
Abstract
Lung cancer is a deeply malignant tumor with high incidence and mortality. Despite the rapid development of diagnosis and treatment technology, abundant patients with lung cancer are still inevitably faced with recurrence and metastasis, contributing to death. Lymphatic metastasis is the first step of distant metastasis and an important prognostic indicator of non-small cell lung cancer. Tumor-induced lymphangiogenesis is involved in the construction of the tumor microenvironment, except promoting malignant proliferation and metastasis of tumor cells, it also plays a crucial role in individual response to treatment, especially immunotherapy. Thus, this article reviews the current research status of lymphatic metastasis in non-small cell lung cancer, in order to provide some insights for the basic research and clinical and translational application in this field.
Similar content being viewed by others

Introduction
Lung cancer ranks as the leading cause of cancer-related deaths [1]. Non-small cell lung cancer (NSCLC) accounts for approximately 85% lung cancer [2]. Despite the advanced medical treatments now available, the long-term prognosis is still disillusionary. Patients who underwent surgery at an early stage are still susceptible to metastasis or recurrence [3, 4]. In NSCLC, lymph node (LN) metastasis is the most primary and crucial metastatic route [5, 6]. Clinical treatment and prognosis also depend on the extent of local LN involvement, known as ‘N-stage‘ [7, 8]. This may be due to the presence of occult micrometastatic cancer cells prior to diagnosis and surgery, which include LN micrometastasis [4, 9].
In human body, the two fundamental roles of lymphatic vessels are fluid transport and immunosurveillance [10]. Lymphatic vascular system can transport fluids, cells, and biomolecules between peripheral tissues and the circulatory system, maintaining tissue homeostasis [11]. Initial lymphatic vessels are lined by a single layer of lymphatic endothelial cells (LECs) in button-like junctions, with a discontinuous basement membrane that lacks smooth muscle cells [12]. Unidirectional and blunt-ended initial lymphatic capillaries uptake extravasated interstitial fluid (ISF) rich in leukocytes, lipids and proteins and form lymph, which is then transported into collecting lymphatic vessels. The endothelial cells of the collecting lymphatic vessels are connected in tighter zipper-like junctions and surrounded by smooth muscle cells, and have special valves prevented retrograde flow [13, 14] (Fig. 1). Lymph drains various antigens and activated antigen-presenting cells to LNs, while delivering immune cells and response factors back to bloodstream [12]. Lymphatic system can actively promotes tumor cells migrating to lymphatic vessels [15], meanwhile tumor-derived growth factors stimulate intratumoral and peritumoral lymphangiogenesis, facilitating lymphovascular invasion (LVI) to remodel tumor microenvironment (TME) [16]. Cancer cells that invade lymphatic vessels spread into tumor-draining lymph nodes (TDLN) to induce neo-lymphangiogenesis. Sprouting and proliferation of LECs mediate lymphatic expansion in tumor-draining LNs [17]. This constitutes an intermediate platform for lymphatic metastasis of cancer cells, formatting the lymphatic pre-metastasis ecological niche and creating a favorable microenvironment for metastasis [18](Figure.1). In recent years, immunotherapy has brought wish to patients with advanced NSCLC, while the immunotherapy effect of different populations seems to be different, and the expression of programmed death 1 (PD-1)/ programmed death ligand 1 (PD-L1) is the main drug reference index in clinical practice [19]. As an important component of TME, lymphatic system functions an important role in regulating immune response [20].We summarized some interesting genes, which regulated lymphatic metastasis of NSCLC, exerted synergistic role in immunotherapy at the same time. They seems to have great potential to be used as prognostic indicators for evaluating immunotherapy and synergistic therapeutic targets just like tumor anti-angiogenesis therapy [21, 22]. Lymphatic metastasis have been reported in other carcinomas, such as breast cancer [23], ovarian cancer [24], cervical cancer [25], prostate cancer [26], bladder cancer [27], liver cancer [28], gastric cancer [29], pancreatic cancer [30], colorectal cancer [31] and so on, however, the mechanism of lymphatic metastasis in NSCLC has not been systematically reviewed. Understanding the mechanism of tumor-associated lymphangiogenesis is of great significance in prognosis and therapeutic target identification in patients with NSCLC lymphatic metastasis.

The structure of lymphatic system and tumor-associated lymphatic metastasis in NSCLC. (A) Initial lymphatic vessel (LV) is lined by a single layer of LECs without a continuous basement membrane to uptake ISF and macromolecules by the blood vessels. LECs produce the chemokine gradients of CCL21 to entry immune cells expressing CCR7 into initial LV. (B) The lymphatic flow reaches TDLN though afferent LV, where the lymph permeates in subcapsular and medullary sinuses and eventually come into the efferent LV. Tumor cells, leukocyte, migratory dendritic cells (DCs), antigens, tumor-derived secreted factors (TDSFs), and tumor-derived extracellular vesicles (EVs) drain the subcapsular sinuses (SCS). Newborn LECs create and maintain chemokine gradients that direct DC migration. And CD169 + SCS macrophages capture tumor-derived material for antigen presentation. These culminate a pre-micrometastasis niche that crosses metastasis and immunity supporting tumor cell proliferation, adhesion, invasion, and LN immune suppression. (C) Various cells, including tumor cells, secrete growth factors to activate receptors on the LEC surface to regulate LEC growth and migration and remodel LV networks. Lymphangiogenesis-mediating receptors involve ligands or interacting proteins, homologous receptors, and specific LECs markers
Lymphatic vascular markers
During embryonic development, the formation of lymphatic vessels occurs after that of blood vessels. Venous endothelial cells express high levels of vascular endothelial growth factor receptor (VEGFR) -3 and upregulate LYVE-1 expression. The transcription factor SOX-18 interacts with the venous nuclear receptor COUP-TFII to express the lymphatic vessel specific TF Prox-1. Prox-1 in turn activates vascular endothelial growth factor (VEGF) -C-mediated VEGFR-3 expression to form stable lymphatic endothelial progenitor cells [15]. Subsequently, LECs express co-receptor Neuropilin-2 (NRP-2) synergistically sensitizing VEGF-C signaling. Under a VEGF-C concentration gradient, LECs express other specific markers, such as the transmembrane glycoprotein podoplanin(PDPN) and adhesion molecules, separating venous and lymphatic vessels [32, 33]. It was testified that LEC-specific marker genes expressed robustly in sequencing samples and distinct gene expression profiles in different LN LECs were modified by a similar pattern [17].
Except happening during embryonic development, the growth of new lymphatic vessels is induced in pathological circumstance.
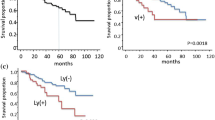
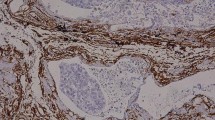
Lymphatic vascular density (LVD) is used as an evaluation index for lymphangiogenesis [34], in addition, various LECs-specific endothelial markers have been used to evaluate tumor-associated lymphangiogenesis by immunohistochemical methods, including Prox-1 [34], VEGFR-3 [35, 36], LVYE-1 [37], Podoplanin [34], D2-40 [38, 39], NRP-2 [40] and others (Fig. 1). Numerous studies have shown the expression of VEGF-C/-D and VEGFR-3 positively correlated with LVI, LVD, and lymph node metastasis (LNM) in NSCLC [41, 42]. Peritumor had higher VEGF-C and VEGF-D expression and were associated with more advanced regional LNM [35]. In lung adenocarcinoma (LUAD), LVD is higher in the tumor stroma of PNPD + tissue [34], while in lung squamous cell carcinoma (LSCC), podoplanin does not promote cell migration, but also down-regulates VEGF-C by regulating JNK pathway [35]. Many markers affecting LNM in NSCLC were also associated with clinicopathological factors and prognosis (Table 1).
Main signaling factors and their receptors of lymphangiogenesis in NSCLC
The central to lymphangiogenesis is the proliferation and migration of LECs. In NSCLC, LECs mediate lymphatic vessel formation and meanwhile contribute to the acquisition of a metastatic phenotype by cancer cells. Various secretory factors are induced to express and promote LECs-mediated lymphangiogenesis and lymphatic metastasis (Fig. 2; Table 2).

Main signaling pathways and major therapeutic targets contributing to lymphangiogenesis and lymphatic metastasis in NSCLC. In NSCLC, tumor cells induce the secretion of various factors that promote LECs-mediated lymphangiogenesis. Meanwhile this process contributes to the acquisition of the aggressive phenotypes, such as proliferation, migration, invasion, EMT, drug-resistance, and apoptosis in cancer cells
VEGF
VEGF family belongs to the platelet-derived growth factor supergene family, which has a vital function in numerous physiological and pathological processes, especially angiogenesis and lymphangiogenesis. It encompasses seven homodimeric proteins, namely VEGF-A, VEGF-B, VEGF-C, VEGF-D, VEGF-E (virally encoded), VEGF-F (Snake venom VEGF) and placental growth factor (PIGF) [43, 44]. In the past we have focused a great deal of attention on the role of VEGF-A in regulating angiogenesis due to its important role in tumor homeostasis and metastasis [45]. Although VEGF-A also plays a role in tumor lymphangiogenesis, the VEGF-C/D/VEGFR-3 axis is currently recognized as a central molecular mechanism and major driver of lymphangiogenesis [46, 47]. VEGF-C and VEGF-D can be derived from various cells, including tumor cells, immune cells, etc [12]. VEGF-C and VEGF-D are upregulated in NSCLC and interact with VEGFR-3 to activate the MAPK/ERK or PI3K/AKT pathways, to stimulate LECs proliferation, migration and tube formation [48, 49]. Only lymphangiogenesis makes use of VEGFR-3 activation by VEGF-C/-D. Angiogenesis does not require this activation. VEGF-C has a substantially higher affinity for VEGFR-3, even though it can also bind to the VEGFR-2 on blood vascular endothelium in mature form. VEGFR-3 may also have a function in blood vessel formation by regulating VEGFR-2-mediated signaling [50].
In some studies, no angiogenesis was induced in the lesions despite growing LNs showing hypoxic markers [51]. Mineral dust-induced gene (Mdig), an oxygen-sensitive protein, might boost tumor growth and angiogenesis through activation of EGFR/VEGF-A/VEGF-R1/R2 pathway, it impeded lymphangiogenesis by blocking the HIF-1α/VEGF-C/D/VEGFR-3 axis [52]. Upon hypoxia, HIF-1α induced CCAAT/enhancer binding protein-δ (C/EBP-δ) to stabilize HIF-1α, forming a positive feedback mechanism. C/EBP-δ could regulate VEGF-C autocrine signaling through HIF-1α to promoted the transport of LECs and lymphatic vessel network generation in vitro [53].
NRP-2, a membrane coreceptor, was a significant molecular regulator of VEGFR-3 activation [54]. Transforming growth factor-β (TGF-β) signaling preferentially increased the abundance of NRP-2b, enhancing cellular migration, invasion, and tumorsphere formation in NSCLC [55]. When triggered by the corresponding ligand EphrinB2, the EphB4 receptor enhanced the internalization of VEGF-C/R-3 [56]. EFNA4, a member of the ephrin (EPH) family and encoded Ephrin A4 as the ligand for Eph receptors. It was upregulated in lung cancer patients with LNM and overexpression of EFNA4 contributed to the proliferation, migration and adhesion of lung tumor cells [57].
Some classical pathways of angiogenesis have been shown to play an important role in mediating lymphangiogenesis. As well, VEGF-A was proved to involve regulating and independently initiating lymphangiogenesis [58]. Higher expression of VEGF-A and VEGFR-3 has been proved associated with LNM in lung cancer cells [59], one study discovered the independence of VEGF-A-stimulated lymphangiogenesis, which is not exclusively dominated by VEGF-C/D [60]. The adipokine angiopoietin-like protein 2 (ANGPTL2) is an extracellular ligand for the angiopoietin receptor Tie2, its expression was upregulated in NSCLC with LNM and positively correlated with VEGF-A expression [61]. In hypoxic conditions, it has the potential to trigger the expression of HIF-1α and boost the abundance of both VEGF-A and ANGPTL2 [62]. In another study, ANGPTL2 was found to mediate VEGF-A-dependent LEC tube formation and migration through the integrin α5β1/p38/NF-κB pathway [63]. ANGPTL2 could also promote M2 polarization of tumor-associated macrophages (TAMs) through NF-κB pathway to enhance proliferation, invasion, migration of NSCLC cells and tube formation of LECs [64]. While VEGF-A appeared to correlate negatively with LNM in tumor mesenchyme, which might suggest the influence of tumor-mesenchymal interactions in lymphatic metastasis of NSCLC [59]. In addition, the formation of the lymphatic vasculature depends on the agonist role of Ang-2, and serum Ang-2 levels were associated with tumor dissemination and lymphatic invasion. The levels of Ang-2 were higher in patients with LNM in NSCLC [65, 66].
Other growth factors
Platelet-derived growth factors (PDGFs) and their receptors, PDGFRs, are important factors affecting LNM in lung cancer [67]. PDGF-A was discovered to be paracrine by stimulating PDGFR-expressing LECs in tumor cells, co-expression of PDGF-B and VEGFR-3 in lung cancer tissues was connected with LNM and poor prognosis [68, 69]. Another study found that PDGF-B, PDGFR-β, and LMVD expression in tissues correlated with lymphatic metastasis, and was also highly correlated with elevated levels of platelet [70]. This implied that platelet secreted cytokines such as PDGFs to promote lymphangiogenesis. Meanwhile, platelet itself promoted tumor cell proliferation and metastasis. It prolonged the abnormal aggregation and survival of tumor cells in the peripheral circulation and guided in their immune escape. Studies found that elevated platelet counts (even when the counts were in the normal range) were significantly associated with higher rates of LNM. This mean that anti-platelet therapy might be a peculiar way to manage lymphangiogenesis and tumor progression in NSCLC patients [71, 72].
As well, the hepatocyte growth factors (HGFs) and its receptor c-Met were highly expressed in NSCLC. HGF-α/c-Met might synergize with the VEGF-C pathway in inducing lymphangiogenesis [73]. Noticeably, NRP-2b specifically promoted HGF-induced p-AKT, whereas inhibition of c-MET attenuated NRP-2b-dependent cells migration [55]. Insulin-like growth factor binding protein 7 (IGFBP7) expression was associated with metastatic clinicopathologic features and high LVD in NSCLC. It was also effective in enhancing LEC tubular structure formation and LNM [74]. Furthermore, the co-expressions of fibroblast growth factor 2 (FGF2) /VEGFR-3 and FGFR-1/PDGF-B in tumor cells were also significant predictors of a poor prognosis [75].
Other mechanisms
As mentioned above, some genes might regulate growth factors such as VEGF-C through some pathways, but there were also other molecules and pathways that appear to be directly associated with NSCLC lymphangiogenesis. Shh and Gli1 in the sonic hedgehog (Shh) signaling pathway were significantly correlated with the expression of LYVE-1. Shh signaling pathway initiated LNM through LYVE-1-dependent lymphangiogenesis [76]. Overexpressed STAT3 was an independent LN micrometastasis risk factor and promoted micrometastasis in early-stage NSCLC [77]. Similarly, the expression of SCC-S2 was also linked with LNM in associated analysis [78]. Overexpression of SCP3 was found to be positively correlated with VEGF-C and VEGF-D and predicted poor prognosis in patients with LNM [79]. There was also a potential link between Syk and VEGF-C in LUAD [80], low Syk expression predicted a poorer independent prognosis [81, 82].
Moreover, an increasing number of non-coding RNAs have been demonstrated to regulate lymphangiogenesis. LECs absorbed EV-packaged circTLCD4-RWDD3, which stimulated Prox-1 transcription and induced lymphangiogenesis and LNM in NSCLC. The process of sorting of circTLCD4-RWDD3 into EVs was induced by SUMOylation of hnRNPA2B1, which could activate ALIX to recruit ESCRT-III [83]. In another way, it was identified the first LEC-specific long non-coding RNA, LETR1, could regulate critical targets involved in LEC survival and growth, which deserved to be explored in NSCLC in the future [84]. Similar effects were found in microRNA (miRNA/miR). MiR-128 were significantly downregulated in NSCLC tissues and cells, overexpressed MiR-128significantly curbed VEGF-C expression, which in turn restricted VEGFR-3-induced activation of ERK, p38, and AKT signaling pathways [85]. MiR-22 also negatively regulated VEGFR-3 to mediate lymphangiogenesis [86].
Tumor cells-LECs-TME crosstalk in NSCLC lymphatic metastasis
TME with chemokines and other cytokines
Patients in NSCLC with LNM have a stronger interplay network in the TME. Crosstalk between cancer cells and types of stromal cells in tumor tissue may lead to a specific metastasis microenvironment while contributing to LNM [87]. VEGF-C is a strong chemoattractant for macrophages and other inflammatory cells, which generate VEGF-C and influence the TME [54]. Tumor cells secrete other paracrine signaling molecules that function in parallel to VEGFR-3 to facilitate the recruitment of LVs. VEGF-C-mediated chemokines and their receptors are common factors mediating interactions in TME. When silencing VEGF-C, it had an inhibitory effect on the expression of VEGFR-2, VEGFR-3, CXCR4, and CCR7, and regulated tumor cells proliferation and invasion through AKT, ERK, and p38 signaling pathways [88]. CCR7 interacting with its ligands functioned in the directional migration of lymphocytes transporting and homing to LNs during tumor immune responses [89]. In metastatic lung cancer cell lines, overexpression of CCR7 greatly promoted VEGF-D expression and was regulated by the ERK1/2 and AKT signaling pathways [49]. In addition, TNF-α could activate NF-κB pathway in LECs to promote their secretion of CCL21 and promote metastasis and invasion of lung cancer cells through the CCR7-CCL21 axis. After specific antagonism of the NF-κB pathway with PDTC, CCL21 secretion was significantly reduced, and lung cancer cell metastasis was also reduced in the co-culture system of LECs and lung cancer cells [90].
So are the inflammatory factors, interleukin (IL)-7 induced the generation of c-Fos/c-Jun heterodimers through IL-7 receptor (IL-7R), which facilitated the binding of transcription factor AP-1 to the VEGF-D promoter [91, 92]. IL-17 upregulated VEGF-C levels in NSCLC cells through the p-ERK1/2 kinase pathway, which enhanced LECs chemotaxis and endothelial cord formation [93, 94]. IL-1α expression was enhanced and high levels of VEGF-A, VEGF-C, and VEGF-D were detected in macrophages in the tumor stroma. IL-1-driven inflammatory signaling induces CXC chemokines via cancer cells leading to M2-type macrophage recruitment [95]. The expression of COX-2 and VEGF-C levels was significantly increased in several highly metastatic lung cancer cell lines, COX-2-mediated VEGF-C expression dependent on the endogenous PGE2 pathway mediated by the EP1/4 receptor [96, 97]. Reactive oxygen modulator 1 (Romo1), which induced reactive oxygen species in mitochondria, affected cancer cell invasion and proliferation through sustained inflammation. Romo1 could induce lymphatic metastasis in NSCLC by modulating sustained inflammation/VEGF signaling [98]. Lipopolysaccharide (LSP) induced Thymic stromal lymphopoietin (TSLP) release from human lung macrophages (HLMs), which process could be enhanced by Th2 cytokine IL-4. Incubation of HLMs with TSLP induced the release of TNF-α, VEGF-A, angiopoietin 2 and VEGF-C, indicating the role of TSLP system in lymphangiogenesis through a Th2-dependent pathway in lung cancer and other chronic inflammatory disorders [99]. What’s more, contingency signals such as hyperthermia and oxidative stress stimulated the transcription factor LEDGF/p75 to activate VEGF-C signaling transcription, in order to control structural changes in the lymphovascular system [100]. In inflammatory environment, neutrophils could also increase the bioavailability and bioactivity of VEGF-A by secreting MMP-9 and heparanase, while secreting VEGF-D at a low extent to promote lymphangiogenesis [101].
Immune microenvironment
TDLN is the specific site of tumor-induced tolerance. Primary tumors colonize LNs, which then influence the innate and adaptive immune system to advance the tumor [102]. LVs promote tumor metastasis and may increase anti-tumor effects by boosting tumor-associated antigens presentation to the immune system [103]. Immune surveillance occurs in the LNs by activating antigen-specific helper CD4 + T cells, cytotoxic CD8 + T cells and decoy receptors. Then it produces cytokines and other controlled immune responses to target cancer cells. Tumors induce immunosuppression by activating macrophages to help establish TME, promoting expression of suppressor molecules by cancer cells, and down-regulating cytotoxic T-lymphocytes (CTL). Metastatic LNs usually fail to construct effective anti-tumor immunity and can alter the sensitivity of cancer cells to immune surveillance [16, 104, 105].
High tumor mutational burden and PD-L1 expression in NSCLC were linked to enhanced intratumoral immune cell infiltration and LVI [106]. Tumor-infiltrating CD8 + T cells become dysfunctional and more immunosuppressive. PD-1 + CD + 8 T lymphocytes might be immune checkpoint blockade (ICB) -responsive and essential for anti-tumor immunity [107,108,109]. Moreover, host regulatory T cells (Treg) could induce conversion of naive tumor antigen-specific CD4 + T cells into anergy and peripherally induced Tregs in a genetically engineered lung adenocarcinoma mouse model. By specifically targeting Tregs, antitumor immune responses could be further enhanced by reducing the production of anergic T cells and releasing the brake on effector immunological response [110]. In metastatic LNs of primary NSCLC patients, PD-L1 + CSCs modulated the immune system by influencing affecting T-cell frequency and phenotype. PD-L1 + CSCs were positively correlated with Tregs, PD-1 + CD4 + T, and Tim3 + CD4 + T. PD-L1 + CSCs had an immunosuppressive potential, which correlated with LNM, progressed lung cancer, poor prognosis, and drug resistance [105].
The immune microenvironment is also inextricably linked to the inflammatory manifestations of tumors. Immune-infiltrated NSCLC cells had high expression of soluble immune suppressive factors indoleamine 2,3-dioxygenase 1 (IDO1) and PD-1. IDO1 was higher expressed in inflamed tumors and tertiary lymphoid structures (TLS), a robust predictor of immune checkpoint inhibitors (ICI) efficacy. In a T-cell-inflamed TME and/or TLS, targeting IDO pathway combining anti-PD-1/PD-L1, might be a potential target to reinvigorate TLS-driven antitumor immunity [111]. TLS maturation is also associated with major pathological response, and being an independent predictor for DFS in resectable neoadjuvant chemoimmunotherapy (anti-PD-1 antibody plus chemotherapy) [112]. Removal of the mediastinal lymph nodes (MLN) increased the anti-tumoral activity of NK cell and reversed its exhaustion [113]. Meanwhile, MLN removal could improve immunosenescent phenotype, immune checkpoint receptor expression, and cytotoxicity by CTLs [114].
The interference of tumor lymphangiogenesis by macrophage polarization intervene also provides a new perspective on personalized treatment. Mouse macrophages (predominantly infiltrated M2-like TAMs) treated with Paclitaxel (PTX) triggered lymphatic vascular activity in naive tumor cells in a VEGF-C/VEGFR-3-dependent manner, which facilitated LEC invasiveness and migratory properties [115]. Macrophages expressing VEGFR-3 stimulated tumor metastasis by releasing the histone cathepsin, which enhanced the activity of the heparanase. Thus, blocking the VEGF-C/VEGFR3 axis in activated macrophages not only directly inhibited lymphangiogenesis but also blocked the pro-metastatic activity of macrophages in mice after chemotherapy [115]. Studies have shown that high VEGF-C with high M2 ratio (CD163+/CD68+) was an independent prognostic factor in NSCLC patients and significantly associated with angiogenesis and lymphangiogenesis [127].
TGF-β signaling ensured the structure integrity of lymphatic vessels and lymphatic homeostasis, encouraging tumor lymphatic metastasis in LECs [116]. In early LSCC, the expression of TGF-β1 in PDPN + CAFs was higher, which was correlated with CD204 + TAM infiltration, suggesting that it was related to the immunosuppressive microenvironment [117]. As mentioned above, TGF-β1 might work in the process of inducing EMT and promoting the acquisition of CSCs-like characteristics [118]. TGF-β-induced active demethylation could upregulate CD147, targeting CD147 methylation might be beneficial in preventing tumor invasion and metastasis [119].
Migration and distant metastatic of NSCLC cells
Epithelial-mesenchymal transition (EMT) and cell migration
LECs might regulate the migration and adhesion of tumor cells in addition to lymphangiogenesis. EMT is an important process in lymphatic dissemination and metastasis. EMT phenotype can be characterized by epithelial markers (E-Cadherin and β-Catenin) and mesenchymal markers (N-Cadherin and Vimentin) [120]. KAI1 inhibited β-Catenin-mediated EMT and played a metastatic inhibitory role during tumor invasion, angiogenesis, and lymphangiogenesis [121]. Downregulation of miR-148a was found to be associated with NSCLC LNM as well as shorter survival, DNMT1 expression was reduced by miR-148a overexpression, which resulted in decreased DNA methylation of E-Cadherin, leading to a rise in E-Cadherin protein levels [122]. In pathological N0 lymph nodes of NSCLC patients, micrometastatic tumor cells as well as positive expression of VEGF-C were analyzed. There was also a relationship between lymphangiogenesis, micrometastasis and adhesion molecules with specific histology (E- Cadherin, α/β/γ- Catenin) [123]. Transcription factors of EMT, SNAI2 and TWIST1, were also involved in lymph node progression, dependent on the TGF-β pathway partly [124, 125].
Inhibition of VEGF-C paracrine inhibited migration, invasion, and EMT in lung cancer cell lines and reduced the percentage of CSCs-like cells, reducing tumor drainage and cancer cell spread [41]. EMT promoted cancer progression by cancer stem cells (CSCs) forming that are more tumorigenic [55]. TGF-β might work in the process of inducing EMT and promoting the acquisition of CSCs-like characteristics, then upregulating VEGFR-3 expression [118]. Another study testified TGF-β exposure enhanced tumor cell adhesion and migration on LECs. In vivo experiments, targeting of TGF-β and integrin β3 significantly reduced LNM, suggesting a more effective combination therapy [126].
JAM-C promoted lymphangiogenesis and LNM by increasing the migratory capacity of cancer cells and modulating VEGF-C-mediated activation of integrinβ1 or ERK [48]. p-S6 was also significantly elevated in NSCLC patients with LNM. Inhibition of p-S6 reduced the migration and invasion of NSCLC cells [127].
Distant metastasis
We know that lymphangiogenesis is often accompanied by sentinel LNM [128]. While distant metastasis may also be derived from LN metastasis, or immunological tolerance induced by LN colonization. Lymphangiogenic metastatic sites exist in distant LNs or organs. It is extrapolated that the induction of lymphangiogenesis occurs at these metastatic sites, which further accelerates dissemination by transgenic mouse models in other tumors with metastases [11, 129]. Overexpression of VEGF-C in tumor cells encouraged intra-lymphatic spread of metastases. In clinical studies, we have found axillary lymph nodes being a rare site of LNM had a higher incidence of metastasis in BRAF mutated patients with NSCLC compared to those in non-BRAF mutated [130]. While whether the molecular mechanisms of lymphangiogenesis at distant metastasis are the same as the aforementioned need to be further explored in cancer models used in experiments.
Anti-lymphangiogenic therapy
It has long been appreciated that patients bearing LNM suffered poor prognosis compared with those lacking LNM. While the treatment paradigm for NSCLC has changed dramatically in the last decades. For resectable NSCLC, lobectomy with regional LN dissection is the primary treatment. While for locally advanced NSCLC, it is prone to combined with chemotherapy, immunotherapy, targeted therapy or radiotherapy as neoadjuvant therapies [131].
Systematic lymphadenectomy is an crucial component of complete surgical operation for resectable NSCLC [132,133,134]. In the case of small-sized NSCLC, a comprehensive LN dissection is advised during surgery [135]. However, it has been debatable whether lymphadenectomy is helpful for the overall survival of patients [132, 133]. Measures to improve the quality of LN dissection in NSCLC are still needed to explore in the future. For instance, techniques such as transcervical extended mediastinal lymphadenectomy (TEMLA) could improve the 5-year OS of patients with stage IIIA-IIIB (N2) NSCLC after neoadjuvant chemotherapy or chemoradiotherapy [136, 137]. The role of removing tumor draining LNs helps better understand immunotherapeutic approach.
Research data have showed immunotherapies had considerably improved the survival of patients with NSCLC, even at the end of life [138, 139]. Treating patients harboring PD-L1 + CSCs and PD-1 + CD4 + T cells with anti-PD-1/PD-L1 therapies might improve their prognosis [105]. Neoadjuvant immunotherapy elicited a substantial response in LNM and was more effective in LN downstaging [140]. In clinical trials, neoadjuvant pembrolizumab with chemotherapy followed by resection in resectable and early-stage NSCLC, or neoadjuvant nivolumab plus platinum-based chemotherapy in resectable and stage IIIA or IIIB NSCLC, both enjoyed better prognosis than with chemotherapy alone [141, 142].
Maximum standardized uptake (SUVmax) and mean standardized uptake (SUVmean) values were significantly higher in patients with LNM than in who without LNM before underwent preparative PET/CT for diagnosis and staging [143]. The prognosis of NSCLC patients could be predicted by combining the coefficient of variation (CoV) of 18 F-FDG PET/CT images of the primary tumors with the CoV of the targeted LNs [144]. A significant factor in determining a high degree of locoregional tumor control following definitive chemoradiotherapy, was the high sensitivity detection of involved LNs and their incorporation into the radiation target volume [145]. Combining anti-PD-1 blockade with radiotherapy could overcome immunotherapy resistance and strengthen the immune response. The InTRist study provided the strategy for anti-PD-1 toripalimab plus chemotherapy followed by concurrent chemoradiotherapy (cCRT) for bulky LA-NSCLC [146].
As an antibody targeting VEGF-A, bevacizumab combined with ICIs, with or without chemotherapy had been approved for the initial treatment of unresectable NSCLC [147]. However, studies on NSCLC lymphangiogenesis-specific targeted agents were still incomplete. Numerous studies on the molecular mechanisms of NSCLC lymphatic metastasis demonstrate the potential of lymphangiogenic therapeutic targets. Some drugs might delay the progression of NSCLC by modulating the tumor lymphangiogenic pathway (Fig. 2). Studies emerged on monoclonal antibodies (mAb) targeting VEGF-C/D [148, 149] and VEGFR-2/3 [150, 151], as well as soluble constructs of VEGFR-2/3 [152, 153]. These serve as anti-angiogenic targets and can also provide ideas for anti-lymphangiogenesis. Mice inoculated with Lewis lung cells (LLC) -sVEGFR-2 had significantly fewer LYVE-1 + lymphatic vessels and pulmonary lymph node micrometastases, and VEGFR-2, VEGFR-3, and MMP were inhibited. sVEGFR-2 could be a target for inhibiting the VEGF-C pathway that impedes lymphatic metastasis in NSCLC [154]. EGFR-TKIs (gefitinib, afatinib, and AZD9291) could inhibit VEGF-C secretion, further impairing the proliferation, migration, and tube formation of LECs. The three EGFR-TKIs reduced the expression of VEGFR-2/3, VEGF-C, and CCR7 through the JAK/STAT3 signaling pathway, FAK phosphorylation and c-Myc, this mechanism reduced NSCLC cell proliferation and metastasis to lymphatic vessels to prevent distant metastasis. Meanwhile, afatinib suppressed tumor growth and lymphangiogenesis in a dose-dependent manner in the xenograft mouse model [155]. The small molecule inhibitor Nintedanib blocked the structural domains of all FGFR, PDGFR, and VEGFR receptors by binding to ATP-binding sites in kinases. Animal studies demonstrated a significant reduction in intratumoral LVD treated with Nintedanib. Nintedanib inhibited VEGF-C-induced signaling blocking tumor lymphangiogenesis in NSCLC cells [156]. IL-1/IL-1R signaling driven inflammatory stimuli and upregulation of VEGF-C expression enhanced lymphangiogenesis. Experiments demonstrated that the IL-1R antagonist anakinra inhibited tumor growth, lymphangiogenesis, and LNM by suppressing VEGF-A and VEGF-C expression, and levels of CXC chemokines in macrophages co-cultured with highly metastatic cancer cells [95]. Bioinformatics analysis revealed that high expression of BIRC5/HIF1A/FLT4 was associated with primary NSCLC lymphangiogenesis and metastasis. Small molecule kinase inhibitor drugs have been shown to have better specificity, selectivity, and safety than conventional chemotherapeutic agents. Among them, the quinoline-derived small molecule HN-N07 inhibited the target genes BIRC5/HIF1A/FLT4, and became a potential inhibitor of the NSCLC cancer-causing signaling pathway [157]. Some of the growth factors and their receptors mentioned above, as well as other mechanistic targets, may be potential targets for LN-positive NSCLC. For example, aspirin reduces PDGF and VEGF levels in platelet release [158]. The COX-2-specific inhibitor Celecoxib led to a reduction in COX-2 and VEGF-C expression and LYVE-1-positive vessels [96]. This all requires further clinical trials to confirm the efficacy of pathway target inhibitors in NSCLC lymphatic metastasis.
Furin-like pro-protein convertases (FPPC), strongly upregulating in tumor cells, could cleave signaling protein semaphorin-3 C (sema3C), which induced cytoskeletal collapse in LECs. Whereas active point mutation of furin protease cleavage-resistant sema3C (FR-sema3C) inhibited VEGF-C-induced phosphorylation of VEGFR-3, ERK1/2, and AKT, which inhibited the proliferation of LECs. This suggested that full-length FR-sema3C may be further developed into a novel antitumor drug [159]. Itraconazole (ITCZ) was a potent inhibitor of endothelial cell proliferation and inhibits angiogenesis. It was found that expression of LMVD and VEGF-C were significantly reduced in the high-dose ITCZ group. It suggests that ITCZ may inhibit malignant pleural effusion by inhibiting lymphangiogenesis in mice [160].
Further, endobronchial endotumor chemotherapy was used through systemic radiotherapy or before surgery. Endotumor lymphatic therapy cloud be administered by using a needle catheter through a flexible bronchoscope to inject cisplatin or other cytotoxic agents, into malignant tissue located in the airway lumen or peribranchial structures. Eradication of micrometastases or occult metastases in regional LNs that migrate to the area of the draining tumor was achieved through prophylactic or therapeutic treatment [161]. In addition, siRNAs provide a method to silence specific oncogenes to control tumor growth. Tumor-targeting nanostructured lipid carriers improve the stability, solubility, and cell permeability of drugs and siRNAs. siRNA nanostructures, as an innovative way to meet clinical needs, can be introduced into a variety of therapeutic combinations [162]. The new technology provided new precision for the precise use of drugs for lymphatic vessels.
Conclusion
It is well known that NSCLC is a disease with poor prognosis, often accompanied by recurrence and metastasis, lymphatic metastasis is a common mode of metastasis for NSCLC. In recent years, researches on neoplastic lymphangiogenesis and LNM in NSCLC have made great progress. The evidence is compelling that the extent of LNM is crucial prognostic judgement for overall survival of patient in NSCLC. Tumor cells and other immune cells secrete cytokines and chemokines, regulating the generation of nascent ducts and promoting the invasion and metastasis in tumor lymphatic microenvironment. Numerous studies have analyzed the correlation between clinicopathological features and lymphatic vessel-related indicators. And there are already some standard quantifiable assays for identifying robustly expressed lymphatic vessel markers. However, currently commonly used markers, such as PDPN or LYVE-1, are also expressed epithelially on other cells or regulated by other factors, which can lead to experimental errors.
This review combed the pathways of NSCLC-regulated lymphatic vessel formation. This will help to understand the specific mechanisms of lymphatic vessel formation in the TME. Genomics, transcriptomics, and proteomics can help identify potential drivers and assist in predicting efficacy and prognosis. Single-cell sequencing techniques can also detect cell population heterogeneity to better understand the biological changes that occur with tumor-associated LNM.
Individualized combination therapies based on targeting and immunotherapy for NSCLC have been updated over the past decades. Drugs targeting angiogenesis have also gradually moved into a mature stage, particularly bevacizumab, have been approved for use in clinical treatment and have achieved good therapeutic effects, so the research of specific drugs targeting lymphangiogenesis has great potential. It is targeting key molecules in the lymphatic immune microenvironment and reversing tumor immunosuppression. By synergizing with immune checkpoint inhibitors and targeting suppressive immune cells to reduce tumor lymphatic vessel formation. In addition, the theory and practice of surgery and radiotherapy have been advancing. Precise and stabilized localizing of pivotal molecules in the lymphangiogenic pathway through si-RNA technology. All of this requires more prospective biomarker trials and extensive clinical trials. Identification of lymphoid markers as well as designing better experimental models to validate theories are all future endeavors. The future holds promise for the rationalization of combining anti-lymphangiogenic drugs with current targeted or immunological approaches.
Data availability
No datasets were generated or analysed during the current study.
Abbreviations
- NSCLC:
-
non-small cell lung cancer
- LN:
-
lymph node
- LECs:
-
lymphatic endothelial cells
- ISF:
-
interstitial fluid
- LSMCs:
-
lymphatic smooth muscle cells
- LV:
-
lymphatic vessel
- LVI:
-
lymphatic vessel invasion
- TME:
-
tumor microenvironment
- TDLN:
-
tumor-draining lymph nodes
- PD-1:
-
programmed death 1
- PD-L1:
-
programmed death ligand 1
- DCs:
-
dendritic cell
- TDSFs:
-
tumor-derived secreted factors
- EVs:
-
extracellular vesicles
- SCS:
-
subcapsular sinuses
- VEGF:
-
vascular endothelial growth factor
- VEGFR:
-
vascular endothelial growth factor receptor
- LYVE-1:
-
lymphatic vessel endothelial hyaluronan receptor-1
- SOX18:
-
sex-determining region Y-box 18
- COUP-TFII:
-
the chicken ovalbumin upstream promoter transcription factor II
- Prox-1:
-
Prospero homeobox-1 protein
- NRP-2:
-
Neuropilin-2
- PDPN:
-
podoplanin
- LVD:
-
Lymphatic vascular density
- ptLVD:
-
peritumor LVD
- LNM:
-
lymph node metastasis
- LUAD:
-
lung adenocarcinoma
- LSCC:
-
lung squamous cell carcinoma
- PIGF:
-
placental growth factor
- Mdig:
-
Mineral dust-induced gene
- C/EBP-δ:
-
CCAAT/enhancer binding protein-δ
- TGF-β:
-
transforming growth factor-β
- EPH:
-
ephrin
- ANGPTL2:
-
the adipokine angiopoietin-like protein 2
- TAMs:
-
tumor-associated macrophages
- PDGFs:
-
Platelet-derived growth factors
- HGFs:
-
hepatocyte growth factors
- IGFBP7:
-
insulin-like growth factor binding protein 7
- FGF2:
-
fibroblast growth factor 2
- Shh signaling pathway:
-
sonic hedgehog signaling pathway
- miRNA/mi-R:
-
microRNA
- OS:
-
overall survival
- RFS:
-
relapse-free survival
- DSS:
-
disease-specific survival
- DFS:
-
disease-free survival
- IL:
-
Interleukin
- IL-7R:
-
IL-7 receptor
- Romo1:
-
reactive oxygen modulator 1
- LSP:
-
Lipopolysaccharide
- TSLP:
-
Thymic stromal lymphopoietin
- HLMs:
-
human lung macrophages
- CTL:
-
cytotoxic T-lymphocytes
- ICB:
-
immune checkpoint blockade
- Treg:
-
regulatory T cells
- IDO1:
-
indoleamine 2,3-dioxygenase 1
- TLS:
-
tertiary lymphoid structures
- ICI:
-
immune checkpoint inhibitors
- MLN:
-
mediastinal lymph nodes
- PTX:
-
Paclitaxel
- EMT:
-
epithelial-mesenchymal transition
- CSCs:
-
cancer stem cells
- JAM-C:
-
junctional adhesion molecule-C
- TEMLA:
-
transcervical extended mediastinal lymphadenectomy
- CoV:
-
coefficient of variation
- cCRT:
-
concurrent chemoradiotherapy
- mAb:
-
monoclonal antibodies
- FPPC:
-
furin-like pro-protein convertases
- sema3C:
-
semaphorin-3 C
- FR-sema3C:
-
furin protease cleavage-resistant sema3C
- ITCZ:
-
Itraconazole
- HUVECs:
-
human umbilical vein–derived endothelial cells
- HLECs:
-
human lymphatic endothelial cells
- LLC:
-
Lewis lung cells
- 3LL:
-
Lewis lung adenocarcinoma cells
References
Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA Cancer J Clin. 2023;73:17–48.
Herbst RS, Morgensztern D, Boshoff C. The biology and management of non-small cell lung cancer. Nature. 2018;553:446–54.
Liang W, He J, Shen Y, Shen J, He Q, Zhang J, et al. Impact of examined Lymph Node count on Precise Staging and Long-Term Survival of Resected Non-small-cell Lung Cancer: a Population Study of the US SEER database and a Chinese multi-institutional Registry. J Clin Oncol off J Am Soc Clin Oncol. 2017;35:1162–70.
Wang C, Wu Y, Shao J, Liu D, Li W. Clinicopathological variables influencing overall survival, recurrence and post-recurrence survival in resected stage I non-small-cell lung cancer. BMC Cancer. 2020;20:150.
Paduch R. The role of lymphangiogenesis and angiogenesis in tumor metastasis. Cell Oncol Dordr. 2016;39:397–410.
Suhail Y, Cain MP, Vanaja K, Kurywchak PA, Levchenko A, Kalluri R, et al. Syst Biology Cancer Metastasis Cell Syst. 2019;9:109–27.
Dai C, Ren Y, Xie D, Zheng H, She Y, Fei K et al. Does Lymph Node Metastasis have a negative prognostic impact in patients with NSCLC and M1a disease? J Thorac Oncol off Publ Int Assoc Study Lung Cancer. 2016;11:1745–54.
Hwang JK, Page BJ, Flynn D, Passmore L, McCaul E, Brady J, et al. Validation of the Eighth Edition TNM Lung Cancer Staging System. J Thorac Oncol off Publ Int Assoc Study Lung Cancer. 2020;15:649–54.
Uramoto H, Tanaka F. Recurrence after surgery in patients with NSCLC. Transl Lung Cancer Res. 2014;3:242–9.
Norrmén C, Tammela T, Petrova TV, Alitalo K. Biological basis of therapeutic lymphangiogenesis. Circulation. 2011;123:1335–51.
Dieterich LC, Tacconi C, Ducoli L, Detmar M. Lymphatic vessels in cancer. Physiol Rev. 2022;102:1837–79.
Petrova TV, Koh GY. Biological functions of lymphatic vessels. Science. 2020;369:eaax4063.
Hu X, Luo J. Heterogeneity of tumor lymphangiogenesis: Progress and prospects. Cancer Sci. 2018;109:3005–12.
Alitalo K. The lymphatic vasculature in disease. Nat Med. 2011;17:1371–80.
Tammela T, Alitalo K, Lymphangiogenesis. Molecular mechanisms and future promise. Cell. 2010;140:460–76.
Oliver G, Kipnis J, Randolph GJ, Harvey NL. The lymphatic vasculature in the 21st Century: Novel Functional roles in Homeostasis and Disease. Cell. 2020;182:270–96.
Commerford CD, Dieterich LC, He Y, Hell T, Montoya-Zegarra JA, Noerrelykke SF, et al. Mechanisms of Tumor-Induced Lymphovascular Niche formation in draining Lymph Nodes. Cell Rep. 2018;25:3554–e35634.
Nagahashi M, Ramachandran S, Rashid OM, Takabe K. Lymphangiogenesis: a new player in cancer progression. World J Gastroenterol. 2010;16:4003–12.
Lahiri A, Maji A, Potdar PD, Singh N, Parikh P, Bisht B, et al. Lung cancer immunotherapy: progress, pitfalls, and promises. Mol Cancer. 2023;22:40.
Viúdez-Pareja C, Kreft E, García-Caballero M. Immunomodulatory properties of the lymphatic endothelium in the tumor microenvironment. Front Immunol. 2023;14:1235812.
Tu J, Liang H, Li C, Huang Y, Wang Z, Chen X, et al. The application and research progress of anti-angiogenesis therapy in tumor immunotherapy. Front Immunol. 2023;14:1198972.
Chen R, Manochakian R, James L, Azzouqa A-G, Shi H, Zhang Y, et al. Emerging therapeutic agents for advanced non-small cell lung cancer. J Hematol OncolJ Hematol Oncol. 2020;13:58.
To B, Isaac D, Andrechek ER. Studying lymphatic metastasis in breast Cancer: current models, strategies, and clinical perspectives. J Mammary Gland Biol Neoplasia. 2020;25:191–203.
Pal S, Bhowmick S, Sharma A, Sierra-Fonseca JA, Mondal S, Afolabi F, et al. Lymphatic vasculature in ovarian cancer. Biochim Biophys Acta Rev Cancer. 2023;1878:188950.
Li Y, Gao X, Huang Y, Zhu X, Chen Y, Xue L, et al. Tumor microenvironment promotes lymphatic metastasis of cervical cancer: its mechanisms and clinical implications. Front Oncol. 2023;13:1114042.
Wu P-Y, Lin Y-C, Huang Y-L, Chen W-M, Chen C-C, Lee H. Mechanisms of lysophosphatidic acid-mediated lymphangiogenesis in prostate Cancer. Cancers. 2018;10:413.
Liu S, Chen X, Lin T. Lymphatic metastasis of bladder cancer: molecular mechanisms, diagnosis and targeted therapy. Cancer Lett. 2021;505:13–23.
Roy S, Banerjee P, Ekser B, Bayless K, Zawieja D, Alpini G, et al. Targeting Lymphangiogenesis and Lymph Node Metastasis in Liver Cancer. Am J Pathol. 2021;191:2052–63.
Liu P, Ding P, Sun C, Chen S, Lowe S, Meng L, et al. Lymphangiogenesis in gastric cancer: function and mechanism. Eur J Med Res. 2023;28:405.
Fink DM, Steele MM, Hollingsworth MA. The lymphatic system and pancreatic cancer. Cancer Lett. 2016;381:217–36.
Huang C, Chen Y. Lymphangiogenesis and colorectal cancer. Saudi Med J. 2017;38:237–44.
Hu Z, Zhao X, Wu Z, Qu B, Yuan M, Xing Y, et al. Lymphatic vessel: origin, heterogeneity, biological functions, and therapeutic targets. Signal Transduct Target Ther. 2024;9:9.
Rezzola S, Sigmund EC, Halin C, Ronca R. The lymphatic vasculature: an active and dynamic player in cancer progression. Med Res Rev. 2022;42:576–614.
Xu S, Yang J, Xu S, Zhu Y, Zhang C, Liu L, et al. Lymphatic vessel density as a prognostic indicator in Asian NSCLC patients: a meta-analysis. BMC Pulm Med. 2018;18:128.
Ko YH, Jung C-K, Lee M-A, Byun JH, Kang JH, Lee KY, et al. Clinical significance of vascular endothelial growth factors (VEGF)-C and -D in resected non-small cell lung cancer. Cancer Res Treat. 2008;40:133–40.
Renyi-Vamos F, Tovari J, Fillinger J, Timar J, Paku S, Kenessey I, et al. Lymphangiogenesis correlates with lymph node metastasis, prognosis, and angiogenic phenotype in human non-small cell lung cancer. Clin Cancer Res off J Am Assoc Cancer Res. 2005;11:7344–53.
Jackson DG, Prevo R, Clasper S, Banerji S. LYVE-1, the lymphatic system and tumor lymphangiogenesis. Trends Immunol. 2001;22:317–21.
Jin S, Zhu W, Shi Q, Zhang Z, Guo R. Clinicopathological significance of lymphatic vessel density marked by D2-40 and E-cadherin expression in non-small-cell lung cancer. Med Oncol Northwood Lond Engl. 2012;29:3157–61.
Takanami I. Lymphatic microvessel density using D2-40 is associated with nodal metastasis in non-small cell lung cancer. Oncol Rep. 2006;15:437–42.
Wang J, Huang Y, Zhang J, Xing B, Xuan W, Wang H, et al. NRP-2 in tumor lymphangiogenesis and lymphatic metastasis. Cancer Lett. 2018;418:176–84.
Khromova N, Kopnin P, Rybko V, Kopnin BP. Downregulation of VEGF-C expression in lung and colon cancer cells decelerates tumor growth and inhibits metastasis via multiple mechanisms. Oncogene. 2012;31:1389–97.
Li Q, Dong X, Gu W, Qiu X, Wang E. Clinical significance of co-expression of VEGF-C and VEGFR-3 in non-small cell lung cancer. Chin Med J (Engl). 2003;116:727–30.
Ferreira IG, Pucca MB, de Oliveira IS, Cerni FA, Jacob B, de C S, Arantes EC. Snake venom vascular endothelial growth factors (svVEGFs): Unravelling their molecular structure, functions, and research potential. Cytokine Growth Factor Rev. 2021;60:133–43.
Patel SA, Nilsson MB, Le X, Cascone T, Jain RK, Heymach JV. Molecular mechanisms and future implications of VEGF/VEGFR in Cancer Therapy. Clin Cancer Res off J Am Assoc Cancer Res. 2023;29:30–9.
Apte RS, Chen DS, Ferrara N. VEGF in Signaling and Disease: Beyond Discovery and Development. Cell. 2019;176:1248–64.
Laakkonen P, Waltari M, Holopainen T, Takahashi T, Pytowski B, Steiner P, et al. Vascular endothelial growth factor receptor 3 is involved in tumor angiogenesis and growth. Cancer Res. 2007;67:593–9.
El-Chemaly S, Levine SJ, Moss J. Lymphatics in lung disease. Ann N Y Acad Sci. 2008;1131:195–202.
Hao S, Yang Y, Liu Y, Yang S, Wang G, Xiao J, et al. JAM-C promotes lymphangiogenesis and nodal metastasis in non-small cell lung cancer. Tumour Biol J Int Soc Oncodevelopmental Biol Med. 2014;35:5675–87.
Sun L, Zhang Q, Li Y, Tang N, Qiu X. CCL21/CCR7 up-regulate vascular endothelial growth factor-D expression via ERK pathway in human non-small cell lung cancer cells. Int J Clin Exp Pathol. 2015;8:15729–38.
Zhang L, Zhou F, Han W, Shen B, Luo J, Shibuya M, et al. VEGFR-3 ligand-binding and kinase activity are required for lymphangiogenesis but not for angiogenesis. Cell Res. 2010;20:1319–31.
Jeong H-S, Jones D, Liao S, Wattson DA, Cui CH, Duda DG, et al. Investigation of the lack of Angiogenesis in the formation of Lymph Node metastases. J Natl Cancer Inst. 2015;107:djv155.
Zhou H, Geng F, Chen Y, Du J, Zhang X, Liu B, et al. The mineral dust-induced gene, mdig, regulates angiogenesis and lymphangiogenesis in lung adenocarcinoma by modulating the expression of VEGF-A/C/D via EGFR and HIF-1α signaling. Oncol Rep. 2021;45:60.
Min Y, Ghose S, Boelte K, Li J, Yang L, Lin PC. C/EBP-δ regulates VEGF-C autocrine signaling in lymphangiogenesis and metastasis of lung cancer through HIF-1α. Oncogene. 2011;30:4901–9.
Kuonqui K, Campbell A-C, Sarker A, Roberts A, Pollack BL, Park HJ, et al. Dysregulation of lymphatic endothelial VEGFR3 signaling in Disease. Cells. 2023;13:68.
Gemmill RM, Nasarre P, Nair-Menon J, Cappuzzo F, Landi L, D’Incecco A, et al. The neuropilin 2 isoform NRP2b uniquely supports TGFβ-mediated progression in lung cancer. Sci Signal. 2017;10:eaag0528.
Wu B, Rockel JS, Lagares D, Kapoor M. Ephrins and eph receptor signaling in tissue repair and fibrosis. Curr Rheumatol Rep. 2019;21:23.
Zhao X, Chen Y, Sun X, He Z, Wu T, Wu C, et al. Oncogenic EFNA4 amplification promotes Lung Adenocarcinoma Lymph Node Metastasis. Cancers. 2022;14:4226.
Hirakawa S, Kodama S, Kunstfeld R, Kajiya K, Brown LF, Detmar M. VEGF-A induces tumor and sentinel lymph node lymphangiogenesis and promotes lymphatic metastasis. J Exp Med. 2005;201:1089–99.
Donnem T, Al-Shibli K, Al-Saad S, Delghandi MP, Busund L-T, Bremnes RM. VEGF-A and VEGFR-3 correlate with nodal status in operable non-small cell lung cancer: inverse correlation between expression in tumor and stromal cells. Lung Cancer Amst Neth. 2009;63:277–83.
Björndahl MA, Cao R, Burton JB, Brakenhielm E, Religa P, Galter D, et al. Vascular endothelial growth factor-a promotes peritumoral lymphangiogenesis and lymphatic metastasis. Cancer Res. 2005;65:9261–8.
Sasaki H, Suzuki A, Shitara M, Hikosaka Y, Okuda K, Moriyama S, et al. Angiopoietin-like protein ANGPTL2 gene expression is correlated with lymph node metastasis in lung cancer. Oncol Lett. 2012;4:1325–8.
Qin S, Yi M, Jiao D, Li A, Wu K. Distinct roles of VEGFA and ANGPT2 in lung adenocarcinoma and squamous cell carcinoma. J Cancer. 2020;11:153–67.
Liu P-I, Jiang Y-J, Chang A-C, Huang C-L, Fong Y-C, Guo J-H, et al. ANGPTL2 promotes VEGF-A synthesis in human lung cancer and facilitates lymphangiogenesis. Aging. 2023;15:1652–67.
Wei X, Nie S, Liu H, Sun J, Liu J, Li J, et al. Angiopoietin-like protein 2 facilitates non-small cell lung cancer progression by promoting the polarization of M2 tumor-associated macrophages. Am J Cancer Res. 2017;7:2220–33.
Xu Y, Zhang Y, Wang Z, Chen N, Zhou J, Liu L. The role of serum angiopoietin-2 levels in progression and prognosis of lung cancer: a meta-analysis. Med (Baltim). 2017;96:e8063.
Tsakogiannis D, Nikolakopoulou A, Zagouri F, Stratakos G, Syrigos K, Zografos E, et al. Update overview of the role of angiopoietins in Lung Cancer. Med Kaunas Lith. 2021;57:1191.
Papadopoulos N, Lennartsson J. The PDGF/PDGFR pathway as a drug target. Mol Aspects Med. 2018;62:75–88.
Liu J, Liu C, Qiu L, Li J, Zhang P, Sun Y. Overexpression of both platelet-derived growth factor-BB and vascular endothelial growth factor-C and its association with lymphangiogenesis in primary human non-small cell lung cancer. Diagn Pathol. 2014;9:128.
Donnem T, Al-Saad S, Al-Shibli K, Busund L-T, Bremnes RM. Co-expression of PDGF-B and VEGFR-3 strongly correlates with lymph node metastasis and poor survival in non-small-cell lung cancer. Ann Oncol. 2010;21:223–31.
Zhang N, Hu H, Fu Y, He F, Wang L, Zhuang S, et al. The overexpression of PDGF-BB and its receptor is correlated with lymphatic metastasis in patients with non-small cell lung cancer. Int J Clin Exp Pathol. 2018;11:6010–7.
Qu C-H, Li T, Tang Z-P, Zhu X-R, Han J-Y, Tian H. Platelet Count is Associated with the rate of Lymph Node Metastasis in Lung Adenocarcinoma. Cancer Manag Res. 2020;12:9765–74.
Liu HB, Gu XL, Ma XQ, Lv TF, Wu Y, Xiao YY, et al. Preoperative platelet count in predicting lymph node metastasis and prognosis in patients with non-small cell lung cancer. Neoplasma. 2013;60:203–8.
Zhang N, Xie F, Gao W, Yu S, Qiu L, Lin W, et al. Expression of hepatocyte growth factor and c-Met in non-small-cell lung cancer and association with lymphangiogenesis. Mol Med Rep. 2015;11:2797–804.
Zhao W, Wang J, Zhu B, Duan Y, Chen F, Nian W, et al. IGFBP7 functions as a potential lymphangiogenesis inducer in non-small cell lung carcinoma. Oncol Rep. 2016;35:1483–92.
Donnem T, Al-Shibli K, Al-Saad S, Busund L-T, Bremnes RM. Prognostic impact of fibroblast growth factor 2 in non-small cell lung cancer: coexpression with VEGFR-3 and PDGF-B predicts poor survival. J Thorac Oncol off Publ Int Assoc Study Lung Cancer. 2009;4:578–85.
Hwang J, Kang MH, Yoo YA, Quan YH, Kim HK, Oh SC, et al. The effects of sonic hedgehog signaling pathway components on non-small-cell lung cancer progression and clinical outcome. World J Surg Oncol. 2014;12:268.
Yu Y, Zhao Q, He X-P, Wang Z, Liu X-Y, Zhang Z-P. Signal transducer and activator of transcription 3 overexpression promotes lymph node micrometastasis in early-stage non-small cell lung cancer. Thorac Cancer. 2018;9:516–22.
Dong Q-Z, Zhao Y, Liu Y, Wang Y, Zhang P-X, Jiang G-Y, et al. Overexpression of SCC-S2 correlates with lymph node metastasis and poor prognosis in patients with non-small-cell lung cancer. Cancer Sci. 2010;101:1562–9.
Kitano H, Chung J-Y, Noh KH, Lee Y-H, Kim TW, Lee SH, et al. Synaptonemal complex protein 3 is associated with lymphangiogenesis in non-small cell lung cancer patients with lymph node metastasis. J Transl Med. 2017;15:138.
Sun Q, Peng C, Cong B, Hao Y, Guo J, Zhao Y, et al. Involvement of syk and VEGF-C in invasion of lung adenocarcinoma A549 cells. J Cancer Res Ther. 2016;12:640–4.
Liu L, Liu H, Luo S, Patz EF, Glass C, Su L, et al. Novel genetic variants of SYK and ITGA1 related lymphangiogenesis signaling pathway predict non-small cell lung cancer survival. Am J Cancer Res. 2020;10:2603–16.
Kowalczuk O, Laudanski J, Laudanski W, Niklinska WE, Kozlowski M, Niklinski J. Lymphatics-associated genes are downregulated at transcription level in non-small cell lung cancer. Oncol Lett. 2018;15:6752–62.
Diao X, Guo C, Zheng H, Zhao K, Luo Y, An M, et al. SUMOylation-triggered ALIX activation modulates extracellular vesicles circTLCD4-RWDD3 to promote lymphatic metastasis of non-small cell lung cancer. Signal Transduct Target Ther. 2023;8:426.
Ducoli L, Agrawal S, Sibler E, Kouno T, Tacconi C, Hon C-C, et al. LETR1 is a lymphatic endothelial-specific lncRNA governing cell proliferation and migration through KLF4 and SEMA3C. Nat Commun. 2021;12:925.
Hu J, Cheng Y, Li Y, Jin Z, Pan Y, Liu G, et al. microRNA-128 plays a critical role in human non-small cell lung cancer tumourigenesis, angiogenesis and lymphangiogenesis by directly targeting vascular endothelial growth factor-C. Eur J Cancer Oxf Engl 1990. 2014;50:2336–50.
Dong Z, Xu Q-H, Zhu Y-B, Wang Y-F, Xiong J, Dang S. Investigation of targeting relationship between micro-rna-22 and Vegfr3 in lung squamous cell carcinoma. Comb Chem High Throughput Screen. 2021;24:148–54.
Quail DF, Joyce JA. Microenvironmental regulation of tumor progression and metastasis. Nat Med. 2013;19:1423–37.
Feng Y, Hu J, Ma J, Feng K, Zhang X, Yang S, et al. RNAi-mediated silencing of VEGF-C inhibits non-small cell lung cancer progression by simultaneously down-regulating the CXCR4, CCR7, VEGFR-2 and VEGFR-3-dependent axes-induced ERK, p38 and AKT signalling pathways. Eur J Cancer Oxf Engl 1990. 2011;47:2353–63.
Salem A, Alotaibi M, Mroueh R, Basheer HA, Afarinkia K. CCR7 as a therapeutic target in Cancer. Biochim Biophys Acta Rev Cancer. 2021;1875:188499.
Zhang S, Wang H, Xu Z, Bai Y, Xu L. Lymphatic metastasis of NSCLC involves Chemotaxis effects of lymphatic endothelial cells through the CCR7-CCL21 Axis modulated by TNF-α. Genes. 2020;11:1309.
Jian M, Qingfu Z, Yanduo J, Guocheng J, Xueshan Q. Anti-lymphangiogenesis effects of a specific anti-interleukin 7 receptor antibody in lung cancer model in vivo. Mol Carcinog. 2015;54:148–55.
Ming J, Zhang Q, Qiu X, Wang E. Interleukin 7/interleukin 7 receptor induce c-Fos/c-Jun-dependent vascular endothelial growth factor-D up-regulation: a mechanism of lymphangiogenesis in lung cancer. Eur J Cancer Oxf Engl 1990. 2009;45:866–73.
Chen X, Xie Q, Cheng X, Diao X, Cheng Y, Liu J, et al. Role of interleukin-17 in lymphangiogenesis in non-small-cell lung cancer: enhanced production of vascular endothelial growth factor C in non-small-cell lung carcinoma cells. Cancer Sci. 2010;101:2384–90.
Chen X, Wan J, Liu J, Xie W, Diao X, Xu J, et al. Increased IL-17-producing cells correlate with poor survival and lymphangiogenesis in NSCLC patients. Lung Cancer Amst Neth. 2010;69:348–54.
Watari K, Shibata T, Kawahara A, Sata K, Nabeshima H, Shinoda A, et al. Tumor-derived interleukin-1 promotes lymphangiogenesis and lymph node metastasis through M2-type macrophages. PLoS ONE. 2014;9:e99568.
Liu H, Yang Y, Xiao J, Lv Y, Liu Y, Yang H, et al. COX-2-mediated regulation of VEGF-C in association with lymphangiogenesis and lymph node metastasis in lung cancer. Anat Rec Hoboken NJ. 2007;2010(293):1838–46.
Guo X, Chen Y, Xu Z, Xu Z, Qian Y, Yu X. Prognostic significance of VEGF-C expression in correlation with COX-2, lymphatic microvessel density, and clinicopathologic characteristics in human non-small cell lung cancer. Acta Biochim Biophys Sin. 2009;41:217–22.
Kim HJ, Jo MJ, Kim BR, Kim JL, Jeong YA, Na YJ, et al. Overexpression of Romo1 is an unfavorable prognostic biomarker and a predictor of lymphatic metastasis in non-small cell lung cancer patients. OncoTargets Ther. 2018;11:4233–46.
Braile M, Fiorelli A, Sorriento D, Di Crescenzo RM, Galdiero MR, Marone G, et al. Human lung-Resident Macrophages Express and are targets of thymic stromal lymphopoietin in the Tumor Microenvironment. Cells. 2021;10:2012.
Cohen B, Addadi Y, Sapoznik S, Meir G, Kalchenko V, Harmelin A, et al. Transcriptional regulation of vascular endothelial growth factor C by oxidative and thermal stress is mediated by lens epithelium-derived growth factor/p75. Neoplasia N Y N. 2009;11:921–33.
Tan KW, Chong SZ, Wong FHS, Evrard M, Tan SM-L, Keeble J, et al. Neutrophils contribute to inflammatory lymphangiogenesis by increasing VEGF-A bioavailability and secreting VEGF-D. Blood. 2013;122:3666–77.
Basto PA, Reticker-Flynn NE. Interrogating the roles of lymph node metastasis in systemic immune surveillance. Clin Exp Metastasis. 2024.
Kataru RP, Baik JE, Park HJ, Ly CL, Shin J, Schwartz N, et al. Lymphatic-specific intracellular modulation of receptor tyrosine kinase signaling improves lymphatic growth and function. Sci Signal. 2021;14:eabc0836.
Bui K, Hong Y-K. Ras pathways on Prox1 and lymphangiogenesis: insights for therapeutics. Front Cardiovasc Med. 2020;7:597374.
Raniszewska A, Vroman H, Dumoulin D, Cornelissen R, Aerts JGJV, Domagała-Kulawik J. PD-L1 + lung cancer stem cells modify the metastatic lymph-node immunomicroenvironment in nsclc patients. Cancer Immunol Immunother CII. 2021;70:453–61.
Mitchell KG, Negrao MV, Parra ER, Li J, Zhang J, Dejima H, et al. Lymphovascular Invasion is Associated with Mutational Burden and PD-L1 in Resected Lung Cancer. Ann Thorac Surg. 2020;109:358–66.
Yang G, Cai S, Hu M, Li C, Yang L, Zhang W, et al. Functional status and spatial architecture of tumor-infiltrating CD8 + T cells are associated with lymph node metastases in non-small cell lung cancer. J Transl Med. 2023;21:320.
Rahim MK, Okholm TLH, Jones KB, McCarthy EE, Liu CC, Yee JL, et al. Dynamic CD8 + T cell responses to cancer immunotherapy in human regional lymph nodes are disrupted in metastatic lymph nodes. Cell. 2023;186:1127–e114318.
Durgeau A, Virk Y, Corgnac S, Mami-Chouaib F. Recent advances in targeting CD8 T-Cell immunity for more effective Cancer immunotherapy. Front Immunol. 2018;9:14.
Alonso R, Flament H, Lemoine S, Sedlik C, Bottasso E, Péguillet I, et al. Induction of anergic or regulatory tumor-specific CD4 + T cells in the tumor-draining lymph node. Nat Commun. 2018;9:2113.
Bessede A, Peyraud F, Le Moulec S, Cousin S, Cabart M, Chomy F, et al. Upregulation of indoleamine 2,3-Dioxygenase 1 in Tumor cells and tertiary lymphoid structures is a Hallmark of Inflamed Non-small Cell Lung Cancer. Clin Cancer Res off J Am Assoc Cancer Res. 2023;29:4883–93.
Sun X, Liu W, Sun L, Mo H, Feng Y, Wu X, et al. Maturation and abundance of tertiary lymphoid structures are associated with the efficacy of neoadjuvant chemoimmunotherapy in resectable non-small cell lung cancer. J Immunother Cancer. 2022;10:e005531.
Cikman DI, Esen F, Engin A, Turna A, Agkoc M, Yilmaz A, et al. Mediastinal lymph node removal modulates natural killer cell exhaustion in patients with non-small cell lung cancer. Immunol Res. 2023;71:959–71.
Engin A, Turna A, Esen F, Agkoc M, Cikman DI, Saglam OF, et al. Mediastinal lymph node removal ameliorates cytotoxic T-lymphocyte functions in patients with non-small cell lung cancer. Tumori. 2023;109:97–104.
Alishekevitz D, Gingis-Velitski S, Kaidar-Person O, Gutter-Kapon L, Scherer SD, Raviv Z, et al. Macrophage-Induced Lymphangiogenesis and Metastasis following Paclitaxel Chemotherapy is regulated by VEGFR3. Cell Rep. 2016;17:1344–56.
Fukasawa K, Hanada K, Ichikawa K, Hirashima M, Takagi T, Itoh S, et al. Endothelial-specific depletion of TGF-β signaling affects lymphatic function. Inflamm Regen. 2021;41:35.
Suzuki J, Aokage K, Neri S, Sakai T, Hashimoto H, Su Y, et al. Relationship between podoplanin-expressing cancer-associated fibroblasts and the immune microenvironment of early lung squamous cell carcinoma. Lung Cancer Amst Neth. 2021;153:1–10.
Duan L, Ye L, Zhuang L, Zou X, Liu S, Zhang Y, et al. VEGFC/VEGFR3 axis mediates TGFβ1-induced epithelial-to-mesenchymal transition in non-small cell lung cancer cells. PLoS ONE. 2018;13:e0200452.
Liao C-G, Liang X-H, Ke Y, Yao L, Liu M, Liu Z-K, et al. Active demethylation upregulates CD147 expression promoting non-small cell lung cancer invasion and metastasis. Oncogene. 2022;41:1780–94.
Steinestel K, Eder S, Schrader AJ, Steinestel J. Clinical significance of epithelial-mesenchymal transition. Clin Transl Med. 2014;3:17.
Zhou L, Yu L, Wu S, Feng Z, Song W, Gong X. Clinicopathological significance of KAI1 expression and epithelial-mesenchymal transition in non-small cell lung cancer. World J Surg Oncol. 2015;13:234.
Chen Y, Min L, Zhang X, Hu S, Wang B, Liu W, et al. Decreased miRNA-148a is associated with lymph node metastasis and poor clinical outcomes and functions as a suppressor of tumor metastasis in non-small cell lung cancer. Oncol Rep. 2013;30:1832–40.
Yamashita T, Uramoto H, Onitsuka T, Ono K, Baba T, So T, et al. Association between lymphangiogenesis-/micrometastasis- and adhesion-related molecules in resected stage I NSCLC. Lung Cancer Amst Neth. 2010;70:320–8.
Lafuente-Sanchis A, Olmo A, Carretero J, Alcacer Fernandez-Coronado J, Estors-Guerrero M, Martínez-Hernández NJ, et al. Clinical significance of epithelial-mesenchymal transition-related markers expression in the micrometastatic sentinel lymph node of NSCLC. Clin Transl Oncol off Publ Fed Span Oncol Soc Natl Cancer Inst Mex. 2020;22:381–91.
Emprou C, Le Van Quyen P, Jégu J, Prim N, Weingertner N, Guérin E, et al. SNAI2 and TWIST1 in lymph node progression in early stages of NSCLC patients. Cancer Med. 2018;7:3278–91.
Salvo E, Garasa S, Dotor J, Morales X, Peláez R, Altevogt P, et al. Combined targeting of TGF-β1 and integrin β3 impairs lymph node metastasis in a mouse model of non-small-cell lung cancer. Mol Cancer. 2014;13:112.
Tang Y, Luo J, Zhou Y, Zang H, Yang Y, Liu S, et al. Overexpressed p-S6 associates with lymph node metastasis and predicts poor prognosis in non-small cell lung cancer. BMC Cancer. 2022;22:564.
Reticker-Flynn NE, Zhang W, Belk JA, Basto PA, Escalante NK, Pilarowski GOW, et al. Lymph node colonization induces tumor-immune tolerance to promote distant metastasis. Cell. 2022;185:1924-1942.e23.
Ma Q, Dieterich LC, Ikenberg K, Bachmann SB, Mangana J, Proulx ST, et al. Unexpected contribution of lymphatic vessels to promotion of distant metastatic tumor spread. Sci Adv. 2018;4:eaat4758.
McEvoy SH, Halpenny DF, Viteri-Jusué A, Hayes SA, Plodkowski AJ, Riely GJ, et al. Investigation of patterns of nodal metastases in BRAF mutant lung cancer. Lung Cancer Amst Neth. 2017;108:62–5.
Wang M, Herbst RS, Boshoff C. Toward personalized treatment approaches for non-small-cell lung cancer. Nat Med. 2021;27:1345–56.
Manfredini B, Zirafa CC, Filosso PL, Stefani A, Romano G, Davini F, et al. The role of Lymphadenectomy in Early-Stage NSCLC. Cancers. 2023;15:3735.
Gabryel P, Skrzypczak P, Roszak M, Campisi A, Zielińska D, Bryl M, et al. Influencing factors on the quality of Lymph Node Dissection for Stage IA Non-small Cell Lung Cancer: a Retrospective Nationwide Cohort Study. Cancers. 2024;16:346.
Call S, Reig-Oussedik N, Obiols C, Sanz-Santos J, Ochoa-Alba JM, Cabanillas LR et al. Video-assisted mediastinoscopic lymphadenectomy (VAMLA): mature results for staging non-small cell lung cancer with normal mediastinum. J Thorac Cardiovasc Surg. 2024;S0022-5223(24)00098 – 9.
Choi S, Yoon DW, Shin S, Kim HK, Choi YS, Kim J, et al. Importance of Lymph Node Evaluation in ≤ 2-cm pure-solid Non-small Cell Lung Cancer. Ann Thorac Surg. 2023;S0003–4975(23):00001–2.
Zielinski M, Szlubowski A, Kołodziej M, Orzechowski S, Laczynska E, Pankowski J, et al. Comparison of endobronchial ultrasound and/or endoesophageal ultrasound with transcervical extended mediastinal lymphadenectomy for staging and restaging of non-small-cell lung cancer. J Thorac Oncol off Publ Int Assoc Study Lung Cancer. 2013;8:630–6.
Kwiatkowski R, Zieliński M, Paluch J, Gabor J, Swinarew A. Enhancing patient selection in Stage IIIA-IIIB NSCLC: Invasive Lymph Node Restaging after Neoadjuvant Therapy. J Clin Med. 2024;13:422.
Kerekes DM, Frey AE, Prsic EH, Tran TT, Clune JE, Sznol M et al. Immunotherapy initiation at the end of life in patients with metastatic Cancer in the US. JAMA Oncol. 2024;e236025.
Grumberg V, Cotté F-E, Giroux-Leprieur E, Gaudin A-F, Lebbé C, Borget I. Clinical benefit of anti-PD-(L)1 immunotherapies in advanced cancer in France: a population-based estimate from 2014 to 2021. ESMO Open. 2024;9:102240.
Zhai W-Y, Zhao Z-R, Chen S, Yu H, Lin Y-B, Wang Y-Z, et al. Response of primary tumor and lymph node in non-small cell lung cancer after neoadjuvant immunotherapy: a pooled analysis. J Immunother Cancer. 2022;10:e005160.
Provencio M, Nadal E, González-Larriba JL, Martínez-Martí A, Bernabé R, Bosch-Barrera J, et al. Perioperative Nivolumab and Chemotherapy in Stage III Non-small-cell Lung Cancer. N Engl J Med. 2023;389:504–13.
Wakelee H, Liberman M, Kato T, Tsuboi M, Lee S-H, Gao S, et al. Perioperative Pembrolizumab for Early-Stage Non-small-cell Lung Cancer. N Engl J Med. 2023;389:491–503.
Kandemir O, Demir F. An investigation of the relationship between 18F-FDG PET/CT Parameters of Primary Tumors and Lymph Node Metastasis in Resectable Non-small Cell Lung Cancer. Curr Radiopharm. 2023.
Pellegrino S, Fonti R, Vallone C, Morra R, Matano E, De Placido S, et al. Coefficient of variation in metastatic lymph nodes determined by 18F-FDG PET/CT in patients with Advanced NSCLC: combination with coefficient of variation in primary tumors. Cancers. 2024;16:279.
Guberina M, Herrmann K, Pöttgen C, Guberina N, Hautzel H, Gauler T, et al. Prediction of malignant lymph nodes in NSCLC by machine-learning classifiers using EBUS-TBNA and PET/CT. Sci Rep. 2022;12:17511.
Wang Y, Deng L, Wang J, Zhang T, Wang W, Wang X, et al. Induction PD-1 inhibitor toripalimab plus chemotherapy followed by concurrent chemoradiotherapy and consolidation toripalimab for bulky locally advanced non-small-cell lung cancer: protocol for a randomized phase II trial (InTRist study). Front Immunol. 2023;14:1341584.
Reck M, Popat S, Grohé C, Corral J, Novello S, Gottfried M, et al. Anti-angiogenic agents for NSCLC following first-line immunotherapy: Rationale, recent updates, and future perspectives. Lung Cancer Amst Neth. 2023;179:107173.
Bokhari SMZ, Hamar P. Vascular endothelial growth Factor-D (VEGF-D): an angiogenesis bypass in malignant tumors. Int J Mol Sci. 2023;24:13317.
Hajrasouliha AR, Funaki T, Sadrai Z, Hattori T, Chauhan SK, Dana R. Vascular endothelial growth factor-C promotes alloimmunity by amplifying antigen-presenting cell maturation and lymphangiogenesis. Invest Ophthalmol Vis Sci. 2012;53:1244–50.
Tammela T, Zarkada G, Wallgard E, Murtomäki A, Suchting S, Wirzenius M, et al. Blocking VEGFR-3 suppresses angiogenic sprouting and vascular network formation. Nature. 2008;454:656–60.
Chiorean EG, Hurwitz HI, Cohen RB, Schwartz JD, Dalal RP, Fox FE, et al. Phase I study of every 2- or 3-week dosing of ramucirumab, a human immunoglobulin G1 monoclonal antibody targeting the vascular endothelial growth factor receptor-2 in patients with advanced solid tumors. Ann Oncol off J Eur Soc Med Oncol. 2015;26:1230–7.
Rini BI, Michaelson MD, Rosenberg JE, Bukowski RM, Sosman JA, Stadler WM, et al. Antitumor activity and biomarker analysis of sunitinib in patients with bevacizumab-refractory metastatic renal cell carcinoma. J Clin Oncol off J Am Soc Clin Oncol. 2008;26:3743–8.
Becker J, Pavlakovic H, Ludewig F, Wilting F, Weich HA, Albuquerque R, et al. Neuroblastoma progression correlates with downregulation of the lymphangiogenesis inhibitor sVEGFR-2. Clin Cancer Res off J Am Assoc Cancer Res. 2010;16:1431–41.
Maehana S, Nakamura M, Ogawa F, Imai R, Murakami R, Kojima F, et al. Suppression of lymphangiogenesis by soluble vascular endothelial growth factor receptor-2 in a mouse lung cancer model. Biomed Pharmacother Biomedecine Pharmacother. 2016;84:660–5.
Zhang Y, Yang X, Liu H, Cai M, Shentu Y. Inhibition of Tumor Lymphangiogenesis is an important part that EGFR-TKIs Play in the treatment of NSCLC. J Cancer. 2020;11:241–50.
Regan E, Sibley RC, Cenik BK, Silva A, Girard L, Minna JD, et al. Identification of Gene expression differences between Lymphangiogenic and non-lymphangiogenic non-small cell Lung Cancer Cell lines. PLoS ONE. 2016;11:e0150963.
Chen L-C, Mokgautsi N, Kuo Y-C, Wu ATH, Huang H-S. In Silico evaluation of HN-N07 small molecule as an inhibitor of Angiogenesis and Lymphangiogenesis Oncogenic signatures in Non-small Cell Lung Cancer. Biomedicines. 2023;11:2011.
Jayaram P, Yeh P, Patel SJ, Cela R, Shybut TB, Grol MW, et al. Effects of aspirin on growth factor release from freshly isolated leukocyte-rich platelet-rich plasma in healthy men: a prospective fixed-sequence controlled Laboratory Study. Am J Sports Med. 2019;47:1223–9.
Mumblat Y, Kessler O, Ilan N, Neufeld G. Full-length Semaphorin-3 C is an inhibitor of Tumor Lymphangiogenesis and Metastasis. Cancer Res. 2015;75:2177–86.
Wang Y, Yao Y, Liu H, Ma X, Lv T, Yuan D, et al. Itraconazole can inhibit malignant pleural effusion by suppressing lymphangiogenesis in mice. Transl Lung Cancer Res. 2015;4:27–35.
Celikoglu F, Celikoglu SI, Goldberg EP. Intratumoural chemotherapy of lung cancer for diagnosis and treatment of draining lymph node metastasis. J Pharm Pharmacol. 2010;62:287–95.
Kumar V, Yadavilli S, Kannan R. A review on RNAi therapy for NSCLC: opportunities and challenges. Wiley Interdiscip Rev Nanomed Nanobiotechnol. 2021;13:e1677.
Acknowledgements
Not applicable.
Funding
This work was supported by grants from the National Natural Science Foundation of China (No. 82072591 to ZW), Jiangsu Province Capability Improvement Project through Science, Technology and Education; Jiangsu Provincial Medical Key Discipline Cultivation Unit (NO. JSDW202235 to ZW), Bethune Medical Science Research Foundation Project (NO.2022-YJ-085-J-Z-ZZ-006 to ZW), “123” advantageous disciplines, core technologies of the Second Affiliated Hospital of Nanjing Medical University, Postgraduate Research & Practice Innovation Program of Jiangsu Province (No. SJCX23_0657 to LM).
Author information
Authors and Affiliations
Contributions
XZ and LM wrote and drafted the manuscript, figures, and tables. MX and YS organized and polished up the figures and tables. ZW revised and designed the manuscript. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Declaration of competing interest
The authors declare that there is no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhang, X., Ma, L., Xue, M. et al. Advances in lymphatic metastasis of non-small cell lung cancer. Cell Commun Signal 22, 201 (2024). https://doi.org/10.1186/s12964-024-01574-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12964-024-01574-1