
Abstract
Background
Diabetic peripheral neuropathy (DPN) is the most prevalent complication of diabetes, and has been demonstrated to be independently associated with cardiovascular events and mortality. This aim of this study was to investigate the subclinical left ventricular (LV) myocardial dysfunction in type 2 diabetes mellitus (T2DM) patients with and without DPN.
Methods
One hundred and thirty T2DM patients without DPN, 61 patients with DPN and 65 age and sex-matched controls who underwent cardiovascular magnetic resonance (CMR) imaging were included, all subjects had no symptoms of heart failure and LV ejection fraction ≥ 50%. LV myocardial non-infarct late gadolinium enhancement (LGE) was determined. LV global strains, including radial, circumferential and longitudinal peak strain (PS) and peak systolic and diastolic strain rates (PSSR and PDSR, respectively), were evaluated using CMR feature tracking and compared among the three groups. Multivariable linear regression analyses were performed to determine the independent factors of reduced LV global myocardial strains in T2DM patients.
Results
The prevalence of non-infarct LGE was higher in patients with DPN than those without DPN (37.7% vs. 19.2%, p = 0.008). The LV radial and longitudinal PS (radial: 36.60 ± 7.24% vs. 33.57 ± 7.30% vs. 30.72 ± 8.68%; longitudinal: − 15.03 ± 2.52% vs. − 13.39 ± 2.48% vs. − 11.89 ± 3.02%), as well as longitudinal PDSR [0.89 (0.76, 1.05) 1/s vs. 0.80 (0.71, 0.93) 1/s vs. 0.77 (0.63, 0.87) 1/s] were decreased significantly from controls through T2DM patients without DPN to patients with DPN (all p < 0.001). LV radial and circumferential PDSR, as well as circumferential PS were reduced in both patient groups (all p < 0.05), but were not different between the two groups (all p > 0.05). Radial and longitudinal PSSR were decreased in patients with DPN (p = 0.006 and 0.003, respectively) but preserved in those without DPN (all p > 0.05). Multivariable linear regression analyses adjusting for confounders demonstrated that DPN was independently associated with LV radial and longitudinal PS (β = − 3.025 and 1.187, p = 0.014 and 0.003, respectively) and PDSR (β = 0.283 and − 0.086, p = 0.016 and 0.001, respectively), as well as radial PSSR (β = − 0.266, p = 0.007).
Conclusions
There was more severe subclinical LV dysfunction in T2DM patients complicated with DPN than those without DPN, suggesting further prospective study with more active intervention in this cohort of patients.
Similar content being viewed by others
Explore related subjects
Find the latest articles, discoveries, and news in related topics.Background
The substantial global increase in the incidence of diabetes has led to a parallel increase in the rates of diabetes-related deaths and complications [1, 2]. Diabetic peripheral neuropathy (DPN) involving the outer nerves of the limbs is one of the most common complications of diabetes and affects over 50% of patients with type 2 diabetes mellitus (T2DM) [3]. In addition, it has been demonstrated to be independently associated with cardiovascular events and mortality in a number of studies [4,5,6]. Therefore, early detection of myocardial impairment in this cohort of patients is essential to prevent progression and subsequent increases in morbidity and mortality.
Current screening methods for diabetic cardiomyopathy mainly rely on left ventricular ejection fraction (LVEF) measurements that are based on global ventricular volume measurements, whether using echocardiography or CMR, which have inherent limitations, as they can only detect moderate to severe cardiac dysfunction. Interestingly, a large body of published data has shown that the echocardiography speckle tracking and cardiovascular magnetic resonance feature tracking (CMR-FT) techniques can detect and monitor the progression of subclinical myocardial dysfunction, which can further predict cardiovascular events [7, 8]. Although echocardiography is currently the most convenient method for cardiac examination, it has a low spatial resolution and is highly dependent on the operator and angle, making it unsuitable for some patients with a poor echo window. CMR-FT, which is derived from a cine balanced steady-state free precession (bSSFP) sequence, has the advantages of a wide field of view, no anatomical plane restriction, and a semiautomatic and time-saving postprocessing procedure. In addition, late gadolinium enhancement (LGE) is a most advantage of MRI compared to the echocardiography, which is used to assess myocardial tissue characteristics [9, 10].
Therefore, the aim of this study was to evaluate subclinical left ventricular (LV) myocardial dysfunction in type 2 diabetes mellitus (T2DM) patients with and without DPN using CMR-FT. The results might provide additional information on the link between the risk of cardiovascular disease and DPN.
Methods
Study population
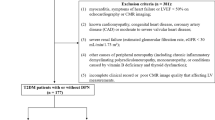
Between January 2015 and June 2023, T2DM patients who had undergone CMR examinations were initially screened. T2DM was diagnosed according to the current American Diabetes Association guideline [11]. DPN was clinically diagnosed using the diagnostic criteria introduced by the American Diabetes Association in 2017 [12]. Chronic kidney disease (CKD) is clinically defined by the presence of persistent estimated glomerular filtration rate (eGFR) < 60 mL/min/1.73 m2. The exclusion criteria included patients with coronary artery disease (confirmed by electrocardiogram, echocardiography, angiography, coronary computed tomographic angiography or CMR, or previous myocardial infarction or coronary revascularization), symptoms of heart failure, left ventricular ejection fraction < 50% on echocardiography or CMR imaging, other primary cardiomyopathies, moderate to severe valvular disease, atrial fibrillation, severe renal failure (eGFR < 30 mL/min/1.73 m2), other causes of peripheral neuropathy (including chronic inflammatory demyelinating polyradiculoneuropathy, mononeuropathy, or conditions caused by vitamin B deficiency and thyroid dysfunction), incomplete clinical records and poor CMR image quality inadequate for analysis. Finally, 191 patients with T2DM were enrolled in this study, including 130 patients without DPN (75 males and 55 females, mean age 56.5 ± 9.7 years) and 61 patients with DPN (38 males and 23 females, mean age 55.3 ± 10.2). In addition, 65 age- and sex-matched healthy individuals (34 males and 31 females; mean age, 55.4 ± 9.9 years) were enrolled as the control group. The inclusion criteria for the control group were as follows: no diabetes or impaired glucose tolerance, hypertension, ischemic heart disease, cardiomyopathy, abnormal electrocardiogram, abnormalities detected with CMR (abnormal ventricular motion, valvular stenosis or regurgitation, decreased LVEF, etc.) or other cardiovascular disease-related symptoms.
This study (No. 2019-878) was approved by the Biomedical Research Ethics Committees of our hospital and complied with the Declaration of Helsinki. Written informed consent was waived due to the retrospective nature of the study.
CMR protocol
All subjects underwent CMR imaging on a 3 T whole-body scanner MAGNETOM Skyra or Trio Tim (Siemens Medical Solutions, Erlangen, Germany) in the supine position. The balanced steady-state free precession sequence (repetition time [TR] = 3.4 ms or 2.81 ms, echo time [TE] = 1.22 ms, flip angle = 50° or 40°, slice thickness = 8 mm, field of view [FOV] = 340 × 285 mm or 250 × 300 mm, matrix size = 256 × 166 or 208 × 139) with breath holding and ECG triggering was performed to acquire cine images, including a stack of contiguous short-axis slices covering the entire left ventricle from base to apex and one four- and two-chamber long-axis slice. Twenty-five frames were reconstructed per breath-hold acquisition. The LGE images in the entire LV short-axis stack and from the two-, three- and four-chamber views were acquired to exclude patients with infarct LGE and identify those with non-infarct LGE 10–15 min after contrast agent administration using the segmented-turbo-FLASH–phase-sensitive inversion recovery sequence (TR/TE, 300 ms/1.44 ms or 750 ms/1.18 ms, slice thickness, 8 mm, FOV, 275 × 400 mm or 400 × 270 mm, matrix size = 256 × 184 and flip angle, 40°).
Image analysis
All CMR data were uploaded to offline commercial software (Cvi42, v.5.11.2; Circle Cardiovascular Imaging, Inc., Calgary, Canada) and analyzed by two experienced radiologists with more than five years of experience in CMR interpretation, who were blinded to the clinical data.
The endo- and epicardial contours of left ventricle were semiautomatically delineated at the end-diastolic and end-systolic phases on the short-axis cine images in the Short-3D module. The papillary muscles and moderator bands were included in the ventricular cavity and excluded from the myocardial muscle. The global parameters of LV geometry and function, including end-diastolic volume (EDV), end-systolic volume (ESV), stroke volume (SV), LVEF and LV mass, were computed automatically; LVEDV, LVESV, LVSV and LV mass were indexed to the body surface area (BSA) (LVEDVI, LVESVI, LVSVI and LVMI, respectively). The LV remodeling index was calculated as the ratio of LV mass to LVEDV.
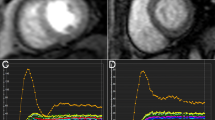
The short-axis and long-axis four- and two-chamber cine images were loaded into the tissue tracking module for the LV myocardial strain analysis. The endo- and epicardial contours were semiautomatically delineated with papillary muscles and moderator bands excluded in all series at the end-diastolic phase. Subsequently, the LV global strain parameters (Fig. 1) were acquired automatically, including global radial, circumferential and longitudinal peak strain (PS) and peak systolic and diastolic strain rates (PSSR and PDSR, respectively). PS was defined as the relative thickening, shortening and lengthening of the myocardium from end diastole (reference phase). PSSR and PDSR are defined as the maximum strain rate during the contraction and relaxation phases, respectively.

Representative CMR left ventricular pseudocolor images of long-axis two- and four-chamber images at the end-systole and CMR-derived global longitudinal peak strain (GLS) curves in a normal control (A1–A3), T2DM patient without DPN (B1–B3) and T2DM patient complicated with DPN (C1–C3)
For late gadolinium enhancement (LGE) analysis, the LGE images were visually evaluated by two observers in combination and categorized into 3 patterns, that is none, infarct, or non-infarct patterns [13].
Statistical analysis
All continuous variables were assessed for normality with the Shapiro–Wilk test. Continuous variables are presented as the means ± standard deviations (SD) for normally distributed variables or the medians (25–75% interquartile ranges) for skewed variables. Comparisons between three groups were performed with one-way analysis of variance (ANOVA) with the post hoc Bonferroni correction for normally distributed variables and Kruskal–Wallis tests for variables with skewed distributions. The duration of T2DM and HbA1c levels were compared between the patient groups with Mann–Whitney U test. Categorical variables are presented as percentages and were compared using Chi-square tests. Variables with p < 0.1 in the univariable analysis, as well as age, sex and diabetes duration were included in the stepwise multivariable linear regression analyses to determine the predictors of LV systolic and diastolic function in patients with T2DM. The diabetic duration was divided into long (> 5 years) and short (≤ 5 years) term duration which were included in the univariable and multivariable analysis. Two-tailed p values < 0.05 were considered statistically significant, and statistical analyses were performed with SPSS version 23.0 (IBM, Armonk, New York, USA).
Results
Baseline characteristics
The main clinical characteristics of the study cohort are shown in Table 1. Although age was not significantly different between the patient groups, patients with DPN had a longer diabetes duration (p = 0.003) and higher incidences of dyslipidemia (63.9% vs. 42.3%, p = 0.008), retinopathy (29.5% vs. 4.6%, p < 0.001) and CKD (24.6% vs. 12.3%, p = 0.037) than those without DPN. As expected, both patient groups showed higher fasting blood glucose levels than the control group (all p < 0.001), and patients with DPN had significantly higher HbA1c levels than those without DPN (p = 0.001). In addition, BMI, mean SBP and DBP were significantly higher in patients with or without DPN than in controls (all p < 0.05), but they were not significantly different between the patient groups.
No significant differences in the use of medications were observed between patient groups except for statins and insulin, which were most frequently used in patients with DPN (p = 0.006 and < 0.001, respectively).
Characteristics of LV geometry and strain parameters
The CMR findings for the study cohort are shown in Table 2. T2DM patients without and with DPN had a larger LV mass than the control group (p = 0.007 and 0.002, respectively), and the differences were present even after adjustment for BSA (p = 0.006 and 0.001, respectively). The LV remodeling index in the patient groups without and with DPN was significantly higher than that in the control group (p = 0.034 and = 0.017 respectively). Besides, the prevalence of non-infarct LGE was significantly higher in subjects with DPN compared with those without DPN (37.7% vs. 19.2%, p = 0.008). The LVEDV, LVEDVI, LVESV, LVESVI, LVSV, LVSVI and LVEF were not significantly different among the three groups (all p > 0.05).
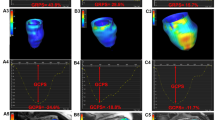
Regarding the strain parameters (Fig. 2), the LV radial and longitudinal PS, as well as longitudinal PDSR were decreased progressively from controls through T2DM patients without DPN to patients with DPN (all p < 0.001). LV radial and circumferential PDSR, as well as circumferential PS were reduced in both patient groups (all p < 0.05), but were not significantly different between these groups (all p > 0.05). In addition, radial and longitudinal PSSR were decreased in patients with DPN (p = 0.006 and 0.003, respectively) but preserved in patients without DPN (all p > 0.05).

Comparion of left ventricular global strain parameters among controls, T2DM (DPN−) and T2DM (DPN+) groups. GRS global radial peak strain, GCS global circumferential peak strain, GLS global longitudinal peak strain, PSSR peak systolic strain rate, PDSR peak diastolic strain rate, R radial, C circumferential, L longitudinal, T2DM type 2 diabetes mellitus, DPN diabetic peripheral neuropathy
Determinants of subclinical LV dysfunction in T2DM patients
After univariable linear regression analyses (Tables 3 and 4), DPN was significantly associated with all three directions of LV global PS (all p < 0.05), radial and longitudinal PSSR and PDSR (all p < 0.1). Retinopathy was significantly associated with radial and longitudinal PS and PDSR, as well as radial and circumferential PSSR (all p < 0.05). Dyslipidemia was significantly associated with radial PS, PSSR and PDSR (all p < 0.05). In addition, LGE was significantly associated with all directions of LV global PS (all p ≤ 0.001), PSSR (p < 0.05) and PDSR (p < 0.1) except circumferential PSSR (p = 0.655). Results of other univariable analyses are shown in the tables.
Multivariable linear regression analyses adjusting for confounders demonstrated that DPN was independently associated with LV radial and longitudinal PS (β = − 3.030 and 1.187, p = 0.014 and 0.003, respectively) and PDSR (β = 0.281 and − 0.086, p = 0.016 and 0.001, respectively), as well as radial PSSR (β = − 0.266, p = 0.007). CKD was independently associated with LV longitudinal PS (β = 1.045, p = 0.042). Dyslipidemia was independently associated radial PS, PSSR and PDSR (β = 3.773, 0.212 and -0.450, all p < 0.05). Additionally, LGE was independently associated with radial, circumferential and longitudinal PS (β = − 4.070, 1.401 and 2.020, all p ≤ 0.002), radial and longitudinal PSSR (β = − 0.266 and 0.103, p = 0.012 and < 0.001, respectively), and longitudinal PDSR (β = − 0.076, P = 0.014).
Discussion
Assessment of myocardial deformation by strain and strain rate is sensitive to detect subclinical myocardial systolic and diastolic dysfunction, in which PS and PSSR reflect myocardial systolic function, while PDSR is a sensitive marker of LV diastolic dysfunction. In T2DM patients without complicated DPN, we observed increases in LV myocardial mass and remodeling index and decreases in three directional PS and PDSR compared with the controls, but no significant differences in LVEDVI, LVESVI, LVSVI and LVEF among the groups. These findings indicate that LV myocardial systolic and diastolic function measured by CMR-FT were impaired at the early stage before the reduction of LVEF, which was consistent with previous studies [14, 15]. In addition, the presence of LGE indicating myocardial fibrosis was also observed in these patients. Taken together, detection of early alternations in the LV myocardium enable early intervention and implementation of preventative strategies in T2DM patients.
In diabetes, hyperglycemia and lipotoxicity related to insulin resistance may lead to suppressed glucose oxidation, increased free fatty acid metabolism, inadequate calcium handling, mitochondrial dysfunction, increased oxidative stress, interstitial and perivascular fibrosis, and cardiomyocyte hypertrophy and stiffness, which may contribute to reduced ventricular compliance at the early stage [16, 17]. A recent meta-analysis including a large number of patients (n = 5053) showed that diabetes was associated with a higher degree of myocardial fibrosis assessed by histological collagen volume fraction and extracellular volume fraction [18], and previous studies have detected diastolic dysfunction in the diabetic hearts without hypertrophy [19, 20]. With the aggravation of aforementioned pathologies along with impairment in excitation–contraction coupling, microvascular abnormalities manifesting as microvascular endothelial inflammation, rarefaction and perivascular collagen, and end-product deposition, and increased LV wall thickness and mass may lead to systolic dysfunction [21, 22]. Some studies have demonstrated an adverse effect of T2DM on subclinical LV systolic strains and myocardial microvascular impairment [23, 24].
Further analysis in our patients revealed that the magnitude of LV radial and longitudinal PS as well as longitudinal PDSR were markedly lower in patients with DPN than in both controls and patients without DPN, and radial and longitudinal PSSR were reduced in patients with DPN but preserved in those without DPN. However, the LV geometry was not significantly different between the patient groups. In addition, we identified that DPN was independently associated with the magnitude of LV radial and longitudinal PS and PDSR, as well as radial PSSR after adjustment for confounding factors. Thus, we speculated that subclinical LV dysfunction was progressed in T2DM patients with DPN even without progressive alterations in LV geometry, which was consistent with previous speckle-tracking echocardiography study [25]. Subendocardial myocardial fibers predominantly affected by coronary microvascular dysfunction are impaired early and severer, then manifesting as independent association between DPN and LV longitudinal PS and PDSR. The results that DPN was not associated with circumferential PS and PDSR indicate subepicardial myocardial impairment was not decreased progressively in our patients with DPN. Because both subendocardial and subepicardial fibers contribute to LV radial function[26], decreased LV radial PS and PDSR may mainly be caused by impaired subendocardial fibers when circumferential function was not progressively decreased.
Several studies have shown that the main mechanisms involved in DPN are longstanding hyperglycemia, dyslipidemia and insulin resistance, which may cause common pathophysiological changes in multiple organs, such as mitochondrial dysfunction, oxidative stress, accumulation of advanced glycation end products, lipotoxicity, increased inflammatory cytokine synthesis and microvascular complications [3, 27, 28]. Myocardial dysfunction may be involved when these changes occur in the heart. An elevated HbA1c level is a known cardiovascular risk factor and associated with higher degrees of myocardial fibrosis [18], its reduction will lead to reduced risks of both macro- and microvascular disease [29]. Our results revealed higher HbA1c levels in patients with DPN, indicating poor glycemic control, higher metabolic disorder and myocardial fibrosis; however, it was not associated with myocardial dysfunction. A potential explanation for this discrepancy is that HbA1c levels may not be a good indicator of long-term glycemic control, as it only reflects glycemic control over the past 3–4 months. Besides, we found that patients with DPN had a higher incidence of dyslipidemia and it was independently associated with worsening LV radial PS, PSSR and PDSR, which may indicate that determining the pathophysiological mechanisms underlying the effect of dyslipidemia will provide mechanistic targets for developing new targeted therapies for DPN and related myocardial dysfunction.
A previous study revealed that microvascular alterations, similar to those observed in diabetic retinopathy and nephropathy, appear to be associated with pathological alterations of nerves [30], which may lead to reduced peripheral nerve nutrition and impaired nerve function. Chung et al. reported a more frequent prevalence of retinopathy in patients with T2DM presenting peripheral neuropathy [31], and it was consistent with our findings. Reduced flow in the left anterior descending artery was observed in patients with retinopathy [32]. The study by Sørensen et al. reported a decrease in myocardial perfusion reserve in patients with retinopathy that was associated with diastolic dysfunction [33]. According to our results, the retinopathy and CKD were significantly associated with LV myocardial dysfunction. Zhang et al. demonstrated that kidney dysfunction may aggravate the deterioration of LV strain in T2DM patients [34], and another study revealed that the LV global longitudinal strain is a superior predictor of all-cause and cardiovascular mortality when compared with ejection fraction in advanced CKD patients [35]. In addition, the study by Baltzis et al. showed that patients with DPN had a higher risk of myocardial ischemia than those without DPN using technetium-99 m sestamibi single-photon emission computed tomographic imaging [36], which was consistent with our finding that patients with DPN had higher proportion of non-infarct LGE indicating severer microvascular dsyfunction [37]. These observations suggest that the common mechanism of microvascular impairment in diabetic complications plays an important role in myocardial dysfunction in patients with DPN. It is highly stimulating developing future targeted medications improving microvascular function to improve prognosis in T2DM patients; for example, glucagon-like peptide-1(GLP-1) has been shown to have benefits for patients with microvascular complication [38].
LGE could be used as a surrogate for replacement fibrosis and very little is known regarding nonischemic LGE implications in T2DM patients [39]. In the present study, we found a high prevalence of non-infarct LGE in T2DM patients and even higher proportion in those with DPN, and it was independently associated with worsening LV systolic (three directional PS as well as radial ad longitudinal PSSR) and diastolic (longitudinal PDSR) dysfunction. A previous study showed that T2DM patients with non-ischemic LGE lesions had increased ECV [39], and a recent study revealed that coronary microvascular dysfunction was significantly associated with the development of myocardial fibrosis in patients with T2DM [40]. Considering higher prevalence of non-infarct LGE in patients with DPN, they may have severer myocardial structural and functional impairment in T2DM with DPN, which may explain the poor cardiac outcomes in these patients.
Limitations
There are several limitations in our study. Firstly, this was a retrospective, single-center, observational study involving a relatively limited sample size, which may introduce selection bias and limit the ability to establish causality. Therefore, a prospective, multicenter study is desirable to validate our results. Secondly, we only included diabetic patients without heart failure and preserved LVEF, the generalizability of our findings to patients with heart failure is worth to be further investigated. Thirdly, Although LGE is the technique of choice for diagnosis of replacement fibrosis, it cannot evaluate diffuse myocardial fibrosis. Native and postcontrast T1-mapping can assess the extent and distribution of diffuse myocardial fibrosis, however, it was not available in our series and will be implemented in our further studies. Furthermore, not all the patients underwent nerve conduction tests, and selection bias may exist because subclinical DPN with no signs or symptoms of neuropathy could not be diagnosed. However, our data reflect routine clinical practice in diagnosing DPN, and further studies are required to explore LV changes in patients with subclinical DPN. Finally, the inherent cross-sectional design of this study prevented us from drawing conclusions on causality. Long-term longitudinal studies are needed to investigate the ability of impaired LV strains and non-infarct LGE to predict cardiovascular outcomes in patients complicated with DPN.
Conclusions
There was more non-infarct LGE lesions and worsening subclinical LV dysfunction in T2DM patients complicated with DPN than those without DPN, which may suggest further prospective study with even more extensive therapeutic interventions in this cohort of patients to improve patient outcomes.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- T2DM:
-
Type to diabetes mellitus
- DPN:
-
Diabetic peripheral neuropathy
- LV:
-
Left ventricular
- CMR:
-
Cardiovascular magnetic resonance
- CMR-FT:
-
CMR feature tracking
- EDV:
-
End-diastolic volume
- ESV:
-
End-diastolic volume
- SV:
-
Stroke volume
- CO:
-
Cardiac output
- EF:
-
Ejection fraction
- LVMI:
-
LV mass index
- PS:
-
Peak strain
- PSSR:
-
Peak systolic strain rates
- PDSR:
-
Peak diastolic strain rates
- LGE:
-
Late gadolinium enhancement
References
Saeedi P, Petersohn I, Salpea P, Malanda B, Karuranga S, Unwin N, et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: results from the International Diabetes Federation Diabetes Atlas, 9(th) edition. Diabetes Res Clin Pract. 2019;157: 107843.
van Dieren S, Beulens JW, van der Schouw YT, Grobbee DE, Neal B. The global burden of diabetes and its complications: an emerging pandemic. Eur J Cardiovasc Prev Rehabil. 2010;17(Suppl 1):S3-8.
Feldman EL, Callaghan BC, Pop-Busui R, Zochodne DW, Wright DE, Bennett DL, et al. Diabetic neuropathy. Nat Rev Dis Primers. 2019;5(1):41.
Forsblom CM, Sane T, Groop PH, Totterman KJ, Kallio M, Saloranta C, et al. Risk factors for mortality in Type II (non-insulin-dependent) diabetes: evidence of a role for neuropathy and a protective effect of HLA-DR4. Diabetologia. 1998;41(11):1253–62.
Margariti A. Peripheral neuropathy may be a potential risk of cardiovascular disease in diabetes mellitus. Heart. 2014;100(23):1823–4.
Brownrigg JR, Davey J, Holt PJ, Davis WA, Thompson MM, Ray KK, et al. The association of ulceration of the foot with cardiovascular and all-cause mortality in patients with diabetes: a meta-analysis. Diabetologia. 2012;55(11):2906–12.
Pedrizzetti G, Claus P, Kilner PJ, Nagel E. Principles of cardiovascular magnetic resonance feature tracking and echocardiographic speckle tracking for informed clinical use. J Cardiovasc Magn Reson. 2016;18(1):51.
Kalam K, Otahal P, Marwick TH. Prognostic implications of global LV dysfunction: a systematic review and meta-analysis of global longitudinal strain and ejection fraction. Heart. 2014;100(21):1673–80.
Zulet P, Islas F, Ferrandez-Escarabajal M, Bustos A, Cabeza B, Gil-Abizanda S, et al. Diabetes mellitus is associated to high-risk late gadolinium enhancement and worse outcomes in patients with nonischemic dilated cardiomyopathy. Cardiovasc Diabetol. 2024;23(1):35.
Wang J, Li Y, Guo YK, Huang S, Shi R, Yan WF, et al. The adverse impact of coronary artery disease on left ventricle systolic and diastolic function in patients with type 2 diabetes mellitus: a 3.0T CMR study. Cardiovasc Diabetol. 2022;21(1):30.
Chamberlain JJ, Rhinehart AS, Shaefer CF Jr, Neuman A. Diagnosis and management of diabetes: synopsis of the 2016 American Diabetes Association Standards of Medical Care in Diabetes. Ann Intern Med. 2016;164(8):542–52.
Pop-Busui R, Boulton AJ, Feldman EL, Bril V, Freeman R, Malik RA, et al. Diabetic neuropathy: a position statement by the American Diabetes Association. Diabetes Care. 2017;40(1):136–54.
Schulz-Menger J, Bluemke DA, Bremerich J, Flamm SD, Fogel MA, Friedrich MG, et al. Standardized image interpretation and post-processing in cardiovascular magnetic resonance—2020 update: Society for Cardiovascular Magnetic Resonance (SCMR): Board of Trustees Task Force on Standardized Post-Processing. J Cardiovasc Magn Reson. 2020;22(1):19.
Yan WF, Xu HY, Jiang L, Zhang L, Guo YK, Li Y, et al. Early longitudinal changes in left ventricular function and morphology in diabetic pigs: evaluation by 3.0T magnetic resonance imaging. Cardiovasc Diabetol. 2023;22(1):6.
Zhou S, Zhang Z, Zhang Z, Gao Y, Li G, Lou M, et al. Evaluation of left ventricular systolic and diastolic function in subjects with prediabetes and diabetes using cardiovascular magnetic resonance-feature tracking. Acta Diabetol. 2022;59(4):491–9.
Miki T, Yuda S, Kouzu H, Miura T. Diabetic cardiomyopathy: pathophysiology and clinical features. Heart Fail Rev. 2013;18(2):149–66.
Grigorescu ED, Lacatusu CM, Floria M, Mihai BM, Cretu I, Sorodoc L. Left ventricular diastolic dysfunction in type 2 diabetes-progress and perspectives. Diagnostics. 2019;9(3):121.
Salvador DB, Gamba MR, Gonzalez-Jaramillo N, Gonzalez-Jaramillo V, Raguindin PFN, Minder B, et al. Diabetes and myocardial fibrosis: a systematic review and meta-analysis. JACC: Cardiovasc Imaging. 2022;15(5):796–808.
Schannwell CM, Schneppenheim M, Perings S, Plehn G, Strauer BE. Left ventricular diastolic dysfunction as an early manifestation of diabetic cardiomyopathy. Cardiology. 2002;98(1–2):33–9.
Ha JW, Lee HC, Kang ES, Ahn CM, Kim JM, Ahn JA, et al. Abnormal left ventricular longitudinal functional reserve in patients with diabetes mellitus: implication for detecting subclinical myocardial dysfunction using exercise tissue Doppler echocardiography. Heart. 2007;93(12):1571–6.
Cao Y, Zeng W, Cui Y, Kong X, Wang M, Yu J, et al. Increased myocardial extracellular volume assessed by cardiovascular magnetic resonance T1 mapping and its determinants in type 2 diabetes mellitus patients with normal myocardial systolic strain. Cardiovasc Diabetol. 2018;17(1):7.
Oka S, Kai T, Hoshino K, Watanabe K, Nakamura J, Abe M, et al. Effects of empagliflozin in different phases of diabetes mellitus-related cardiomyopathy: a prospective observational study. BMC Cardiovasc Disord. 2021;21(1):217.
Li XM, Jiang L, Guo YK, Ren Y, Han PL, Peng LQ, et al. The additive effects of type 2 diabetes mellitus on left ventricular deformation and myocardial perfusion in essential hypertension: a 3.0 T cardiac magnetic resonance study. Cardiovasc Diabetol. 2020;19(1):161.
Liu X, Yang ZG, Gao Y, Xie LJ, Jiang L, Hu BY, et al. Left ventricular subclinical myocardial dysfunction in uncomplicated type 2 diabetes mellitus is associated with impaired myocardial perfusion: a contrast-enhanced cardiovascular magnetic resonance study. Cardiovasc Diabetol. 2018;17(1):139.
Chen Y, Wang Y, Zhang Y, Li M, Zhang W, Zhou Y, et al. Association of peripheral neuropathy with subclinical left ventricular dysfunction in patients with type 2 diabetes. J Diabetes Complic. 2023;37(2): 108406.
Claus P, Omar AMS, Pedrizzetti G, Sengupta PP, Nagel E. Tissue tracking technology for assessing cardiac mechanics: principles, normal values, and clinical applications. JACC Cardiovasc Imaging. 2015;8(12):1444–60.
Rumora A, Kim B, Feldman EL. A role for fatty acids in peripheral neuropathy associated with type 2 diabetes and prediabetes. Antioxid Redox Signal. 2022;37(7–9):560–77.
Roustit M, Loader J, Deusenbery C, Baltzis D, Veves A. Endothelial dysfunction as a link between cardiovascular risk factors and peripheral neuropathy in diabetes. J Clin Endocrinol Metab. 2016;101(9):3401–8.
Stratton IM, Adler AI, Neil HA, Matthews DR, Manley SE, Cull CA, et al. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study. BMJ. 2000;321(7258):405–12.
Giannini C, Dyck PJ. Ultrastructural morphometric abnormalities of sural nerve endoneurial microvessels in diabetes mellitus. Ann Neurol. 1994;36(3):408–15.
Chung JO, Cho DH, Chung DJ, Chung MY. Association between diabetic polyneuropathy and cardiovascular complications in type 2 diabetic patients. Diabetes Metab J. 2011;35(4):390–6.
Akasaka T, Yoshida K, Hozumi T, Takagi T, Kaji S, Kawamoto T, et al. Retinopathy identifies marked restriction of coronary flow reserve in patients with diabetes mellitus. J Am Coll Cardiol. 1997;30(4):935–41.
Sorensen MH, Bojer AS, Broadbent DA, Plein S, Madsen PL, Gaede P. Cardiac perfusion, structure, and function in type 2 diabetes mellitus with and without diabetic complications. Eur Heart J Cardiovasc Imaging. 2020;21(8):887–95.
Zhang Y, Wang J, Ren Y, Yan WF, Jiang L, Li Y, et al. The additive effects of kidney dysfunction on left ventricular function and strain in type 2 diabetes mellitus patients verified by cardiac magnetic resonance imaging. Cardiovasc Diabetol. 2021;20(1):11.
Reboldi G, Krishnasamy R, Isbel NM, Hawley CM, Pascoe EM, Burrage M, et al. Left ventricular global longitudinal strain (GLS) Is a superior predictor of all-cause and cardiovascular mortality when compared to ejection fraction in advanced chronic kidney disease. PLoS ONE. 2015;10(5): e0127044.
Baltzis D, Roustit M, Grammatikopoulou MG, Katsaboukas D, Athanasiou V, Iakovou I, et al. Diabetic peripheral neuropathy as a predictor of asymptomatic myocardial ischemia in type 2 diabetes mellitus: a cross-sectional study. Adv Ther. 2016;33(10):1840–7.
Li XM, Shi R, Shen MT, Yan WF, Jiang L, Min CY, et al. Subclinical left ventricular deformation and microvascular dysfunction in T2DM patients with and without peripheral neuropathy: assessed by 3.0 T cardiac magnetic resonance imaging. Cardiovasc Diabetol. 2023;22(1):256.
Ishibashi Y, Matsui T, Takeuchi M, Yamagishi S. Glucagon-like peptide-1 (GLP-1) inhibits advanced glycation end product (AGE)-induced up-regulation of VCAM-1 mRNA levels in endothelial cells by suppressing AGE receptor (RAGE) expression. Biocheml Biophys Res Commun. 2010;391(3):1405–8.
Bojer AS, Sorensen MH, Vejlstrup N, Goetze JP, Gaede P, Madsen PL. Distinct non-ischemic myocardial late gadolinium enhancement lesions in patients with type 2 diabetes. Cardiovasc Diabetol. 2020;19(1):84.
Zhao W, Li K, Tang L, Zhang J, Guo H, Zhou X, et al. Coronary microvascular dysfunction and diffuse myocardial fibrosis in patients with type 2 diabetes using quantitative perfusion MRI. J Magn Reson Imaging. 2024. https://doi.org/10.1002/jmri.29296.
Acknowledgements
Not applicable.
Funding
This work was supported by grants from the National Natural Science Foundation of China (82371925, 81971586, 81771887, 821201080 and 82202115) and 1·3·5 project for disciplines of excellence, West China Hospital, Sichuan University (ZYGD23019).
Author information
Authors and Affiliations
Contributions
XML, KS and LJ contributed to the study design, data analysis and manuscript writing. XML, JW, WFY, YG and MTS were responsible for collecting, sorting and analyzed the data. RS, GZ and XJL participated in editing and review of the manuscript. YKG and ZGY participated in the study design and revised the manuscript. All authors read and approved the final version of submitted manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Biomedical Research Ethics Committee of our hospital approved this study (No. 2019-878), which was performed in accordance with the Declaration of Helsinki. Written informed consent have been waived owing to the retrospective nature of this study.
Consent for publication
Not applicable.
Competing interests
The authors declare that there are no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Li, XM., Shi, K., Jiang, L. et al. Assessment of subclinical LV myocardial dysfunction in T2DM patients with diabetic peripheral neuropathy: a cardiovascular magnetic resonance study. Cardiovasc Diabetol 23, 217 (2024). https://doi.org/10.1186/s12933-024-02307-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12933-024-02307-x