
Abstract
Background
This is an exploratory study using a novel imaging modality, quantitative ultrashort time-to-echo, contrast enhanced (QUTE-CE) magnetic resonance imaging to evaluate the permeability of the blood–brain barrier in a rat model of type 2 diabetes with the presumption that small vessel disease is a contributing factor to neuropathology in diabetes.
Methods
The BBZDR/Wor rat, a model of type 2 diabetes, and age-matched controls were studied for changes in blood–brain barrier permeability. QUTE-CE, a quantitative vascular biomarker, generated angiographic images with over 500,000 voxels that were registered to a 3D MRI rat brain atlas providing site-specific information on blood–brain barrier permeability in 173 different brain areas.
Results
In this model of diabetes, without the support of insulin treatment, there was global capillary pathology with over 84% of the brain showing a significant increase in blood–brain barrier permeability over wild-type controls. Areas of the cerebellum and midbrain dopaminergic system were not significantly affected.
Conclusion
Small vessel disease as assessed by permeability in the blood–brain barrier in type 2 diabetes is pervasive and includes much of the brain. The increase in blood–brain barrier permeability is a likely contributing factor to diabetic encephalopathy and dementia.
Similar content being viewed by others


Background
Vascular dementia is a serious consequence of diabetes [1]. Prolonged exposure to high blood levels of glucose, typical of type 2 diabetes, affects capillary endothelial structure, function and permeability [2]. Failure in the blood brain barrier lies at the foundation of cerebral small vessel disease and contributes to the pathogenesis of diabetic encephalopathy [3] Methods for in vivo quantification and localization of changes in blood–brain barrier permeability are needed to understand and diagnose the early onset of vascular dementia with type 2 diabetes.
Imaging the subtle changes in blood–brain permeability is not possible with standard imaging protocols but can be assessed with dynamic contrast enhanced (DCE) MRI [4]. However, dynamic contrast enhanced MRI has several limitations. The concentration versus time curve for gadolinium-based contrast agent is typically 15–30% inaccurate; therefore, DCE-MRI has not proven useful clinically [5]. It is also difficult to model the effects of contrast agent on both T2* and T1 given the short acquisition time, and strong dependence on microstructural properties such as vessel size, tortuosity and orientation. These and other methodological issues with the use of DCE-MRI for blood–brain barrier permeability have resulted in significant differences in the reported rates of leakage [5].
To address this issue, a novel imaging modality, quantitative ultrashort time-to-echo, contrast enhanced (QUTE-CE) MRI [6] was used to study changes in blood–brain barrier in the BBZDR/Wor rat an inbred rat strain model of type 2 diabetes [7]. QUTE-CE MRI utilizes Ultrashort-Time-to-Echo (UTE) sequences with ferumoxytol, an FDA-approved superparamagnetic iron oxide nanoparticles (SPIONs) formula already used off-label for human MRI, as a contrast agent to produce positive contrast angiograms with low error of quantification [6, 8].
Research design and methods
Animals
This study used male Bio-Breeding Zucker diabetic rats (BBZDR/Wor rats) (n = 8) and age-matched non-diabetic BBDR littermates (n = 7). The founding population was established by Biomere (Worcester, MA). The company decided to retire the breeding line and made a gift of their last animals to the Center for Translational NeuroImaging. The obese male BBZDR/Wor rat spontaneously develops type 2 diabetes at approximately 10 weeks of age (~ 100%) when fed standard rat chow. BBZDR/Wor diabetic rat displays all clinical symptoms typically associated with type 2 diabetes including dyslipidemia, hyperglycemia, insulin resistance, and hypertension [7],
Rats were maintained on a 12 h:12 h light–dark cycle with a light on at 07:00 h, allowed access to food and water ad libitum and were treated with intraperitoneal injections of saline at indications of weight loss. All animal experiments were conducted in accordance with the Northeastern University Division of Laboratory Animal Medicine and Institutional Animal Care and Use Committee. (https://academic.oup.com/ilarjournal/article/45/3/292/704910).
Access to rats was dependent upon the breeding schedule and resulting genotypes. This required we run two separate imaging studies, each with four rats from each genotype, separated by 6 months.
Imaging
Studies were done on a Bruker Biospec 7.0 T/20 cm USR horizontal magnet (Bruker, Billerica, MA, USA) and a 20-G/cm magnetic field gradient insert (ID = 12 cm) capable of a 120 μs rise time. Radio frequency signals were sent and received with a quadrature volume coil built into the rat restrainer (Animal Imaging Research, Holden, Massachusetts). All rats imaged under 1–2% isoflurane while keeping a respiratory rate of 40–50 breadths/min. At the beginning of each imaging session, a high-resolution anatomical data set was collected using the RARE pulse sequence with following parameters, 35 slice of 0.7 mm thickness; field of view 3 cm; 256 × 256; repetition time [TR] 3900 ms; effective echo time [TE] 48 ms; number of excitations 3; 6 min 14 s acquisition time.
Rats were imaged prior to and following an i.v. bolus of 6 mg/ml Fe of Ferumoxytol. The injected volume was tailored for each rat (assuming 7% blood by body weight) to produce a starting blood concentration of 200 μg/ml Fe (2 × the clinical dose approved for use in humans). The QUTE-CE MRI image parameters of TE = 13 µs, TR = 4 ms, and flip angle = 20° utilized a high radio frequency pulse bandwidth of 200 kHz. Therefore, the pulse duration was short (6.4 µs) compared to the T2 of the approximate ferumoxytol concentration (4.58 ms for 3.58 mM, i.e. 200 µg/ml to minimize signal blur and reduce the probability for a curved trajectory of the magnetization vector Mz. A 3 ×3×3 cm3 field-of-view was used with a matrix mesh size of 180× 180×180 to produce 167 µm isotropic resolution.
Images were motion-corrected, aligned spatially, and resliced using MATLAB SPM12 toolbox developed at UCL (https://www.fil.ion.ucl.ac.uk/spm/). The pre-contrast UTE images were set as the baseline. For each rat in each imaging session, the voxel wise percentage change of signal intensity was calculated as (post-con – baseline)/(blood intensity change) *100% as described in our previous work [10], where blood intensity change is a normalization factor calculated by the post-con blood signal intensity minus baseline blood signal intensity. A 173-region rat brain atlas (Ekam Solutions LLC, Boston, MA, US) was fit to T2-weighted RARE anatomical data set for each rat data set taken at each imaging session, using software developed at Northeastern University Center for Translational Neuroimaging (CTNI), considering the variations in brain size and positions. The fitted atlas was transferred to UTE imaging. Once the images were co-registered to the atlas, custom MATLAB code was used to mask individual brain regions for ferumoxytol measurement. Post contrast UTE images are shown for a control and diabetic rat in Additional file 1: Figure S1.
Mode of percentage change distribution for each of the 173 brain areas for control and BBZDR/Wor rats was statistically compared using a Wilcoxon rank-sum test with the alpha set at 0.05. Data was analyzed by co-authors Cai and Kulkarni blind to the identity of the groups.
Data and resource availability
All data can be accessed through a link to Mendeley. DOI to follow.
Results
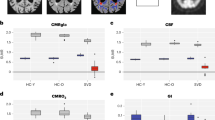
Table 1 shows all the brain areas (147/173) that were significantly different (α p < 0.05) in blood–brain barrier permeability between BBZDR/Wor rats and their littermate controls. Note in all cases BBZDR/Wor rats showed greater permeability. The location of these areas can be are visualized in the surrounding 2D and 3D images generated with the rat MRI atlas shown in Fig. 1. All areas in red in the 2D representations show significantly greater blood–brain barrier permeability in the BBZDR/Wor rats as compared to controls. Table 2 shows all brain areas (26/173) that were not significantly different in blood–brain barrier permeability between BBZDR/Wor rats and their littermate controls. These areas shown in white are localized to the prefrontal ctx, midbrain and cerebellum. These nonaffected areas are coalesced into 3D volumes and pictured in the glass brain in yellow.

Imaging blood brain barrier permeability. Quantitative ultra-short time-to-echo, contrast enhanced imaging of blood brain barrier permeability comparing BBZDR/Wor rats and their littermate controls. All areas in red show significantly greater permeability in type 2 diabetic as compared to controls
Discussion
QUTE-CE MRI, was developed as a quantitative vascular biomarker [6]. Ferumoxytol (Feraheme™) MRI with optimized 3D Ultra-Short Time-to-echo (UTE) Pulse Sequences produces angiographic images unparalleled to time-of-flight imaging or gadolinium-based first-pass imaging. The contrast agent is ferumoxytol, an ultra-small superparamagnetic iron oxide nanoparticle with a dextran coating. Since the size exceeds the cutoff (~ 6 nm) for glomerular filtration, ferumoxytol is not cleared by the kidney, and instead is an excellent blood pool contrast agent with a long intravascular half-life of ~ 15 h [9]. Numerous clinical MRI studies using ferumoxytol have been conducted in children and adults, demonstrating no major adverse effects, thus QUTE-CE can be readily used in the clinic to study blood–brain barrier permeability [10]. We recently published a study mapping the absolute physiological cerebral blood volume (CBV) of the awake rat brain, including measurements of microvasculature density and vascular functional reserve [8]. QUTE-CE MRI can be used for identifying hyper- or hypo-vascularization, small vessel density, blood–brain barrier permeability and vascular reserve and vascular responsivity to CO2 challenge at the individual voxel and regional levels using our rat 3D MRI atlas. As demonstrated in this study with the BBZDR/Wor rats, a preclinical model of type 2 diabetes, this imaging technology could be used to diagnose and evaluate blood brain permeability and disease progression in diabetic encephalopathy in the clinic.
Limitations and future directions
As a pilot study with a small population of rats there were several limitations: (1) Females were not studied. Unfortunately, only males develop diabetes in the BBZDR/Wor strain of rats [7]. (2) While the blood–brain permeability was pervasive in this late-stage model of diabetes and not unexpected, postmortem histology would have confirmed the capillary pathology and helped to understand why areas like the cerebellum and midbrain were spared. (3) In the future, a thorough comparison between DCE and QUTE-CE should be done to provide quantitative data on the differences and similarities between both imaging techniques. (4) More common rat models of T2DB should be tested like the Goto-Kakizaki GK rat [11] or high-fat diet, streptozotocin treated Wistar rat (HFD/STZ) [12].
Conclusion
Small vessel disease as assessed by permeability in the blood–brain barrier in type 2 diabetes is pervasive and includes much of the brain. The increase in blood–brain barrier permeability is a likely contributing factor to diabetic encephalopathy and dementia.
Availability of data and materials
All data can be accessed through a link to Mendeley. DOI to follow.
Abbreviations
- QUTE-CE:
-
Quantitative ultrashort time-to-echo, contrast enhanced
- BBB:
-
Blood brain barrier
- CBV:
-
Cerebral blood volume
- DCE:
-
Dynamic contrast enhanced
- BBZDR:
-
Male Bio-Breeding Zucker diabetic rats
- TR:
-
Repetition time
- TE:
-
Echo time
- RARE:
-
Rapid acquisition with relaxation enhancement
References
Pasquier F, Boulogne A, Leys D, Fontaine P. Diabetes mellitus and dementia. Diabetes Metab. 2006. https://doi.org/10.1016/s1262-3636(07)70298-7.
Allen CL, Bayraktutan U. Antioxidants attenuate hyperglycaemia-mediated brain endothelial cell dysfunction and blood-brain barrier hyperpermeability. Diabetes Obes Metab. 2009. https://doi.org/10.1111/j.1463-1326.2008.00987.x.
Bogush M, Heldt NA, Persidsky Y. Blood brain barrier injury in diabetes: unrecognized effects on brain and cognition. J Neuroimmune Pharmacol. 2017. https://doi.org/10.1007/s11481-017-9752-7.
Starr JM, Wardlaw J, Ferguson K, MacLullich A, Deary IJ, Marshall I. Increased blood-brain barrier permeability in type II diabetes demonstrated by gadolinium magnetic resonance imaging. J Neurol Neurosurg Psychiatry. 2003. https://doi.org/10.1136/jnnp.74.1.70.
Raja R, Rosenberg GA, Caprihan A. MRI measurements of Blood–Brain Barrier function in dementia: a review of recent studies. Neuropharmacology. 2018. https://doi.org/10.1016/j.neuropharm.2017.10.034.
Gharagouzloo CA, McMahon PN, Sridhar S. Quantitative contrast-enhanced MRI with superparamagnetic nanoparticles using ultrashort time-to-echo pulse sequences. Magn Reson Med. 2015. https://doi.org/10.1002/mrm.25426.
Tirabassi RS, Flanagan JF, Wu T, Kislauskis EH, Birckbichler PJ, Guberski DL. The BBZDR/Wor rat model for investigating the complications of type 2 diabetes mellitus. ILAR J. 2004. https://doi.org/10.1093/ilar.45.3.292.
Gharagouzloo CA, Timms L, Qiao J, Fang Z, Nneji J, Pandya A, Kulkarni P, van de Ven AL, Ferris C, Sridhar S. Quantitative vascular neuroimaging of the rat brain using superparamagnetic nanoparticles: New insights on vascular organization and brain function. NeuroImage. 2017. https://doi.org/10.1016/j.neuroimage.2017.09.003.
Bremerich J, Bilecen D, Reimer P. MR angiography with blood pool contrast agents. Eur Radiol. 2007. https://doi.org/10.1007/s00330-007-0712-0.
Muehe AM, Feng D, von Eyben R, Luna-Fineman S, Link MP, Muthig T, Huddleston AE, Neuwelt EA, Daldrup-Link HE. Safety report of ferumoxytol for magnetic resonance imaging in children and young adults. Invest Radiol. 2016. https://doi.org/10.1097/RLI.0000000000000230.
Kuwabara WMT, Panveloski-Costa AC, Yokota CNF, Pereira JNB, Filho JM, Torres RP, Hirabara SM, Curi R, Alba-Loureiro TC. Comparison of Goto-Kakizaki rats and high fat diet-induced obese rats: are they reliable models to study type 2 diabetes mellitus? PLoS ONE. 2017. https://doi.org/10.1371/journal.pone.0189622.
Ding G, Yan T, Chen J, Chopp M, Li L, Li Q, Cui C, Ning R, Jiang Q. Persistent cerebrovascular damage after stroke in type two diabetic rats measured by magnetic resonance imaging. Stroke. 2015. https://doi.org/10.1161/STROKEAHA.114.007538.
Acknowledgements
We thank Biomere (Worcester, Massachusetts, USA) for providing the BBZDR/Wor rats and their age-matched non-diabetic BBDR littermates for these studies.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
All of the authors have contributed substantially to the manuscript. Concept, drafting and interpretation—CFF, JQ. Execution and analysis—JQ, PK, CML, KFGR. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable to humans. All animal experiments were conducted in accordance with the Northeastern University Division of Laboratory Animal Medicine and Institutional Animal Care and Use Committee.
Consent for publication
Not applicable.
Competing interests
CFF has a financial interest in Animal Imaging Research, the company that makes the RF electronics and holders for animal imaging.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Additional file 1: Figure S1.
Shown are raw data from a control and diabetic rat following ferumoxytol injection. The normalized UTE signal is registered to the original anatomy.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Qiao, J., Lawson, C.M., Rentrup, K.F.G. et al. Evaluating blood–brain barrier permeability in a rat model of type 2 diabetes. J Transl Med 18, 256 (2020). https://doi.org/10.1186/s12967-020-02428-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12967-020-02428-3