
Abstract
Background
Current guidelines recommend a single inhaler maintenance and reliever therapy (SMART) regimen for moderate to severe asthma. However, evidence for the inhaled corticosteroid plus fast-onset-acting β2-agonist (ICS/FABA) as reliever therapy in management of intermittent and mild asthma patients is lacking.
Objective
To systematically explore efficacy and safety of the proof-of-concept of the ICS plus FABA regimen in a single inhaler as reliever therapy across children and adults with intermittent and mild persistent asthma.
Methods
We searched online bibliographic databases for randomized controlled trials (RCTs) involving the as-needed use of ICS/FABA as monotherapy in intermittent or mild asthma patients. The primary outcomes were exacerbations and the hazard ratio (HR) of the time to first exacerbation.
Results
Six RCTs (n = 1300) met the inclusion criteria. Compared with the as-needed FABA regimen, the as-needed use of ICS/FABA as monotherapy statistically reduced exacerbations (RR = 0.56, P = 0.001). Compared with regular ICS regimen, the as-needed ICS/FABA therapy had slightly higher risk of exacerbations (RR = 1.39, P = 0.011). The HR for time to first exacerbations in the ICS/FABA regimen was significant lower when compared with FABA regimen (HR = 0.52, P = 0.002) but had no difference when compared with ICS regimen (HR = 1.30, P = 0.286). The corticosteroid exposure in the daily ICS regimen was 2- to 5-fold compared with as-needed use of ICS/FABA regimen.
Conclusions
Our analysis shows that the ICS/FABA as a symptom-driven therapy may be a promising alternative regimen for the patients with intermittent or mild asthma, but it needs further real-world RCTs to confirm these findings.
Similar content being viewed by others

Introduction
Asthma is characterized by airway inflammation, airway hyper-responsiveness, and variable airflow limitation [1], with an estimated 300 million affected individuals in the world [2, 3]. Currently, clinical research and management initiatives primarily focus on severe asthma [4,5,6], while more than half of patients have intermittent or mild diseases [7,8,9], and there is a largely unexplored but important burden of disease in this group [10]. Short-acting β2-agonists (SABA) can quickly relieve the symptoms [11], but it has no significant anti-inflammatory effects [12].Intermittent or mild asthma patients are recommended to initiate treatment with maintenance of low-dose inhaled corticosteroids (ICS) if they require a SABA more than twice a week [13, 14] or twice a month [1]. In addition, in a real-life setting, poor adherence of ICS as a controller is associated with significant asthma-related morbidity. Furthermore, some patients with intermittent or mild asthma prefer to take anti-asthma therapy intermittently and occasionally when they experience few symptoms [15, 16]. Therefore, alternative strategies for long-term management of intermittent or mild asthma is to be needed.
It is now well established that a fixed combination of ICS/LABA inhaler for both maintenance and reliever therapy (SMART regimen), which significantly reduces the risk of severe exacerbations and systemic corticosteroid exposure compared with standard fixed-dose regimen in moderate and severe asthma patients, has been recommended for patients with steps 3 to 5 in guidelines [1]. However, it could not be generalized to patients with steps 1 and 2 being equivalent to intermittent or mild persistent asthma (GINA steps 1 and 2) (Table 1), because there is a lack of evidence for the combination corticosteroid/fast-onset-acting β2-agonist (ICS/FABA) in a single inhaler as reliever therapy in the management of these patients. A proof-of-concept study indicated that in patients with mild asthma, the symptom-driven use of ICS and SABA in a single inhaler resulted in efficacy similar to that seen with regular ICS therapy [17]. Hence, in this proof-of-concept systematic review, we systematically explored the efficacy and safety of the ICS plus FABA regimen in a single inhaler as reliever therapy compared with the as-needed use of FABA regimen and the daily use of ICS regimen in children and adults with intermittent and mild persistent asthma based on randomized controlled trials.
Methods
This study was in adherence to the Preferred Reporting in Systematic Reviews and Meta-Analyses (PRISMA) guidelines [18].
Selection criteria
The eligible studies were randomized controlled trials (RCTs) including patients with intermittent or mild persistent asthma. The eligible interventions included the as-needed use of ICS plus FABA regimen as only one treatment in a single inhaler or separate inhalers in comparison with the regular ICS regimen or the as-needed use of FABA regimen. Any types of fast-onset-acting β2-agonists such as SABA (salbutamol, terbutaline or others) or FABA (formoterol but not salmeterol) were allowed.
Data sources and searching
We searched MEDLINE (Ovid), EMBASE (Ovid), Epub Ahead of Print, In-Process & Other Non-Indexed Citations (Ovid) and Cochrane Central Register of Controlled Trials (CENTRAL, Ovid) up to October 10, 2017, for randomized controlled trials involving the as-needed use of ICS/FABA as monotherapy in intermittent or mild asthma patients. To increase sensitivity for founding the intermittent and mild asthma trials, we included broader asthma severity terms contained total asthma spectrum (The medical subject headings (MeSH) terms used as described in Additional file 1: Table S1). There was no language restriction for the search. We also manually reviewed reference lists of relevant reports and contacted with the manufacturer of budesonide/formoterol inhaler (Symbicort®, AstraZeneca AB) for any unpublished studies and/or additional unpublished data from published studies. To identify ongoing trials, we also searched the WHO International Clinical Trials Registry Platform (ICTRP) and ClinicalTrials.gov.
Study selection
To validate this proof-of-concept of the combination as-needed use of the ICS plus FABA regimen in intermittent and mild asthma, we included all studies that involved the use of the ICS and the FABA in a single inhaler or separate inhalers as reliever therapy. Two reviewers (XZ & GW) independently selected articles on the basis of title and/or abstract for full text scrutiny. Disagreements were resolved by consensus or, if required, a third reviewer serving as the arbitrator (GW as the corresponding author).
Data extraction
Two reviewers independently extracted information from included studies for the following characteristics such as authors, study design, total duration of study, details of any ‘run in’ period, study centers and location, inclusion criteria, exclusion criteria, diagnostic criteria of asthma, asthma severity, sample size, age, gender, baseline lung function, inhaler device, daily dose of steroid presented as beclomethasone dipropionate (BDP) equivalent, adherence, dropouts or withdrawals and outcomes.
Quality assessment
The bias risk of the different studies was assessed with the components recommended by the Cochrane Collaboration for randomized trials [19]. These components include random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting and other bias. For each component, individual team members judged whether the risk of bias in a given study was “low,” “high,” or “unclear.” Any disagreements were referred to the third reviewer.
Primary and secondary outcomes
The primary objective of this study was to explore the efficacy of the as-needed use ICS/FABA regimen, and therefore the primary outcome was the exacerbations defined by the criteria of moderate to severe exacerbations of American Thoracic Society (ATS)/European Respiratory Society (ERS) [20]. Furthermore, we also calculated the severe exacerbations and the hazard ratio (HR) of the time to first exacerbation after randomization within these included studies.
The secondary outcomes included nocturnal awakenings times, the percentage of asthma symptom-free days, the number of rescue medication required per day, forced expiratory volume in one second (FEV1) percentage of predicted value. In addition, in terms of the safety profile, we assessed the number of dropout, serious adverse events, corticosteroid exposure and linear growth during the study period just in the children and adolescent subgroup.
Statistical analysis
We treated exacerbations data using patients as the unit of analysis (rather than events) to avoid repeating. Where zero counts existed for an dichotomous outcome in one arm of a trial, we added a value of 0.5 to permit meta-analysis, and where zero counts existed in both arms of a trial, we omitted the trial from the analysis of that outcome according to Cochrane principles [19]. We presented dichotomous data as risk ratio (RR), continuous data as the standardized mean difference (SMD) and time-to-event data as hazard ratio (HR) with 95% confidence intervals. Specially, a software named GetData Graph Digitizer v.2.26 [21] (DR MyCommerce, Inc.) was used to dig out the detailed data from Kaplan–Meier curves of the time to first exacerbation for calculating the HR, which was described in detail in the Methods section in this article’s Additional file 1. For missing data, we contacted investigators or study sponsors in order to obtain where possible. Otherwise, we dealt with missing data according to the Cochrane handbook recommending principals [19, 22]. All analyses were performed using an intention to treat approach. For the primary outcome of exacerbations, we calculated the number needed to treat (NNT) for assessing the different levels of risk. Heterogeneity was assessed with the Q statistic and the I2 statistic. A random-effects model [23] was used to pool data if substantial heterogeneity was observed (I2 > 50% or P < 0.1 for Q statistic), otherwise we used a fixed-effects model [24]. If there were more than 10 trials, a funnel plot would be created to explore possible publication bias. The quality of a body of evidence for primary outcomes was rated using the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) system [25] (GRADEpro Guideline Development Tool, McMaster University, 2015).
In addition, because adherence is very important in regular or fixed maintenance therapy, we undertook an additional meta-analysis of auxiliary information was performed to pool real-life adherence of the daily use of ICS treatment in patients with persistent asthma who were present in a real-world setting. The detailed method and results were provided in the Methods and Results section in this article’s Additional file 1.
Data were combined with the Stata 14.0 software (College Station, TX). Statistical significance was assumed for P < 0.05.
Results
Studies retrieved and characteristics
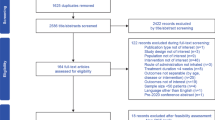
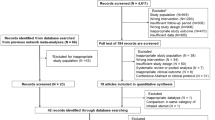
Figure 1 shows details of study identification, inclusion, and exclusion. Our search strategy initially yielded 10,612 citations, and the AstraZeneca (AstraZeneca AB) provided thirteen studies. Finally, six RCTs were included in this meta-analysis [17, 26,27,28,29,30].

Flow of study identification, inclusion, and exclusion
Table 2 shows the characteristics of the included studies. Generally, there were five parallel trials and one crossover trial [26]. According to the recommendation of the Cochrane Handbook for Systematic Reviews of Interventions [19], we judged the suitability and acceptability of the cross-over design in our study (Additional file 1: Table S2). One thousand and three hundred subjects were included for analysis (Table 2). There were 674 (6 studies; 46.2% female; median age: 25.9 [range: 2.3–39.9] years), 317 (5 studies; 54.9% female; median age: 23.6 [range: 2.3–40.6] years) and 609 (5 studies; 46.1% female; median age: 23.4 [range: 2.4–39.9] years) subjects in the as-needed use of ICS/FABA regimen, the as-needed use of FABA regimen and in the daily use of ICS regimen, respectively. The diagnostic criteria for asthma in the included studies were based on the guidelines recommendation except for the study by Papi et al. [30] on frequent wheezing in the previous 6 months. There was one study on intermittent asthma and 5 studies on mild persistent asthma. All subjects in these included studies were requested to have the adherence of daily ICS with more than 75%. The average FEV1 percentage of predicted value were 95.4 (SD = 13.1), 94.8 (SD = 12.0) and 94.0 (SD = 12.1) for the as-needed use of ICS/FABA, as-needed use of FABA and the daily ICS regimens groups, respectively. The ICS/FABA regimens used included beclomethasone/salbutamol, budesonide/formoterol, beclomethasone and salbutamol, beclomethasone/salbutamol and fluticasone propionate and salbutamol, respectively. The regular ICS regimens used involved beclomethasone, budesonide and fluticasone propionate, respectively. The FABA regimens used were presented as formoterol, terbutaline and salbutamol. The median intervention duration was 24 (ranged from 6 to 44) weeks.
The quality of reporting in the reviewed studies was generally good. The risk of bias is shown in Additional file 1: Table S2. All studies were multicenter trials except Lazarinis et al’s study [28]. All the included studies were randomized double-blind trials, except the study of Papi et al. [30] was an unclear risk in random sequence generation, Lazarinis et al’s study [28] there was an unclear risk in blinding and Haahtela et al’s study [27] there was an unclear risk in allocation concealment and blinding.
Primary outcomes
Compared with the as-needed FABA regimen, the as-needed use of ICS/FABA as monotherapy statistically reduced moderate to severe exacerbations (RR = 0.56, 95%-CI = [0.40, 0.78], P = 0.001, I2 = 56.6%, Fig. 2a, Table 3). The number needed to treat for an additional beneficial outcome (NNTB) was 10 and the number of avoided events per 1000 was 101 (95%-CI = [51, 138]). Compared with regular ICS regimen, the as-needed ICS/FABA regimen had slightly higher risk of moderate to severe exacerbations (RR = 1.39, 95%-CI = [1.08, 1.79], P = 0.011, I2 = 45.4%, Fig. 2b), and the number needed to treat for an additional harmful outcome (NNTH) was 17 and the number of excess events per 1000 was 57 (95%-CI = [12, 116]).

Effects of the as-needed ICS/FABA, daily ICS, and as-needed FABA regimens on moderate to severe exacerbations. a ICS/FABA vs FABA regimen; b ICS/FABA vs ICS regimen; c Risk ratio across three regimens. ICS, inhaled corticosteroids; FABA, fast-onset-acting β2-agonist; ICS/FABA, inhaled corticosteroids/fast-onset-acting β2-agonist
We also explored the difference of severe exacerbations [20] between the as-needed ICS/FABA, the regular ICS and the as-needed FABA regimens (Fig. 3). As a result, the as-needed ICS/FABA regimen significantly reduced severe exacerbations (RR = 0.64, 95%-CI = [0.44, 0.95], P = 0.026, I2 = 0.0%) compared to FABA regimen and the NNTB was 16 and the number of avoided events per 1000 was 62 (95%-CI = [9, 96]). In comparison with the regular ICS regimen, the as-needed ICS/FABA regimen had increased risk of severe exacerbations (RR = 1.34, 95%-CI = [1.02, 1.75], P = 0.034, I2 = 29.2%) and the NNTH was 18 and the number of excess events per 1000 was 56 (95%-CI = [3, 123]).

Effects of the as-needed ICS/FABA, daily ICS, and as-needed FABA regimens on severe exacerbations. a ICS/FABA vs FABA regimen; b ICS/FABA vs ICS regimen; c Risk ratio across three regimens. ICS, inhaled corticosteroids; FABA, fast-onset-acting β2-agonist; ICS/FABA, inhaled corticosteroids/fast-onset-acting β2-agonist
Like the study by Yancey and colleagues [31], we grouped the data of the time to first exacerbation, obtained by GetData Graph Digitizer [32], into a five-day interval life table and established a life-table curves to illustrate the difference in the time to first exacerbation for each of the three treatments (Fig. 4a). As a result, the hazard ratio (HR) for time to first exacerbations after randomization in the ICS/FABA regimen was significant lower when compared with FABA regimen (HR = 0.520, 95%-CI = [0.345, 0.785], P = 0.002) but did not reach statistical difference when compared with ICS regimen (HR = 1.295, 95%-CI = [0.805, 2.083], P = 0.286) (Fig. 4b).

Life-table curves of the time to first exacerbation (a) and hazard ratio (b) across the as-needed ICS/FABA (n = 303), as-needed FABA (n = 248) and regular ICS (n = 288) regimens. ICS, daily use of inhaled corticosteroids regimen; FABA, as-needed use of fast-onset-acting β2-agonist regimen; ICS/FABA, as-needed use of inhaled corticosteroids/fast-onset-acting β2-agonist regimen
The quality of evidence body rated by GRADE for primary outcomes is summarized in Table 4. Compared with the as-needed FABA regimen, the as-needed use of ICS/FABA as monotherapy probably reduces moderate to severe exacerbations and the hazard for the time to first exacerbation (moderate-quality evidence). The as needed ICS/FABA regimen probably has slightly higher risk of moderate to severe exacerbations and increases the hazard for the time to first exacerbation compared with regular ICS regimen (moderate-quality evidence). In addition, compared with FABA regimen, regular ICS regimen probably reduces the hazard for the time to first exacerbation (moderate-quality evidence).
Secondary outcomes
Compared with the FABA regimen, the ICS/FABA regimen showed a decrease in nocturnal awakenings (SMD = −0.29, 95%-CI = [−0.49, −0.09], P = 0.004, I2 = 8.7%, Table 5) and a marked improvement in FEV1% predicted (SMD = 0.77, 95%-CI = [0.11, 1.44], P < 0.001, I2 = 91.3%) but there was no significant difference in the percentage of asthma symptom-free days between these two regimens. The as-needed ICS/FABA regimen had a trend to reduce number of rescue medication required per day but this did not reach a statistical significance (SMD = −0.14, 95%-CI = [−0.29, 0.01], P = 0.076, I2 = 18.0%). In comparison with ICS regimen, the as-needed ICS/FABA regimen had a decreased percentage of asthma symptom-free days (SMD = −0.25, 95%-CI = [−0.37, −0.13], P < 0.001, I2 = 0.0%) and more rescue medication required per day (SMD = 0.19, 95%-CI = [0.08, 0.31], P = 0.001, I2 = 16.2%), but there was no statistical significance in nocturnal awakening times and improvement of FEV1% predicted between these two regimens.
Subgroup analysis
We also performed a subgroup analyses based on adults, and children or adolescents. In the adult subgroup, the as-needed ICS/FABA regimen had a significant decrease in moderate to severe exacerbations compared with the FABA regimen (RR = 0.24, 95%-CI = [0.10, 0.54], P = 0.001, I2 = 0.0%, Table 3) and the NNTB was 8 and the number of avoided events per 1000 was 120 (95%-CI = [73, 142], Table 5) but this failed to reach statistical difference in severe exacerbations (RR = 0.17, 95%-CI = [0.02, 1.35], P = 0.093, I2 = 0.0%). Furthermore, the as-needed ICS/FABA regimen significantly reduced rescue medication required per day (SMD = −0.23, 95% CI = [−0.43, −0.02], P = 0.029, I2 = 0.0%) and improved FEV1% predicted (SMD = 0.41, 95%-CI = [0.19, 0.62], P < 0.001, I2 = 0.0%) compared with the FABA regimen. In addition, we did not find any statistical difference in moderate to severe exacerbations (RR = 0.58, 95%-CI = [0.21, 1.57], P = 0.284), severe exacerbations (RR = 0.12, 95%-CI = [0.01, 2.38], P = 0.166), and other secondary outcomes (Table 5) between the ICS/FABA and regular ICS regimen.
In the children and adolescent subgroup, in comparison to the FABA regimen, the ICS/FABA regimen significantly reduced nocturnal awakenings times (SMD = −0.42, 95%-CI = [−0.75, −0.10], P = 0.010, Table 5) and improved FEV1% predicted (SMD = 1.42, 95%-CI = [1.06, 1.79], P < 0.001), but there was no statistical difference in moderate to severe exacerbations (RR = 0.76, 95%-CI = [0.53, 1.10], P = 0.147, I2 = 0.0%, Table 3) or severe exacerbations (RR = 0.72, 95%-CI = [0.49, 1.07], P = 0.107). When compared with the ICS regimen, the ICS/FABA regimen had higher of exacerbations (RR = 1.50, 95%-CI = [1.15, 1.96], P = 0.003, I2 = 18.4%) and severe exacerbations (RR = 1.40, 95%-CI = [1.07, 1.84], P = 0.014, I2 = 0.0%), a significant reduction in the percentage of asthma symptom-free days (SMD = −0.27, 95%-CI = [−0.41, −0.14], P < 0.001, I2 = 0.0%), more rescue medication required per day (SMD = 0.22, 95%-CI = [0.08, 0.35], P = 0.001, I2 = 49.5%) and reduced FEV1% predicted (SMD = −0.36, 95%-CI, [−0.69, −0.03], P = 0.033), but did not reach statistical significance on the nocturnal awakening times.
Safety
There were 9.4% (n = 58), 15.8% (n = 50) and 7.7% (n = 43) of participates who withdrew from the studies in the ICS/FABA regimen, the FABA regimen and the ICS regimen, respectively, which indicated more dropouts in the FABA regimen when compared to the ICS/FABA and the daily ICS regimens in the children and adolescent subgroup (Additional file 1: Table S3). It reported eight serious adverse events (such as bacterial pneumonia and hemoptysis) in all included studies (Additional file 1: Table S4), which had no difference between regimens. In terms of the linear growth. The study by Martinez et al [29] indicated that, compared with the FABA group, children with the daily use of ICS regimen grew 1.1 cm (SD = 0.3) less (P < 0·0001) during the 44-week treatment period, but no significant growth effect was found in children with the as-needed ICS/FABA regimen (0.3 cm, SD = 0.2, P = 0.26). During the 16-week treatment interval, Fitzpatrick et al [26] found that children with the as-needed use of ICS/FABA regimen grew 0.2011 cm (SE = 0.2097, P = 0.3381) higher than children with the daily use of ICS regimen.
Adherence of the daily use of ICS treatment
An additional meta-analysis was performed to pool the real-life adherence of the daily use of ICS treatment in patients with persistent asthma. The studies selection flow and characteristics of included studies were provided in the Methods and Results sections in the Additional file 1. The adherence of daily ICS regimen was calculated using the proportion of days covered (PDC) and defined as the total number of days with supply dispensed during the follow-up over the number of days of follow-up. Using a random-effects model, ICS adherence was 37.6% (95% CI = [33.1, 42.2], Additional file 1: Table S9).
Discussion
To our best knowledge, this is the first proof-of-concept systematic review and meta-analysis to systematically explore the efficacy and safety of the ICS/FABA regimen in single inhaler as reliever therapy in intermittent and mild asthma. Our study included the six trials with 1300 patients and suggests that the as-needed use of ICS/FABA regimen significantly reduces exacerbations, including severe exacerbations, nocturnal awakening, prolongs time to first exacerbation and improves FEV1% predicted as compared to the as-needed FABA regimen, but it is inferior to the regular ICS regimen except for time to first exacerbation. The safety analysis indicated that the regular ICS regimen especially in a long-term treatment would lead to a small reduction in growth compared to either as-needed ICS/FABA or FABA regimens in the children and adolescent population. Our study shows that the ICS/FABA regimen in a single inhaler as a symptom-driven therapy would be a promising alternative regimen in management of intermittent or mild persistent asthma.
There are two important characteristics about the included RCTs for this meta-analysis. The first is the limited number of subjects involved in this meta-analysis, which resulted in under-powering with less than 0.80 to find statistical difference in some outcomes, especially in the sub-group meta-analysis, although most of the included studies calculated adequate power for their specific primary outcomes rather than ours in this study. The second is all included studies were completed in an ideal setting but not in real-world conditions [33], because all included subjects were requested to have an adherence of more than 75% before recruitment. In the real-world setting, the adherence of daily ICS was only 37.6% (95% CI = [33.1, 42.2]) in our additional meta-analysis. Therefore, the regular ICS regimen would not be more effective than the as-needed ICS/FABA strategy as poor adherence to ICS is correlated with asthma-related outcomes [34].
Despite effective pharmacological options for treating asthma, most patients fail to achieve good control in the real world. Non-adherence is common, with over-reliance on SABA and under-use of ICS frequently being observed. Therefore, there is a real need to consider new approaches to improve outcomes. One regimen that has attracted attention and controversy is single inhaler for maintenance and relief therapy (SMART). The SMART or single inhaler therapy (SiT) means that a single inhaler contains two drugs. One of these drugs acts quickly and termed the ‘reliever’, and the other one works much more slowly and is called the ‘preventer’. patients on SMART have one inhaler for use every day to control their underlying inflammation and also for symptom relief. The timely ICS use at the time of increased symptoms can improve asthma outcomes by reducing exacerbation risk [35]. In recent decades, evidence has demonstrated that using combined ICS and FABA as reliever medication can reduce the exacerbation rate [36,37,38] and have a lower total ICS exposure, without compromising outcomes against current best practice strategies using a fixed-dose ICS/LABA combination inhaler. But most of this evidence comes from moderate to severe asthma patients, who have a greater risk of exacerbations. Thus, GINA [1] recommended ICS/formoterol, a ICS/FABA inhaler, as reliever medication for moderate to severe asthma patients except for patients with intermittent and mild asthma. In our study, we extended this efficacy to the population with intermittent and mild asthma in significant improvements of nocturnal awakening times, FEV1% predicted, exacerbations and the time to first exacerbation compared the as-needed use of ICS/FABA regimen with the as-needed FABA regimen.
A possible concern with as-needed ICS/FABA is that inadequate anti-inflammatory treatment may be given to some patients, who would be at higher risk of exacerbations. Treatment with daily ICS at low doses decreases the risk of severe exacerbations and improves asthma control in patients with mild persistent asthma [39, 40]. Good adherence is needed for the efficiency of daily ICS therapy, but patients trend to use ICS intermittently and occasionally [15, 16]. Previous research has shown that nonadherence of ICS results in poor clinical control and increases school and work absenteeism, unscheduled health-care utilization, morbidity, and mortality [34, 41, 42]. We performed an additional meta-analysis in the adherence of the daily ICS therapy in a real-world setting in this study, and found the real-life adherence of daily use of ICS was 37.6% (95% CI = [33.1, 42.2]) with obvious heterogeneity between real-world RCTs and observational studies (Additional file 1: Table S9), while, it was more than 75% in our included studies significantly related to the reduced asthma exacerbations [43]. With regard to potential corticosteroid side effects, treatment with the as-needed ICS/FABA regimen was characterized by a lower average ICS dose and in children or adolescent population, by a higher linear growth than treatment with regular daily ICS regimen.
Based on the results of our study, the current recommendation from guidelines that regular ICS should be initiated only when patients use their SABA more than twice per week needs to be revisited, because the evidence that this approach works in real-life clinical practice is limited. The potential benefits of this approach were compromised by both low rates of ICS prescription in patients, even in the setting of poor control, and poor adherence by patients who were prescribed ICS regimen. Accordingly, the as-needed ICS/FABA regimen would be a promising alternative therapy, which might represent an effective, safe, and novel therapy for the treatment of intermittent and mild asthma. It may be particularly useful for selected patients who adhere poorly to their regular daily ICS regimen.
From a clinical point of view, the as-needed use of ICS/FABA regimen is a promising choice for the long-term management of intermittent and mild asthma. Exacerbations are major determinants of the direct cost of asthma, and preventing exacerbations is one of the key goals in asthma management [44]. In our study, compared with the as-needed use of FABA regimen, the as-needed use of ICS/FABA as monotherapy statistically reduced moderate to severe exacerbations and severe exacerbations. In addition, the number of patients that need to be treated for one of them to benefit from decreased moderate to severe exacerbations compared with the as-needed use of FABA regimen was 10 (the number of moderate to severe exacerbations that to be decreased from treating 1000 patients compared with the as-needed use of FABA regimen was 101 ((95%-CI = [51, 138])) and the number of patients that need to be treated for one of them to benefit from decreased severe exacerbations compared with the as-needed use of FABA regimen was 16 (the number of severe exacerbations that to be decreased from treating 1000 patients compared with the as-needed use of FABA regimen was 62 (95%-CI = [9, 96])). On the other hand, as we had mentioned above, good adherence is needed for the efficiency of daily ICS therapy, and there are some interventions to improve adherence to ICS may take many forms, including audiovisual reminders [45, 46], electronic monitoring [46], interactive voice response system via mobile phone [47], text message reminders [48] and parent education [49]. However, the magnitude of the improvements in adherence was generally not large (range from 4% to 20%) [50]. This improvement does not ensure the good adherence of ICS regimen (75%). Besides, the successful interventions to promote adherence were complex and multi-faceted and included combinations of counselling, education, more convenient care, self-monitoring, reinforcement, reminders, and other forms of additional attention or supervision [51, 52].
There are several limitations to this study that needs to be addressed. First, this study aimed to demonstrate the proof-of-concept whether the ICS/FABA in a single inhaler as reliever therapy in intermittent and mild persistent asthma was feasible in clinical practice, therefore two of included studies [29, 30] involved the use of the ICS and the FABA in separate inhalers but not in a single inhaler. Second, we included the limited number of studies that had inadequate power to find some difference in the subgroup analysis. Third, we used GetData Graph Digitizer to mine data and the Cochrane handbook recommended principals to deal with missing data, which would result in some potential impact on outcomes. Fourth, there was obvious heterogeneity in some outcomes such as the moderate to severe exacerbations, but it could be partly explained by different age groups. Fifth, all included RCTs were completed in an ideal condition with more than 75% of adherence rather than a real-world setting. To provide additional information in real-life adherence of regular ICS regimen, we pooled the rates of adherence across real-world RCTs and observational studies.
Conclusions
In conclusion, our study suggests that the as-needed use of ICS/FABA regimen significantly reduces exacerbations, nocturnal awakening times, extend time to first exacerbation and improves FEV1% predicted compared to the as-needed FABA regimen, but it is inferior to the regular ICS regimen except for time to first exacerbation. With regard to potential corticosteroid side effects, it indicated that the regular ICS regimen especially in a long-term treatment would lead to grow less than either the as-needed ICS/FABA or FABA regimens in the children and adolescent population. This study displays that the ICS/FABA regimen in a single inhaler as a symptom-driven therapy would be a promising alternative regimen particularly for the very patients with intermittent or mild asthma who adhere poorly to their regular ICS regimen. However, further real-world RCTs are needed to confirm these findings.
Abbreviations
- BDP:
-
Beclomethasone dipropionate
- CI:
-
Confidence interval
- FEV1 :
-
Forced expiratory volume in one second
- HR:
-
Hazard ratio
- ICS:
-
Inhaled corticosteroids
- ICS/FABA:
-
The combination corticosteroid/fast-onset-acting β2-agonist
- LABA:
-
Long-acting β2-agonists
- NNT:
-
The number needed to treat
- NNTB:
-
The number needed to treat for an additional beneficial outcome
- NNTH:
-
The number needed to treat for an additional harmful outcome
- PDC:
-
The proportion of days covered
- RR:
-
Risk ratio
- SABA:
-
Short-acting β2-agonist
- SMD:
-
The standardized mean difference
References
Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention, 2016. Available from: www.ginasthma.org.
Masoli M, Fabian D, Holt S, Beasley R. The global burden of asthma: executive summary of the GINA dissemination committee report. Allergy. 2004;59(5):469–78.
The Global Asthma Report. Auckland. New Zealand: Global Asthma Network; 2014. Available from: http://www.globalasthmanetwork.org/publications/Global_Asthma_Report_2014.pdf
Chung KF, Wenzel SE, Brozek JL, Bush A, Castro M, Sterk PJ, et al. International ERS/ATS guidelines on definition, evaluation and treatment of severe asthma. Eur Respir J. 2014;43(2):343–73.
Jarjour NN, Erzurum SC, Bleecker ER, Calhoun WJ, Castro M, Comhair SA, et al. Severe asthma: lessons learned from the National Heart, Lung, and Blood Institute severe asthma research program. Am J Respir Crit Care Med. 2012;185(4):356–62.
Wang G, Wang F, Gibson PG, Guo M, Zhang WJ, Gao P, et al. Severe and uncontrolled asthma in China: a cross-sectional survey from the Australasian severe asthma network. J Thorac Dis. 2017;9(5):1333–44.
Kwok MY, Walsh-Kelly CM, Gorelick MH, Grabowski L, Kelly KJ. National Asthma Education and prevention program severity classification as a measure of disease burden in children with acute asthma. Pediatrics. 2006;117(4 Pt 2):S71–7.
Rabe KF, Adachi M, Lai CK, Soriano JB, Vermeire PA, Weiss KB, et al. Worldwide severity and control of asthma in children and adults: the global asthma insights and reality surveys. J Allergy Clin Immunol. 2004;114(1):40–7.
Wang L, Liang R, Zhou T, Zheng J, Liang BM, Zhang HP, et al. Identification and validation of asthma phenotypes in Chinese population using cluster analysis. Ann Allergy Asthma Immunol. 2017;119(4):324–32.
Ding B, Small M. Disease burden of mild asthma: findings from a cross-sectional real-world survey. Adv Ther. 2017;34(5):1109–27.
Using beta 2-stimulants in asthma. Drug Ther Bull. 1997;35(1):1–4. http://dtb.bmj.com/content/35/1/1.long.
Gill SK, Marriott HM, Suvarna SK, Peachell PT. Evaluation of the anti-inflammatory effects of beta-adrenoceptor agonists on human lung macrophages. Eur J Pharmacol. 2016;793:49–55.
National Heart, Lung and Blood Institute, National Asthma Education and Prevention Program. Expert panel report 3: guidelines for the diagnosis and management of asthma. Full report 2007. Available at: http://www.sciencedirect.com/science/article/pii/S0091674907018234?via%3Dihub. Accessed 20 Jan 2017.
British Thoracic Society Scottish Intercollegiate Guidelines Network. British Guideline on the Management of Asthma. Thorax. 2008;63(Suppl 4):iv1–121.
Stempel DA, Stoloff SW, Carranza Rosenzweig JR, Stanford RH, Ryskina KL, Legorreta AP. Adherence to asthma controller medication regimens. Respir Med. 2005;99(10):1263–7.
Suissa S, Ernst P, Benayoun S, Baltzan M, Cai B. Low-dose inhaled corticosteroids and the prevention of death from asthma. N Engl J Med. 2000;343(5):332–6.
Papi A, Canonica GW, Maestrelli P, Paggiaro P, Olivieri D, Pozzi E, et al. Rescue use of beclomethasone and albuterol in a single inhaler for mild asthma. N Engl J Med. 2007;356(20):2040–52.
Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg (London, England). 2010;8(5):336–41.
Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.handbook.cochrane.org.
Reddel HK, Taylor DR, Bateman ED, Boulet LP, Boushey HA, Busse WW, et al. An official American Thoracic Society/European Respiratory Society statement: asthma control and exacerbations: standardizing endpoints for clinical asthma trials and clinical practice. Am J Respir Crit Care Med. 2009;180(1):59–99.
Fedorov, S., 2002. GetData Graph Digitizer version 2.24. Available at www.getdata-graph-digitizer.com.
Furukawa TA, Barbui C, Cipriani A, Brambilla P, Watanabe N. Imputing missing standard deviations in meta-analyses can provide accurate results. J Clin Epidemiol. 2006;59(1):7–10.
DerSimonian R, Laird N. Meta-analysis in clinical trials revisited. Contemp Clin Trials. 2015;45(Pt A):139–45.
Mantel N, Haenszel W. Statistical aspects of the analysis of data from retrospective studies of disease. J Natl Cancer Inst. 1959;22(4):719–48.
Schünemann H BJ, Guyatt G, Oxman A, editors. GRADE handbook for grading quality of evidence and strength of recommendations. 2013. The GRADE Working Group 2013. Available at: https://gdt.gradepro.org/app/handbook/handbook.html.
Fitzpatrick AM, Jackson DJ, Mauger DT, Boehmer SJ, Phipatanakul W, Sheehan WJ, et al. Individualized therapy for persistent asthma in young children. J Allergy Clin Immunol. 2016;21:21.
Haahtela T, Tamminen K, Malmberg LP, Zetterstrom O, Karjalainen J, Yla-Outinen H, et al. Formoterol as needed with or without budesonide in patients with intermittent asthma and raised NO levels in exhaled air: a SOMA study. Eur Respir J. 2006;28(4):748–55.
Lazarinis N, Jorgensen L, Ekstrom T, Bjermer L, Dahlen B, Pullerits T, et al. Combination of budesonide/formoterol on demand improves asthma control by reducing exercise-induced bronchoconstriction. Thorax. 2014;69(2):130–6.
Martinez FD, Chinchilli VM, Morgan WJ, Boehmer SJ, Lemanske RF, Mauger DT, et al. Use of beclomethasone dipropionate as rescue treatment for children with mild persistent asthma (TREXA): a randomised, double-blind, placebo-controlled trial. Lancet (London, England). 2011;377(9766):650–7.
Papi A, Nicolini G, Baraldi E, Boner AL, Cutrera R, Rossi GA, et al. Regular vs prn nebulized treatment in wheeze preschool children. Allergy. 2009;64(10):1463–71.
Yancey SW, Ortega HG, Keene ON, Mayer B, Gunsoy NB, Brightling CE, et al. Meta-analysis of asthma-related hospitalization in mepolizumab studies of severe eosinophilic asthma. J Allergy Clin Immunol. 2017;139(4):1167–75.e2.
Zhou L, Jiang Y, Yan T, Di G, Shen Z, Shao Z, et al. The prognostic role of cancer stem cells in breast cancer: a meta-analysis of published literatures. Breast Cancer Res Treat. 2010;122(3):795–801.
Price DB. Time to get real: critical and imperative change required in evidence evaluation. J Thorac Dis. 2016;8(Suppl 5):S431–4.
Williams LK, Pladevall M, Xi H, Peterson EL, Joseph C, Lafata JE, et al. Relationship between adherence to inhaled corticosteroids and poor outcomes among adults with asthma. J Allergy Clin Immunol. 2004;114(6):1288–93.
Rabe KF, Atienza T, Magyar P, Larsson P, Jorup C, Lalloo UG. Effect of budesonide in combination with formoterol for reliever therapy in asthma exacerbations: a randomised controlled, double-blind study. Lancet. 2006;368(9537):744–53.
Scicchitano R, Aalbers R, Ukena D, Manjra A, Fouquert L, Centanni S, et al. Efficacy and safety of budesonide/formoterol single inhaler therapy versus a higher dose of budesonide in moderate to severe asthma. Curr Med Res Opin. 2004;20(9):1403–18.
O'Byrne PM, Bisgaard H, Godard PP, Pistolesi M, Palmqvist M, Zhu Y, et al. Budesonide/formoterol combination therapy as both maintenance and reliever medication in asthma. Am J Respir Crit Care Med. 2005;171(2):129–36.
Cates CJ, Karner C. Combination formoterol and budesonide as maintenance and reliever therapy versus current best practice (including inhaled steroid maintenance), for chronic asthma in adults and children. Cochrane Database Syst Rev. 2013;4:Cd007313.
Pauwels RA, Pedersen S, Busse WW, Tan WC, Chen YZ, Ohlsson SV, et al. Early intervention with budesonide in mild persistent asthma: a randomised, double-blind trial. Lancet. 2003;361(9363):1071–6.
O'Byrne PM, Barnes PJ, Rodriguez-Roisin R, Runnerstrom E, Sandstrom T, Svensson K, et al. Low dose inhaled budesonide and formoterol in mild persistent asthma: the OPTIMA randomized trial. Am J Respir Crit Care Med. 2001;164(8 Pt 1):1392–7.
Birkhead G, Attaway NJ, Strunk RC, Townsend MC, Teutsch S. Investigation of a cluster of deaths of adolescents from asthma: evidence implicating inadequate treatment and poor patient adherence with medications. J Allergy Clin Immunol. 1989;84(4 Pt 1):484–91.
Milgrom H, Bender B, Ackerson L, Bowry P, Smith B, Rand C. Noncompliance and treatment failure in children with asthma. J Allergy Clin Immunol. 1996;98(6 Pt 1):1051–7.
Williams LK, Peterson EL, Wells K, Ahmedani BK, Kumar R, Burchard EG, et al. Quantifying the proportion of severe asthma exacerbations attributable to inhaled corticosteroid nonadherence. J Allergy Clin Immunol. 2011;128(6):1185–91.e2.
Fitzgerald JM, Bateman E, Hurd S, Boulet LP, Haahtela T, Cruz AA, et al. The GINA asthma challenge: reducing asthma hospitalisations. Eur Respir J. 2011;38(5):997–8.
Charles T, Quinn D, Weatherall M, Aldington S, Beasley R, Holt S. An audiovisual reminder function improves adherence with inhaled corticosteroid therapy in asthma. J Allergy Clin Immunol. 2007;119(4):811–6.
Onyirimba F, Apter A, Reisine S, Litt M, McCusker C, Connors M, et al. Direct clinician-to-patient feedback discussion of inhaled steroid use: its effect on adherence. Ann Allergy Asthma Immunol. 2003;90(4):411–5.
Mulvaney SA, Ho YX, Cala CM, Chen Q, Nian H, Patterson BL, et al. Assessing adolescent asthma symptoms and adherence using mobile phones. J Med Internet Res. 2013;15(7):e141.
Johnson KB, Patterson BL, Ho YX, Chen Q, Nian H, Davison CL, et al. The feasibility of text reminders to improve medication adherence in adolescents with asthma. JAMIA. 2016;23(3):449–55.
Bender BG. Overcoming barriers to nonadherence in asthma treatment. J Allergy Clin Immunol. 2002;109(6 Suppl):S554–9.
Normansell R, Kew KM, Stovold E. Interventions to improve adherence to inhaled steroids for asthma. Cochrane Database Syst Rev. 2017;4:Cd012226.
Haynes RB, McDonald H, Garg AX, Montague P. Interventions for helping patients to follow prescriptions for medications. Cochrane Database Syst Rev. 2002;2:Cd000011.
Clarenbach CF, Nicod LP, Kohler M. Real-world asthma management with inhaler devices in Switzerland-results of the asthma survey. J Thorac Dis. 2016;8(11):3096–104.
British Thoracic Society, Scottish Intercollegiate Guidelines Network. British guideline on the management of asthma. Thorax. 2014;69(Suppl 1):1–192.
Chinese Medical Association of respiratory disease branch Asthma Study Group. [The Chinese guideline for asthma management and prevention]. Zhonghua Jie He He Hu Xi Za Zhi 2016;39(9):675–697. doi:https://doi.org/10.3760/cma.j.issn.1001-0939.2016.09.007. Chinese.
GEMA. 2009 (Spanish guideline on the management of asthma). J Investig Allergol Clin Immunol. 2010;20(Suppl 1):1–59.
Ichinose M, Sugiura H, Nagase H, Yamaguchi M, Inoue H, Sagara H, et al. Japanese guidelines for adult asthma 2017. Allergol Int. 2017;66(2):163–89.
Al-Moamary MS, Alhaider SA, Idrees MM, Al Ghobain MO, Zeitouni MO, Al-Harbi AS, et al. The Saudi initiative for asthma - 2016 update: guidelines for the diagnosis and management of asthma in adults and children. Ann Thorac Med. 2016;11(1):3–42.
Acknowledgements
All authors thank Prof. Eric D. Bateman, Division of Pulmology, Department of Medicine, University of Cape Town, South Africa, for providing important intellectual comments to this manuscript.
Funding
This study was supported by the National Natural Science Foundation of China (no. 81370122, 81570023 and 81670023), Science and Technology Foundation of Sichuan Province (2015SZ0121), Science and Technology Foundation of Chengdu (2014-HM01–00294-SF), the Youth Science Funding of Sichuan University (no. 2011SCU04B17), and the Program for New Century Excellent Talents in University (no. NCET-12-0380).
Availability of data and materials
The authors declare that all data supporting the findings of this study are available within the following articles and its supplementary information files.
1, Fitzpatrick AM, Jackson DJ, Mauger DT, Boehmer SJ, Phipatanakul W, Sheehan WJ, et al. Individualized Therapy for Persistent Asthma in Young Children. J Allergy Clin Immunol. 2016;138(6):1608-1618.http://www.sciencedirect.com/science/article/pii/S0091674916312179
2, Haahtela T, Tamminen K, Malmberg LP, Zetterstrom O, Karjalainen J, Yla-Outinen H, et al. Formoterol as needed with or without budesonide in patients with intermittent asthma and raised NO levels in exhaled air: A SOMA study. The European respiratory journal. 2006;28(4):748–55. http://erj.ersjournals.com/content/erj/28/4/748.full.pdf
3, Lazarinis N, Jorgensen L, Ekstrom T, Bjermer L, Dahlen B, Pullerits T, et al. Combination of budesonide/formoterol on demand improves asthma control by reducing exercise-induced bronchoconstriction. Thorax. 2014;69(2):130–6. http://thorax.bmj.com/content/thoraxjnl/69/2/130.full.pdf
4, Martinez FD, Chinchilli VM, Morgan WJ, Boehmer SJ, Lemanske RF, Mauger DT, et al. Use of beclomethasone dipropionate as rescue treatment for children with mild persistent asthma (TREXA): a randomised, double-blind, placebo-controlled trial. Lancet (London, England). 2011;377(9766):650–7. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4852146/
5, Papi A, Canonica GW, Maestrelli P, Paggiaro P, Olivieri D, Pozzi E, et al. Rescue use of beclomethasone and albuterol in a single inhaler for mild asthma. The New England journal of medicine. 2007;356(20):2040–52. http://www.nejm.org/doi/full/10.1056/nejmoa063861
6, Papi A, Nicolini G, Baraldi E, Boner AL, Cutrera R, Rossi GA, et al. Regular vs prn nebulized treatment in wheeze preschool children. Allergy. 2009;64(10):1463–71. http://onlinelibrary.wiley.com/doi/10.1111/j.1398-9995.2009.02134.x/epdf
Author information
Authors and Affiliations
Contributions
GW made substantial contributions to conception and design, acquisition of data, analysis and interpretation of data and drafting the manuscript. XZ made substantial contributions to conception and design, acquisition of data, and analysis and interpretation of data. HPZ made substantial contributions to conception and design and revised the manuscript critically for important intellectual content. LW made substantial contributions to conception and design and revised the manuscript critically for important intellectual content. DYK revised the manuscript critically for important intellectual content. PJB revised the manuscript critically for important intellectual content. Professor GW made substantial contributions to conception and design, acquisition of data, analysis and interpretation of data, and drafting the manuscript and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
P.J. Barnes has served on Scientific Advisory Boards of AstraZeneca, Boehringer-Ingelheim, Chiesi, GlaxoSmithKline, Glenmark, Johnson & Johnson, Napp, Novartis, Takeda, Pfizer, Prosonix, RespiVert, Teva and Zambon and has received research funding from AstraZeneca, Boehringer-Ingelheim, Chiesi, Novartis and Takeda. GW, XZ, HPZ, LW, DYK and GW declare that there are no competing interests associated with the study.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional files
Additional file 1:
The online material of corticosteroid plus β2-agonist in a single inhaler as reliever therapy in intermittent and mild asthma: A proof-of-concept systematic review and meta-analysis. (DOCX 80 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Wang, G., Zhang, X., Zhang, H.P. et al. Corticosteroid plus β2-agonist in a single inhaler as reliever therapy in intermittent and mild asthma: a proof-of-concept systematic review and meta-analysis. Respir Res 18, 203 (2017). https://doi.org/10.1186/s12931-017-0687-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12931-017-0687-6