
Abstract
Background
The study aimed to assess chronic diseases, multimorbidity, and QoL among patients attending two different treatment settings in Thailand.
Methods
In all, 1409 attendees of three monk healer or three health centres were assessed with self-reported measures on chronic conditions and Quality of Life (QoL).
Results
Results indicate that the most common chronic conditions were common mental disorder (25.2%), followed by hypertension (22.8%), high blood cholesterol (18.0%), fatigue disorder (14.4%), diabetes (14.0%), migraine headaches (13.7%), sleeping problem (12.2%), and ulcer (11.0%). In all, 40.6% had multimorbidity (two or more chronic conditions) (42.4% in the monk healer and 38.9% in the primary care setting). In ANCOVA analysis, adjusted for sex, age, employment status, marital status, education, economic status, comorbidity, and health care setting, the poorest overall QoL was found among clients with common mental disorders (58.5 mean score), followed by emphysema or asthma (60.2), sleeping problem (61.5), migraine headaches (62.7), fatigue disorder (63.3), substance use disorder (63.6) and ulcer (64.3). The overall QoL was poorer among monk healer clients (66.5) than primary care patients (68.8). In adjusted logistical regression analysis, being a monk healer attendee, older age (55–93 years), and high debt were positively, and being employed and better overall quality of life were negatively associated with multimorbidity, overall, for the monk healer and primary care setting. In adjusted linear regression analyses, primary health care attenders, older age, were employed and post-secondary education increased the odds of better overall QoL.
Conclusion
Multimorbidity was higher among clients attending monk healers than those attending primary care facilities and QoL was poorer among clients seeking care from monk healers than those attending primary care. High multimorbidity was found and major chronic conditions were found to have poor QoL. Determinants of multimorbidity and QoL in two different treatment settings provide information to improve the management of chronic conditions.
Similar content being viewed by others


Background
Chronic conditions are common among patients in primary care settings. Multimorbidity (coexistence of two or more chronic conditions) has been found in Southeast Asian countries [1]. In Odisha state of India, 28.3% of patients (≥ 18 years) in primary care (30.7% in public care and 24.6% in private care) had multimorbidity [2], and in rural primary care in Kerala, India, the prevalence of multimorbidity was 16.2% (≥ 18 years) [3]. In a study among chronic disease primary care patients in four Greater Mekong countries, the majority (72.6%) had multimorbidity [1]. In Singapore, among adult patients with chronic diseases in public sector primary care clinics, 39.6% of those who had used traditional and complementary medicine (TCM) in the past year and 28.1% who had not used (TCM) had multimorbidity [4]. Several studies [4,5,6,7], including in Cambodia, Thailand, Singapore, USA, and Vietnam, showed that patients with multimorbidity are more likely to utilize traditional and complementary medicine (TCM) than patients without multimorbidity. In a further study, multimorbidity of chronic physical and mental illnesses was associated with higher TCM use [8]. In comparing the morbidity pattern of patients of traditional Chinese medicine practitioners with Chinese medical practitioners in Hong Kong population, showing that for chronic illnesses TCM was the preferred treatment [9]. Multimorbidity has been identified as a major challenge for health care systems, which are based on single disease-specific management [2]. Therefore, an understanding of the prevalence of multimorbidity in both a TCM and conventional primary health setting are vital in designing more effective primary care [2]. There is, to our knowledge, no information on multimorbidity in a traditional health practitioner (THP) setting. It is hypothesized that attendees of THP (monk healer) have a higher prevalence of multimorbidity than primary care attendees. Monk healers are Thai THP providing various types of treatments, including herbal medicine, physical therapy, and Buddhist practices, such as prayer [10, 11].
Chronic conditions persist for a long time and affect functional ability and quality of life negatively [12]. “Health-related quality of life (HRQoL) is a multi-dimensional concept that includes domains related to physical, mental, emotional, and social functioning” [13], and is commonly used to describe overall well-being and health [14] and general health needs [15]. Several studies [1, 12, 16, 17] show that multimorbidity in primary care patients is negatively associated with QoL. Among primary care patients in Southeast Asian countries, poorer QoL was identified in cancer, mental disorders, asthma, chronic obstructive pulmonary disease (COPD) and cardiovascular diseases (CVD) [18]. Among Chinese primary care patients, depression and osteoarthritis had the lowest QoL compared to many other chronic diseases [19]. In a multicountry study, arthritis, COPD and CVD had the lowest QoL scores [20]. We did not find a study describing the overall QoL among attendees of THP, however, in a study in Brazil, the overall QoL was 65.2 (range 0–100) among attendees of primary health care [21]. It is not clear if QoL among attendees differs by monk healer or primary care setting. It was hypothesised that together with a higher prevalence of multimorbidity in the monk healer compared to the primary care setting, QoL would be poorer among clients attending monk healers than those attending primary care.
As reviewed previously [1], factors associated with multimorbidity may include older age, female sex, lower socioeconomic status, and low QoL. Lower QoL among primary care patients, as previously reviewed [18], may be associated with multimorbidity, older age, being female, not married or cohabiting, lower education, rural residence and substance use. The study aimed to assess chronic diseases, multimorbidity, and QoL among patients attending monk healers and primary care health centres in Thailand. Study findings could help in identifying patient groups with differentially impaired QoL within multimorbidity and designing specific care plans.
Methods
Design and participants
Using a cross-sectional study design, 1409 adult attendees of two treatment settings (primary care and monk healer) were interviewed by a trained professional nurse consecutively from six sites in the eastern and central region of Thailand over a period of four months in 2018/2019. Study sites were purposefully selected with the inclusion criteria that they had at least five adult patients per day. The “Office of The Committee for Research Ethics (Social Sciences), Mahidol University (No.: 2017/055.1403)” approved the study, and written informed consent was provided by participants.
Measures
Sample characteristics included marital status, highest educational level, gender, age, work, and economic status (extent of debt).
Chronic conditions. Clients were asked about 16 health care providers’ diagnosed chronic conditions, such as asthma, diabetes, emphysema, and hypertension (see Table 1).
Typical mental problems (somatization, generalized anxiety disorder, and major depression) were sourced from (1) in Thailand validated “Patient Health Questionnaire-9 (PHQ-9)” [22, 23]. (Cronbach’s alpha 0.88), (2) the “Generalized anxiety disorder 7-item (GAD-7)” [24] (Cronbach’s alpha 0.92), and (3) The “Patient Health Questionnaire-15 somatic symptoms (PHQ- 15)” [25]. (Cronbach’s alpha 0.83).
Substance use disorders were assessed with the in Thailand validated “Ultrarapid Alcohol, Smoking, and Substance Involvement Screening Test (ASSIST-Lite)” [26]. Cronbach alpha of the ASSIST-Lite in this study was 0.90.
Quality of Life (Qol) was assessed with the World Health Organization Quality of Life (WHOQol)-8, consisting of physical domain (2 items), psychological domain (2 items), environmental domain (2 items), and social domain (2 items) [27, 28]. Each item was scored from 1 (worst) to 5 (best), and summed to result in 2-items subscales and 8-items overall WHOQoL, which was then converted into a 0–100 scale, with higher scores indicating better QoL [18] (Cronbach alpha 0.86).
Data analysis
The descriptive characteristics of the sample, multimorbidity, and QoL were calculated as percentage, means and standard deviation. Analysis of covariance (ANCOVA) was utilized to assess the associations between five measures of QoL (the four QoL domains: Psychological, Physical, Social and Environment, and overall QoL) and various chronic diseases and adjustments were made for age, sex, employment status, marital status, education, economic status, comorbidity, and health care setting. Multivariable logistic regression was utilized to estimate the predictors of multimorbidity, overall and two treatment settings. Independent variables included sociodemographic factors, quality of life, and type of health care setting. Multi-variable linear regression was used for the assessment of the impact of explanatory variables (socio-demographic factors and type of health care setting) on overall QoL in the multimorbidity population, overall and two treatment settings. p values < 0.05% were used to indicate statistical significance. The data were analysed using “IBM-SPSS for Windows, version 25 (Chicago, IL, USA)”.
Results
Sample and multimorbidity characteristics
Participants included 1409 attendees of two treatment settings (response rate 97%), 723 of primary care and 686 of monk healers. The age of participants was significantly higher in the health centre (Mean 53.3 years) than in the monk healer setting (Mean 47.3 years). The proportion of two or more chronic conditions (multimorbidity) was 40.6%, 42.4% in the monk healer and 38.9% in the primary care setting. Further sociodemographic characteristics by the percentage of multimorbidity (≥ 2 chronic conditions) are described in Table 1.
Prevalence of chronic conditions and morbidity
From 12 health care providers diagnosed chronic conditions and two interview-based assessed chronic conditions (common mental disorder and substance use disorder), the most common was common mental disorder (25.2%), followed by hypertension (22.8%), high blood cholesterol (18.0%), fatigue disorder (14.4%), diabetes (14.0%), migraine headaches (13.7%), sleeping problem (12.2%), and ulcer (11.0%). In all, 35.8% had no chronic condition, 23.5% had one chronic condition, 15.1% had two, 9.8% had three, and 15.7% had four or more chronic conditions. The prevalence of emphysema or asthma, osteoporosis, cancer, substance use disorders, heart attack or stroke, common mental disorders, sore joints, and sleeping problems was higher among monk healer attendees, while the prevalence of diabetes and hypertension was higher in primary care attendees (see Table 2).
The percentage with the highest comorbidity was common mental disorder (48.9%), followed by hypertension (48.4%), high blood cholesterol (41.1%), fatigue disorder (33.3%), migraine headaches (30.4%), diabetes (27.9%), sleeping problem (27.0%), ulcer (22.6%), sore joints (18.7%), substance use disorder (13.0%), heart attack or stroke (11.6%), emphysema or asthma (8.5%) and cancer (7.2%). The highest mean multimorbidity reported was for osteoporosis (5.48), followed by emphysema or asthma (5.38), heart attack or stroke (5.32), cancer (5.14), fatigue disorder (4.35), sleep problem (4.29), sore joints (4.20), ulcer (4.03), high cholesterol (3.95), migraine headaches (3.84), diabetes (3.65), hypertension (3.39) common mental disorder (3.28), and substance use disorder (2.54).
Quality of Life in chronic conditions and multimorbidity
In ANCOVA analysis, adjusted for sex, age, employment status, marital status, education, economic status, comorbidity, and health care setting, the poorest overall QoL was found among clients with common mental disorders (58.5 mean score), followed by emphysema or asthma (60.2), sleeping problem (61.5), migraine headaches (62.7), fatigue disorder (63.3), substance use disorder (63.6) and ulcer (64.3). The highest overall QoL score was found among clients with hypertension (67.6 mean score), followed by high blood cholesterol (67.2), and diabetes (66.7). The overall QoL was significantly higher (71.2 mean score) in clients with no chronic conditions, compared to those with four or more chronic conditions (61.8 mean score).
The overall QoL score was 67.5, while the social QoL domain had the highest score (72.1), followed by the physical QoL subdomain (68.9), and the lowest were in the psychological QoL subdomain (64.0) and the environmental QoL sub-domain (64.7). The overall QoL was poorer among monk healer clients (66.5) than primary care patients (68.8).
Psychological QoL scores were the lowest for common mental disorders (53.1) and emphysema or asthma (54.5), fatigue disorder (57.7), and sleeping problems (58.7). Physical QoL was the lowest for common mental disorders (60.6), emphysema or asthma (61.3), sleeping problem (62.1), osteoporosis (63.8), sleeping problems (64.4) and heart attack or stroke (64.6). Social QoL was the lowest for common mental disorders (63.3), sleeping problem (65.9), emphysema or asthma (66.0), migraine headaches (67.5) and substance use disorder (67.7), while environmental QoL was the lowest for common mental disorder (56.5), sleeping problem (59.2), emphysema or asthma (59.0), and migraine headaches (59.4). In patients with multimorbidity (four or more chronic conditions) scores for the four QoL subdomains (psychological, physical, social and environment) and overall QoL significantly decreased (see Table 3).
Associations with multimorbidity
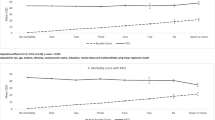
In adjusted logistical regression analysis, being a monk healer attendee (Adjusted Odds Ratio-AOR: 1.36, 95% Confidence Interval-CI 1.03–1.78, p < 0.05), older age (55–93 years) (AOR: 2.62, 95% CI 1.77–3.86, p < 0.001), and high debt (AOR: 1.45, 95% CI 1.09–1.93, p < 0.05) were positively, and being employed (AOR: 0.54, 95% CI 0.41–0.73, p < 0.001) and better overall quality of life (AOR: 0.96, 95% CI 0.95–0.97, p < 0.001) were negatively associated with multimorbidity, overall, for the monk healer and primary care setting. In addition, having post-secondary education was positively associated with multimorbidity in the monk healer setting, and having secondary education (compared to primary or less education) was negatively associated with multimorbidity in the primary care setting (see Table 4).
Associations with quality of life in multimorbidity
In adjusted linear regression analyses, primary health care attenders (Adjusted Coefficient-ACoef.: 6.18, 95% CI 2.93 to 9.42, p < 0.001), older age (ACoef.: 0.14, 95% CI 0.02 to 0.27, p < 0.05), post-secondary education (ACoef.: 8.77, 95% CI 4.51 to 13.05, p < 0.001) and being employed (ACoef.: 3.80, 95% CI 0.69 to 6.90, p < 0.05) was associated with higher overall QoL. Female sex, higher formal education, and being married or cohabiting were associated with higher overall QoL among monk healer attenders, and having post-secondary education and being employed were associated with better overall QoL among primary care attenders (see Table 5).
Discussion
This is the first study assessing chronic conditions, multimorbidity, and QoL in patients attending two different treatment settings in Asia. The study found a high prevalence of multimorbidity (40.6%) (42.4% in the monk healer and 38.9% in the primary care setting), which was higher than in primary care in India (28.3% Odisha state, 16.2% in Kerala) [2, 3]. The prevalence of multimorbidity was higher in monk healers than primary care attendees. This result is in line with several studies [4,5,6,7,8] showing that patients with multimorbidity are more likely to utilize traditional and complementary medicine (TCM) than patients without multimorbidity. In this study, clients attending monk healers had more likely mental and substance use disorders than those attending primary care. Patients with coexisting physical and mental disorders have higher functional disabilities and poor quality of life compared to those with physical conditions only, and are therefore more likely to attend monk healers than primary care to improve their functional status, which was not successfully treated in primary care [8]. The lower prevalence of multimorbidity in primary care may be related to lower availability of specialists and supporting services [2], primary care health centres in Thailand provide preventive and basic acute care, mainly provided by professional nurses. Patients with higher education seem to more likely consult monk healers and secondary care (district hospitals) directly. Consistent with a previous review [29], this study found that the highest proportion of comorbidity was found for common mental disorders (48.9%) and hypertension (48.4%). Somewhat similar to a previous study [29], this study found that the highest mean multimorbidity was among patients with emphysema or asthma (5.38), heart attack or stroke (5.32), and cancer (5.14) and to a lower extent for hypertension (3.39).
The study found that the overall QoL was poorer among monk healer clients (66.5) than primary care patients (68.8), but was a little higher than in primary care patients in Brazil (65.2) [21]. In agreement with previous studies, the poorest overall QoL was found among clients with common mental disorders (58.5 mean score), emphysema or asthma (60.2), sleeping problems (61.5), and migraine headaches (62.7), compared to many other chronic diseases, probably due to their more symptomatic presentation [19, 30]. On the other hand, patients reporting more asymptomatic or less disabling conditions, such as hypertension and high blood cholesterol, had better QoL scores, as also found in previous studies [20]. The finding that heart attack or stroke, cancer, and arthritis were not significantly associated with lower overall QoL was unexpected, since previous studies found such associations [18]. Furthermore, the study confirmed that different chronic diseases affected specific domains of QoL differently, as also found previously [18, 19]. Having a common mental disorder or a sleep problem was not only impacting negatively on psychological QoL but also on other QoL subdomains, such as physical, social, and/or environmental, which may have the implication of managing mental and physical problems concurrently [19].
Consistent with some studies [31,32,33], this study found that older age and lower socioeconomic status (in debt and not employed) was associated with multimorbidity. Moreover, this study confirms findings from a previous review on the existence of a negative association between QoL and multimorbidity [16]. The possible association between QoL and multimorbidity may have implications for health care management in the different health care settings in Thailand [34], especially because being a client of a monk healer was associated with multimorbidity. Unlike some previous studies [31] that found a preponderance of multimorbidity among women, this study did not find any sex differences in the prevalence of multimorbidity.
Consistent with some previous studies [18, 30, 35, 36], this study found that sociodemographic variables (older age, better education, and being employed) were associated with higher QoL scores. Higher education and being employed may be associated with higher awareness of a healthy lifestyle and easier access to health services, which in turn may lead to improved health as well as QoL [37]. Among clients visiting a monk healer, being female and married or cohabiting were associated with better QoL. Being married or cohabiting has a vital role in social support, as opposed to living alone, and may facilitate QoL [37]. To address multimorbidity and improve QoL, a person-centred approach has been proposed by tackling the health issues of a particular patient in a combined fashion [38]. In this line, it would be important to coordinate within the network of healthcare providers from primary care and monk healer settings of care to ensure continuity of care for the patient [38].
This study had several limitations because it was cross-sectional and information was collected by self-report. The study was conducted with patients from conveniently selected monk healer and primary health facilities, who compared to specialist care tended to have probably milder or more stable conditions. Some of the included chronic diseases such as cancer and osteoporosis in the study had small subgroup sample sizes, which limited the detection of associations. The study did not assess the perceived severity of the chronic conditions, which could have an impact on QoL, and should be assessed in future studies.
Conclusion
Multimorbidity was higher among clients attending monk healers than those attending primary care facilities and QoL was poorer among clients seeking care from monk healers than those attending primary care. The study found a high prevalence of multimorbidity (40.6%) (42.4% in the monk healer and 38.9% in the primary care setting). Older age, having high debt, and being a client of a monk healer increased and being employed and overall QoL decreased the odds of multimorbidity. Being a primary health care attender, older age, post-secondary education and employment was associated with better overall QoL. Determinants of multimorbidity and QoL in two different treatment settings provide information to improve the management of chronic conditions.
Availability of data and materials
The data for the current study will not be shared publicly as participants were informed at the time of providing consent that only researchers involved in the project would have access to the information they provided.
Abbreviations
- ANCOVA:
-
Analysis of Covariance
- ASSIST-Lite:
-
Ultrarapid Alcohol, Smoking, and Substance Involvement Screening Test
- COPD:
-
Chronic obstructive pulmonary disease
- CVD:
-
Cardiovascular disease
- GAD:
-
Generalized anxiety disorder
- PHQ:
-
Patient Health Questionnaire
- QoL:
-
Quality of Life
- TCM:
-
Traditional and complementary medicine
- THP:
-
Traditional health practitioner
References
Pengpid S, Peltzer K. Multimorbidity in chronic conditions: Public primary care patients four Greater Mekong countries. Int J Environ Res Public Health. 2017;14(9):1019. https://doi.org/10.3390/ijerph14091019.
Pati S, Swain S, Knottnerus JA, Metsemakers JFM, van den Akker M. Magnitude and determinants of multimorbidity and health care utilization among patients attending public versus private primary care: a cross-sectional study from Odisha, India. Int J Equity Health. 2020;19(1):57. https://doi.org/10.1186/s12939-020-01170-y.
Vargese SS, Mathew E, Johny V, Kurian N, Gayathri AV, Raju AS. Prevalence and pattern of multimorbidity among adults in a primary care rural setting. CEGH. 2020;8(2):482–5. https://doi.org/10.1016/j.cegh.2019.10.014.
Lee GB, Charn TC, Chew ZH, Ng TP. Complementary and alternative medicine use in patients with chronic diseases in primary care is associated with perceived quality of care and cultural beliefs. Fam Pract. 2004;21(6):654–60. https://doi.org/10.1093/fampra/cmh613.
Peltzer K, Pengpid S. The use of herbal medicines among chronic disease patients in Thailand: a cross-sectional survey. J Multidiscip Healthc. 2019;12:573–82. https://doi.org/10.2147/JMDH.S212953.
Peltzer K, Pengpid S, Puckpinyo A, Yi S, le Anh V. The utilization of traditional, complementary and alternative medicine for non-communicable diseases and mental disorders in health care patients in Cambodia, Thailand and Vietnam. BMC Complement Altern Med. 2016;16:92. https://doi.org/10.1186/s12906-016-1078-0.
Mbizo J, Okafor A, Sutton MA, Leyva B, Stone LM, Olaku O. Complementary and alternative medicine use among persons with multiple chronic conditions: results from the 2012 National Health Interview Survey. BMC Complement Altern Med. 2018;18(1):281. https://doi.org/10.1186/s12906-018-2342-2.
Alwhaibi M, Bhattacharya R, Sambamoorthi U. Type of Multimorbidity and Complementary and Alternative Medicine Use among Adults. Evid Based Complement Alternat Med. 2015;2015:362582. https://doi.org/10.1155/2015/362582.
Wong W, Lam CLK, Bian XZ, Zhang ZJ, Ng ST, Tung S. Morbidity pattern of traditional Chinese medicine primary care in the Hong Kong population. Sci Rep. 2017;7(1):7513. https://doi.org/10.1038/s41598-017-07538-5.
Chan-iam W, Yodmalee B, Nakornriab M. Thai Traditional Medicine at Wat Nong Ya Nang Buddhist, Uthai Thani Province. J Food Health Bioenviron Sci. 2019;12(2):40–7.
Kaewla W, Wiwanitkit V. Local primary health care by local religious center: A case study of a Mahayana Buddhist temple, Thailand. Ann Trop Med Public Health. 2015;8:226.
Pati S, Swain S, Knottnerus JA, Metsemakers JFM, van den Akker M. Health related quality of life in multimorbidity: a primary-care based study from Odisha, India. Health Qual Life Outcomes. 2019;17(1):116. https://doi.org/10.1186/s12955-019-1180-3.
Healthy People 2020. Health-Related Quality of Life and Well-Being. URL: https://www.healthypeople.gov/2020/about/foundation-health-measures/Health-Related-Quality-of-Life-and-Well-Being. Accessed 10 Aug 2020
Muhwezi WW, Okello ES, Turiho AK. Gender-based profiling of Quality of Life (QOL) of primary health care (PHC) attendees in central Uganda: a cross sectional analysis. Afr Health Sci. 2010;10(4):374–85.
Borges TL, Miasso AI, Reisdofer E, Dos Santos MA, Vedana KG, Hegadoren KM. Common mental disorders in primary health care units: associated factors and impact on quality of life. J Am Psychiatric Nurses Assoc. 2016;22(5):378–86. https://doi.org/10.1177/1078390316655207.
Fortin M, Lapointe L, Hudon C, Vanasse A, Ntetu AL, Maltais D. Multimorbidity and quality of life in primary care: a systematic review. Health Qual Life Outcomes. 2004;2:51.
Quah JHM, Wang P, Ng RRG, Luo N, Tan NC. Health-related quality of life of older Asian patients with multimorbidity in primary care in a developed nation. Geriatr Gerontol Int. 2017;17(10):1429–37. https://doi.org/10.1111/ggi.12881.
Pengpid S, Peltzer K. The impact of chronic diseases on the quality of life of primary care patients in Cambodia, Myanmar and Vietnam. Iran J Public Health. 2018;47(9):1308–16.
Lam CL, Lauder IJ. The impact of chronic diseases on the health-related quality of life (HRQOL) of Chinese patients in primary care. Fam Pract. 2000;17(2):159–66. https://doi.org/10.1093/fampra/17.2.159.
Alonso J, Ferrer M, Gandek B, Ware JE Jr, Aaronson NK, Mosconi P, et al. IQOLA Project GroupHealth-related quality of life associated with chronic conditions in eightcountries: results from the International Quality of Life Assessment (IQOLA) Project. Qual Life Res. 2004;13(2):283–98.
Almeida-Brasil CC, Silveira MR, Silva KR, Lima MG, Faria CDCM, Cardoso CL, et al. Quality of life and associated characteristics: application of WHOQOL-BREF in the context of Primary Health Care. Cien Saude Colet. 2017;22(5):1705–16. https://doi.org/10.1590/1413-81232017225.20362015.
Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Internal Med. 2001;16(9):606–13.
Lotrakul M, Sumrithe S, Saipanish R. Reliability and validity of the Thai version of the PHQ-9. BMC Psychiatry. 2008;8:46. https://doi.org/10.1186/1471-244X-8-46.
Spitzer RL, Kroenke K, Williams JB, Lowe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092–7. https://doi.org/10.1001/archinte.166.10.1092.
Kroenke K, Spitzer RL, Williams JB. The PHQ–15: validity of a new measure for evaluating the severity of somatic symptoms. Psychosom Med. 2002;64:258–66.
Ali R, Meena S, Eastwood B, Richards I, Marsden J. Ultra-rapid screening for substance-use disorders: the Alcohol, Smoking and Substance Involvement Screening test (ASSIST-Lite). Drug Alcohol Depend. 2013;132(1–2):352–61.
Schmidt S, Mühlan H, Power M. The EU-ROHISQOL 8-item index: psychometric results of a cross-cultural field study. Eur J Pub Health. 2006;16(4):420–8. https://doi.org/10.1093/eurpub/cki155.
Da Rocha NS, Power MJ, Bushnell DM, Fleck MP. The EUROHIS-QOL 8-item index: comparative psychometric properties to its parent WHOQOL-BREF. Value Health J Int Soc Pharmacoecon Outcomes Res. 2012;15(3):449–57. https://doi.org/10.1016/j.jval.2011.11.035.
Sinnige J, Braspenning J, Schellevis F, Stirbu-Wagner I, Westert G, Korevaar J. The prevalence of disease clusters in older adults with multiple chronic diseases—a systematic literature review. PLoS ONE. 2013;8:e79641.
Tüzün H, Aycan S, İlhan MN. Impact of comorbidity and socioeconomic status on quality of life in patients with chronic diseases who attend primary health care centres. Cent Eur J Public Health. 2015;23(3):188–94.
Mujica-Mota RE, Roberts M, Abel G, Elliott M, Lyratzopoulos G, Roland M, Campbell J. Common patterns of morbidity and multi-morbidity and their impact on health-related quality of life: evidence from a national survey. Qual Life Res. 2015;24(4):909–18. https://doi.org/10.1007/s11136-014-0820-7.
Phaswana-Mafuya N, Peltzer K, Chirinda W, Musekiwa A, Kose Z, Hoosain E, Davids A, Ramlagan S. Self-reported prevalence of chronic non-communicable diseases and associated factors among older adults in South Africa. Glob Health Action. 2013;6:20936.
Violan C, Foguet-Boreu Q, Flores-Mateo G, Salisbury C, Blom J, Freitag M, Glynn L, Muth C, Valderas JM. Prevalence, determinants and patterns of multimorbidity in primary care: a systematic review of observational studies. PLoS ONE. 2014;9:e102149.
Arokiasamy P, Uttamacharya U, Jain K, Biritwum RB, Yawson AE, Wu F, Guo Y, Maximova T, Espinoza BM, Rodríguez AS, et al. The impact of multimorbidity on adult physical and mental health in low- and middle-income countries: what does the study on global ageing and adult health (SAGE) reveal? BMC Med. 2015;13:178.
Deng Q, Wang LM, Zhang M. Quality of life and related influencing factors in Chinese adults. Zhonghua Liu Xing Bing Xue Za Zhi. 2016;37(2):243–7.
Heyworth IT, Hazell ML, Linehan MF, Frank TL. How do common chronic conditions affect health-related quality of life? Br J Gen Pract. 2009;59(568):e353–8.
Minh HV, Ng N, Byass P, Wall S. Patterns of subjective quality of life among older adults in rural Vietnam and Indonesia. Geriatr Gerontol Int. 2012;12(3):397–404.
Belche JL, Berrewaerts MA, Ketterer F, Henrard G, Vanmeerbeek M, Giet D. De la maladie chronique à la multimorbidité : quel impact sur l’organisation des soins de santé ? [From chronic disease to multimorbidity: which impact on organization of health care]. Presse Med. 2015;44(11):1146–54. https://doi.org/10.1016/j.lpm.2015.05.016.
Acknowledgements
Not applicable.
Funding
The study was supported by the South African Department of Higher Education.
Author information
Authors and Affiliations
Contributions
All authors fulfil the criteria for authorship. SP and KP conceived and designed the research, performed statistical analysis, drafted the manuscript and made critical revision of the manuscript for key intellectual content. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the institutional review board of the “Office of The Committee for Research Ethics (Social Sciences), Mahidol University (No.: 2017/055.1403)”, and all participants gave written informed consent prior to the study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Pengpid, S., Peltzer, K. Chronic conditions, multimorbidity, and quality of life among patients attending monk healers and primary care clinics in Thailand. Health Qual Life Outcomes 19, 61 (2021). https://doi.org/10.1186/s12955-021-01707-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12955-021-01707-x