
Abstract
Background
Previously reported associations between vitamin D status, as measured by serum 25-hydroxyvitamin D [25(OH)D] concentrations, and cardiometabolic risk factors were largely limited by variability in 25(OH)D assay performance. In accordance with the Vitamin D Standardization Program, serum 25(OH)D measurement was recently standardized in the National Health and Nutrition Examination Survey (NHANES) to reduce laboratory and method related differences in serum 25(OH)D results. We evaluated the overall and ethnic-specific associations between the newly standardized serum 25(OH)D concentrations and cardiometabolic risk in U.S. adults.
Methods
This study examined standardized 25(OH)D data from five cycles of the NHANES (2001–2010). The total sample included 7674 participants (1794 Mexican-Americans, 4289 non-Hispanic whites, and 1591 non-Hispanic blacks) aged ≥ 20 years who were examined in the morning after overnight fasting. Serum 25(OH)D was directly measured by liquid chromatography-tandem mass spectrometry (LC-MS/MS) in 2007–2010, and was predicted from LC-MS/MS equivalents for 2001–2006. Serum 25(OH)D levels were categorized into quartiles (<43.4, 43.4–58.6, 58.7–74.2, ≥74.3 nmol/L). Cardiometabolic risk was defined by the homeostatic model assessment of insulin resistance (HOMA-IR), metabolic syndrome (MetS), and Framingham cardiovascular disease (CVD) risk. Prevalence ratios and 95% confidence intervals were calculated using modified Poisson regression.
Results
After full adjustment for confounders, serum 25(OH)D ≥74.3 nmol/L was associated with lower cardiometabolic risk compared to 25(OH)D <43.4 nmol/L in the overall sample [HOMA-IR: 0.70 (0.59, 0.84); MetS: 0.82 (0.74, 0.91); CVD risk: 0.78 (0.66, 0.91)]. These associations remained significant in Mexican-Americans [HOMA-IR: 0.54 (0.35, 0.82); MetS: 0.73 (0.55, 0.96)], non-Hispanic whites [HOMA-IR: 0.81 (0.68, 0.96); MetS: 0.84 (0.73, 0.95); CVD risk: 0.78 (0.64, 0.93)]; and in non-Hispanic blacks [HOMA-IR: 0.67 (0.45, 0.99); MetS: 0.75 (0.56, 0.97); CVD risk: 0.58 (0.41, 0.81)].
Conclusions
Low vitamin D status is a significant risk factor for cardiometabolic disease in U.S. adults based on standardized serum 25(OH)D results, irrespective of ethnic background. Future studies using standardized 25(OH)D data are needed to confirm these results, particularly amongst U.S. blacks with 25(OH)D concentrations above 75 nmol/L.
Similar content being viewed by others

Background
A role in the renin-angiotensin aldosterone system (RAAS) and extensive immunomodulatory properties have identified vitamin D as a potential modifiable risk factor in cardiometabolic disorders [1–3]. Measurement of vitamin D status is based on circulating total 25-hydroxyvitamin D [25(OH)D] concentrations, which reflect both food intake and endogenous production of vitamin D. Low serum 25(OH)D levels have been linked to a range of non-skeletal health conditions in adults, including metabolic disorders and cardiovascular diseases [4–8]. In addition, vitamin D is thought to play a protective role against the development of type-2 diabetes by improving the insulin secretion of pancreatic beta cells and by maintaining glucose homeostasis [9–13]. However, studies investigating the relation between vitamin D status and cardiometabolic disorders are inconsistent [14–17]. Among the possible explanations for this discrepancy include the substantial heterogeneity among definitions for vitamin D deficiency, different age and ethnic distributions, and large variations in the performance of serum 25(OH)D assays.
Previous analyses of the NHANES have relied on unstandardized serum 25(OH)D measured by the Diasorin radioimmunoassay (RIA) kit, a method that has been criticized for its lack of precision and documented bias [18, 19]. In accordance with the vitamin D Standardization Program (VDSP), the National Center for Health Statistics (NCHS) of the Centers for Disease Control and Prevention (CDC) recently released the standardized serum 25(OH)D data files in October, 2015 [20]. The standardized 25(OH)D data provide the most reliable estimates of serum 25(OH)D concentrations using the ultra-high performance liquid chromatography-tandem mass spectrometry (LC-MS/MS) method [21]. The LC-MS/MS method has improved sensitivity and specificity for serum 25(OH)D metabolites compared to previous immunoassay methods, and the standardization of serum 25(OH)D data allows for comparison across different survey cycles of the NHANES, providing sufficient power to study risk associated with varying concentrations of serum 25(OH)D. Thus, previously reported associations between serum 25(OH)D with cardiometabolic disorders using unstandardized serum 25(OH)D data from previous cycles of NHANES (1988–1994, and 2001–2006) were likely affected by method-related variations in serum 25(OH)D assays.
In addition to the assay-related differences in serum 25(OH)D results, ethnic variations in the relationship between vitamin D status and cardiometabolic disorders have been documented, with mixed results. For example, ethnic-specific differences in diabetes risk by serum 25(OH)D status have been confirmed in previous NHANES cycles (1988–1994, and 2001–2006), where an inverse relationship between unstandardized 25(OH)D concentrations and type-2 diabetes risk was observed in Mexican-Americans and non-Hispanic whites, but not in non-Hispanic blacks [22, 23]. Similarly, 25(OH)D concentrations were significantly associated with fatal stroke and heart failure in NHANES III, with increased risk seen in white participants with low 25(OH)D, but not in black participants [24]. Finally, in a prospective study, an increased risk of coronary heart disease events was reported in white or Chinese participants with low serum 25(OH)D, but not in blacks or Hispanics [25].
Previous analyses using unstandardized data were likely confounded by large variations in serum 25(OH)D results, and ethnic-specific analyses were further constrained by small sample sizes in underrepresented populations, such as U.S. blacks, adding more uncertainty to these estimates. Accurate assessment of the overall and ethnic-specific variations in vitamin D is therefore crucial, and dependent upon the use of standardized data with sufficient statistical power to examine ethnic differences in the relationship between vitamin D status and cardiometabolic risk. Thus, the purpose of this study was to provide a comprehensive assessment of cardiometabolic risk including insulin resistance, metabolic syndrome, and cardiovascular disease risk in relation to serum 25(OH)D levels in U.S. adults, and to estimate the ethnic-specific associations using the newly standardized serum 25(OH)D data from NHANES 2001–2010.
Subjects and methods
Participants
Conducted by the NCHS, NHANES is a series of stratified, multistage probability surveys designed to collect cross-sectional data on the health and nutritional status of the civilian, non-institutionalized U.S. population. NHANES is an ongoing survey and data are reported in 2-year intervals, which are available for public use [26]. NHANES oversamples certain under-represented groups in the population, including Mexican Americans, blacks, older adults and those of lower socioeconomic status. Each survey cycle consists of an in-home interview, physical examinations and laboratory tests. Descriptions of the standardized protocols used for data handling during the interview, laboratory, and physical examinations have been previously published [27].
We initially identified 23,968 adults ≥20 years with available standardized serum 25(OH)D data from 2001–2010. We excluded 10,939 participants who fasted < 8 h, 466 pregnant women, 1355 participants in “other Hispanic” or “other race” category, 73 with serum albumin < 2.9 g/dL, 1081 with estimated glomerular filtration rate (eGFR) < 60 mL/min/1.73 m2, and 2380 participants with missing covariate information. Those in the “other Hispanic” category were excluded due to a change in the 2007–2010 NHANES sampling design, where Hispanics were oversampled instead of only the Mexican-American population [28]. As such, we only included those in the “Mexican-American” category. The final analytical sample included 7674 adults ≥20 years who fasted for ≥ 8 h and self-identified themselves as Mexican-American (MA), non-Hispanic white (NH-white), or non-Hispanic black (NH-black). A flowchart for study sample derivation is shown in Fig. 1. NHANES was approved by the NCHS institutional board and all adults provided written informed consent [29].

Flowchart showing the exclusion criteria for sample derivation, NHANES 2001–2010
Measurement of serum 25(OH)D
For 2007–2010, serum 25(OH)D metabolites were analyzed by the CDC laboratory using the LC-MS/MS method and total serum 25(OH)D (nmol/L) was calculated as the sum of 25(OH)D3 and 25(OH)D2, excluding the C3-epi-25(OH)D3 metabolite. For 2001–2006, serum 25(OH)D levels were initially measured using the Diasorin RIA kit (Stillwater, MN); however, due to concerns about bias and imprecision for the Diasorin RIA assay, the CDC developed regression equations to convert RIA values to LC-MS/MS equivalents for NHANES 1988–1994 and 2001–2006 [30]. In order to combine serum 25(OH)D measurements, we used the predicted LC-MS/MS equivalent total serum 25(OH)D data from 2001–2006 and the total serum 25(OH)D data from 2007–2010.
Outcome variables
Insulin resistance
Insulin resistance was estimated by the homeostatic model assessment-insulin resistance index (HOMA-IR), calculated as the product of the fasting insulin concentration (μU/ml) and the fasting plasma glucose concentration (mmol/L), divided by 22.5 [31]. We defined insulin resistance as HOMA-IR ≥ 75th percentile (sex- and ethnic-specific). Fasting glucose concentrations were measured by a Hexokinase enzymatic method, and serum insulin concentrations were measured by a radioimmunoassay in 2001–2002, a two-site immunoenzymometric method in 2003–2004 and an ELISA two-site enzyme immunoassay method in 2005–2010.
Metabolic syndrome
We used the revised U.S. National Cholesterol Education Program Adult Treatment Panel III (NCEP/ATPIII) report to define MetS [32] as 3 or more of the following 5 criteria: 1) waist circumference (WC) ≥ 102 cm in men or ≥ 88 cm in women; 2) triglycerides ≥ 1.7 mmol/L or medication; 3) high density lipid (HDL) cholesterol < 1.0 mmol/L in men or < 1.3 mmol/L in women or medication; 4) blood pressure (BP) ≥ 130/85 mmHg or treatment for hypertension; 5) fasting blood glucose ≥ 5.6 mmol/L or treatment for diabetes. WC and BP data were collected during physical examinations and descriptions of the standardized protocol are provided in the NHANES Anthropometry Procedures Manual [33]. Up to four BP readings were obtained during the physical examination and the average BP was estimated using the BP protocol provided by NHANES [34]. Triglycerides were measured enzymatically in serum samples from the morning session. HDL-cholesterol was measured using either the Heparin manganese precipitation method or a direct HDL-cholesterol immunoassay method. Prescription medication use was self-reported during the in-home interview. Using the standardized generic prescription drug codes, medication use was classified into four drug categories; HDL-specific medications, lipid medications, anti-hypertensive medications, and anti-hyperglycemic medications.
Framingham CVD Risk
The Framingham CVD risk score was used to estimate the 10-year composite risk for coronary heart disease, stroke, peripheral artery disease, and heart failure [35]. In the first step of the algorithm, point scores for age, sex, total and HDL cholesterol, SBP, treatment of hypertension, smoking, and diabetes status were assigned [35]. CVD risk scores were subsequently computed for each participant based on age- and sex-specific criteria (range for men: −3 to ≥ 18; women: −3 to ≥ 21), which were then translated into a participant’s absolute 10-year risk for a CVD event. The specific details on the point scores for the CVD risk algorithm is provided in Tables five-eight in reference [35]. In our study, an absolute risk of ≥ 15% was defined as “high” and an absolute risk of < 15% as “low” for 10-year predicted risk. These cutoffs were calibrated to approximate the absolute CVD risk associated with insulin resistance (12.6%) and MetS (14.9%) in our study sample.
Total cholesterol was measured enzymatically at Johns Hopkins lipid laboratory (Baltimore, MD). Treatment of hypertension was established from self-reported anti-hypertensive medications. Smoking status (0 = nonsmokers, 1 = current smokers) was self-reported during the in-home interview. Diabetes status was defined as a fasting glucose ≥ 126 mg/dL (7.0 mmol/L) or current use of diabetes medication.
Confounders
Age, sex, ethnicity, smoking status, educational attainment, physical activity (PA), dietary supplement intake and use of medications were self-reported by questionnaire during the in-home interview. Educational attainment was categorized as less than high school, high school graduate, and some college or college graduate or higher. The PA questionnaire included a series of questions related to participant’s daily activities, leisure-time activities, and sedentary activities at home. Participants self-reported the number of days in the past month or in a typical week they engaged in daily and leisure time activities and the average duration for these activities. A metabolic equivalent (MET) of 4.0 for moderate, and 8.0 for vigorous intensity PA were used to estimate the MET minutes/week for each participant. Supplemental intake of vitamin D for 2007–2010 was obtained from 24-h dietary recall, and total daily vitamin D intake was estimated across all supplement sources for 2001–2006. Vitamin D supplementation was categorized as “any” versus “nonusers”. Season corresponds to season of blood draw, which was reported by NHANES as winter months (November–April) and summer months (May–October). Standing height and weight were measured during the physical examination and were used to calculate body mass index (BMI: kg/m2).
Statistical analysis
For descriptive statistics, weighted means for continuous variables and weighted percentages for categorical variables along with 95% confidence intervals (CIs) were used. Differences in descriptive statistics across ethnic groups were assessed by survey-weighted Wald-F-Test and Chi-square tests to examine the independence of means and frequencies, respectively.
Modified Poisson regression models with robust error variances were used to estimate the prevalence ratios (PRs) and 95% CIs for cohort studies [36, 37]. Serum 25(OH)D concentrations were categorized into quartiles (<43.4, 43.4–58.6, 58.7–74.2, ≥74.3 nmol/L). To calculate the PRs for each outcome, the lowest 25(OH)D quartile (<43.4 nmol/L) was considered as the referent group (PR = 1.00). The models were adjusted for confounders such as age, sex, ethnicity, education, season of blood draw (winter, summer), survey cycle (corresponding to survey year), BMI, vitamin D supplement use, smoking, total PA and relevant medication use (lipid-lowering and anti-hyperglycemic medications). The adjustment of these confounders in the models were based on the association of the confounder variables with both the outcome measures and serum 25(OH)D levels. Pairwise interactions with ethnicity and age were explored by including the product terms in the models (i.e. 25(OH)D*ethnicity and 25(OH)D*age). Models for insulin resistance, MetS, and CVD risk were subsequently stratified by ethnicity, and the CVD risk model was further stratified by age groups (i.e. 20–59 and ≥ 60 years). To explore the possibility of differential bias by comorbid conditions, a series of sensitivity analyses were conducted after the exclusion of participants with physician diagnosed diabetes and CVD (congestive heart failure, coronary hearts disease, angina, heart attack, and stroke), and relevant medication use (i.e. lipid, blood pressure, and anti-hyperglycemic medications).
To ensure the representativeness of the data, clinical fasting weights were applied to account for survey cluster design, oversampling, and nonresponse. Statistical analysis was performed using SAS 9.4 (Cary, NC) survey procedures, which appropriately accounted for cluster sampling and the complex sample design of NHANES. All statistical tests were two-tailed at the alpha = 0.05 level of significance.
Results
Participant characteristics
Baseline characteristics of the participants are shown in Table 1. Overall, the mean age of the sample was 45.3 (44.7, 45.9), and the majority of the sample was NH-white (55.9% NH-white, 23.4% MA, and 20.7% NH-black). Of the 7674 participants, 22.5% (21.0, 24.1) were taking vitamin D supplements, with supplement use significantly higher in NH-whites [24.8% (22.8, 26.7)] compared to MAs [13.0% (11.0, 15.0)] and NH-blacks [14.7% (12.1, 17.3)]. The prevalence of MetS in the total sample was 36.1% (34.6, 37.6), and NH-whites had the highest prevalence of MetS [36.9% (35.0, 38.8)] compared to MAs [34.8% (31.5, 38.1)] and NH-blacks [31.6% (29.0, 34.0)]. The absolute CVD risk in the total sample was 7.92% (7.63, 8.20), and NH-Whites had significantly higher absolute CVD risk [8.26% (7.93, 8.59)] compared to MAs [5.85% (5.40, 6.31)] and NH-blacks [7.19% (6.77, 7.61)].
Serum 25(OH)D and HOMA-IR
The adjusted PRs for cardiometabolic risk by 25(OH)D quartiles in the total sample are shown in Table 2. After adjusting for age, sex, BMI, PA, ethnicity, season, survey cycle, education, smoking, and use of vitamin D supplement, lipid-lowering and anti-hyperglycemic medications, the highest 25(OH)D quartile (≥74.3 nmol/L) had a 30% relative risk reduction in HOMA-IR [0.70 (0.59, 0.84)] compared to those in the lowest quartile (<43.4 nmol/L). The associations remained significant across all ethnic groups (Table 3). The highest relative risk reduction was observed in MAs [0.54 (0.35, 0.82)], followed by NH-blacks [0.67 (0.45, 0.99), and NH-whites [0.81 (0.68, 0.96)] with serum 25(OH)D ≥74.3 nmol/L compared to the lowest 25(OH)D quartile (<43.4 nmol/L).
Serum 25(OH)D and MetS
Overall, serum 25(OH)D levels ≥74.3 nmol/L were associated with a 18% risk reduction in MetS [0.82 (0.74, 0.91)] compared to the lowest 25(OH)D quartile (Table 2). The association of serum 25(OH)D with MetS remained significant across all ethnic-groups (Table 3). For MAs, the second 25(OH)D quartile (Q2: 43.4–58.6 nmol/L) had a 20% relative risk reduction in MetS [0.80 (0.66, 0.97) and the highest quartile a 27% risk reduction in MetS [0.73 (0.55, 0.96)] compared to the lowest quartile. Significant associations were observed only in the highest 25(OH)D quartile in NH-whites [0.84 (0.73, 0.95)] and NH-blacks [0.74 (0.56, 0.97)] compared to the lowest quartile.
Serum 25(OH)D and CVD risk
In the overall sample, the relative reduction in CVD risk was 14% in the second 25(OH)D quartile [0.86 (0.76, 0.98)], and 22% in the highest versus lowest 25(OH)D quartile [0.78 (0.66, 0.91)] (Table 2). In ethnic-specific analyses, significant associations were observed amongst the highest versus lowest quartiles for NH-whites [0.78 (0.64, 0.93)] and NH-blacks [0.58 (0.41, 0.81)], but not in MAs [0.90 (0.69, 1.16)] (Table 3).
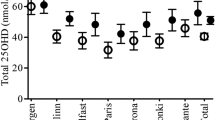
There was a significant interaction between serum 25(OH)D and age in the CVD risk model. This is consistent with the Framingham CVD risk because age is the most heavily weighted variable in the algorithm, as shown in Fig. 2. Therefore, we further stratified the association of serum 25(OH)D with CVD risk by age groups (20–59 and ≥ 60 years). Table 4 shows the adjusted PRs of CVD risk associated with 25(OH)D quartiles by age category. Overall, stratification by age resulted in similar results compared to the main model, except that the PRs for CVD risk in participants for 20–59 years old were lower compared to participants ≥ 60 years old. Age stratification did not affect the observed non-significant association of 25(OH) with CVD risk in MAs. For NH-blacks, significant associations were attained in participants ≥ 60 years for the highest quartile [0.63 (0.45, 0.870], but no significant association was found in participants 20–59 years old.

Prevalence of cardiovascular disease risk (≥15%) by age status in participants ≥ 20 years, NHANES 2001–2010. *P < 0.05
Sensitivity analyses
After excluding participants with comorbid conditions, the estimates of PRs for the adjusted associations of 25(OH)D with HOMA-IR, MetS and CVD risk remained statistically significant (Table 2). Similarly in the ethnic-specific analyses, the adjusted associations of 25(OH)D with HOMA-IR, MetS and CVD risk were numerically similar in MAs and NH-Whites after excluding participants with comorbid conditions, although the associations were attenuated for NH-Blacks due to significant reductions in the number of events, particularly in the highest serum 25(OH)D quartile (Table 3). Overall, the sensitivity analyses revealed the stability of the PRs estimates in the original models.
Discussion
In this study, we have shown that standardized serum 25(OH)D concentrations were inversely associated with insulin resistance, MetS and CVD risk in a nationally representative sample of U.S. adults. These associations remained significant across all ethnic subgroups, except for CVD risk in MAs. Overall, the results of our study suggest that serum 25(OH)D concentrations ≥ 75 nmol/L may be the optimal threshold in relation to cardiometabolic risk. To our knowledge, this study provides the most recently updated and comprehensive estimate of the association between standardized serum 25(OH)D levels and cardiometabolic risk, and unlike previous studies, our findings demonstrate that low 25(OH)D is a significant risk factor for cardiometabolic risk in U.S. blacks.
The inverse associations between vitamin D status and insulin resistance, MetS and CVD risk are aligned with previous epidemiologic studies. Of note, previous analyses of NHANES have found an inverse association between unstandardized serum 25(OH)D levels with insulin resistance and pre-diabetes [11, 38], MetS [4], and CVD mortality [39]. Similarly, prospective studies have shown an inverse association between serum 25(OH)D and insulin resistance [40] and incident CVD in the Framingham Offspring Study [5], and incidence of MetS in a cohort of non-diabetic adults [8].
Previous studies have shown ethnic differences in the association of serum 25(OH)D with cardiometabolic risk factors. Ethnic differences between serum 25(OH)D and risk of diabetes were found in NHANES III [22], and confirmed in NHANES 2001–2006 with significant inverse associations in MAs and NH-whites, but not in NH-Blacks [23]. In a prospective study, Robinson-Cohen et al. [25] reported a significant increase in the risk of coronary heart disease events with low 25(OH)D levels in whites and Chinese, but not in black or Hispanic participants from the Multi-Ethnic Study of Atherosclerosis. Lutsey et al. [41] also observed that low 25(OH)D levels were a stronger risk factor for the development of heart failure in whites than black participants from the Atherosclerosis Risk in Communities study. Conversely, our results showed a significant inverse association of standardized 25(OH)D with cardiometabolic risk in MAs, NH-Whites, and NH-blacks.
Our results are in contrast to the vitamin D paradox observed in blacks, where prior studies have suggested that even though blacks have circulating 25(OH)D in the deficient range (<50 nmol/L), a compensatory mechanism exists in relation to bone health [42, 43]. At this time, it is not fully understood whether other compensatory mechanisms exist in relation to cardiovascular health outcomes, but it has been speculated that vitamin D binding protein (DBP) levels in blacks are significantly lower compared to whites to compensate for lower total serum 25(OH)D in blacks. It has also been suggested that total 25(OH)D may not be the best biomarker of vitamin D status in blacks [44]. However, the monoclonal immunoassay used by Powe et al. [44] has been criticized for its lack of sensitivity to DBP polymorphisms, which provides erroneous results for vitamin D metabolites [45]. Using a novel LC-MS/MS method, Henderson et al. [46] recently showed that levels of DBP do not vary between whites and blacks. Therefore, it is possible that the use of immunoassays in a population with a low range of vitamin D metabolites results in inaccurate total 25(OH)D concentrations in blacks and that the results from existing immunoassays might be insufficient to allow identification of a significant association within these populations.
Previous attempts to assess the ethnic-specific association between cardiometabolic disorders and 25(OH)D have been limited due to reliance on samples with a low number of blacks within the upper range of 25(OH)D concentrations (i.e. ≥ 75 nmol/L). In comparison with prior work, our results suggest significant risk reductions in NH-blacks, which we speculate is due to reduced variation from the standardization of 25(OH)D measurements across all NHANES survey cycles [30]. Moreover, the lowest levels of 25(OH)D were observed in NH-blacks in our study, supporting the hypothesis that black Americans have reduced cutaneous synthesis of vitamin D due to increased skin pigmentation and decreased sun exposure [47]. In support of this hypothesis, Alzaman et al. [48] did not observe any systemic difference in the absorption or bioavailability of oral vitamin D metabolites between US blacks and whites, neither do their results support the paradoxical clinical correlates of vitamin D in US blacks [48]. Taken together, our results add to the current evidence by demonstrating that total circulating 25(OH)D is a significant biomarker of cardiometabolic risk in U.S. blacks.
Although mechanisms relating vitamin D deficiency and cardiometabolic risk factors are not fully elucidated, several important mechanisms warrant discussion. Insulin resistance is the core trait of the metabolic disturbances observed in MetS, type-2 diabetes and CVD risk [49]. The presence of vitamin D receptors (VDRs) in pancreatic β-cells suggest that the active metabolite 1-α-25-dihydroxyvitamin D3 (1,25(OH)2D3) could directly influence insulin secretion [50]. Since insulin secretion is a calcium dependent process, it is possible that 1,25(OH)2D3 modulates insulin secretion by increasing intracellular calcium levels [50]. Moreover, vitamin D deficiency promotes secondary hyperparathyroidism, stimulates the RAAS, which in turn increases the secretion of aldosterone [51]. Both low serum 25(OH)D and high PTH levels are related to arterial stiffness and vascular dysfunction, which are significant elements of hypertension and CVD risk [52]. It is possible that lower 25(OH)D and higher serum PTH levels could synergistically or independently play a role in the pathogenesis of developing hypertension and future CVD [53]. Due to the lack of data in our study, we were not able to elucidate the role of PTH in our analyses, however, the exclusion of participants with eGFR < 60 mL/min/1.73 m2 reduces the potential confounding of secondary hyperparathyroidism caused by chronic renal failure and the impaired vitamin D metabolism by the diseased kidneys. Future studies using standardized serum 25(OH)D data are needed to re-evaluate the optimal 25(OH)D thresholds that maximally suppress PTH levels [54]. The complexity of vitamin D and PTH metabolism makes it challenging to fully disentangle the individual contributions of these factors and warrants further investigation.
In addition, the relationship between vitamin D deficiency and metabolic traits of these diseases is confounded by adiposity where individuals with obesity have lower serum 25(OH)D levels compared to normal-weight individuals and this is consistent across different age and ethnic groups [55–58]. Hence, serum 25(OH)D concentrations are related to fat mass and changes in serum PTH, and adipokines, such as leptin and adiponectin, may be crucial in elucidating the relationship between vitamin D, PTH and metabolic disturbances [59, 60]. It is possible that normal vitamin D metabolism may be disrupted in obesity due to elevated levels of serum leptin, which has been shown to suppress the conversion of 25(OH)D to 1,25(OH)2D3 [61]. Although we were not able to further adjust for leptin levels, we adjusted for BMI, which is a proxy for fat mass and leptin levels [62]. Moreover, given that obesity and metabolic diseases are associated with low-grade inflammation, the anti-inflammatory and immunomodulatory properties of vitamin D have been suggested and supported by previous studies showing an inverse, but inconsistent, relationship between vitamin D and inflammatory markers such as C-reactive protein (CRP) [63–65]. A recent Mendelian randomization study found no causal relationship between vitamin D and CRP [66], which suggests that it is unlikely that vitamin D deficiency directly contributes to increased inflammation or vice versa. In our study, we found no evidence of the potential confounding effect of CRP levels on the relationship between serum 25(OH)D and all outcome measures (data not shown). Taken together, experimental and observational studies suggest that the relationship between vitamin D and cardiometabolic disorders are multimodal and mediated through direct and indirect pathways. Further, it is important that the results of this study are interpreted according to variation in vitamin D metabolism genes, which could explain the heterogeneity of responses to vitamin D deficiency across ethnic groups [67].
Although the evidence from previous observational studies and our results suggest that serum 25(OH)D levels ≥ 75 nmol/L are associated with lower risk of cardiometabolic disorders compared to 25(OH)D ≤ 50 nmol/L, these findings have not been consistent in clinical trials [68–71]. Among the possible explanations for these differences include the substantial heterogeneity in the definition of vitamin D deficiency, different age structure and target population (i.e., vitamin D deficient versus sufficient individuals), primary versus secondary prevention of CVD, differences in the available assays used to measure vitamin D metabolites, as well as the inclusion of different confounders in their analyses. Although the relationship between optimal vitamin D status and cardiovascular health remains to be elucidated, the standardization of serum 25(OH)D data and the large sample size of our study allowed a comprehensive estimate of the association between 25(OH)D and cardiometabolic risk in US adults using a nationally representative survey sample. Given that many risk factors for CVD are clustered in insulin resistance and MetS, it is reasonable to speculate that low 25(OH)D is a significant risk factor in their development, which may ultimately contribute to increased CVD risk. Future studies must be sufficiently powered to estimate the overall benefit, as well as study the risks and benefits associated with varying circulating 25(OH)D concentrations in ethnic subpopulations.
There are several limitations to this study. Due to the cross-sectional design, we are unable to rule out the possibility of reverse causation. Although we have adjusted for potential confounders, we cannot rule out residual confounding or the effect of unmeasured confounders. Further, seasonality of serum 25(OH)D levels in NHANES must be considered a confounder because of the sampling design wherein data is collected from northern states in the summer and southern states in the winter. This sampling design results in higher average 25(OH)D and an increased range of 25(OH)D concentrations in northern states. Despite these limitations, our study provides national estimates of the association between serum 25(OH)D and cardiometabolic risk in the U.S. population and in ethnic subgroups using standardized serum 25(OH)D data from 2001–2010.
Conclusions
In this large national sample, standardized serum 25(OH)D concentrations were significantly associated with cardiometabolic risk including insulin resistance, MetS and CVD risk in U.S. adults, and low 25(OH)D is a significant risk factor for cardiometabolic risk in MAs, NH-whites, and NH-blacks. Standardization of serum 25(OH)D allows accurate assessment of vitamin D status, and future studies are needed to re-evaluate these risks in black Americans with serum 25(OH)D concentrations above 75 nmol/L.
Abbreviations
- 1,25(OH)2D3 :
-
1-α-25-dihydroxyvitamin D3
- 25(OH)D:
-
Serum 25-hydroxyvitamin D
- CDC:
-
Center for Disease Control and Prevention
- CI:
-
Confidence interval
- CRP:
-
C-reactive protein
- CVD:
-
Cardiovascular disease
- eGFR:
-
Estimated glomerular filtration rate
- HOMA-IR:
-
Homeostatic Model Assessment of Insulin Resistance
- LC-MS/MS:
-
Liquid Chromatography-tandem Mass Spectrometry
- MA:
-
Mexican-American
- MetS:
-
Metabolic Syndrome
- NCHS:
-
National Center for Health Statistics
- NHANES:
-
National Health and Nutrition Examination Survey
- NH-black:
-
Non-hispanic black
- NH-white:
-
Non-hispanic white
- PR:
-
Prevalence ratio
- PTH:
-
Parathyroid hormone
- RAAS:
-
Renin-angiotensin aldosterone system
- RIA:
-
Radioimmunoassay
- VDSP:
-
Vitamin D Standardization Program
References
Wang L, Song Y, Manson JE, Pilz S, Marz W, Michaelsson K, et al. Circulating 25-hydroxy-vitamin D and risk of cardiovascular disease: a meta-analysis of prospective studies. Circ Cardiovasc Qual Outcomes. 2012;5(6):819–29.
Elamin MB, Abu Elnour NO, Elamin KB, Fatourechi MM, Alkatib AA, Almandoz JP, et al. Vitamin D and cardiovascular outcomes: a systematic review and meta-analysis. J Clin Endocrinol Metab. 2011;96(7):1931–42.
Forouhi NG, Ye Z, Rickard AP, Khaw KT, Luben R, Langenberg C, et al. Circulating 25-hydroxyvitamin D concentration and the risk of type 2 diabetes: results from the European prospective investigation into cancer (EPIC)-Norfolk cohort and updated meta-analysis of prospective studies. Diabetologia. 2012;55(8):2173–82.
Ford E, Ajani U, McGuire L, Liu S. Concentrations of serum vitamin D and the metabolic syndrome among US adults. Diabetes Care. 2005;28(5):1228–30.
Wang TJ, Pencina MJ, Booth SL, Jacques PF, Ingelsson E, Lanier K, et al. Vitamin D deficiency and risk of cardiovascular disease. Circulation. 2008;117(4):503–11.
Skaaby T, Husemoen LLN, Pisinger C, Jorgensen T, Thuesen BH, Fenger M, et al. Vitamin D status and changes in cardiovascular risk factors: a prospective study of a general population. Cardiology. 2012;123(1):62–70.
García-Bailo B, Da Costa LA, Arora P, Karmali M, El-Sohemy A, Badawi A. Plasma vitamin D and biomarkers of cardiometabolic disease risk in adult Canadians, 2007–2009. Prev Chronic Dis. 2013;10:E91.
Kayaniyil S, Harris SB, Retnakaran R, Vieth R, Knight JA, Gerstein HC, et al. Prospective association of 25(OH)D with metabolic syndrome. Clin Endocrinol (Oxf). 2014;80(4):502–7.
Chiu KC, Chu A, Go VLW, Saad MF. Hypovitaminosis D is associated with insulin resistance and beta cell dysfunction. Am J Clin Nutr. 2004;79(5):820–5.
Kayaniyil S, Vieth R, Retnakaran R, Knight JA, Qi Y, Gerstein HC, et al. Association of vitamin D with insulin resistance and beta-cell dysfunction in subjects at risk for type 2 diabetes. Diabetes Care. 2010;33(6):1379–81.
Zhao G, Ford ES, Li C. Associations of serum concentrations of 25-hydroxyvitamin D and parathyroid hormone with surrogate markers of insulin resistance among U.S. adults without physician-diagnosed diabetes: NHANES, 2003–2006. Diabetes Care. 2010;33(2):344–7.
Kayaniyil S, Retnakaran R, Harris SB, Veith R, Knight JA, Gerstein HC, et al. Prospective associations of vitamin D with β-cell function and glycemia: the PROspective metabolism and ISlet cell evaluation (PROMISE) cohort study. Diabetes. 2011;60(11):2947–53.
Kabadi SM, Lee BK, Liu L. Joint effects of obesity and vitamin D insufficiency on insulin resistance and type 2 diabetes: results from the NHANES 2001–2006. Diabetes Care. 2012;35(10):2048–54.
Reis JP, von Mühlen D, Kritz-Silverstein D, Wingard DL, Barrett-Connor E. Vitamin D, parathyroid hormone levels, and the prevalence of metabolic syndrome in community-dwelling older adults. Diabetes Care. 2007;30(6):1549–55.
Rueda S, Fernández-Fernández C, Romero F, Martínez De Osaba MJ, Vidal J. Vitamin D, PTH, and the metabolic syndrome in severely obese subjects. Obes Surg. 2008;18(2):151–4.
Hjelmesaeth J, Hofsø D, Aasheim ET, Jenssen T, Moan J, Hager H, et al. Parathyroid hormone, but not vitamin D, is associated with the metabolic syndrome in morbidly obese women and men: a cross-sectional study. Cardiovasc Diabetol. 2009;8:7.
Muscogiuri G, Sorice GP, Prioletta A, Policola C, Della Casa S, Pontecorvi A, et al. 25-hydroxyvitamin D concentration correlates with insulin-sensitivity and BMI in obesity. Obesity. 2010;18(10):1906–10.
Roth HJ, Schmidt-Gayk H, Weber H, Niederau C. Accuracy and clinical implications of seven 25-hydroxyvitamin D methods compared with liquid chromatography-tandem mass spectrometry as a reference. Ann Clin Biochem. 2008;45(Pt 2):153–9.
Sempos CT, Vesper HW, Phinney KW, Thienpont LM, Coates PM, Vitamin D. Vitamin D standardization program (VDSP). Vitamin D status as an international issue: national surveys and the problem of standardization. Scand J Clin Lab Invest Suppl. 2012;243:32–40.
CDC/National Center for Health Statistics. Analytical Note for 25-Hydroxyvitamin D Data Analysis using NHANES III (1988–1994), NHANES 2001–2006, and NHANES 2007–2010 (October 2015). http://wwwn.cdc.gov/nchs/nhanes/VitaminD/AnalyticalNote.aspx. Accessed 1 Sept 2016.
Schleicher RL, Sternberg MR, Lacher DA, Sempos CT, Looker AC, Durazo-Arvizu RA, et al. The vitamin D status of the US population from 1988 to 2010 using standardized serum concentrations of 25-hydroxyvitamin D shows recent modest increases. Am J Clin Nutr. 2016;104(2):454–61.
Scragg R, Sowers M, Bell C. Serum 25-Hydroxyvitamin D, Diabetes, and Ethnicity in the Third National Health and Nutrition Examination Survey. Diabetes Care. 2004;27(12):2813–8.
Christensen MHE, Scragg RK. Consistent ethnic specific differences in diabetes risk and vitamin D status in the National Health and Nutrition Examination Surveys. J Steroid Biochem Mol Biol. 2016;164:4-10.
Michos ED, Reis JP, Post WS, Lutsey PL, Gottesman RF, Mosley TH, et al. 25-hydroxyvitamin D deficiency is associated with fatal stroke among whites but not blacks: the NHANES-III linked mortality files. Nutrition. 2012;28(4):367–71.
Robinson-Cohen C, Hoofnagle AN, Ix JH, Sachs MC, Tracy RP, Siscovick DC, et al. Racial differences in the association of serum 25-hydroxyvitamin D concentration with coronary heart disease events. JAMA. 2013;310(2):179.
NHANES - National Health and Nutrition Examination Survey Homepage. http://www.cdc.gov/nchs/nhanes/index.htm. Accessed 16 Aug 2016.
National Health and Nutrition Examination Survey: Plan and Operations, 1999–2010. http://www.cdc.gov/nchs/data/series/sr_01/sr01_056.pdf. Accessed 16 Aug 2016.
National Health and Nutrition Examination Survey: Sample Design, 2007–2010. http://www.cdc.gov/nchs/data/series/sr_02/sr02_160.pdf. Accessed 16 Aug 2016.
NHANES - NCHS Research Ethics Review Board Approval. http://www.cdc.gov/nchs/nhanes/irba98.htm. Accessed 16 Aug 2016.
Schleicher RL, Sternberg MR, Lacher DA, Sempos CT, Looker AC, Durazo-Arvizu RA, et al. A method-bridging study for serum 25-hydroxyvitamin D to standardize historical radioimmunoassay data to liquid chromatography-tandem mass spectrometry. Natl Health Stat Rep. 2016;93:1–16.
Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC. Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia. 1985;28(7):412–9.
Grundy SM. Diagnosis and management of the metabolic syndrome: an American heart association/national heart, lung, and blood institute scientific statement. Circulation. 2005;112(17):2735–52.
CDC. National Health and Nutrition Examination Survey: Anthropometry Procedures Manual, 2009. http://www.cdc.gov/nchs/data/nhanes/nhanes_09_10/BodyMeasures_09.pdf. Accessed 16 Aug 2016.
CDC. National Health and Nutrition Examination Survey: Physician Examination Procedures Manual, 2000. http://www.cdc.gov/nchs/data/nhanes/pe.pdf. Accessed 16 May 2016.
D’Agostino RB, Vasan RS, Pencina MJ, Wolf PA, Cobain M, Massaro JM, et al. General cardiovascular risk profile for use in primary care: the Framingham heart study. Circulation. 2008;117(6):743–53.
Zou G. A modified poisson regression approach to prospective studies with binary data. Am J Epidemiol. 2004;159(7):702–6.
Zhao K. Proper estimation of relative risk using PROC GENMOD in population studies. Proceedings of the Western Users of SAS Software Conference; Western Users of SAS Software Conference; November 13–15, 2013; Las Vegas, NV. 2013. pp. 1–14. http://wuss.org/Proceedings13/81_Paper.pdf. Accessed 1 Sept 2016.
Shankar A, Sabanayagam C, Kalidindi S. Serum 25-hydroxyvitamin d levels and prediabetes among subjects free of diabetes. Diabetes Care. 2011;34(5):1114–9.
Zhao G, Ford ES, Li C, Croft JB. Serum 25-hydroxyvitamin D levels and all-cause and cardiovascular disease mortality among US adults with hypertension. J Hypertens. 2012;30(2):284–9.
Liu E, Meigs JB, Pittas AG, Mckeown NM, Economos CD, Booth SL, et al. Plasma 25-hydroxyvitamin d is associated with markers of the insulin resistant phenotype in nondiabetic adults. J Nutr. 2009;139(2):329–34.
Lutsey PL, Michos ED, Misialek JR, Pankow JS, Loehr L, Selvin E, et al. Race and vitamin D binding protein gene polymorphisms modify the association of 25-hydroxyvitamin D and incident heart failure. JACC Hear Fail. 2015;3(5):347–56.
Aloia J, Mikhail M, Dhaliwal R, Shieh A, Usera G, Stolberg A, et al. Free 25(OH)D and the vitamin D paradox in African Americans. J Clin Endocrinol Metab. 2015;100(9):3356–63.
Wright NC, Chen L, Niu J, Neogi T, Javiad K, Nevitt MA, et al. Defining physiologically “Normal” vitamin D in African Americans. Osteoporos Int. 2012;23(9):2283–91.
Powe CE, Evans MK, Wenger J, Zonderman AB, Berg AH, Nalls M, et al. Vitamin D-binding protein and vitamin D status of black Americans and white Americans. N Engl J Med. 2013;369(21):1991–2000.
Hoofnagle AN, Eckfeldt JH, Lutsey PL. Vitamin D-binding protein concentrations quantified by mass spectrometry. N Engl J Med. 2015;373(15):1480–2.
Henderson CM, Lutsey PL, Misialek JR, Laha TJ, Selvin E, Eckfeldt JH, et al. Measurement by a novel LC-MS/MS methodology reveals similar serum concentrations of vitamin D-binding protein in blacks and whites. Clin Chem. 2016;62(1):179–87.
Clemens TL, Adams JS, Henderson SL, Holick MF. Increased skin pigment reduces the capacity of skin to synthesise vitamin D3. Lancet (London, England). 1982;1(8263):74–6.
Alzaman NS, Dawson-Hughes B, Nelson J, D’Alessio D, Pittas AG. Vitamin D status of black and white Americans and changes in vitamin D metabolites after varied doses of vitamin D supplementation. Am J Clin Nutr. 2016;104(1):205–14.
Van Gaal LF, Mertens IL, De Block CE. Mechanisms linking obesity with cardiovascular disease. Nature. 2006;444(7121):875–80.
Bouillon R, Carmeliet G, Verlinden L, van Etten E, Verstuyf A, Luderer HF, et al. Vitamin D and human health: lessons from vitamin D receptor null mice. Endocr Rev. 2008;29(6):726–76.
Tomaschitz A, Ritz E, Pieske B, Fahrleitner-Pammer A, Kienreich K, Horina JH, et al. Aldosterone and parathyroid hormone: a precarious couple for cardiovascular disease. Cardiovasc Res. 2012;94(1):10–9.
Al Mheid I, Patel R, Murrow J, Morris A, Rahman A, Fike L, et al. Vitamin D status is associated with arterial stiffness and vascular dysfunction in healthy humans. J Am Coll Cardiol. 2011;58(2):186–92.
Kestenbaum B, Katz R, de Boer I, Hoofnagle A, Sarnak MJ, Shlipak MG, et al. Vitamin D, parathyroid hormone, and cardiovascular events among older adults. J Am Coll Cardiol. 2011;58(14):1433–41.
Binkley N, Dawson-Hughes B, Durazo-Arvizu R, Thamm M, Tian L, Merkel JM, et al. Vitamin D measurement standardization: The way out of the chaos. J Steroid Biochem Mol Biol. December 2016.
Arunabh S, Pollack S, Yeh J, Aloia JF. Body fat content and 25-hydroxyvitamin D levels in healthy women. J Clin Endocrinol Metab. 2003;88(1):157–61.
Parikh SJ, Edelman M, Uwaifo GI, Freedman RJ, Semega-Janneh M, Reynolds J, et al. The relationship between obesity and serum 1,25-dihydroxy vitamin D concentrations in healthy adults. J Clin Endocrinol Metab. 2004;89(3):1196–9.
Snijder MB, van Dam RM, Visser M, Deeg DJ, Dekker JM, Bouter LM, et al. Adiposity in relation to vitamin D status and parathyroid hormone levels: a population-based study in older men and women. J Clin Endocrinol Metab. 2005;90(7):4119–23.
Rajakumar K, de las Heras J, Chen TC, Lee S, Holick MF, Arslanian SA. Vitamin D status, adiposity, and lipids in black American and Caucasian children. J Clin Endocrinol Metab. 2011;96(5):1560–7.
Maetani M, Maskarinec G, Franke AA, Cooney RV. Association of leptin, 25-hydroxyvitamin D, and parathyroid hormone in women. Nutr Cancer. 2009;61(2):225–31.
Grethen E, Hill KM, Jones R, Cacucci BM, Gupta CE, Acton A, et al. Serum leptin, parathyroid hormone, 1,25-dihydroxyvitamin D, fibroblast growth factor 23, bone alkaline phosphatase, and sclerostin relationships in obesity. J Clin Endocrinol Metab. 2012;97(5):1655–62.
Tsuji K, Maeda T, Kawane T, Matsunuma A, Horiuchi N. Leptin stimulates fibroblast growth factor 23 expression in bone and suppresses renal 1alpha,25-dihydroxyvitamin D3 synthesis in leptin-deficient mice. J Bone Miner Res. 2010;25(8):1711–23.
Ruhl CE, Harris TB, Ding J, Goodpaster BH, Kanaya AM, Kritchevsky SB, et al. Body mass index and serum leptin concentration independently estimate percentage body fat in older adults. Am J Clin Nutr. 2007;85(4):1121–6.
Shea MK, Booth SL, Massaro JM, Jacques PF, D'Agostino Sr RB, Dawson-Hughes B, et al. Vitamin K and vitamin D status: associations with inflammatory markers in the Framingham offspring study. Am J Epidemiol. 2008;167(3):313–20.
Michos ED, Streeten EA, Ryan KA, Rampersaud E, Peyser PA, Bielak LF, et al. Serum 25-hydroxyvitamin D levels are not associated with subclinical vascular disease or C-reactive protein in the old order Amish. Calcif Tissue Int. 2009;84(3):195–202.
Amer M, Qayyum R. Relation between serum 25-hydroxyvitamin D and C-reactive protein in asymptomatic adults (from the continuous National Health and Nutrition Examination Survey 2001 to 2006). Am J Cardiol. 2012;109(2):226–30.
Liefaard MC, Ligthart S, Vitezova A, Hofman A, Uitterlinden AG, Kiefte-De Jong JC, et al. Vitamin D and C-reactive protein: a mendelian randomization study. Stover CM, ed. Plos One. 2015;10(7):e0131740.
Levin GP, Robinson-Cohen C, de Boer IH, Houston DK, Lohman K, Liu Y, et al. Genetic variants and associations of 25-hydroxyvitamin D concentrations with major clinical outcomes. JAMA. 2012;308(18):1898–905.
Avenell A, Cook JA, Maclennan GS, Mcpherson GC. Vitamin D supplementation and type 2 diabetes: a substudy of a randomised placebo-controlled trial in older people (RECORD trial, ISRCTN 51647438). Age Ageing. 2009;38(5):606–9.
Trivedi DP, Doll R, Khaw KT. Effect of 4 monthly oral vitamin D3 (cholecalciferol) supplementation on fractures and mortality in men and women living in the community: randomised double blind controlled trial. BMJ. 2003;326(7387):469.
Mitchell DM, Leder BZ, Cagliero E, Mendoza N, Henao MP, Hayden DL, et al. Insulin secretion and sensitivity in healthy adults with low vitamin D are not affected by high-dose ergocalciferol administration: a randomized controlled trial. Am J Clin Nutr. 2015;102:385–92.
Lacroix AZ, Kotchen J, Anderson G, Brzyski R, Cauley JA, Cummings SR, et al. Calcium plus vitamin D supplementation and mortality in postmenopausal women: the women’s health initiative calcium-vitamin D randomized controlled trial. J Gerontol A Biol Sci Med Sci. 2009;64A(5):559–67.
Acknowledgements
Not applicable.
Funding
This study was not funded.
Availability of data and materials
The datasets used in this study are made publicly available by CDC [http://www.cdc.gov/nchs/nhanes/index.htm] and the data supporting the conclusions of this article are included within the article (Tables and figure).
Authors’ contributions
The authors’ responsibilities were as follows: data acquisition (BA), conception (BA, SMK, CIA), statistical analysis (BA, MAR), drafting of manuscript (BA), critical review, editing, and interpretation of results (BA, SMK, MAR, and CIA). All authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
NHANES was approved by the NCHS institutional board and all adults provided written informed consent [29].
Author information
Authors and Affiliations
Corresponding author
Additional information
The original version of this article was revised. Table 3B in both the PDF and online versions were misaligned.
An erratum to this article is available at http://dx.doi.org/10.1186/s12937-017-0251-8.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Al-khalidi, B., Kimball, S.M., Rotondi, M.A. et al. Standardized serum 25-hydroxyvitamin D concentrations are inversely associated with cardiometabolic disease in U.S. adults: a cross-sectional analysis of NHANES, 2001–2010. Nutr J 16, 16 (2017). https://doi.org/10.1186/s12937-017-0237-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12937-017-0237-6