
Abstract
Background
The prognostic role of changes in body fat in patients with idiopathic pulmonary fibrosis (IPF) remains underexplored. We investigated the association between changes in body fat during the first year post-diagnosis and outcomes in patients with IPF.
Methods
This single-center, retrospective study included IPF patients with chest CT scan and pulmonary function test (PFT) at diagnosis and a one-year follow-up between January 2010 and December 2020. The fat area (cm2, sum of subcutaneous and visceral fat) and muscle area (cm2) at the T12-L1 level were obtained from chest CT images using a fully automatic deep learning-based software. Changes in the body composition were dichotomized using thresholds dividing the lowest quartile and others, respectively (fat area: -52.3 cm2, muscle area: -7.4 cm2). Multivariable Cox regression analyses adjusted for PFT result and IPF extent on CT images and the log-rank test were performed to assess the association between the fat area change during the first year post-diagnosis and the composite outcome of death or lung transplantation.
Results
In total, 307 IPF patients (69.3 ± 8.1 years; 238 men) were included. During the first year post-diagnosis, fat area, muscle area, and body mass index (BMI) changed by -15.4 cm2, -1 cm2, and − 0.4 kg/m2, respectively. During a median follow-up of 47 months, 146 patients had the composite outcome (47.6%). In Cox regression analyses, a change in the fat area < -52.3 cm2 was associated with composite outcome incidence in models adjusted with baseline clinical variables (hazard ratio [HR], 1.566, P = .022; HR, 1.503, P = .036 in a model including gender, age, and physiology [GAP] index). This prognostic value was consistent when adjusted with one-year changes in clinical variables (HR, 1.495; P = .030). However, the change in BMI during the first year was not a significant prognostic factor (P = .941). Patients with a change in fat area exceeding this threshold experienced the composite outcome more frequently than their counterparts (58.4% vs. 43.9%; P = .007).
Conclusion
A ≥ 52.3 cm2 decrease in fat area, automatically measured using deep learning technique, at T12-L1 in one year post-diagnosis was an independent poor prognostic factor in IPF patients.
Similar content being viewed by others

Background
Idiopathic pulmonary fibrosis (IPF) is a chronic, progressive idiopathic interstitial lung disease characterized by worsening respiratory symptoms, physiological impairment, and eventual death due to respiratory failure or its comorbidities [1]. Most IPF patients have progressive disease courses, with their median survival ranging from 2.5 to 3.5 years [2, 3]. Therefore, physicians need noninvasive and reproducible indicators to predict the prognosis, including forced vital capacity (FVC); diffusing capacity of carbon monoxide (DLCO); the gender, age, and physiology (GAP) index; and respiratory hospitalization [4,5,6,7,8,9,10].
During the first year after diagnosis, approximately 15–20% of IPF patients lose more than 5% of their weight [11, 12]. An increase in caloric requirements due to the increased work of breathing and decreased appetite by side-effects of antifibrotics, persistent cough, or psychosocial issues such as depression are presumed to cause unintended weight loss in IPF patients [13]. Indeed, studies have reported that low baseline body mass index (BMI) [14,15,16,17] or a decrease in body weight and BMI during the disease course [11, 12, 14, 15, 18,19,20,21,22] can adversely affect the prognosis of patients with IPF. However, these somatotype indicators only reflect the total weight (i.e., a sum of body fat, muscle, bone, and organs), not the body composition. Therefore, the prognostic role of body composition in patients with IPF remained underexplored, particularly in relation to body fat.
Recent advances in deep learning techniques have improved the quantification of body composition using diagnostic images such as computed tomography (CT). This approach can directly quantify each body component (e.g., fat or muscle) objectively and reproducibly [23, 24]. This study investigated the changes in body fat measured in chest CT images during the first year post-diagnosis using deep learning-based body composition analyses, and assessed the association between these changes and outcomes in patients with IPF.
Methods
This retrospective study was approved by the Institutional Review Board of Seoul National University Hospital, and the requirement for written informed consent was waived (IRB No.: 2208-165-1354).
Study sample
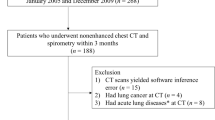
This single-center, cohort study included consecutive patients diagnosed with IPF between January 2010 and December 2020 at a tertiary hospital. IPF was diagnosed through multi-disciplinary team discussions, following the integration of clinical, radiological, and histological data when available. Among the IPF patients, we excluded patients without either baseline (i.e., at diagnosis) or one-year follow-up pulmonary function test (PFT) results and chest CT images. Baseline and one-year follow-up PFT and chest CT were defined with a buffer of 3 additional months to account for variability in patients’ follow-up strategy (i.e., examinations of 3 months before and after diagnosis were defined as baseline examinations; examinations within 9 and 15 months after diagnosis were defined as 1-year follow-up examinations). Given that our patient cohort consisted of individuals whose IPF diagnosis was established at our center, it was ensured that they maintained a stable disease course during the first year after diagnosis.
Clinical-radiological variables
Clinical data, including age, sex, BMI, smoking status, GAP index, use of antifibrotic agents, and PFT results (FVC and DLCO) were obtained from the electronic medical records. BMI was categorized as underweight (< 18.5 kg/m2), normal (18.5–24.9 kg/m2), overweight (25-29.9 kg/m2), and obese (> 30 kg/m2) [25]. Given the prognostic value of FVC and DLCO [26,27,28], the thresholds for significant declines in FVC and DLCO were defined as absolute declines of 5% and 10% from the baseline results, respectively. On the baseline chest CT images, one thoracic radiologist (J.Y.L. with 5 years of experience in thoracic images) measured the pulmonary artery diameter in the axial plane at the bifurcation, orthogonal to the long axis of the pulmonary artery [29, 30].
Commercially available deep learning-based texture analysis software (AVIEW Lung Texture version 1.1.43.7, Coreline Soft) was used to quantify IPF disease extent (performed by one radiologist [J.H.L.] with 11 years of experience in body imaging). This tool performs fully automatic segmentation of the total lung parenchyma and each finding (ground-glass opacity, reticular opacity, honeycombing cyst, emphysema, and consolidation) on CT images and provides quantification results as a percentage (%) of the total lung volume. IPF disease extent was defined as the sum of ground-glass opacity, reticular opacity, and honeycombing cysts.
CT examination
CT scans were acquired with 11 CT scanners (Brilliance 64, Ingenuity, ICT 256, Phillips Medical Systems, Best, the Netherlands; Sensation 16, Somatom Definition, Somtom Forse, Iqon Spectral CT, Siemens Medical Solutions, Forchheim, Germany; Aquilion One, Toshiba, Tokyo, Japan; Discovery CT750 HD, LightSpeed Ultra, Revolution, GE Medical Systems, Waukesha, Wis). The detailed parameters for CT acquisition were as follows: tube voltage, 100–120 kVp; tube current, standard (reference mAs, 60–120) to low-dose (reference mAs, 30) with automatic exposure control; slice thickness, 0.75-3.0 mm; reconstruction interval, 1.0–3.0 mm; and standard or sharp reconstruction kernel. All CT image data were evaluated regardless of intravenous contrast medium use. In contrast-enhanced CT scans, post-contrast CT images were obtained 60 s after the injection of 90 mL of iodinated contrast medium (iopamidol; iodine content, 300 mg/mL) at 3 mL/s, followed by 30 mL of saline chaser at the same rate.
Body composition analysis
Baseline and one-year follow-up CT images were imported into commercially available deep learning-based body composition analysis software (DEEPCATCH, v1.1.8.0, MEDICALIP Co. Ltd.). One radiologist (J.H.L.) confirmed the completeness of the software’s segmentation results. The software calculated CT-derived parameters, including subcutaneous fat area (cm2), visceral fat area (cm2), and muscle area (cm2) at T12-L1. Specifically, volumes of subcutaneous fat, visceral fat, and muscle at T12-L1 were captured and then normalized by dividing by the height of the T12-L1 vertebral bodies, and these values were defined as body composition areas, respectively. We used this measurement approach instead of using whole-body composition results obtained on chest CT because not all patients had exactly the same CT scan coverage. Indeed, multi-slice averaged body composition analysis results at the level of T12-L1 are known to be well correlated with whole-body composition [31]. Therefore, in this study, the subcutaneous and visceral fat areas were summed and defined as body fat area to represent whole-body fat. The fat areas and muscle areas from baseline and one-year follow-up CT images and their differences were obtained.
Outcomes
The outcome of this study was the occurrence of death or lung transplantation, defined as a composite outcome. Survival status and date of death were acquired from a database of the Ministry of the Interior and Safety, Korea, and information on lung transplantation was obtained from electronic medical records. Survival time was censored on March 31, 2023. For individuals who died or underwent lung transplantation, the time of censoring was defined as the date of death or transplantation, respectively.
Statistical analysis
Continuous variables are presented as mean values with standard deviations or median values with interquartile ranges according to the normality of the data distribution.
Spearman correlation coefficients were used to evaluate the relationship of changes in the fat or muscle area with changes in weight, BMI, and PFT results.
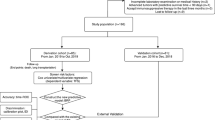
To analyze the prognostic value of change in the fat area, univariable and multivariable Cox regression analyses were performed. For multivariable regression analyses, variables with a P-value < 0.2 in the univariable analysis and BMI (both results at baseline and change in follow-up) were included. BMI was used despite being non-significant in the univariable analysis because it has been reported as a significant prognostic factor in IPF patients [12, 14,15,16,17, 19]. To robustly evaluate the prognostic value of change in the fat area, we separately performed multivariable regression analyses with the following variables: (a) baseline clinical-radiological variables, (b) baseline clinical-radiological variables including the GAP score [32], and (c) variables obtained at one-year follow-up visits, such as a change in BMI or PFT results. As there are no established optimal cut-off values for body composition in IPF patients, we categorized them into either the lowest quartile or the upper three quartiles based on their baseline body composition and the change during the first year, respectively. This approach derived from assessing the association between change in the fat area during the first year after diagnosis and each of event (composite outcome and death), using natural cubic splines in a Cox regression model (Appendix S1 and Fig S1).
A Kaplan-Meier plot was drawn, and the log-rank test was performed according to whether patients were categorized in the lowest quartile of fat area change. As a sensitivity analysis, the above-described survival analyses were performed for the outcome of death alone.
To assess the effect of baseline BMI on the prognostic value of fat area change, we performed subgroup analyses in IPF patients whose baseline BMI was < 25 kg/m2 and ≥ 25 kg/m2 separately. We set the thresholds to define the lowest quartile of fat change in each group, respectively.
All statistical analyses were performed using SPSS version 21.0 (IBM Corp.) and SAS version 9.4 (SAS Institute Inc.), and a P-value of < 0.05 was considered to indicate statistical significance.
Results
Baseline characteristics
A total of 307 individuals (238 men and 69 women; mean age, 69 ± 8.1 years) were included in this study (Fig. 1). The baseline characteristics of this study sample are described in Table 1. At baseline, the mean BMI was 24.5 ± 3.0 kg/m2 (underweight, n = 6 [2.0%]; normal, n = 179 [58.3%]; overweight, n = 108 [35.2%]; obese, n = 14 [4.6%]). Furthermore, 209 (68.1%) patients were ever smokers. The baseline FVC and DLCO were 80.8 ± 16.5% and 64.9 ± 17.9% predicted, respectively. The median baseline GAP score was 3 (interquartile range [IQR], 2–4), and the median total IPF extent was 12.3% (IQR, 7.6–18.3%).

Flow diagram showing the study sample
The median intervals between PFT and CT were both 12 months (IQR: 11–13 months for PFT; 11–14 months for CT). During the first year post-diagnosis, BMI decreased by 0.4 kg/m2 (24.1 ± 3.0 kg/m2 at follow-up). Ninety-three (30.3%) and 59 (19.2%) patients had absolute declines of FVC of 5% and DLCO of 10%, respectively. During a median follow-up duration of 47 months (IQR, 33–64 months), 146 patients had the composite outcomes (47.6%; death, n = 139, 45.3%; lung transplantation, n = 15, 4.9%).
Body composition analysis results
The median baseline fat area was 191.4 cm2 (IQR, 136.7-255.8 cm2), and the median baseline muscle area was 100.8 cm2 (IQR, 84.7-112.5 cm2). At the one-year follow-up CT, the median fat and muscle areas were 165.0 cm2 (IQR, 115.5-226.5 cm2) and 100.7 cm2 (IQR, 83.5-113.8 cm2), respectively. The median changes in the fat area and muscle area were − 15.4 cm2 (IQR, -52.3 to 9.9 cm2) and − 1.0 cm2 (IQR, -7.4 to 6.1 cm2), respectively. Therefore, the thresholds splitting patients into the lowest quartile and others were − 52.3 cm2 for fat area change and − 7.4 cm2 for muscle area change, respectively (Fig. 2).

Waterfall plot for the change in the fat area during the first year post-diagnosis in the study sample. The threshold splitting the lowest quartile and others was − 52.3 cm2
Relationship of body composition analyses with weight, BMI, and PFT results
A change in the fat area during the first year post-diagnosis was positively correlated with weight change (r = .328; P < .001), BMI change (r = .335; P < .001) (Fig S2), and FVC decline (r = .122; P = .032). DLCO showed no significant correlation with change in the fat area (r = .036; P = .527). A change in muscle area was correlated with weight change (r = 314; P < .001) and BMI change (r = .301; P < .001), but not with FVC decline (r=-.022; P = .704) and DLCO decline (r = .008; P = .887) (Table 2).
Survival analyses
The results of the Cox regression analyses for the composite outcomes are described in Table 3. In the univariable analyses, age, baseline GAP, baseline FVC, baseline DLCO, a decline of FVC of 5% or a decline of DLCO of 10% during the first year post-diagnosis, baseline pulmonary artery diameter, IPF extent on baseline CT, and the decrease in the fat area were significant (all P values < 0.05).
After adjusting for baseline clinical-radiological variables, including age, sex, baseline PFT results, and IPF extent on baseline CT, a change of the fat area <-52.3 cm2 during the first year post-diagnosis was associated with the composite outcome (adjusted hazard ratio [HR]: 1.566, 95% confidence interval [CI]: 1.066, 2.300, P = .022). In another model in which sex, age, and PFT results were treated as GAP scores, this fat change also predicted a poor prognosis (adjusted HR: 1.503; 95% CI: 1.026, 2.202, P = .036). In the model with variables obtained at the one-year follow-up, including changes in BMI and PFT during the first year post-diagnosis, this threshold for fat loss maintained its prognostic value for the composite outcome (adjusted HR: 1.495; 95% CI: 1.039, 2.151; P = .03), but a change in BMI did not (P = .941). Figures 3 and 4 represent IPF cases exemplifying the prognostic values of the change in the fat area during the first year post-diagnosis. In the Cox regression analysis where body composition parameters were treated as continuous variables, the change in fat area during the first year post-diagnosis was significant in univariable analyses. However, it was not significant in the multivariable analyses (Table S1 and Table S2).

Representative case of fully automated CT-based body composition analysis in (A) baseline and (B) one-year follow-up CT images in a patient belonging to the upper three quartiles of the change in fat area. Axial images at the T12-L1 vertebral level demonstrate visceral fat (green), subcutaneous fat (yellow), and skeletal muscle (red). Between CT images, the fat area increased by 80.3 cm2 (baseline: 140.7 cm2, one-year follow-up: 221.0 cm2). This patient remained under follow-up for 83 months without receiving lung transplantation or dying

Representative case of fully automated CT-based body composition analysis in (A) baseline and (B) one-year follow-up CT images in a patient belonging to the lowest quartile of the change in fat area. Axial images at the T12-L1 vertebral level demonstrate visceral fat (green), subcutaneous fat (yellow), and skeletal muscle (red). Between CT images, the fat area decreased by 89.9 cm2 (baseline: 370.0 cm2, one-year follow-up: 280.1 cm2). This patient died 10 months later despite receiving a lung transplantation
The results for death alone as an outcome are described in Table 4. A <-52.3 cm2 change in the fat area was also associated with death alone (adjusted HRs in all models > 1; all P values < 0.05).
As shown by the Kaplan-Meier curves, patients with a <-52.3 cm2 fat area change had higher frequencies of the composite outcome (58.4% vs. 43.9%, P = .007) and death (58.3% vs. 44.2%, P = .008) than their counterparts (Fig. 5).

(A) Kaplan-Meier curve for the composite outcome with the log-rank test. Patients with a ≥ 52.3 cm2 decrease of fat area at T12-L1 during the first year post-diagnosis disease course were more likely to have the composite outcome than their counterparts (58.4% versus 43.9%, P = .007). (B) Kaplan Meier curve for death with the log-rank test. Patients with a ≥ 52.3 cm2 decrease in fat area at T12-L1 during the first year post-diagnosis had a higher frequency of death than those without it (58.3% versus 44.2%, P = .008)
Subgroup analyses
Among 185 patients with underweight or normal baseline BMI, the lowest quartile of fat area decrease (threshold: -40.2 cm2) was associated with significantly higher rates of the composite outcomes in all Cox regression models of baseline clinical-radiological variables (adjusted HR: 1.704; 95% CI: 1.042, 2.787, P = .034), baseline clinical-radiological variables including GAP score (adjusted HR: 1.652; 95% CI: 1.027, 2.659, P = .039), and variables obtained at one-year follow-ups (adjusted HR: 1.954; 95% CI: 1.224, 3.119, P = .005) (Table S3). The results for death alone as an outcome are described in Table S4.
However, in the 122 patients with overweight or obese BMI at the baseline, fat area change (threshold: -75.4 cm2) was not associated with the composite outcome (P = .518) or death (P = .646) (Table S5 and Table S6).
Discussion
The clinical course of idiopathic pulmonary fibrosis (IPF) and the rate of disease progression are unpredictable and heterogeneous [1]. To stratify the prognosis of patients with IPF, several prognostic factors, including pulmonary function test (PFT) results, fibrosis extent on CT images, mean pulmonary arterial pressure, aging, and cigarette smoke, have been developed [1, 6, 13, 30, 32, 33]. Although weight loss and low baseline BMI have been identified as poor prognostic factors in IPF patients [11, 14, 15, 17, 18, 20,21,22], the prognostic role of change in body fat remains unclear because of difficulties in measuring body composition. While body composition parameters obtained from bioelectric impedance and dual-energy X-ray absorptiometry have shown correlations with lung function, health-related quality of life, and survival in IPF and other fibrotic interstitial lung diseases, their focus has primarily been on fat-free mass or skeletal muscle, rather than body fat [34,35,36]. We addressed this issue in 307 IPF patients, using deep learning applied to chest CT images. A change in the fat area showed a positive correlation with a decline in FVC (r = .122; P = .032). A <-52.3 cm2 change in the fat area was a significant prognostic factor for the composite outcome and death alone after adjusting for various baseline clinical-radiological variables and variables obtained at one-year follow-ups, including PFT results and IPF extent. However, a change in BMI during the first year was not a significant prognostic factor. In subgroup analyses, a decrease in the fat area was a prominent prognostic factor in patients with an underweight to normal baseline BMI.
CT imaging is a fundamental aspect for IPF evaluation, including diagnosis, longitudinal follow-up, and prognostication [37]. Although IPF extent on CT images is a well-known prognostic factor in patients with IPF [38], other quantitative prognostic information can be obtained using CT images. Body composition analysis results are a prime example [23], and in this perspective, we explored the prognostic value of the change in body fat derived from CT images. Given the prognostic value of body fat change based on routinely performed CT images was proven in this study, patients’ prognostic and nutritional information can be obtained without additional radiation exposure or medical expenditure.
The results of this study are in line with previous studies assessing the prognostic value of weight loss and its association with FVC decline in IPF patients. Specifically, significant weight loss, defined as ≥ 5% of baseline weight, was an independent predictor of mortality [11, 12, 15, 18,19,20,21,22, 39], acute exacerbation [15], and hospitalization [16] in IPF patients. Regarding PFT results, a greater FVC decline in IPF patients was reported to be associated with significant weight loss and low baseline BMI [11, 14, 15, 20, 21]. Considering these results, a decrease in body fat is speculated to affect FVC decline, a key prognostic factor in IPF patients. Nevertheless, as demonstrated in the multivariable regression analyses, a considerable change in body fat (e.g., -52.3 cm2 in our study) was an independent prognostic factor after adjusting for declines in PFT results and IPF extent. In summary, we speculate that a decrease in body fat contributes to a poor prognosis in IPF patients both as an independent prognostic factor and by negatively affecting PFT results. While the association remains unclear, the decrease in body fat might be attributed to the pulmonary disease itself. The progression of IPF and the increase in dyspnea can impact the patient’s nutritional status, leading to greater malnutrition. Moreover, these nutritional deterioration might exacerbate dyspnea, creating a vicious cycle that ultimately contributes to adverse outcomes, potentially leading to death [4, 16, 40,41,42].
Segmenting and measuring body fat directly from CT images, using deep learning techniques, can better reflect the relationship between individuals’ metabolic status and prognosis than using weight and BMI, which represent a simple summation of the entire body weight, including skeletal muscle, bone, and organs [23, 43]. In our study, while baseline BMI was a significant prognostic factor in line with previous studies [14,15,16,17], the change in BMI during the first year was not; in contrast, the change in fat area during the first year consistently demonstrated prognostic value. We speculate that because BMI reflects other organs, which rarely change over the first year, the change in BMI during the early follow-up period may not hold prognostic value. In addition, the prognostic value of BMI decrease might be prominent in patients with high BMI. Indeed, baseline BMI were higher in prior study proving prognostic value of BMI decrease (28.2 kg/m2 [12] and 29.9 km/m2 [19]) than that of our study sample (24.5 kg/m2). In line with this, our subgroup analysis results showed that a decline in BMI had a negative prognostic effect only in overweight to obese patients. In contrast, since only fat can be extracted from CT images, it allows for a more thorough exploration of prognostic implications.
Several limitations of this study should be considered. First, this was a retrospective study, and many patients were excluded because they lacked available baseline or one-year follow-up CT or PFT results. Despite buffering for 3 months to alleviate variability in the patients’ follow-up strategy, we still did not sufficiently cover the heterogeneous follow-up strategies in many patients. However, extending the buffering period beyond 3 months might compromise the original purpose of this study. Second, heterogeneity in CT vendors, machines, and reconstruction protocols (e.g., reconstruction kernel) might have affected the quantification results. To mitigate this limitation, we used standard-kernel and thin-slice thickness images as much as possible because these reconstruction protocols were aligned with those of the training datasets of the body composition analysis software for this study. Future research using unified CT protocols or deep learning-based kernel conversion may be needed. Third, our study did not validate the threshold of significant fat change (-52.3 cm2) in an independent IPF cohort. Moreover, although we demonstrated that the association pattern between fat change during the first year and each outcome was not linear, the inconsistency in the prognostic significance of fat area change when treated as a continuous variable raises concerns about the robustness of our results. Therefore, additional validation studies with independent datasets are necessary to prove the prognostic implication of this threshold. Fourth, unlike our results, several studies have reported low baseline skeletal muscle and its decrease during follow-up as an adverse prognostic factor in IPF patients [44,45,46]. Differences in measurement methods (e.g., measurement of erector muscle versus all muscles) and the slight change in skeletal muscle quantification results in our study (e.g., a change of -0.1 cm2 during the first year) might explain this discrepancy. Further multi-center studies with consistent measurement methods will be needed to investigate the prognostic value of skeletal muscle quantification in IPF patients. Finally, although we analyzed one-year follow-up CT images, additional serial CT images of shorter intervals or beyond one year could provide more information about body composition changes and their prognostic value in IPF patients.
Conclusion
In conclusion, a ≥ 52.3 cm2 decrease in fat area, automatically measured using deep learning technique, at T12-L1 in the first year post-diagnosis was an independent poor prognostic factor in patients with IPF. A management strategy to maintain body fat might improve outcomes in IPF patients.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding authors on reasonable request.
Abbreviations
- IPF:
-
Idiopathic pulmonary fibrosis
- FVC:
-
Forced vital capacity
- DLCO :
-
Diffusing capacity of carbon monoxide
- GAP:
-
Gender, age, and physiology
- BMI:
-
Body mass index
- PFT:
-
Pulmonary function tests
References
Podolanczuk AJ, Thomson CC, Remy-Jardin M, Richeldi L, Martinez FJ, Kolb M, Raghu G. Idiopathic pulmonary fibrosis: state of the art for 2023. Eur Respir J 2023;61.
Ley B, Collard HR, King TE Jr. Clinical course and prediction of survival in idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2011;183:431–40.
Fernández Pérez ER, Daniels CE, Schroeder DR, St Sauver J, Hartman TE, Bartholmai BJ, Yi ES, Ryu JH. Incidence, prevalence, and clinical course of idiopathic pulmonary fibrosis: a population-based study. Chest. 2010;137:129–37.
Kishaba T, Nagano H, Nei Y, Yamashiro S. Body mass index-percent forced vital capacity-respiratory hospitalization: new staging for idiopathic pulmonary fibrosis patients. J Thorac Dis. 2016;8:3596–604.
Collard HR, King TE Jr., Bartelson BB, Vourlekis JS, Schwarz MI, Brown KK. Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2003;168:538–42.
Flaherty KR, Andrei AC, Murray S, Fraley C, Colby TV, Travis WD, Lama V, Kazerooni EA, Gross BH, Toews GB, Martinez FJ. Idiopathic pulmonary fibrosis: prognostic value of changes in physiology and six-minute-walk test. Am J Respir Crit Care Med. 2006;174:803–9.
Flaherty KR, Mumford JA, Murray S, Kazerooni EA, Gross BH, Colby TV, Travis WD, Flint A, Toews GB, Lynch JP 3rd, Martinez FJ. Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia. Am J Respir Crit Care Med. 2003;168:543–8.
Hanson D, Winterbauer RH, Kirtland SH, Wu R. Changes in pulmonary function test results after 1 year of therapy as predictors of survival in patients with idiopathic pulmonary fibrosis. Chest. 1995;108:305–10.
Salisbury ML, Xia M, Zhou Y, Murray S, Tayob N, Brown KK, Wells AU, Schmidt SL, Martinez FJ, Flaherty KR. Idiopathic pulmonary fibrosis: gender-age-physiology Index Stage for Predicting Future lung function decline. Chest. 2016;149:491–8.
du Bois RM, Weycker D, Albera C, Bradford WZ, Costabel U, Kartashov A, Lancaster L, Noble PW, Raghu G, Sahn SA, et al. Ascertainment of individual risk of mortality for patients with idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2011;184:459–66.
Nakatsuka Y, Handa T, Kokosi M, Tanizawa K, Puglisi S, Jacob J, Sokai A, Ikezoe K, Kanatani KT, Kubo T, et al. The clinical significance of Body Weight loss in idiopathic pulmonary fibrosis patients. Respiration. 2018;96:338–47.
Pugashetti J, Graham J, Boctor N, Mendez C, Foster E, Juarez M, Harper R, Morrissey B, Kadoch M, Oldham JM. Weight loss as a predictor of mortality in patients with interstitial lung disease. Eur Respir J 2018:52.
Luppi F, Kalluri M, Faverio P, Kreuter M, Ferrara G. Idiopathic pulmonary fibrosis beyond the lung: understanding disease mechanisms to improve diagnosis and management. Respir Res. 2021;22:109.
Jouneau S, Crestani B, Thibault R, Lederlin M, Vernhet L, Valenzuela C, Wijsenbeek M, Kreuter M, Stansen W, Quaresma M, Cottin V. Analysis of body mass index, weight loss and progression of idiopathic pulmonary fibrosis. Respir Res. 2020;21:312.
Kreuter M, Bendstrup E, Jouneau S, Maher TM, Inoue Y, Miede C, Lievens D, Crestani B. Weight loss and outcomes in subjects with progressive pulmonary fibrosis: data from the INBUILD trial. Respir Res. 2023;24:71.
Jouneau S, Rousseau C, Lederlin M, Lescoat A, Kerjouan M, Chauvin P, Luque-Paz D, Guillot S, Oger E, Vernhet L, Thibault R. Malnutrition and decreased food intake at diagnosis are associated with hospitalization and mortality of idiopathic pulmonary fibrosis patients. Clin Nutr. 2022;41:1335–42.
Fang C, Huang H, Guo J, Ferianc M, Xu Z. Real-world experiences: efficacy and tolerability of pirfenidone in clinical practice. PLoS ONE. 2020;15:e0228390.
Lee JK, Chung C, Kim J, Cho HS, Kim HC. Clinical impact of weight loss on mortality in patients with idiopathic pulmonary fibrosis: a retrospective cohort study. Sci Rep. 2023;13:5774.
Kulkarni T, Yuan K, Tran-Nguyen TK, Kim YI, de Andrade JA, Luckhardt T, Valentine VG, Kass DJ, Duncan SR. Decrements of body mass index are associated with poor outcomes of idiopathic pulmonary fibrosis patients. PLoS ONE. 2019;14:e0221905.
Lee JS, Martin-Schwarze A, Freiheit E, Trzaskoma B, Burg C. Real-world clinical outcomes based on body Mass Index and annualized weight change in patients with idiopathic pulmonary fibrosis. Adv Ther. 2023;40:691–704.
Kalininskiy A, Rackow AR, Nagel D, Croft D, McGrane-Minton H, Kottmann RM. Association between weight loss and mortality in idiopathic pulmonary fibrosis. Respir Res. 2022;23:377.
Kim TH, Shin YY, Kim HJ, Song MJ, Kim YW, Lim SY, Lee YJ, Park JS, Cho YJ, Lee JH, et al. Impact of body weight change on clinical outcomes in patients with idiopathic pulmonary fibrosis receiving pirfenidone. Sci Rep. 2022;12:17397.
Lee JH, Choi SH, Jung KJ, Goo JM, Yoon SH. High visceral fat attenuation and long-term mortality in a health check-up population. J Cachexia Sarcopenia Muscle. 2023;14:1495–507.
Lee YS, Hong N, Witanto JN, Choi YR, Park J, Decazes P, Eude F, Kim CO, Chang Kim H, Goo JM, et al. Deep neural network for automatic volumetric segmentation of whole-body CT images for body composition assessment. Clin Nutr. 2021;40:5038–46.
Obesity and overweight. World Health Organization. 2021. https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight. Accessed 20 Sep 2023.
Zappala CJ, Latsi PI, Nicholson AG, Colby TV, Cramer D, Renzoni EA, Hansell DM, du Bois RM, Wells AU. Marginal decline in forced vital capacity is associated with a poor outcome in idiopathic pulmonary fibrosis. Eur Respir J. 2010;35:830–6.
Robbie H, Daccord C, Chua F, Devaraj A. Evaluating disease severity in idiopathic pulmonary fibrosis. Eur Respir Rev 2017;26.
Raghu G, Remy-Jardin M, Richeldi L, Thomson CC, Inoue Y, Johkoh T, Kreuter M, Lynch DA, Maher TM, Martinez FJ, et al. Idiopathic pulmonary fibrosis (an update) and progressive pulmonary fibrosis in adults: an Official ATS/ERS/JRS/ALAT Clinical Practice Guideline. Am J Respir Crit Care Med. 2022;205:e18–e47.
Aluja Jaramillo F, Gutierrez FR, Díaz Telli FG, Yevenes Aravena S, Javidan-Nejad C, Bhalla S. Approach to Pulmonary Hypertension: from CT to clinical diagnosis. Radiographics. 2018;38:357–73.
Shin S, King CS, Puri N, Shlobin OA, Brown AW, Ahmad S, Weir NA, Nathan SD. Pulmonary artery size as a predictor of outcomes in idiopathic pulmonary fibrosis. Eur Respir J. 2016;47:1445–51.
Hong JH, Hong H, Choi YR, Kim DH, Kim JY, Yoon JH, Yoon SH. CT analysis of thoracolumbar body composition for estimating whole-body composition. Insights Imaging. 2023;14:69.
Lee SH, Kim SY, Kim DS, Kim YW, Chung MP, Uh ST, Park CS, Jeong SH, Park YB, Lee HL, et al. Predicting survival of patients with idiopathic pulmonary fibrosis using GAP score: a nationwide cohort study. Respir Res. 2016;17:131.
du Bois RM, Weycker D, Albera C, Bradford WZ, Costabel U, Kartashov A, King TE Jr., Lancaster L, Noble PW, Sahn SA, et al. Forced vital capacity in patients with idiopathic pulmonary fibrosis: test properties and minimal clinically important difference. Am J Respir Crit Care Med. 2011;184:1382–9.
Machado FV, Bloem AEM, Schneeberger T, et al. Relationship between body composition, exercise capacity and health-related quality of life in idiopathic pulmonary fibrosis. BMJ Open Respir Res. 2021;8(1):e001039.
Nishiyama O, Yamazaki R, Sano H, et al. Fat-free mass index predicts survival in patients with idiopathic pulmonary fibrosis. Respirology. 2017;22(3):480–5.
Guler SA, Hur SA, Lear SA, Camp PG, Ryerson CJ. Body composition, muscle function, and physical performance in fibrotic interstitial lung disease: a prospective cohort study. Respir Res. 2019;20(1):56.
Barnes H, Humphries SM, George PM, Assayag D, Glaspole I, Mackintosh JA, Corte TJ, Glassberg M, Johannson KA, Calandriello L, et al. Machine learning in radiology: the new frontier in interstitial lung diseases. Lancet Digit Health. 2023;5:e41–e50.
Jacob J, Bartholmai BJ, Rajagopalan S, Kokosi M, Nair A, Karwoski R, Walsh SL, Wells AU, Hansell DM. Mortality prediction in idiopathic pulmonary fibrosis: evaluation of computer-based CT analysis with conventional severity measures. Eur Respir J 2017;49.
Doubková M, Švancara J, Svoboda M, Šterclová M, Bartoš V, Plačková M, Lacina L, Žurková M, Binková I, Bittenglová R, et al. EMPIRE Registry, Czech Part: impact of demographics, pulmonary function and HRCT on survival and clinical course in idiopathic pulmonary fibrosis. Clin Respir J. 2018;12:1526–35.
Holst M, Nielsen C, Sørensen LF, et al. A 1-year follow-up study in patients with idiopathic pulmonary fibrosis regarding adverse outcomes to unintended weight loss. Nutrition. 2023;108:111964.
Otoupalova E, Smith S, Cheng G, Thannickal VJ. Oxidative stress in Pulmonary Fibrosis. Compr Physiol. 2020;10(2):509–47.
Balasubramanian VP, Varkey B. Chronic obstructive pulmonary disease: effects beyond the lungs. Curr Opin Pulm Med. 2006;12(2):106–12.
Body mass index. : considerations for practitioners. Centers for Disease Control and Prevention. https://stacks.cdc.gov/view/cdc/25368. Accessed 20 Sep 2023.
Moon SW, Choi JS, Lee SH, Jung KS, Jung JY, Kang YA, Park MS, Kim YS, Chang J, Kim SY. Thoracic skeletal muscle quantification: low muscle mass is related with worse prognosis in idiopathic pulmonary fibrosis patients. Respir Res. 2019;20:35.
Suzuki Y, Aono Y, Kono M, Hasegawa H, Yokomura K, Naoi H, Hozumi H, Karayama M, Furuhashi K, Enomoto N, et al. Cause of mortality and sarcopenia in patients with idiopathic pulmonary fibrosis receiving antifibrotic therapy. Respirology. 2021;26:171–9.
Nakano A, Ohkubo H, Taniguchi H, Kondoh Y, Matsuda T, Yagi M, Furukawa T, Kanemitsu Y, Niimi A. Early decrease in erector spinae muscle area and future risk of mortality in idiopathic pulmonary fibrosis. Sci Rep. 2020;10:2312.
Acknowledgements
The authors wish to extend their gratitude to Dr. Myoung-jin Jang, PhD, from the Medical Research Collaborating Center at Seoul National University Hospital, for her verification of the statistical results of this study.
Funding
This study was supported by the Seoul National University Hospital Research Fund (grant number: 03-2023-0280).
Author information
Authors and Affiliations
Contributions
All the authors contributed to study design, data acquisition, data interpretation, and writing of the manuscript. Specifically, JHL and JP contributed to the concept, design of the study, data acquisition, data analysis, interpretation of data, writing the first draft of this paper, and critical revision of the manuscript. JYL conducted data analysis including statistical analysis and wrote the first draft of this paper. SHY and JMG contributed interpretation of data and critical revision of the manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This retrospective study was in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Seoul National University Hospital, and the requirement for written informed consent was waived (IRB No.: 2208-165-1354).
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Lee, J.Y., Yoon, S.H., Goo, J.M. et al. Association between body fat decrease during the first year after diagnosis and the prognosis of idiopathic pulmonary fibrosis: CT-based body composition analysis. Respir Res 25, 103 (2024). https://doi.org/10.1186/s12931-024-02712-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12931-024-02712-6