
Abstract
Background
It is believed that deposition of amyloid beta (Aβ) in the brain is the central pathological changes of Alzheimer’s disease (AD), which triggers a series of pathological processes. However, the relationship between dyslipidemia and AD is uncertain. Considering the peripheral Aβ levels are related to brain Aβ deposition, we explore the relationships between blood lipids and plasma Aβ.
Methods
Participants who lived in the selected village of Xi’an for more than 3 years were enrolled, aged 40–85 years (n = 1282, 37.9% male). Fasting blood lipid, plasma Aβ levels, basic information and living habits were measured. Multiple linear regressions were used.
Results
In total population, blood lipids were not associated with plasma Aβ. After stratified by blood pressure, serum total cholesterol (TC) and low-density lipoprotein (LDL-c) were positively associated with plasma Aβ42 levels (βTC = 0.666, PTC = 0.024; βLDL-c = 0.743, PLDL-c = 0.011, respectively) in normal blood pressure. LDL-c was negatively associated with plasma Aβ40 levels (β = − 0.986, P = 0.037) in high blood pressure.
Conclusion
Elevated plasma Aβ42 levels are associated with higher TC and LDL-c in normal blood pressure. Elevated plasma Aβ40 levels are associated with lower LDL-c in high blood pressure. This indicated that the relationships between blood lipids and plasma Aβ were confounded by blood pressure.
Similar content being viewed by others


Introduction
Alzheimer’s disease (AD) is the most common cause of dementia. Toxic plaque formed by the deposition of amyloid beta (Aβ) peptide in the brain is the main characteristic pathogenesis of AD [1]. Aβ peptides are natural products of metabolism consisting of 39 to 43 amino acids, formed by fragmentation of amyloid-β protein precursor (APP) through the sequential enzymatic actions of secretases [2]. In the process of Aβ formation, APP is first cleaved by β-secretase (known as BACE1), releasing sAPPβ into the extra cellular fluid and cerebrospinal fluid (CSF). The remaining fragment is then cleaved by γ-secretase to produce damaging amyloid-β42 (Aβ42) and other Aβ isoform (Aβ40 down to Aβ17). In addition, full-length APP is also cleaved by β and α-secreatase to form Aβ16 down to Aβ13 [3]. Under normal circumstance, most of the production is amyloid-β40 (Aβ40) and only a small amount of Aβ42 which is more likely to deposit and has neurotoxic. Aβ present in the brain can be eliminated by various means, including degradation of Aβ degrading enzymes, cell clearance, blood brain barrier (BBB) transport, CSF and interstitial lymphatic drainage, clearance of peripheral cells and tissues, etc. Due to the imbalance of Aβ production and clearance, a large number of neuritic plaques (formed by Aβ deposition) are present in the cerebral cortex, hippocampus, and some subcortical nuclei. Aβ deposition in the brain may be the initiating factor in AD process, which is called “amyloid hypothesis” [4]. It has been suggested that Aβ levels in the brain and plasma are in a dynamic balance. Deposition of Aβ in the brain subsequently affects plasma concentration [5]. Peripheral transport of Aβ can reduce its accumulation in the brain, suggesting that the Aβ concentration in plasma is related to the deposition of Aβ in the brain [6].
Dyslipidemia is one of the important risk factor for cardiovascular disease and stroke. Numerous studies showed that blood lipids were also significantly associated with the risk of AD [7,8,9], but with conflicting results. Several epidemiological, laboratory research and clinical studies supported the hypothesis that higher levels of cholesterol may induce the development of AD [10,11,12,13], while others had not confirmed or inversed association with the risk of AD [14,15,16]. The effects of blood lipids levels on Aβ deposition in the brain were unclear.
Considering that plasma Aβ concentration is related to cerebral Aβ levels and mounting evidence had indicated that blood pressure is related to plasma Aβ levels significantly, we conducted a cross-sectional study to explore the effects of blood pressure on the relationships between blood lipids and plasma Aβ levels in a community population.
Methods
Participants
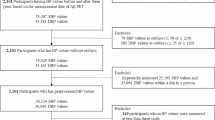
From October 2014 to March 2015, all aged 40 or more villagers in Qubao village which taken by cluster sampling method near Xi’an were enrolled. There were similar lifestyles and population composition between this village and other rural areas of Xi’an. Inclusion criteria: 1) resident villager or who has lived in this area for 3 years or more, 2) agree to participate in this study and provided informed consent (N = 2011). Exclusion criteria: 1) severe cardiac, pulmonary, liver, kidney dysfunction, hematological, acute infection, or tumors, 2) those who have taken lipid-lowering drugs (n = 70), 3) those who showed aberrant plasma Aβ42, Aβ40 levels (n = 529) or blood lipids levels (n = 2) (exceeding 3 standard deviations from the mean), 4) sample hematolysis (n = 128). Total of 1282 participants were included in our analysis (Fig. 1).

Flow chart of participant screening. Aβ, amyloid beta
Definition of covariates
The diseases and related conditions involved in this study are defined according to the guidelines [17, 18] as follows: 1) A person with a current systolic blood pressure (SBP) ≥140 mmHg and/or diastolic blood pressure (DBP) ≥90 mmHg is defined as high blood pressure. On the contrary, it is defined as normal blood pressure. Blood pressure measured with taking antihypertensive drugs and/or a current SBP ≥ 140 mmHg and/or a DBP ≥90 mmHg is defined as a hypertensive patient. 2) High fasting blood glucose (FBG) was defined as at least 7 mmol/L. 3) According the guidelines for the prevention and treatment of dyslipidemia in Chinese adults (revised edition 2016), high serum total cholesterol (TC) was defined as at least 5.18 mmol/L, high triglyceride (TG) was defined as at least 1.70 mmol/L, high serum low-density lipoprotein (LDL-c) was defined as at least 3.37 mmol/L and low serum high-density lipoprotein (HDL-c) was defined as less than 1.04 mmol/L. Any abnormality in blood lipids is defined as dyslipidemia. 4) Apolipoprotein E (ApoE ε4) carriers were defined as having at least one allele of ε4, while non-carriers referred to the ones without any ε4 allele.
Questionnaire survey
A uniform questionnaire was used for all subjects, first of all, face to face consultation to collect general information, followed by physical examination and blood sample collection.
Blood pressure measurement
Blood pressure (BP) was measured by a nurse using a mercury sphygmomanometer on each participant’s right arm with a regular adult cuff (Shanghai Medical Instruments Co. Shanghai, China) in the morning, before breakfast (from 8 a.m. to 10 a.m.). Setting BP was measure again after 10 min of rest, and the average of the twice was recorded.
Laboratory evaluation
All subjects were collected 5 ml of venous blood sample from 8 a.m. in the morning (at least 8 h on an empty stomach). 1) Then the blood sample was placed in a serum tube containing a coagulant and was gently inverted upside and down and stood for 30 min. Next, the sample was centrifuged at 3000 rpm for 15 min at room temperature for 2 h and quickly stored at − 80 °C until later measurement. TC, TG, HDL-c and LDL-c levels were detected by enzymatic method using an automated biochemical analyzer (C501, Roche, Sweden). Quality indicators accord with the quality requirements set by the US National Cholesterol Education Program. 2) Plasma levels of Aβ40, Aβ42 were measured with commercially available quantitative enzyme-linked immunosorbent assay kits (ELISA, Yuanye Co. Shanghai, China), and the sensitivity of each assay was 1.0 pg/ml, respectively. Measurements were performed using an RT-6000 analyzer (Rayto Co. Shenzhen. China) at 450 nm, and concentrations were calculated from the standard curve. All measurements were performed in duplicate and the results averaged. The intra-assay and inter-assay coefficients of variation were less than 7 and 9%, respectively. 3) Determination of ApoE genotypes: According to manufacturer’s protocol, genomic DNA from blood samples in the EDTA anticoagulant tubes was extracted by blood genomic deoxyribonucleic acid (DNA) extraction kit (Tiangen Co. Beijing. China). We amplified 244 base pair of the ApoE gene fragment using a polymerase chain reaction (PCR) thermocycler, the length of which included two polymorphic sites at amino acid residues 112 and 158(15). Sequence of the PCR products was tested by Sanger sequencing (Sangon Co. Shanghai. China). Finally, we used direct interpretation of the sequencing chromatogram to determine the ApoE genotype.
Statistical analysis
Before doing statistical analysis, we tested the distribution of each covariate by using Skewness, Kurtosis and P-P plots. Covariates that nearly conformed to normal distribution included age, pulse rate, waistline, hip circumference, BMI, SBP, DBP, TC, HDL-c, LDL-c which were expressed as mean (SD) and were compared between different groups by using an unpaired Student’s t-test. Non-normal distribution covariates included education, levels of TG and FBG were expressed as median (interquartile range) and were compared by Mann-Whitney U-test. Categorical variables were expressed as the number (percentage) and were compared by X2test. For serum lipid, participants were divided into dyslipidemia group and normal blood lipids group. Differences between two groups were compared. We used simple linear correlation scatter plot to roughly observe the linear trend between blood lipids and plasma Aβ levels. We performed multiple liner regression models to explore the statistical significance of the association after adjusting for other confounding factors including age, sex, education years, smoking, drinking, physical activity level, and history of heart disease, waist circumference, hip circumference, BMI, pulse rate, SBP, DBP, FBG and ApoE ε4 genotype (ApoE is involved in the regulation of Aβ metabolism, aggregation and deposition [19]).
Two secondary analyses were performed. First, associations between blood lipids and Aβ were analyzed in total study population. Because TC was collinear with LDL-c, two models were built. Model 1: TG, TC, HDL-c and other covariates mentioned above. Model 2: TG, LDL-c, HDL-c and other covariates mentioned above. Second, to rule out the possibility of BP affecting the relationship between blood lipids and plasma Aβ, we divided the total population into high blood pressure and normal blood pressure according to the standard of SBP greater than or equal to 140 mmHg and/or DBP greater than or equal to 90 mmHg and compared the relationship again in new two-tiered crowd (Model 3, Model 4).
All statistical analyses were performed with IBM SPSS Statistics version 24.0. A two-side P value of less than 0.05 was the threshold for statistical significance.
Results
Characteristics of the population
As shown in the Table 1, participants with dyslipidemia (n = 644) were older, higher ratios of hypertension, diabetes mellitus, higher levels of BMI, SBP, DBP, FBG, TC, LDL-c, TG and lower levels of education and HDL-c than those with normal lipids.
Association between plasma Aβ levels and blood lipids in the total population
In the total population, plasma Aβ levels had no differences between dyslipidemia group and normal lipids group (Table 2). No linear trends were found (Figs. 2, 3). After adjusting for confounding factors as described above, no correlations were found between blood lipids and plasma Aβ levels (Table 3).

Correlations of TC, Log TG, HDL-c, LDL-c and plasma Aβ42 in total study population. Simple linear correlations between TC, Log TG, HDL-c, LDL-c and plasma Aβ42 were shown respectively in picture (a, b, c, d). Aβ, amyloid beta. TC, total cholesterol. TG, triglyceride. HDL-c, high-density lipoprotein. LDL-c, low-density lipoprotein

Correlations of TC, Log TG, HDL-c, LDL-c and plasma Aβ40 in total study population. Simple linear correlations between TC, Log TG, HDL-c, LDL-c and plasma Aβ40 were shown respectively in picture (a, b, c, d). Aβ, amyloid beta. TC, total cholesterol. TG, triglyceride. HDL-c, high-density lipoprotein. LDL-c, low-density lipoprotein
The effects of blood pressure on plasma Aβ levels and blood lipids levels
After re-stratified by blood pressure (Table 4), participants with high blood pressure (n = 548) were older, more diabetes mellitus, cardiovascular disease and stroke, high levels of waistline, hip circumference, BMI, SBP, DBP, FBG, TC, LDL-c, TG and a lower levels of education and HDL-c levels.
Association of plasma Aβ levels and blood lipids stratified by blood pressure
In normal blood pressure group, Aβ42 levels were higher in the high TC and high LDL-c group than that in the normal group (Table 5). Positive linear trends were found between TC, LDL-c levels and plasma Aβ42 levels in normal blood pressure group (Fig. 4a, b). Negative linear trend was found between LDL-c levels and plasma Aβ40 levels in high blood pressure group (r = − 0.089, P = 0.038). Consistent with previous analysis, TC and LDL-c were independently and positively associated with plasma Aβ42 levels after re-stratified in the normal blood pressure. LDL-c was negatively associated with plasma Aβ40 levels in high blood pressure group (Table 6).

Correlations of TC, LDL-c and plasma Aβ42 in normal blood pressure group. Simple linear correlations between TC, LDL-c and plasma Aβ42 were shown respectively in picture (a, b). Aβ, amyloid beta. TC, total cholesterol. LDL-c, low-density lipoprotein
Discussion
In this population-based study, we found that TC and LDL-c were positively correlated with plasma Aβ42 levels in normal blood pressure. LDL-c was negatively associated with plasma Aβ40 levels in the high blood pressure. This finding was independent of age, sex, ApoE ε4 and other confounding factors. This indicated that the relationships between blood lipids and plasma Aβ were confounded by blood pressure.
Studies have shown that hyperlipidemia may play a role in the development of AD [20]. A 13-year follow-up study showed that higher LDL-c and TC levels were associated with an increased risk of AD [7]. A study containing 7053 community-dwelling elderly suggested low TG was associated with decreased incident AD in women [21]. Elevated HDL-c levels might be associated with a decreased risk of AD were also found in elderly individuals [8]. Therefore, elevated blood lipids may play a role in the progression of AD [9].
However, the relationship between blood lipids and plasma Aβ is not fully determined. Positively correlation of HDL-c levels with Aβ42 in not using statins was observed and no relationships of Aβ42 with TC and LDL-c [22]. Inverse trend was observed between HDL-c and Aβ42 levels, although not significant [23]. Regression analysis considering the multiple influences of baseline parameters TC, LDL-c, HDL-c, TG, BMI, lnHbA1c and presence of at least one ApoE ε4 allele on the lnAβ42 at 5 years revealed TC as the only significant predictor. Excluding TC from the list of independent variables, LDL-c was the single negative predictor [24]. A double-blind, randomized, placebo-controlled study showed that after giving subjects with lovastatin 40 mg or 60 mg per day for 3 months, serum Aβ concentrations were lower than baseline measurements compared with the placebo group [25]. There was also reports in the literature that pravastatin at 10 mg/d does not decrease plasma levels of either Aβ40 or Aβ42 in humans [26]. The possible reason for the difference between the reported results in the literature and our study may be the research population, inclusion criteria, exclusion criteria and method for measuring Aβ has not been unified [27]. Compared with the INNO-BIA assay, the ELISA measured Aβ40 levels are slightly lower and Aβ42 levels are slightly higher [27]. Our previous research has proved the methods are credible [28, 29]. More research is still needed.
In present study, we did not find the relationship between dyslipidemia and plasma Aβ levels in the total population. However, after stratified by blood pressure, we found that TC and LDL-c were positively correlated with plasma Aβ42 levels in normal blood pressure, but not in the hypertension group, indicated that the relationship between blood lipids and Aβ is confounded by the blood pressure. Hypertension is the most important risk factor for cardiovascular disease and stroke. Also, growing evidence indicate that hypertension is a major risk factor for AD. Hypertension has an effect on blood lipids and Aβ [30]. Elevated blood pressure had effects on the Aβ [31,32,33]. Our previous study found that elevation in PP was associated with increased plasma Aβ40 and decreased log-transformed soluble advanced glycosylation end product-specific receptor (sRAGE), the underlying mechanism may be relevant to peripheral Aβ clearance [31]. Therefore, we explored the effect of blood pressure on the relationship between blood lipids and plasma Aβ.
The mechanism of dislipidemia related to plasma Aβ levels is not clear. Hypercholesterolemia may cause the deposition of Aβ in the brain by affecting the translocation of endothelial cells across the BBB [34]. The injured BBB in turn induces inflammation, resulting in an increase gap of brain microvascular endothelial cells [35, 36]. The damage of BBB may affect the expression of low-density lipoprotein receptor-related protein 1 (LRP1) and decrease the function of Aβ transport out of the brain. It may also promotes the expression of RAGE and increase the transport of plasma Aβ to the central nervous system, which ultimately causes Aβ deposition in the brain [37]. These findings suggest that dyslipidemia is associated with increased Aβ deposition in the brain. The process of brain Aβ from the center to the periphery is its main pathway of clearance, elevated plasma Aβ levels associated with increased Aβ deposition in the brain [38]. Therefore, blood lipids are associated with plasma Aβ may relate to the increased deposition of Aβ in the brain.
Recent years, study had also suggested that hyperlipidemia can affect Aβ metabolism [39]. TC is mainly concentrated in membrane microdomains termed lipid rafts where considerable evidence indicates that the amyloidogenic processing of APP largely occurs [39]. TC can enhance the activity of BACE1 (the rate-limiting enzyme for Aβ generation) and promote it’s localization to lipid rafts, otherwise, it can also act as a positive regulator of γ-secretase to further increase the activity of it [40]. BACE1 transcription increased in mice feed with high-fat and TC, suggesting that hypercholesterolemia increases the production of Aβ by affecting the activity of secretase [41]. In addition, increased TC in cell membranes can inhibit the function of α-secretase, promote the cleavage of APP by β-secretase and γ-secretase, and eventually lead to increased Aβ production [42].
An important question is why TC and LDL-c are related to plasma Aβ42 in normal blood pressure, and why LDL-c is correlated with plasma Aβ40 in high blood pressure rather than Aβ42. Aβ peptides are mainly produced in the brain, are transported to the cerebrospinal fluid and plasma, and are degraded in the periphery [43]. This degradation is of importance as it allows lowering the whole brain Aβ content. Aβ peptides, particularly Aβ42, are highly water insoluble molecules requiring lipid environments to be transported to the places of their degradation or excretion [44]. In addition, in normal blood pressure, the blood vessels walls are not damaged and transportation of Aβ is unrestricted. This is not the case in high blood pressure, where blood vessels might be damaged and transportation of Aβ peptides is consequently deteriorated. Therefore, in normal blood pressure, Aβ42 correlated with TC and LDL-c may as it’s strongly hydrophobic and the integrity of the vascular wall. In high blood pressure, Aβ40 peptides negatively associated with LDL-c as lower amount of Aβ peptides are transported through the blood vessels at all. Moreover, Aβ is highly hydrophobic peptides and requires lipid environment for its solubility. Positive correlation of TC and LDL-c with Aβ42 might simply reflect the better condition for solubility.
Limitations
First, the design of this study did not allow for causal assumptions between plasma Aβ levels and dyslipidemia. It was difficult to determine whether dyslipidemia led to plasma Aβ change. The results need to be validated in additional longitudinal cohort studies. Second, we did not analyze the relationships of dyslipidemia and plasma Aβ levels in mild cognitive impairment (MCI) or dementia patients because of the rather small sample size. Third, Aβ deposition in the brain or CSF could not be obtained. The effects of peripheral Aβ clearance on brain Aβ accumulation must be investigated. Finally, we did not detect blood oxidized low-density lipoprotein (ox-LDL) level. It has been reported that ox-LDL is more toxic and plays a more important role in the pathogenesis of AD [45].
Conclusions
In summary, out research find that elevated plasma Aβ42 levels are associated with higher TC and higher LDL-c in normal blood pressure. Elevated plasma Aβ40 levels are associated with lower LDL-c in high blood pressure. This indicated that the relationship between blood lipids and plasma Aβ was confounded by blood pressure. Considering the close relationship between plasma Aβ and deposition in the brain, we explore the relationship between plasma Aβ and blood lipids to provide some help for the auxiliary diagnosis of AD. Additional large-scale cohort studies and convincible evidence-based medical researches are required.
Availability of data and materials
The data used in this study are available from the corresponding author if needed.
Abbreviations
- AD:
-
Alzheimer’s disease
- APP:
-
Amyloid beta protein precursor
- Aβ:
-
Amyloid beta
- BBB:
-
Blood brain barrier
- DBP:
-
Diastolic blood Pressure
- FBG:
-
Fast blood glucose
- HDL-c:
-
High-density lipoprotein
- LDL-c:
-
Low-density lipoprotein
- LRP1:
-
Low-density lipoprotein receptor-related protein 1
- PCR:
-
Polymerase chain reaction
- PP:
-
Pulse pressure
- RAGE:
-
Advanced glycosylation end product-specific receptor
- SBP:
-
Systolic blood pressure
- TC:
-
Total cholesterol
- TG:
-
Triglyceride
References
Hardy J, Selkoe DJ. Medicine - the amyloid hypothesis of Alzheimer's disease: Progress and problems on the road to therapeutics. Sci. 2002;297:353–6.
Chow VW, Mattson MP, Wong PC, Gleichmann M. An overview of APP processing enzymes and products. NeuroMolecular Med. 2010;12:1–12.
Blennow K, Hampel H, Weiner M, Zetterberg H. Cerebrospinal fluid and plasma biomarkers in Alzheimer disease. Nat Rev Neurol. 2010;6:131–44.
Querfurth HW, LaFerla FM. Mechanisms of disease Alzheimer's disease. N Engl J Med. 2010;362:329–44.
Shah NS, Vidal JS, Masaki K, Petrovitch H, Ross GW, Tilley C, et al. Midlife blood pressure, plasma beta-amyloid, and the risk for Alzheimer disease the Honolulu Asia aging study. Hypertens. 2012;59:780–U782.
DeMattos RB, Bales KR, Cummins DJ, Paul SM, Holtzman DM. Brain to plasma amyloid-beta efflux: a measure of brain amyloid burden in a mouse model of Alzheimer's disease. Sci. 2002;295:2264–7.
Schilling S, Tzourio C, Soumare A, Kaffashian S, Dartigues JF, Ancelin ML, et al. Differential associations of plasma lipids with incident dementia and dementia subtypes in the 3C study: a longitudinal, population-based prospective cohort study. PLoS Med. 2017;14.
Reitz C, Tang MX, Schupf N, Manly JJ, Mayeux R, Luchsinger JA. Association of Higher Levels of high-density lipoprotein cholesterol in elderly individuals and lower risk of late-onset Alzheimer disease. Arch Neurol. 2010;67:1491–7.
Cedazo-Minguez A, Ismail MA, Mateos L. Plasma cholesterol and risk for late-onset Alzheimer's disease. Expert Rev Neurother. 2011;11:495–8.
Kivipelto M, Helkala EL, Laakso MP, Hanninen T, Hallikainen M, Alhainen K, et al. Midlife vascular risk factors and Alzheimer's disease in later life: longitudinal, population based study. Br Med J. 2001;322:1447–51.
Solomon A, Kareholt I, Ngandu T, Winblad B, Nissinen A, Tuomilehto J, et al. Serum cholesterol changes after midlife and late-life cognition - twenty-one-year follow-up study. Neurol. 2007;68:751–6.
Sparks DL, Scheff SW, Hunsaker JC, Liu HC, Landers T, Gross DR. Induction of Alzheimer-like Beta-amyloid Immunoreactivity in the brains of rabbits with dietary-cholesterol. Exp Neurol. 1994;126:88–94.
Simons M, Keller P, De Strooper B, Beyreuther K, Dotti CG, Simons K. Cholesterol depletion inhibits the generation of beta-amyloid in hippocampal neurons. Proc Natl Acad Sci U S A. 1998;95:6460–4.
Li G, Shofer JB, Kukull WA, Peskind ER, Tsuang DW, Breitner JCS, et al. Serum cholesterol and risk of Alzheimer disease - a community-based cohort study. Neurol. 2005;65:1045–50.
Mielke MM, Zandi PP, Sjogren M, Gustafson D, Ostling S, Steen B, et al. High total cholesterol levels in late life associated with a reduced risk of dementia. Neurol. 2005;64:1689–95.
Stewart R, White LR, Xue QL, Launer LJ. Twenty-six-year change in total cholesterol levels and incident dementia - the Honolulu-Asia aging study. Arch Neurol. 2007;64:103–7.
Mancia G, Fagard R, Narkiewicz K, Redon J, Zanchetti A, Bohm M, et al. ESH/ESC guidelines for themanagement of arterial hypertension the task force for the management ofarterial hypertension of the European society ofHypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens. 2013;2013(31):1281–357.
Xu Y, Wang LM, He J, Bi YF, Li M, Wang TG, et al. Prevalence and control of diabetes in Chinese adults. JAMA. 2013;310:948–58.
Kanekiyo T, Xu HX, Bu GJ. ApoE and a beta in Alzheimer's disease: accidental encounters or partners? Neuron. 2014;81:740–54.
Proitsi P, Kim M, Whiley L, Simmons A, Sattlecker M, Velayudhan L, et al. Association of blood lipids with Alzheimer's disease: a comprehensive lipidomics analysis. Alzheimers Dement. 2017;13:140–51.
Ancelin ML, Ripoche E, Dupuy AM, Barberger-Gateau P, Auriacombe S, Rouaud O, et al. Sex differences in the associations between lipid levels and incident dementia. J Alzheimers Dis. 2013;34:519–28.
Abdullah L, Luis C, Paris D, Ait-ghezala G, Mouzon B, Allen E, et al. High serum a beta and Vascular risk factors in first-degree relatives of Alzheimer's disease patients. Mol Med. 2009;15:95–100.
Balakrishnan K, Verdile G, Mehta PD, Beilby J, Nolan D, Galvao DA, et al. Plasma a beta 42 correlates positively with increased body fat in healthy individuals. J Alzheimers Dis. 2005;8:269–82.
Blasko I, Kemmler G, Jungwirth S, Wichart I, Weissgram S, Jellinger K, et al. Prospective study on association between plasma amyloid beta-42 and atherosclerotic risk factors. J Neural Transm. 2011;118:663–72.
Friedhoff LT, Cullen EI, Geoghagen NSM, Buxbaum JD. Treatment with controlled-release lovastatin decreases serum concentrations of human beta-amyloid (a beta) peptide. Int J Neuropsychopharmacol. 2001;4:127–30.
Ishii K, Tokuda T, Matsushima T, Miya F, Shoji S, Ikeda S, et al. Pravastatin at 10 mg/day does not decrease plasma levels of either amyloid-beta (a beta) 40 or a beta 42 in humans. Neurosci Lett. 2003;350:161–4.
Brown BM, Peiffer JJ, Taddei K, Lui JK, Laws SM, Gupta VB, et al. Physical activity and amyloid-beta plasma and brain levels: results from the Australian imaging, biomarkers and lifestyle study of ageing. Mol Psychiatry. 2013;18:875–81.
Zhao BY, Shang SH, Li P, Chen C, Dang LJ, Jiang Y, et al. The gender- and age- dependent relationships between serum lipids and cognitive impairment: a cross-sectional study in a rural area of Xi'an, China. Lipids Health Dis. 2019;18.
Gao L, Jiang Y, Wei S, Shang S, Li P, Chen C, et al. The level of plasma amyloid-beta(40) is correlated with peripheral transport proteins in cognitively Normal adults: a population-based cross-sectional study. J Alzheimers Dis. 2018;65:951–61.
Sharma R, Raghuram TC, Rao UB, Moffatt RJ, Krishnaswamy K. The effect of fat intake and antihypertensive drug therapy on serum lipid profile: a cross-sectional survey of serum lipids in male and female hypertensives. Mol Cell Biochem. 2010;343:37–47.
Jiang Y, Shang SH, Li P, Chen C, Dang L, Wang JJ, et al. Pulse pressure is associated with plasma amyloid-beta transport dysfunction. J Hypertens. 2018;36:569–79.
Zhao W, Wang J, Ho L, Ono K, Teplow DB, Pasinetti GM. Identification of antihypertensive drugs which inhibit amyloid-beta protein Oligomerization. J Alzheimers Dis. 2009;16:49–57.
Langbaum JBS, Chen KW, Launer LJ, Fleisher AS, Lee W, Liu XF, et al. Blood pressure is associated with higher brain amyloid burden and lower glucose metabolism in healthy late middle-age persons. Neurobiol Aging. 2012;33.
Cao DF, Fukuchi KI, Wan H, Kim H, Li L. Lack of LDL receptor aggravates learning deficits and amyloid deposits in Alzheimer transgenic mice. Neurobiol Aging. 2006;27:1632–43.
Ehrlich D, Humpel C. Chronic vascular risk factors (cholesterol, homocysteine, ethanol) impair spatial memory, decline cholinergic neurons and induce blood-brain barrier leakage in rats in vivo. J Neurol Sci. 2012;322:92–5.
Acharya NK, Levin EC, Clifford PM, Han M, Tourtellotte R, Chamberlain D, et al. Diabetes and hypercholesterolemia increase blood-brain barrier permeability and brain amyloid deposition: beneficial effects of the LpPLA2 inhibitor Darapladib. J Alzheimers Dis. 2013;35:179–98.
Chen C, Li XH, Tu Y, Sun HT, Liang HQ, Cheng SX, et al. A beta-AGE AGGRAVATES COGNITIVE DEFICIT IN RATS VIA RAGE PATHWAY. Neurosci. 2014;257:1–10.
Marques MA, Kulstad JJ, Savard CE, Green PS, Lee SP, Craft S, et al. Peripheral amyloid-beta levels regulate amyloid-beta clearance from the central nervous system. J Alzheimers Dis. 2009;16:325–9.
Gamba P, Testa G, Sottero B, Gargiulo S, Poli G, Leonarduzzi G. The link between altered cholesterol metabolism and Alzheimer's disease. Environ Stressors Biol Med. 2012;1259:54–64.
Wahrle S, Das P, Nyborg AC, McLendon C, Shoji M, Kawarabayashi T, et al. Cholesterol-dependent gamma-secretase activity in buoyant cholesterol-rich membrane microdomains. Neurobiol Dis. 2002;9:11–23.
Wang RS, Li JJ, Diao SY, Kwak YD, Liu L, Zhi LT, et al. Metabolic stress modulates Alzheimer's beta-Secretase gene transcription via SIRT1-PPAR gamma-PGC-1 in neurons. Cell Metab. 2013;17:685–94.
Vetrivel KS, Thinakaran G. Membrane rafts in Alzheimer's disease beta-amyloid production. Biochim Biophys Acta. 1801;2010:860–7.
Tarasoff-Conway JM, Carare RO, Osorio RS, Glodzik L, Butler T, Fieremans E, et al. Clearance systems in the brain-implications for Alzheimer disease. Nat Rev Neurol. 2015;11:457–70.
Jung SS, Nalbantoglu J, Cashman NR. Alzheimer's beta-amyloid precursor protein is expressed on the surface of immediately ex vivo brain cells: a flow cytometric study. J Neurosci Res. 1996;46:336–48.
Aldred S, Bennett S, Mecocci P. Increased low-density lipoprotein oxidation, but not total plasma protein oxidation, in Alzheimer's disease. Clin Biochem. 2010;43:267–71.
Acknowledgements
We were thankful for the cooperation of all participants in our study.
Funding
This work was supported by the Nature Science Foundation of China (No. 81771168) and the Key Research & Development Programs of Shanxi Province (No. 2018ZDXM-SF-052).
Author information
Authors and Affiliations
Contributions
HNW took part in the survey, did the statistical analysis and wrote the manuscript. GL performed the analysis and data acquisition. SSH designed the study, collected and took part in the statistical analysis. WS contributed to the treatment of the blood specimens. CC, JY, DLJ, WJ, HK, DMY, and WJY took part in the survey and collected samples. QQM provided technical guidance in all stages of the study. All authors have read and approved the final article.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All individuals received information about the study and were able to cooperate to complete the questionnaire survey. For illiterate participants, their relatives agreed on the informed consent. The privacy rights of the participants had always been observed. The Ethics Committee of The First Affiliated Hospital of Xi’an JiaoTong University gave ethical approval.
Consent for publication
All the participants provided written informed consent for the publication of the results of this study.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Hu, N., Gao, L., Jiang, Y. et al. The relationship between blood lipids and plasma amyloid beta is depend on blood pressure: a population-based cross-sectional study. Lipids Health Dis 19, 8 (2020). https://doi.org/10.1186/s12944-020-1191-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12944-020-1191-4