
Abstract
Introduction
Short-acting β2-agonist (SABA) reliever overuse is common in asthma, despite availability of inhaled corticosteroid (ICS)-based maintenance therapies, and may be associated with increased risk of adverse events (AEs). This systematic literature review (SLR) and meta-analysis aimed to investigate the safety and tolerability of SABA reliever monotherapy for adults and adolescents with asthma, through analysis of randomized controlled trials (RCTs) and real-world evidence.
Methods
An SLR of English-language publications between January 1996 and December 2021 included RCTs and observational studies of patients aged ≥ 12 years treated with inhaled SABA reliever monotherapy (fixed dose or as needed) for ≥ 4 weeks. Studies of terbutaline and fenoterol were excluded. Meta-analysis feasibility was dependent on cross-trial data comparability. A random-effects model estimated rates of mortality, serious AEs (SAEs), and discontinuation due to AEs (DAEs) for as-needed and fixed-dose SABA treatment groups. ICS monotherapy and SABA therapy were compared using a fixed-effects model.
Results
Forty-two studies were identified by the SLR for assessment of feasibility. Final meta-analysis included 24 RCTs. Too few observational studies (n = 2) were available for inclusion in the meta-analysis. One death unrelated to treatment was reported in each of the ICS, ICS + LABA, and fixed-dose SABA groups. No other treatment-related deaths were reported. SAE and DAE rates were < 4%. DAEs were reported more frequently in the SABA treatment groups than with ICS, potentially owing to worsening asthma symptoms being classified as an AE. SAE risk was comparable between SABA and ICS treatments.
Conclusions
Meta-analysis of data from RCTs showed that deaths were rare with SABA reliever monotherapy, and rates of SAEs and DAEs were comparable between SABA reliever and ICS treatment groups. When used appropriately within prescribed limits as reliever therapy, SABA does not contribute to excess rates of mortality, SAEs, or DAEs.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Inhaled short-acting β2-agonists (SABA) have been widely used to relieve acute asthma symptoms since the 1950s; however, some evidence suggests that SABA overuse may be associated with increased risk of adverse events (AEs). |
An unmet need exists for evidence of the safety of SABA therapy when used for symptom relief in patients with asthma. |
This SLR and meta-analysis, investigating SABA safety data from randomized controlled trials over the past 25 years, showed that deaths were rare and SAEs were uncommon in patients with asthma treated with SABA reliever monotherapy, and few patients in SABA reliever therapy treatment arms discontinued owing to AEs. |
Similar results were noted across both the SABA reliever treatment groups and ICS-based maintenance therapy groups. |
These results support the use of SABA reliever therapy when administered appropriately within prescribed limits, providing a timely contribution to current discourse on the use of SABA reliever therapies in clinical practice. |
Introduction
Current management of asthma involves use of medications to target relief of acute symptoms or provide long-term symptom control [1]. Short-acting β2-agonist (SABA) therapy has been the most widely used rescue medication for relief of acute asthma symptoms since the 1950s [2,3,4] with salbutamol (also referred to as albuterol) introduced in 1968 [4]. However, since 2019 the Global Initiative for Asthma (GINA) has moved away from recommending SABA as the preferred option for reliever therapy, either alone or in conjunction with inhaled corticosteroid (ICS) maintenance therapy [5, 6]. GINA currently recommends two treatment tracks for the management of asthma defined by the choice of reliever therapy, either as-needed ICS-formoterol or as-needed SABA [6].
Despite the wide range of available maintenance therapies, overuse of SABA by patients with asthma for symptom relief appears to be associated with underuse of maintenance asthma therapies [7]. Database studies using a retrospective cohort [SABA use IN Asthma (SABINA) program] reported an increased risk of adverse outcomes associated with SABA overuse across the spectrum of asthma severity, which has led to speculation that SABA overuse and dependency may be associated with an increased risk of mortality and an increase in asthma-related healthcare utilization [8].
This has added to historical concerns relating to the safety of SABA therapies, particularly those that emerged as a result of the epidemics of asthma mortality in the 1960s and 1970s and were associated with high-dose preparations of isoproterenol and fenoterol [9, 10]. The clinically important studies of SABA safety outcomes in New Zealand and Canada in the early 1990s further reinforced these concerns by showing excess mortality associated with greater use of fenoterol [11,12,13,14,15]. SABA therapies such as salbutamol and terbutaline have not been associated with an increased risk of mortality [10].
Proactive regular dosing is associated with reduced mortality from asthma [16], exacerbation risk [17], and airway inflammation [18]. The appropriate use of SABA as a reliever in conjunction with regularly dosed ICS-based maintenance therapy may facilitate more controlled dosing.
The aims of this systematic literature review (SLR) and meta-analysis were to identify and summarize published data reporting the safety and tolerability of SABA as a reliever therapy for adults and adolescents with asthma from randomized control trials (RCTs) or a real-world setting, and to obtain pooled incidence of mortality and serious adverse events (SAEs) for SABA monotherapy versus ICS with or without long-acting β2-agonist (LABA) therapy.
Methods
Study Design
An SLR was conducted to identify published studies with data relating to the safety (specifically mortality and SAEs) of SABAs in adults and adolescents with asthma, followed by an assessment of feasibility to quantitatively compare safety outcomes between SABA monotherapy as a reliever and treatments of interest via meta-analysis. Finally, meta-analyses were conducted on the selected studies for all outcomes of interest.
Systematic Literature Review
The SLR was conducted in accordance with the methodology outlined by the Cochrane Collaboration, Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines, and the National Institute for Health and Care Excellence (NICE). SLR methods were defined by a prospectively designed study protocol that was registered in PROSPERO (PROSPERO ID: CRD42022320237).
Primary co-endpoints of interest were the proportion of patients with mortality due to any cause reported at any timepoint (all-cause mortality) and the proportion of patients with mortality due to treatment reported at any timepoint (treatment-related mortality). Secondary outcomes were the proportion of patients with treatment-related adverse events (TRAEs), SAEs, and safety-related treatment discontinuations reported at any timepoint (DAEs).
Identification of Studies
Systematic literature searches were conducted in MEDLINE and Embase via Ovid SP using free-text search terms and specific terms for the disease, treatment, relevant study design filters, and a time limitation to the last 25 years. The search terms used are presented in Tables S1 and S2 of the supplementary appendix.
Following removal of duplicates, a reference list of the identified studies was exported to an EndNote library (version X9) and uploaded to Distiller Systematic Review software, an online program that transparently facilitates the selection process.
Two independent reviewers (A.M. and L.M.) screened each title, abstract, and full-text article on the basis of the predefined population, intervention, comparator, outcomes, study design, and time (PICOS-T) inclusion/exclusion criteria. A third independent reviewer (A.K.) resolved any disagreements regarding article eligibility. All reviewers were independent of the study sponsor.
To supplement the database searches, abstracts and presentations from the 2020–2022 meetings of the following conferences were reviewed: European Respiratory Society (ERS), European Academy of Allergy and Clinical Immunology (EAACI), American Academy of Allergy, Asthma and Immunology (AAAAI), American Thoracic Society (ATS), and British Thoracic Society (BTS). The reference lists of eligible SLRs were also reviewed manually as per the search criteria to ensure comprehensive identification of relevant studies.
Study Selection
Clinical trials and observational studies were eligible for inclusion if they enrolled adults and adolescents (≥ 12 years old) diagnosed with asthma and were published in English between 1 January 1996 and 9 December 2021. Studies conducted before 1996 were not considered for inclusion as they were frequently observational with confounding factors related to mortality. Additionally, most studies pre-1996 related to treatment with high-dose isoproterenol or fenoterol. Following regulatory intervention, formulations with lower doses were used clinically and, in turn, mortality rates reduced [19]. Therefore, studies conducted before regulatory intervention do not support the objective of assessing appropriate SABA reliever use (in particular salbutamol) within prescribed limits and were not included.
The treatment of interest was SABA reliever monotherapy, either on a fixed-dose schedule or as needed for symptom relief, with a duration of at least 4 weeks. Placebo arms permitting as-needed SABA as a reliever therapy were also considered as SABA monotherapy. Relevant comparators included SABA monotherapy (a different schedule or inhaler type) or inhaled asthma medications (e.g., ICS ± LABA) with SABA as needed (including placebo arms). Single-arm studies were eligible, as a comparator was not required. A full summary of the PICOS-T eligibility criteria is presented in Table 1.
Data Extraction
Data extraction was performed using a customized data extraction template (DET) that was developed in Microsoft Excel [for Microsoft 365 MSO (16.0.14326.21008) 32-bit] for this study. During data extraction, a zero incidence was imputed for RCTs not reporting mortality events, as trial ethics require this type of event to be reported.
A single independent investigator trained in the critical assessment of evidence captured the data using the DET, and a second independent investigator validated all extracted data against the source article to ensure accuracy and completeness. Discrepancies between investigators were resolved in discussion with a third, senior investigator by comparing the collected data with information provided in the published article. As recommended by NICE, the Cochrane Risk of Bias Assessment Tool was used to assess the risk of bias of included trials [20].
Feasibility Assessment
The feasibility of conducting meta-analysis to quantitatively compare overall mortality rates and other secondary AE outcomes for SABA reliever monotherapy with those of SABA reliever in combination with ICS ± LABA therapy was assessed. Similarity of study design, treatment characteristics, and comparability of patients across trials, as well as confounding factors with respect to populations (age, asthma severity, smoking history, treatment history), were examined. Differences in definitions and timing of safety outcomes were also assessed.
Meta-analysis
Following assessment of feasibility, meta-analysis of proportions extracted/calculated for each study was conducted for all outcomes of interest. The planned meta-analyses including the primary outcomes of interest (mortality) and other outcomes and timepoints of interest are summarized in Table 2.
Meta-analysis was performed on aggregate studies for data available as a dichotomous dependent variable. Mortality, SAEs, and DAEs for as-needed and fixed-dose SABA were estimated using a random-effects meta-analytic approach (REM) from logit-transformed proportions, assuming a non-zero random-effects variance, whereas ICS monotherapy was compared with SABA using a fixed effects meta-analytic approach (FEM) from log-odds ratios, assuming homogeneity of study effects. Outputs from the meta-analysis are reported as logit proportions and 95% confidence intervals (CI) for the REM model and as odds ratios and 95% CI for the FEM model.
Heterogeneity was measured using Cochran’s Q and the I2 measure [21]. An I2 value of 0% indicated no observed heterogeneity. Where significant and substantive heterogeneity in effects was observed, sensitivity analysis was performed to explore whether the heterogeneity was attributable to a few outlying studies or was consistent across the full sample of studies.
Final analysis was conducted for three treatment groups: SABA monotherapy fixed-dose pooled estimate, SABA monotherapy as-needed dose pooled estimate, and ICS monotherapy versus SABA.
For studies that evaluated ICS versus SABA, if a third treatment (e.g., leukotriene receptor antagonist therapy) was included it was not included in the meta-analysis.
Ethics Approval
This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Results
Systematic Literature Review
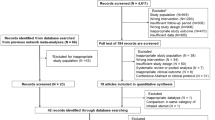
Details of the SLR are shown in Fig. 1. The SLR identified 2586 unique abstract records from the Medline and EMBASE databases following removal of duplicates. Screening of these abstracts identified 164 full-text articles that were assessed for inclusion in the SLR.

PRISMA diagram illustrating the outcomes of the systematic literature review
Elimination based on eligibility criteria identified 42 records for inclusion in the SLR. The most common reasons for full-text exclusion were the intervention not being of interest (n = 48) and outcomes inseparable by patient age, disease, or intervention (n = 25). Of the 42 studies included in the SLR, 40 were RCTs and 2 were observational studies.
As the 2 observational studies were not comparable in design, the 40 RCTs were evaluated in the feasibility assessment, from which it was determined that 24 would be included in the final meta-analysis. Notable excluded publications within the date limits were the Abramson 2001 [22] study (investigating the role of β-agonists in asthma mortality), as mortality was not reported as a safety outcome; Nelson 2006 [23], as no intervention of interest was studied; and the SYGMA 2 2018 study [24], as terbutaline was not a SABA treatment of interest in the SLR PICOS-T criteria.
Only two of the identified studies [25, 26] reported patient deaths (n = 3), and these were determined to be unrelated to the study treatments [SABA (n = 1) or ICS ± LABA (n = 2)] by the study investigators.
Feasibility Assessment
Feasibility assessment determined that the base-case meta-analyses would be restricted to RCTs with a minimum of 12 weeks duration as this was the most common timepoint assessed in the studies. No study was excluded on the basis of differences in baseline characteristics or outcome definition. Asthma of any severity was included in the base-case analysis; however, a sensitivity analysis was recommended for studies enrolling patients with mild or mild-to-moderate asthma to determine if asthma severity had an impact on safety events. No analysis was performed to compare ICS + LABA with SABA owing to insufficient data for mortality, SAEs, and DAEs. Treatment-related mortality was not reported in any study and therefore could not be analyzed. TRAEs were not analyzed as the studies reported outcomes in various formats and frequently included asthma symptoms as part of the definition. A full summary of the study, patient, and treatment characteristics included in the feasibility assessment along with the reasons for exclusion from the meta-analysis where applicable is presented in Table S3 of the supplementary appendix.
Study Characteristics
Details of the 24 trials included in the final meta-analysis are presented in Table 3. All were multicentric, and most (n = 18) were conducted in the USA. Trials enrolled between 115 and 895 participants; mean age was 28–49 years, and the proportion of female participants was between 31% and 67%. In ten studies that reported smoking status, 4–11% of patients reported currently smoking and 12–23% reported a history of smoking. No study reported comorbidities of interest (gastrointestinal reflux disease, nasal polyps, and chronic rhinitis).
The main asthma therapy used by patients prior to trial enrollment was ICS with or without additional maintenance therapies. The breakdown of asthma therapies used before enrollment was: any ICS (32–100%), ICS monotherapy (60%), ICS/LABA (39–44%), LABA monotherapy (21–34%).
All trials evaluated SABA as a reliever therapy: 20 of 24 trials included a placebo arm with SABA reliever monotherapy used as needed as a rescue medication; 11 assessed the safety of SABA as a fixed-dose treatment; 12 evaluated ICS monotherapy versus SABA reliever monotherapy; and 3 evaluated ICS + LABA versus placebo with SABA reliever therapy.
The Cochrane Risk of Bias Assessment Tool was used to assess the risk of bias of included trials. All included studies were judged to be of moderate-to-good quality. In all trials, the treatments were randomly assigned to the subjects; however, the allocation sequence was concealed in just four studies. In three trials, participants, carers, and people delivering the interventions were aware of the intervention assigned to the participants. All trials included appropriate analysis to estimate the effect of assignment to intervention. Among the trials, outcome data were reported in all/nearly all participants randomized; also, appropriate methods were undertaken to measure these outcomes. The outcome assessors were aware of the intervention received by study participants in three trials. A summary of the Cochrane Risk of Bias assessment for the 24 trials included in the meta-analysis is presented in Table S4 of the supplementary appendix.
Meta-analysis
The key results from the meta-analysis are summarized in Table 4.
Mortality
Pooled Fixed-Dose SABA
Base-case meta-analysis of ten trials that included a fixed-dose SABA arm returned a pooled rate of mortality of 0.22% (95% CI 0.10%, 0.52%) with no heterogeneity identified (Fig. 2). One trial [25] reported a single death; the patient in this trial was randomized to albuterol four times daily and died from acute pancreatitis. This death was judged to be unrelated to the study treatment.

Forest plot showing pooled incidence of base-case mortality for fixed-dose SABA at 12+ weeks. I2 gives the percentage of variation across the studies resulting from heterogeneity rather than chance. Q-statistic p value (QEp) indicates statistical significance of the interstudy variation. CI confidence interval. No studies with as-needed SABA reported mortality
Sensitivity analysis using studies with durations of 12–16 weeks did not change the results for this fixed-dose treatment group. The pooled rate of mortality and heterogeneity in this sensitivity analysis case was 0.2% and 0%, respectively. Two trials were removed because of durations of 24 weeks [27] and 52 weeks [28]. The sensitivity analysis limited to studies enrolling patients with mild-to-moderate asthma did not affect the meta-analysis results compared with the base case. The mortality rate remained at 0.2%. Fitzgerald 1999 [27] was removed from this analysis for enrolling patients with more severe asthma.
ICS or ICS + LABA versus SABA Reliever Monotherapy
Two deaths were reported in a single trial enrolling patients with mild asthma that included three treatment arms: (i) ICS + LABA as needed, (ii) ICS maintenance therapy (+ SABA as needed), and (iii) SABA as needed [26]. No deaths were reported in the SABA as-needed arm. One death was reported in the ICS maintenance (+ SABA as needed) arm (suicide) and one death in the ICS + LABA arm (vehicular accident), neither of which was judged by investigators to be treatment related. No deaths were reported in the other trials included in this analysis, and meta-analysis was not possible.
Discontinuations Due to Adverse Events
Pooled Fixed-Dose SABA
Seven trials reported DAEs for patients with asthma on fixed-dose SABA therapy, six of which were trials of salbutamol/albuterol, and one was of levalbuterol. The incidence of DAEs ranged from 1% to 7% across the trials. Pooled incidence was 3.3% (95% CI 1.8%, 6.0%), with high heterogeneity driven by the Hamilos 2007 [28] trial, which had a 52-week duration (Fig. 3a). Pooled incidence was reduced to 2.7% (95% CI 1.6%, 4.5%) following sensitivity analysis limited to studies of fixed-dose SABA with timepoints of 12–16 weeks. No sensitivity analysis by asthma severity was necessary for the fixed-dose SABA group as all patients had mild-to-moderate asthma. Full results of each sensitivity analysis performed are presented in the supplementary appendix.

Forest plots showing pooled incidence of base-case DAEs for fixed-dose and as-needed SABA and odds ratios for base-case DAEs for ICS versus SABA at 12+ weeks. I2 gives the percentage of variation across the studies resulting from heterogeneity rather than chance. Q-statistic p value (QEp) indicates statistical significance of the interstudy variation. CI confidence interval
Pooled As-Needed SABA
Thirteen trials reported DAEs for patients taking as-needed SABA reliever therapy in a placebo arm. Salbutamol/albuterol was the treatment in all 13 trials. The incidence of DAEs ranged from 0% to 16% across trials with a pooled incidence of 3.9% (95% CI 2.3%, 6.5%). Inclusion of the Meltzer 2009 trial, which considered worsening symptoms to be a DAE, resulted in moderate heterogeneity (Fig. 3b). Sensitivity analysis limiting study duration to 12–16 weeks reduced pooled incidence to DAEs to 3.5% (95% CI 2.0%, 6.1%) with heterogeneity of approximately 74%, similar to the base-case analysis. Sensitivity analysis limited to studies of patients with mild-to-moderate asthma produced results similar to the base-case analysis (3.9%, 95% CI 2.2%, 6.7%).
ICS Maintenance Therapy versus SABA Reliever Monotherapy
DAEs were reported for ten trials in which an ICS maintenance therapy was compared with SABA as reliever therapy in patients with asthma. The incidence of DAEs ranged from 0% to 16%. The proportion of patients with DAEs in the SABA reliever group was the same as or lower than in the ICS group in four trials. For the remaining trials, incidence of DAEs was higher in the SABA reliever groups, which could be attributed to inclusion of worsening asthma symptoms as an AE. SABA reliever monotherapy groups did not receive maintenance therapies.
Odds of DAE for patients in the ICS group were approximately half of those for patients in the SABA monotherapy group [odds ratio (OR) 0.52, 95% CI 0.35, 0.76], with little heterogeneity (Fig. 3c). Sensitivity analyses were almost identical to the base-case analysis when limiting duration to 12–16 weeks (OR 0.51, 95% CI 0.34, 0.78) and limiting asthma severity to mild to moderate (OR 0.50, 95% CI 0.32, 0.76).
Serious Adverse Events
Pooled Fixed-Dose SABA
Four trials reported the incidence of SAEs for patients with asthma on fixed-dose SABA treatment.
SABAs under investigation were salbutamol/albuterol in three trials, and both levalbuterol and racemic albuterol in one trial. The incidence of SAEs ranged from 1% to 5% with a pooled incidence of 1.9% (95% CI 0.9%, 3.8%), and high heterogeneity (75%) (Fig. 4a). Sensitivity analysis limiting study duration (12–16 weeks) showed a slightly reduced pooled incidence of 1.3% (95% CI 0.8%, 2.1%).

Forest plots showing pooled incidence of base-case SAEs for fixed-dose and as-needed SABA and odds ratios for base-case SAEs for ICS versus SABA at 12+ weeks. I2 gives the percentage of variation across the studies resulting from heterogeneity rather than chance. Q-statistic p value (QEp) indicates statistical significance of the interstudy variation. CI confidence interval
Pooled As-Needed SABA
Six trials reported SAEs for patients receiving as-needed SABA therapy, all of which investigated albuterol as the study treatment. The incidence of SAEs ranged from 0% to 5% with a pooled incidence of 1.9% (95% CI 0.9%, 4.1%) and little heterogeneity (44%) (Fig. 4b). Sensitivity analysis limiting study duration (12–16 weeks) resulted in a slight increase in pooled incidence to 2.0% (95% CI 0.5%, 7.5%). However, when limited by asthma severity (mild to moderate), pooled incidence of SAEs was reduced to 1.4% (95% CI 0.6%, 3.1%).
ICS Maintenance Therapy versus SABA Reliever Monotherapy
Four trials in which ICS maintenance therapy was compared with SABA reliever therapy reported SAEs. The incidence of SAEs ranged from 0% to 5% and was similar between the ICS and SABA reliever treatment groups. Meta-analysis results were similar to individual trial results (OR 0.95, 95% CI 0.46, 1.95) with no heterogeneity (Fig. 4c). Sensitivity analysis resulted in a similar OR of 0.92 (95% CI 0.34, 2.44) when limited by study duration (12 weeks), and the OR increased slightly to 1.07 (95% CI 0.41, 2.79) from base case when limited to mild-to-moderate asthma. Exclusion of studies in which exacerbations were defined as an SAE resulted in a reduced OR of 0.84 (95% CI 0.31, 2.31).
Discussion
This SLR and meta-analysis, performed using available SABA safety data from approximately 5000 patients enrolled in RCTs and published over a 25-year period from 1996 to 2021, identified no evidence of treatment-related mortality in any of the included trials. All-cause mortality was rare, with a pooled incidence of 0.22% for patients taking SABA. Only three patients died, from causes considered not related to treatment (suicide, vehicular accident, acute pancreatitis), two of whom were randomized to ICS regimens (with and without LABA). Because only two studies reported deaths in either treatment group, no meta-analysis was possible and no conclusions regarding mortality rates for SABA-treated patients compared with ICS-treated patients could be made.
SAEs were rarely reported by patients administered fixed-dose or as-needed SABA therapy. The reported incidence of SAEs was ≤ 5% in these groups, and in many cases, the incidence was 1% or 2%, despite some studies including asthma exacerbations as SAEs. The risk of SAEs did not differ for patients treated with ICS alone versus those treated with SABA as a reliever, and this observation remained valid in sensitivity analyses that limited the severity of asthma and treatment duration.
Among patients taking SABA as needed, the absence of ICS-based maintenance therapy placed the patients at greater risk of worsening asthma, thereby potentially leading to increased risk of DAEs. This may explain the higher incidence of DAEs (16%) reported in one outlier study [29] which included worsening symptoms as adverse events that lead to discontinuation. However, information on the types of AE that led to discontinuation was not specified in this trial, so the proportion of patients who discontinued because of worsening asthma symptoms is not clear. The risk of treatment discontinuation due to AEs was lower with ICS maintenance therapy than with SABA reliever therapy; however, comparability of the types of AEs that led to discontinuation between the two groups could not be determined.
These observations regarding the relationship between worsening asthma and the absence of an ICS-based maintenance therapy suggest that uncontrolled asthma may be the main reason for mortality and adverse outcomes in patients with asthma. Potentially, the overuse of SABA may be the result of uncontrolled asthma and not the cause of adverse outcomes or serious adverse effects.
Underuse of regular ICS-based maintenance therapy may contribute to overuse or inappropriate dosing of SABA reliever therapy. However, in contrast to reports from the SABINA program suggesting that SABA reliever use is dose-dependently associated with an increased risk of exacerbations [8], the underuse of maintenance therapy may be what leads to increased risk of asthma exacerbations and mortality [7]. As a retrospective database analysis, the SABINA study represents a snapshot of real-world practice. Although the number of patients whose ICS prescriptions had been dispensed more than doubled by the end of the observation period, approximately 85% of patients continued to overuse SABA relievers throughout the period [8], suggesting that inadequate control of asthma led to increased frequency of exacerbations and mortality rather than overuse of SABA as a reliever therapy. As shown in our analysis of SABA safety from RCTs, the appropriate use of SABA prescribed as a reliever for acute symptoms should not lead to undue concerns of increased mortality or SAE risk for adults and adolescents with asthma. This is particularly pertinent for SABA reliever therapies approved for treating patients suffering with an acute exacerbation of asthma [1, 6].
The marked disparity in the definitions of SABA reliever overuse also makes it difficult to determine the contribution of as-needed SABA use to adverse outcomes. GINA defines the overuse of SABA as three canisters or more per year (approximately 1.2 puffs per day) [6], whereas for more than 20 years, clinical trials have defined SABA overuse as administration of more than eight puffs of an SABA inhaler per day.
This meta-analysis showed that in RCTs—which defined SABA overuse at a higher threshold than the GINA definition—deaths were rare and incidence of SAE/DAE was low. The threshold for overuse in the SABINA studies was much lower (collection of more than three canisters in 1 year) [8], so it remains unclear if the increased risk of mortality reported in the SABINA studies represents an overestimation of adverse effects related to overuse of SABA reliever therapies.
This inconsistency in the definition of SABA reliever therapy overuse raises the question of what dosages of SABA have the least risk of mortality and adverse events. In this study, the maximum dosage of SABA reliever therapy prescribed was salbutamol 400 µg four times daily (1600 µg per day). Other dosages of salbutamol (referred to as albuterol in some studies) were 180 µg four times daily (720 µg per day) and 100 µg, 90 µg, and 80 µg as needed. Inclusion of studies using these dosages did not contribute to an increased risk of mortality, SAEs, or DAEs, suggesting that these dosages are within the acceptable range for SABA reliever therapy.
The publication date range chosen for inclusion in the SLR excluded the seminal studies from New Zealand and Canada that showed excess mortality associated with higher doses of fenoterol. However, these older studies reporting the safety of SABA were mostly observational and had multiple factors that confounded the association with mortality [9]. A review by Beasley (1991) [19] concluded that the self-administration of high-dose, nonselective, potent inhaled β-agonists above prescribing limits was associated with an increased risk of mortality [19]. This resulted in regulatory warnings being applied to isoproterenol and fenoterol [19] and led to a reduction in mortality associated with SABA reliever use [10]. Of further note, many patients in these studies did not receive treatment with an ICS-based maintenance therapy [15]. A further review concluded that other SABA molecules (salbutamol and terbutaline) do not have a direct association with an increased risk of mortality for patients with asthma [10].
A newly published double-blind, crossover, single-center, placebo-controlled non-inferiority study[30] compared the bronchodilator response to salbutamol and budesonide/formoterol in adults with stable asthma [30]. This study found no evidence of non-inferiority against a boundary of a forced expiratory volume in 1 s (FEV1) of − 0.06 L for the difference between budesonide/formoterol 200/6 µg compared with salbutamol 200 µg at the timepoint of 2 min [30]. There were 33 adverse events reported among 22 participants [30]. Only one adverse event (headache) was thought to be related to the administration of salbutamol [30]. A potential concern is that patients switching from SABA reliever therapy to budesonide/formoterol monotherapy may fail to achieve similar fast, effective, and safer symptom relief.
Another notable study not included in this meta-analysis owing to the publication date range was Castle (1993) [31], which concluded that treatment with salmeterol or salbutamol was not associated with a mortality rate in excess of that predicted over the period of interest [31], in contrast to the findings of the New Zealand and Canadian studies. This study further proposed that patients with severe/uncontrolled asthma, who have the greatest risk of mortality, should not receive high doses of SABA as their main or only therapy.
Study Limitations
While this study has several strengths such as the rigorous review protocol, independent dual review of the studies, and cross-checking of bibliographies, which ensured complete identification of available evidence, several factors limit interpretation of the data. The main limitation was the publication and reporting bias inherent in all literature reviews. A lack of detail regarding patient characteristics, particularly in older studies, limited the ability to assess comparability of the patients enrolled. However, sensitivity analyses found that asthma severity had no impact on the results of the meta-analysis for the safety outcomes of interest. Whether adverse outcomes associated with SABA use were directly related to treatment or to underlying poor asthma control that resulted in increased SABA use could not be determined.
The study findings are limited to patients who were eligible for enrollment in RCTs and had medical observation over a period of 12–52 weeks. This population likely had less comorbidity than patients in the clinical setting, and treatments were likely to have been administered in a controlled way using appropriate dosages. The effects of long-term (> 52 weeks) SABA reliever use, for example, on exacerbation risk, long-term lung function, or cumulative systemic steroid morbidity, were not investigated and cannot be determined from this analysis. The availability of any longer-term data is limited, in part owing to the relatively short duration of follow-up in any RCT. The absence of observational study data limits extrapolation of the results to patients in the real world who control their asthma with long-term SABA reliever therapy, and may have poor maintenance treatment adherence, SABA reliever overuse, or limited access to healthcare monitoring. Future studies investigating the potential effects of SABA used as a reliever in conjunction with ICS-based maintenance therapy use (exacerbation risk, lung function decline, cumulative systemic steroid use), may also be of value.
The studies selected for inclusion in the meta-analysis reported the most robust data to permit the analysis; however, the meta-analysis was not a complete assessment of the literature. Some publications identified in the initial literature searches evaluated mortality in patients with asthma but were excluded from the SLR and meta-analysis because the data for patients administered SABA reliever monotherapy were not reported separately.
Conclusions
This comprehensive meta-analysis of data available from published clinical trials indicates that treatment with SABA as a reliever therapy does not result in increased mortality or excess SAEs in adult and adolescent patients when used within prescribed limits for symptom relief. The risk of mortality, SAEs, and DAEs did not appear to differ from that of ICS-based maintenance therapies. To supplement the key outcomes of this study, future well-designed studies focusing on this subset of patients with asthma (particularly those who are poorly adherent and unlikely to be well monitored) would be beneficial to determine whether the low rates of mortality, SAEs, and DAEs reported in this study are similarly reflected in a real-world setting.
References
National Heart LaBI. Guidelines for the diagnosis and management of asthma (EPR-3); 2007. https://www.nhlbi.nih.gov/sites/default/files/media/docs/EPR-3_Asthma_Full_Report_2007.pdf. Accessed May 2022.
Crompton G. A brief history of inhaled asthma therapy over the last fifty years. Prim Care Respir J. 2006;15:326–31.
Hills T, Beasley R. The history and future of short-acting β2-agonist therapy in asthma. Respirology. 2020;25:246–8.
Sanders M. Inhalation therapy: an historical review. Prim Care Respir J. 2007;16:71–81.
Global Initiative for Asthma (GINA). Global Strategy for asthma management and prevention; 2018. https://ginasthma.org/wp-content/uploads/2019/01/2018-GINA.pdf. Accessed June 2022.
Global Initiative for Asthma (GINA). Global Strategy for Asthma Management and Prevention; 2022. https://ginasthma.org/wp-content/uploads/2022/05/GINA-Main-Report-2022-FINAL-22-05-03-WMS.pdf. Accessed May 2022.
Gibbons DC, Aggarwal B, Fairburn-Beech J, et al. Treatment patterns among non-active users of maintenance asthma medication in the United Kingdom: a retrospective cohort study in the Clinical Practice Research Datalink. J Asthma. 2021;58:793–804.
Nwaru BI, Ekstrom M, Hasvold P, Wiklund F, Telg G, Janson C. Overuse of short-acting β2-agonists in asthma is associated with increased risk of exacerbation and mortality: a nationwide cohort study of the global SABINA programme. Eur Respir J. 2020. https://doi.org/10.1183/13993003.01872-2019.
Sears MR, Taylor DR. The beta 2-agonist controversy. Observations, explanations and relationship to asthma epidemiology. Drug Saf. 1994;11:259–83.
Beasley R, Pearce N, Crane J, Burgess C. Beta-agonists: what is the evidence that their use increases the risk of asthma morbidity and mortality? J Allergy Clin Immunol. 1999;104:S18-30.
Crane J, Pearce N, Burgess C, Beasley R. Fenoterol and asthma death. N Z Med J. 1989;102:356–7.
Pearce N, Crane J, Burgess C, Grainger J, Beasley R. Fenoterol and asthma mortality in New Zealand. N Z Med J. 1990;103:73–5.
Grainger J, Woodman K, Pearce N, et al. Prescribed fenoterol and death from asthma in New Zealand, 1981–7: a further case–control study. Thorax. 1991;46:105–11.
Spitzer WO, Ernst P, Suissa S, et al. Fenoterol and death from asthma. Med J Aust. 1992;157:567–8.
Suissa S, Ernst P, Boivin JF, et al. A cohort analysis of excess mortality in asthma and the use of inhaled beta-agonists. Am J Respir Crit Care Med. 1994;149:604–10.
Suissa S, Ernst P, Benayoun S, Baltzan M, Cai B. Low-dose inhaled corticosteroids and the prevention of death from asthma. N Engl J Med. 2000;343:332–6.
Busse W, Stempel D, Aggarwal B, et al. Insights from the AUSTRI study on reliever use before and after asthma exacerbations. J Allergy Clin Immunol Pract. 2022;10:1916-182.E2.
Ye Q, He X-O, D’Urzo A. A review on the safety and efficacy of inhaled corticosteroids in the management of asthma. Pulm Ther. 2017;3:1–18.
Beasley R, Pearce N, Crane J, Windom H, Burgess C. Asthma mortality and inhaled beta agonist therapy. Aust N Z J Med. 1991;21:753–63.
National Institute for Health Care Excellence. Guide to the Methods of Technology Appraisal 2013. London: National Institute for Health and Care Excellence (NICE) Copyright © 2013 National Institute for Health and Clinical Excellence, unless otherwise stated. All rights reserved; 2013.
Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327:557–60.
Abramson MJ, Bailey MJ, Couper FJ, et al. Are asthma medications and management related to deaths from asthma? Am J Respir Crit Care Med. 2001;163:12–8.
Nelson HS, Weiss ST, Bleecker ER, Yancey SW, Dorinsky PM, Group SS. The salmeterol multicenter asthma research trial: a comparison of usual pharmacotherapy for asthma or usual pharmacotherapy plus salmeterol. Chest. 2006;129:15–26.
O’Byrne PM, FitzGerald JM, Bateman ED, et al. Inhaled combined budesonide–formoterol as needed in mild asthma. N Engl J Med. 2018;378:1865–76.
Pleskow W, LaForce CF, Yegen U, Matos D, Della CG. Formoterol delivered via the dry powder Aerolizer inhaler versus albuterol MDI and placebo in mild-to-moderate asthma: a randomized, double-blind, double-dummy trial. J Asthma. 2003;40:505–14.
Beasley R, Holliday M, Reddel HK, et al. Controlled trial of budesonide–formoterol as needed for mild asthma. N Engl J Med. 2019;380:2020–30.
FitzGerald JM, Chapman KR, Della Cioppa G, et al. Sustained bronchoprotection, bronchodilatation, and symptom control during regular formoterol use in asthma of moderate or greater severity. The Canadian FO/OD1 Study Group. J Allergy Clin Immunol. 1999;103:427–35.
Hamilos DL, D’Urzo A, Levy RJ, et al. Long-term safety study of levalbuterol administered via metered-dose inhaler in patients with asthma. Ann Allergy Asthma Immunol. 2007;99:540–8.
Meltzer EO, Korenblat PE, Weinstein SF, Noonan M, Karafilidis J. Efficacy and safety evaluation of ciclesonide in mild-to-moderate persistent asthma previously treated with inhaled corticosteroids. Allergy Asthma Proc. 2009;30:293–303.
Kearns N, Williams M, Bruce P, et al. Single dose of budesonide/formoterol turbuhaler compared to salbutamol pMDI for speed of bronchodilator onset in asthma: a randomised cross-over trial. Thorax. 2022. https://doi.org/10.1136/thorax-2022-219052.
Castle W, Fuller R, Hall J, Palmer J. Serevent nationwide surveillance study: comparison of salmeterol with salbutamol in asthmatic patients who require regular bronchodilator treatment. BMJ. 1993;306:1034–7.
Bensch G, Lapidus RJ, Levine BE, et al. A randomized, 12-week, double-blind, placebo-controlled study comparing formoterol dry powder inhaler with albuterol metered-dose inhaler. Ann Allergy Asthma Immunol. 2001;86:19–27.
Berger WE, Ford LB, Mahr T, et al. Efficacy and safety of fluticasone propionate 250 microg administered once daily in patients with persistent asthma treated with or without inhaled corticosteroids. Ann Allergy Asthma Immunol. 2002;89:393–9.
Condemi JJ, Chervinsky P, Goldstein MF, et al. Fluticasone propionate powder administered through Diskhaler versus triamcinolone acetonide aerosol administered through metered-dose inhaler in patients with persistent asthma. J Allergy Clin Immunol. 1997;100:467–74.
Drazen JM, Israel E, Boushey HA, et al. Comparison of regularly scheduled with as-needed use of albuterol in mild asthma. Asthma Clinical Research Network. N Engl J Med. 1996;335:841–7.
Galant SP, Lawrence M, Meltzer EO, Tomasko M, Baker KA, Kellerman DJ. Fluticasone propionate compared with theophylline for mild-to-moderate asthma. Ann Allergy Asthma Immunol. 1996;77:112–8.
Galant SP, van Bavel J, Finn A, et al. Diskus and diskhaler: efficacy and safety of fluticasone propionate via two dry powder inhalers in subjects with mild-to-moderate persistent asthma. Ann Allergy Asthma Immunol. 1999;82:273–80.
Jacobson K, Chervinsky P, Noonan M, Kane RE, Banerji D, Uryniak T. Placebo-controlled, comparative study of the efficacy and safety of triamcinolone acetonide inhalation aerosol with the non-CFC propellant HFA-134a in patients with asthma. Azmacort HFA Clinical Study Group. Ann Allergy Asthma Immunol. 1999;83:327–33.
Kavuru M, Melamed J, Gross G, et al. Salmeterol and fluticasone propionate combined in a new powder inhalation device for the treatment of asthma: a randomized, double-blind, placebo-controlled trial. J Allergy Clin Immunol. 2000;105:1108–16.
Kemp J, Wolfe J, Grady J, et al. Salmeterol powder compared with albuterol aerosol as maintenance therapy for asthma in adolescent and adult patients. Clin Ther. 1998;20:270–82.
Malmstrom K, Rodriguez-Gomez G, Guerra J, et al. Oral montelukast, inhaled beclomethasone, and placebo for chronic asthma. A randomized, controlled trial. Montelukast/beclomethasone study group. Ann Intern Med. 1999;130:487–95.
Nathan RA, Pinnas JL, Schwartz HJ, et al. A six-month, placebo-controlled comparison of the safety and efficacy of salmeterol or beclomethasone for persistent asthma. Ann Allergy Asthma Immunol. 1999;82:521–9.
Nathan RA, Rooklin A, Schoaf L, et al. Efficacy and tolerability of fluticasone propionate/salmeterol administered twice daily via hydrofluoroalkane 134a metered-dose inhaler in adolescent and adult patients with persistent asthma: a randomized, double-blind, placebo-controlled, 12-week study. Clin Ther. 2006;28:73–85.
Nelson H, Kemp JP, Bieler S, Vaughan LM, Hill MR. Comparative efficacy and safety of albuterol sulfate spiros inhaler and albuterol metered-dose inhaler in asthma. Chest. 1999;115:329–35.
Salat D, Popov D, Sykes AP. Equivalence of salbutamol 200 microg four times daily propelled by propellants 11 and 12 or HFA 134a in mild to moderate asthmatics. Eastern European study group. Respir Med. 2000;94 Suppl B:S22-8.
Sheffer AL, LaForce C, Chervinsky P, Pearlman D, Schaberg A. Fluticasone propionate aerosol: efficacy in patients with mild to moderate asthma. Fluticasone Propionate Asthma Study Group. J Fam Pract. 1996;42:369–75.
Tammivaara R, Aalto E, Lehtonen K, et al. Comparison of a novel salbutamol multidose powder inhaler with a salbutamol metered dose inhaler in patients with asthma. CTR. 1997;58:734–44.
Taylor DR, Town GI, Herbison GP, et al. Asthma control during long-term treatment with regular inhaled salbutamol and salmeterol. Thorax. 1998;53:744–52.
Tinkelman DG, Bleecker ER, Ramsdell J, et al. Proventil HFA and ventolin have similar safety profiles during regular use. Chest. 1998;113:290–6.
ZuWallack R, Adelglass J, Clifford DP, et al. Long-term efficacy and safety of fluticasone propionate powder administered once or twice daily via inhaler to patients with moderate asthma. Chest. 2000;118:303–12.
Acknowledgements
Funding
This study (study ID 218222), along with the Rapid Service and Open Access Fees for publication were funded by GSK.
Medical Writing, Editorial, and Other Assistance
Ananth Kashyap (AK), Evidera, acted as the third independent reviewer for the systematic literature review. Analyses were performed by Evidera, funded by GSK. Editorial support (in the form of writing assistance, including preparation of the draft manuscript under the direction and guidance of the authors, incorporating authors’ comments for each draft, assembling tables and figures, grammatical editing, and referencing) was provided by Nichola Nolan, MSc, of Fishawack Indicia Ltd, UK, part of Fishawack Health, and was funded by GSK.
Author Contributions
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Disclosures
TS has received speaker fees from GSK, AstraZeneca, Novartis, Boehringer Ingelheim, and Sanofi. GW has received speaker fees from GSK in the past 5 years; GG has received research grants from Novartis, GSK, Boehringer Ingelheim, AstraZeneca, and Sanofi, and for acting as a consultant/advisor/speaker for GSK, AstraZeneca, Novartis, and Sanofi; MALA has served as a speaker for Novartis and Roussel; AdR has reported receipt of personal fees from Novartis, GSK, Boehringer Ingelheim, AstraZeneca, and Sanofi; AM and LM are employees of Evidera; GL, BA, SF, AgR, and AP are full-time employees of GSK and hold shares in GSK. Systematic literature review and meta-analysis was conducted by Amber Martin (AM) and Lalith Mittal (LM). All authors participated in drafting the manuscript or revising it critically for important intellectual content and gave final approval of the version to be published.
Compliance with Ethics Guidelines
This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Corresponding author
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Sriprasart, T., Waterer, G., Garcia, G. et al. Safety of SABA Monotherapy in Asthma Management: a Systematic Review and Meta-analysis. Adv Ther 40, 133–158 (2023). https://doi.org/10.1007/s12325-022-02356-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12325-022-02356-2