
Abstract
Glioblastoma (GBM) is an aggressive type of cancer that originates in the cells called astrocytes, which support the functioning of nerve cells. It can develop in either the brain or the spinal cord and is also known as glioblastoma multiform. GBM is a highly aggressive cancer that can occur in either the brain or spinal cord. The detection of GBM in biofluids offers potential advantages over current methods for diagnosing and treatment monitoring of glial tumors. Biofluid-based detection of GBM focuses on identifying tumor-specific biomarkers in blood and cerebrospinal fluid. To date, different methods have been used to detect biomarkers of GBM, ranging from various imaging techniques to molecular approaches. Each method has its own strengths and weaknesses. The present review aims to scrutinize multiple diagnostic methods for GBM, with a focus on proteomics methods and biosensors. In other words, this study aims to provide an overview of the most significant research findings based on proteomics and biosensors for the diagnosis of GBM.
Similar content being viewed by others

Introduction
Glioblastoma is the most common and aggressive primary malignant brain tumor in adults. In 2016, the World Health Organization (WHO) categorized gliomas into three major types based on histological approaches: astrocytoma, oligodendroglioma, and Ependymomas [1, 2]. The risk factors for GBM are almost indefinable, and the clinical course is usually fatal [3, 4]. Diagnosis is based on histopathological findings, but the evaluation of molecular markers, such as methylation of the O6-methylguanyl-DNA methyltransferase (MGMT) promoter and isocitrate dehydrogenase (IDH), as well as broader molecular profiling, can be prognostic [3, 4]. Secondary GBM arises from anaplastic astrocytoma or low-grade diffuse astrocytoma and occur in young patients. They have a low degree of necrosis, are predominantly located in the frontal lobe, and have a significantly improved prognosis compared to primary GBM [5, 6]. Although primary and secondary glioblastoma are almost indistinguishable histologically; they have different genetic and epigenetic profiles [5,6,7].
Several incomplete and definitive efforts have been made to identify specific associations between GBM and occupational exposure and environmental factors. Ionizing radiation is one of the few identified risk factors that clearly shows an increased risk of developing glioma [8, 9]. Radiation-induced GBM is typically observed years after therapeutic radiation for another disease or tumor has been administered. Other environmental exposures, such as pesticides, PVC, smoking, petroleum refining, and synthetic rubber manufacturing have been inaccurately associated with the development of glioma [10]. The presentation of newly diagnosed GBM patients critically varies depending on the location and size of the tumor and the anatomy of the affected brain [11]. Patients often present with intracranial hypertension symptoms, including localized or progressive neurological defects and headaches [11].
Early diagnostic imaging for GBM may include magnetic resonance imaging (MRI) or computed tomography (CT) [12]. MRI with gadolinium contrast highlights almost all GBMs, revealing irregularly shaped masses with hypointense necrotic centers and dense highlight rings [12]. Necrosis is a hallmark of GBM, and the existence is necessary for brain tumors to be classified as grade IV or GBM by the WHO classification system [12]. Treatment of newly diagnosed GBM requires an interdisciplinary approach. The current standard of care involves maximally safe surgical excision followed by combination radiotherapy with temozolomide (TMZ), an oral alkylating chemotherapy agent, and adjuvant chemotherapy with TMZ. However, comprehensive and complete surgical resection of GBM is difficult, as these tumors are often invasive and located in eloquent areas of the brain, that control movement, language, and sensation. This study aims to confirm recent advances in GBM detection, from imaging techniques to proteomics and biosensors.
GBM biomarkers and detection methods
Different biomarkers are used for different types of tumors. In GBM, nucleic acids, proteins, small molecules, microRNAs (miRNAs), circulating tumor cells (CTCs), extracellular vesicles, tumor tissues, and body fluids are commonly used [13,14,15]. Biofluid-based detection of glial tumors offers multiple approaches to improving the quality of life in patients with GBM [16]. Early detection of tumors using screening methods can delay the progression of tumor and increase the likelihood of successful treatment [17]. For example, in the more common malignancies such as breast and colon cancer, early discovery of solid tumors has been established through mammography and colonoscopy screenings, which has become a well-established clinical paradigm [18,19,20,21,22,23].
The analysis of malignant markers in biofluids was initially recognized in colorectal cancer, where elevated levels of serum carcinoembryonic antigen were detected [24,25,26]. However, the diagnostic importance of this normal physiological protein is limited, as its levels are not necessarily elevated and high ranges are associated with a variety of other cancers [25, 27]. Timely diagnosis and sensitive treatment monitoring remain major challenges in treating GBM [28]. Clinically, response assessment is primarily based on laboratory tests and magnetic resonance imaging (MRI) [28, 29]. However, both MRI and laboratory tests are insensitive measures of disease status. For example, the lowest reliable resolution detection by MRI is on the order of millimeters [28, 29]. Efforts to take advantage of the powerful imaging capabilities of MRI have led to alternative advances. Advanced MRI techniques such as diffusion-weighted imaging (DWI), dynamic contrast-enhanced perfusion imaging (DSC), and MR spectroscopy (MRS) are theorized to provide physiological information that cannot be obtained by conventional anatomical MRI alone. For example, proton-based MRS (or 1HMRS) provides information about metabolic composition within selected target tissue regions, conceptually similar to an “electronic biopsy”. Comparing the relative concentrations of these metabolites reveals factors that help assess the presence of viable tumors within the sample area, such as B cell membrane turnover and neuronal viability. MRS is more attractive than non-diagnostic techniques as it adds only 15 to 30 min to the traditional MRI technique routinely used in the management of patients with malignant glioma [30, 31]. Therefore, extracellular vesicles (EVs) are a reservoir biomarkers with great potential for assessing glioblastoma tumors in situ [30, 32]. Several molecular markers are still under investigation but are routinely used in GBM patients, including isocitrate dehydrogenase (IDH), O6-methylguanine DNA methyltransferase (MGMT), VEGF, and epidermal growth factor receptor (EGFR). In addition, tumor suppressor protein TP53, phosphatases, tensin homolog (PTEN), p16INK4a gene, phospholipid metabolites, cancer stem cells, and most recently, imaging biomarkers have all been extensively validated in clinical settings [33] (Table 1).
Proteomics
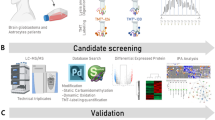
Proteomics-based platforms are becoming increasingly powerful in identifying potential disease mechanisms and biomarkers [53]. Proteomics involves using highly complex protein screening techniques for large-scale biological understanding [53]. This information can be combined with genomic data to achieve a better understanding of the underlying biological mechanisms in Guillain–Barré syndrome (GBS) [53, 54]. A typical sample pretreatment method for proteomics analysis is to digest proteins with proteases (such as trypsin or LysC) into peptides, separate them by reversed-phase C18 liquid chromatography, and analyze them using mass spectrometry (LCMS/MS) [55]. Figure 1 for a brief introduction to the proteomics technique.

Illustration of proteomics method [56]
Proteomics approaches can be readily employed to elucidate the natural production mechanisms of microorganisms and plants [57, 58]. This strategy has also been successfully applied to different types of diseases, such as periodontitis, Alzheimer’s disease, thyroid disease, and various types of tumors [59, 60]. In glioma, proteomics techniques have identified changes in protein expression, but the consistency and biological significance of these changes have not been established [61]. Many innovative proteomic studies are being conducted on several aspects of glioma immunotherapy, including oncolytic viruses, monoclonal antibodies, dendritic cell (DC) vaccines, and chimeric antigen receptor (CAR) T cells [61]. Therefore, the application of proteomics in immunotherapy may accelerate research into GBM treatment [61]. Human proteomic analysis based on clinical blood mass spectrometry (MS) is a powerful tool for studying cancer biomarkers [62]. Numerous clinical trials for GBM using various quantitative approaches have been reported in the last decade. Sequential window acquisition of all theoretical fragment ion spectra mass spectrometry (SWATH-MS) is a novel quantitative method that combines a highly specific data-independent acquisition (DIA) method with a novel targeted data extraction strategy to acquire the resulting fragment ion dataset [62]. SWATH-MS analysis offers several advantages in discovering proteomics, including the high reproducibility and reliable quantitative information [63]. By combining SWATHMS and QTAP analysis, eight candidate biomarkers were discovered in the plasma of GBM patients [64]. Mass spectrometry-based label-free quantitative proteomics has been developed to identify and characterize proteins that are differentially expressed in GBM to gain a better understanding of the interactions and functions that lead to disease states. Advanced identification of upstream regulators provides novel potential therapeutic targets. GBM tumors were analyzed by SDS PAGE fractions with internal DNA markers followed by liquid chromatography–tandem mass spectrometry (MS) [65]. The main challenge in GBM research has been identifying new molecular therapeutic targets and accurate diagnostic/prognostic biomarkers. Many current clinical therapeutic targets for immunotoxins and ligand-directed toxins against high-grade glioma cells (HGG) are surface sialylated glycoproteins [66]. A single-cell surface sialoprotein in human GBM tissue, human astrocytes, fetal and adult human neural progenitor cells (NPCs) was characterized and accurately quantified using a bioorthogonal chemistry reporter (BOCR) strategy combined with label-free quantitative mass spectrometry (LFQMS) were established for characterize and accurately quantify of GBM. This approach comprehensively identifies new biomarkers and therapeutic targets for treating malignant glioma using quantitative sialoglycoprotein proteomics with clinically relevant patient-derived primary glioma cells [66]. Additionally, a simple and sensitive targeted proteomic method was established to quantify membrane and protein transcription factors in the degenerated protein pathways of glioblastoma cells. This method utilized liquid chromatography and mass spectrometry assays to provide high detection sensitivity and quantitative data for prognostic analysis and efficacy testing [67]. The most malignant form of all gliomas is GBM, which is characterized by a poor response to treatment and a high degree of heterogeneity. The subventricular zone (SVZ) is a key site of brain neurogenesis and is rich in neural stem cells. Because GBM tumors are often located near the SVZ, they can be classified as either SVZ− or SVZ+. Tumors that are in close proximity to the SVZ are categorized as SVZ+, while tumors that are distant from SVZ are classified as SVZ−. To gain insight into the increased aggressiveness of SVZ+ tumors, proteomics systems such as LCMS/MS and 2DDIGE were applied to examine possible proteomics changes between the two subtypes. While serum proteomic analysis revealed significant changes in various lipid-carrying and acute phase proteins, tissue proteomic analysis showed significant changes in regulatory proteins, lipid binding, cytoskeleton, chaperones, and cell cycle. These results provide clues to the molecular basis behind the increased aggression of SVZ + GBM tumors and may lead to the identification of rational therapeutic targets for improving the treatment of these highly invasive tumors [68].
Real-time quantitative PCR (qRTPCR) and mass spectrometry (MS) were utilized to identify potential targets for long non-coding RNA (lncRNA) HULC that promote GBM progression [69, 70]. A proteomics-based approach in patient samples was used to identify T-cell target antigens in integrated glioblastoma stem cells. A novel immunogenic protein that frequently induces tumor-specific T-cell responses in GBM patients and is also detected in therapy-resistant, restless and slow-cycling GSCs in vitro was discovered in this study. The stable expression of these T cell targets in primary and recurrent GBM supports their suitability for future clinical applications [71].
The results suggest that proteomics involves the use of highly complex protein screening techniques that can be used for a large-scale biological understanding of GBM. This information can be combined with genomic data to provide a better understanding of the underlying biological mechanisms involved in GBM.
Biosensor technology
The monitoring and diagnosing various disorders require significant efforts to regularly test blood samples and conduct related tests [72,73,74]. However, these tests require common analytical techniques, efficient personnel to perform them, and time to collect the necessary samples for clinical trials [75]. Laboratory tests enable qualified personnel to monitor and diagnose a variety of diseases [73, 75]. Specific analytes are known to be specific to a particular disease and may be helpful in monitoring their progression [76, 77]. The clinical usefulness of biochemical tests is determined by their sensitivity to detect disease without false-negative results, and specificity to avoid false positives in individuals who are not ill [76]. Biosensors use the specificity of biomolecules in conjunction with physicochemical transducers to convert biological signals into optical/electrochemical signals [78]. Refer to Fig. 2 for a schematic of biosensor technology.

Schematic of biosensor technology
Numerous metabolite-based biosensors are available to monitor clinically essential parameters such as blood sugar, urea, uric acid, lactic acid, cholesterol, and more [56]. These biosensors are larger than the additional laboratory analysis of substances involved in the clinical analysis [72]. Enzymes are well known for developing biosensors due to their specificity as biological sensor materials and their role in clinical diagnostics has been known for several years. However, enzymes are less stable in solution and need to be immobilized and stabilized for use in biosensor devices [79]. The immobilized phase provides excellent stability and can be reused. Cross-linking, covalent binding, physisorption, encapsulation, and capture are some of the methods used to stabilize enzymes for developing biosensor devices [80]. The matrix or support selected for immobilization depends on the nature of the immobilization method and the biomolecule. Various matrices such as polymer films and carbon, graphite, membranes, gels, LB films, diaphoresis, and conductive polymers have been practiced to immobilize biomolecules/enzymes for developing various types of biosensors [80,81,82].
Developed biosensors for the detection of GBS biomarkers
This study produced a novel and sensitive electrogenic chemiluminescent (ECL) biosensor system for detecting the p16INK4a gene using a functional paste nanofiber composite-modified screen-printed carbon electrode (SPCE) [83]. Misfolded mutations in the DNA-binding domain of p53 affect its conformation and its ability to bind to chromatin, thereby affecting its ability to regulate target gene expression and cell cycle checkpoint function in many cancers, including GBM. Small molecule drugs that restore the structure and function of misfolded p53 may enhance chemotherapy by activating p53-mediated aging. To determine small molecule-mediated folding changes in the p53 protein a molecular complementation biosensor (NRLUCp53CRLUC) for split renilla-luciferase (RLUC) was constructed. After the initial evaluation of biosensors in three different cell lines, the constructed platform identified the p53P98L mutant endogenously in GBM cells [84]. Fluorescent resonance/Forster energy transfer (FRET) is a non-radiant energy transfer between two molecules that can occur when the two molecules are in close proximity (< 10 nm) [85, 86]. As a result, FRET can be used to measure whether two molecules, such as a ligand and a receptor, interact with each other [85, 86]. For FRET to occur, the fluorescence emission spectrum of the donor must overlap with the absorption spectrum of the acceptor, and the orientations of the transition dipoles must be approximately parallel [85, 86]. Refer to Fig. 3 for an illustration of the FRET-based method in the detection of protein–protein interactions.

Illustrates the FRET-based approach for detecting protein–protein interactions. Using FRET-based probes, glioma cells that invade the brain parenchyma have higher Rac1 and Cdc42 activity and lower RhoA activity than cells that penetrate the perivascular area. In other words, the FRET-based method was useful for monitoring the invasion mode of GBM cells. This can be controlled by balancing the activity of Rho-family GTPase and Cdc42-specific GEF
Electric cell-substrate impedance sensing (ECIS) is a label-free, real-time impedance-based technique for analyzing cell behavior based on cell adhesion [87]. Several research papers have shown that ECIS is appropriate and can measure GBM cell adhesion. Findings indicated that ECIS reliably measures the adhesion of the differentiated GBM cells on various array types. In addition, ECIS can measure the migration behavior of differentiated GBM cells on the ECIS electrode after alteration [88]. However, GBM stem cells are adhesive, ECIS has a significantly lower ability to measure adhesion compared to differentiated counterparts. This means that while ECIS can be useful for some GBM cultures, it may not be very useful for weakly adherent stem cells [88]. An electrochemical biosensor was developed to detect formaldehyde in aqueous solutions using the enzyme formaldehyde dehydrogenase coupled with a carbon nanotube (CNT) modified screen print electrode (SPE). The proposed system screens the amperometric response to formaldehyde released from U251 human GBM cells in a biosensor compartment in response to treatment with various anticancer prodrugs composed of formaldehyde and butyric acid [74, 89,90,91]. Surface plasmon polaritons (SPPs), also known as surface plasma waves, are a unique electromagnetic field mode that can appear at the interface between a dielectric and a metal. These SPPs behave almost exactly like a free electron plasma [92, 93]. Surface plasmons are characterized by their propagation constants and magnetic field distribution, and they are in transverse magnetic mode (magnetic vectors are perpendicular to the wave propagation direction and parallel to the interface) [92, 93]. Localized surface plasmon resonance (LSPR)-based biosensing provides a sensitive, unlabeled, inexpensive, and rapid method for detecting biomolecular interactions with nanoscale spatial resolution [94,95,96]. This technique has promising applications for the robust and sensitive detection of biomolecular interactions. The portability and small size of sensors allow for the miniaturization of sensors to scales not achievable with other planar methods, such as SPR. LSPR-based biosensing devices are easy to manufacture using inexpensive sensing platform. The usefulness of LSPR-based sensing can be enhanced by integrating it into multiplexed microfluidic devices [94, 95]. Refer to Fig. 4 for a schematic of the LSPR biosensor.

Schematic illustration of LSPR biosensor
In GBM, secreted lactate promotes the expression of differentiation cluster 44 (CD44) and the release of cell-derived nanovesicles (30–200 nm), such as exosomes, which promotes the malignant progression of tumors. In fatal brain tumors, lactate-driven upregulation of malignant glioblastoma cells (GM) promoted the release of CD44-rich exosomes, increased GM migration and endothelial cell formation, and secreted exosomes. It has been discovered that CD44 can be sensitized by the “capture” of titanium and identifiable by the LSPR biosensor (Refer to Fig. 5) [97].

This figure is adapted from Ref. [97]
This figure represents a highly sensitive method for detecting exosomal CD44 and CD133 by TIC-AFM and TiN–NH-LSPR biosensors to track the progression of GBM in mice. In the tumor microenvironment (TME), GBM cells utilize accumulated extracellular lactate for their survival, in part by upregulating CD44 and CD133, and releasing exosome. These exosomes not only make the cells more malignant but also enables neighboring ECs to become more angiogenic.
CDK5 kinase is activated through contact with various partners, including p35/p25 regulators. Active CDK5 plays a vital role in some neural functions, and its hyperactivity contributes to various human cancers and some neurodegenerative processes, especially neuroblastoma and GBM. A probe partner that interacts with CDK5 and a synthetic fluorescent quinolimide-tagged peptide derived from CDK5 calyx were implemented in vitro to detect N2a neuroblastoma and U87 GBM cells [98].
Surface-enhanced resonant Raman scattering (SERRS) is a sensitive and selective method for characterizing bio-molecular sites that exhibit electronic transitions at energies close to or consistent with the laser frequency used [99, 100]. Biomolecules are adsorbed on a suitable metal substrate, usually silver, and measurements are typically performed in situ in a buffer or support medium. This procedure has several advantages. Resonance sensitivity and surface-enhanced Raman scattering (SERS) sensitivity can be combined to enable the use of these methods for measuring nanoscale concentrations [99,100,101]. The detection of SE(R)RS nanoparticles using Raman spectroscopy-based imaging approach has significant advantages over other molecular contrast agent approaches [102]. For example, compared to fluorescence imaging, our SERRS nanoprobes not only have exhibit superior sensitivity but also have much higher photostability than current fluorochromes [102]. When excited by a single 785 nm excitation source, SERRS nanoparticles with different Raman reporters emits a complex spectrum [102,103,104]. The ability of integrin-targeted surface-enhanced resonance Raman spectroscopy (SERRS) nanoparticles to accurately depict the true tumor extent in a GBM mouse model that closely mimicking the pathology in humans was appropriately explored. This Raman spectroscopy-based nanoparticle imaging technology shows promise to enabling highly accurate visualization of the true extent of malignant brain tumors [102]. A fluorescent peptide reporter of CDK5 kinase activity derived from a library of CDK5-specific substrates, has been constructed. Its ability to respond to recombinant CDK5/p25 has been recognized and sensitive changes in fluorescence intensity report the CDK5 activity of glioblastoma cell extract. A cell-permeable variant of this biosensor has been further developed, which can be used to map CDK5 activation dynamics spatially and temporally. This offers an exciting opportunity to develop diagnostic assays for neuropathology associated with overactivated CDK5, and companion assays to assess responses to new therapies targeting this kinase [105]. A localized surface plasmon resonance (LSPR) sensor chip was developed to detect infinitesimal amount of exosomal biomarkers. The sensor chip utilized self-assembly silver nanoparticles decorated on gold nano-islands (Ag@AuNIs) sensor chip was used to provide site-specific bio-conjunction of biotinylated antibodies for detecting exosomal surface biomarkers [106, 107]. Additionally, a magnetic covalent organic framework nanospheres-based miRNA biosensor was created for sensitive glioma detection [108] (Table 2).
Comparisons of proteomics and biosensors technology in the identification of GBM
As previously mentioned, there are several ways to diagnose GBM, each with its own advantages and drawbacks. The primary objective of this study is to help guide the selection of an appropriate method for diagnosing GBM. To achieve this goal, this section compares proteomics and biosensing methods. Table 3 summarizes the advantages and disadvantages of proteomics and biosensors in identifying GBM.
Conclusion
Proteomics analysis is a valuable technique in GBM-related research for determining the interrelationships between intracellular proteins. It can provide both qualitative and quantitative information, identify the type of protein expressed, and investigate the phenotype of each expressed protein under different conditions. Similarly, biosensors are potent tools for diagnosing glioma. Validated studies have shown that using biosensors to identify biomarkers in body fluids is appropriate. Other techniques, such as MRI and proteomics, may be suitable for studying tumors, their structure, size, and morphology. In summary, biosensors play an important role in advancing GB sensors for fast, efficient, and inexpensive detection. Continued work and progress in large-scale plasmonic nanostructures is being achieved using various techniques such as microsphere lithography, fabrication of superparamagnetic particles, interference lithography, nanoimprinting, and new designs with improved performance. A more accurate reading method that reduces costs and enables easier testing with large area substrates, along with signal amplification is useful for SPR, LSPR, SEF, SERS, and SEIRA methods.
Availability of data and materials
Not applicable.
References
Kamran N, Alghamri MS, Nunez FJ, Shah D, Asad AS, Candolfi M, Altshuler D, Lowenstein PR, Castro MG. Current state and future prospects of immunotherapy for glioma. Immunotherapy. 2018;10(4):317–39.
Wen PY, Huse JT. 2016 World Health Organization classification of central nervous system tumors. CONTINUUM: Lifelong Learn Neurol. 2017;23(6):1531–47.
Alexander BM, Cloughesy TF. Adult glioblastoma. J Clin Oncol. 2017;35(21):2402–9.
Davis ME. Glioblastoma: overview of disease and treatment. Clin J Oncol Nurs. 2016;20(5):S2.
Stragliotto G, Pantalone MR, Rahbar A, Söderberg-Nauclér C. Valganciclovir as add-on to standard therapy in secondary glioblastoma. Microorganisms. 2020;8(10):1471.
Kleihues P, Ohgaki H. Primary and secondary glioblastomas: from concept to clinical diagnosis. Neuro Oncol. 1999;1(1):44–51.
Yousefi B, Mohammadlou M, Abdollahi M, Salek Farrokhi A, Karbalaei M, Keikha M, Kokhaei P, Valizadeh S, Rezaiemanesh A, Arabkari V. Epigenetic changes in gastric cancer induction by Helicobacter pylori. J Cell Physiol. 2019;234(12):21770–84.
Ellor SV, Pagano-Young TA, Avgeropoulos NG. Glioblastoma: background, standard treatment paradigms, and supportive care considerations. Los Angeles: SAGE Publications; 2014.
Shafiei M, Ghasemian A, Eslami M, Nojoomi F, Rajabi-Vardanjani H. Risk factors and control strategies for silicotuberculosis as an occupational disease. New Microbes New Infect. 2019;27:75–7.
Johnson DR, Fogh SE, Giannini C, Kaufmann TJ, Raghunathan A, Theodosopoulos PV, Clarke JL. Case-based review: newly diagnosed glioblastoma. Neuro-oncol Pract. 2015;2(3):106–21.
Young RM, Jamshidi A, Davis G, Sherman JH. Current trends in the surgical management and treatment of adult glioblastoma. Ann Transl Med. 2015;3(9):121.
Scribner EY. Mathematical modeling of brain tumors advances patient care, oncogenesis, and the use of in silico clinical trials. The University of Alabama at Birmingham; 2017.
Birkó Z, Nagy B, Klekner Á, Virga J. Novel molecular markers in glioblastoma-benefits of liquid biopsy. Int J Mol Sci. 2020;21(20):7522.
Zhou E, Li Y, Wu F, Guo M, Xu J, Wang S, Tan Q, Ma P, Song S, Jin Y. Circulating extracellular vesicles are effective biomarkers for predicting response to cancer therapy. EBioMedicine. 2021;67:103365–103365.
Amirsaadat S, Jafari-Gharabaghlou D, Dadashpour M, Zarghami N. Potential anti-proliferative effect of nano-formulated curcumin through modulating micro RNA-132, Cyclin D1, and hTERT genes expression in breast cancer cell lines. J Clust Sci. 2023. https://doi.org/10.1007/s10876-023-02404-z.
Krol I, Castro-Giner F, Maurer M, Gkountela S, Szczerba BM, Scherrer R, Coleman N, Carreira S, Bachmann F, Anderson S. Detection of circulating tumour cell clusters in human glioblastoma. Br J Cancer. 2018;119(4):487–91.
Figueroa JM, Carter BS. Detection of glioblastoma in biofluids. J Neurosurg. 2017;129(2):334–40.
Mogheri F, Jokar E, Afshin R, Akbari AA, Dadashpour M, Firouzi-amandi A, Serati-Nouri H, Zarghami N. Co-delivery of metformin and silibinin in dual-drug loaded nanoparticles synergistically improves chemotherapy in human non-small cell lung cancer A549 cells. J Drug Deliv Sci Technol. 2021;66:102752.
Ahmadi S, Dadashpour M, Abri A, Zarghami N. Long-term proliferation and delayed senescence of bone marrow-derived human mesenchymal stem cells on metformin co-embedded HA/Gel electrospun composite nanofibers. J Drug Deliv Sci Technol. 2023;80:104071.
Nejati K, Rastegar M, Fathi F, Dadashpour M, Arabzadeh A. Nanoparticle-based drug delivery systems to overcome gastric cancer drug resistance. J Drug Deliv Sci Technol. 2022;70:103231.
Eslami M, Yousefi B, Kokhaei P, Hemati M, Nejad ZR, Arabkari V, Namdar A. Importance of probiotics in the prevention and treatment of colorectal cancer. J Cell Physiol. 2019;234(10):17127–43.
Salek Farrokhi A, Mohammadlou M, Abdollahi M, Eslami M, Yousefi B. Histone deacetylase modifications by probiotics in colorectal cancer. J Gastrointest Cancer. 2020;51:754–64.
Ghorbani F, Kokhaei P, Ghorbani M, Eslami M. Application of different nanoparticles in the diagnosis of colorectal cancer. Gene Rep. 2020;21:100896.
Ota T, Sakashita K, Sawada R, Seki K, Maeda H, Tanaka N, Tsujinaka T. Long-term survival with nivolumab followed by irinotecan after total gastrectomy in alpha-fetoprotein-producing gastric cancer: a case report and review of the literature. Surgical Case Reports. 2023 Dec;9(1):1-8.
Aoki T, Kondo Y, Karakida K, Naito H, Kajiwara H, Ota Y. A mucinous adenocarcinoma of the lip with elevated serum carcinoembryonic antigen levels: a case report. Oral Maxillofac Surg. 2020;24(1):127–32.
Hemmati M, Yousefi B, Bahar A, Eslami M. Importance of heme oxygenase-1 in gastrointestinal cancers: functions, inductions, regulations, and signaling. J Gastrointest Cancer. 2021;52:454–61.
Salek Farrokhi A, Darabi N, Yousefi B, Askandar RH, Shariati M, Eslami M. Is it true that gut microbiota is considered as panacea in cancer therapy? J Cell Physiol. 2019;234(9):14941–50.
Sorensen AG, Batchelor TT, Wen PY, Zhang W-T, Jain RK. Response criteria for glioma. Nat Clin Pract Oncol. 2008;5(11):634–44.
Grossman SA, Batara JF. Current management of glioblastoma multiforme. Semin Oncol. 2004;31:635–44.
Hallal S, Azimi A, Wei H, Ho N, Lee MYT, Sim H-W, Sy J, Shivalingam B, Buckland ME, Alexander-Kaufman KL. A comprehensive proteomic SWATH-MS workflow for profiling blood extracellular vesicles: a new avenue for glioma tumour surveillance. Int J Mol Sci. 2020;21(13):4754.
Mondal A, Ashiq K, Phulpagar P, Singh DK, Shiras A. Effective visualization and easy tracking of extracellular vesicles in glioma cells. Biol Proced Online. 2019;21(1):1–12.
Liu H, Kang M, Wang J, Blenkiron C, Lee A, Wise M, Chamley L, Chen Q. Estimation of the burden of human placental micro-and nano-vesicles extruded into the maternal blood from 8 to 12 weeks of gestation. Placenta. 2018;72:41–7.
Carlsson SK, Brothers SP, Wahlestedt C. Emerging treatment strategies for glioblastoma multiforme. EMBO Mol Med. 2014;6(11):1359–70.
Li X, Feng Q, Jiang X. Microfluidic synthesis of Gd-based nanoparticles for fast and ultralong MRI signals in the solid tumor. Adv Healthc Mater. 2019;8(20):1900672.
Alves TR, Lima FRS, Kahn SA, Lobo D, Dubois LGF, Soletti R, Borges H, Neto VM. Glioblastoma cells: a heterogeneous and fatal tumor interacting with the parenchyma. Life Sci. 2011;89(15):532–9.
Akers JC, Ramakrishnan V, Kim R, Phillips S, Kaimal V, Mao Y, Hua W, Yang I, Fu C-C, Nolan J. miRNA contents of cerebrospinal fluid extracellular vesicles in glioblastoma patients. J Neurooncol. 2015;123(2):205–16.
Buruiană A, Florian ȘI, Florian AI, Timiș T-L, Mihu CM, Miclăuș M, Oșan S, Hrapșa I, Cataniciu RC, Farcaș M, et al. The roles of miRNA in glioblastoma tumor cell communication: diplomatic and aggressive negotiations. Int J Mol Sci. 2020;21(6):1950.
Brown HM, Pu F, Dey M, Miller J, Shah MV, Shapiro SA, Ouyang Z, Cohen-Gadol AA, Cooks RG. Intraoperative detection of isocitrate dehydrogenase mutations in human gliomas using a miniature mass spectrometer. Anal Bioanal Chem. 2019;411(30):7929–33.
Das A, Hawkins C, Tabori U. Germline predisposition to glial neoplasms in children and young adults: a narrative review. Glioma. 2021;4(4):68.
Suh CH, Kim HS, Jung SC, Choi CG, Kim SJ. Imaging prediction of isocitrate dehydrogenase (IDH) mutation in patients with glioma: a systemic review and meta-analysis. Eur Radiol. 2019;29(2):745–58.
Peng H, Huo J, Li B, Cui Y, Zhang H, Zhang L, Ma L. Predicting isocitrate dehydrogenase (IDH) mutation status in gliomas using multiparameter MRI radiomics features. J Magn Reson Imaging. 2021;53(5):1399–407.
Yekula A, Yekula A, Muralidharan K, Kang K, Carter BS, Balaj L. Extracellular vesicles in glioblastoma tumor microenvironment. Front Immunol. 2020;10:3137–3137.
Brevet M, Johnson ML, Azzoli CG, Ladanyi M. Detection of EGFR mutations in plasma DNA from lung cancer patients by mass spectrometry genotyping is predictive of tumor EGFR status and response to EGFR inhibitors. Lung Cancer. 2011;73(1):96–102.
González-Pérez L-V, Isaza-Guzmán D-M, Arango-Pérez E-A, Tobón-Arroyave S-I. Analysis of salivary detection of P16INK4A and RASSF1A promoter gene methylation and its association with oral squamous cell carcinoma in a Colombian population. J Clin Exp Dent. 2020;12(5):e452.
Hung K-S, Hong C-Y, Lee J, Lin S-K, Huang SC, Wang T-M, Tse V, Sliverberg GD, Weng S-C, Hsiao M. Expression of p16INK4A induces dominant suppression of glioblastoma growth in situ through necrosis and cell cycle arrest. Biochem Biophys Res Commun. 2000;269(3):718–25.
Morillon A-C, Yakkundi S, Thomas G, Gethings LA, Langridge JI, Baker PN, Kenny LC, English JA, McCarthy FP. Association between phospholipid metabolism in plasma and spontaneous preterm birth: a discovery lipidomic analysis in the cork pregnancy cohort. Metabolomics. 2020;16(2):1–10.
Nalli C, Somma V, Andreoli L, Büttner T, Schierack P, Mahler M, Roggenbuck D, Tincani A. Anti-phospholipid IgG antibodies detected by line immunoassay differentiate patients with anti-phospholipid syndrome and other autoimmune diseases. Autoimmun Highlights. 2018;9(1):1–11.
Rezaei MB, Alipour Astaneh SD. Lipid peroxidation inhibition, superoxide anion and nitric oxide radical scavenging properties of thymus daenensis and anethum graveolens essential oils. 2011.
Wang S, Ren W, Wang J, Jiang Z, Saeed M, Zhang L, Li A, Wu A. Black TiO 2-based nanoprobes for T 1-weighted MRI-guided photothermal therapy in CD133 high expressed pancreatic cancer stem-like cells. Biomat Sci. 2018;6(8):2209–18.
Lathia JD, Mack SC, Mulkearns-Hubert EE, Valentim CLL, Rich JN. Cancer stem cells in glioblastoma. Genes Dev. 2015;29(12):1203–17.
Juric D, Andre F, Singer CF, Sohn J, Campone M, Loibl S, Conte P, Iwata H, Ciruelos E, Mayer IA. Abstract P4–10–04: clinical outcomes of alpelisib in hormone receptor-positive, human epidermal growth factor receptor-2-negative advanced breast cancer by next-generation sequencing-detected PIK3CA alteration status and phosphatase and tensin homolog loss: biomarker analysis from the SOLAR-1 study. In: AACR; 2020.
Yang J-M, Schiapparelli P, Nguyen HN, Igarashi A, Zhang Q, Abbadi S, Amzel LM, Sesaki H, Quiñones-Hinojosa A, Iijima M. Characterization of PTEN mutations in brain cancer reveals that pten mono-ubiquitination promotes protein stability and nuclear localization. Oncogene. 2017;36(26):3673–85.
Dutt MJ, Lee KH. Proteomic analysis. Curr Opin Biotechnol. 2000;11(2):176–9.
Fredman G, Skov L, Mann M, Dyring-Andersen B. Towards precision dermatology: emerging role of proteomic analysis of the skin. Dermatology. 2022;238(2):185–94.
Hedrick VE, LaLand MN, Nakayasu ES, Paul LN. Digestion, purification, and enrichment of protein samples for mass spectrometry. Curr Protoc Chem Biol. 2015;7(3):201–22.
Mobed A, Ahmadalipour A, Fakhari A, Kazem SS, Saadi GK. Bioassay: a novel approach in antipsychotic pharmacology. Clin Chim Acta. 2020;509:30–5.
Tocmo R, Veenstra JP, Huang Y, Johnson JJ. Covalent modification of proteins by plant-derived natural products: proteomic approaches and biological impacts. Proteomics. 2021;21(3–4):1900386.
Sadeghzadeh J, Shahabi P, Farhoudi M, Ebrahimi-kalan A, Mobed A, Shahpasand K. Tau protein biosensors in the diagnosis of neurodegenerative diseases.
Gouveia D, Grenga L, Pible O, Armengaud J. Quick microbial molecular phenotyping by differential shotgun proteomics. Environ Microbiol. 2020;22(8):2996–3004.
Binti Badlishah Sham NI, Lewin SD, Grant MM. Proteomic investigations of in vitro and in vivo models of periodontal disease. PROTEOMICS—Clin Appl. 2020;14(3):1900043.
Chen L, Qin D, Guo X, Wang Q, Li J. Putting proteomics into immunotherapy for glioblastoma. Front Immunol. 2021;12:593255.
Jayaram S, Gupta MK, Polisetty RV, Cho WC, Sirdeshmukh R. Towards developing biomarkers for glioblastoma multiforme: a proteomics view. Expert Rev Proteomics. 2014;11(5):621–39.
Gautam P, Nair SC, Gupta MK, Sharma R, Polisetty RV, Uppin MS, Sundaram C, Puligopu AK, Ankathi P, Purohit AK. Proteins with altered levels in plasma from glioblastoma patients as revealed by iTRAQ-based quantitative proteomic analysis. PLoS ONE. 2012;7:e46153.
Miyauchi E, Furuta T, Ohtsuki S, Tachikawa M, Uchida Y, Sabit H, Obuchi W, Baba T, Watanabe M, Terasaki T. Identification of blood biomarkers in glioblastoma by SWATH mass spectrometry and quantitative targeted absolute proteomics. PLoS ONE. 2018;13(3):e0193799.
Heroux MS, Chesnik MA, Halligan BD, Al-Gizawiy M, Connelly JM, Mueller WM, Rand SD, Cochran EJ, LaViolette PS, Malkin MG, et al. Comprehensive characterization of glioblastoma tumor tissues for biomarker identification using mass spectrometry-based label-free quantitative proteomics. Physiol Genomics. 2014;46(13):467–81.
Autelitano F, Loyaux D, Roudieres S, Deon C, Guette F, Fabre P, Ping Q, Wang S, Auvergne R, Badarinarayana V. Identification of novel tumor-associated cell surface sialoglycoproteins in human glioblastoma tumors using quantitative proteomics. PLoS ONE. 2014;9(10):e110316.
Nguyen CDL, Malchow S, Reich S, Steltgens S, Shuvaev KV, Loroch S, Lorenz C, Sickmann A, Knobbe-Thomsen CB, Tews B, et al. A sensitive and simple targeted proteomics approach to quantify transcription factor and membrane proteins of the unfolded protein response pathway in glioblastoma cells. Sci Rep. 2019;9(1):8836.
Gollapalli K, Ghantasala S, Kumar S, Srivastava R, Rapole S, Moiyadi A, Epari S, Srivastava S. Subventricular zone involvement in Glioblastoma—A proteomic evaluation and clinicoradiological correlation. Sci Rep. 2017;7(1):1449.
Ye S, Wu J, Wang Y, Hu Y, Yin T, He J. Quantitative proteomics analysis of glioblastoma cell lines after lncRNA HULC silencing. Sci Rep. 2021;11(1):12587.
Gholizadeh O, Akbarzadeh S, Moein M, Yasamineh S, Hosseini P, Afkhami H, Amini P, Dadashpour M, Tahavvori A, Eslami M. The role of non-coding RNAs in the diagnosis of different stages (HCC, CHB, OBI) of hepatitis B infection. Microb Pathog. 2023;176:105995.
Rapp C, Warta R, Stamova S, Nowrouzi A, Geisenberger C, Gal Z, Roesch S, Dettling S, Juenger S, Bucur M, et al. Identification of T cell target antigens in glioblastoma stem-like cells using an integrated proteomics-based approach in patient specimens. Acta Neuropathol. 2017;134(2):297–316.
Chauhan N, Maekawa T, Kumar DNS. Graphene based biosensors—accelerating medical diagnostics to new-dimensions. J Mater Res. 2017;32(15):2860–82.
Mobed A, Razavi S, Ahmadalipour A, Shakouri SK, Koohkan G. Biosensors in Parkinson’s disease. Clin Chim Acta. 2021;518:51–8.
Eslami M, Peyghan AA. DNA nucleobase interaction with graphene like BC3 nano-sheet based on density functional theory calculations. Thin Solid Films. 2015;589:52–6.
Piunno PA, Krull UJ. Trends in the development of nucleic acid biosensors for medical diagnostics. Anal Bioanal Chem. 2005;381(5):1004–11.
Mascini M, Tombelli S. Biosensors for biomarkers in medical diagnostics. Biomarkers. 2008;13(7–8):637–57.
Aminabad ED, Mobed A, Hasanzadeh M, Feizi MAH, Safaralizadeh R, Seidi F. Sensitive immunosensing of α-synuclein protein in human plasma samples using gold nanoparticles conjugated with graphene: an innovative immuno-platform towards early stage identification of Parkinson’s disease using point of care (POC) analysis. RSC Adv. 2022;12(7):4346–57.
Sadighbathi S, Mobed A. Genosensors, a nanomaterial-based platform for microRNA-21 detection, non-invasive methods in early detection of cancer. Clin Chim Acta. 2022;530:27–38.
Huang X, Zhu Y, Kianfar E. Nano biosensors: properties, applications and electrochemical techniques. J Market Res. 2021;12:1649–72.
Zahirinejad S, Hemmati R, Homaei A, Dinari A, Hosseinkhani S, Mohammadi S, Vianello F. Nano-organic supports for enzyme immobilization: scopes and perspectives. Colloids Surf, B. 2021;204:111774.
Khan MR. Current and future role of immobilized enzymes in medical field. Curr Med Drug Res. 2021;5(1):1–9.
Izadi M, Tahmasebi S, Pustokhina I, Yumashev AV, Lakzaei T, Alvanegh AG, Roshangar L, Dadashpour M, Yousefi M, Ahmadi M. Changes in Th17 cells frequency and function after ozone therapy used to treat multiple sclerosis patients. Mult Scler Relat Disord. 2020;46:102466.
Wang X, Wang Y, Shan Y, Jiang M, Jin X, Gong M, Xu J. A novel and sensitive electrogenerated chemiluminescence biosensor for detection of p16INK4a gene based on the functional paste-like nanofibers composites-modified screen-printed carbon electrode. J Electroanal Chem. 2018;823:368–77.
Paulmurugan R, Afjei R, Sekar TV, Babikir HA, Massoud TF. A protein folding molecular imaging biosensor monitors the effects of drugs that restore mutant p53 structure and its downstream function in glioblastoma cells. Oncotarget. 2018;9(30):21495–511.
Wu L, Huang C, Emery BP, Sedgwick AC, Bull SD, He X-P, Tian H, Yoon J, Sessler JL, James TD. Förster resonance energy transfer (FRET)-based small-molecule sensors and imaging agents. Chem Soc Rev. 2020;49(15):5110–39.
Kaur A, Kaur P, Ahuja S. Förster resonance energy transfer (FRET) and applications thereof. Anal Methods. 2020;12(46):5532–50.
Wegener J, Keese CR, Giaever I. Electric cell–substrate impedance sensing (ECIS) as a noninvasive means to monitor the kinetics of cell spreading to artificial surfaces. Exp Cell Res. 2000;259(1):158–66.
Robilliard LD, Yu J, Jun S-M, Anchan A, Finlay G, Angel CE, Graham ES. Can ECIS biosensor technology be used to measure the cellular responses of glioblastoma stem cells? Biosensors. 2021;11(12):498.
Bareket L, Rephaeli A, Berkovitch G, Nudelman A, Rishpon J. Carbon nanotubes based electrochemical biosensor for detection of formaldehyde released from a cancer cell line treated with formaldehyde-releasing anticancer prodrugs. Bioelectrochemistry. 2010;77(2):94–9.
Eslami M, Vahabi V, Peyghan AA. Sensing properties of BN nanotube toward carcinogenic 4-chloroaniline: a computational study. Physica E. 2016;76:6–11.
Yang Y, Sun A, Eslami M. A density functional theory study on detection of amphetamine drug by silicon carbide nanotubes. Physica E. 2021;125:114411.
Singh P. SPR biosensors: historical perspectives and current challenges. Sens Actuators, B Chem. 2016;229:110–30.
Nguyen HH, Park J, Kang S, Kim M. Surface plasmon resonance: a versatile technique for biosensor applications. Sensors. 2015;15(5):10481–510.
Cottat M, Thioune N, Gabudean A-M, Lidgi-Guigui N, Focsan M, Astilean S, Lamy de la Chapelle M. Localized surface plasmon resonance (LSPR) biosensor for the protein detection. Plasmonics. 2013;8(2):699–704.
Hall WP, Ngatia SN, Van Duyne RP. LSPR biosensor signal enhancement using nanoparticle−antibody conjugates. J Phys Chem C. 2011;115(5):1410–4.
Eslami M, Moradi M, Moradi R. DFT investigation of hydrogen adsorption on the C3N nanotube. Vacuum. 2016;133:7–12.
Thakur A, Xu C, Li WK, Qiu G, He B, Ng S-P, Wu C-ML, Lee Y. In vivo liquid biopsy for glioblastoma malignancy by the AFM and LSPR based sensing of exosomal CD44 and CD133 in a mouse model. Biosens Bioelectron. 2021;191:113476.
Fueyo-González F, Herranz R, Plesselova S, Giron MD, Salto R, Paredes JM, Orte A, Morris MC, González-Vera JA. Quinolimide-based peptide biosensor for probing p25 in vitro and in living cells. Sens Actuators, B Chem. 2021;339:129929.
Campion A, Kambhampati P. Surface-enhanced Raman scattering. Chem Soc Rev. 1998;27(4):241–50.
Corio P, Brown S, Marucci A, Pimenta M, Kneipp K, Dresselhaus G, Dresselhaus M. Surface-enhanced resonant Raman spectroscopy of single-wall carbon nanotubes adsorbed on silver and gold surfaces. Phys Rev B. 2000;61(19):13202.
Yasamineh S, Yasamineh P, Kalajahi HG, Gholizadeh O, Yekanipour Z, Afkhami H, Eslami M, Kheirkhah AH, Taghizadeh M, Yazdani Y. A state-of-the-art review on the recent advances of niosomes as a targeted drug delivery system. Int J Pharm. 2022;624:121878.
Huang R, Harmsen S, Samii JM, Karabeber H, Pitter KL, Holland EC, Kircher MF. High precision imaging of microscopic spread of glioblastoma with a targeted ultrasensitive SERRS molecular imaging probe. Theranostics. 2016;6(8):1075.
Harmsen S, Huang R, Wall MA, Karabeber H, Samii JM, Spaliviero M, White JR, Monette S, O’Connor R, Pitter KL. Surface-enhanced resonance Raman scattering nanostars for high-precision cancer imaging. Sci Transl Med. 2015;7(271):271ra277-271ra277.
Amirazad H, Dadashpour M, Zarghami N. Application of decellularized bone matrix as a bioscaffold in bone tissue engineering. J Biol Eng. 2022;16(1):1–18.
Peyressatre M, Laure A, Pellerano M, Boukhaddaoui H, Soussi I, Morris MC. Fluorescent biosensor of CDK5 kinase activity in glioblastoma cell extracts and living cells. Biotechnol J. 2020;15(9):1900474.
Liu L, Thakur A, Kar Li W, Qiu G, Yang T, He B, Lee Y, Lawrence Wu C-M. Site specific biotinylated antibody functionalized Ag@AuNIs LSPR biosensor for the ultrasensitive detection of exosomal MCT4, a glioblastoma progression biomarker. Chem Eng J. 2022;446:137383.
Dadashpour M, Firouzi-Amandi A, Pourhassan-Moghaddam M, Maleki MJ, Soozangar N, Jeddi F, Nouri M, Zarghami N, Pilehvar-Soltanahmadi Y. Biomimetic synthesis of silver nanoparticles using Matricaria chamomilla extract and their potential anticancer activity against human lung cancer cells. Mater Sci Eng, C. 2018;92:902–12.
Liang D, Zhang X, Wang Y, Huo T, Qian M, Xie Y, Li W, Yu Y, Shi W, Liu Q, et al. Magnetic covalent organic framework nanospheres-based miRNA biosensor for sensitive glioma detection. Bioact Mater. 2022;14:145–51.
Hirata E, Yukinaga H, Kamioka Y, Arakawa Y, Miyamoto S, Okada T, Sahai E, Matsuda M. In vivo fluorescence resonance energy transfer imaging reveals differential activation of Rho-family GTPases in glioblastoma cell invasion. J Cell Sci. 2012;125(Pt 4):858–68.
Hamdan M, Righetti PG. Modern strategies for protein quantification in proteome analysis: advantages and limitations. Mass Spectrom Rev. 2002;21(4):287–302.
Srzentić K, Fornelli L, Laskay UA, Monod M, Beck A, Ayoub D, Tsybin YO. Advantages of extended bottom-up proteomics using Sap9 for analysis of monoclonal antibodies. Anal Chem. 2014;86(19):9945–53.
Conrotto P, Souchelnytskyi S. Proteomic approaches in biological and medical sciences: principles and applications. Exp Oncol. 2008;30:171–80.
Li X, Chen N, Zhou X, Gong P, Wang S, Zhang Y, Zhao Y. A review of specialty fiber biosensors based on interferometer configuration. J Biophotonics. 2021;14(6):e202100068.
Kucherenko I, Soldatkin O, Dzyadevych S, Soldatkin A. Electrochemical biosensors based on multienzyme systems: main groups, advantages and limitations—a review. Anal Chim Acta. 2020;1111:114–31.
Plekhanova YV, Reshetilov A. Microbial biosensors for the determination of pesticides. J Anal Chem. 2019;74(12):1159–73.
Acknowledgements
The authors would like to thank the stem cell Research Center of Tabriz University of Medical Sciences.
Funding
The authors did not receive support from any organization for the submitted work.
Author information
Authors and Affiliations
Contributions
AH and HA: Conceptualization Writing—original draft preparation, FR and IA: Writing—review and editing, VA, BH, YY: Writing—review and editing. MD, ME and FG, Supervision, conceptualization, funding acquisition, reviewing and editing. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors have no relevant financial or non-financial interests to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Hosseini, A., Ashraf, H., Rahimi, F. et al. Recent advances in the detection of glioblastoma, from imaging-based methods to proteomics and biosensors: A narrative review. Cancer Cell Int 23, 98 (2023). https://doi.org/10.1186/s12935-023-02947-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12935-023-02947-1