
Abstract
Background
The purpose of this systematic review was to examine the associations between school-related sedentary behaviours and indicators of health and well-being in children and youth (~ 5–18 years) attending school.
Methods
This review was conducted to inform the development of School-Related Sedentary Behaviour Recommendations. Peer-reviewed, published, or in-press articles in English were included. Reviews, meta-analyses, and case studies were excluded; all other study designs were eligible. Further, articles had to meet the a priori study criteria for population, intervention, comparator (PROSPERO ID: CRD42021227600). Embase, MEDLINE® ALL, and PsycINFO were searched. Risk of bias was assessed for individual experimental studies using the Cochrane risk of bias assessment tool, and in observational studies based on the GRADE framework and in line with previous systematic reviews examining sedentary behaviours in children. Overall quality of evidence was assessed using the GRADE framework for each outcome category and study design. Results were synthesized narratively, grouped by study design and outcome category. Further, several high-level summaries were conducted to help interpret results.
Results
Evidence was synthesized from 116 reports, including 1,385,038 participants and 1173 extracted associations. More school-related sedentary behaviour was favourably associated with nearly one-third of extracted associations for cognitive (33%) and social-emotional (32%) indicators (e.g., less anxiety), but unfavourably associated with other movement behaviours (e.g., less physical activity) (35%). Active lessons were favourable (72%), compared to more school-related sedentary behaviours, when examining associations for all health and well-being indicators. More homework was favourable across all health and well-being indicators in 4% of extracted associations for primary school children, and 25% of extracted associations for secondary school children. However, ≥2 h/day of homework appeared to be unfavourable for health and well-being. Limitations for synthesized studies included generally low quality of evidence and a lack of studies in South American, African, or low-middle income countries.
Conclusions
Findings can help inform policy makers, schools, and teachers, regarding the amount of homework assigned and the introduction of active lessons into the classroom to enhance health and well-being of children. More research is needed examining school-related sedentary behaviours and indicators of health and well-being in low- and middle-income countries.
Similar content being viewed by others

Background
Sedentary behaviour is defined as any waking behaviour characterized by an energy expenditure ≤1.5 metabolic equivalents (METs) while in a sitting, reclining, or lying posture [1]. Accumulating high levels of sedentary behaviour is unfavourably associated with a breadth of health and well-being outcomes in school-aged children and youth or adolescents [2, 3]. However, according to an estimated global average, children accumulate 8 h/day of sedentary time [4], which represents approximately 50% of the waking day. Thus, children’s health and well-being may be at risk due to excessive time spent engaged in sedentary behaviours.
In line with the public health concerns surrounding children’s sedentary behaviours, Canada and Australia released 24-h movement behaviour guidelines for children and youth or young-people that included specific sedentary behaviour benchmarks [5, 6]. Specifically, it was recommended that children and youth should spend no more than 2 h/day engaged in recreational screen time and sitting for extended periods should be limited. These recommendations were informed by Carson et al.’s [2] systematic review of 235 studies, which included some studies examining school-related sedentary behaviours [7,8,9,10,11,12]. However, recommendations specifically for the school setting were not made since this was not an objective of the review.
The school is recognized as an important setting for promoting children’s health and well-being, based on the capacity of a school to incorporate health- and well-being-related curricula, establish a health- and well-being-related culture, and engage sources outside of the school that influence children’s behaviours (e.g., families, communities) [13]. Further, children spend a large amount of time in school, and the net global school attendance rates are 89% for primary (~ 5–12 years) and 66% for secondary (~ 13–17 years) school-aged children [14, 15]. Evidence indicates that children spend most of their school day sedentary, with one meta-analysis estimating that on average 63% of the school-day is spent sedentary for children and adolescents in the United States [16]. Further, sedentary behaviour in school directly accounted for an average of ~ 40% of total weekday sedentary behaviour in a sample of Spanish children and adolescents [17].
Schools, and policy makers, also dictate the volume of homework assigned to children, which ranges from 3 to 10 h/week of sedentary time according to global averages for 15-year-olds [18]. Considering the amount of sedentary time accumulated in schools, and assigned by schools, sedentary behaviour recommendations specific to the school setting may be important and relevant for children’s health and well-being. However, the development of school-related sedentary behaviour recommendations is precluded by the lack of a comprehensive literature synthesis examining the relationship between school-related sedentary behaviours and indicators of health and well-being.
Several previous reviews have examined aspects of school-related sedentary behaviours and indicators of health and well-being [19,20,21,22,23,24,25,26]. However, the scope of these reviews were narrow for included: study designs, health and well-being indicators, and school-related sedentary behaviours. For instance, these reviews have only examined experimental study designs. Some reviews examined any school-related intervention [19, 23], while the others were specific to recess [25], classrooms [22, 26], or standing desks in particular [20, 21, 24]. The two reviews that examined any school-related interventions were specific to adiposity indicators in primary school-aged children [23], and physical activity in older adolescents [19]. Further, of the reviews examining a broad spectrum of health and well-being indicators, two were specific to standing desk interventions [20, 24] and the other was specific to recess [25]. Collectively, these reviews have not provided an up-to-date and exhaustive overview of the associations between school-related sedentary behaviours and health and well-being indicators.
Based on the lack of representation across study designs, health and well-being indicators, and school-related sedentary behaviour exposures in previous systematic reviews, a comprehensive systematic review is needed, that builds on Carson et al.’s [2] review, to inform the development of school-related sedentary behaviour recommendations. Therefore, the objective of this systematic review was to comprehensively examine the associations between school-related sedentary behaviours and indicators of health and well-being in children and youth (~ 5–18 years) attending school. Further objectives of this study included examining differences in associations across school-related sedentary behaviour exposure types (e.g., homework, sedentary time) and age groups, as well as examining any dose-response associations for school-related sedentary behaviours with health and well-being indicators.
Methods
Context
This systematic review was conducted to act as a source of evidence informing the development of the School-Related Sedentary Behaviour Recommendations, conducted by members of the Sedentary Behaviour Research Network (SBRN). Members of the SBRN Recommendations Steering Committee and an international expert panel met to determine key methodological decisions when conceptualizing this review. Details of the final guidelines are available elsewhere [27]. A summary of the methodology specific to the current review is presented below.
Protocol and registration
This systematic review was registered with the international prospective register of systematic reviews (PROSPERO; Registration ID: CRD42021227600) and followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [28].
Eligibility criteria
Only peer-reviewed, published, or in-press articles in English were included. Reviews, meta-analyses, and case studies were excluded, but all other study designs were eligible. Further, articles had to meet the a priori study criteria for population, intervention, comparator, and outcome (PICO) [29] in line with the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) framework [30, 31].
Population (participants)
Apparently healthy (i.e., general populations, including those with overweight/obesity, but not samples exclusively with a diagnosed medical condition) children and youth (~ 5–18 years) attending primary or secondary school. For studies measuring multiple time points (e.g., longitudinal), school attendance was needed for at least one measurement time point. The following post-hoc sample size exclusion criteria were imposed in line with previous systematic reviews [2, 32]: experimental/intervention studies needed a minimum sample size of ≥30 participants, while observational studies needed a minimum sample size of ≥300 participants.
Intervention (exposures)
Duration, patterns, and types of school-related sedentary behaviours. Sedentary behaviour is defined according to the SBRN as any waking behavior characterized by an energy expenditure ≤1.5 METs, while in a sitting, reclining, or lying posture [1]. For this review, the operational definition of sedentary behaviours included behaviours typically involving sedentary postures and low energy expenditure (e.g., homework, screen time [iPad/tablet/touch-screen, smart phone], time spent sitting). All sedentary behaviours needed to be school-related, which refers to sedentary behaviours occurring during school hours (e.g., classroom, recess) or outside of school hours but influenced by the school (e.g., homework, studying). Traditional class time was assumed to be sedentary, and activities that could displace sedentary behaviours (e.g., adding more physical education (PE) classes to the schedule) were included as a proxy for sedentary behaviour reduction. Sedentary behaviours were not operationally defined as failing to meet physical activity guidelines [1]. For experimental studies, interventions that targeted multiple health behaviours (e.g., standing time and nutrition) were not included. If possible, results were to be separated based on the context of school-related sedentary behaviours as: outside of school hours (e.g., homework), during school instructional time (e.g., classroom), and during school free-time (e.g., recess). However, to better align with the extracted school-related sedentary behaviour exposures, post-hoc categories were created for: active breaks, active lessons, additional physical activity, homework, recess/PE, screen time, standing desks, and sedentary time.
Comparator
Various durations, patterns, or types of school-related sedentary behaviours. However, a comparator or control group was not required.
Outcomes (indicators)
Outcome or indicator categories were selected based on previous systematic reviews [2, 33], and through expert input and consensus. Based on the GRADE framework, health and well-being outcome categories were ranked as “critical” or “important” by the steering committee and expert panel, since only critical or important outcomes should be used to inform guideline recommendations [34]. Critical outcomes included: adiposity indicators (e.g., body mass index, waist circumference, skinfolds, bio-electrical impedance analysis), biomarkers (e.g., lipid profile, insulin, glucose, blood pressure), cognitive indicators (e.g., academic achievement, executive functions, literacy), musculoskeletal growth (e.g., bone mineral density, fat free mass, height), risks (injury)/harm (e.g., “text neck”/anterior head syndrome, eyestrain, headaches), and social-emotional indicators (e.g., classroom time on task, prosocial behaviour, sociability, self-esteem). Important outcomes included: fitness (e.g., grip strength, shuttle run, flexibility) and other movement behaviours (e.g., physical activity, sleep, non-school-related sedentary behaviours).
Information sources and search strategy
This review adopted and modified a previous search strategy, developed with and peer-reviewed by academic librarians with expertise in systematic review search strategies [2]. Search terms were updated to include sedentary behaviours that were not common or did not exist in 2016 (e.g., Zoom), and to include terms specific to school-related sedentary behaviours (e.g., homework). Search strategies were modified specifically for the databases Ovid Embase, Ovid MEDLINE® ALL, and Ovid PsycINFO. A date limit was used to exclude articles published before January 1, 2014 to reduce overlap with the previous systematic review [2]. The most recent search was conducted on January 7, 2021. For the full search strategy, see Additional File 1. Records were imported into Covidence (Veritas Health Innovation, Melbourne, Australia) and deduplication was completed before screening for eligibility.
Study selection
At level 1 screening, titles and abstracts of all potentially relevant articles were reviewed by the lead author (NK) and one other independent reviewer (BC, YH, or SV) in Covidence. Eligible articles meeting the screening criteria by either reviewer proceeded to level 2 full-text screening. The lead author (NK) and another independent reviewer (BC, YH, or SV) screened the full-text articles for inclusion or exclusion. Discrepancies in article inclusion or exclusion were resolved through discussion and consensus between the 2 reviewers, or by including a third reviewer (TS) to reach consensus.
Data collection process and data items
Data were extracted from eligible articles into Google Sheets templates. All studies were extracted by one reviewer and verified by another reviewer, with one reviewer (NK) extracting or verifying each study and the other reviewers (BC, YH, or SV) independently performing the reciprocal extraction or verification. For each study, descriptive characteristics were extracted including author, publication year, country, study design, and sample size. Details for the exposure, outcome, and study results were extracted for each study. When studies reported results from multiple models (e.g., bivariate and adjusted linear regression models), the most fully adjusted results were used to summarize findings. However, if models with similar covariates were reported (e.g., adjusted for BMI, and adjusted for body fat percentage), results from both models were extracted for comparison. Statistical significance of extracted results was defined as p < 0.05 regardless of how individual studies defined statistical significance.
Risk of bias in individual studies and across studies
Risk of bias was assessed or verified for individual studies by one reviewer (NK) and the other reviewers (BC, YH, or SV) independently performed the reciprocal assessment or verification. To assess risk of bias for individual experimental studies, the Cochrane risk of bias assessment tool was used [35]. For assessing risk of bias in observational studies, criteria were determined based on recommendations for types of characteristics to examine from the GRADE framework, and in line with similar systematic reviews examining sedentary behaviours in children [2, 32]. The assessed criteria consisted of the following domains: selection bias, performance bias, selective reporting bias, detection bias, attrition bias, and other biases (e.g., inadequate control for key confounders). The results for study-level risk of bias can be found in Additional File 3. The GRADE framework was used to assess the overall quality of evidence for each outcome category and study design [36]. Quality of evidence was ranked as “high”, “moderate”, “low”, or “very low”, corresponding to the confidence that the true effect aligns with the estimated effect (e.g., very low = true effect is distinctly different from the estimated effect; high = confident that the true effect is close to the estimated effect) [36]. The ranked quality of evidence started at high for randomised trials and low for other study designs. Quality of evidence was downgraded if serious limitations were seen in the domains of risk of bias, inconsistency, indirectness, or imprecision. If no downgrades occurred then quality of evidence could be upgraded based on large magnitudes of effect, dose-response gradients, or sufficiently controlling for residual confounding. Quality of evidence ratings were performed by one reviewer and presented to the broader expert panel for consensus.
Synthesis of results
Due to heterogeneity across school-related sedentary exposures and outcomes, meta-analyses were not conducted. Instead, narrative syntheses were performed. Specifically, extracted results were coded in the direction of null, favourable (i.e., desired or beneficial), or unfavourable (i.e., undesired or adverse) based on the significance and direction of an association between the school-related sedentary behaviour exposure and the outcome. For consistency, result directions (e.g., favourable, unfavourable) were reported as the relationship between sedentary behaviour and the indicator of health and well-being. As previously discussed, traditional class time was assumed to be sedentary, and activities that could displace sedentary behaviours (e.g., adding more physical education (PE) classes to the schedule) were included as a proxy for sedentary behaviour reduction. For instance, if higher durations of recess were associated with higher grades, this was described as more sedentary behaviour being unfavourable for academic achievement. In contrast, if a longitudinal study found that more homework was associated with higher grades, this was described as more homework being favourable for academic achievement.
For each health and well-being indicator category, when all extracted results for a study were in the same direction, this study was classified as consistently null, favourable, or unfavourable. When the direction of findings for extracted results for a study were not consistent (e.g., one study finding more sedentary behaviour was favourable and null for two extracted results in the same health and well-being indicator category), the study was classified as mixed. When mixed results were observed, attempts were made to explain the inconsistent findings (e.g., dose-response relationships). Studies comparing different types of sedentary behaviours (e.g., screen vs paper-based learning) were not coded as favourable or unfavourable with sedentary behaviour in general, but instead framed relative to each of the specific sedentary behaviours being examined (e.g., sedentary game favourable for cognitive indicators when compared to sedentary lesson). Summary tables also included subsections for each category of school-related sedentary behaviours. To assist with the interpretation of results, high-level summaries of results that omitted the mixed category by counting the frequency of individual results being null, favourable, or unfavourable were also generated. High-level results were summarized by outcome and exposure categories, as well as the age categories of primary school-aged (~ 5–12 years) and secondary school-aged (~ 13–18 years) children. When sample ages spanned across primary and secondary school-age ranges, results were omitted from the age sub-categorizations.
Results
Study selection
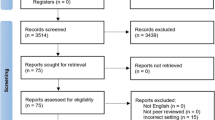
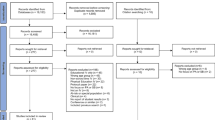
Figure 1 illustrates the PRISMA flowchart for included studies. After screening, 116 studies were included and had all relevant data extracted and quality of evidence rated for the qualitative synthesis.

PRISMA Flowchart
Study characteristics
The 116 included articles, including 112 samples (or unique studies), are summarized by outcome category in Additional File 2; Supplementary Tables 1–8. For the articles from the same study [37,38,39,40,41,42,43], there was only one instance of the same results being presented in more than one article. Specifically, two articles from one study reported on the same associations for other movement behaviours [37, 43], so results specific to other movement behaviours were only used from the first study [43]. Though, both studies contributed unique findings to other health and well-being outcome categories, so study exclusion was not necessary. Extracted data across study designs included 1,385,038 participants, of which 1,327,091 were from unique samples. Of the 116 articles, 5 examined multiple countries, including Australia and the United Kingdom [44]; Czech Republic and Poland [45]; Fiji, Kiribati, Samoa, Solomon Islands, Tonga, and Vanuatu [46]; Indonesia, Lao PDR, Philippines, Thailand, and Timor-Leste [47]; Belgium, Greece, Hungary, Netherlands, and Switzerland [48]. Data were collected from a total of 43 countries, with the most frequent being the United States (n = 19/131), China (n = 16/131), and Australia (n = 14/131), and the most frequent continents being Europe (n = 45/131), Asia (n = 35/131), and North America (n = 25/131) (See Fig. 2). As well, according to World Bank income classifications, data were collected from high (70.8%), upper-middle (17.5%), lower-middle (8.0%), and low (3.6%) income countries. Baseline mean ages ranged from 6 to 17 years and from school grades 1 to 12. Experimental study designs were used in 44 studies, including clustered RCTs (n = 20), RCTs (n = 3), cross-over trials (n = 5), and non-randomised interventions (n = 16). Observational study designs were used in 79 studies (longitudinal [n = 14] and cross-sectional [n = 65]). Of those studies, five articles contained results for two study designs (cross-sectional and longitudinal: n = 3; non-randomised intervention and longitudinal: n = 1; non-randomised intervention and cross-sectional: n = 1) and two articles contained the results of two different samples/experiments (non-randomised interventions: n = 1; clustered RCTs: n = 1). The school-related sedentary exposures (including those that imply the displacement of sedentary behaviour) included homework (n = 57), recess/PE (n = 16), standing desks (n = 12), sedentary time (n = 9), active breaks (n = 9), additional physical activity (n = 8), screen time (n = 8), and active lessons (n = 7)—some studies measured multiple exposures.

Number of Studies by Country
Synthesis of results
Critical outcomes
Adiposity indicators
Thirty-two studies examined the association between school-related sedentary behaviours and adiposity indicators (See Additional File 2, Supplementary Table 1 for the individual studies). The study designs for these articles were clustered RCT (n = 4), non-randomised intervention (n = 4), longitudinal (n = 3), and cross-sectional (n = 21). For a summary of the measured adiposity indicators, see Table 1.
Among clustered RCT study designs, null findings were consistently reported in 4/4 studies [49,50,51,52]. The consistent null findings were reported for the school-related sedentary exposures of additional physical activity [49, 50], recess/PE [51], and standing desks [52]. Overall, the quality of evidence was rated as low due to a very serious risk of indirectness. For a description of quality of evidence assessments, see Table 1.
For non-randomised interventions, findings were consistently reported as null in 2/4 studies [53, 54], mixed in 1/4 studies [55], and more sedentary behaviour was unfavourable for adiposity indicators in 1/4 studies [56]. Organizing by categories of school-related sedentary behaviour exposures, consistent null findings were reported recess/PE [53], while more sedentary behaviour was unfavourable for adiposity indicators when compared to active breaks [56], suggesting a benefit for displacing sedentary behaviour with active breaks. For standing desks, 1/2 studies reported consistent null findings [54]. Overall, the quality of evidence was rated as very low due to serious risk of bias and serious risk of indirectness.
Among longitudinal studies, homework was the only school-related sedentary exposure. Findings were consistently reported as null in 1/3 studies [57] and more homework was favourable for adiposity indicators in 1/3 studies, indicating that higher levels of homework were associated with lower adiposity [58]. While findings were reported as mixed (i.e., null and unfavourable) in 1/3 studies, a dose response relationship partly explained the mixed findings with unfavourable associations seen for ≥3 h/day of studying time [59], suggesting that homework above that threshold was associated with higher adiposity. Overall, the quality of evidence was rated as very low due to serious risk of bias.
For cross-sectional studies, findings were consistently reported as null in 10/21 studies [47, 60,61,62,63,64,65,66,67,68], more sedentary behaviour was unfavourable for adiposity indicators in 4/21 studies [41, 69,70,71], and mixed for 7/21 studies [38, 46, 48, 72,73,74,75]. Organizing by categories of school-related sedentary behaviour exposures, consistent null associations were seen for active breaks [60] and additional physical activity [60]. More sedentary behaviour was unfavourable for adiposity indicators in 2/11 studies examining homework [41, 69], 1/6 studies examining sedentary time [71], and 1/5 studies examining recess/PE [70]. Overall, the quality of evidence was rated as very low due to serious risk of bias and serious risk of indirectness.
Biomarkers
A total of 4 studies examined the association between school-related sedentary behaviours and biomarkers (See Additional File 2, Supplementary Table 2 for the individual studies). Study designs included clustered RCTs (n = 2), non-randomised intervention (n = 1), and longitudinal (n = 1). For a summary of the measured biomarkers, see Table 2.
Across all study designs and exposure categories, consistent null findings were observed. This included 2/2 clustered RCTs assessing additional physical activity [49] and recess/PE [51], 1/1 non-randomised intervention assessing standing desks [54], and 1/1 longitudinal study assessing homework [76]. The quality of evidence was rated as either moderate (clustered RCT) or very low (non-randomised intervention and longitudinal) due to serious risk of bias for all study designs, as well as very serious risk of imprecision (non-randomised intervention) and serious risk of imprecision (longitudinal).
Cognitive indicators
A total of 29 studies examined the association between school-related sedentary exposures and cognitive indicators (See Additional File 2, Supplementary Table 3 for the individual studies). The study designs for these articles were clustered RCT (n = 7), RCT (n = 3), cross-over trial (n = 2), non-randomised intervention (n = 3), longitudinal (n = 3), and cross-sectional (n = 11). One article contained two clustered RCT studies [77]. For a summary of the measured cognitive indicators, see Table 3.
Among the clustered RCT study design, findings were consistently reported as null in 4/7 studies [37, 43, 78, 79], and mixed in 1/7 studies [52]. Additionally, 2/7 studies (2 studies, 1 article) compared types of sedentary behaviours [77]. Of the 2 studies comparing types of sedentary behaviours, screen-based learning was compared to usual classroom learning [77]. Based on categories of school-related sedentary exposures, consistent null associations were seen for active breaks [78], active lessons [79], and additional physical activity [37, 43]; while screen-based learning was favourable for cognitive indicators compared to the usual classroom condition [77]. Overall, the quality of evidence was rated as moderate due to serious risk of indirectness.
Among RCT study designs, no overall consistent null, favourable, or unfavourable directions of results were observed with 1/3 studies reporting mixed findings [80] and 2/3 studies comparing types of sedentary behaviours [81, 82] also with no clear direction in findings. Mixed findings were explained in one study by dose of physical activity, as null associations were observed when comparing no active breaks to one active break, while more sedentary behaviour was unfavourable for cognitive indicators when comparing no active breaks to two active breaks [80]. Overall, the quality of evidence was rated as high due to no serious risks to quality of evidence.
For cross-over study designs, screen time was the only school-related sedentary exposure and comparing types of sedentary behaviours were the only extracted results [83, 84]. A consistent direction of results was seen in 1/2 articles, as the paper-based condition was favourable for cognitive indicators compared to the screen-based condition [83]. Specifically, when taking the same paper-based or tablet-based math quiz, children performed better in the paper-based condition across all sub-scales of the quiz [83]. Whereas, in the other study no consistent direction of findings were reported between paper and screen based comparisons [84]. Overall, the quality of evidence was rated as high due to no serious risks to quality of evidence observed.
Among non-randomised interventions, findings were consistently reported as null in 2/3 studies [85, 86], and 1/3 studies compared types of sedentary behaviours [87]. Based on categories of school-related sedentary exposures, consistent null associations were observed for standing desks [85, 86]. Overall, the quality of evidence was rated as very low due to serious risk of bias.
For longitudinal study designs, the only exposure observed was homework. More homework was consistently favourable for cognitive indicators in 1/3 studies [88]. The 2/3 studies with mixed findings included dose-response relationships with favourable associations (e.g., “high homework” levels), and null associations (e.g., “medium homework” levels) [40, 89]. Overall, the quality of evidence was rated as very low due to serious risk of bias.
Among cross-sectional study designs, more school-related sedentary behaviour was consistently null for cognitive indicators in 1/11 studies [90], unfavourable for cognitive indicators in 1/11 studies [91], favourable for cognitive indicators in 6/11 studies [62, 63, 68, 92,93,94], and mixed for 3/11 studies [95,96,97]. Based on categories of school-related sedentary exposures, consistent null findings were observed for recess/PE [90] and sedentary time [68]. As well, 5/9 studies reported more homework was favourable for cognitive indicators [62, 63, 92,93,94], while 1/9 studies reported more homework was unfavourable for cognitive indicators [91]. Overall, the quality of evidence was rated as very low due to a serious risk of bias.
Musculoskeletal growth
A total of 3 studies examined the association between school-related sedentary behaviours and musculoskeletal growth (See Additional File 2, Supplementary Table 4 for the individual studies). Study designs included clustered RCT (n = 1), non-randomised intervention (n = 1), and cross-sectional (n = 1). For a summary of the measured musculoskeletal growth see Table 4.
For the clustered RCT and non-randomised intervention, the only exposure observed was recess/PE. Consistent null associations were observed in both studies [51, 53]. Overall, the quality of evidence was rated as low for the clustered RCT due to serious risk of bias and serious risk of imprecision, and very low for the non-randomised intervention due to serious risk of bias, very serious risk of indirectness, and serious risk of imprecision.
For the cross-sectional study, the only exposure observed was homework. Findings were mixed, with null results observed for boys and more homework favourable for musculoskeletal growth in girls [69]. Specifically, homework was positively associated with fat-free mass index in girls, but no significant associations were detected for boys. Overall, the quality of evidence was rated as very low for serious risk of bias and serious risk of imprecision.
Risks (injury)/harm
A total of 19 studies examined the association between school-related sedentary behaviours and risks (injury)/harm (See Additional File 2, Supplementary Table 5 for the individual studies). Study designs included a cross-over trial (n = 1), non-randomised interventions (n = 3), longitudinal (n = 1), and cross-sectional (n = 14). Additionally, one of these articles included longitudinal and cross-sectional study designs. For a summary of the measured outcomes, see Table 5.
The cross-over trial exposure was standing desks. Findings were mixed, with more sedentary behaviour null and unfavourable for risks/harms when comparing traditional classroom designs to standing desks [98]. Overall, the quality of evidence was rated as very low due to very serious risk of bias and very serious risk of imprecision.
For the non-randomised interventions, the only observed exposure was standing desks. Consistent null findings were observed for each of the included studies [54, 55, 85]. Overall, the quality of evidence was rated as very low due to very serious risk of bias.
The longitudinal study exposure was homework. Findings were mixed but included dose-response relationships with unfavourable associations for ≥2 h of cram school (tutoring centres) attendance, and null associations for 0.5–1.9 h/day [99]. Overall, the quality of evidence was rated as very low due to serious risk of bias and serious risk of imprecision.
For the cross-sectional studies, null findings were observed in 2/14 studies [63, 100], more sedentary behaviour was unfavourable for risks/harms in 5/14 studies [94, 101,102,103,104], and mixed in 7/14 studies [99, 105,106,107,108,109,110]. More sedentary behaviour was consistently unfavourable for risks/harms when compared to recess/PE (indicating recess/PE was beneficial for preventing risks/harms) [103]. More screen time was also consistently unfavourable for risks/harms [104]. More homework was consistently null in 2/12 studies [63, 100] and unfavourable for risks/harms in 3/12 studies [94, 101, 102]. Mixed findings for homework included dose-response relationships in 5/12 studies, with unfavourable results (e.g., “too much” homework associated with more shoulder pain), null results (e.g., no association between “not enough” homework and shoulder pain), and favourable results (e.g., 6–8 h/day of studying or sitting associated with less neck and shoulder pain [sample median: 8–10 h/day of studying or sitting]) [99, 105,106,107, 110]. Overall, the quality of evidence was rated as very low due to serious risk of bias.
Social-emotional indicators
Twenty-one studies examined the association between school-related sedentary behaviours and social-emotional indicators (See Additional File 2, Supplementary Table 6 for the individual studies). Study designs included clustered RCTs (n = 4), non-randomised intervention (n = 1), longitudinal (n = 4), and cross-sectional (n = 12). For a summary of the measured outcomes, see Table 6.
Among clustered RCTs, a consistent direction in results was observed as null in 1/4 studies [49], more sedentary behaviour was unfavourable for social-emotional indicators in 2/4 studies [111, 112], and 1/4 studies reported a mix of null and unfavourable findings and compared types of sedentary behaviours [113]. For exposure categories, more sedentary behaviour was consistently null for additional physical activity [49]. More sedentary behaviour was consistently unfavourable for social-emotional indicators when compared to active lessons in 2/4 studies. One study found a sedentary game was favourable for social-emotional indicators when compared to a sedentary lesson [113]. Overall, the quality of evidence was rated as low due to very serious risk of indirectness.
For the non-randomised intervention, the only observed exposure was standing desks. More sedentary behaviour was consistently favourable for social-emotional indicators [85]. Specifically, the standing desk intervention group had higher total difficulties (i.e., hyperactivity, emotional symptoms, conduct problems, and peer problems) scores, compared to the traditional classroom control group. Overall, the quality of evidence was rated as very low very due to serious risk of imprecision.
Among longitudinal studies, findings were consistently observed as null in 1/4 studies [114] and mixed in 3/4 studies [57, 115, 116]. While no consistent findings were observed across exposure categories, 1/3 studies examining the exposure of homework reported consistent null findings [114]. Overall, the quality of evidence was rated as very low due to serious risk of bias.
For the cross-sectional studies, findings were consistently reported as null in 2/12 studies [71, 117], while more sedentary behaviour was favourable in 1/12 studies [118], unfavourable in 1/12 studies [119], and mixed findings were reported for 8/12 studies [39, 63, 65, 68, 120,121,122,123]. No consistent findings were reported across exposure categories. However, consistent findings in some studies were observed as null for homework [117], and sedentary time [71]. More homework was favourable for social-emotional indicators [118] and unfavourable for social-emotional indicators [119]. Overall, the quality of evidence was rated as very low due to serious risk of bias.
Important outcomes
Fitness
Thirteen studies examined the association between school-related sedentary behaviours and fitness (See Additional File 2, Supplementary Table 7 for the individual studies). Study designs included clustered RCTs (n = 6), non-randomised interventions (n = 2), and cross-sectional (n = 5). For a summary of the measured outcomes, see Table 7.
Among the clustered RCTs, findings were consistently observed as null in 3/6 studies [37, 50, 51], more sedentary behaviour was unfavourable for 1/6 studies [49], and mixed findings were reported in 2/6 studies [124, 125]. Consistent null findings were observed for the exposure category recess/PE [51]. Null associations were observed in 2/4 studies examining additional physical activity. As well, more sedentary behaviour was unfavourable for fitness in 1/4 studies examining additional physical activity, indicating that incorporating more physical activity in the school day schedule was beneficial for fitness. Overall, the quality of evidence was rated as very low due to very serious risk of indirectness.
The non-randomised interventions exposure was active breaks. More sedentary behaviour was unfavourable for fitness when comparing traditional sedentary classrooms with classrooms adding active breaks to the class [56, 126]. Overall, the quality of evidence was rated as very low due to serious risk of indirectness.
Among the cross-sectional studies, findings were consistently observed as null in 4/5 studies [60, 62, 92, 127] and more sedentary behaviour was unfavourable for fitness in 1/5 studies [71]. Across the exposure categories, consistent null findings were observed for active breaks [60], additional physical activity [60], homework [62, 92], and recess/PE [60]. More sedentary time was unfavourable for fitness in 1/2 studies [71] and null in 1/2 studies [127]. Overall, the quality of evidence was rated as very low due to serious risk of bias and serious risk of indirectness.
Other movement behaviours
A total of 61 studies examined the association between school-related sedentary behaviours and other movement behaviours (See Additional File 2, Supplementary Table 8 for the individual studies). Study designs included clustered RCTs (n = 14), cross-over trials (n = 3), non-randomised interventions (n = 14), longitudinal (n = 5), and cross-sectional (n = 25). Of these articles, multiple study designs were observed for combinations of longitudinal and non-randomised intervention (n = 1), cross-sectional and non-randomised intervention (n = 1), and cross-sectional and longitudinal (n = 2). Further, one article included results from two non-randomised interventions [44]. For a summary of the measured outcomes see Table 8.
Among the clustered RCTs, findings were consistently observed as null in 4/14 studies [43, 49, 51, 52], more sedentary behaviour was unfavourable for other movement behaviours in 2/14 studies [111, 128], and mixed findings were reported in 8/14 studies [50, 78, 79, 125, 129,130,131,132]. Null findings were observed for recess/PE [51]. Consistent null findings were observed in 2/6 studies examining additional physical activity [43, 49], and 1/3 studies examining standing desks [52]. Further, more sedentary behaviour was consistently unfavourable for other movement behaviours in 1/3 studies comparing traditional lessons with active lessons [111], and 1/7 studies comparing traditional school days with school days incorporating various forms of additional physical activity [128]. Overall, the quality of evidence was rated as low due to very serious risk of indirectness.
For the cross-over trials, more school-related sedentary behaviour was consistently unfavourable for other movement behaviours in 1/3 studies [133] and mixed findings were reported for 2/3 studies [98, 134]. No exposure category contained only null, favourable, or unfavourable directions of results. More sedentary behaviours were consistently unfavourable for other movement behaviours in 1/2 studies comparing usual sedentary conditions to standing desks [133]. Overall, the quality of evidence was rated as low due to very serious risk of bias.
Among non-randomised interventions, associations between school-related sedentary behaviour and other movement behaviours were consistently null in 1/14 studies [54], more sedentary behaviour was unfavourable for other movement behaviours in 4/14 studies [55, 56, 115, 135], and mixed findings were reported in 9/14 studies [44, 53, 54, 85, 86, 136,137,138,139]. No consistent directions of results were seen across exposure categories. More sedentary behaviours were consistently unfavourable for other movement behaviours in 2/3 studies comparing a typical school day with school days incorporating active breaks [56, 115] and 2/8 studies comparing traditional classrooms to those with standing desks [55, 135]. Overall, the quality of evidence was rated as very low due to serious risk of bias and serious risk of indirectness.
For longitudinal studies, associations between school-related sedentary behaviour and other movement behaviours were observed as null in 1/5 studies [140], more sedentary behaviour was unfavourable for other movement behaviours in 1/5 studies [42], and mixed findings were reported in 3/5 studies [57, 115, 141]. No consistent trends were seen across exposure categories. More sedentary behaviour was consistently unfavourable for other movement behaviours in 1/3 studies examining homework [42], and null in 1/2 studies examining recess/PE [140]. Overall, the quality of evidence was rated as very low due to serious risk of bias.
Among cross-sectional studies, associations between school-related sedentary behaviour and other movement behaviours findings were consistently null for 3/25 studies [123, 140, 142], while more sedentary behaviour was unfavourable for other movement behaviours in 5/25 studies [42, 71, 143,144,145], favourable for other movement behaviours in 2/25 studies [121, 146], and mixed for 15/25 studies [45, 62, 74, 75, 91, 93, 94, 108, 137, 147,148,149,150,151,152]. Across exposure categories, no consistent directions of results towards null, favourable, and unfavourable were seen. Consistent null findings were observed in 2/18 studies examining homework [123, 142], and 1/4 studies examining recess/PE [140]. More sedentary behaviour was consistently favourable for other movement behaviours in 2/18 studies examining homework [121, 146], and consistently unfavourable for other movement behaviours in 2/18 studies examining homework [42, 143], 1/4 studies examining recess/PE [144], and 2/3 studies examining sedentary time [71, 145]. Overall, the quality of evidence was rated as very low due to serious risk of bias.
High level summary of results
To facilitate the interpretation of the findings in this review, high-level summaries of results ungrouped from study designs, were completed for each extracted result that was classified as null, favourable, or unfavourable. For the high-level summary by outcome category, most results were null (See Table 9). However, more sedentary behaviour was favourably associated with approximately one-third of extracted associations for cognitive (33%) and social-emotional (32%) indicators. As well, more school-related sedentary behaviour was unfavourably associated with around one-third of extracted associations for other movement behaviours (35%). Ranges of quality of evidence are only presented in the high-level outcome category summary, since quality of evidence was rated by outcome categories and study design, but not for the high-level exposure category summary. Table 10 shows a high-level summary by exposure type, where null results were most frequently observed. However, more school-related sedentary behaviour was unfavourably associated with any health and well-being indicator when compared to active lessons in 72% of the extracted associations—indicating a benefit for active lessons in 72% of extracted associations. While 100% of results for screen time was also unfavourable, this only represented one extracted result, as most extracted associations for screen time compared types of sedentary behaviours.
To further aide interpretation of the review findings, high-level summaries of results by outcome and exposure categories were also examined separately for primary (~ 5–12 years) and secondary (~ 13–18 years) school-aged children (See Table 11). For instance, more homework was favourable for any health and well-being indicator in 4% of extracted results for primary school children, and 25% of extracted results for secondary school children. Further, more sedentary behaviour was favourable for secondary school-aged children in nearly half of extracted associations for cognitive (48%) and social-emotional indicators (42%), compared to slightly over 10% for cognitive (14%) and for social-emotional (12%) indicators in primary school-aged children.
Several instances of mixed directions of associations being explained by dose-response relationships between homework and health and well-being indicators were observed. Thus, a summary table was created to compile these associations, and explore the various dose-response relationships between homework and health and well-being indicators (See Table 12). A possible trend was seen for ≥2 h/day of homework being unfavourable for health and well-being. Trends in the null or favourable directions of associations were less apparent.
Discussion
Summary of evidence
To help inform School-Related Sedentary Behaviour Recommendations, this systematic review examined the associations between school-related sedentary behaviours and inidcators of health and well-being in school-aged (~ 5–18 years) children. This was the first review to examine a comprehensive set of school-related sedentary behaviours and inidcators of health and well-being. Evidence was synthesized from 116 reports, including 1,385,038 participants and 1173 extracted associations. Based on high level summaries, the association between school-related sedentary behaviours and indicators of health and well-being were predominantly null. However, some evidence indicated more school-related sedentary behaviours could be favourable for cognitive and social-emotional indicators, and unfavourable for other movement behaviours. Further, when displacing school-related sedentary behaviours, active lessons were the most beneficial for students’ overall health and well-being. Compared to primary school-aged children, secondary school-aged children seemed to benefit from homework and had more favourable associations between school-related sedentary behaviours and cognitive and social-emotional indicators. Though high-level findings should be interpreted with some caution as findings are pooled across study designs and subsequent quality of evidence. The lower range of quality of evidence was very low for all health and well-being indicator categories, but upper ranges were observed as high for cognitive indicators.
Carson et al’s [2] review of sedentary behaviour and indicators of health and well-being in school-aged children found that homework was beneficial for cognitive indicators. Similarly, in the current review a favourable association between school-related sedentary behaviour and indicators of health and well-being was most frequently observed in the homework exposure category. These favourable associations seemed to be mainly for cognitive and social-emotional indicators. When examining dose-response relationships, higher levels of homework appeared to be unfavourable for health and well-being. Reverse causality could be an alternative explanation for the dose-response association between higher durations of time spent on homework and worse health and well-being, as children that spend more time on homework could be struggling to complete their assignments. Fernández-Alonso et al. [97] found homework duration was negatively associated with academic achievement at the individual level, but positively associated when looking at the amount the school assigns. While this could indicate there are benefits for schools to assign more homework, potential benefits should be interpreted with caution as further analyses revealed schools that assigned more homework widened the gap at the individual level for time spent on homework and academic achievement [97]. Thus, it could be said that assigning more homework at a school level adds inequity to students who struggle to complete homework based on cognitive or time constraints (e.g., after school employment). Further, placing an additional sedentary behaviour burden on children through homework and studying in pursuit of academic success could displace time in a 24-h day that could otherwise be spent on sleep and physical activity. This time displacement would ironically be counter-productive, based on the benefits to cognitive indicators from physical activity and adequate sleep for school-aged children [153, 154]. Regardless, homework demonstrated favourable associations with cognitive and social-emotional indicators, and is likely a valuable activity for children in moderation and at an age-appropriate level. For instance, in this review most favourable associations between homework and indicators of health and well-being were for secondary school-aged children. Thus, when determining the amount of homework assigned to children, teachers should consider how homework will enhance the academic development of all children, if homework is displacing time spent on other behaviours beneficial to academic development, and if the amount of homework is age-appropriate.
For school-related sedentary behaviour exposure categories, active lessons were overwhelmingly beneficial for health and well-being when displacing school-related sedentary behaviours. Active lessons are appealing since they simultaneously displace sedentary time and focus on educational pursuits. Further, within this review, evidence suggested that active lessons could improve children’s time on task behaviours or attention during class [111,112,113]. Additionally, no difference in content recall was observed when comparing content delivered through active lessons or traditional sedentary classroom conditions [79], suggesting that active lessons do not detract from learning objectives and could in fact enhance learning. Further, some studies not only incorporated active lessons into the school-day, but also conducted active lessons outside of the classroom. Considering the benefits of outdoor time for a range of health and well-being indicators [155,156,157], combining active lessons and outdoor time provides an additional opportunity to improve the health and well-being of school-aged children. Interestingly, most studies that examined active lessons were in the health and well-being indicator category of other movement behaviours (physical activity during active lessons), with 5 extracted associations for social-emotional indicators (time on task) and 1 extracted association for cognitive indicators (lesson content recall). Additionally, active lessons were only examined in primary school-aged children. Thus, future studies are needed to examine the benefits of active lessons across a range of health and well-being indicators, especially in outdoor settings where further benefits could be seen (e.g., myopia prevention [156]), and in secondary school-aged children.
Studies examining screen-based sedentary behaviours and indicators of health and well-being compared screen-based class time with other types of school-related sedentary behaviours (e.g., typical classroom time). Thus, it was difficult to make a broad claim that sedentary behaviour was favourable or unfavourable for health and well-being in high level summaries since sedentary behaviours were being compared to one another. Paper-based assessments (e.g., quizzes, writing accuracy) were favourable when compared to screen-based assessments [83, 84]. However, school-related screen time was beneficial when compared to non-educational screen time and traditional classroom learning, when lessons were built around screen time to serve a specific pedagogical purpose [77, 81, 82, 87]. Thus, it could be concluded that school-related screen time can be beneficial when it is meaningfully developed to serve a specific pedagogical purpose, and not implemented simply for the novelty of screens. Importantly, for several studies screen-based learning was seen as a means of meeting the United Nations Sustainable Development Goal of ensuring inclusive and equitable quality education for all [77, 81, 82]. Specifically, screen-based learning was examined to help overcome barriers specific to Malawi, where “school days are short, classrooms are overcrowded and poorly resourced, and teachers are frequently under qualified” [82]. While the merits of face-to-face learning versus screen-based learning can be debated, neither side can ignore the necessity of finding solutions for overcoming country specific barriers to delivering high-quality education for all children. Further, contingency plans are needed to prevent disrupted education if face-to-face learning in the classroom is not a possibility, as was seen in the COVID-19 crisis [158]. While COVID-19 could be seen as a global barrier to high-quality education, rural settings and low-middle income countries were disproportionately disrupted through a lack of infrastructure and equipment available to access online learning [158]. Thus, future research examining screen-based versus face-to-face learning should continue to reflect on how study results translate to inclusive and equitable education for all children internationally.
Limitations
Several limitations of the included studies were observed. First, the quality of evidence was most frequently rated as very low. Future research should consider how study and evidence quality is evaluated [35, 36] when designing observational and experimental studies (e.g., exposure and outcome variables with sufficient psychometric evaluation, randomly sampling participants or schools), to aide the creation of high quality evidence. Second, most studies were cross-sectional. To better understand the causative mechanisms between school-related sedentary behaviours and indicators of health and well-being, more high-quality research is needed using longitudinal and experimental study designs. Third, few studies examined the health and well-being indicator categories of musculoskeletal growth (n = 3) and biomarkers (n = 4) compared to categories such as other movement behaviours (n = 62 studies). Fourth, 96% of studies were conducted in Europe, Asia, and North America with very few studies conducted in South America and Africa. Additionally, 71% of studies were conducted in high-income countries. More research is urgently needed to fill this gap, as review findings are limited in their ability to generalize to schools in Africa, South America, and low-middle income countries.
Further, several limitations existed specific to this review. First, the conceptualization of school-related sedentary behaviours included physical activity. Movement behaviours during the school day can be classified such that physical activity and sedentary behaviour (excluding screen time) are mutually exclusive and exhaustive, equating to perfectly collinear categories. Thus, any change to physical activity necessitates an equivalent change to sedentary behaviour, assuming no changes have been made to the length of the school day and sleep time is not part of the school day. Instead of assuming sedentary behaviours are displaced when adding physical activity, compositional analyses can examine this displacement. While two included studies used compositional analyses [61, 127], a future review should exclusively synthesize studies using compositional analyses to better understand the movement behaviour displacements occurring in the school setting. Further, a future review could examine compositional analyses studies while also considering possible compensations with recreational sedentary behaviours outside of school time. Second, we deviated from our review protocol by adding a post-hoc sample size exclusion criteria. While a deviation from protocol is not ideal, excluded participants (n = 3229) would have contributed less than 1% to the total number of participants. Further, excluding studies with smaller sample sizes increased our confidence that associations represent a true effect [159]. Third, while the comprehensive scope of this review can be considered a strength for informing guideline development, it may also be considered a limitation when summarizing findings. Specifically, a broad search, inclusion criteria, and outcome categories (e.g., fitness comprised of domains such as flexibility, aerobic endurance, muscular power) may have introduced heterogeneity to exposure and outcome variables, making it difficult to conduct meta-analyses. Ideally, this broad review will guide future reviews aimed at answering more narrowly focused research questions. Lastly, the gap between the last search (January 2021) and the submission (October 2021) of this review could warrant updating the search strategy. However, there was only a 6-month gap between the most recent search and the review findings informing the development of guidelines in June 2021 [27].
Conclusions
Our findings suggest more school-related sedentary behaviour is unfavourable for other movement behaviours, but favourable for cognitive and social emotional indicators. Favourable associations between more school-related sedentary behaviour and cognitive and social emotional indicators were mainly related to homework. However, favourable associations were primarily observed for secondary school-aged children and a dose-response relationship was observed as high levels of homework were unfavourable for health and well-being indicators. Further, when displacing school-related sedentary behaviours, active lessons were the most beneficial for health and well-being. Our findings have important implications for policy makers, schools, and teachers, with regard to the amount of homework assigned and the introduction of active lessons into the classroom to enhance the learning, health and well-being of children. More research is needed examining screen-based learning and indicators of health and well-being, as well as school-related sedentary behaviours overall in low- and middle-income countries.
Availability of data and materials
All data generated or analysed during this study are included in this published article and its supplementary information files.
References
Tremblay MS, Aubert S, Barnes JD, Saunders TJ, Carson V, Latimer-Cheung AE, et al. Sedentary behavior research network (SBRN) – terminology consensus project process and outcome. Int J Behav Nutr Phys Act. 2017;14(1):75.
Carson V, Hunter S, Kuzik N, Gray CE, Poitras VJ, Chaput J-P, et al. Systematic review of sedentary behaviour and health indicators in school-aged children and youth: an update. Appl Physiol Nutr Metab. 2016;41(6):S240–S65.
Chaput J-P, Willumsen J, Bull F, Chou R, Ekelund U, Firth J, et al. 2020 WHO guidelines on physical activity and sedentary behaviour for children and adolescents aged 5–17 years: summary of the evidence. Int J Behav Nutr Phys Act. 2020;17(1):1–9.
Bauman AE, Petersen CB, Blond K, Rangul V, Hardy LL. The descriptive epidemiology of sedentary behaviour. Sedentary behaviour epidemiology. Cham: Springer; 2018. p. 73–106.
Tremblay MS, Carson V, Chaput J-P, Connor Gorber S, Dinh T, Duggan M, et al. Canadian 24-hour movement guidelines for children and youth: an integration of physical activity, sedentary behaviour, and sleep. Appl Physiol Nutr Metab. 2016;41(6):S311–S27.
Okely A, Ghersi D, Loughran S, Cliff D, Shilton T, Jones R. Australian 24-hour movement guidelines for children (5–12 years) and young people (13–17 years): an integration of physical activity, sedentary behaviour. Canberra: Australian Government; 2019.
Bowers AJ, Berland M. Does recreational computer use affect high school achievement? Educ Technol Res Dev. 2013;61(1):51–69.
O'Dea JA, Mugridge AC. Nutritional quality of breakfast and physical activity independently predict the literacy and numeracy scores of children after adjusting for socioeconomic status. Health Educ Res. 2012;27(6):975–85.
Hong TK, Trang NH, Dibley MJ, Sibbritt DW, Binh PN, Hanh TT. Factors associated with adolescent overweight/obesity in Ho chi minh city. Int J Pediatr Obes. 2010;5(5):396–403.
Zhang J, Seo DC, Kolbe L, Middlestadt S, Zhao W. Trends in overweight among school children and adolescents in seven Chinese provinces, from 1991–2004. Int J Pediatr Obes. 2010;5(5):375–82.
Zhang J, Seo D-C, Kolbe L, Middlestadt S, Zhao W. Associated trends in sedentary behavior and BMI among Chinese school children and adolescents in seven diverse Chinese provinces. Int J Behav Med. 2012;19(3):342–50.
Seo D-C, Niu J. Trends in underweight and overweight/obesity prevalence in Chinese youth, 2004–2009. Int J Behav Med. 2014;21(4):682–90.
Langford R, Bonell CP, Jones HE, Pouliou T, Murphy SM, Waters E, et al. The WHO health promoting school framework for improving the health and well-being of students and their academic achievement. Cochrane Database Syst Rev. 2014;4:CD008958.
UNESCO IfS. School enrollment, secondary (% net). 2020.
UNESCO IfS. School enrollment, primary (% net). 2020.
Egan CA, Webster CA, Beets MW, Weaver RG, Russ L, Michael D, et al. Sedentary time and behavior during school: a systematic review and meta-analysis. Am J Health Educ. 2019;50(5):283–90.
Grao-Cruces A, Sánchez-Oliva D, Padilla-Moledo C, Izquierdo-Gómez R, Cabanas-Sánchez V, Castro-Piñero J. Changes in the school and non-school sedentary time in youth: the UP&DOWN longitudinal study. J Sports Sci. 2020;38(7):780–6.
OECD. PISA 2012 results: what makes schools successful (volume IV) 2013.
Hynynen ST, van Stralen MM, Sniehotta FF, Araújo-Soares V, Hardeman W, Chinapaw MJM, et al. A systematic review of school-based interventions targeting physical activity and sedentary behaviour among older adolescents. Int Rev Sport Exerc Psychol. 2016;9(1):22–44.
Guirado T, Chambonnière C, Chaput J-P, Metz L, Thivel D, Duclos M. Effects of classroom active desks on children and adolescents’ physical activity, sedentary behavior, academic achievements and overall health: a systematic review. Int J Env Res Pub He. 2021;18(6):2828.
Minges KE, Chao AM, Irwin ML, Owen N, Park C, Whittemore R, et al. Classroom standing desks and sedentary behavior: a systematic review. Pediatrics. 2016;137(2):e20153087.
McMichan L, Gibson A-M, Rowe DA. Classroom-based physical activity and sedentary behavior interventions in adolescents: a systematic review and meta-analysis. J Phys Act Health. 2018;15(5):383–93.
Podnar H, Jurić P, Karuc J, Saez M, Barceló MA, Radman I, et al. Comparative effectiveness of school-based interventions targeting physical activity, physical fitness or sedentary behaviour on obesity prevention in 6-to 12-year-old children: a systematic review and meta-analysis. Obes Rev. 2021;22(2):e13160.
Sherry AP, Pearson N, Clemes SA. The effects of standing desks within the school classroom: a systematic review. Prev Med Rep. 2016;3:338–47.
Parrish A-M, Chong KH, Moriarty AL, Batterham M, Ridgers ND. Interventions to change school recess activity levels in children and adolescents: a systematic review and meta-analysis. Sports Med. 2020:1–29.
Watson A, Timperio A, Brown H, Best K, Hesketh KD. Effect of classroom-based physical activity interventions on academic and physical activity outcomes: a systematic review and meta-analysis. Int J Behav Nutr Phys Act. 2017;14(1):1–24.
Saunders TJ, Rollo S, Kuzik N, Demchenko I, Bélanger S, Brisson-Boivin K, et al. School-Related Sedentary Behaviour Recommendations. https://ijbnpa.biomedcentral.com/articles/10.1186/s12966-022-01259-3.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Bmj. 2021;372:89.
Schardt C, Adams MB, Owens T, Keitz S, Fontelo P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med Inform Decis Mak. 2007;7(1):1–6.
Guyatt G, Oxman AD, Akl EA, Kunz R, Vist G, Brozek J, et al. GRADE guidelines: 1. Introduction—GRADE evidence profiles and summary of findings tables. J Clin Epidemiol. 2011;64(4):383–94.
Guyatt GH, Oxman AD, Sultan S, Glasziou P, Akl EA, Alonso-Coello P, et al. GRADE guidelines: 9. Rating up the quality of evidence. J Clin Epidemiol. 2011;64(12):1311–6.
Poitras VJ, Gray CE, Janssen X, Aubert S, Carson V, Faulkner G, et al. Systematic review of the relationships between sedentary behavior and health indicators in the early years (aged 0-4 years). BMC Public Health. 2017;17(5):868.
Saunders TJ, McIsaac T, Douillette K, Gaulton N, Hunter S, Rhodes RE, et al. Sedentary behaviour and health in adults: an overview of systematic reviews. Appl Physiol Nutr Metab. 2020;45(10 (Suppl. 2):S197–217.
Guyatt GH, Oxman AD, Kunz R, Atkins D, Brozek J, Vist G, et al. GRADE guidelines: 2. Framing the question and deciding on important outcomes. J Clin Epidemiol. 2011;64(4):395–400.
Higgins J. Cochrane handbook for systematic reviews of interventions. Version 5.1. 0 [updated march 2011]. The Cochrane collaboration. www cochrane-handbook org; 2011.
Guyatt GH, Oxman AD, Vist G, Kunz R, Brozek J, Alonso-Coello P, et al. GRADE guidelines: 4. Rating the quality of evidence—study limitations (risk of bias). J Clin Epidemiol. 2011;64(4):407–15.
Aadland KN, Ommundsen Y, Anderssen SA, Bronnick KS, Moe VF, Resaland GK, et al. Effects of the active smarter kids (ASK) physical activity school-based intervention on executive functions: a cluster-randomized controlled trial. Scand J Educ Res. 2019;63(2):214–28.
Farajian P, Panagiotakos DB, Risvas G, Malisova O, Zampelas A. Hierarchical analysis of dietary, lifestyle and family environment risk factors for childhood obesity: the GRECO study. Eur J Clin Nutr. 2014;68(10):1107–12.
Gilchrist JD, Battista K, Patte KA, Faulkner G, Carson V, Leatherdale ST. Effects of reallocating physical activity, sedentary behaviors, and sleep on mental health in adolescents. Ment Health Phys Act. 2021;20:100380.
Hunter S, Leatherdale ST, Carson V. The 3-year longitudinal impact of sedentary behavior on the academic achievement of secondary school students. J Sch Health. 2018;88(9):660–8.
Magriplis E, Farajian P, Panagiotakos DB, Risvas G, Zampelas A. The relationship between behavioral factors, weight status and a dietary pattern in primary school aged children: the GRECO study. Clin Nutr. 2019;38(1):310–6.
Patte KA, Qian W, Leatherdale ST. Modifiable predictors of insufficient sleep durations: a longitudinal analysis of youth in the COMPASS study. Prev Med. 2018;106:164–70.
Resaland GK, Aadland E, Moe VF, Aadland KN, Skrede T, Stavnsbo M, et al. Effects of physical activity on schoolchildren's academic performance: the active smarter kids (ASK) cluster-randomized controlled trial. Prev Med. 2016;91:322–8.
Clemes SA, Barber SE, Bingham DD, Ridgers ND, Fletcher E, Pearson N, et al. Reducing children's classroom sitting time using sit-to-stand desks: findings from pilot studies in UK and Australian primary schools. J Public Health (Oxf). 2016;38(3):526–33.
Jakubec L, Fromel K, Chmelik F, Groffik D. Physical activity in 15-17-year-old adolescents as compensation for sedentary behavior in school. Int J Env Res Pub He. 2020;17(9):3281.
Pengpid S, Peltzer K. Overweight and obesity and associated factors among school-aged adolescents in six pacific island countries in Oceania. Int J Env Res Pub He. 2015;12(11):14505–18.
Pengpid S, Peltzer K. Underweight and overweight or obesity and associated factors among school-going adolescents in five ASEAN countries, 2015. Diabetes Metab Syndr. 2019;13(6):3075–80.
van Stralen MM, Yildirim M, Wulp A, te Velde SJ, Verloigne M, Doessegger A, et al. Measured sedentary time and physical activity during the school day of European 10- to 12-year-old children: the ENERGY project. J Sci Med Sport. 2014;17(2):201–6.
Meyer U, Schindler C, Zahner L, Ernst D, Hebestreit H, Van Mechelen W, et al. Long-term effect of a school-based physical activity program (KISS) on fitness and adiposity in children: a cluster-randomized controlled trial. PLoS One. 2014;9(2):e87929.
Seljebotn PH, Skage I, Riskedal A, Olsen M, Kvalo SE, Dyrstad SM. Physically active academic lessons and effect on physical activity and aerobic fitness. The active school study: a cluster randomized controlled trial. Prev Med Rep. 2019;13:183–8.
Muller UM, Walther C, Adams V, Mende M, Adam J, Fikenzer K, et al. Long term impact of one daily unit of physical exercise at school on cardiovascular risk factors in school children. Eur J Prev Cardiol. 2016;23(13):1444–52.
Parrish A-M, Trost SG, Howard SJ, Batterham M, Cliff D, Salmon J, et al. Evaluation of an intervention to reduce adolescent sitting time during the school day: the ‘Stand up for Health’ randomised controlled trial. J Sci Med Sport. 2018;21(12):1244–9.
Cronholm F, Rosengren BE, Karlsson C, Karlsson MK. A comparative study found that a seven-year school-based exercise programme increased physical activity levels in both sexes. Acta Paediatr. 2018;107(4):701–7.
Contardo Ayala AM, Salmon J, Timperio A, Sudholz B, Ridgers ND, Sethi P, et al. Impact of an 8-month trial using height-adjustable desks on children’s classroom sitting patterns and markers of cardio-metabolic and musculoskeletal health. Int J Env Res Pub He. 2016;13(12):1227.
Contardo Ayala AM, Sudholz B, Salmon J, Dunstan DW, Ridgers ND, Arundell L, et al. The impact of height-adjustable desks and prompts to break-up classroom sitting on adolescents’ energy expenditure, adiposity markers and perceived musculoskeletal discomfort. PLoS One. 2018;13(9):e0203938.
Chesham RA, Booth JN, Sweeney EL, Ryde GC, Gorely T, Brooks NE, et al. The daily mile makes primary school children more active, less sedentary and improves their fitness and body composition: a quasi-experimental pilot study. BMC Med. 2018;16(1):64.
Maume DJ. Social relationships and the sleep-health nexus in adolescence: evidence from a comprehensive model with bi-directional effects. Sleep Health. 2017;3(4):284–9.
Rutten C, Boen F, Seghers J. Changes in physical activity and sedentary behavior during the transition from elementary to secondary school. J Phys Act Health. 2014;11(8):1607–13.
Lee EY, Kang B, Yang Y, Yang HK, Kim H-S, Lim S-Y, et al. Study time after school and habitual eating are associated with risk for obesity among overweight Korean children: a prospective study. Obes Facts. 2018;11(1):46–55.
Cheung PC, Franks PA, Kramer MR, Kay CM, Drews-Botsch CD, Welsh JA, et al. Elementary school physical activity opportunities and physical fitness of students: a statewide cross-sectional study of schools. PLoS One. 2019;14(1):e0210444.
Compernolle S, Van Dyck D, De Cocker K, Palarea-Albaladejo J, De Bourdeaudhuij I, Cardon G, et al. Differences in context-specific sedentary behaviors according to weight status in adolescents, adults and seniors: a compositional data analysis. Int J Env Res Pub He. 2018;15(9):1916.
Ishihara T, Morita N, Nakajima T, Okita K, Sagawa M, Yamatsu K. Modeling relationships of achievement motivation and physical fitness with academic performance in Japanese schoolchildren: moderation by gender. Physiol Behav. 2018;194:66–72.
Sanders T, Parker PD, del Pozo-Cruz B, Noetel M, Lonsdale C. Type of screen time moderates effects on outcomes in 4013 children: evidence from the longitudinal study of Australian children. Int J Behav Nutr Phys Act. 2019;16:117.
Zhang T, Cai L, Ma L, Jing J, Chen Y, Ma J. The prevalence of obesity and influence of early life and behavioral factors on obesity in Chinese children in Guangzhou. BMC Public Health. 2016;16(100968562):954.
Zhang Y, Zhang D, Li X, Ip P, Ho F, Jiang Y, et al. Daily time-use patterns and obesity and mental health among primary school students in Shanghai: a population-based cross-sectional study. Sci Rep. 2017;7(1):16200.
da Costa BGG, da Silva KS, Malheiros LEA, Minatto G, de Lima LRA, Petroski EL. Are adolescents really being sedentary or inactive when at school? An analysis of sedentary behaviour and physical activity bouts. Eur J Pediatr. 2018;177(11):1705–10.
Hubbard K, Economos CD, Bakun P, Boulos R, Chui K, Mueller MP, et al. Disparities in moderate-to-vigorous physical activity among girls and overweight and obese schoolchildren during school- and out-of-school time. Int J Behav Nutr Phys Act. 2016;13:39.
Rajala K, Kankaanpaa A, Laine K, Itkonen H, Goodman E, Tammelin T. Associations of subjective social status with accelerometer-based physical activity and sedentary time among adolescents. J Sports Sci. 2019;37(2):123–30.
Xue H, Tian G, Duan R, Quan L, Zhao L, Yang M, et al. Sedentary behavior is independently related to fat mass among children and adolescents in South China. Nutrients. 2016;8(11):667.
Khan MMA, Karim M, Islam AZ, Islam MR, Khan HTA, Khalilullah MI. Prevalence of overweight and obesity among adolescents in Bangladesh: do eating habits and physical activity have a gender differential effect? J Biosoc Sci. 2019;51(6):843–56.
Gu X, Zhang T, Chen S, Keller MJ, Zhang X. School-based sedentary behavior, physical activity, and health-related outcomes among hispanic children in the United States: a cross-sectional study. Int J Env Res Pub He. 2020;17(4):1197.
Ren H, Zhou Z, Liu WK, Wang X, Yin Z. Excessive homework, inadequate sleep, physical inactivity and screen viewing time are major contributors to high paediatric obesity. Acta Paediatr, Int J Paediatr. 2017;106(1):120–7.
Kantanista A, Osinski W. Underweight in 14 to 16 year-old girls and boys: prevalence and associations with physical activity and sedentary activities. Ann Agric Environ Med. 2014;21(1):114–9.
Michaud I, Chaput J-P, O'Loughlin J, Tremblay A, Mathieu M-E. Long duration of stressful homework as a potential obesogenic factor in children: a QUALITY study. Obesity. 2015;23(4):815–22.
Sigmund E, Sigmundova D, Hamrik Z, Geckova AM. Does participation in physical education reduce sedentary behaviour in school and throughout the day among normal-weight and overweight-to-obese Czech children aged 9-11 years? Int J Env Res Pub He. 2014;11(1):1076–93.
Gopinath B, Hardy LL, Kifley A, Baur LA, Mitchell P. Activity behaviors in schoolchildren and subsequent 5-yr change in blood pressure. Med Sci Sports Exerc. 2014;46(4):724–9.
Pitchford NJ, Chigeda A, Hubber PJ. Interactive apps prevent gender discrepancies in early-grade mathematics in a low-income country in sub-Sahara Africa. Dev. 2019;22(5):e12864.
Calvert HG, Barcelona JM, Melville D, Turner L. Effects of acute physical activity on NIH toolbox-measured cognitive functions among children in authentic education settings. Ment Health Phys Act. 2019;17:100293.
Norris E, Shelton N, Dunsmuir S, Duke-Williams O, Stamatakis E. Virtual field trips as physically active lessons for children: a pilot study. BMC Public Health. 2015;15(100968562):366.
Altenburg TM, Chinapaw MJM, Singh AS. Effects of one versus two bouts of moderate intensity physical activity on selective attention during a school morning in Dutch primary schoolchildren: a randomized controlled trial. J Sci Med Sport. 2016;19(10):820–4.
Pitchford NJ. Development of early mathematical skills with a tablet intervention: a randomized control trial in Malawi. Front Psychol. 2015;6:485.
Pitchford NJ, Outhwaite LA. Secondary benefits to attentional processing through intervention with an interactive maths app. Front Psychol. 2019;10:2633.
Hassler Hallstedt M, Ghaderi A. Tablets instead of paper-based tests for young children? Comparability between paper and tablet versions of the mathematical Heidelberger Rechen test 1-4. Educ Assess. 2018;23(3):195–210.
Frangou S-M, Wikgren J, Sintonen S, Kairaluoma L, Vasari P. The effect of writing modality on recollection in children and adolescents. Res Learn Technol. 2019;27:2239.
Sherry AP, Pearson N, Ridgers ND, Johnson W, Barber SE, Bingham DD, et al. Impacts of a standing desk intervention within an english primary school classroom: a pilot controlled trial. Int J Env Res Pub He. 2020;17(19):1–19.
Wick K, Faude O, Manes S, Zahner L, Donath L. I can stand learning: a controlled pilot intervention study on the effects of increased standing time on cognitive function in primary school children. Int J Env Res Pub He. 2018;15(2):356.
Hanghoj T, Lieberoth A, Misfeldt M. Can cooperative video games encourage social and motivational inclusion of at-risk students? Br J Educ Technol. 2018;49(4):775–99.
Corder K, Atkin AJ, Bamber DJ, Brage S, Dunn VJ, Ekelund U, et al. Revising on the run or studying on the sofa: prospective associations between physical activity, sedentary behaviour, and exam results in British adolescents. Int J Behav Nutr Phys Act. 2015;12:106.
Aggio D, Smith L, Fisher A, Hamer M. Context-specific associations of physical activity and sedentary behavior with cognition in children. Am J Epidemiol. 2016;183(12):1075–82.
Rasberry CN, Tiu GF, Kann L, McManus T, Michael SL, Merlo CL, et al. Health-related behaviors and academic achievement among high school students - United States, 2015. MMWR Morb Mortal Wkly Rep. 2017;66(35):921–7.
Peiro-Velert C, Valencia-Peris A, Gonzalez LM, Garcia-Masso X, Serra-Ano P, Devis-Devis J. Screen media usage, sleep time and academic performance in adolescents: clustering a self-organizing maps analysis. PLoS One. 2014;9(6):e99478.
Huang X, Zeng N, Ye S. Associations of sedentary behavior with physical fitness and academic performance among chinese students aged 8-19 years. Int J Env Res Pub He. 2019;16(22):4494.
Tang S, Patrick ME. Technology and interactive social media use among 8th and 10th graders in the U.S. and associations with homework and school grades. Comput Hum Behav. 2018;86:34–44.
Wang S, Hao X, Ma X, Yu Y, Wu L, Wang Y, et al. Associations between poor vision, vision-related behaviors and mathematics achievement in chinese students from the cnaeq-peh 2015. Int J Env Res Pub He. 2020;17(22):1–19.
Esteban-Cornejo I, Martinez-Gomez D, Sallis JF, Cabanas-Sanchez V, Fernandez-Santos J, Castro-Pinero J, et al. Objectively measured and self-reported leisure-time sedentary behavior and academic performance in youth: the UP&DOWN study. Prev Med. 2015;77:106–11.
Yamada M, Sekine M, Tatsuse T, Asaka Y. Association between lifestyle, parental smoke, socioeconomic status, and academic performance in Japanese elementary school children: the super diet education project. Environ Health Prev Med. 2019;24(1):22.
Fernandez-Alonso R, Alvarez-Diaz M, Suarez-Alvarez J, Muniz J. Students’ achievement and homework assignment strategies. Front Psychol. 2017;8:286.
Ee J, Parry S, de Oliveira BIR, McVeigh JA, Howie E, Straker L. Does a classroom standing desk intervention modify standing and sitting behaviour and musculoskeletal symptoms during school time and physical activity during waking time? Int J Env Res Pub He. 2018;15(8):1668.
Ku PW, Steptoe A, Lai YJ, Hu HY, Chu D, Yen YF, et al. The associations between near visual activity and incident myopia in children: a nationwide 4-year follow-up study. Ophthalmology. 2019;126(2):214–20.
Zhang X, Wang Y, Pan C, Yang W, Xiang Y, Yang J, et al. Effect of genetic-environmental interaction on Chinese childhood myopia. J Ophthalmol. 2020;2020:6308289.
Gelfand AA, Pavitt S, Ross AC, Szperka CL, Irwin SL, Bertisch S, et al. Later high school start time is associated with lower migraine frequency in adolescents. Headache. 2020;61(2):343–50.
Singh NK, James RM, Yadav A, Kumar R, Asthana S, Labani S. Prevalence of myopia and associated risk factors in schoolchildren in North India. Optometry Vision Sci. 2019;96(3):200–5.
Shan Z, Deng G, Li J, Li Y, Zhang Y, Zhao Q. How schooling and lifestyle factors effect neck and shoulder pain? A cross-sectional survey of adolescents in China. Spine. 2014;39(4):E276–E83.
Harris C, Straker L, Pollock C, Smith A. Children, computer exposure and musculoskeletal outcomes: the development of pathway models for school and home computer-related musculoskeletal outcomes. Ergonomics. 2015;58(10):1611–23.
Dianat I, Alipour A, Asgari JM. Risk factors for neck and shoulder pain among schoolchildren and adolescents. J Paediatr Child Health. 2018;54(1):20–7.
Gheysvandi E, Dianat I, Heidarimoghadam R, Tapak L, Karimi-Shahanjarini A, Rezapur-Shahkolai F. Neck and shoulder pain among elementary school students: prevalence and its risk factors. BMC Public Health. 2019;19(1):1299.
Guan H, Yu NN, Wang H, Boswell M, Shi Y, Rozelle S, et al. Impact of various types of near work and time spent outdoors at different times of day on visual acuity and refractive error among Chinese school-going children. PLoS One. 2019;14(4):e0215827.
Martinez-Lopez EJ, Hita-Contreras F, Moral-Garcia JE, Grao-Cruces A, Ruiz JR, Redecillas-Peiro MT, et al. Association of low weekly physical activity and sedentary lifestyle with self-perceived health, pain, and well-being in a Spanish teenage population. Sci Sports. 2015;30(6):342–51.
Yu B, Dai L, Sun W, Chen J, Du L, Deng N, et al. Prenatal and neonatal factors for the development of childhood visual impairment in primary and middle school students: a cross-sectional survey in Guangzhou, China. BMJ Open. 2020;10(9):e032721.
Zhang Y, Deng G, Zhang Z, Zhou Q, Gao X, Di L, et al. A cross sectional study between the prevalence of chronic pain and academic pressure in adolescents in China (Shanghai). BMC Musculoskelet Disord. 2015;16(100968565):219.
Riley N, Lubans DR, Morgan PJ, Young M. Outcomes and process evaluation of a programme integrating physical activity into the primary school mathematics curriculum: the EASY minds pilot randomised controlled trial. J Sci Med Sport. 2015;18(6):656–61.
Bartholomew JB, Golaszewski NM, Jowers E, Korinek E, Roberts G, Fall A, et al. Active learning improves on-task behaviors in 4th grade children. Prev Med. 2018;111:49–54.
Grieco LA, Jowers EM, Errisuriz VL, Bartholomew JB. Physically active vs. sedentary academic lessons: a dose response study for elementary student time on task. Prev Med. 2016;89:98–103.
Babic MJ, Smith JJ, Morgan PJ, Eather N, Plotnikoff RC, Lubans DR. Longitudinal associations between changes in screen-time and mental health outcomes in adolescents. Ment Health Phys Act. 2017;12:124–31.
Carlson JA, Engelberg JK, Cain KL, Conway TL, Mignano AM, Bonilla EA, et al. Implementing classroom physical activity breaks: associations with student physical activity and classroom behavior. Prev Med. 2015;81:67–72.
Hamer M, Yates T, Sherar LB, Clemes SA, Shankar A. Association of after school sedentary behaviour in adolescence with mental wellbeing in adulthood. Prev Med. 2016;87:6–10.
da Costa BGG, Chaput JP, Lopes MVV, da Costa RM, Malheiros LEA, Silva KS. Association between lifestyle behaviors and health-related quality of life in a sample of Brazilian adolescents. Int J Env Res Pub He. 2020;17(19):1–11.
Calpbinici P, Tas AF. Virtual behaviors affecting adolescent mental health: the usage of internet and mobile phone and cyberbullying. J Child Adolesc Psychiatr Nurs. 2019;32(3):139–48.
Xu F, Chen G, Stevens K, Zhou H, Qi S, Wang Z, et al. Measuring and valuing health-related quality of life among children and adolescents in mainland China - a pilot study. PLoS One. 2014;9(2):e89222.
Anez E, Fornieles-Deu A, Fauquet-Ars J, Lopez-Guimera G, Punti-Vidal J, Sanchez-Carracedo D. Body image dissatisfaction, physical activity and screen-time in Spanish adolescents. J Health Psychol. 2018;23(1):36–47.
Ellis WE, Dumas TM, Forbes LM. Physically isolated but socially connected: psychological adjustment and stress among adolescents during the initial COVID-19 crisis. Can J Behav Sci / Rev Can Sci Comportement. 2020;52(3):177–87.
Lin IH, Ko C-H, Chang Y-P, Liu T-L, Wang P-W, Lin H-C, et al. The association between suicidality and internet addiction and activities in Taiwanese adolescents. Compr Psychiatry. 2014;55(3):504–10.
Lushington K, Wilson A, Biggs S, Dollman J, Martin J, Kennedy D. Culture, extracurricular activity, sleep habits, and mental health: a comparison of senior high school Asian-Australian and Caucasian-Australian adolescents. Int J Forensic Ment Health. 2015;44(1–2):139–57.
Ekstrom A, Ostenberg AH, Bjorklund G, Alricsson M. The effects of introducing Tabata interval training and stability exercises to school children as a school-based intervention program. Int J Adolesc Med Health. 2019;31(4):20170043.
Kolle E, Solberg RB, Safvenbom R, Dyrstad SM, Berntsen S, Resaland GK, et al. The effect of a school-based intervention on physical activity, cardiorespiratory fitness and muscle strength: the School in Motion cluster randomized trial. Int J Behav Nutr Phys Act. 2020;17(1):154.
Harris BH, Chen W. Technology-enhanced classroom activity breaks impacting children's physical activity and fitness. J Clin Med. 2018;7(7):165.
Burns RD, Kim Y, Byun W, Brusseau TA. Associations of school day sedentary behavior and physical activity with gross motor skills: use of compositional data analysis. J Phys Act Health. 2019;16(10):811–7.
Reznik M, Wylie-Rosett J, Kim M, Ozuah PO. A classroom-based physical activity intervention for urban kindergarten and first-grade students: a feasibility study. Child Obes. 2015;11(3):314–24.
Wells NM, Myers BM, Henderson CR. School gardens and physical activity: a randomized controlled trial of low-income elementary schools. Prev Med. 2014;69(Suppl):S27–33.
Ridgers ND, Lamb KE, Timperio A, Brown H, Salmon J. Investigating children’s short-term responses to imposed or restricted physical activity. J Phys Act Health. 2018;15(4):239–46.
Silva DR, Minderico CS, Pinto F, Collings PJ, Cyrino ES, Sardinha LB. Impact of a classroom standing desk intervention on daily objectively measured sedentary behavior and physical activity in youth. J Sci Med Sport. 2018;21(9):919–24.
Verloigne M, Ridgers ND, De Bourdeaudhuij I, Cardon G. Effect and process evaluation of implementing standing desks in primary and secondary schools in Belgium: a cluster-randomised controlled trial. Int J Behav Nutr Phys Act. 2018;15:94.
Kariippanon KE, Cliff DP, Okely AD, Parrish A-M. Flexible learning spaces reduce sedentary time in adolescents. J Sci Med Sport. 2019;22(8):918–23.
Rees-Punia E, Holloway A, Knauft D, Schmidt MD. Effects of school gardening lessons on elementary school children's physical activity and sedentary time. J Phys Act Health. 2017;14(12):959–64.
Sudholz B, Contardo Ayala AM, Timperio A, Dunstan DW, Conroy DE, Abbott G, et al. The impact of height-adjustable desks and classroom prompts on classroom sitting time, social, and motivational factors among adolescents. J Sport Health Sci. 2020. In Press, Corrected Proof.
Galle F, Pecoraro P, Calella P, Cerullo G, Imoletti M, Mastantuono T, et al. Classroom active breaks to increase children's physical activity: a cross-sectional study in the province of Naples, Italy. Int J Env Res Pub He. 2020;17(18):1–10.
Schneller MB, Schipperijn J, Nielsen G, Bentsen P. Children's physical activity during a segmented school week: results from a quasi-experimental education outside the classroom intervention. Int J Behav Nutr Phys Act. 2017;14:80.
Moller NC, Tarp J, Kamelarczyk EF, Brond JC, Klakk H, Wedderkopp N. Do extra compulsory physical education lessons mean more physically active children - findings from the childhood health, activity, and motor performance school study Denmark (the CHAMPS-study DK). Int J Behav Nutr Phys Act. 2014;11:121.
Kidokoro T, Shimizu Y, Edamoto K, Annear M. Classroom standing desks and time-series variation in sedentary behavior and physical activity among primary school children. Int J Env Res Pub He. 2019;16(11):1892.
Morton KL, Corder K, Suhrcke M, Harrison F, Jones AP, van Sluijs EMF, et al. School polices, programmes and facilities, and objectively measured sedentary time, LPA and MVPA: associations in secondary school and over the transition from primary to secondary school. Int J Behav Nutr Phys Act. 2016;13:54.
Tokiya M, Kaneita Y, Itani O, Jike M, Ohida T. Predictors of insomnia onset in adolescents in Japan. Sleep Med. 2017;38:37–43.
Brunetti VC, O'Loughlin EK, O'Loughlin J, Constantin E, Pigeon E. Screen and nonscreen sedentary behavior and sleep in adolescents. Sleep Health. 2016;2(4):335–40.
Yeo SC, Jos AM, Erwin C, Lee SM, Lee XK, Lo JC, et al. Associations of sleep duration on school nights with self-rated health, overweight, and depression symptoms in adolescents: problems and possible solutions. Sleep Med. 2019;60(100898759):96–108.
Sharma B, Chavez RC, Nam EW. Prevalence and correlates of insufficient physical activity in school adolescents in Peru. Rev Saude Publica. 2018;52(0135043, t5x):51.
Burns RD, Brusseau TA, Fang Y, Myrer RS, Fu Y, Hannon JC. Predictors and grade level trends of school day physical activity achievement in low-income children from the U.S. Prev Med Rep. 2015;2:868–73.
Jaafar J, Shaaban J, Rahman RA, Noor NM. Physical activity and its associated factors among adolescents in secondary schools in northeast peninsular Malaysia. Indian J Public Health Res Dev. 2020;11(7):1345–51.
Chen T, Wu Z, Shen Z, Zhang J, Shen X, Li S. Sleep duration in Chinese adolescents: biological, environmental, and behavioral predictors. Sleep Med. 2014;15(11):1345–53.
Jiang X, Hardy LL, Baur LA, Ding D, Wang L, Shi H. Sleep duration, schedule and quality among urban Chinese children and adolescents: associations with routine after-school activities. PLoS One. 2015;10(1):e0115326.
Li S, Yang Q, Chen Z, Jin X, Jiang F, Shen X. Homework schedule: an important factor associated with shorter sleep duration among Chinese school-aged children. Behav Sleep Med. 2014;12(5):389–97.
Sun W-q, Spruyt K, Chen W-j, Jiang Y-r, Schonfeld D, Adams R, et al. The relation among sleep duration, homework burden, and sleep hygiene in Chinese school-aged children. Behav Sleep Med. 2014;12(5):398–411.
Widome R, Berger AT, Lenk KM, Erickson DJ, Laska MN, Iber C, et al. Correlates of short sleep duration among adolescents. J Adolesc. 2019;77:163–7.
Street NW, McCormick MC, Austin SB, Slopen N, Habre R, Molnar BE. Examining family and neighborhood level predictors of sleep duration in urban youth. Fam Syst Health. 2018;36(4):439–50.
Poitras VJ, Gray CE, Borghese MM, Carson V, Chaput J-P, Janssen I, et al. Systematic review of the relationships between objectively measured physical activity and health indicators in school-aged children and youth. Appl Physiol Nutr Metab. 2016;41(6):S197–239.
Chaput J-P, Gray C, Poitras V, Carson V, Gruber R, Birken C, et al. Systematic review of the relationships between sleep duration and health indicators in school-aged children and youth. Appl Physiol Nutr Metab. 2016;41(6):S266–S82.
Gray C, Gibbons R, Larouche R, Sandseter EBH, Bienenstock A, Brussoni M, et al. What is the relationship between outdoor time and physical activity, sedentary behaviour, and physical fitness in children? A systematic review. Int J Env Res Pub He. 2015;12(6):6455–74.
Xiong S, Sankaridurg P, Naduvilath T, Zang J, Zou H, Zhu J, et al. Time spent in outdoor activities in relation to myopia prevention and control: a meta-analysis and systematic review. Acta Ophthalmol. 2017;95(6):551–66.
Kondo MC, Jacoby SF, South EC. Does spending time outdoors reduce stress? A review of real-time stress response to outdoor environments. Health Place. 2018;51:136–50.
Dhawan S. Online learning: a panacea in the time of COVID-19 crisis. J Educ Technol Syst. 2020;49(1):5–22.
Button KS, Ioannidis JP, Mokrysz C, Nosek BA, Flint J, Robinson ES, et al. Power failure: why small sample size undermines the reliability of neuroscience. Nat Rev Neurosci. 2013;14(5):365–76.
Acknowledgements
We would like to thank Iryna Demchenko, Kara Brisson-Boivin, Marsha Costello, Chris Markham, Michelle Ponti, Maribeth Rogers Neale, Tony van Rooij for contributing to the conceptualization of this manuscript and planning of the methodology.
Funding
JS is supported by a National Health and Medical Research Council Investigator Grant (APP 1176885), this funding did not influence the design of the study and collection, analysis, and interpretation of data and in writing this manuscript.
Author information
Authors and Affiliations
Contributions
All authors contributed to the conceptualization of this manuscript and planning of the methodology. NK, BGGC, YH, and SV screened all relevant articles, extracted data, and assessed risk of bias for individual studies. TS acted as a third reviewer when a discrepancy for study exclusion/inclusion existed between two reviewers. NK synthesized main results, while BGGC, YH, and SV created supplementary tables. NK drafted the manuscript and all authors contributed to the review and revision of the final paper. All authors have approved the manuscript and consented for submission.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
TS has received honoraria for public talks on the health impacts of sedentary behaviour and physical activity for both children and adults. KW and WYH are associate editors for IJBNPA. MST is Founder, Chair and Leader of the Sedentary Behaviour Research Network, but receives no compensation or financial benefit in this capacity.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Kuzik, N., da Costa, B.G.G., Hwang, Y. et al. School-related sedentary behaviours and indicators of health and well-being among children and youth: a systematic review. Int J Behav Nutr Phys Act 19, 40 (2022). https://doi.org/10.1186/s12966-022-01258-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12966-022-01258-4