
Abstract
Background
Not all lung adenocarcinoma (LUAD) patients with activating epidermal growth factor receptor (EGFR) mutations respond to tyrosine kinase inhibitors (TKIs) as intended. Thus, biomarkers are needed to identify patients who benefit most from EGFR-targeted therapy. Our previous in vitro data has shown that the co-signal molecule B7-H3 determines EGFR-TKI gefitinib susceptibility of EGFR-mutated LUAD cell lines, based on the potential crosslinking between B7-H3-induced signaling and EGFR signaling.
Methods
We detected tumoral B7-H3 expression in the original biopsy from 56 treatment-naïve LUAD patients and analyzed the association between high/low B7-H3 expression with the clinical outcomes of first-line anti-EGFR therapy. The main criteria for the analysis of response were overall response rate (ORR), disease control rate (DCR), and progression-free survival (PFS), and the secondary criterion was overall survival (OS).
Results
In the subgroups of B7-H3 high and low expression, the ORR were 16.0% (4/25) and 74.2% (23/31) (p<0.001), and the DCR were 36.0% (9/25) and 87.1% (27/31) (p<0.001), respectively. The PFS of B7-H3 high [median 8.7, 95% confidence interval (CI) 4.0–13.4] was significantly worse than that of B7-H3 low (median not reached) [HR 6.54 (95% CI 2.18–19.60), p=0.001]. The median OS was 15.9 (95% CI 10.0–21.8) months in the B7-H3 high cohort and 25.7 (95% CI 9.0–42.4) months in the B7-H3 low subjects [HR 2.08 (95% CI 1.07–4.02), p=0.03], respectively. Both the univariate and multivariate analyses identified B7-H3 as an independent factor associated with poor PFS (p=0.001, p=0.000) and OS (p=0.03, p=0.015).
Conclusion
B7-H3 may serve as a potential biomarker to predict clinical outcomes in EGFR-mutated LUAD patients treated with first-line EGFR-TKIs.
Similar content being viewed by others


Background
Of the non-small-cell lung cancer (NSCLC) patients, epidermal growth factor receptor (EGFR) mutations account for approximately 30% of cases in China [1], 12% in the USA [2], and 10% in France [3] and are most common among patients with lung adenocarcinoma (LUAD) [3, 4]. In-frame deletions in exon 19 (19 Del) and a point mutation in exon 21 that substitutes an arginine for a leucine at codon 858 (21 L858R) constitute nearly 90% of all EGFR mutations [5, 6]. Over the past decade, the tyrosine kinase inhibitors (TKIs) target EGFR has been demonstrated to improve clinical outcomes for NSCLC patients harboring activating EGFR mutations [7]. Unfortunately, approximately 30% of patients exhibit primary resistance to EGFR-TKIs [8, 9], and the factors involved in de novo resistance remain unidentified. Thus, more predictive clinical and biological characteristics are needed to identify patients who will benefit most from anti-EGFR therapy.
The co-signal molecule B7-H3 (CD276) is abnormally upregulated in NSCLC and plays a negative role in cancer progression [10,11,12]. Previous studies have indicated that tumoral B7-H3 triggers pro-tumorigenic signals to promote cancer invasion, migration, angiogenesis, drugs sensitivity, and Warburg effect in a series of solid tumors including NSCLC [13,14,15,16,17,18,19,20]. Our previous in vitro study has shown that B7-H3 knock-out increased gefitinib susceptibility of LUAD cell lines harboring 19 Del or 21 L858R mutations. Our further results uncovered the potential crosslinking between B7-H3-induced signaling and EGFR signaling in EGFR-mutated LUAD cell lines [21]. Thus, we speculate that the level of B7-H3 expression in LUAD is associated with EGFR-TKIs response.
In this study, we retrospectively analyzed the association of stratified (high vs. low) B7-H3 expression with clinical outcomes of LUAD patients treated with the first-line EGFR-TKIs. The findings contribute to evaluate B7-H3 profiling as a potential biomarker to identify patients at the screening who may derive improved clinical benefit from EGFR-targeted therapy.
Methods
Patients
From October 2016 through May 2021, a total of 56 LUAD patients in the Second Hospital of Anhui Medical University were enrolled in this study. The inclusion criteria were as follows: (1) advanced (stage IIIB, IIIC, and IV) LUAD patients harboring activating EGFR mutations, including 19 Del and 21 L858R; (2) patients were treatment-naive and received gefitinib (250 mg, q.d), Icotinib (125 mg, t.i.d), or erlotinib (150 mg, q.d) until disease progression or the advent of intolerable adverse effects; and (3) duration of treatment was at least 3 months at the time of data analysis. The exclusion criteria were as follows: (1) patients with age ≤18 years old; (2) sufficient information on treatment was unavailable. All patients provided written informed consent for the collection and analyses of tissue samples. The study was conducted in the principles of the Declaration of Helsinki and was approved by the Ethics Committee for the Second Hospital of Anhui Medical University (NO. 2021SHAMU0014).
The main criteria for the analysis of response were overall response rate (ORR), disease control rate (DCR), and progression-free survival (PFS), and the secondary criterion was overall survival (OS). The above indicators were evaluated according to the classified tumor response and disease progression based on Response Evaluation Criteria in Solid Tumors (RECIST version 1.1) [22, 23].
Assessment of EGFR mutations
Activating EGFR mutations, 19 Del and 21 L858R of 56 patients were analyzed by using fresh, frozen specimens obtained from the original biopsy before any treatment. Tissue DNA was isolated by the TIANamp Genomic DNA kit (Spin Column) (TIAGEN Biotech, Beijing, China). Exon 19 Del and 21 L858R were detected by ADx-AMRS (Amplified Refractory Mutation System) EGFR Mutations Detection Kit (Amoy Diagnostics, Xiamen, China) and MX3000P (Stratagene, La Jolla, USA) real-time PCR system according to the manufacturer’s instructions. A positive or negative result could be reached if it met the criterion that was defined by the manufacturer’s instruction. All the mutant results of ADx-AMRS were confirmed by direct DNA sequencing.
Tissue processing and B7-H3 expression quantification
B7-H3 expression was analyzed by immunohistochemistry on formalin-fixed, paraffin-embedded (FFPE) slides. In brief, sections of 4-μm thickness were performed heat-mediated antigen retrieval with citrate buffer (10-mM citrate, 0.05% Tween 20, pH 6.0) for 20 min at 100 °C. The slides were then removed from heat and allowed to cool down at room temperature in the buffer for 20 min. Next, immunostaining was performed by using the anti-CD276 antibody [SP206] (ab227670) (Abcam, Cambridge, MA, USA) at a dilution of 1:100 for 10 min at room temperature. The slides were then incubated with Biotin-Streptavidin Horseradish Peroxidase (HRP) Detection System (SP-9000, ZSGB-BIO, Beijing, China) and 3,3N-diaminobenzidine tertrahydrochloride (DAB) (ZLI-9017, ZSGB-BIO). By using the Olympus BX51 Microscopes (Tokyo, Japan), B7-H3 expression was evaluated by two pathologists in a blinded manner to avoid unintentional bias. All procedures followed the manufacturers’ protocols.
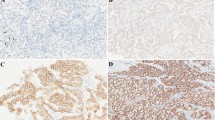
An immunohistochemical grading was made by incorporating the intensity of staining and the percentage of positive tumor cells as previously described [24,25,26]. The intensity of membranous and cytoplasmatic B7-H3 expression in lung cancer cells was defined traditionally as 0 (no staining), 1 (weak), 2 (intermediate), and 3 (strong). The percentage of positive cells was categorized as follows: 0 (<5%), 1 (5–25%), 2 (26–50%), 3 (51–75%), and 4 (>75%). An overall histochemical score was assigned to each case by multiplying the staining intensity by the percentage grade, which yielded a range from 0 to 12. All the specimens were divided into two groups: B7-H3 low (<6) and B7-H3 high group (6–12) (Fig. 1).

Immunohistochemical evaluation of tumoral B7-H3 expression in LUAD. A B7-H3 intensity 0 (negative). B, C B7-H3 low expression. D–F B7-H3 high expression (D cytoplasmatic staining. E Membranous staining. F Membranous and cytoplasmatic staining) (×200)
Statistical analysis
Ratio comparison of high/low B7-H3 expression between groups defined by demographic and pathological characteristics (age, sex, tumor size, staging, mutation subtypes, and TKIs) and of ORR or DCR between patients with stratified B7-H3 expression was performed using Pearson’s chi-square (χ2) or Fisher’s exact test. Univariate and multivariate Cox proportional hazards models were fitted to assess the hazard rates (HRs, 95% CIs) of these demographic and pathological features on anti-EGFR response. The survival characteristics of B7-H3 high/low subgroups were analyzed and plotted to visualize by the Kaplan-Meier model (log-rank test). All analyses were performed using the SPSS version 22.0 (Chicago, IL). P<0.05 was considered statistically significant.
Results
Relationship between tumoral B7-H3 expression and clinicopathological characteristics
Figure 2 shows the trial profile, and Table 1 shows the baseline characteristics of the 56 LUAD patients included in this study. The median age was 64 years, with a maximum age of 82 and a minimum of 32 years. There are no significant differences of the proportions of high/low B7-H3 expression between <60 (n=24) and ≥60 (n=32) aged, and between male (n=31) and female (n=25) patients. Most patients (n=54) did not have a smoking history except two former smokers (≥1 year since cessation). Also, B7-H3 expression levels were observed not to be significantly related to the clinicopathological characteristics including tumor size (≤30 mm vs. >30 mm) and staging (III B/C vs. IV). The association between B7-H3 expression and EGFR mutation patterns (19 Del and 21 L858R) was also assessed and again found no statistical difference. Of these patients, 30 received gefitinib, 22 received Icotinib, and 4 received erlotinib as the first-line therapy, respectively. Being a retrospective study, the participated patients are randomized to receive anti-EGFR therapy and the distribution of high/low B7-H3 expression was insignificant (p=0.839, Fisher’s exact test in R×C contingency tables). Taken together, the detection prior to EGFR-targeted therapy showed no significant differences of B7-H3 expression between age, sex, tumor size and staging, mutation patterns and selected EGFR-TKIs.

Trial profile at cutoff date for analysis (May 12, 2021)
EGFR-TKI response rates in LUAD patients with high and low B7-H3 expression
Thirty-six patients (64.3%) were still alive at the time of the study. The median follow-up time was 19.6 months, and the min to max follow-up time was 2.1–42.8 months. Of the 56 patients who could be evaluated, no patients had a complete response (CR), 27 had a partial response (PR), 9 had stable disease (SD), and 20 had progressive disease (PD). Accordingly, the total ORR and DCR are 48.2% (27/56) and 64.3% (36/56), respectively. The PR, SD, and PD numbers in B7-H3 high patients were 4, 5, and 16, and in the B7-H3 low cohort were 23, 4, and 4, respectively, Accordingly, in the subgroups of B7-H3 high and low, the ORR was 16.0% (4/25) and 74.2% (23/31) (p<0.001, chi-square test), and the DCR were 36.0% (9/25) and 87.1% (27/31) (p<0.001, chi-square test), respectively.
Survival analysis of anti-EGFR therapy associated with stratified B7-H3 expression
Patients with B7-H3 high expression had significantly worse PFS [median 8.7, 95% CI 4.0–13.4] than that of B7-H3 low (median not reached) [HR 6.54 (95% CI 2.18–19.60), p=0.001 by the stratified log-rank test] (Fig. 3A). The median OS was 15.9 (95% CI 10.0–21.8) months in the B7-H3 high group and 25.7 (95% CI 9.0–42.4) months in the low B7-H3 subjects [HR 2.08 (95% CI 1.07–4.02), p=0.03 by the stratified log-rank test], respectively (Fig. 3B). Overall, the tumoral B7-H3 level is closely relevant to clinical outcomes of the first-line ant-EGFR therapy in LUAD.

Kaplan-Meier survival curves of B7-H3 low/high LUAD patients treated with first-line EGFR-TKIs. A Progression-free survival. B Overall survival
Finally, both the univariate and multivariate analysis identified B7-H3 as an independent factor associated with poor PFS (p=0.001, p=0.000) and OS (p=0.03, p=0.015) in LUAD patients receiving anti-EGFR therapy. However, the clinicopathologic variables including age, sex, tumor size, EGFR-TKIs, and mutation subtypes have no correlation with poor survival (supplementary Table 1). The smoking history of patients was not incorporated in this study since only 2 patients were categorized as former smokers (≥1 year since cessation). Taken together, these results suggested that B7-H3 is eligible for acting as a predictor in LUAD patients treated with first-line EGFR-TKIs.
Discussion
Anti-EGFR-targeted therapy has brought many benefits to EGFR-mutated NSCLC patients [27]. Previous study based on meta-analysis has shown that PD-L1 expression might be a predictive biomarker for EGFR-mutant NSCLC treated with EGFR-TKIs [28]. In this study, we showed that the expression level of tumoral B7-H3 is eligible for precise prediction of EGFR-target therapy in EGFR-mutated LUAD patients. These results confirm our previous in vitro observation that B7-H3 knock-out increased gefitinib susceptibility of LUAD cell lines harboring exon 19 Del and 21 L858R mutations [21]. B7-H3 effects may be derived from the underlying cross-linking between EGFR signaling and B7-H3-induced signaling which share the majority of downstream cascades in tumor cells [15,16,17,18,19,20, 29]. This facilitates the interaction between the two molecules, as has been proved by our results [21], through the mutual regulation of the potentially constructed signaling network. Thus, it is very likely that B7-H3-induced signaling acts as alternative activating pathways for overcoming EGFR-TKI effects.
Of the 56 LUAD patients treated with the first-line EGFR-TKIs, the B7-H3 low cohort had significantly higher ORR and DCR and better PFS and OS than patients with B7-H3 high. Several studies have also examined the prognostic value of B7-H3 in NSCLC patients. Altan et al. have shown that only a high B7-H3 level (highest 10% vs. lowest 90%) was associated with poor OS while no correlation with survival was observed in B7-H3 positive vs. negative cases [11]. On the other hand, Inamura et al. showed that high B7-H3 expression was associated with shorter lung cancer-specific survival and OS in moderate/heavy-smoking patients (smoking index, SI ≥ 400) but not in non/light smoking patients (SI < 400) [10]. These results indicated that the association of B7-H3 expression with OS is group-limited. Whether there is a corresponding relationship between the top 10 percentile and the moderate/heavy-smoking patients is yet to be confirmed, although the two studies have unanimously shown the consistent association of elevated B7-H3 with smoking history. Our study differs from these studies in that (1) the smoking history was not incorporated since only 2 patients were categorized as former smokers (≥1 year since cessation), (2) we compared both the short-term (ORR, DCR, PFS) and long-term (OS) indicators in LUAD patients defined as B7-H3 high and low, and (3) we take treatment measure, the anti-EGFR therapy into B7-H3-based survival observation. Overall, our study demonstrates that B7-H3 acts as a predictor of clinical outcomes in LUAD patients treated with EGFR-TKIs.
It is to be noted that total ORR (48.2%) of the 56 patients in this study is substantially lower than previous clinical trials including First-SIGNAL (55.4%) [30], EURTAC (58–64%) [31], WJTOG3405 (62.1%) [32], IPASS (71.2%) [33], NEJ002 (73.7%) [9], and OPTIMAL (83%) [34], all of which were likewise based on first generation EGFR-TKI treatment. One possible explanation is the fact that this is a retrospective study. In most cases, the available medical data were gathered from repeated hospitalization, which may lead to the loss of the follow-up of patients with rather stable diseases [35]. As a result, no patients were observed to have a complete response in our study. Another possibility is the limitations of the small sample size of this study, thus further validation in a larger patient cohort is needed. On the other hand, DCR, a composite of ORR and SD, reached up to 87.1% in the B7-H3 low cohort, further indicating the predictive role of B7-H3 in anti-EGFR therapy since DCR is useful to measure the efficacy of therapies that have tumoristatic effects rather than tumoricidal effects [23]. Our results showed that the distribution of high and low B7-H3 expression has no association with age, sex, tumor size, staging, and EGFR mutation patterns. Similar results have been demonstrated in a study using samples from 3 retrospective cohorts of NSCLC patients [11]. However, baseline data from other groups showed that tumoral B7-H3 expression was higher in males, smokers, and more frequent in NSCLC patients with poor differentiation, larger tumor size, and wild-type EGFR [10, 12]. The inconsistency may in part resulted from the sampling variation as the patients in the present study all had advanced (III B/C and IV stage) diseases, with EGFR mutations and almost all had never smoked. It is unclear if EGFR mutations down-regulate B7-H3 expression to favor tumor immune escape in this context. Thus, a prognostic risk model, as it was generated in lung squamous cell cancer analysis, will be conducive to further elucidate the association between the two genes [36]. In our study, both the univariate and multivariate analysis showed that B7-H3 is an independent factor associated with poor PFS and OS whereas the clinicopathologic variables (age, sex, tumor size, TKIs, and mutation subtypes) have no correlation with poor survival of anti-EGFR therapy. These results contrast with previous studies which indicated a better response was associated with 19 Del rather than 21 L858R mutations [8, 37], and an age between 61 and 70 years of 197 patients received erlotinib [8]. However, the West Japan Oncology Group (WJTOG) 3405 study reported no associations between PFS and sex, age (<65 vs. ≥65 years), smoking history, and mutation subtypes in NSCLC patients, irrespective of gefitinib or cisplatin plus docetaxel treatment [32]. The possible explanations for these inconsistencies are differences in age grouping and of EGFR-TKIs used between studies. Further study using the propensity score matching analysis may be needed [38, 39].
Conclusions
In conclusion, our study demonstrates that higher tumoral B7-H3 expression is correlated with poorer response in LUAD patients treated with EGFR-TKIs. Thus, B7-H3 is eligible for acting as a predictor for anti-EGFR therapy in EGFR-mutated LUAD. Together, this work furthers our understanding of the EGFR targeted therapy in LUAD by proactively identification of patients who will benefit most from anti-EGFR treatment.
Availability of data and materials
All data generated or analyzed during this study are included in this published article and its supplementary information files.
References
Wu YL, Zhong WZ, Li LY, Zhang XT, Zhang L, Zhou CC, et al. Epidermal growth factor receptor mutations and their correlation with gefitinib therapy in patients with non-small cell lung cancer. A meta-analysis based on updated individual patient data from six medical centers in mainland China. J Thorac Oncol. 2007;2:430–9.
Yang SH, Mechanic LE, Yang P, Landi MT, Bowman ED, Wampfler J, et al. Mutations in the tyrosine kinase domain of the epidermal growth factor receptor in non-small cell lung cancer. Clin Cancer Res. 2005;11:2106–10.
Barlesi F, Mazieres J, Merlio J-P, Debieuvre D, Mosser J, Lena H, et al. Routine molecular profiling of patients with advanced non-small-cell lung cancer: results of a 1-year nationwide programme of the French Cooperative Thoracic Intergroup (IFCT). Lancet. 2016;387:1415–26.
Kris MG, Johnson BE, Berry LD, Kwiatkowski DJ, Iafrate AJ, Wistuba II, et al. Using multiplexed assays of oncogenic drivers in lung cancers to select targeted drugs. JAMA. 2014;311(19):1998–2006.
Wu YL, Zhou C, Hu CP, Feng J, Lu S, Huang Y, et al. Afatinib versus cisplatin plus gemcitabine for first-line treatment of Asian patients with advanced non-small-cell lung cancer harbouring EGFR mutations (LUX-Lung 6): an open-label, randomised phase 3 trial. Lancet Oncol. 2014;15(2):213–22.
Li S, Li X. Analysis of EGFR, KRAS, and PIK3CA gene mutation rates and clinical distribution in patients with different types of lung cancer. World J Surg Oncol. 2021;19(1):197.
Li R, Zhou X, Yao H, Li L. Four generations of EGFR TKIs associated with different pathogenic mutations in non-small cell lung carcinoma. J Drug Target. 2020;28(9):861–72.
Rosell R, Moran T, Queralt C, Porta R, Cardenal F, Camps C, et al. Screening for epidermal growth factor receptor mutations in lung cancer. N Engl J Med. 2009;361(10):958–67.
Maemondo M, Inoue A, Kobayashi K, Sugawara S, Oizumi S, Isobe H, et al. Gefitinib or chemotherapy for non-small-cell lung cancer with mutated EGFR. N Engl J Med. 2010;362(25):2380–8.
Inamura K, Yokouchi Y, Kobayashi M, Sakakibara R, Ninomiya H, Subat S, et al. Tumor B7-H3 (CD276) expression and smoking history in relation to lung adenocarcinoma prognosis. Lung Cancer. 2017;103:44–51.
Altan M, Pelekanou V, Schalper KA, Toki M, Gaule P, Syrigos K, et al. B7-H3 expression in NSCLC and its association with B7-H4, PD-L1 and tumor-infiltrating lymphocytes. Clin Cancer Res. 2017;23(17):5202–9.
Yim J, Koh J, Kim S, Song SG, Ahn HK, Kim YA, et al. Effects of B7-H3 expression on tumour-infiltrating immune cells and clinicopathological characteristics in non-small-cell lung cancer. Eur J Cancer. 2020;133:74–85.
Yu TT, Zhang T, Lu X, Wang RZ. B7-H3 promotes metastasis, proliferation, and epithelial-mesenchymal transition in lung adenocarcinoma. Onco Targets Ther. 2018;11:4693–700.
Bonk S, Tasdelen P, Kluth M, Hube-Magg C, Makrypidi-Fraune G, Möller K, et al. High B7-H3 expression is linked to increased risk of prostate cancer progression. Pathol Int. 2020;70(10):733–42.
Flem-Karlsen K, Tekle C, Andersson Y, Flatmark K, Fodstad Ø, Nunes-Xavier CE. Immunoregulatory protein B7-H3 promotes growth and decreases sensitivity to therapy in metastatic melanoma cells. Pigment Cell Melanoma Res. 2017;30(5):467–76.
Lin L, Cao L, Liu Y, Wang K, Zhang X, Qin X, et al. B7-H3 promotes multiple myeloma cell survival and proliferation by ROS-dependent activation of Src/STAT3 and c-Cbl-mediated degradation of SOCS3. Leukemia. 2019;33(6):1475–86.
Zhong C, Tao B, Chen Y, Guo Z, Yang X, Peng L, et al. B7-H3 regulates glioma growth and cell invasion through a JAK2/STAT3/Slug-dependent signaling pathway. Onco Targets Ther. 2020;13:2215–24.
Kang FB, Wang L, Jia HC, Li D, Li HJ, Zhang YG, et al. B7-H3 promotes aggression and invasion of hepatocellular carcinoma by targeting epithelial-to-mesenchymal transition via JAK2/STAT3/Slug signaling pathway. Cancer Cell Int. 2015;21(1):570.
Zhou L, Zhao Y. B7-H3 induces ovarian cancer drugs resistance through an PI3K/AKT/BCL-2 signaling pathway. Cancer Manag Res. 2019;11:10205–14.
Li Z, Liu J, Que L, Tang X. The immunoregulatory protein B7-H3 promotes aerobic glycolysis in oral squamous carcinoma via PI3K/Akt/mTOR pathway. J Cancer. 2019;10(23):5770–84.
Ding M, Liao H, Zhou N, Yang Y, Guan S, Chen L. B7-H3-induced signaling in lung adenocarcinoma cell lines with divergent epidermal growth factor receptor mutation patterns. Biomed Res Int. 2020;2020:8824805.
Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45(2):228–47.
Villaruz LC, Socinski MA. The clinical viewpoint: definitions, limitations of RECIST, practical considerations of measurement. Clin Cancer Res. 2013;19(10):2629–36.
Saeednejad Zanjani L, Madjd Z, Axcrona U, Abolhasani M, Rasti A, Asgari M, et al. Cytoplasmic expression of B7-H3 and membranous EpCAM expression are associated with higher grade and survival outcomes in patients with clear cell renal cell carcinoma. Ann Diagn Pathol. 2020;46:151483.
Xu QX, Li EM, Zhang YF, Liao LD, Xu XE, Wu ZY, et al. Overexpression of sigma1 receptor and its positive associations with pathologic TNM classification in esophageal squamous cell carcinoma. J Histochem Cytochem. 2012;60(6):457–66.
Liu Y, Meng F, Wang J, Liu M, Yang G, Song R, et al. A novel oxoglutarate dehydrogenase-like mediated miR-214/TWIST1 negative feedback loop inhibits pancreatic cancer growth and metastasis. Clin Cancer Res. 2019;25(17):5407–21.
Xu X, Li R, Zhu P, Zhang P, Chen J, Lin Y, et al. Clinical efficacy and safety of maintenance therapy for advanced non-small cell lung cancer: a retrospective real-world study. World J Surg Oncol. 2021;19(1):231.
Peng Z, Lin H, Zhou K, Deng S, Mei J. Predictive value of pretreatment PD-L1 expression in EGFR-mutant non-small cell lung cancer: a meta-analysis. World J Surg Oncol. 2021;19(1):145.
Janku F, Stewart DJ, Kurzrock R. Targeted therapy in non-small-cell lung cancer--is it becoming a reality? Nat Rev Clin Oncol. 2010;7(7):401–14.
Han JY, Park K, Kim SW, Lee DH, Kim HY, Kim HT, et al. First-SIGNAL: first-line single-agent iressa versus gemcitabine and cisplatin trial in never-smokers with adenocarcinoma of the lung. J Clin Oncol. 2012;30(10):1122–8.
Rosell R, Carcereny E, Gervais R, Vergnenegre A, Massuti B, Felip E, et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): a multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2012;13(3):239–46.
Mitsudomi T, Morita S, Yatabe Y, Negoro S, Okamoto I, Tsurutani J, et al. Gefitinib versus cisplatin plus docetaxel in patients with non-small-cell lung cancer harbouring mutations of the epidermal growth factor receptor (WJTOG3405): an open label, randomised phase 3 trial. Lancet Oncol. 2010;11(2):121–8.
Mok TS, Wu YL, Thongprasert S, Yang CH, Chu DT, Saijo N, et al. Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N Engl J Med. 2009;361(10):947–57.
Zhou C, Wu YL, Chen G, Feng J, Liu XQ, Wang C, et al. Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): a multicentre, open-label, randomised, phase 3 study. Lancet Oncol. 2011;12(8):735–42.
Manja V, Lakshminrusimha S. Epidemiology and Clinical Research Design, Part 1: Study Types. Neoreviews. 2014;15(12):e558–69.
Jia E, Ren N, Guo B, Cui Z, Zhang B, Xue J. Construction and validation of a novel prognostic model for lung squamous cell cancer based on N6-methyladenosine-related genes. World J Surg Oncol. 2022;20(1):59.
Yang W, Gao Y, Li X, Zhang J, Liu T, Feng X, et al. Postoperative survival of EGFR-TKI-targeted therapy in non-small cell lung cancer patients with EGFR 19 or 21 mutations: a retrospective study. World J Surg Oncol. 2017;15(1):197.
Chai Y, Ma Y, Feng W, Lu H, Jin L. Effect of surgery on survival in patients with stage III N2 small cell lung cancer: propensity score matching analysis and nomogram development and validation. World J Surg Oncol. 2021;19(1):258.
Wu LL, Lai JJ, Liu X, Huang YY, Lin P, Long H, et al. Association between number of dissected lymph nodes and survival in stage IA non-small cell lung cancer: a propensity score matching analysis. World J Surg Oncol. 2020;18(1):322.
Acknowledgements
Not applicable.
Funding
This work was supported by the Natural Science Foundation of Anhui Province (Grant No. 1808085MH229) and Key Research and Development Program of Anhui Province (Grant No. 202004j07020027).
Author information
Authors and Affiliations
Contributions
LC made contributions to the conception and design. YY, JH, BH, and JZ performed the experiments. XW and ZF performed histopathological and immunohistochemical analyses. HC was responsible for the acquisition of the clinical data. YY, YC, FP, and LC performed the statistical analysis. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was conducted in the principles of the Declaration of Helsinki, and the subject and investigator signed written informed consent and was approved by the Ethics Committee for the Second Hospital of Anhui Medical University.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Additional file Table S1.
Univariate and multivariate Cox proportional hazards regression models for PFS and OS.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yang, Y., Huang, Jf., Hu, Bq. et al. B7-H3 is eligible for predicting clinical outcomes in lung adenocarcinoma patients treated with EGFR tyrosine kinase inhibitors. World J Surg Onc 20, 159 (2022). https://doi.org/10.1186/s12957-022-02634-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12957-022-02634-x