
Abstract
Background
The Triglyceride glucose (TyG) index-related indicators improve risk stratification by identifying individuals prone to atherosclerosis early in life. This study aimed to examine the relation between TyG-waist circumference-to-height ratio (TyG-WHtR) and coronary heart disease.
Methods
Data from four National Health and Nutrition Examination Surveys (NHANES) cycles between 2011 and 2018 were used for a cross-sectional study. The association between TyG-WHtR and coronary heart disease risk was examined using a multifactorial logistic regression model, and corresponding subgroup analyses were performed. Nonlinear correlations were analyzed using smooth curve fitting and threshold effects analysis. When nonlinear connections were discovered, appropriate inflection points were investigated using recursive methods.
Results
TyG-WHtR and coronary heart disease were significantly positively correlated in the multifactorial logistic regression analysis. Subgroup analyses and interaction tests revealed that gender, age, smoking status, and cancer were not significantly associated with this correlation (P for interaction > 0.05). Furthermore, utilizing threshold effect analysis and smooth curve fitting, a nonlinear connection with an inflection point of 0.36 was observed between TyG-WHtR and coronary heart disease.
Conclusions
According to this study, the American population is far more likely to have coronary heart disease if they have higher TyG-WHtR levels.
Similar content being viewed by others

Introduction
Cardiovascular disease, one of the conditions with the highest rates of morbidity and mortality globally, presents a public health challenge as well as a significant financial and psychological burden on patients and their families [1]. Approximately one-quarter of all deaths in the US are attributed to coronary heart disease annually [2]. Atherosclerosis and coronary heart disease are closely associated; in coronary heart disease, atherosclerotic plaques form in the coronary arteries that supply the myocardium, reducing blood flow perfusion to the heart [3]. Metabolic syndrome plays a significant role in the development of coronary heart disease, with varying levels of correlation between the incidence and prevalence of coronary heart disease, suggesting that there may be specific common disease progressions between them. Diabetes mellitus, dyslipidemia, and metabolic dysfunction, a collection of concurrent conditions characterized by insulin resistance [4, 5], are of great interest in actively investigating the precise mechanisms by which metabolic dysfunction influences the onset of coronary heart disease. Determining relevant pathways is crucial for diagnosing, treating, and preventing coronary heart disease.
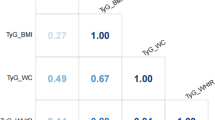
Insulin resistance (IR) is a condition in which the body is less sensitive and responsive to the effects of insulin. Patients with IR are more likely to develop various metabolic diseases, including dyslipidemia, hypertension, and abnormal blood sugar levels. These conditions increase the risk of atherosclerosis, inflammation, and coagulation abnormalities and are also significantly associated with a worse prognosis for cardiovascular disease [1, 6,7,8]. The TyG index is a correlative indicator of metabolic dysfunction that determines the levels of glucose and triglycerides in fasting blood. The TyG index has recently gained recognition as a reliable and user-friendly alternative to IR with significant therapeutic implications for identifying metabolic dysfunction [9]. The TyG index outperformed the homeostasis model assessment of insulin resistance in predicting coronary artery calcification [10]. It is substantially correlated with carotid atherosclerosis, even after controlling for conventional cardiovascular risk factors [11]. In individuals with type 2 diabetes, Chen et al. recently noted an independent correlation between the TyG index and severe coronary artery stenosis [12]. The TyG index is linked to an increased risk of cardiovascular disease, atherosclerosis, and coronary artery calcification [10, 13]. The TyG-related index is a more reliable predictor of IR and cardiometabolic risk than is the TyG index alone [14, 15]. Additionally, correlative indices, such as Triglyceride glucose-body mass index (TyG-BMI), Triglyceride glucose-waist circumference (TyG-WC), and Triglyceride glucose-waist circumference-to-height ratio (TyG-WHtR), which incorporate anthropometric measurements of obesity in addition to TyG, are more accurate predictors of Insulin resistance and cardiometabolic risk than is the TyG index alone [16,17,18,19]. Furthermore, the integrated association score of TyG and anatomical indicators of obesity is a more precise indicator of the degree of insulin resistance. Therefore, early monitoring of insulin resistance in obese individuals is crucial to avoid a poor prognosis in coronary heart disease.
To the best of our knowledge, there is inadequate data on the association between TyG-WHtR levels and coronary heart disease. Identifying practical and helpful markers that allow early intervention in metabolic factors in individuals at high risk of coronary heart disease is crucial. Thus, our investigation aimed to examine the association between TyG-WHtR indices and the risk of coronary heart disease using a large-scale, cross-sectional, population-based study.
Methods
Data sources and study population
The Centers for Disease Control and Prevention conducted the NHANES study of the ambulatory population in the United States to evaluate the health, nutritional status, and lifestyle of Americans. The NHANES employs a sophisticated multistage stratified sampling strategy and releases data biennially. The National Center for Health Statistics Research Ethics Review Board approved all technique utilized in the NHANES study. All survey respondents provided written informed consent. During the survey, participants completed several questions and pertinent tests. The five main components of the NHANES database are screening, diet, laboratory, questionnaire, and demographic data. This analysis used data from four NHANES cycles from 2011 to 2018.
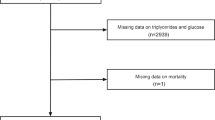
Studies on research designs have been published [20]. Overall, 39,156 participants were identified from the NHANES statistics spanning 2011 to 2018. The exclusion criteria included: 16,539 participants under 20 years of age, 13,429 participants with missing TyG and WHtR data, and 37 participants with missing coronary heart disease data. Ultimately, we analyzed the outcome data of 9,151 participants (Fig. 1).

Flow chart
Definitions of TyG-WHtR and coronary heart disease
The TyG index measures triglyceride and fasting blood glucose levels to quantify insulin resistance. The following formula was used to calculate the correlation index: TyG = Ln[fasting blood glucose(mg/dL)×fasting triglyceride(mg/dL)/2] [21]; WHtR = waist circumference/height; TyG-WHtR = TyG×WHtR [18]. The exposure variable in our study was TyG-WHtR.
A trained interviewer asked patients a series of questions about their coronary heart disease history. Participants were asked, “Has a doctor or other health professional ever told you that you had coronary heart disease?” They responded with either “yes” or “no.” Those who were unsure or declined to respond were considered absent. Coronary heart disease was the outcome variable in our analysis [22].
Study variables
The covariates included age, gender, race, annual household income, education level, smoking status, drinking status, hypertension, diabetes, dietary supplement use, regular exercise, cancer, and cholesterol levels. Race was categorized as Mexican American, Other Hispanic, Non-Hispanic White, Non-Hispanic Black, or Other. Educational level was designated as less than 9th grade, 9th–11th grade, high school graduate, AA degree, or college graduate or above. Annual household income was grouped with a threshold of USD 100,000. Smoking status was determined by having smoked more than 100 cigarettes in a lifetime. Drinking status was defined based on consuming more than 12 drinks per year, with those answering “yes” considered drinkers. Medical professionals confirmed diagnoses of hypertension, diabetes, and cancer. Waist circumference and height, vital measurements taken during a medical checkup, along with fasting blood glucose, triglyceride, and total cholesterol levels, were assessed using relevant laboratory tests. For more detailed information on how these variables were measured, please refer to visit the NHANES website: www.cdc.gov/nchs/nhanes/.
Statistical analysis
All statistical analyses were performed by considering intricate multistage cluster surveys and using proper NHANES sampling weights in compliance with the Centers for Disease Control and Prevention criteria. The participants were divided into groups based on the presence of TyG-WHtR and coronary heart disease. Continuous data are represented as mean ± standard deviation, and categorical variables are expressed as frequency percentages [20]. All variables were evaluated for variance using the chi-square test, nonparametric Kruskal–Wallis test, or analysis of variance. The participants were divided into groups depending on the presence of TyG-WHtR and coronary heart disease. To identify any possible correlation between the TyG-WHtR index (continuous or tertile) and coronary heart disease, multivariate logistic regression analysis was used to determine the odds ratio (OR) and 95% confidence interval (CI) in three distinct models. Using multivariate regression analysis, the independent relation between TyG-WHtR and coronary heart disease was examined using three distinct models. The crude model was not adjusted for correlation, the minimally adjusted model was adjusted for age, gender, and race, and the fully adjusted model was adjusted for education level, smoking status, drinking status, hypertension, diabetes, dietary supplement use, regular exercise, cancer, and cholesterol. The model was fully adjusted for age, gender, and race. The subgroup analyses of TyG-WHtR and coronary artery disease were stratified using criteria based on gender, age, smoking status, hypertension, and cancer. A threshold effect analysis was used to examine the relation and inflection points between TyG-WHtR and coronary heart disease. Finally, we characterized the nonlinear connection between TyG-WHtR and coronary heart disease risk using smooth curve fitting. R Studio (version 4.3.1) and EmpowerStats (version 2.0) were used for statistical analysis. Statistical significance was set at P<0.05.
Results
Baseline characteristics of participants
A total of 9,151 individuals were included in the study, with a mean age of 49.57 ± 17.38 years. Among the participants, 51.31% were male and 48.69% were female. The racial composition was as follows: 13.51% Mexican Americans, 10.83% Other Hispanics, 37.92% Non-Hispanic White, 21.21% Non-Hispanic Black, and 16.53% from other racial backgrounds. Coronary heart disease was diagnosed in 4.04% of the participants.
The clinical features of the individuals are listed in Table 1, arranged according to the TyG-WHtR tertiles. The tertiles were statistically significant for age, gender, race, annual household income, educational level, smoking status, drinking status, hypertension, diabetes, cancer, cholesterol, and coronary heart disease (P < 0.05). Participants in the Tertiles 3 group tended to be older, male, and Non-Hispanic White, with an annual household income under $100,000, a higher education level, and higher cholesterol levels.
The clinical features of the individuals are listed in Table 2, according to whether they had coronary heart disease. Age, gender, race, annual household income, educational level, smoking status, hypertension, diabetes, dietary supplement use, regular exercise, cancer, cholesterol level, and the TyG-WHtR were significantly associated with the presence or absence of coronary heart disease (P < 0.05). Patients with coronary heart disease tended to be older, male, Non-Hispanic White, with an annual household income under $100,000, educated to an AA degree, with smoking status, hypertension, dietary supplement use, and higher TyG-WHtR levels than those without the condition.
Relation between TyG-WHtR and coronary heart disease
The findings of the multivariate regression analysis of TyG-WHtR and coronary heart disease are shown in Table 3. The fully adjusted model revealed that the association between TyG-WHtR and coronary heart disease was significantly positive (OR = 1.83; 95% CI: 1.28–2.62, P = 0.0008), indicating a higher TyG-WHtR value increases the odds of developing coronary heart disease. This association was evident in both the crude (OR = 2.26; 95% CI: 1.87–2.72, P < 0.0001) and minimally adjusted model (OR = 1.85; 95% CI: 1.48–2.32, P < 0.0001). For additional sensitivity analyses, TyG-WHtR was converted from continuous to categorical variables (Tertiles 1, 2, and 3). In the fully adjusted model, participants in Tertile 3 had a 77% higher risk of coronary heart disease than those in Tertile 1 (OR = 1.77; 95% CI: 1.13–2.76, P = 0.0121). Furthermore, all three models had trend tests with P values of < 0.05, indicating statistical significance.
Age, gender, race, education level, hypertension, dietary supplement use, and cholesterol level remained substantially linked to coronary heart disease risk in the fully adjusted models (Table 4). To determine whether these findings were applicable to the current population, we conducted a subgroup analysis by gender, age, smoking status, hypertension, and cancer. As shown in Fig. 2, there was a positive link between TyG-WHtR and coronary heart disease risk in both males (OR = 1.58; 95% CI: 1.01–2.50) and participants without hypertension (OR = 3.41, 95% CI: 1.60–7.28). The results of the interaction test demonstrated that there was no statistically significant difference in the association between TyG-WHtR and coronary heart disease according to gender, age, smoking status, or cancer, suggesting that these factors did not significantly affect the positive relation (P > 0.05 for interaction test).

Subgroup analysis
This nonlinear connection between TyG-WHtR and coronary heart disease risk was better characterized when all-variable smoothed curve fitting was considered. Smooth curve fitting revealed a U-shaped relation between TyG-WHtR and coronary heart disease (Fig. 3), with a log-likelihood ratio of 0.018 and a breakpoint of 0.36 (Table 5).

Smooth curve fitting. The red curve indicates the smooth curve fit between the variables; the two blue curves indicate the 95% confidence intervals of the fitted results
Smoothed curves were subsequently constructed for the gender and hypertension subgroups based on the outcomes of the subgroup analyses. Surprisingly, TyG-WHtR was positively correlated with coronary heart disease risk in the subgroup of male but had a U-shaped association with coronary heart disease risk in the hypertension subgroup (Fig. 4).

Smoothed curve fitting for subgroup analysis. A: Curve fitting with gender as the subgroup; B: Curve fitting with hypertension as the subgroup
Discussion
To the best of our knowledge, this is the first study to evaluate the association between risk and TyG-WHtR in individuals with coronary heart disease. In this cross-sectional survey, higher continuous and categorical TyG-WHtR concentrations were associated with an increased risk of coronary heart disease. The proportion of individuals at high risk of coronary heart disease increased significantly with a gradual increase in TyG-WHtR. Other risk variables had no effect on this relation. The number of people who experienced this connection was consistent with the findings of the subgroup analyses and interaction tests. With an inflection point of 0.36, a U-shaped relation was observed between TyG-WHtR levels and coronary heart disease. Around the 0.36 inflection point, this investigation revealed a strong association between TyG-WHtR and coronary heart disease. In the highest TyG-WHtR tertile, the risk of coronary heart disease increased 1.77-fold (Tertiles 3 vs. Tertiles 1).
Insulin resistance is a significant risk factor for coronary heart disease, which can lead to vascular endothelial damage, the development of atherosclerotic plaques, and other conditions that accelerate the progression of coronary heart disease [23, 24]. Recently, the TyG index was employed to measure atherosclerosis in individuals with cardiovascular disease [25,26,27]. An observational research cohort study showed that TyG-WC was positively correlated with the risk of the first myocardial infarction. According to the multivariate-adjusted model, as TyG-WC quartiles increased, so did the risk of myocardial infarction [28]. This notion is supported by our data. Additionally, a cohort of observational studies showed that an elevated TyG index was linked to an increased likelihood of developing chronic kidney disease and that chronic kidney disease could be prevented by early metabolic factor intervention, which would lower the incidence of cardiovascular disease as well as prospective death [29]. According to one study, a higher TyG index was linked to an increased risk of adverse cardiovascular events in patients receiving percutaneous coronary intervention for ST-segment elevation myocardial infarction [14]. An increased TyG index is substantially linked to an increased risk of atherosclerosis and renal microvascular damage, according to a study by Zhao [30, 31]. WHtR is a straightforward and readily accessible marker of generalized and abdominal obesity. Relevant studies have demonstrated that WHtR is more effective in identifying cardiometabolic risk factors than is waist circumference and body mass index for abdominal fat deposition, which are significantly associated with coronary heart disease [32, 33]. Furthermore, WHtR is a better option than waist circumference for examining the association between obesity and cardiovascular disease in individuals with lower body mass indices [34]. Additionally, according to a meta-analysis of 52 cohort studies, shorter patients had a higher risk of developing coronary heart disease [19]. Thus, the current study investigated the risk correlations between TyG-WHtR and coronary heart disease. These results indicated a positive correlation between coronary heart disease and TyG-WHtR levels. A U-shaped relation with a breakpoint of 0.36 was also found between TyG-WHtR levels and coronary heart disease. The study results indicated a connection between elevated TyG-WHtR levels and an increased risk of coronary heart disease.
The precise mechanism by which TyG-WHtR is associated with cardiovascular disease remains unclear [1]. Atherosclerosis may develop owing to systemic lipid abnormalities caused by IR, such as elevated triglycerides, enhanced low-density lipemia, postprandial lipemia, and decreased high-density lipoprotein levels. This may be the fundamental mechanism of action [35]. In addition, reduced insulin activity in the established ischemic myocardium restricts glucose accessibility. This causes changes in the metabolism of fatty acids, which increase oxygen consumption in the heart and decrease its ability to compensate for non-infarcted regions [36]. Second, many adipokines and hormones produced by abdominal adipose tissue may cause endocrine-metabolic comorbidities [37]. Increased adipocyte size (hypertrophy) and number (hyperplasia) are associated with local and systemic chronic inflammation. Following the infiltration of inflammatory cells, inflammatory mediators and oxidative stressors are released, resulting in severe metabolic disorders that can directly affect the cardiovascular system and accelerate the development of atherosclerosis [38, 39]. The progression of coronary heart disease may be worsened by pathologic metabolic disturbances, such as hypertriglyceridemia, increased free fatty acids, adipose tissue emission of proinflammatory cytokines, hepatic IR and inflammation, amplified secretion of very-low-density lipoproteins, and impaired clearance of triglyceride-rich lipoproteins [37, 40].
Study strengths and limitations
The findings of this study have significant implications for clinical practice. This study hypothesized that TyG-WHtR, an inexpensive and readily available marker, is associated with coronary heart disease risk. Therefore, prevention and treatment should be considered in patients with various risk factors. The data used in the analysis performed in this research were derived from the NHANES database, a well-designed, well-sampled program with the advantages of high representativeness, large datasets, and long-term monitoring. The anthropometric and laboratory data collected for this study were also of excellent quality. To conduct a relatively thorough analysis, this study used different methods: first, a large sample size and reliable data were used; second, covariate adjustments were made throughout the investigation of the relation between TyG-WHtR and coronary artery disease; and third, the exposure factors in this study were examined as categorical and continuous variables in two separate approaches. Smoothed curve fitting with a threshold effect analysis was employed to further investigate the nonlinear link between TyG-WHtR and coronary heart disease. The possibility of false positives was further decreased by the sensitivity analysis. As this was a cross-sectional study, it may have been influenced by other factors. However, thorough statistical corrections lessened the influence of confounding variables.
Nevertheless, this study has several limitations. First, this cross-sectional study examined the relation between TyG-WHtR and coronary heart disease. To further elucidate the connection between TyG-WHtR and coronary heart disease, several prospective studies, along with basic research, must be conducted at later time points. The data were collected at a specific point in time, and the lack of corresponding longitudinal data did not indicate a causal relation. Second, there is a possibility of bias because some indicators, such as recall, were partially collected through questionnaires rather than through objective measurement indications. Some variables, such as genetic and environmental factors, may still impact our results, even after several covariate adjustments. As a result, a significant number of further multidisciplinary investigations must be carried out to confirm our findings. Furthermore, cross-sectional studies cannot demonstrate temporal and causal correlations, and TyG-WHtR was evaluated only at baseline in this study. TyG-WHtR variations were not measured during the course of the inquiry. This study found a positive correlation between TyG-WHtR and coronary heart disease risk. However, further experiments are needed to confirm the mechanism underlying this correlation and the reduction of coronary heart disease risk by controlling the TyG-WHtR level in the clinic.
Conclusions
In conclusion, this study demonstrated for the first time that elevated TyG-WHtR levels are associated with a higher risk of coronary heart disease in the United States. In this study, TyG-WHtR levels were associated with coronary heart disease risk in a “U-shaped” relation with a threshold value of 0.36. The results of this study provide a useful and convenient marker for early intervention of metabolic factors in people at a high risk of coronary heart disease.
Data availability
No datasets were generated or analysed during the current study.
Abbreviations
- TyG:
-
Triglyceride glucose
- TyG-WHtR:
-
Triglyceride glucose-waist to height ratio
- TyG-BMI:
-
Triglyceride glucose-body mass index
- TyG-WC:
-
Triglyceride glucose-waist circumference
- OR:
-
Odds ratio
- CI:
-
Confidence interval
- IR:
-
Insulin resistance
- NHANES:
-
National Health and Nutrition Examination Survey
- CHD:
-
Coronary heart disease
References
Tao LC, Xu JN, Wang TT, Hua F, Li JJ. Triglyceride-glucose index as a marker in cardiovascular diseases: landscape and limitations. Cardiovasc Diabetol. 2022;21:68.
Tsao CW, Aday AW, Almarzooq ZI, Alonso A, Beaton AZ, Bittencourt MS, Boehme AK, Buxton AE, Carson AP, Commodore-Mensah Y, et al. Heart Disease and Stroke Statistics-2022 update: a Report from the American Heart Association. Circulation. 2022;145:e153–639.
Liang X, Huang Y, Han X. Associations between coronary heart disease and risk of cognitive impairment: a meta-analysis. Brain Behav. 2021;11:e02108.
Powell-Wiley TM, Poirier P, Burke LE, Despres JP, Gordon-Larsen P, Lavie CJ, Lear SA, Ndumele CE, Neeland IJ, Sanders P, et al. Obesity and Cardiovascular Disease: A Scientific Statement from the American Heart Association. Circulation. 2021;143:e984–1010.
Dugani SB, Moorthy MV, Li C, Demler OV, Alsheikh-Ali AA, Ridker PM, Glynn RJ, Mora S. Association of Lipid, inflammatory, and metabolic biomarkers with age at Onset for Incident Coronary Heart Disease in Women. JAMA Cardiol. 2021;6:437–47.
Demirci I, Haymana C, Candemir B, Meric C, Yuksel B, Eser M, Akin O, Akin S, Ersoz Gulcelik N, Sonmez A. Triglyceride-glucose index levels in patients with congenital hypogonadotropic hypogonadism and the relationship with endothelial dysfunction and insulin resistance. Endokrynol Pol. 2021;72:232–7.
Ahn SH, Lee JH, Lee JW. Inverse association between triglyceride glucose index and muscle mass in Korean adults: 2008–2011 KNHANES. Lipids Health Dis. 2020;19:243.
Jiang ZZ, Zhu JB, Shen HL, Zhao SS, Tang YY, Tang SQ, Liu XT, Jiang TA. A high triglyceride-glucose index value is Associated with an increased risk of carotid plaque burden in subjects with prediabetes and New-Onset type 2 diabetes: a real-world study. Front Cardiovasc Med. 2022;9:832491.
Mirr M, Skrypnik D, Bogdanski P, Owecki M. Newly proposed insulin resistance indexes called TyG-NC and TyG-NHtR show efficacy in diagnosing the metabolic syndrome. J Endocrinol Invest. 2021;44:2831–43.
Kim MK, Ahn CW, Kang S, Nam JS, Kim KR, Park JS. Relationship between the triglyceride glucose index and coronary artery calcification in Korean adults. Cardiovasc Diabetol. 2017;16:108.
Behnoush AH, Mousavi A, Ghondaghsaz E, Shojaei S, Cannavo A, Khalaji A. The importance of assessing the triglyceride-glucose index (TyG) in patients with depression: a systematic review. Neurosci Biobehav Rev. 2024;159:105582.
Chen X, Liu D, He W, Hu H, Wang W. Predictive performance of triglyceride glucose index (TyG index) to identify glucose status conversion: a 5-year longitudinal cohort study in Chinese pre-diabetes people. J Transl Med. 2023;21:624.
Sun Z, Liu J, Sun J, Xu Z, Liu W, Mao N, Chu T, Guo H, Che K, Xu X, et al. Decreased Regional spontaneous brain activity and cognitive dysfunction in patients with Coronary Heart Disease: a resting-state functional MRI study. Acad Radiol. 2023;30:1081–91.
Lim J, Kim J, Koo SH, Kwon GC. Comparison of triglyceride glucose index, and related parameters to predict insulin resistance in Korean adults: an analysis of the 2007–2010 Korean National Health and Nutrition Examination Survey. PLoS ONE. 2019;14:e0212963.
Sheng G, Lu S, Xie Q, Peng N, Kuang M, Zou Y. The usefulness of obesity and lipid-related indices to predict the presence of non-alcoholic fatty liver disease. Lipids Health Dis. 2021;20:134.
Cheng Y, Fang Z, Zhang X, Wen Y, Lu J, He S, Xu B. Association between triglyceride glucose-body mass index and cardiovascular outcomes in patients undergoing percutaneous coronary intervention: a retrospective study. Cardiovasc Diabetol. 2023;22:75.
Liu L, Peng J, Wang N, Wu Z, Zhang Y, Cui H, Zang D, Lu F, Ma X, Yang J. Comparison of seven surrogate insulin resistance indexes for prediction of incident coronary heart disease risk: a 10-year prospective cohort study. Front Endocrinol (Lausanne). 2024;15:1290226.
Dang K, Wang X, Hu J, Zhang Y, Cheng L, Qi X, Liu L, Ming Z, Tao X, Li Y. The association between triglyceride-glucose index and its combination with obesity indicators and cardiovascular disease: NHANES 2003–2018. Cardiovasc Diabetol. 2024;23:8.
Xuan W, Liu D, Zhong J, Luo H, Zhang X. Impacts of triglyceride glucose-Waist to height ratio on diabetes incidence: a secondary analysis of a Population-based Longitudinal Data. Front Endocrinol (Lausanne). 2022;13:949831.
Wang Y, Zhuang Y, Lin C, Hong H, Chen F, Ke J. The neutrophil-to-lymphocyte ratio is associated with coronary heart disease risk in adults: a population-based study. PLoS ONE. 2024;19:e0296838.
Yao Y, Wang B, Geng T, Chen J, Chen W, Li L. The association between TyG and all-cause/non-cardiovascular mortality in general patients with type 2 diabetes mellitus is modified by age: results from the cohort study of NHANES 1999–2018. Cardiovasc Diabetol. 2024;23:43.
Abdalla SM, Yu S, Galea S. Trends in Cardiovascular Disease Prevalence by Income Level in the United States. JAMA Netw Open. 2020;3:e2018150.
Che B, Zhong C, Zhang R, Pu L, Zhao T, Zhang Y, Han L. Triglyceride-glucose index and triglyceride to high-density lipoprotein cholesterol ratio as potential cardiovascular disease risk factors: an analysis of UK biobank data. Cardiovasc Diabetol. 2023;22:34.
Zhao J, Fan H, Wang T, Yu B, Mao S, Wang X, Zhang W, Wang L, Zhang Y, Ren Z, Liang B. TyG index is positively associated with risk of CHD and coronary atherosclerosis severity among NAFLD patients. Cardiovasc Diabetol. 2022;21:123.
da Silva A, Caldas APS, Hermsdorff HHM, Bersch-Ferreira AC, Torreglosa CR, Weber B, Bressan J. Triglyceride-glucose index is associated with symptomatic coronary artery disease in patients in secondary care. Cardiovasc Diabetol. 2019;18:89.
Wang X, Xu W, Song Q, Zhao Z, Meng X, Xia C, Xie Y, Yang C, Jin P, Wang F. Association between the triglyceride-glucose index and severity of coronary artery disease. Cardiovasc Diabetol. 2022;21:168.
Wang J, Huang X, Fu C, Sheng Q, Liu P. Association between triglyceride glucose index, coronary artery calcification and multivessel coronary disease in Chinese patients with acute coronary syndrome. Cardiovasc Diabetol. 2022;21:187.
Hu J, Cai X, Li N, Zhu Q, Wen W, Hong J, Zhang D, Yao X, Luo Q, Sun L. Association between triglyceride glucose Index-Waist circumference and risk of first myocardial infarction in Chinese hypertensive patients with obstructive sleep apnoea: an Observational Cohort Study. Nat Sci Sleep. 2022;14:969–80.
Zhu Q, Chen Y, Cai X, Cai L, Hong J, Luo Q, Ren Y, Guo Y, Li N. The non-linear relationship between triglyceride-glucose index and risk of chronic kidney disease in hypertensive patients with abnormal glucose metabolism: a cohort study. Front Med (Lausanne). 2022;9:1018083.
Shi W, Xing L, Jing L, Tian Y, Yan H, Sun Q, Dai D, Shi L, Liu S. Value of triglyceride-glucose index for the estimation of ischemic stroke risk: insights from a general population. Nutr Metab Cardiovasc Dis. 2020;30:245–53.
Alizargar J, Bai CH, Hsieh NC, Wu SV. Use of the triglyceride-glucose index (TyG) in cardiovascular disease patients. Cardiovasc Diabetol. 2020;19:8.
Iliodromiti S, Celis-Morales CA, Lyall DM, Anderson J, Gray SR, Mackay DF, Nelson SM, Welsh P, Pell JP, Gill JMR, Sattar N. The impact of confounding on the associations of different adiposity measures with the incidence of cardiovascular disease: a cohort study of 296 535 adults of white European descent. Eur Heart J. 2018;39:1514–20.
Miao H, Zhou Z, Yang S, Zhang Y. The association of triglyceride-glucose index and related parameters with hypertension and cardiovascular risk: a cross-sectional study. Hypertens Res. 2024;47:877–86.
Chen J, Li M, Hao B, Cai Y, Li H, Zhou W, Song Y, Wang S, Liu H. Waist to height ratio is associated with an increased risk of mortality in Chinese patients with heart failure with preserved ejection fraction. BMC Cardiovasc Disord. 2021;21:263.
Yang Q, Vijayakumar A, Kahn BB. Metabolites as regulators of insulin sensitivity and metabolism. Nat Rev Mol Cell Biol. 2018;19:654–72.
Riehle C, Abel ED. Insulin signaling and heart failure. Circ Res. 2016;118:1151–69.
Aparecida Silveira E, Vaseghi G, de Carvalho Santos AS, Kliemann N, Masoudkabir F, Noll M, Mohammadifard N, Sarrafzadegan N, de Oliveira C. Visceral obesity and its Shared Role in Cancer and Cardiovascular Disease: a scoping review of the pathophysiology and pharmacological treatments. Int J Mol Sci 2020;21.
Roy P, Orecchioni M, Ley K. How the immune system shapes atherosclerosis: roles of innate and adaptive immunity. Nat Rev Immunol. 2022;22:251–65.
Hou P, Fang J, Liu Z, Shi Y, Agostini M, Bernassola F, Bove P, Candi E, Rovella V, Sica G, et al. Macrophage polarization and metabolism in atherosclerosis. Cell Death Dis. 2023;14:691.
Gugliucci A. Biomarkers of dysfunctional visceral fat. Adv Clin Chem. 2022;109:1–30.
Acknowledgements
We thank the National Center for Health Statistics of the Centers for Disease Control for Health Statistics employees for organizing, compiling, and developing the NHANES data and building the public database.
Funding
This work was Sponsored by Fujian provincial health technology project (NO. 2022ZD01008).
Author information
Authors and Affiliations
Contributions
Conceptualization, ZY and WY; Formal analysis, ZY and WY; Methodology, ZY, WY, SP and KJ; Software, WY, SP and KJ; Supervision, KJ and CF; Visualization, KJ and CF; Writing-original draft, ZY and WY; Writing-review & editing, ZY, WY, SP, KJ and CF.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The National Center for Health Statistics Institutional Ethics Review Board examined and authorized studies involving human subjects, and all participants gave their written informed consent to participate in the study after agreeing to the survey and giving their permission in writing.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhuang, Y., Wang, Y., Sun, P. et al. Association between triglyceride glucose-waist to height ratio and coronary heart disease: a population-based study. Lipids Health Dis 23, 162 (2024). https://doi.org/10.1186/s12944-024-02155-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12944-024-02155-4