
Abstract
Background
Triglyceride–glucose (TyG) index, a simple surrogate marker of insulin resistance, has been reported to be associated with arterial stiffness. However, previous studies were limited by the cross-sectional design. The purpose of this study was to explore the longitudinal association between TyG index and progression of arterial stiffness.
Methods
A total of 6028 participants were derived from the Kailuan study. TyG index was calculated as ln [fasting triglyceride (mg/dL) × fasting glucose (mg/dL)/2]. Arterial stiffness was measured using brachial-ankle pulse wave velocity (baPWV). Arterial stiffness progression was assessed by the annual growth rate of repeatedly measured baPWV. Multivariate linear regression models were used to estimate the cross-sectional association of TyG index with baPWV, and Cox proportional hazard models were used to investigate the longitudinal association between TyG index and the risk of arterial stiffness.
Results
Multivariate linear regression analyses showed that each one unit increase in the TyG index was associated with a 39 cm/s increment (95%CI, 29–48 cm/s, P < 0.001) in baseline baPWV and a 0.29 percent/year increment (95%CI, 0.17–0.42 percent/year, P < 0.001) in the annual growth rate of baPWV. During 26,839 person-years of follow-up, there were 883 incident cases with arterial stiffness. Participants in the highest quartile of TyG index had a 58% higher risk of arterial stiffness (HR, 1.58; 95%CI, 1.25–2.01, P < 0.001), as compared with those in the lowest quartile of TyG index. Additionally, restricted cubic spline analysis showed a significant dose–response relationship between TyG index and the risk of arterial stiffness (P non-linearity = 0.005).
Conclusion
Participants with a higher TyG index were more likely to have a higher risk of arterial stiffness. Subjects with a higher TyG index should be aware of the following risk of arterial stiffness progression, so as to establish lifestyle changes at an early stage.
Similar content being viewed by others

Background
Cardiovascular disease (CVD) has climbed to the first cause of death and premature death in China [1, 2]. Arterial stiffness, one of the earliest functional damage in the vascular aging process, directly influenced the cardiovascular system by degenerating arterial elasticity and increasing pulse pressure [3, 4]. A growing number of studies demonstrated that arterial stiffness was a predictor for future cardiovascular events such as myocardial infarction, unstable angina, heart failure, and ischemic or hemorrhagic stroke [5, 6]. Considering that the pathology of arterial stiffness is a long-term progression, there is an urgent need for available and reliable markers to identify patients in the early stage and formulate appropriate preventive strategies.
Insulin resistance (IR) is regarded as an important contributing factor for arterial stiffness and the development of CVD due to the production of inflammatory factors and the following endothelial damage [7,8,9]. The triglyceride–glucose (TyG) index, which is calculated from fasting blood glucose (FBG) and fasting triglyceride (TG) levels, has been proposed as a surrogate marker of IR with better performance than the homeostasis model assessment of IR (HOMA-IR) [10,11,12]. Some previous studies have indicated a positive association of TyG index with cardiovascular risk including coronary artery disease, stroke, myocardial infarction, and carotid atherosclerosis [12,13,14,15,16,17]. Recently, a growing number of studies have been conducted to investigate the relationship between TyG index and arterial stiffness [11, 15, 17,18,19,20]. However, most previous studies were conducted with a cross-sectional study design, but not a cohort study on the progression of arterial stiffness. Therefore, we extend previous findings and provide a longitudinal perspective to explore the association between TyG index and the progression of arterial stiffness measured using brachial-ankle pulse wave velocity (baPWV).
Methods
Study population
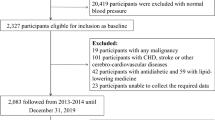
The participants were derived from Kailuan cohort, a prospective cohort established at Kailuan General Hospital and 10 affiliated hospitals, which has been described in detail elsewhere [21]. Briefly, from June 2006 to October 2007, participants from Kailuan community were enrolled and completed the first survey including questionnaires, physical examinations, and laboratory assessments, with an every 2-year follow-up. Since the third survey in 2010, a subcohort of the nested study on vascular health was conducted, with the baPWV tests to assess the health status of artery wall [22]. In this study, we included participants according to the following criteria: (1) individuals participated in at least one survey in 2010–2011, 2012–2013, 2014–2015, or 2016–2017, and received the first baPWV test; (2) individuals had complete baseline data of FBG and TG. There were 34,099 subjects who met the criteria. Then, we excluded participants who: (1) were taking antidiabetic or antihyperlipidemic agents at baseline; (2) had a history of CVD or cancer at baseline; (3) had baPWV tests less than three. Finally, a total of 6028 participants were included for analysis.
The study was performed according to the guidelines of the Declaration of Helsinki and was approved by the Ethics Committee of the Kailuan General Hospital (Approval Number: 2006–05). Written informed consent was obtained from all participants.
Data collection and definition
Information on demographics (e.g., age, sex), medical history (e.g., medications), and lifestyle (e.g., smoking status, alcohol consumption, physical activity), was collected by a structural questionnaire. Smoking and drinking status were stratified into two levels: current and never or former. Active physical activity was defined as “≥ 80 min/week”. Anthropometric data including weight, height, and waist circumference was measured by trained staff. Body mass index (BMI) was defined as the weight (kg)/height (m)2. Blood pressure was measured in the seated position using a mercury sphygmomanometer, and the average of three readings was calculated as systolic blood pressure (SBP) and diastolic blood pressure (DBP). Mean arterial blood pressure (MAP) was defined as 1/3*SBP + 2/3*DBP [23]. Hypertension was defined as either SBP or DBP ≥ 140/90 mmHg, antihypertensive medication use, or a self-reported history of hypertension. Diabetes was defined as FBG ≥ 7.0 mmol/L or self-reported history of diabetes.
Blood samples were collected after fasting for 8 to 12 h. Biochemical parameters including FBG, TG, total cholesterol (TC), high-density lipoprotein (HDL), low-density lipoprotein (LDL), and high-sensitivity C-reactive protein (hs-CRP) were measured on the Hitachi 747 auto-analyzer (Hitachi, Tokyo, Japan). FBG and TG levels were measured by the hexokinase/glucose-6-phosphate dehydrogenase method and the enzymatic colorimetric method, respectively. TyG index was calculated as ln [fasting triglyceride (mg/dL) × fasting glucose (mg/dL)/2] [24].
BaPWV measurement
BaPWV was measured by a BP-203 RPE III networked arterial stiffness detection device (Omron Health Medical [China]Co., LTD), as detailed elsewhere [22, 25, 26]. Measurements were repeated twice for each participant at a 5 min interval, with the second data considered the final value. The larger value between the left and right sides was used for analysis. BaPWV ≥ 1800 cm/s was considered as arterial stiffness according to the previous studies [27]. The progression of arterial stiffness was appraised by the annual growth rate of baPWV, which was calculated as
\(i, d2, di, {baPWV}_{1},{baPWV}_{i}\,and\, \overline{r }\) represented the survey ordinal number, the duration from baseline to the second survey, the duration from baseline to the \({i}_{th}\) survey, the baseline baPWV, the value of baPWV at the \({i}_{th}\) survey, and annual growth rate of baPWV, respectively.
Statistical analysis
Continuous variables with normal and skewed distributions were described as the mean ± standard deviation (SD) and the medians with interquartile ranges, respectively, whereas categorical variables were described as frequencies and percentages. Missing data for baseline covariates were imputed by the multiple imputation. To investigate linear trends of baseline characteristics across quartiles of TyG index, chi-square test for linear trend was used for categorical variables, and one-way analysis of variance for linear trend and Kruskal–Wallis test was performed for continuous variables with normal and skewed distributions, respectively. The TyG index was assessed by both quartiles and continuous variables. The associations of TyG index with baPWV at baseline and the annual growth rate of baPWV were estimated using multivariate linear regression models. Covariates referred to factors significantly associated with the progression of arterial stiffness and were ascertained according to prior published literature [23, 28], including age, sex, physical activity, smoking, alcohol drinking, BMI, hs-CRP, diabetes, and MAP.
Additionally, to investigate the association between TyG index and the risk of arterial stiffness, 680 participants with baPWV ≥ 1800 cm/s at baseline were excluded from the dataset. The remaining 5348 subjects without arterial stiffness were followed up to Jul 2020. Multivariate Cox proportional hazard regression was used to estimate the adjusted hazard ratios (HRs) and 95% confidence intervals (95%CIs) for arterial stiffness across the quartiles of the TyG index. In addition, we carried out restricted cubic spline analysis to explore the dose–response relationship between TyG index and baPWV as well as the risk of arterial stiffness. Three knots were placed at the 10th, 50th, and 90th percentiles, and the median of TyG index was used for reference point.
To avoid the potential bias due to measurement frequency, the associations between TyG index and the progression of arterial stiffness were reanalyzed among participants with at least two baPWV tests (N = 12,706), and the results were presented in Supplement materials as a sensitivity analysis. We also presented baseline characteristics of those with at least two baPWV tests according to the quartiles of the TyG index, and shown these overall characteristics for participants with only two baPWV tests and those with at least three baPWV tests in Supplement materials. All statistical analyses were performed using R software (version 4.0.2), and a two-tailed P value < 0.05 was considered statistically significant.
Results
Baseline characteristics
A total of 34,099 participants received baPWV tests with complete data of FBG and TG. After a series of exclusion criteria, 6028 individuals were included in the present study (Additional file 1: Fig. S1). Clinical and laboratory characteristics at baseline are presented in Table 1 according to the quartiles of the TyG index. Compared with participants in the lowest quartile group, participants with a higher TyG index tended to be older, men, more obese with higher BMI and waist circumference, and current smokers or drinkers. Likewise, significant differences in biological parameters were observed among the groups. SBP, DBP, MAP, FPG, TC, TG, LDL, and hs-CRP of the participants in the highest TyG index quartile were significantly higher than those in the first quartile. Moreover, the high TyG index groups had a higher prevalence of comorbidities such as diabetes and hypertension.
TyG index and baPWV
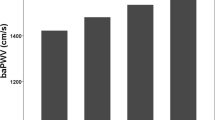
Overall, there was a significant positive association of TyG index with baPWV at baseline (Table 2, Fig. 1a). The linear regression models revealed that each one unit increment of TyG index was associated with a 39 cm/s change in baPWV (95% CI, 29–48 cm/s, P < 0.001) after adjusting for age, sex, physical activity, smoking, alcohol drinking, BMI, hs-CRP, diabetes, and MAP. In the categorical analysis, compared with those in the first quartile of TyG index, the adjusted β for participants in the second, third and highest quartile of TyG index were 19 (95% CI, 2–36 cm/s, P = 0.032), 50 (95% CI, 32–67 cm/s, P < 0.001), and 71 (95% CI, 52–90 cm/s, P < 0.001), respectively.

The associations of TyG index with baPWV at baseline (a) and annual growth rate of baPWV (b). Data were fitted using the linear regression models of the restricted cubic spline with 3 knots at 10, 50, and 90th percentiles of baseline TyG index. TyG index triglyceride-glucose index,CI confidence interval. The reference point was the median of the TyG index in the 6028 participants. The solid line represented point estimation on the association of TyG index with baPWV, and the shaded portion represented 95% CI estimation. Covariates in the model included age, sex, smoking, alcohol drinking, physical activity, MAP, diabetes, hs-CRP, and BMI
We further assessed the association of the TyG index with the annual growth rate of baPWV and found that the growth rate of baPWV had a statically significant increment in participants with a high TyG index (Fig. 1b). Overall, each one unit increase in the TyG index was responsible for a 0.29 percent/year increment in the average growth rate of baPWV after adjusting for all covariates (95% CI, 0.17–0.42 percent/year, P < 0.001). When TyG index was assessed as quartiles, as compared with those in the first quartile, β for participants in the second, third, and highest quartile of TyG index were 0.34 (95% CI, 0.11–0.57 percent/year, P = 0.003), 0.52 (95% CI, 0.29–0.76 percent/year, P < 0.001), and 0.45 (95% CI, 0.20–0.71 percent/year, P < 0.001) in the fully adjusted model, respectively.
TyG index and arterial stiffness
During 26,839 person-years of follow-up, there were 883 incident cases of arterial stiffness among the 5348 participants. The incident rate presented an increasing trend in four groups divided by the quartiles of TyG index, which were 14.46, 26.21, 44.78, and 49.87 per 1000 person-years, respectively. The association between the baseline TyG index and the risk of arterial stiffness is presented in Table 3. After adjusting for all covariates, the risk for arterial stiffness increased 22% (95% CI, 1.10–1.35, P < 0.001) with each one-unit increase of TyG index. Taking the lowest quartile as a reference, the adjusted HRs (95% CIs) in the second, third and highest quartiles of TyG index were 1.27 (1.00–1.62), 1.69 (1.35–2.12), and 1.58 (1.25–2.01), respectively. In addition, restricted cubic spline analysis (Fig. 2) showed the dose–response relationship between TyG index and the risk of arterial stiffness. (P non-linearity = 0.005).

The associations of TyG index with risk of arterial stiffness. Data were fitted using a Cox regression model of the restricted cubic spline with 3 knots at 10th, 50th, and 90th percentiles of baseline TyG index. TyG index triglyceride-glucose index, HR hazard ratio, CI confidence interval. The reference point was the median of the TyG index in the 5348 participants. The solid line represented point estimation on the association of TyG index with the risk of arterial stiffness, and the shaded portion represented 95% CI estimation. Covariates in the model included age, sex, smoking, alcohol drinking, physical activity, MAP, diabetes, hs-CRP, and BMI
Sensitivity analysis
The baseline characteristics of participants with only two baPWV tests and at least three baPWV tests was shown in Additional file 2: Table S1. Overall, the characteristics between the two groups were similar. In addition, the results of sensitivity analyses showed similar significant associations between TyG index and the progression of arterial stiffness among participants with at least two baPWV tests. (Additional file 2: Table S2–S4).
Discussion
In this study, we identified a significant association of the TyG index with baPWV as a quantitative marker of arterial stiffness. The TyG index was related to baPWV at baseline as well as the annual growth rate of baPWV in form of both quartiles and continuous variables. Furthermore, the TyG index was observed to be associated with the incidence of arterial stiffness assessed by baPWV after adjusting for age, sex, smoking, alcohol drinking, physical activity, MAP, diabetes, hs-CRP, and BMI at baseline. To the best of our knowledge, this is the first study to reveal the relationship between the TyG index and the progression of arterial stiffness in a large prospective cohort.
Recently, quite a few cohort studies have confirmed that the TyG index could play a predictive role in adverse cardiovascular events [14, 29,30,31,32]. Furthermore, several researchers transferred their attention to the association of TyG index with the progression of arterial-related pathology, particularly coronary artery calcium (CAC) and coronary plaque progression (PP). Two studies in Korea suggested that elevated TyG index was associated with a higher risk for CAC progression [16, 33]. In addition, Won et al. reported that the participants with the highest tertile TyG index had a 1.65-fold higher risk of coronary PP and 1.78-fold of rapid PP compared with the lowest tertile [34]. However, to our knowledge, little is currently known about the relationship between TyG index and arterial stiffness progression. Previous researchers have explored a cross-sectional association of TyG index with arterial stiffness assessed by baPWV. For instance, Lee and his colleagues found a nearly three-fold higher risk of increased baPWV in men and two-fold in women for the highest quartiles TyG index compared with the lowest quartiles in a general population [11]. Similarly, Won et al. demonstrated a linear relationship between the TyG index and the baPWV in both non-diabetics and diabetics [18]. This association was also observed in hypertensive patients [17]. Consistent with the abovementioned studies, findings from the present study also showed a significant cross-sectional association between TyG index and increased baPWV. We further investigate the longitudinal relationship of TyG index with the risk of arterial stiffness progression assessed by repeated measurement of baPWV, and found that a higher TyG index predicted a higher risk and faster progression of arterial stiffness. These findings extended the limited available evidence on the association between TyG index and arterial stiffness and may be helpful for early identification of subjects with a high risk of arterial stiffness, so as to take appropriate strategies to prevent CVD.
Although the exact biological mechanisms underlying the association remain unclear, the possible crucial pathway may be linked to IR. Generally, IR perturbs insulin signaling at the level of the intimal cells including endothelial cells, vascular smooth muscle cells, and macrophages, leading to a varying degree of oxidative responses and impaired endothelial function [35,36,37]. Moreover, IR drives the development of atherogenic dyslipidemia, and generates a lowgrade inflammatory state [7]. Previous researches have proved that inflammation was a key biological process involved in the pathogenesis of arterial stiffness, and it was often marked by CRP [8, 23, 37]. In our study, we observed that people with the highest quartile TyG index had a higher level of hs-CRP than those in the first quartile group. Nevertheless, the association of TyG index with arterial stiffness was still significant after adjustment for hs-CRP. This indicated an independent effect of TyG index on arterial stiffness progression. Due to relatively limited studies on this issue so far, more studies are warranted to be conducted for elucidating the exact pathways.
Simental-Mendía et al. firstly introduced TyG index as a surrogate to identify IR, and suggested the higher sensitivity of TyG index than HOMA-IR [24]. Subsequently, they also reported that TyG index closely mirrors the euglycemic-hyperinsulinemic clamp test, the gold standard technique in the assessment of insulin sensitivity [38]. In our study, we compared the diagnostic values of the TyG index, FBG, and TG for arterial stiffness by receiver operating characteristics curve and the area under the curve, and found that TyG index had a better predictive value than FBG and TG alone (data not shown), which was consistent with previous studies [39,40,41]. With an increasing number of studies supporting the strong predictive value of TyG index for the development of CVDs and other chronic diseases such as type 2 diabetes [42, 43], TyG index has been widely recognized as a simple and effective marker for disease prediction and prevention. A high TyG index could alert people to establish early lifestyle changes able to reduce the progression or incidence of disease.
Our study has several limitations. First, although most available demographic and clinical variables were incorporated into the model for adjustment, some residual or unmeasured confounding parameters such as the dose of alcoholic beverages and the consumption of macronutrients and nutrients could have affected the results. Second, it should be noted that the participants in this study were all from the Kailuan community, thus the findings may not be generalizable to other populations. Third, owing to a lack of records on serum insulin, we could not compare the TyG index with HOMA-IR and the hyperinsulinemic-euglycemic clamp test. Fourth, as a long-term cohort study, there existed an unavoidable bias caused by loss to follow-up. However, the sensitivity analysis showed that the associations between TyG index and the progression of arterial stiffness remained in the participants with at least two baPWV tests.
Conclusions
In conclusion, participants with a higher TyG index were more likely to have a higher risk of arterial stiffness. Subjects with a higher TyG index should be aware of the following risk of arterial stiffness progression, so as to establish lifestyle changes at an early stage.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- CVD:
-
Cardiovascular disease
- TyG index:
-
Triglyceride-glucose index
- IR:
-
Insulin resistance
- HOMA-IR:
-
Homeostasis model assessment of insulin resistance
- baPWV:
-
Brachial-ankle pulse wave velocity
- BMI:
-
Body mass index
- SBP:
-
Systolic blood pressure
- DBP:
-
Diastolic blood pressure
- MAP:
-
Mean arterial blood pressure
- FBG:
-
Fasting blood glucose
- TG:
-
Triglyceride
- TC:
-
Total cholesterol
- HDL:
-
High-density lipoprotein
- LDL:
-
Low-density lipoprotein
- hs-CRP:
-
High-sensitivity C-reactive protein
- SD:
-
Standard deviation
- HR:
-
Hazard ratio
- CI:
-
Confidence interval
- CAC:
-
Coronary artery calcium
- PP:
-
Plaque progression
References
Zhou M, Wang H, Zeng X, Yin P, Zhu J, Chen W, et al. Mortality, morbidity, and risk factors in China and its provinces, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2019;394:1145–58.
Yang G, Wang Y, Zeng Y, Gao GF, Liang X, Zhou M, et al. Rapid health transition in China, 1990–2010: findings from the Global Burden of Disease Study 2010. Lancet. 2013;381:1987–2015.
Zhang R, Xie J, Yang R, Li R, Chong M, Zhang X, et al. Association between ideal cardiovascular health score trajectories and arterial stiffness: the Kailuan Study. Hypertens Res. 2020;43:140–7.
van Popele NM, Grobbee DE, Bots ML, Asmar R, Topouchian J, Reneman RS, et al. Association between arterial stiffness and atherosclerosis: the Rotterdam Study. Stroke. 2001;32:454–60.
Mitchell GF, Hwang SJ, Vasan RS, Larson MG, Pencina MJ, Hamburg NM, et al. Arterial stiffness and cardiovascular events: the Framingham Heart Study. Circulation. 2010;121:505–11.
Laurent S, Boutouyrie P, Asmar R, Gautier I, Laloux B, Guize L, et al. Aortic stiffness is an independent predictor of all-cause and cardiovascular mortality in hypertensive patients. Hypertension. 2001;37:1236–41.
Laakso M, Kuusisto J. Insulin resistance and hyperglycaemia in cardiovascular disease development. Nat Rev Endocrinol. 2014;10:293–302.
Vlachopoulos C, Dima I, Aznaouridis K, Vasiliadou C, Ioakeimidis N, Aggeli C, et al. Acute systemic inflammation increases arterial stiffness and decreases wave reflections in healthy individuals. Circulation. 2005;112:2193–200.
Hanley AJ, Williams K, Stern MP, Haffner SM. Homeostasis model assessment of insulin resistance in relation to the incidence of cardiovascular disease: the San Antonio Heart Study. Diabetes Care. 2002;25:1177–84.
Irace C, Carallo C, Scavelli FB, De Franceschi MS, Esposito T, Tripolino C et al. Markers of insulin resistance and carotid atherosclerosis. A comparison of the homeostasis model assessment and triglyceride glucose index. Int J Clin Pract. 2013;67:665–672.
Lee SB, Ahn CW, Lee BK, Kang S, Nam JS, You JH, et al. Association between triglyceride glucose index and arterial stiffness in Korean adults. Cardiovasc Diabetol. 2018;17:41.
Kim MK, Ahn CW, Kang S, Nam JS, Kim KR, Park JS. Relationship between the triglyceride glucose index and coronary artery calcification in Korean adults. Cardiovasc Diabetol. 2017;16:108.
da Silva A, Caldas APS, Hermsdorff HHM, Bersch-Ferreira AC, Torreglosa CR, Weber B, et al. Triglyceride-glucose index is associated with symptomatic coronary artery disease in patients in secondary care. Cardiovasc Diabetol. 2019;18:89.
Hong S, Han K, Park CY. The triglyceride glucose index is a simple and low-cost marker associated with atherosclerotic cardiovascular disease: a population-based study. BMC Med. 2020;18:361.
Lambrinoudaki I, Kazani MV, Armeni E, Georgiopoulos G, Tampakis K, Rizos D, et al. The TyG Index as a Marker of Subclinical Atherosclerosis and Arterial Stiffness in Lean and Overweight Postmenopausal Women. Heart Lung Circ. 2018;27:716–24.
Park K, Ahn CW, Lee SB, Kang S, Nam JS, Lee BK, et al. Elevated TyG Index Predicts Progression of Coronary Artery Calcification. Diabetes Care. 2019;42:1569–73.
Li M, Zhan A, Huang X, Hu L, Zhou W, Wang T, et al. Positive association between triglyceride glucose index and arterial stiffness in hypertensive patients: the China H-type Hypertension Registry Study. Cardiovasc Diabetol. 2020;19:139.
Won KB, Park GM, Lee SE, Cho IJ, Kim HC, Lee BK, et al. Relationship of insulin resistance estimated by triglyceride glucose index to arterial stiffness. Lipids Health Dis. 2018;17:268.
Zhao S, Yu S, Chi C, Fan X, Tang J, Ji H, et al. Association between macro- and microvascular damage and the triglyceride glucose index in community-dwelling elderly individuals: the Northern Shanghai Study. Cardiovasc Diabetol. 2019;18:95.
Poon AK, Meyer ML, Tanaka H, Selvin E, Pankow J, Zeng D, et al. Association of insulin resistance, from mid-life to late-life, with aortic stiffness in late-life: the Atherosclerosis Risk in Communities Study. Cardiovasc Diabetol. 2020;19:11.
Wu S, Huang Z, Yang X, Zhou Y, Wang A, Chen L, et al. Prevalence of ideal cardiovascular health and its relationship with the 4-year cardiovascular events in a northern Chinese industrial city. Circ Cardiovasc Qual Outcomes. 2012;5:487–93.
Zheng M, Zhang X, Chen S, Song Y, Zhao Q, Gao X, et al. Arterial Stiffness Preceding Diabetes: A Longitudinal Study. Circ Res. 2020;127:1491–8.
Llaurado G, Ceperuelo-Mallafre V, Vilardell C, Simo R, Freixenet N, Vendrell J, et al. Arterial stiffness is increased in patients with type 1 diabetes without cardiovascular disease: a potential role of low-grade inflammation. Diabetes Care. 2012;35:1083–9.
Simental-Mendia LE, Rodriguez-Moran M, Guerrero-Romero F. The product of fasting glucose and triglycerides as surrogate for identifying insulin resistance in apparently healthy subjects. Metab Syndr Relat Disord. 2008;6:299–304.
Wu S, Jin C, Li S, Zheng X, Zhang X, Cui L, et al. Aging, Arterial Stiffness, and Blood Pressure Association in Chinese Adults. Hypertension. 2019;73:893–9.
Xue H, Li JJ, Wang JL, Chen SH, Gao JS, Chen YD, et al. Changes in pulse pressure x heart rate, hs-CRP, and arterial stiffness progression in the Chinese general population: a cohort study involving 3978 employees of the Kailuan Company. J Geriatr Cardiol. 2019;16:710–6.
Takashima N, Turin TC, Matsui K, Rumana N, Nakamura Y, Kadota A, et al. The relationship of brachial-ankle pulse wave velocity to future cardiovascular disease events in the general Japanese population: the Takashima Study. J Hum Hypertens. 2014;28:323–7.
Ferreira I, Boreham CA, Twisk JW, Gallagher AM, Young IS, Murray LJ, et al. Clustering of metabolic syndrome risk factors and arterial stiffness in young adults: the Northern Ireland Young Hearts Project. J Hypertens. 2007;25:1009–20.
Li S, Guo B, Chen H, Shi Z, Li Y, Tian Q, et al. The role of the triglyceride (triacylglycerol) glucose index in the development of cardiovascular events: a retrospective cohort analysis. Sci Rep. 2019;9:7320.
Sanchez-Inigo L, Navarro-Gonzalez D, Fernandez-Montero A, Pastrana-Delgado J, Martinez JA. The TyG index may predict the development of cardiovascular events. Eur J Clin Invest. 2016;46:189–97.
Wang L, Cong HL, Zhang JX, Hu YC, Wei A, Zhang YY, et al. Triglyceride-glucose index predicts adverse cardiovascular events in patients with diabetes and acute coronary syndrome. Cardiovasc Diabetol. 2020;19:80.
Wang A, Wang G, Liu Q, Zuo Y, Chen S, Tao B, et al. Triglyceride-glucose index and the risk of stroke and its subtypes in the general population: an 11-year follow-up. Cardiovasc Diabetol. 2021;20:46.
Won KB, Park EJ, Han D, Lee JH, Choi SY, Chun EJ, et al. Triglyceride glucose index is an independent predictor for the progression of coronary artery calcification in the absence of heavy coronary artery calcification at baseline. Cardiovasc Diabetol. 2020;19:34.
Won KB, Lee BK, Park HB, Heo R, Lee SE, Rizvi A, et al. Quantitative assessment of coronary plaque volume change related to triglyceride glucose index: The Progression of AtheRosclerotic PlAque DetermIned by Computed TomoGraphic Angiography IMaging (PARADIGM) registry. Cardiovasc Diabetol. 2020;19:113.
Bornfeldt KE, Tabas I. Insulin resistance, hyperglycemia, and atherosclerosis. Cell Metab. 2011;14:575–85.
Symons JD, McMillin SL, Riehle C, Tanner J, Palionyte M, Hillas E, et al. Contribution of insulin and Akt1 signaling to endothelial nitric oxide synthase in the regulation of endothelial function and blood pressure. Circ Res. 2009;104:1085–94.
Donato AJ, Machin DR, Lesniewski LA. Mechanisms of Dysfunction in the Aging Vasculature and Role in Age-Related Disease. Circ Res. 2018;123:825–48.
Guerrero-Romero F, Simental-Mendia LE, Gonzalez-Ortiz M, Martinez-Abundis E, Ramos-Zavala MG, Hernandez-Gonzalez SO et al. The product of triglycerides and glucose, a simple measure of insulin sensitivity. Comparison with the euglycemic-hyperinsulinemic clamp. J Clin Endocrinol Metab. 2010;95:3347–3351.
Hu C, Zhang J, Liu J, Liu Y, Gao A, Zhu Y, et al. Discordance between the triglyceride glucose index and fasting plasma glucose or HbA1C in patients with acute coronary syndrome undergoing percutaneous coronary intervention predicts cardiovascular events: a cohort study from China. Cardiovasc Diabetol. 2020;19:116.
Jin JL, Cao YX, Wu LG, You XD, Guo YL, Wu NQ, et al. Triglyceride glucose index for predicting cardiovascular outcomes in patients with coronary artery disease. J Thorac Dis. 2018;10:6137–46.
Su WY, Chen SC, Huang YT, Huang JC, Wu PY, Hsu WH et al. Comparison of the Effects of Fasting Glucose, Hemoglobin A1c, and Triglyceride-Glucose Index on Cardiovascular Events in Type 2 Diabetes Mellitus. Nutrients. 2019;11.
Ding X, Wang X, Wu J, Zhang M, Cui M. Triglyceride-glucose index and the incidence of atherosclerotic cardiovascular diseases: a meta-analysis of cohort studies. Cardiovasc Diabetol. 2021;20:76.
da Silva A, Caldas APS, Rocha D, Bressan J. Triglyceride-glucose index predicts independently type 2 diabetes mellitus risk: A systematic review and meta-analysis of cohort studies. Prim Care Diabetes. 2020;14:584–93.
Acknowledgements
We thank all study participants and the members of the survey teams at the 11 hospitals of the Kailuan Medical Group.
Funding
No funding was received.
Author information
Authors and Affiliations
Contributions
SW, MW, and LX made substantial contributions to the conception and design of the study, data collection and analysis, drafting of the manuscript and served as the equally contributing first authors of the manuscript. YW and YT made substantial contributions to study design, intellectual direction, and revision of the drafting of the manuscript. SC made contributions to data collection. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was performed according to the guidelines of the Declaration of Helsinki and was approved by the Ethics Committee of the Kailuan General Hospital (Approval Number: 2006–05). Written informed consent was obtained from all participants.
Consent for publication
Not applicable.
Competing interests
These authors declare that they have no conflicts of interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Fig. S1.
Flow chart of study population.
Additional file 2: Table S1.
Baseline characteristics of participants with only two and at least three baPWV tests. Table S2. Baseline characteristics of participants with at least two baPWV tests. Table S3. Association of TyG index with baPWV in participants with at least two baPWV tests. Table S4. Association of TyG index with arterial stiffness in participants with at least two baPWV tests.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wu, S., Xu, L., Wu, M. et al. Association between triglyceride-glucose index and risk of arterial stiffness: a cohort study. Cardiovasc Diabetol 20, 146 (2021). https://doi.org/10.1186/s12933-021-01342-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12933-021-01342-2