof Matthew Dallas Griffin at University of Galway.
Author information
Authors and Affiliations
Contributions
Jing Wen: Writing- Original draft preparation; Dale Creaven: revising the manuscript; Xiangshu Luan: investigation and discussion; Jiemin Wang: Conceptualization, supervision and reviewing and revising the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare that they do not have any competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wen, J., Creaven, D., Luan, X. et al. Comparison of immunotherapy mediated by apoptotic bodies, microvesicles and exosomes: apoptotic bodies’ unique anti-inflammatory potential. J Transl Med 21, 478 (2023). https://doi.org/10.1186/s12967-023-04342-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12967-023-04342-w