
Abstract
Background
Stroke has been found to be highly correlated with the triglyceride-glucose (TyG) index. The relation between the TyG index changes and stroke, however, has seldom been reported, and current researches mentioning the TyG index concentrate on individual values. We aimed to investigate whether the level and the change of TyG index was associated with the incidence of stroke.
Methods
Sociodemographic, medical background, anthropometric and laboratory information were retrospectively collected. Classification was conducted using k-means clustering analysis. Logistic regressions were to determine the relationship between different classes with changes in the TyG index and incidence of stroke, taking the class with the smallest change as a reference. Meanwhile, restricted cubic spline regression was applied to examine the links of cumulative TyG index and stroke.
Results
369 (7.8%) of 4710 participants had a stroke during 3 years. Compared to class 1 with the best control of the TyG Index, the OR for class 2 with good control was 1.427 (95% CI, 1.051–1.938), the OR for class 3 with moderate control was 1.714 (95% CI, 1.245–2.359), the OR for class 4 with worse control was 1.814 (95% CI, 1.257–2.617), and the OR for class 5 with consistently high levels was 2.161 (95% CI, 1.446–3.228). However, after adjusting for multiple factors, only class 3 still had an association with stroke (OR 1.430, 95%CI, 1.022-2.000). The relation between the cumulative TyG index and stroke was linear in restricted cubic spline regression. In subgroup analysis, similar results were shown in participants without diabetes or dyslipidemia. There is neither additive nor multiplicative interaction between TyG index class and covariates.
Conclusion
A constant higher level with worst control in TyG index indicated a higher risk of stroke.
Similar content being viewed by others


Introduction
Insulin resistance (IR), a new risk factor for stroke, is considered to be an early manifestation of type 2 diabetes, which is present not only in diabetes but also in many non-diabetic patients [1]. It is closely related to risk factors for cerebrovascular disease, such as atherosclerosis, hypertension, atrial fibrillation, coronary heart disease and type 2 diabetes [2,3,4,5].
There are a number of methods to assess IR and the gold standard is the hyperinsulinemic glucose clamp (HEC) [6]. But HEC requires intravenous infusion of glucose and insulin and multiple blood samples [7]. The procedure is complex and costly and is not widely used in clinical practice. HOMA-IR (Homeostasis model assessment of IR) is widely used and has been shown to be effective in predicting the occurrence of cardiovascular and cerebrovascular diseases [7,8,9,10,11,12]. However, it is necessary to measure fasting insulin levels in patients, which is of limited clinical use. The triglyceride-glucose (TyG) index, as a simple alternative surrogate of IR, is easily obtained from clinical laboratory test results and is associated with the occurrence and recurrence of stroke. Further research has shown that the TyG index is superior to HOMA-IR in predicting stroke [13, 14].
Nevertheless, there are fewer studies dealing with change of TyG index and stroke incidence. This article aimed to evaluate whether the level and the change in TyG index predicted the incidence of stroke using data from the “China Health and Retirement Longitudinal Study (CHARLS)”.
Methods
Study population
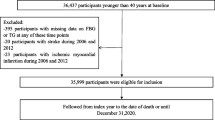
CHARLS is a nationally representative longitudinal survey of the middle-aged and older population (≥ 45 years) conducted by the National School of Development at Peking University. Detailed information on the study population has been reported in other publications [15]. To date, the nationwide baseline study has been conducted in 2011–2012, with Wave 2 in 2013, Wave 3 in 2015 and Wave 4 in 2018. Blood samples were also collected at baseline (including 11,847 participants) and wave 3 (including 13,420 participants). For this analysis, participants had to be aged 45 years and older. Complete data on fast blood glucose (FBG) and triglycerides (TG) were required. People were excluded if they had had a stroke before 2015. 4,710 respondents had complete data in both 2012 and 2015 in this cohort (68.7%) and were considered eligible to participate finally (Fig. 1).

Flowchart of the study population
Data assessment
The change of TyG index and stroke
Stroke was the main outcome of this study. Individuals who self-reported “yes” to the question of “Have you been diagnosed with stroke by a doctor?” or had specific answers with questions of “Treat stroke by Take Chinese Traditional Medicine/Take Western Modern Medicine/Physical Therapy/Acupuncture and Moxibustion/Occupational Therapy/None of the Above” were regarded as people with stroke.
The exposure of this study was the change of TyG index respectively collected in 2012 and 2015. The TyG index was calculated by the formula ln[TG (mg/dl) × FBG (mg/dl)/2] [16]. The cumulative TyG index was determined by the expression: (TyG2012 + TyG2015)/2*time(2015−2012) [17].
Data collection
Baseline demographic information (age, sex, Hukou, education and marital status), basic anthropometric measurements (systolic blood pressure (SBP), diastolic blood pressure (DBP) and body mass index (BMI)) and potential risk factors (hypertension, diabetes, dyslipidemia, heart problems, smoking status and alcohol drinking status) were reviewed. Primary prevention included antihypertensive treatments, lipid-lowering treatments and hypoglycaemic treatments. Laboratory examination contained fast blood glucose (FBG), total cholesterol (TC), triglyceride (TG), high-density lipoprotein cholesterol (HDL), low-density lipoprotein cholesterol (LDL) and glycosylated Hemoglobin, Type A1c (HbA1c) [18].
Statistical analysis
The data set of the 3-year transition of the TyG index was analyzed and classified into 5 classes using K-means clustering. K-means clustering is a technique that has the goal of dividing N observations into K clusters. Each observation is assigned to the cluster with the closest mean value, which serves as the prototype of the cluster. As the number of categorized classes was increased, the maximum number of classes recruited was 5, with each class containing no less than two data. When the number of clusters equaled to 5, the effect of k-means clustering was better than others. Further categorization into final classes was performed for each of the 5 classes that met the criteria below: Class 1, the TyG index was from 8.01 in 2012 to 8.14 in 2015, representing better control of TyG index; Class 2, the TyG index was from 8.64 in 2012 to 8.41 in 2015, representing good control of TyG index; Class 3, the TyG index was from 8.68 in 2012 to 9. 17 in 2015, representing moderate control of TyG index; class 4, the TyG index was from 9.48 in 2012to 8.93 in 2015, from high level to low level, representing worse control for its higher cumulative TyG index than class 3; class 5, the TyG index was from 9.88 in 2012 to 9.93 in 2015, representing worst and terrible control of TyG index (Fig. 2).
Descriptive statistics (means and standard deviations, SD, for continuous data and percentages for categorical data) were used to report basic characteristics. The t-test or Mann-Whitney U test for continuous variables and the chi-squared test or Fisher’s exact test for categorical variables were used to analyze differences in baseline characteristics between classes. Univariate and multivariate logistic regression analysis were performed with factors important for stroke incidence. A restricted cubic spline model was then carried out for examining the shape of the correlation between cumulative TyG index and stroke. We chose four knots at 20th, 40th, 60th and 80th. Also, we performed several subgroup analyses and interaction analysis to discover potential impact factors. The relative excess risk due to interaction (RERI), the attributable proportion due to interaction (AP) and the synergy index (SI) were utilized to evaluate the additive interaction. The effects of interaction analysis between TyG index classes and covariate were reported by ORs (95%CI). Statistical analyses were performed using R version 4.0.3 software (http://www.R-project.org/). Two-sided P < 0.05 was considered statistically significant.

The TyG index clustering by k-means clustering
Results
Baseline characteristics of study participants
This study included 4,710 participants with an average age of 58.73 ± 8.88 years and 44.48% males. The mean TyG index was 8.67 ± 0.64 in 2012 and 8.68 ± 0.62 in 2015 and the mean cumulative TyG index was 26.02 ± 1.69. Compared with class 1, participants in the other classes had fewer current smokers and drinkers, higher BMI, SBP and DBP, a higher prevalence of hypertension, diabetes, dyslipidemia and heart disease, and had higher FBG, TC, TG, LDL, HbA1 levels and lower HDL levels (Table 1).
Odds ratios for incident stroke
After 3 years, 369 (7.8%) participants had developed a stroke (Table 2). Comparing to class 1, the ORs for incident stroke were 1.427 (1.051, 1.938) for class 2, 1.714 (1.245, 2.359) for class 3, and 1.814 (1.257, 2.617) for class 4. It was interesting that class 3 and class 4 had approximate TyG index but different tendency, and class 4 had a higher risk of stroke than class 3. Class 5, with the worst control of TyG index, had the highest risk to develop new-onset stroke (OR:2.161, 95% CI, 1.446, 3.228), even though both class 1 and class 5 had elevating TyG index. With adjustment for sex, age, education, marital status, Hukou, smoking status, drinking status, SBP, DBP, BMI, history of hypertension, diabetes, dyslipidemia, heart disease, antihypertensive treatments, lipid-lowering treatments and hypoglycemic treatments (model 3), only class 3 had an increased risk (OR:1.423, 95% CI, 1.017, 1.992). In the restricted cubic spline regression models, the correlation between cumulative TyG index and risk of incident stroke was linear shown in Fig. 3 (P = 0.250). The risk of stroke was increasing with each increase in the cumulative TyG index above 27.64 (OR 1.002, 95% CI, 0.807, 1.246). And with the raising of the cumulative TyG index over 28.20 (OR 1.538, 95% CI, 0.932, 2.538) in class 4 and over 30.66 (OR 1.003, 95% CI, 0.442, 2.276) in class 5, participants were more likely to have an incidence of stroke.

Cubic model of the association between different classes and cumulative TyG index after adjusting for sex, age, education, marital status, Hukou, smoking status, drinking status, SBP, DBP, BMI, history of hypertension, dyslipidemia, diabetes, heart disease, antihypertensive treatments, lipid-lowering treatments and hypoglycemic treatments
Subgroup analyses
We performed subgroup analysis to stratify the relevance between the change in the TyG index and stroke as shown in Table 3. Younger male participants with agriculture Hukou were at-risk population. A positive association was found in patients without diabetes, dyslipidemia or heart disease. No interaction was found between TyG index classes and subgroup variables (Table 4). The SI of education level or marital status in addictive interaction analysis was null because of meaningless statistical value.
Discussion
We discovered from the CHARLS national data that adults over 45 had a greater risk of stroke with a constant and high TyG index. In subgroup analysis, though, patients with diabetes or dyslipedia did not exhibit the association.
Our findings were consistent with other researches that found a linear relationship between the TyG index and the incidence of stroke. In 2020, Shi revealed the independent correlation between the TyG index and ischemic stroke in the general population and indicated that this relationship was linear for the first time [19]. Subsequently, a large prospective cohort study involving patients with acute ischemic stroke showed that TyG index was associated with stroke recurrence [20]. Our restricted cubic spline model revealed the relevance between cumulative TyG and stroke, similar to Cui’s study [17]. Another study also mentioned about change of TyG index, but the change of TyG index was calculated by the TyG index minus that at baseline. They revealed that changes in TyG index independently predicted stroke [21]. However, patients with similar cumulative TyG index may lead to different prognosis like class 3 and class 4 in this study. Studies in patients with hypertension had also shown the same conclusion, and there was no gender difference [22]. An increase in the TyG index was an independent predictor of ischemic stroke in the general population [23, 24]. However, Yang showed that the TyG index was not an efficient predictor of adverse prognosis of cardiovascular and cerebrovascular diseases in non-diabetic patients receiving percutaneous coronary intervention [2]. A meta-analysis included seven cohort studies including participants from Spain, Argentina, China, South Korea and Iran assessed the association between the TyG index and incidence of cardiovascular and cerebrovascular events due to arterial atherosclerosis, and showed that TyG index might be independently related to stroke [25]. In 2022, a meta-analysis involving 11 studies yielded the same results [26].
In model 3 of the multivariate regression analysis, except for class 3, the relationship between classes and stroke risk become insignificant, but the lower limit of the confidence interval was closely to 1. There was a possibility that the results may be positive with an increase in the sample size. In the population with diabetes and dyslipidemia, there was no significant association between each class and the incidence of stroke in the subgroup analysis. The possible reason was that hypoglycemic and lipid-lowering treatments interfered with determining TyG. It was speculated that the use of hypoglycemic and lipid-lowering drugs may be beneficial in preventing the risk of stroke. In subgroup analysis, positive relationship remained in participants without diabetes and dyslipidemia.
The mechanism of insulin resistance leading to stroke has not been clarified, which mainly has the following possibilities: First, insulin resistance leads to endothelial dysfunction, the formation of foam cells and vulnerable plaques, which plays an important role in atherosclerosis. Previous studies have revealed that the TyG index is link with atherosclerosis in the general population [27, 28] and is an independent predictor of plaque progression [29,30,31,32]. At the same time, insulin resistance, as a low-grade inflammatory state, accelerates the progress of atherosclerosis and leads to the synthesis of more inflammatory markers [33, 34]. Second, insulin resistance affects platelet adhesion, activation, and aggregation [35,36,37,38,39], leading to stroke through arterial stenosis or occlusion. Third, insulin resistance seems to be associated with increased sympathetic nervous system activity [16] and impaired cardiac autonomic nervous function [19], which is related to the pathogenesis of acute cardiovascular and cerebrovascular diseases. Fourth, with insulin resistance are more likely to have a high waist circumference, BMI, hypertension, diabetes, cardiovascular disease and dyslipidemia history, and a high level of fasting blood glucose, triglycerides, and glycosylated hemoglobin, all of which are exact risk factors for stroke [19,20,21, 23, 24].
To the best of our knowledge, this is the first study to use cluster analysis to classify changes in the TyG index. Each category represented a different population, with participants with good control having the lowest risk and patients with worst control having the highest risk. In previous studies, the prediction of stroke was mostly based on one value of the TyG index, but the value was different on the other day. The second is that our research population was a representative sample of healthy people from all over the China. Our research focused on dynamic processes and added evidence to the relationship between the TyG index and stroke.
Our study had several limitations. Firstly, although the TyG index was a reliable and convenient surrogate of insulin resistance and had been shown to correlate significantly with HEC and HOMA-IR, this study did not compare the TyG index with the gold standard for insulin resistance and cannot directly explain the relationship between insulin resistance and stroke. Secondly, there may be a bias due to the exclusion of individuals without complete fasting glucose and triglyceride data. Thirdly, there were only two blood tests, and a more detailed development of the TyG index cannot be obtained. Fourthly, the study population was all from China, and the results cannot be extrapolated to other countries.
Conclusions
In the present study, we observed that participants with higher baseline TyG index and a change of elevating TyG index may suffer an increased incidence of stroke. Hence, people with a higher TyG index and poor TyG index control, especially in those without diabetes and dyslipidemia, should pay attention to stroke prevention.
Data Availability
Online repositories contain the datasets used in this investigation. The names of the repository/ repositories and accession number(s) can be found at: http://charls.pku.edu.cn/en.
Abbreviations
- BMI:
-
Body mass index
- CI:
-
Confidence interval
- HDL:
-
Low-density lipoprotein cholesterol
- LDL-C:
-
Low-density lipoprotein cholesterol
- OR:
-
Odds ratio
- TC:
-
Total cholesterol
- TG:
-
Triglyceride
- TyG:
-
Triglyceride-glucose.
References
Kernan WN, et al. Impaired insulin sensitivity among nondiabetic patients with a recent TIA or ischemic stroke. Neurology. 2003;60(9):1447–51.
Yang J, et al. The impact of the triglyceride-glucose index on poor prognosis in NonDiabetic patients undergoing percutaneous coronary intervention. Front Endocrinol (Lausanne). 2021;12:710240.
Zhao Q, et al. Comparison of various insulin resistance surrogates on prognostic prediction and stratification following percutaneous coronary intervention in patients with and without type 2 diabetes mellitus. Cardiovasc Diabetol. 2021;20(1):190.
Chen CL, et al. Association between triglyceride glucose index and risk of New-Onset diabetes among chinese adults: findings from the China Health and Retirement Longitudinal Study. Front Cardiovasc Med. 2020;7:610322.
Shi W, et al. Usefulness of triglyceride-glucose index for detecting prevalent atrial fibrillation in a type 2 diabetic population. Postgrad Med. 2022;134(8):820–8.
Guerrero-Romero F, et al. The product of triglycerides and glucose, a simple measure of insulin sensitivity. Comparison with the euglycemic-hyperinsulinemic clamp. J Clin Endocrinol Metab. 2010;95(7):3347–51.
Smith GI, Mittendorfer B, Klein S. Metabolically healthy obesity: facts and fantasies. J Clin Invest. 2019;129(10):3978–89.
Jing J, et al. Insulin resistance and prognosis of nondiabetic patients with ischemic stroke: the ACROSS-China Study (abnormal glucose regulation in patients with Acute Stroke across China). Stroke. 2017;48(4):887–93.
Cai X, et al. Association between prediabetes and risk of all cause mortality and cardiovascular disease: updated meta-analysis. BMJ. 2020;370:m2297.
Chang Y, et al. Insulin resistance is associated with poor functional outcome after acute ischemic stroke in non-diabetic patients. Sci Rep. 2021;11(1):1229.
Ago T, et al. Insulin resistance and clinical outcomes after acute ischemic stroke. Neurology. 2018;90(17):e1470–7.
Strisciuglio T et al. Insulin resistance predicts severity of coronary atherosclerotic disease in non-diabetic patients. J Clin Med, 2020. 9(7).
Pan Y et al. Post-glucose load measures of insulin resistance and prognosis of nondiabetic patients with ischemic stroke. J Am Heart Assoc, 2017. 6(1).
Wang S, et al. Stronger association of triglyceride glucose index than the HOMA-IR with arterial stiffness in patients with type 2 diabetes: a real-world single-centre study. Cardiovasc Diabetol. 2021;20(1):82.
Zhao Y, et al. Cohort profile: the China Health and Retirement Longitudinal Study (CHARLS). Int J Epidemiol. 2014;43(1):61–8.
Simental-Mendía LE, Rodríguez-Morán M, Guerrero-Romero F. The product of fasting glucose and triglycerides as surrogate for identifying insulin resistance in apparently healthy subjects. Metab Syndr Relat Disord. 2008;6(4):299–304.
Cui H, et al. Cumulative triglyceride-glucose index is a risk for CVD: a prospective cohort study. Cardiovasc Diabetol. 2022;21(1):22.
Chen X, et al. Venous blood-based biomarkers in the China Health and Retirement Longitudinal Study: Rationale, Design, and results from the 2015 Wave. Am J Epidemiol. 2019;188(11):1871–7.
Shi W, et al. Value of triglyceride-glucose index for the estimation of ischemic stroke risk: insights from a general population. Nutr Metab Cardiovasc Dis. 2020;30(2):245–53.
Zhou Y, et al. Triglyceride glucose index and prognosis of patients with ischemic stroke. Front Neurol. 2020;11:456.
Wang A, et al. Change in triglyceride-glucose index predicts the risk of cardiovascular disease in the general population: a prospective cohort study. Cardiovasc Diabetol. 2021;20(1):113.
Yang K, Liu W. Triglyceride and glucose index and sex differences in relation to major adverse Cardiovascular events in hypertensive patients without diabetes. Front Endocrinol (Lausanne). 2021;12:761397.
Zhao Y, et al. Elevated triglyceride-glucose index predicts risk of incident ischaemic stroke: the rural chinese cohort study. Diabetes Metab. 2021;47(4):101246.
Hong S, Han K, Park CY. The triglyceride glucose index is a simple and low-cost marker associated with atherosclerotic cardiovascular disease: a population-based study. BMC Med. 2020;18(1):361.
Ding X, et al. Triglyceride-glucose index and the incidence of atherosclerotic cardiovascular diseases: a meta-analysis of cohort studies. Cardiovasc Diabetol. 2021;20(1):76.
Feng X, et al. Triglyceride-glucose index and the risk of stroke: a systematic review and dose-response Meta-analysis. Horm Metab Res. 2022;54(3):175–86.
Lee SB, et al. Association between triglyceride glucose index and arterial stiffness in korean adults. Cardiovasc Diabetol. 2018;17(1):41.
Guo W, et al. Triglyceride glucose index is Associated with arterial stiffness and 10-Year Cardiovascular Disease Risk in a Chinese Population. Front Cardiovasc Med. 2021;8:585776.
Miao M, et al. Triglyceride-glucose index and common carotid artery intima-media thickness in patients with ischemic stroke. Cardiovasc Diabetol. 2022;21(1):43.
Wu S, et al. Association between triglyceride-glucose index and risk of arterial stiffness: a cohort study. Cardiovasc Diabetol. 2021;20(1):146.
Bornfeldt KE, Tabas I. Insulin resistance, hyperglycemia, and atherosclerosis. Cell Metab. 2011;14(5):575–85.
Ormazabal V, et al. Association between insulin resistance and the development of cardiovascular disease. Cardiovasc Diabetol. 2018;17(1):122.
Rohm TV, et al. Inflammation in obesity, diabetes, and related disorders. Immunity. 2022;55(1):31–55.
Jin A, et al. Mediation of systemic inflammation on insulin resistance and prognosis of nondiabetic patients with ischemic stroke. Stroke. 2023;54(3):759–69.
Du T, et al. Clinical usefulness of lipid ratios, visceral adiposity indicators, and the triglycerides and glucose index as risk markers of insulin resistance. Cardiovasc Diabetol. 2014;13:146.
Ferreiro JL, Gómez-Hospital JA, Angiolillo DJ. Platelet abnormalities in diabetes mellitus. Diab Vasc Dis Res. 2010;7(4):251–9.
Moore SF, et al. Loss of the insulin receptor in murine megakaryocytes/platelets causes thrombocytosis and alterations in IGF signalling. Cardiovasc Res. 2015;107(1):9–19.
Ueno M, et al. Impact of impaired glucose tolerance on clopidogrel response in patients with coronary artery disease. J Thromb Thrombolysis. 2015;40(2):174–81.
Santilli F, et al. Platelet activation in obesity and metabolic syndrome. Obes Rev. 2012;13(1):27–42.
Acknowledgements
The authors thank all the members of the CHALRS for their contributions and the participants who contributed their data.
Funding
None.
Author information
Authors and Affiliations
Contributions
Yaoling Wu wrote the main manuscript text and conceived and designed the study. Yaoling Wu and Yongbiao Yang analyzed the data. Jinsheng Zhang and Shuo Liu carried out literature search. Weiduan Zhuang performed the manuscript review. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The studies involving human participants were reviewed and approved by the Ethics Review Committee of Peking University. The patients/participants provided their written informed consent to participate in this study.
Consent for publication
Not applicable.
Competing interests
The authors declare no potential conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wu, Y., Yang, Y., Zhang, J. et al. The change of triglyceride-glucose index may predict incidence of stroke in the general population over 45 years old. Cardiovasc Diabetol 22, 132 (2023). https://doi.org/10.1186/s12933-023-01870-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12933-023-01870-z