
Abstract
Background
Recent estimates show progress toward malaria elimination is slowing in many settings, underscoring the need for tailored approaches to fight the disease. In addition to essential structural changes, human behaviour plays an important role in elimination. Engagement in malaria behaviours depends in part on psychosocial determinants such as knowledge, perceived risk, and community norms. Understanding the state of research on psychosocial determinants in low malaria transmission settings is important to augment social and behaviour change practice. This review synthesizes research on psychosocial factors and malaria behaviours in low-transmission settings.
Methods
A systematic search of peer-reviewed literature and supplemental manual search of grey literature was conducted using key terms and eligibility criteria defined a priori. Publications from 2000–2020 in the English language were identified, screened, and analysed using inductive methods to determine the relationship between the measured psychosocial factors and malaria behaviours.
Results
Screening of 961 publications yielded 96 for inclusion. Nineteen articles collected data among subpopulations that are at increased risk of malaria exposure in low-transmission settings. Purposive and cluster randomized sampling were common sampling approaches. Quantitative, qualitative, and mixed-methods study designs were used. Knowledge, attitudes, and perceived risk were commonly measured psychosocial factors. Perceived response-efficacy, perceived self-efficacy, and community norms were rarely measured. Results indicate positive associations between malaria knowledge and attitudes, and preventive and care-seeking behaviour. Studies generally report high rates of correct knowledge, although it is comparatively lower among studies of high-risk groups. There does not appear to be sufficient extant evidence to determine the relationship between other psychosocial variables and behaviour.
Conclusions
The review highlights the need to deploy more consistent, comprehensive measures of psychosocial factors and the importance of reaching subpopulations at higher risk of transmission in low transmission contexts. Malaria-related knowledge is generally high, even in settings of low transmission. Programmes and research should work to better understand the psychosocial factors that have been positively associated with prevention and care-seeking behaviours, such as norms, perceived response efficacy, perceived self-efficacy, and interpersonal communication. These factors are not necessarily distinct from that which research has shown are important in settings of high malaria transmission. However, the importance of each factor and application to malaria behaviour change programming in low-transmission settings is an area in need of further research. Existing instruments and approaches are available to support more systematic collection of psychosocial determinants and improved sampling approaches and should be applied more widely. Finally, while human behaviour is critical, health systems strengthening, and structural interventions are essential to achieve malaria elimination goals.
Similar content being viewed by others


Background
Despite significant gains over the past two decades, malaria continues to take the lives of almost 1700 people each day [1]. The most recent World Health Organization (WHO) estimates show progress has stalled in recent years, underscoring the importance of addressing gaps in access to and use of core malaria interventions, and the need for innovative and more tailored approaches to fighting the disease [1].
Human behaviour plays a fundamental role in the prevention, diagnosis, and treatment of malaria. The effectiveness and longevity of insecticide-treated nets (ITNs) have been shown to depend on levels of use and appropriate care of available nets [2]. Likewise, indoor residual spraying (IRS) effectiveness depends on factors such as acceptance of sprayers in the home, willingness to remove household items during spraying, and refraining from post-spray wall modification [3]. Efficacious treatment relies on prompt care-seeking [4] and taking the full course of medication as prescribed to be effective [5].
Whether someone engages in these behaviours may depend on factors such as their level of knowledge about malaria, attitudes towards the recommended solutions, the extent to which malaria is viewed as a threat, perceptions about how well an intervention works (i.e., perceived response-efficacy), their perceived self-efficacy to use it, and social norms around prevention and care-seeking behaviours. Understanding which specific combination of factors influence malaria behaviours in a given context is essential to promoting effective social and behaviour change (SBC) strategies to increase the impact of interventions.
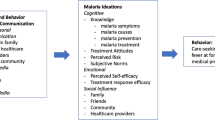
The ideation model (Fig. 1), which encompasses a broad set of psychosocial determinants of behaviour [6], has been used to understand and successfully promote a range of health behaviours across HIV treatment and prevention [7, 8], family planning [9,10,11,12], water, sanitation and hygiene [13], and the Ebola response [14].

Ideation model of communication
A growing body of literature describes how cognitive, emotional, and social constructs contained in the ideation model (i.e., ideational factors) are associated with individual and household malaria behaviours. Single and multi-country studies conducted throughout sub-Saharan Africa have, for example, found ideational variables to be predictive of ownership [15], use [16,17,18], and care of insecticide-treated mosquito nets (ITNs). Studies have also found ideational variables linked to both care-seeking for fever [19, 20] and uptake of intermittent preventive treatment of malaria during pregnancy (IPTp) [21].
While research on ideational factors has been used to better understand and promote malaria behaviours in high-transmission settings, less is known about how ideational factors present in low-transmission settings and the role of these factors in malaria-related behaviours. Areas with low and very low transmission (defined further in Methods section) are distinct from areas with moderate to high levels of transmission in several important ways including: increased geographic focalization of malaria cases; a shift toward cases among adults, particularly men; increased importance of outdoor and occupation-based exposure; and imported malaria cases [22].
While core malaria interventions (ITNs, IRS, testing and treatment for malaria, and IPTp) remain important, a number of other interventions, which may or may not be WHO-recommended, are implemented by malaria programmes in lower transmission settings to target malaria parasites and vectors [23]. These include the use of personal protection measures, such as repellents or insecticide-treated hammock nets to protect higher risk groups, larval source management (LSM), active case detection (ACD) to identify new cases within a household or community, and presumptive chemoprevention approaches, such as mass drug administration (MDA), targeted drug administration, and reactive drug administration to eliminate the parasite reservoir [23].
Understanding specific behaviours related to malaria interventions in low-transmission settings, the drivers of those behaviours, and the context in which they occur will play an important role in achieving malaria elimination [24]. Interventions to affect behaviour change at the individual and household level, such as consistent ITN use will likely be most effective alongside structural changes such as expanding improved housing and LSM [25]. This review was carried out to identify existing research on ideational factors and malaria behaviours in low-transmission contexts and gaps in evidence that can be filled through future research.
Methods
Search strategy
A systematic search of eight academic databases (PubMed, Public Health ProQuest, Academic Search Ultimate, Web of Science, SOC Index, Communication & Mass Media, EMBASE, and Science Direct) was conducted using key terms defined a priori (see Additional file 1). An additional manual search of reference lists of publications belonging to the University of California San Francisco Malaria Elimination Initiative (UCSF-MEI), the Roll Back Malaria (RBM) Partnership to End Malaria, and The U.S. President’s Malaria Initiative (PMI) was performed. For the purposes of this review, “low-transmission settings” were defined as a context characterized by annual parasite incidence (API) lower than 250 cases per 1000 population or Plasmodium falciparum/Plasmodium vivax prevalence rate of < 10%. This definition aligns with A Framework for Malaria Elimination of the WHO [24], which also produced a list of countries that qualify as low-transmission settings according to this definition. This list of countries served as an initial list to inform the search strategy, although searches were not limited only to those identified in the report.
Key search terms included a combination of: “malaria”, one or more psychosocial constructs within the ideational model; and either one or more geographic terms that reflect a low-transmission setting or one or more terms that reflect a key subpopulation that evidence suggests may experience risk focalization in low-transmission settings (see Additional file 1). These key subpopulations include, among others, seasonal workers, forest goers, miners, migrant workers, and internally displaced persons (IDPs). Specifically, psychosocial constructs included in searches included: malaria knowledge; attitudes toward malaria; perceived risk of malaria; perceived response-efficacy of malaria prevention and treatment approaches; one’s perceived self-efficacy to take certain malaria actions; and interpersonal communication. Additionally, three types of perceived social norms were included in the search: the perceived descriptive norm (referring to how an individual perceives their community to think, feel, or act – in this case, related to malaria behaviours); the perceived subjective norm (one’s perceptions of what others who are important to the individual want them to do); and the perceived injunctive norm (whether an individual perceives most people in the community to approve of an action).
Eligibility criteria
The relevance of publications was determined based on inclusion and exclusion criteria defined in Table 1. To minimize outdated information, only studies published from 2000 to 2020 were included. No restrictions were placed on the study design. Publications were limited to the English language. Publications were included if the focus of the research was on investigating the relationship between individual or community psychosocial determinants and malaria behaviour.
Study selection
Search results were imported into Endnote version X9. Following the removal of duplicate articles, study titles were screened to assess eligibility. Then, a separate full-text screening of retained articles was conducted to confirm eligibility. Results were excluded if the publication did not meet all inclusion criteria. Reviewers discussed and resolved through consensus any discordances during the selection process.
Results synthesis
Key characteristics of publications that met inclusion criteria were summarized, including focus population of the study, study design and sampling method, measurement of each psychosocial construct (cognitive, social, emotional) contained in the ideation model, and the malaria behaviour of focus. Following the charting of publications, an inductive thematic analysis method identified common themes related to findings.
Results
A total of 961 titles were screened for inclusion, resulting in 267 publications. that qualified for further screening. Following title screening, a full-text screening was conducted to confirm that the publication met inclusion criteria, which included verification of API or P. falciparum/P. vivax prevalence data as available in the country of publication. The selection process aligned with PRISMA guidelines [26] (Fig. 2). During the full-text screening, 181 publications were determined to be ineligible. Common reasons for exclusion included: the study not taking place in a low-transmission setting (n = 84); the study not measuring or discussing the relationship between psychosocial ideational factors and a malaria behaviour (n = 91); or the full text not being available (n = 6). Five additional grey literature publications were purposively selected, based on collaboration with institutional partners. A recently completed systematic review [27] was not included in the study, but purposively reviewed to ensure that relevant studies were captured.

PRISMA diagram
Study location and population
The majority of research publications (58%) focused on an Asian country. The Greater Mekong Subregion (Cambodia, China (Yunnan Province), Laos, Myanmar, Thailand, and Vietnam) accounted for 25 publications (27%), while Bangladesh, India, Indonesia, Malaysia, and Sri Lanka were also represented. Twenty-nine publications (32%) focused on an African country, with Ethiopia (n = 10), Tanzania/Zanzibar (n = 4), and Zambia (n = 3) the most common locations of research. Countries representing South America, the Pacific, and the Middle East regions encompassed the remaining 10% of publications. Four studies included multiple countries.
Nineteen articles (20%) specified a focalized subpopulation as the subject of the research, citing an increased risk of transmission among the subject group in an otherwise low-transmission area. These subpopulations were identified largely (but not exclusively) based on occupation and included forest workers [28,29,30]; rubber tappers [31, 32]; construction workers [33]; military/security personnel [34]; seasonal migrant workers and miners [35,36,37,38,39]; subsistence agricultural workers [40, 41]; night-time venue workers [70]; refugee communities [42]; and internally displaced communities [43]. Often initial engagement through interviews and/or focus group discussions with key informants, such as Ministry of Health (MOH) staff, National Malaria Programme (NMP) staff, and/or local leaders not only helped to identify which subpopulations experience increased risk in low-transmission settings but also provided information on where and how to engage these populations in data collection.
The remaining articles (n = 72) collected data from general community members, health care providers, or caregivers in settings characterized by low transmission. Pregnant women, child caregivers, and households with children under 5 years old were the focus of only 12 studies. While these groups were not determined to be at additional risk of exposure relative to their communities, they are more likely to develop severe malaria disease than the general population [44]. Further, women of reproductive age living in low-transmission settings have lower acquired immunity to malaria than women living in high-transmission settings [44].
Study design
Table 2 summarizes the study design of included articles, as well as the frequency of measurement for each psychosocial factor and type of malaria behaviour (i.e., prevention or treatment). A total of thirty-one studies (34%) included data on prevention behaviours only, while seven studies (8%) included data on treatment behaviours only. Forty-six studies (51%) included data on both preventive and treatment behaviours. Finally, five studies [34, 45,46,47,48] described psychosocial variables in a setting of low malaria transmission but did not measure associations with human behaviour. Common prevention behaviours measured include the use of ITNs, participation in IRS, and willingness to accept LSM in one’s community. Common treatment behaviours included willingness to accept MDA and seeking testing and care at a health facility.
A quantitative design was used in 60 studies, 93% of which applied a one-time cross-sectional survey. Four studies [42, 49,50,51] used a pre-post longitudinal survey design. Ten studies [29, 45, 48, 52,53,54,55,56,57] implemented a design using only qualitative methods such as focus group discussions and in-depth interviews. The remaining studies utilized a mixed-methods approach, which most commonly included a combination of cross-sectional surveys and in-depth interviews, focus group discussions, or qualitative observations with a subset of the survey sample.
Sample designs included cluster random sampling (n = 28), stratified random sampling (n = 8), simple random sampling (n = 11), purposive sampling (n = 38), and convenience sampling (n = 5). Purposive methods were often employed using time-location and respondent-referral methods such as snowball and respondent-driven sampling, particularly when authors aimed to collect data from individuals whose work or social environment places them at increased risk of transmission. These methods may be useful among subpopulations that are highly mobile, and for whom it is difficult to establish a traditional sampling frame. However, while each of these approaches contains strengths, variable study designs and sampling strategies poses challenges when attempting to compare findings across settings.
Psychosocial measures
Knowledge of malaria was the most commonly measured psychosocial ideational factor and was included in 82 publications (86%). This measurement often included quantitative questions prompting a participant to identify the cause of malaria and common symptoms of infection, ways to diagnose malaria, and ways to prevent infection.
Individual attitudes (59% of publications), and perceived risk of contracting malaria (36% of publications) were routinely measured and discussed. Attitudes were measured in multiple ways, and generally referred to one’s perception related to a care-seeking or prevention measure, e.g., agreement that sleeping under a bed net is comfortable; insecticide-treated clothing is durable or pleasant to wear [31], that the benefits of spraying interior walls outweigh the risks [65]; there is no alternative to seeking care at a health facility when a child has fever; and that care-seeking should occur within 24 h of the onset of fever [103].
Qualitative measures of attitudes primarily utilized open-ended questions to focus on reasons why an intervention is not considered acceptable [29, 48, 65, 104]. Quantitative attitudinal measures were often limited to agreement with one or two statements. While a different psychosocial construct, measures of perceived risk were often miscategorized as “attitudes” in studies and included agreement with closed-ended statements that malaria is dangerous, can be deadly, and/or that the respondent is vulnerable to malaria [53,54,55, 66, 91], although several studies assessed perceived risk via open-ended interview questions [29, 76, 84].
Other psychosocial factors including perceived response efficacy (i.e., one’s belief that a certain action and/or commodity will avoid or resolve the problem; 9% of publications), perceived self-efficacy (i.e., one’s confidence in their ability to perform a specific behaviour; 6% of publications), and interpersonal communication (1% of publications) were less commonly measured by the literature.
Linkages between psychosocial factors and malaria behaviours
A review of these 91 studies offers evidence for multiple linkages between psychosocial factors and malaria behaviours. Prevention and treatment-seeking behaviours were routinely measured across the reviewed articles. Prevention behaviours included net use, net procurement, net maintenance, acceptance of IRS, acceptance of SMC, and smaller-scale interventions such as the use of treated clothing. Treatment behaviours included acceptance of MDA, seeking care for malaria symptoms, types of treatment services sought (e.g., hospital-based services or traditional medicine services), adherence to treatment, and factors motivating prompt or delayed treatment seeking.
Among articles that measured knowledge, there were generally positive associations between one’s level of knowledge about malaria (symptoms and causes) and their behaviour. However, studies also largely cited a high rate of correct knowledge at the time of study while rates of malaria-related behaviours varied. This suggests that knowledge alone may not be sufficient to achieve behaviour change (for examples, see [53, 81,82,83]). While the majority of studies focused on community member knowledge as the subject, others such as Hein et al. [36] assessed health care provider knowledge and discussed a positive relationship between health care provider knowledge of malaria and testing patients with fever for malaria.
Evidence from the reviewed studies suggests that individuals with a high level of perceived susceptibility to malaria are more likely to practice preventive or treatment behaviours [53, 54, 81, 82]. Studies focusing on child caregivers also frequently measured this variable with questions assessing the caretaker’s perception of whether they or the child were at risk for severe malaria. This data was collected in combination with prevention behaviour data. Perceived susceptibility and severity were commonly reported as low in areas of low transmission [41, 60, 61, 76, 84, 101, 108, 111]. Authors in these studies discuss that this may be because the individual does not consider malaria to be a common problem in their community.
Perceived response efficacy of recommended prevention and/or treatment behaviours was measured in seven studies [35, 45, 48, 53, 76, 102, 105], using both quantitative (Likert-scale) and qualitative measures. Of these articles, three assessed the acceptability and perceived effectiveness of ITN usage, two assessed the perceived effectiveness of IRS, one assessed the perceived effectiveness of healthcare worker efforts to increase malaria prevention behaviours, and one assessed the perceived effectiveness of MDA. Results indicate inconsistent associations. A study on perceived effectiveness and MDA participation [34] yielded positive associations, as did a study assessing acceptance of IRS [48]. Other studies, however [45, 76, 102, 105], did not yield a positive association between perceived response efficacy and malaria behaviour. This may be due to other factors producing a stronger effect on the behaviour, such as perceived risk [53].
Other psychosocial determinants, including perceived self-efficacy, interpersonal communication, and norms (i.e., subjunctive, injunctive, and descriptive norms) were not consistently measured across studies. Thus, the study team did not conduct an assessment to identify trends in their relationship to behavioural outcomes.
Discussion
There are several implications of this review for future malaria research and practice in settings of low transmission. These have been summarized in brief, and are presented in Table 3. Each of these implications are then described in further detail.
While the review identified many studies investigating psychosocial drivers of malaria-related behaviours in low-transmission contexts, few included a full range of psychosocial factors that are known precursors to behaviour change. Knowledge, attitudes, and perceived risk regarding malaria were the most common factors measured in the reviewed studies, while other psychosocial factors were neither commonly nor sufficiently measured. These poorly studied factors include descriptive and injunctive norms, perceived response efficacy, perceived self-efficacy, and interpersonal communication. Each of these variables has been shown to influence malaria behaviours in high-transmission settings, and future research in low-transmission settings would benefit from incorporating these variables into research tools.
Studies that measured knowledge and/or perceived risk of malaria generally yielded positive associations with malaria preventive behaviour; for instance, an individual’s level of knowledge or perceived risk was routinely found to be positively associated with their practice of a malaria preventive behaviour in the studies reviewed. In Southeast Asian contexts, these results align with those found in a recent systematic review by Cheng et al. [119], which suggest knowledge of malaria, perceived response efficacy, and positive attitudes toward ITNs are key factors associated with their use. Similarly, positive attitudes towards MDA programmes, perceived self-efficacy, and joint decision-making were emphasized as important influencing factors of MDA participation. Rates of correct knowledge appear to generally be high among the populations studied in the Cheng et al. review, and thus do not offer much room for improvement by way of social and behaviour change programmes aside from maintaining current knowledge. In the present review, individuals with high perceived risk (susceptibility and severity) toward malaria were more likely than those without this perception to practice preventive or care-seeking behaviours. However, perceived risk may tend to remain low in areas that are not characterized by high transmission, as the individual may not consider malaria to be a common problem in their community [40, 55]. Malaria SBC programmes in low-transmission settings may see improved outcomes from reinforcing that malaria is serious and continues to pose a threat to the community, particularly among groups subject to increased risk of exposure or vulnerability.
To determine the links between psychosocial factors and malaria behaviours across settings and over time, additional work is needed to clearly define and standardize measurement. Few reviewed studies included an element of theory, the importance of which has recently been discussed in the context of malaria control [120]. Using theoretical models to hypothesize the relationships between psychosocial factors and behaviour will improve the research design, quality of the research, and local relevance of findings. In the current review, psychosocial variables were often defined and measured differently across studies. Indeed, there is not currently a consensus or a shared definition of most psychosocial variables, nor is measurement consistent across settings. This can be achieved through utilizing standard measures such as those included in questionnaires for the Malaria Behavior Survey (MBS), the Malaria Indicator Survey SBCC module, and the RBM Partnership to End Malaria SBC Indicator Reference Guide. Consistent collection of this set of variables across a range of settings allows for comparison across contexts and over time, while providing the context- specific information needed to inform malaria programmes [120]. Given the positive associations found between perceived susceptibility or severity and practicing malaria behaviours, it will be important for researchers to measure both, as well as behaviours, in settings of low transmission.
This challenge in measurement presents an opportunity for future research in low-transmission settings. In particular, the MBS has been implemented in several high-transmission countries. MBS instruments were designed in collaboration with the RBM partnership and survey items validated in several countries. The MBS recently launched a version of the questionnaire tailored to low-transmission settings. Future research seeking to measure multiple psychosocial variables and malaria behaviours may benefit from using MBS instruments as a point of departure. Broad application of this research method may produce more consistent and comparable measurement of psychosocial determinants, particularly malaria attitudes, which were inconsistently measured among the reviewed studies. Data may then be integrated into ongoing SBC interventions to ensure efficient and strategic use of resources in addressing the determinants that shape malaria prevention and treatment behaviours in low-transmission settings.
There are few published articles focusing on subpopulations that experience disproportionate risk of exposure such as forest goers, gold (or other mineral) miners, rubber tappers, or night-time workers, although there is some recently emerging research to this effect [121]. Studies that focus on these subpopulations utilize respondent-driven sampling and time-location sampling techniques. These studies also routinely engaged government personnel, such as MOH and NMP staff, as well as community leaders before determining an appropriate sampling strategy. Formative engagement such as this has been described in detail and is recommended by the UCSF High Risk Populations Surveillance and Response Guide [122]. As malaria elimination activities may focus further on these subpopulations, there is opportunity and a need to strengthen the sampling methods, as well as the methods to assess and quantify the psychosocial variables that influence malaria prevention and treatment behaviours in low transmission settings. Future research should maintain the practice of engaging with key stakeholders early in the research process to ensure the population sampled is relevant and that research findings can be translated into programmatic applications.
There are several limitations to this review. First, only English publications were included, which may limit the inclusion of technical reports and publications in other languages. This may particularly limit the inclusion of materials from Francophone African contexts such as Senegal. Second, the psychosocial variables included in key search terms drew from the ideation model. While this is not the only model that includes psychosocial determinants of behaviour, it draws on constructs from multiple behavioural theories, including the Health Belief Model, the Theory of Planned Behaviour, the Extended Parallel Process Model and the Social Cognitive Theory and, therefore, is expected to cover a broad range of relevant factors. The authors feel that, overall, this article provides a useful synthesis of available evidence on psychosocial drivers of malaria in low transmission settings. Settings such as South America were more limited than expected. This appears due to the screening criteria. Often, studies based in Central and South America, and the Caribbean measured an ideational factor and behaviour, but did not test the factor-behaviour association, thus rendering the article ineligible. Finally, findings of this review are not intended to suggest that addressing psychosocial determinants alone are sufficient to change behaviour. In the context of malaria elimination, behaviour change relies on functioning health systems, including strong malaria elimination and control programmes. Indeed, broad investments in health systems are requisite to achieve elimination of malaria, as has been previously advocated for by academics and the WHO [116,117,118].
Conclusions
The review highlights the need for more consistent, comprehensive measures of psyctors and the importance of reaching subpopulations at higher risk of transmission in low transmission contexts. Malaria-related knowledge is generally high, even in settings of low transmission. However, malaria-related knowledge in these settings is lower among sub-populations who experience the highest malaria risk. Programmes and research aiming to improve malaria-related behaviours in these settings should work to better understand the psychosocial factors that have been positively associated with prevention and care-seeking behaviours, such as norms, perceived response efficacy, perceived self-efficacy, and interpersonal communication. While these factors are not necessarily distinct from psychosocial factors identified in similar research focused in high malaria transmission settings, it is important to better understand how each factor may influence behaviour in a low transmission context. Further, the implications for malaria behaviour change programming are different and an area in need of further research. Existing research tools and approaches are available to support more systematic collection of psychosocial determinants and improved sampling approaches and should be applied more widely. In low-transmission settings, these tools can provide useful information on people’s beliefs and perceptions toward local interventions. As interventions in low transmission settings are often tailored, capturing this type of data may be useful for both programme evaluation and quality improvement.
References
WHO. World malaria report 2022. Geneva: World Health Organization; 2022.
Koenker H, Kilian A, Hunter G, Acosta A, Scandurra L, Fagbemi B, et al. Impact of a behaviour change intervention on long-lasting insecticidal net care and repair behaviour and net condition in Nasarawa state, Nigeria. Malar J. 2015;14:18.
Opiyo MA, Paaijmans KP. “We spray and walk away”: wall modifications decrease the impact of indoor residual spray campaigns through reductions in post-spray coverage. Malar J. 2020;19:30.
de Savigny D, Mayombana C, Mwageni E, Masanja H, Minhaj A, Mkilindi Y, et al. Care-seeking patterns for fatal malaria in Tanzania. Malar J. 2004;3:27.
Kincaid D, Delate R, Storey D, Figueroa M. Closing the gaps in practice and in theory: evaluation of the scrutinize HIV campaign in South Africa. In: Rice RE, Atkin CK, editors. Public communication campaigns. 4th ed. London: SAGE Publications Inc.; 2013. https://doi.org/10.4135/9781544308449.
Kincaid DL. Mass media, ideation, and behavior: a longitudinal analysis of contraceptive change in the Philippines. Comm Res. 2000;27:723–63.
Babalola S. Readiness for HIV testing among young people in Northern Nigeria: the roles of social norm and perceived stigma. AIDS Behav. 2007;11:759–69.
Bertrand JT, O’Reilly K, Denison J, Anhang R, Sweat M. Systematic review of the effectiveness of mass communication programs to change HIV/AIDS-related behaviors in developing countries. Health Educ Res. 2006;21:567–97.
Babalola S, Folda L, Babayaro H. The effects of a communication program on contraceptive ideation and use among young women in northern Nigeria. Stud Fam Plann. 2008;39:211–20.
Babalola S, Vonrasek C. Communication, ideation and contraceptive use in Burkina Faso: an application of the propensity score matching method. J Fam Plann Reprod Health Care. 2005;31:207–12.
Kincaid DL, Storey JD, Figueroa ME, Underwood CR. Communication, ideation and contraceptive use: the relationships observed in five countries. In: Proceedings of the world congress on communication for development. Washington: World Bank; 2007.
Kincaid DL. Social networks, ideation, and contraceptive behavior in Bangladesh: a longitudinal analysis. Soc Sci Med. 2000;50:215–31.
Naugle DA, Hornik RC. Systematic review of the effectiveness of mass media interventions for child survival in low- and middle-income countries. J Health Commun. 2014;19(Suppl 1):190–215.
Figueroa ME. A theory-based socioecological model of communication and behavior for the containment of the Ebola epidemic in Liberia. J Health Commun. 2017;22(Suppl 1):5–9.
Ricotta E, Boulay M, Ainslie R, Babalola S, Fotheringham M, Koenker H, et al. The use of mediation analysis to assess the effects of a behaviour change communication strategy on bed net ideation and household universal coverage in Tanzania. Malar J. 2015;14:15.
Babalola S, Ricotta E, Awantang G, Lewicky N, Koenker H, Toso M. Correlates of intra-household ITN use in Liberia: a multilevel analysis of household survey data. PLoS ONE. 2016;11: e0158331.
Babalola S, Adedokun ST, McCartney-Melstad A, Okoh M, Asa S, Tweedie I, et al. Factors associated with caregivers’ consistency of use of bed nets in Nigeria: a multilevel multinomial analysis of survey data. Malar J. 2018;17:280.
Storey JD, Babalola SO, Ricotta EE, Fox KA, Toso M, Lewicky N, et al. Associations between ideational variables and bed net use in Madagascar, Mali, and Nigeria. BMC Public Health. 2018;18:484.
Awantang G, Babalola S, Koenker H, Fox K, Toso M, Lewicky N, et al. Correlates of social behavior change communication on care-seeking behaviors for children with fever: an analysis of malaria household survey data from Liberia. Malar J. 2018;17:105.
Do M, Babalola S, Awantang G, Toso M, Lewicky N, Tompsett A. Associations between malaria-related ideational factors and care-seeking behavior for fever among children under five in Mali, Nigeria, and Madagascar. PLoS ONE. 2018;13: e0191079.
Awantang GN, Babalola SO, Koenker H, Fox KA, Toso M, Lewicky N. Malaria-related ideational factors and other correlates associated with intermittent preventive treatment among pregnant women in Madagascar. Malar J. 2018;17:176.
Cotter C, Sturrock HJ, Hsiang MS, Liu J, Phillips AA, Hwang J, et al. The changing epidemiology of malaria elimination: new strategies for new challenges. Lancet. 2013;382:900–11 (Erratum in: Lancet. 2013;382:858).
WHO. Global technical strategy for malaria 2016–2030. Geneva: World Health Organization; 2015.
WHO. A framework for malaria elimination. Geneva: World Health Organization; 2017.
Hausmann-Muela S, Eckl J. Re-imagining malaria—a platform for reflections to widen horizons in malaria control. Malar J. 2015;14:180.
Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. 2015;4:1.
Regmi K, Kunwar A, Ortega L. A systematic review of knowledge, attitudes and beliefs about malaria among the South Asian population. Infect Ecol Epidemiol. 2016;6:30822.
Al-Adhroey AH, Nor ZM, Al-Mekhlafi HM, Mahmud R. Opportunities and obstacles to the elimination of malaria from Peninsular Malaysia: knowledge, attitudes and practices on malaria among aboriginal and rural communities. Malar J. 2010;9:137.
Chen I, Thanh HNT, Lover A, Thao PT, Luu TV, Thang HN, et al. Malaria risk factors and care-seeking behaviour within the private sector among high-risk populations in Vietnam: a qualitative study. Malar J. 2017;16:414.
Moore SJ, Min X, Hill N, Jones C, Zaixing Z, Cameron MM. Border malaria in China: knowledge and use of personal protection by minority populations and implications for malaria control: a questionnaire-based survey. BMC Public Health. 2008;8:344.
Crawshaw AF, Maung TM, Shafique M, Sint N, Nicholas S, Li MS, et al. Acceptability of insecticide-treated clothing for malaria prevention among migrant rubber tappers in Myanmar: a cluster-randomized non-inferiority crossover trial. Malar J. 2017;16:92.
Thomson R, Sochea P, Sarath M, MacDonald A, Pratt A, Poyer S, et al. Rubber plantations and drug resistant malaria: a cross-sectional survey in Cambodia. Malar J. 2019;18:379.
Shivalli S, Pai S, Akshaya KM, D’Souza N. Construction site workers’ malaria knowledge and treatment-seeking pattern in a highly endemic urban area of India. Malar J. 2016;15:168.
Fernando SD, Rodrigo C, de Silva N, Semege S, Rajapakse S, Samaranayake N, et al. Educating the security forces, a high risk group in malaria elimination efforts: an example from Sri Lanka. Int Health. 2014;6:196–202.
Adhikari B, Phommasone K, Pongvongsa T, Soundala X, Koummarasy P, Henriques G, et al. Perceptions of asymptomatic malaria infection and their implications for malaria control and elimination in Laos. PLoS ONE. 2018;13: e0208912.
Hein KT, Maung TM, Htet KKK, Shewade HD, Tripathy JP, Oo SM, et al. Low uptake of malaria testing within 24 h of fever despite appropriate health-seeking among migrants in Myanmar: a mixed-methods study. Malar J. 2018;17:396.
Phyo Than W, Oo T, Wai KT, Thi A, Owiti P, Kumar B, Deepak Shewade H, Zachariah R. Knowledge, access and utilization of bed-nets among stable and seasonal migrants in an artemisinin resistance containment area of Myanmar. Infect Dis Poverty. 2017;6:138.
Wai KT, Kyaw MP, Oo T, Zaw P, Nyunt MH, Thida M, et al. Spatial distribution, work patterns, and perception towards malaria interventions among temporary mobile/migrant workers in artemisinin resistance containment zone. BMC Public Health. 2014;14:463.
Wangroongsarb P, Satimai W, Khamsiriwatchara A, Thwing J, Eliades JM, Kaewkungwal J, et al. Respondent-driven sampling on the Thailand-Cambodia border. II. Knowledge, perception, practice and treatment-seeking behaviour of migrants in malaria endemic zones. Malar J. 2011;10:117.
Peeters Grietens K, Xuan XN, Van Bortel W, Duc TN, Ribera JM, Ba Nhat T, et al. Low perception of malaria risk among the Ra-glai ethnic minority in south-central Vietnam: implications for forest malaria control. Malar J. 2010;9:23.
Saha A, Sarker M, Kabir M, Lu G, Müller O. Knowledge, attitudes, and practices regarding malaria control among the slash and burn cultivators in Rangamati Hill tracts of Bangladesh. Malar J. 2019;18:216.
Cropley L. The effect of health education interventions on child malaria treatment-seeking practices among mothers in rural refugee villages in Belize, Central America. Health Promot Int. 2004;19:445–52.
Kirkby K, Galappaththy GN, Kurinczuk JJ, Rajapakse S, Fernando SD. Knowledge, attitudes and practices relevant to malaria elimination amongst resettled populations in a post-conflict district of northern Sri Lanka. Trans R Soc Trop Med Hyg. 2013;107:110–8.
U.S. centers for disease control and prevention. Treatment of malaria: guidelines for clinicians (United States). 2023. http://www.cdc.gov/malaria/resources/pdf/Malaria_Trx_Guide_for_US_Clinicians_202302c.pdf. Accessed 25 Oct 2023.
Beer N, Ali AS, Eskilsson H, Jansson A, Abdul-Kadir FM, Rotllant-Estelrich G, et al. A qualitative study on caretakers’ perceived need of bed-nets after reduced malaria transmission in Zanzibar, Tanzania. BMC Public Health. 2012;12:606.
Fernando SD, Ainan S, Premaratne RG, Rodrigo C, Jayanetti SR, Rajapakse S. Challenges to malaria surveillance following elimination of indigenous transmission: findings from a hospital-based study in rural Sri Lanka. Int Health. 2015;7:317–23.
Goshu YA, Yitayew AE. Malaria knowledge and its associated factors among pregnant women attending antenatal clinic of Adis Zemen Hospital, North-western Ethiopia, 2018. PLoS ONE. 2019;14: e0210221.
Munguambe K, Pool R, Montgomery C, Bavo C, Nhacolo A, Fiosse L, et al. What drives community adherence to indoor residual spraying (IRS) against malaria in Manhiça district, rural Mozambique: a qualitative study. Malar J. 2011;10:344.
Aung PL, Pumpaibool T, Soe TN, Burgess J, Menezes LJ, Kyaw MP, et al. Health education through mass media announcements by loudspeakers about malaria care: prevention and practice among people living in a malaria endemic area of northern Myanmar. Malar J. 2019;18:362.
Kishore J, Gupta VK, Singh SV, Garg S, Kaur R, Ingle GK. Impact of health education intervention on knowledge and community action for malaria control in Delhi. J Commun Dis. 2008;40:183–92.
Yadav SP, Yadav S, Kuma P, Yadav S. Knowledge, treatment-seeking behaviour and socio-economic impact of malaria in the desert of Rajasthan, India. South Afr J Epidemiol Infect. 2013;28:41–7.
Atkinson JA, Fitzgerald L, Toaliu H, Taleo G, Tynan A, Whittaker M, et al. Community participation for malaria elimination in Tafea Province, Vanuatu: part I. Maintaining motivation for prevention practices in the context of disappearing disease. Malar J. 2010;9:93.
Atkinson JA, Bobogare A, Fitzgerald L, Boaz L, Appleyard B, Toaliu H, et al. A qualitative study on the acceptability and preference of three types of long-lasting insecticide-treated bed nets in Solomon Islands: implications for malaria elimination. Malar J. 2009;8:119.
Baltzell KA, Maglior A, Bangu K, Mngadi N, Prach LM, Whittemore B, et al. “We were afraid of the lion that has roared next to us”; community response to reactive focal mass drug administration for malaria in Eswatini (formerly Swaziland). Malar J. 2019;18:238.
Bauch JA, Gu JJ, Msellem M, Mårtensson A, Ali AS, Gosling R, et al. Perception of malaria risk in a setting of reduced malaria transmission: a qualitative study in Zanzibar. Malar J. 2013;12:75.
Das A, Das Gupta RK, Friedman J, Pradhan MM, Mohapatra CC, Sandhibigraha D. Community perceptions on malaria and care-seeking practices in endemic Indian settings: policy implications for the malaria control programme. Malar J. 2013;12:39.
Monroe A, Mihayo K, Okumu F, Finda M, Moore S, Koenker H, et al. Human behaviour and residual malaria transmission in Zanzibar: findings from in-depth interviews and direct observation of community events. Malar J. 2019;18:220.
Ahmed SM, Hossain S, Kabir MM, Roy S. Free distribution of insecticidal bed nets improves possession and preferential use by households and is equitable: findings from two cross-sectional surveys in thirteen malaria endemic districts of Bangladesh. Malar J. 2011;10:357.
Aung T, Wei C, McFarland W, Aung YK, Khin HS. Ownership and use of insecticide-treated nets among people living in malaria endemic areas of Eastern Myanmar. PLoS ONE. 2016;11: e0162292.
Bamaga OA, Mahdy MA, Mahmud R, Lim YA. Malaria in Hadhramout, a southeast province of Yemen: prevalence, risk factors, knowledge, attitude and practices (KAPs). Parasit Vectors. 2014;7:351.
Dambhare DG, Nimgade SD, Dudhe JY. Knowledge, attitude and practice of malaria transmission and its prevention among the school going adolescents in Wardha district. Central India Glob J Health Sci. 2012;4:76–82.
Deressa W. Individual and household factors associated with ownership of long-lasting insecticidal nets and malaria infection in south-central Ethiopia: a case-control study. Malar J. 2017;16:402.
Douine M, Lazrek Y, Blanchet D, Pelleau S, Chanlin R, Corlin F, et al. Predictors of antimalarial self-medication in illegal gold miners in French Guiana: a pathway towards artemisinin resistance. J Antimicrob Chemother. 2018;73:231–9.
Fernando SD, Abeyasinghe RR, Galappaththy GN, Gunawardena N, Rajapakse LC. Community factors affecting long-lasting impregnated mosquito net use for malaria control in Sri Lanka. Trans R Soc Trop Med Hyg. 2008;102:1081–8.
Gobena T, Berhane Y, Worku A. Women’s knowledge and perceptions of malaria and use of malaria vector control interventions in Kersa, Eastern Ethiopia. Glob Health Action. 2013;6:20461.
Heemskerk, M, Duijves C. Gold miners’ knowledge, attitudes and practices with regard to malaria in Suriname. Bureau Openbare Gezondheidszorg (BOG), Malaria Program. Suriname Ministry of Health. 2018. http://social-solutions.net/data/images/reports/goldminers_knowlegde.pdf. Accessed 19 Oct 2023.
Jusoh N, Shah SA. Influence of risk perception, preventive behavior, movement and environment on malaria infection in Lundu district, Sarawak, Malaysia. Med J Indones. 2007;16:267–76.
Kannathasan S, Antonyrajan A, Srikrishnaraj KA, Karunaratne SH, Karunaweera ND, Surendran SN. Studies on prevalence of anopheline species and community perception of malaria in Jaffna district, Sri Lanka. J Vector Borne Dis. 2008;45:231–9.
Kanyangarara M, Hamapumbu H, Mamini E, Lupiya J, Stevenson JC, Mharakurwa S, et al. Malaria knowledge and bed net use in three transmission settings in southern Africa. Malar J. 2018;17:41.
Khairy S, Al-Surimi K, Ali A, Shubily HM, Al Walaan N, Househ M, et al. Knowledge, attitude and practice about malaria in south-western Saudi Arabia: a household-based cross-sectional survey. J Infect Public Health. 2017;10:499–506.
Madani A, Soleimani-Ahmadi M, Davoodi SH, Sanei-Dehkordi A, Jaberhashemi SA, Zare M, et al. Household knowledge and practices concerning malaria and indoor residual spraying in an endemic area earmarked for malaria elimination in Iran. Parasit Vectors. 2017;10:600.
Podder D, Paul B, Dasgupta A, Bandyopadhyay L, Pal A, Roy S. Community perception and risk reduction practices toward malaria and dengue: a mixed-method study in slums of Chetla, Kolkata. Indian J Public Health. 2019;63:178–85.
Singh MP, Saha KB, Chand SK, Anvikar A. Factors associated with treatment seeking for malaria in Madhya Pradesh, India. Trop Med Int Health. 2017;22:1377–84.
Soleimani-Ahmadi M, Vatandoost H, Zare M, Alizadeh A, Salehi M. Community knowledge and practices regarding malaria and long-lasting insecticidal nets during malaria elimination programme in an endemic area in Iran. Malar J. 2014;13:511.
Utarini A, Winkvist A, Ulfa FM. Rapid assessment procedures of malaria in low endemic countries: community perceptions in Jepara district, Indonesia. Soc Sci Med. 2003;56:701–12.
Lwin MO, Vijaykumar S, Lim G, Theng YL, Foo S. “It’s effective but should I bother?” A study of personal protection measures against Malaria in urban India. Public Health. 2014;128:654–64.
Whidden CE, Premaratne RG, Jayanetti SR, Fernando SD. Patterns and predictive factors of long-lasting insecticidal net usage in a previously high malaria endemic area in Sri Lanka: a cross-sectional survey. Trans R Soc Trop Med Hyg. 2015;109:553–62.
Kotepui KU, Kotepui M, Punsawad C. Knowledge, attitude, and practice related to malaria diagnosis among healthcare workers in hospitals: a cross-sectional survey. J Trop Med. 2019;2019:1414079.
Lwin MM, Sudhinaraset M, San AK, Aung T. Improving malaria knowledge and practices in rural Myanmar through a village health worker intervention: a cross-sectional study. Malar J. 2014;13:5.
Sanjana P, Barcus MJ, Bangs MJ, Ompusunggu S, Elyazar I, Marwoto H, et al. Survey of community knowledge, attitudes, and practices during a malaria epidemic in central Java, Indonesia. Am J Trop Med Hyg. 2006;75:783–9.
Tobgay T, Pem D, Dophu U, Dumre SP, Na-Bangchang K, Torres CE. Community-directed educational intervention for malaria elimination in Bhutan: quasi-experimental study in malaria endemic areas of Sarpang district. Malar J. 2013;12:132.
Yasuoka J, Kikuchi K, Nanishi K, Ly P, Thavrin B, Omatsu T, et al. Malaria knowledge, preventive actions, and treatment-seeking behavior among ethnic minorities in Ratanakiri Province, Cambodia: a community-based cross-sectional survey. BMC Public Health. 2018;18:1206.
Abate A, Degarege A, Erko B. Community knowledge, attitude and practice about malaria in a low endemic setting of Shewa Robit Town, northeastern Ethiopia. BMC Public Health. 2013;13:312.
Aerts C, Revilla M, Duval L, Paaijmans K, Chandrabose J, Cox H, et al. Understanding the role of disease knowledge and risk perception in shaping preventive behavior for selected vector-borne diseases in Guyana. PLoS Negl Trop Dis. 2020;14: e0008149.
Alam MS, Kabir MM, Hossain MS, Naher S, Ferdous NE, Khan WA, et al. Reduction in malaria prevalence and increase in malaria awareness in endemic districts of Bangladesh. Malar J. 2016;15:552.
Bashar K, Al-Amin HM, Reza MS, Islam M, Asaduzzaman, Ahmed TU. Socio-demographic factors influencing knowledge, attitude and practice (KAP) regarding malaria in Bangladesh. BMC Public Health. 2012;12:1084.
Berhane A, Mihreteab S, Ahmed H, Zehaie A, Abdulmumini U, Chanda E. Gains attained in malaria control coverage within settings earmarked for pre-elimination: malaria indicator and prevalence surveys 2012. Eritrea Malar J. 2015;14:467.
Birhanu Z, Yihdego YY, Yewhalaw D. Caretakers’ understanding of malaria, use of insecticide treated net and care seeking-behavior for febrile illness of their children in Ethiopia. BMC Infect Dis. 2017;17:629.
Canavati SE, de Beyl CZ, Ly P, Shafique M, Boukheng T, Rang C, et al. Evaluation of intensified behaviour change communication strategies in an artemisinin resistance setting. Malar J. 2016;15:249.
DePina AJ, Dia AK, de Ascenção Soares Martins A, Ferreira MC, Moreira AL, Leal SV, et al. Knowledge, attitudes and practices about malaria in Cabo Verde: a country in the pre-elimination context. BMC Public Health. 2019;19:850.
Deressa W, Ali A. Malaria-related perceptions and practices of women with children under the age of five years in rural Ethiopia. BMC Public Health. 2009;9:259.
Dhawan G, Joseph N, Pekow PS, Rogers CA, Poudel KC, Bulzacchelli MT. Malaria-related knowledge and prevention practices in four neighbourhoods in and around Mumbai, India: a cross-sectional study. Malar J. 2014;13:303.
Dhewantara PW, Ipa M, Widawati M. Individual and contextual factors predicting self-reported malaria among adults in eastern Indonesia: findings from Indonesian community-based survey. Malar J. 2019;18:118.
Forero DA, Chaparro PE, Vallejo AF, Benavides Y, Gutiérrez JB, Arévalo-Herrera M, et al. Knowledge, attitudes and practices of malaria in Colombia. Malar J. 2014;13:165.
Govere J, Durrheim D, la Grange K, Mabuza A, Booman M. Community knowledge and perceptions about malaria and practices influencing malaria control in Mpumalanga province, South Africa. S Afr Med J. 2000;90:611–6.
Hertz JT, Munishi OM, Sharp JP, Reddy EA, Crump JA. Comparing actual and perceived causes of fever among community members in a low malaria transmission setting in Northern Tanzania. Trop Med Int Health. 2013;18:1406–15.
Hlongwana KW, Mabaso ML, Kunene S, Govender D, Maharaj R. Community knowledge, attitudes and practices (KAP) on malaria in Swaziland: a country earmarked for malaria elimination. Malar J. 2009;8:29.
Joshi AB, Banjara MR. Malaria related knowledge, practices and behaviour of people in Nepal. J Vector Borne Dis. 2008;45:44–50.
Ly P, Thwing J, McGinn C, Quintero CE, Top-Samphor N, Habib N, et al. The use of respondent-driven sampling to assess malaria knowledge, treatment-seeking behaviours and preventive practices among mobile and migrant populations in a setting of artemisinin resistance in Western Cambodia. Malar J. 2017;16:1.
Manana PN, Kuonza L, Musekiwa A, Mpangane HD, Koekemoer LL. Knowledge, attitudes and practices on malaria transmission in Mamfene, KwaZulu-Natal Province, South Africa 2015. BMC Public Health. 2017;18:41 (Erratum in: BMC Public Health. 2017;17:736).
Mbonye AK, Mohamud SM, Bagonza J. Perceptions and practices for preventing malaria in pregnancy in a peri-urban setting in South-western Uganda. Malar J. 2016;15:211.
Shimaponda-Mataa NM, Tembo-Mwase E, Gebreslasie M, Mukaratirwa S. Knowledge, attitudes and practices in the control and prevention of malaria in four endemic provinces of Zambia. South Afr J Infect Dis. 2017;32:29–39.
Paulander J, Olsson H, Lemma H, Getachew A, San Sebastian M. Knowledge, attitudes and practice about malaria in rural Tigray, Ethiopia. Glob Health Action. 2009. https://doi.org/10.3402/gha.v2i0.1839.
Portugaliza HP, Galatas B, Nhantumbo H, Djive H, Murato I, Saúte F, et al. Examining community perceptions of malaria to inform elimination efforts in Southern Mozambique: a qualitative study. Malar J. 2019;18:232.
Roosihermiatie B, Nishiyama M, Nakae K. The human behavioral and socioeconomic determinants of malaria in Bacan Island, North Maluku, Indonesia. J Epidemiol. 2000;10:280–9.
Sabin L, Hecht EMS, Brooks MI, Singh MP, Yeboah-Antwi K, Rizal A, et al. Prevention and treatment of malaria in pregnancy: what do pregnant women and health care workers in East India know and do about it? Malar J. 2018;17:207.
Sood RD, Mittal PK, Kapoor N, Razdan RK, Dua VK, Dash AP. Community awareness, perceptions, acceptability and preferences for using LLIN against malaria in villages of Uttar Pradesh, India. J Vector Borne Dis. 2010;47:243–8.
Tesfay K, Yohannes M, Mardu F, Berhe B, Negash H. Assessment of community knowledge, practice, and determinants of malaria case households in the rural area of Raya Azebo district, Northern Ethiopia, 2017. PLoS ONE. 2019;14: e0222427.
Thandar MM, Kyaw MP, Jimba M, Yasuoka J. Caregivers’ treatment-seeking behaviour for children under age five in malaria-endemic areas of rural Myanmar: a cross-sectional study. Malar J. 2015;14:1.
van Benthem BH, Khantikul N, Panart K, Somboon P, Oskam L. Knowledge and use of preventive measures against malaria in endemic and non-endemic villages in northern Thailand, Southeast Asian. J Trop Med Public Health. 2006;37:243–9.
Vijayakumar KN, Gunasekaran K, Sahu SS, Jambulingam P. Knowledge, attitude and practice on malaria: a study in a tribal belt of Orissa state, India with reference to use of long lasting treated mosquito nets. Acta Trop. 2009;112:137–42.
Wylie BJ, Hashmi AH, Singh N, Singh MP, Tuchman J, Hussain M, et al. Availability and utilization of malaria prevention strategies in pregnancy in eastern India. BMC Public Health. 2010;10:557.
Yasuoka J, Mangione TW, Spielman A, Levins R. Impact of education on knowledge, agricultural practices, and community actions for mosquito control and mosquito-borne disease prevention in rice ecosystems in Sri Lanka. Am J Trop Med Hyg. 2006;74:1034–42.
Yewhalaw D, Kassahun W, Woldemichael K, Tushune K, Sudaker M, Kaba D, et al. The influence of the Gilgel-Gibe hydroelectric dam in Ethiopia on caregivers’ knowledge, perceptions and health-seeking behaviour towards childhood malaria. Malar J. 2010;9:47.
Yimer F, Animut A, Erko B, Mamo H. Past five-year trend, current prevalence and household knowledge, attitude and practice of malaria in Abeshge, south-central Ethiopia. Malar J. 2015;14:230.
malERA Consultative Group on Health Systems and Operational Research. A research agenda for malaria eradication: health systems and operational research. PLoS Med. 2011;8: e1000397.
Stratton L, O’Neill MS, Kruk ME, Bell ML. The persistent problem of malaria: addressing the fundamental causes of a global killer. Soc Sci Med. 2008;67:854–62.
de Savigny D, Adam T. Systems thinking for health systems strengthening. In: de Savigny D, Adam T, editors. Alliance for health policy and systems research. Geneva: World Health Organization; 2009.
Cheng B, Htoo SN, Mhote NPP, Davison CM. A systematic review of factors influencing participation in two types of malaria prevention intervention in Southeast Asia. Malar J. 2021;20:195.
Monroe A, Olapeju B, Moore S, Hunter G, Merritt AP, Okumu F, et al. Improving malaria control by understanding human behaviour. Bull World Health Organ. 2021;99:837–9 (Erratum in: Bull World Health Organ. 2021;99:912).
Olapeju B, Adams C, Hunter G, Wilson S, Simpson J, Mitchum L, et al. Malaria prevention and care seeking among gold miners in Guyana. PLoS ONE. 2020;15: e0244454.
Malaria Elimination Initiative. A malaria elimination guide to targeted surveillance and response in high-risk populations. San Francisco: Institute for Global Health Sciences, University of California; 2020.
Acknowledgements
Not applicable.
Funding
This work, through Breakthrough ACTION at the Johns Hopkins Center for Communication Programs, is funded by the Global Health Bureau of the United States Agency for International Development (USAID) and the U.S. President’s Malaria Initiative (PMI) under the terms of Cooperative Agreement No. AID-OAA-A-17-00017. The opinions and assertions expressed herein are those of the author(s) and do not reflect the official policy or position of USAID, PMI, or the Centers for Disease Control and Prevention. Findings and conclusions in this paper are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention or the United States Agency for International Development.
Author information
Authors and Affiliations
Contributions
AC and JH conducted the search and screening. AC charted the results and drafted the paper. AM, MT, GH, CU, RP, and LvL interpreted the results. SC and JH reviewed the manuscript. AC, AM, and SB designed the study, interpreted results, and reviewed the manuscript. All authors reviewed and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Search terms list.
Additional file 2:
Literature table.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Casella, A., Monroe, A., Toso, M. et al. Understanding psychosocial determinants of malaria behaviours in low-transmission settings: a scoping review. Malar J 23, 15 (2024). https://doi.org/10.1186/s12936-023-04831-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12936-023-04831-9