
Abstract
Objective
To characterize longitudinal changes and correlations between the measures of EQ-5D-Y and generic PedsQL and their associations with clinical changes in children and adolescents with mild-to-moderate chronic kidney disease (CKD).
Methods
Participants were recruited from January 2017 to September 2021 in a medical center in Taiwan. Both instruments were administered in their initial visits and every 6-month subsequent visits. Spearman’s Rho (ρ) was used to assess correlations between the scores of EQ-5D-Y and PedsQL measures in longitudinal changes. Cohen’s effect size (ES) was used to evaluate the changes of scores/subscales over time. In addition, factors associated with longitudinal changes in the score/subscales were explored.
Results
A total of 121 participants were enrolled, and 83 with ≥ 3 HRQOL measures during the 3.5 years follow-up were assessed their changes of HRQOL measures. The correlations (ρ > 0.3) appeared between the changes in the visual analog scale (VAS) of EQ-5D-Y and emotional and social subscales of PedsQL. ES was small (< 0.5) in the VAS and level-sum-score (LSS) of EQ-5D-Y scores for the clinical changes in comorbidities, while some PedsQL subscales were medium to high (0.5–0.8 or > 0.8). Hypertension, mineral bone disorder/anemia, and hyperuricemia associated with the changes in both HRQOL scores were varied by their various domains.
Conclusion
Both EQ-5D-Y and PedsQL of HRQOL measures were responsive to worsened childhood CKD-related comorbidities during the follow-up; however, convergent validity between them was limited in some domains. The LSS of EQ-5D-Y showed greater changes than the VAS by comorbidity status; further comparison with utility weight is needed to determine the better performance of EQ-5D-Y.
Similar content being viewed by others

Introduction
Chronic kidney disease (CKD) is a worldwide public health problem. Children and adolescents with CKD have an increased risk of premature death from cardiovascular disease and end-stage kidney disease requiring kidney replacement therapy such as dialysis and kidney transplantation. In addition, CKD progression is associated with some complications in the pediatric population, including hypertension, hyperlipidemia, anemia, osteodystrophy, growth retardation, and impaired neurocognitive development [1,2,3], which may cause a decline in health-related quality of life (HRQOL) in childhood, adolescents and young adulthood [4,5,6].
Patient-reported outcomes instruments have been used for pediatric CKD, such as generic instruments of the Pediatric Inventory of Quality of Life Scales (PedsQL 4.0) [5, 7,8,9], the 3-level EuroQol Group's Five Dimensions for Youth (EQ-5D-Y 3L) [10], KIDSCREEN 52 [11], Patient Reported Outcomes Measurement Information System [12, 13], and the Health Utilities Index [14]; and end-stage kidney disease-specific PedsQL3.0 [15, 16]. These studies evaluated the impact of CKD or specific comorbidities of CKD progression on patient-reported outcomes focusing on children and adolescents with moderate or advanced childhood CKD [17]. However, few have evaluated pediatric patients with mild CKD (eGFR ≥ 60 ml/min/1.73 m2). Using the Taiwanese version of EQ-5D-Y 3L, our previous work showed that children with mild-to-moderate CKD are able to self-report HRQOL from their own perspective and demonstrated that multiple overt comorbidities were associated with a poor EQ-5D-Y 3L visual analog scale (VAS) [10]. In addition, the changes in CKD comorbidity burden can contribute to a considerable longitudinal discordance in child-parent dyads reported PedsQL scores, particularly in psychosocial domains [18].
Different HRQOL instruments may reflect different theoretical bases, and their content is designed to capture differences in several dimensions, including physical, emotional, mental, and social functioning, in children with chronic illnesses or specific medical interventions [19]. The Taiwan version of EQ-5D-Y has been validated and applied in pediatric kidney [10] as well as PedsQL has been done in pediatric kidney [20] and adiposity [21] populations. Although the PedsQL 4.0 with child self- and parent proxy-report forms has been validated for pediatric CKD [7, 9, 20], it is unknown either PedsQL 4.0 or EQ-5D-Y 3L is a better choice of HRQOL instrument to be regularly used during routine clinical visits in Taiwan yet. This study aimed to compare the psychometric characteristics of EQ-5D-Y and PedsQL Generic score 4.0 in Taiwanese children and adolescents with mild-to-moderate CKD and to investigate potential factors associated with longitudinal changes in HRQOL scores during long-term follow-up.
Material and methods
Patients and study settings
We used data from a prospective cohort study of the Precision Medicine Project for pediatric CKD (PMP-PCKD), which was initiated at the end of 2016 in Kaohsiung Chang Gung Memorial Hospital, a tertiary medical center in Taiwan [3, 22, 23]. Those pediatric patients aged 7–18 years who met the inclusion criteria of CKD and were willing to participate were invited to join the study during their routine visits in outpatient settings.
Measures of HRQOL
The traditional Chinese character of Taiwan version EQ-5D-Y 3L and PedsQL 4.0 instruments were administered to those participants with CKD aged 7–18 years and their parents (mother, father, or relative family) by the trained research coordinator. The standard EQ-5D-Y consists of a descriptive system that includes five dimensions: (1) mobility (“walking about”); (2) self-care (“looking after myself”); (3) usual activities (“doing usual activities”); (4) pain/discomfort (“having pain or discomfort”); and (5) anxiety/depression (“feeling worried, sad, or unhappy”). Each dimension has three ordinal levels to represent its severity. In addition, the sum of all problem level values for the five dimensions to calculate the level-sum-score (LSS) was also used to reflect the severity of different health states [24]. More specifically, the LSS ranges between 5 (health state 11,111 = 1 + 1 + 1 + 1 + 1 = 5) and 15 (health state 33,333 = 3 + 3 + 3 + 3 + 3 = 15) in EQ-5D-Y-3L, with a large LSS indicating a worse health state. The EQ-5D-Y-3L instrument also includes a VAS with the best imaginable health being anchored at 100 and worst imaginable health anchored at 0 to represent the overall health status rated by the participant [25]. All items in EQ-5D-Y-3L refer to the health state for “today”.
PedsQL, a generic instrument, has a parallel child (self) and parent (proxy) forms for children and adolescents aged 5–7, 8–12, and 13–18 years, and a parent report form only for children aged 2–4 years. PedsQL includes 23 items in four domains of physical, emotional, social, and school functioning and provides a total score and its two subscales (Physical Health summary [physical functioning] and Psychosocial Health summary [emotional, social, and school functioning]). Each item was designed to report the problem using a 5-point Likert scale (0: never a problem, 4: always a problem) for a certain condition within the past 30-day period. The reliability and validity of the PedsQL have been confirmed in a pediatric CKD population and other chronic illnesses [7, 26].
Assessments of HRQOL, clinical health data, and outcomes
HRQOL data for this study were collected at study entry (initial visit) and afterward (usually every 6 months) until patients started their dialysis or turned 18 for their latest follow-up visit. All assessments were completed between January 2017 and September 2021. Each child completed both EQ-5D-Y and PedsQL independently in a private space next to the physician’s consulting room in an outpatient setting. Those primary caregiver or other relatives who can provide adequate information about their child’s HRQOL during the outpatient care visit were invited to assess the PedsQL parent proxy version.
Clinical health data related to CKD were collected at the initial visit and at the same time when performing each HRQOL measurement assessments, as described in previous studies [3, 22, 23]. To evaluate the responsiveness of HRQOL measurements across times for CKD pediatric patients, their clinical changes were categorized as “no change”, “improved” (the number of comorbidities decreased), and “worsened” (the number of comorbidities increased) based on the number of comorbid conditions at the time of initial visit (T1) and the latest visit (T2) in the follow-up, same as our previous work [18]. Eight common pediatric CKD comorbid conditions, which were pre-specified as growth retardation (body height or body weight < 3rd percentile), overweight (body mass index > 90th percentile), hypertension (systolic or diastolic blood pressure > 95th percentile), hyperlipidemia (total cholesterol > 200 mg/dL, triglycerides > 95th percentile, or low density lipoprotein > 130 mg/dL), mineral bone disorders (serum phosphate multiplied with serum calcium ≥ 6.5 [≤ 12 years], ≥ 5.5[> 12 years]), anemia (hemoglobin < 5th percentile), hyperuricemia (serum uric acid > 5.9 mg/dL), and proteinuria (urine total protein divided by urine creatinine > 150 mg/g) [3, 18, 22, 23] were also evaluated and compared. Comorbid conditions were based on age- and sex-specific percentile norms in the pediatric population. Kidney function was assessed by determining estimated glomerular filtration rate (eGFR) from serum creatinine (SCr) using the Schwartz bedside Eq. (0.413 × height [cm]/ SCr [mg/dL]) [27]. For the individual CKD comorbid condition, yes-yes (persistent) indicated the specific commodity presented at T1 ( +) and T2 ( +) visits, no-yes (developed) as T1 (-) and T2 ( +), yes–no (improved) as T1 ( +) and T2 (-), and no–no (no change) as T1 (-) and T2 (-).
Statistical analyses
Continuous data were presented as means with standard deviations, and categorical data were presented as numbers and percentages. All enrolled pediatric patients were grouped as children (in elementary school ages of 7–12 years-old) and adolescents of 13–18 years-old to compare their characteristics. We assumed that a strong enough correlation between child self-rated EQ-5D-Y and PedsQL reports was existed in this study. Since the VAS of EQ-5D-Y did not follow a normal distribution, non-parametric Spearman’s Rho (ρ) correlation tests were used to assess the convergent validity between EQ-5D-Y and PedsQL difference from T1 toT2. The correlation coefficients of 0.3 or above were considered as evident correlation [28]. Figure 1 presents the analysis plan of this study. Cohen’s effect size (ES) was applied to measure the responsiveness of HRQOL in clinical changes (defined calculation approach). The paired t-test statistics and ES of change in the VAS and LSS of EQ-5D-Y and PedsQL scores were used for individual-level analysis between T1 and T2. According to Cohen, ES of 0.8 or above was considered large, 0.5 to 0.8 medium, 0.2 to 0.5 small, and < 0.2 was trivial [29].

Analysis and comparison between EQ-5D-Y and PedsQL measures. T1: the initial (baseline) assessment; T2: the latest follow-up assessment
A linear mixed-effect model was used to assess the magnitude of changes in summary scores of EQ-5D-Y, PedsQL and its subscales between T1 and T2 (T2-T1), adjusted for age, gender, type of CKD, and 4-level changes in each comorbidity status between T1 and T2 (no–no [reference], yes–no, no-yes, and yes-yes). The results are presented as estimates of beta (β) with 95% confidence intervals (CI). All analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, United States). The criterion for statistical significance was a two-tailed p-value of < 0.05.
Results
Patient characteristics
A total of 121 children and adolescent responded to both EQ-5D-Y and PedsQL measures in their initial visits. Of them, 83 had ≥ 3 measures of HRQOL and comprehensive laboratory results in 485 patient visits during the 3.5 years follow-up. Forty-five (54%) patients had ≥ 6 time points, 30 patients (36%) had 4–5 time points and 8 patients had 3 time points of assessment were included in the responsiveness analysis of HRQOL about their clinical changes. (1.5 years) Given they were averaged 11.47 (± 3.44) years-old, 57% were boys, 78.8% had at least one common comorbidity (Table 1). Totally, fifty-four percent of children/adolescents were diagnosed with congenital anomalies of the kidney and urinary tract (CAKUT) and 31.41% had their estimated glomerular filtration rate (eGFR) less than 89 ml/min/1.73 m2.While 56% (n = 68) and 44% (n = 53) of them were in the elementary or high school ages, respectively, those child in high school tended to had more severe renal function, overweight, comorbidities of bone disorders/anemia, hyperuricemia and proteinuria and more number of comorbid, than younger children.
HRQOL measures and comorbid conditions in their initial visits
Table 2 presents median summary scores of EQ-5D-Y and PedsQL in their initial visits by the number of baseline comorbidities. In general, both instruments can discriminate those patients’ HRQOL with ≥ 3 comorbid conditions for their lower scores of VAS of EQ-5D-Y and total score of PedsQL than those with less comorbid conditions. Among those patients with ≥ 3 comorbid conditions (n = 28), the median VAS of EQ-5D-Y was 95 (IQR: 90–99.8), and the total score of PedsQL was 89.8 (IQR, 87.0–97.3).
In their initial visits (T1), a very few participants reported “some problems” and “a lot of problems” for the EQ-5D-3L-Y descriptive system and all participants had no problems in “self-care” and “usual activities”. The younger children tended to have any problems on pain/discomfort or anxiety/depression domains but adolescent children reported worse EQ VAS (Table S1). The highest LSS was 8 (n = 1 with 21,122), followed by LSS of 7 (n = 4) and 6 (n = 20). The LSS of EQ-5D-Y appeared similar across all the comorbid condition groups. Children/adolescents had a worst health state (LSS > 5) rated a lower VAS score in their initial visits (Table S2). Higher LSS (ranged 6–7) gave some indications that children/adolescents may rate VAS score differently depending on the dimensions of mobility, pain/discomfort and anxiety/depression.
Convergent validity (correlations between EQ-5D-Y and PedsQL)
For the longitudinal changes in the VAS of EQ-5D-Y, there were few significant correlations (ρ > 0.3), including the changes in the total score and emotional and social domains of patients' self-rated PedsQL (Table 3). Low correlation was observed between “anxiety/depression” of EQ-5D-Y and emotional PedsQL score (ρ, -0.24, p = 0.0203). Cross-sectional correlation coefficients between EQ-5D–Y and PedsQL subscales in their latest follow-up visits (T2) were generally higher (ρ > 0.3) than the longitudinal correlations among a subgroup of children/adolescents in the longitudinal analyses (Tables S3 and 3). Nevertheless, correlations between parent proxy-reported PedsQL scores and child self-reported EQ-5D-Y were also very small (ρ < 0.2 in Table S4).
Responsiveness
Figure 2 presents the distribution of EQ-5D-Y domains by the level of clinical changes in the latest follow-up visit. Most (> 96%) of children and adolescents self-reported no changes in “mobility”, or “usual activities” dimensions of EQ-5D-Y. In their follow-up visits, approximately 15% of participants reported the changes either better or worse or have any problems (vs. no problems) in pain/discomfort” (14.45%) and “anxiety/depression” (13.25%) of EQ-5D-Y.

The proportion of patients by a change in each dimension of EQ-5D-Y during the follow-up period (n = 83); Change: T2 (the latest visit assessment) compared to T1 (the initial visit assessment) for “have any problem” (yes); Worsen (T2:yes, T1:no); Improve (T2:no, T1:yes); No change (T1 = T2)
Table 4 presents the longitudinal differences in HRQOL by the level of changes in CKD-related comorbidity over the study period. The ES was small (0.2–0.5) for the VAS and LSS of EQ-5D-Y by the classification of clinical changes (no change, improvement, and worsening). The ES was large for the total score of PedsQL, corresponding to improved and worsened CKD-related comorbidities (ES > 0.8). The distribution of clinical changes indicated that more patients in the worsened status group had multiple worsened comorbid conditions (i.e., hypertension, hyperlipidemia, mineral bone disorders/anemia, and hyperuricemia) during the follow-up compared to the other health status groups (no change and improved) (Table S5).
Factors associated with responsiveness of HRQOL
Seven linear mixed-effect models were performed to explore the associations between clinical changes and longitudinal changes for the individual HRQOL total or subscale scores. Overall, differences in children’s self-reported EQ-5D-Y and some domains of PedsQL scores were significantly associated with changes in some specific CKD-related comorbidities. The status changes in overweight, hypertension, and hyperuricemia were consistently associated with responsiveness across the summary scores of VAS and LSS of EQ-5D-Y and the total score of PedsQL over time (Tables 5 and 6). For instance, the EQ-5D-Y VAS was responsive to children/adolescents with persistent and developed overweight, developed hypertension, and developed hyperlipidemia (all p < 0.05). Further, adolescents (13–18 years) were associated with decreased VAS of EQ-5D-Y scores over time. The responsiveness of the LSS of EQ-5D-Y was also associated with the baseline number of CKD-related comorbidities, changes in growth retardation, and proteinuria status. The responsiveness of the total score of PedsQL was also significantly associated with mean declined eGFR and mineral bone disorders/anemia.
Furthermore, the responsiveness of each PedsQL subscale score varied depending on the CKD-related comorbidity. For instance, declined physical health (adjusted β, -6.88, p = 0.0149) and school (adjusted β, -12.9, p = 0.0024) PedsQL scores were responsive to persistent mineral bone disorder/anemia; school functioning was responsive to developed hypertension and persistent mineral bone disorder/anemia (Tables 5 and 6). In addition, male patients had lower school PedsQL scores than female patients (adjusted β, -3.17, p = 0.0303).
Discussion
This study aimed to investigate the concordance and responsiveness of HRQOL measures between EQ-5D-Y and PedsQL Generic score 4.0 in Taiwanese children and adolescents with mild-to-moderate CKD over time. Children and adolescents without comorbidity rated their VAS and LSS of EQ-5D-Y as equivalent to those with more comorbidity in their initial visits; similar results were applied for physical health and school domains of PedsQL. We observed both HRQOL instruments could detect the absolute difference in the number of CKD-related comorbidity over time. Furthermore, the associations between status changes in overweight, hypertension, hyperuricemia, and HRQOL changes were consistent between EQ-5D-Y and PedsQL measures.
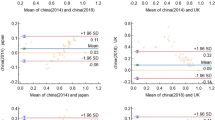
Over 80% of children and adolescents reported VAS of EQ-5D-Y ≥ 90 in their initial visits (median VAS, 97 [IQR, 90, 100]). The high ceiling effects in this study cohort are consistent with those of previous studies that analyzed the same mild-to-moderate CKD cohort [10] and general population samples in Japan [28], Korea [30], and China [31, 32]. It seemed that children and adolescents with CKD felt relatively minor difficulties in “mobility” and “usual activities” on EQ-5D-Y (all participants responded “no problem”). Alternatively, EQ-5D-Y was based on 3-level ordinal response choices, which may not be ideal for measuring changes in children’s HRQO. Studies have found that EQ-5D-Y-5L can reduce the ceiling effect [33, 34] and had greater sensitivity discriminate ability than EQ-5D-Y-3L on pain/discomfort and doing usual activities domains in the pediatric orthopedic population [33].
Moreover, previous studies have indicated the low associations between EQ-5D-Y-3L dimension and PedsQL subscales scores in a cross-sectional fashion, such as in the pediatric orthopedic patients in South Africa [33], pediatric hematologic patients in Indonesia [35], and general population samples in Japan [28]. We found evident correlations (Spearman ρ > 0.3) between longitudinal changes in VAS of EQ-5D-Y and PedsQL for total score, emotional and social subscales (all Spearman ρ = 0.32, all p < 0.005), whereas no correlations (Spearman ρ < 0.3) appeared between each domain of EQ-5D-Y and PedsQL scores. The EQ-5D-Y did not include any environmental factors. Therefore, the VAS of EQ-5D-Y may partially reflect the daily activities of the school-aged children and adolescents’ social and school subscales, but not for each domain. Similarly, the LSS of EQ-5D-Y reflects the 5 domains of health state changes over time, but no correlation with PedsQL scores was observed (Table 3). When the Taiwan version of value set for the EQ-5D-Y is available, values for the health state changes over time may be observed in children with CKD.
This study has important clinical implications. When comparing those with no–no CKD-related comorbidity over time (initial-latest visit), the changed comorbidity status was associated with different degrees of longitudinal changes in VAS and LSS of EQ-5D-Y, and some domains of PedsQL scores. It was expected that the CKD-related comorbidity can persist for several years and has a negative impact on a child’s quality of life during the developmental ages. However, in the linear mixed regression analysis, some discordant associations between a comorbidity status and HRQOL changes appeared in this study cohort. For instance, persistent or developed overweight and hyperlipidemia were associated with increased VAS of EQ-5D-Y and some subscales of PedsQL scores during the follow-up visits. In addition, the increase in HRQOL score over time could be partly due to regular specific medical management at a specific time period, such as when corticosteroids are used to treat glomerular disorders but cause weight gain.
For the psychometric evaluation, Verstraete et al. have suggested that the VAS of EQ-5D-Y performed best in acutely-ill children to discriminate worst health status with the lowest VAS score of EQ-5D-Y than the total score of PedsQL in children and adolescents with acute health conditions [36]. It is also worth mentioning that EQ-5D-Y refers to the “today” health state using a three-level ordinal scale, whereas the five-point Likert scale in the PedsQL refers to the “past month”, which might have an impact on the divergence validity of these HRQOL measures [36, 37].
This is a cohort of pediatric patients with mild-to-moderate CKD. Children and adolescents with a longer duration of disease may have adapted their assessments of HRQOL according to their chronic disease status (e.g., persistent or no changes in some specific CKD comorbidity). These study findings indicate that further investigation of the discordance found in these domains of health associated with a particular treatment or management would enable a better understanding of how HRQOL changes in a particular health domain for CKD children. In addition, it is critical to ensure that HRQOL instruments have demonstrated sensitivity to detecting the changes in health perception and characteristics during a child’s development over time [38].
To our knowledge, we present the first comprehensive direct comparisons of EQ-5D-Y and PedsQL in contemporary pediatric clinical practice over time. This is the first test of the psychometric properties of the EQ-5D-Y and PedsQL in pediatric patients with mild-to-moderate CKD in cooperation with health status changes in longitudinal features. These study results highlight the necessity of long-term HRQOL assessment in children and adolescents with developmental changes in progressive CKD. Furthermore, this study demonstrated that both EQ-5D-Y and PedsQL could detect an evident difference in HRQOL scores according to the dynamic changes in CKD-related comorbid conditions.
It is worth mentioning that correlations between parent proxy-reported PedsQL scores and child self-reported EQ-5D-Y were very small, suggested that parents who rated HRQOL for their child’s health status were different from that of their children who were of the same aspects of HRQOL [18]. These results provide additional support for the importance of focusing on the child’s viewpoint rather than their parents' viewpoint for the ongoing assessment of HRQOL in children and adolescents with CKD. The proxy-version of EQ-5D-Y now is available and recommended for younger children (under the age of 7–8 years) and older children if they cannot complete the instrument themselves [39]. These study results may contribute to the growing evidence related to the measurement properties of both instruments in the pediatric CKD population. Further research is recommended comparing the psychometric performance of parent-proxy version of EQ-5D-Yand PedsQL to guide clinicians on the choice of most appropriate HRQOL instrument for the age-specific children and adolescents with CKD.
This study had some limitations. First, this single-center study included only limited patients who could attend our research clinic; therefore, the results may not be generalizable to the most affected children and adolescents with mild-to-moderate CKD. However, as age and prevalent clinical conditions in this study were similar to the patterns reported in multicenter studies [40], this limitation seems acceptable to the Taiwanese pediatric CKD population. Second, PMP-CKD is an observational study; thus, the specific treatment and management relevant to the mitigation of the severity of CKD-related comorbidity were not accounted for in the changes in HRQOL scores. Finally, we used four-level temporal clinical changes (i.e., persistent, developed, improved, and no change) in each comorbid condition to serve as a proxy of changes in disease burden in the specific period; future studies may be warranted to confirm these study findings.
In summary, this study demonstrated the small to moderate convergent validity between the EQ-5D-Y and PedsQL. The LSS of EQ-5D-Y generally showed a larger effect size than the VAS by the changes in the number of CKD-related comorbidity over time. Further comparisons of utility weights may help determine the responsiveness to changes between VAS and LSS of EQ-5D-Y. Therefore, both EQ-5D-Y and PedsQL can be considered as acceptable valid generic tools to assess HRQOL, reflecting longitudinal changes in HRQOL associated with complex CKD comorbidity management.
Availability of data and materials
The data are not available. According to the informed consent content, participants provided raw data would remain confidential and would not be shared.
References
Becherucci F, Roperto RM, Materassi M, Romagnani P. Chronic kidney disease in children. Clin Kidney J. 2016;9:583–91.
Kang NR, Ahn YH, Park E, Choi HJ, Kim SH, Cho H, Cho MH, Shin JI, Lee JH, Park YS. Mental health and psychosocial adjustment in pediatric chronic kidney disease derived from the KNOW-Ped CKD study. Pediatr Nephrol. 2019;34:1753–64.
Hsu C-N, Lu P-C, Lo M-H, Lin I, Tain Y-L. The association between nitric oxide pathway, blood pressure abnormalities, and cardiovascular risk profile in pediatric chronic kidney disease. Int J Mol Sci. 2019;20:5301.
Wong G, Medway M, Didsbury M, Tong A, Turner R, Mackie F, McTaggart S, Walker A, White S, Howard K, et al. Health and wealth in children and adolescents with chronic kidney disease (K-CAD study). BMC Public Health. 2014;14:307.
de Ferris MED-G, Pierce CB, Gipson DS, Furth SL, Warady BA, Hooper SR. Health-related quality of life in children with chronic kidney disease is affected by the number of medications. Pediatr Nephrol. 2021;36:1307–10.
Grootenhuis MA, Stam H, Last BF, Groothoff JW. The impact of delayed development on the quality of life of adults with end-stage renal disease since childhood. Pediatr Nephrol. 2006;21:538–44.
Gerson AC, Wentz A, Abraham AG, Mendley SR, Hooper SR, Butler RW, Gipson DS, Lande MB, Shinnar S, Moxey-Mims MM. Health-related quality of life of children with mild to moderate chronic kidney disease. Pediatrics. 2010;125:e349–57.
Al-Uzri A, Matheson M, Gipson DS, Mendley SR, Hooper SR, Yadin O, Rozansky DJ, Moxey-Mims M, Furth SL, Warady BA. The impact of short stature on health-related quality of life in children with chronic kidney disease. J Pediatr. 2013;163(736–741): e731.
Kiliś-Pstrusińska K, Medyńska A, Chmielewska IB, Grenda R, Kluska-Jóźwiak A, Leszczyńska B, Niedomagała J, Olszak-Szot I, Miklaszewska M, Szczepańska M. Perception of health-related quality of life in children with chronic kidney disease by the patients and their caregivers: multicentre national study results. Qual Life Res. 2013;22:2889–97.
Hsu C-N, Lin H-W, Pickard AS, Tain Y-L. EQ-5D-Y for the assessment of health-related quality of life among Taiwanese youth with mild-to-moderate chronic kidney disease. Int J Qual Health Care. 2018;30:298–305.
Dotis J, Pavlaki A, Printza N, Stabouli S, Antoniou S, Gkogka C, Kontodimopoulos N, Papachristou F. Quality of life in children with chronic kidney disease. Pediatr Nephrol. 2016;31:2309–16.
DeWalt DA, Gross HE, Gipson DS, Selewski DT, DeWitt EM, Dampier CD, Hinds PS, Huang I-C, Thissen D, Varni JW. PROMIS® pediatric self-report scales distinguish subgroups of children within and across six common pediatric chronic health conditions. Qual Life Res. 2015;24:2195–208.
Selewski DT, Massengill SF, Troost JP, Wickman L, Messer KL, Herreshoff E, Bowers C, Ferris ME, Mahan JD, Greenbaum LA. Gaining the patient reported outcomes measurement information system (PROMIS) perspective in chronic kidney disease: a Midwest pediatric nephrology consortium study. Pediatr Nephrol. 2014;29:2347–56.
Francis A, Didsbury MS, van Zwieten A, Chen K, James LJ, Kim S, Howard K, Williams G, Treidel OB, McTaggart S. Quality of life of children and adolescents with chronic kidney disease: a cross-sectional study. Arch Dis Child. 2019;104:134–40.
Tjaden LA, Grootenhuis MA, Noordzij M, Groothoff JW. Health-related quality of life in patients with pediatric onset of end-stage renal disease: state of the art and recommendations for clinical practice. Pediatr Nephrol. 2016;31:1579–91.
Carlson J, Gerson AC, Matheson MB, Manne S, Warady BA, Hooper SR, Lande M, Harshman LA, Johnson RJ, Shinnar S. A longitudinal analysis of the effect of anemia on health-related quality of life in children with mild-to-moderate chronic kidney disease. Pediatr Nephrol. 2020;35:1659–67.
Ruidiaz-Gómez KS, Higuita-Gutiérrez LF. Impact of chronic kidney disease on health-related quality of life in the pediatric population: meta-analysis. J Pediatr (Rio J). 2021; 97(5):478–89. https://doi.org/10.1016/j.jped.2020.10.013.
Tain Y-L, Lu P-C, Kuo H-C, Hsu C-N. Differences in health-related quality of life in children with chronic kidney disease as reported by children and parent proxies. Pediatr Nephrol. 2023;38(2):519–28.
Petersson C, Simeonsson RJ, Enskar K, Huus K. Comparing children’s self-report instruments for health-related quality of life using the International Classification of Functioning, Disability and Health for Children and Youth (ICF-CY). Health Qual Life Outcomes. 2013;11:75.
Tain Y-L, Lu P-C, Kuo H-C, Hsu C-N. Differences in health-related quality of life in children with chronic kidney disease as reported by children and parent proxies. Pediatr Nephrol. 2023;38:519–28.
Lee C-T, Lin C-Y, Strong C, Lin Y-F, Chou Y-Y, Tsai M-C. Metabolic correlates of health-related quality of life among overweight and obese adolescents. BMC Pediatr. 2018;18:1–8.
Hsu C-N, Lu P-C, Hou C-Y, Tain Y-L. Blood pressure abnormalities associated with gut microbiota-derived short chain fatty acids in children with congenital anomalies of the kidney and urinary tract. J Clin Med. 2019;8:1090.
Hsu C-N, Lu P-C, Lo M-H, Lin I, Chang-Chien G-P, Lin S, Tain Y-L. Gut microbiota-dependent trimethylamine N-oxide pathway associated with cardiovascular risk in children with early-stage chronic kidney disease. Int J Mol Sci. 2018;19:3699.
Devlin N, Parkin D, Janssen B. Methods for analysing and reporting EQ-5D data. Springer Nature. 2020. https://doi.org/10.1007/978-3-030-47622-9.
Wille N, Badia X, Bonsel G, Burström K, Cavrini G, Devlin N, Egmar A-C, Greiner W, Gusi N, Herdman M. Development of the EQ-5D-Y: a child-friendly version of the EQ-5D. Qual Life Res. 2010;19:875–86.
Varni JW, Seid M, Kurtin PS. PedsQL 4.0: reliability and validity of the Pediatric Quality of Life Inventory version 4.0 generic core scales in healthy and patient populations. Med Care. 2001;39:800–12.
Schwartz GJ, Munoz A, Schneider MF, Mak RH, Kaskel F, Warady BA, Furth SL. New equations to estimate GFR in children with CKD. J Am Soc Nephrol. 2009;20:629.
Shiroiwa T, Fukuda T, Shimozuma K. Psychometric properties of the Japanese version of the EQ-5D-Y by self-report and proxy-report: reliability and construct validity. Qual Life Res. 2019;28:3093–105.
Middel B, Van Sonderen E. Statistical significant change versus relevant or important change in (quasi) experimental design: some conceptual and methodological problems in estimating magnitude of intervention-related change in health services research. Int J Integr Care. 2002;2:e15.
Kim S-K, Jo M-W, Kim S-H. A cross sectional survey on health-related quality of life of elementary school students using the Korean version of the EQ-5D-Y. Peer J. 2017;5: e3115.
Pei W, Yue S, Zhi-Hao Y, Ruo-Yu Z, Bin W, Nan L. Testing measurement properties of two EQ-5D youth versions and KIDSCREEN-10 in China. Eur J Health Econ. 2021;22:1083–93.
Pan C-W, Zhong H, Li J, Suo C, Wang P. Measuring health-related quality of life in elementary and secondary school students using the Chinese version of the EQ-5D-Y in rural China. BMC Public Health. 2020;20:1–8.
Verstraete J, Marthinus Z, Dix-Peek S, Scott D. Measurement properties and responsiveness of the EQ-5D-Y-5L compared to the EQ-5D-Y-3L in children and adolescents receiving acute orthopaedic care. Health Qual Life Outcomes. 2022;20:28.
Wang P, Luo N, Tai E, Thumboo J. The EQ-5D-5L is more discriminative than the EQ-5D-3L in patients with diabetes in Singapore. Value Health Reg Issues. 2016;9:57–62.
Fitriana TS, Purba FD, Rahmatika R, Muhaimin R, Sari NM, Bonsel G, Stolk E, Busschbach JJ. Comparing measurement properties of EQ-5D-Y-3L and EQ-5D-Y-5L in paediatric patients. Health Qual Life Outcomes. 2021;19:1–12.
Verstraete J, Scott D. Comparison of the EQ-5D-Y-5L, EQ-5D-Y-3L and PedsQL in children and adolescents. J Patient Rep Outcomes. 2022;6:1–12.
Scott D, Ferguson GD, Jelsma J. The use of the EQ-5D-Y health related quality of life outcome measure in children in the Western Cape, South Africa: psychometric properties, feasibility and usefulness-a longitudinal, analytical study. Health Qual Life Outcomes. 2017;15:1–14.
Colver AF, Merrick H, Deverill M, Le Couteur A, Parr J, Pearce MS, Rapley T, Vale L, Watson R, McConachie H. Study protocol: longitudinal study of the transition of young people with complex health needs from child to adult health services. BMC Public Health. 2013;13:675.
EQ-5D-Y User Guide: Basic information on how to use the EQ-5D-Y instrument. https://euroqol.org/publications/user-guides/EQ5DY/Userguide-EQ5D-Y-23-07.pdf. Accessed 17 Oct 2020.
Chou HH, Lin CY, Chiou YH, Tain YL, Wang YF, Wang HH, Chiou YY. Clinical characteristics and prevalence of complications of chronic kidney disease in children: the Taiwan Pediatric Renal Collaborative study. Pediatr Nephrol. 2016;31:1113–20.
Acknowledgements
We thank all study coordinators, young patients, and their families who participated in this PMP-PCKD study at Kaohsiung Chang Gung Memorial Hospital in Kaohsiung, Taiwan.
We appreciate the discussant, Dr. Ataru Igarashi from Yokohama City University School of Medicine, Unit of Public Health and Preventive Medicine in Japan, for reviewing and commenting on our conference paper with preliminary findings of this study presented at the virtual 2nd EuroQoL Asia Academy Meeting 2021. In addition, we thank the chairs, Drs. Fredrick Purba and Zhihao Yang, and Dr. Luo Nan for their thoughtful comments on the conference paper.
Funding
This Precision Medication Project-Pediatric Chronic Kidney Disease (PMP-PCKD) study was supported by Kaohsiung Chang Gung Memorial Hospital at Kaohsiung, Taiwan (Grant number: CORPG8F1031, CMRPG8I0101, and CMRPG8K0721).
Author information
Authors and Affiliations
Contributions
HCN and LHW contributed to the conceptualization, study design, data interpretation and writing of the manuscript. TYL contributed study design, interpretation of data, and data collection with LPC. HCN and KHC contributed to the data investigation and analysis.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Institutional Review Board of Chang Gung Medical Foundation in Taipei, Taiwan approved this study protocol (approval number: 201801981A3). All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Consent for publication
Written informed consent was obtained before the HRQOL assessment from all individual participants and their parents included in the study.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:
Table S1. Distribution of EQ-5D-Y domains at initial assessment. Table S2. VAS and LSS of EQ-5D-Y at baseline. Table S3. Cross-sectional correlations between EQ-5D-Y and PedsQL scores at initial and latest follow-up assessments. Table S4. Correlations between changes in children’s self-reported EQ-5D-Y and changes in parent-proxy reported PedsQL scores. Table S5. Characteristics of study participants in longitudinal analysis (n = 83).
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Hsu, CN., Tain, YL., Lu, PC. et al. Comparisons of EQ-5D-Y and PedsQL in pediatric patients with mild-to-moderate chronic kidney disease in longitudinal analyses. Health Qual Life Outcomes 21, 117 (2023). https://doi.org/10.1186/s12955-023-02197-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12955-023-02197-9