
Abstract
Background
Supported self-management has been recommended by asthma guidelines for three decades; improving current suboptimal implementation will require commitment from professionals, patients and healthcare organisations. The Practical Systematic Review of Self-Management Support (PRISMS) meta-review and Reducing Care Utilisation through Self-management Interventions (RECURSIVE) health economic review were commissioned to provide a systematic overview of supported self-management to inform implementation. We sought to investigate if supported asthma self-management reduces use of healthcare resources and improves asthma control; for which target groups it works; and which components and contextual factors contribute to effectiveness. Finally, we investigated the costs to healthcare services of providing supported self-management.
Methods
We undertook a meta-review (systematic overview) of systematic reviews updated with randomised controlled trials (RCTs) published since the review search dates, and health economic meta-analysis of RCTs. Twelve electronic databases were searched in 2012 (updated in 2015; pre-publication update January 2017) for systematic reviews reporting RCTs (and update RCTs) evaluating supported asthma self-management. We assessed the quality of included studies and undertook a meta-analysis and narrative synthesis.
Results
A total of 27 systematic reviews (n = 244 RCTs) and 13 update RCTs revealed that supported self-management can reduce hospitalisations, accident and emergency attendances and unscheduled consultations, and improve markers of control and quality of life for people with asthma across a range of cultural, demographic and healthcare settings. Core components are patient education, provision of an action plan and regular professional review. Self-management is most effective when delivered in the context of proactive long-term condition management. The total cost (n = 24 RCTs) of providing self-management support is offset by a reduction in hospitalisations and accident and emergency visits (standard mean difference 0.13, 95% confidence interval −0.09 to 0.34).
Conclusions
Evidence from a total of 270 RCTs confirms that supported self-management for asthma can reduce unscheduled care and improve asthma control, can be delivered effectively for diverse demographic and cultural groups, is applicable in a broad range of clinical settings, and does not significantly increase total healthcare costs. Informed by this comprehensive synthesis of the literature, clinicians, patient-interest groups, policy-makers and providers of healthcare services should prioritise provision of supported self-management for people with asthma as a core component of routine care.
Systematic review registration
RECURSIVE: PROSPERO CRD42012002694; PRISMS: PROSPERO does not register meta-reviews
Similar content being viewed by others


Background
Asthma is common, affecting 334 million people worldwide, and is responsible for substantial morbidity and an increasing burden on healthcare services globally [1]. In the UK, there are over 6 million primary care consultations, and 100,000 hospital admissions each year, at an estimated cost of £1 billion per year [2].
For a quarter of a century [3], national and international guidelines have recommended – unequivocally – that people with asthma should be provided with self-management education reinforced by a personalised asthma action plan and supported by regular review [4, 5], though mode of delivery, personnel delivering the support, the targeted group and the intensity of the intervention vary [6]. The 2014 UK National Review of Asthma Deaths provided a stark reminder of the importance of ensuring that people with asthma respond in a timely and appropriate manner to deteriorating symptoms: only 23% had documented evidence of having been provided with self-management education and 45% of people who died had not sought or received medical attention in their final attack [7].
However, despite self-management being highlighted as a core component of all models of care for people with long-term conditions (LTCs) [8–10] and the concept being well established in the context of asthma [4, 5], in practice only a minority of people with asthma have an action plan [11]. Effective implementation requires a whole systems approach, combining active engagement of patients with the training and motivation of professionals embedded within an organisation in which self-management is valued [12]. Patient organisations, healthcare professionals, policy-makers, commissioners and providers of healthcare services thus need an up-to-date systematic overview of the evidence to inform decisions about prioritisation of supported self-management and to underpin implementation strategies within diverse healthcare systems.
The data presented in this paper are derived from two parallel programmes of work on supported self-management in LTCs commissioned by the National Institute of Health Research: Practical Systematic Review of Self-Management Support (PRISMS) [13] and Reducing Care Utilisation through Self-management Interventions (RECURSIVE) [14]. In the context of asthma, we aimed to answer questions of importance to clinicians, patient-interest groups, managers responsible for developing healthcare services and policy-makers: can supported self-management reduce the use of healthcare resources and improve asthma control? More specifically, in which target groups has it been shown to work, which components are important, in what healthcare contexts, and at what cost?
Methods
We used established methodology for undertaking a meta-review of systematic reviews (PRISMS) and a systematic review of randomised controlled trials (RCTs) (RECURSIVE) [15]. The PRISMS and RECURSIVE reviews were undertaken during 2012–2013 with initial searches completed in November 2012 and May 2012, respectively. We updated the PRISMS searches in March 2015 with a pre-publication update in January 2017, and the RECURSIVE searches in September 2015. RECURSIVE is registered on PROSPERO: CRD42012002694. (PRISMS could not be registered because PROSPERO does not register meta-reviews.)
Search strategy
Table 1 summarises the PICOS criteria, search strategies, sources and search dates; further details are in Additional file 1. The PRISMS search strategy involved searching nine electronic databases using the terms: ‘self-management support’ AND ‘asthma’ AND ‘systematic review’. We defined self-management as ‘the tasks that individuals must undertake to live with one or more chronic conditions. These tasks include having the confidence to deal with medical management, role management and emotional management of their conditions’ [16]. For the update, we searched not only for systematic reviews published after our initial search date but also for RCTs published after the search dates used by the included systematic reviews (see Additional file 2 for the details of these dates). Included systematic reviews were grouped according to the populations studied (children, adults or ethnic minority groups) and the search dates of the reviews extracted. Dates for the update RCT search were set from the date of the latest review search within each population group.
The RECURSIVE search strategy in nine databases comprised the terms: ‘self-management support’ AND ‘long-term condition’ AND ‘healthcare use’ AND ‘randomised controlled trial’. (RECURSIVE included asthma and other LTCs in a single search.) We also specifically sought health economic publications linked to included RCTs.
Identification of relevant papers
Table 2 summarises the PRISMS and RECURSIVE processes. Following training (repeated cycles of duplicate screening of 100 titles, team discussion and clarification of exclusion rules), one reviewer (HLP or GP for PRISMS; LD for the update; MP for RECURSIVE) reviewed titles and abstracts and selected possibly relevant studies. A random sample of titles and abstracts (10% in PRISMS; 40% in RECURSIVE) was examined by a second reviewer (HP for PRISMS; PB or NS for RECURSIVE) working independently as a quality check. The agreement was 97% for the initial search and 99% for the update in PRISMS and 87% for the initial search and 88% for the update in RECURSIVE.
After a similar training process, the full texts of all potentially eligible studies were assessed against the eligibility criteria (see Additional file 3) by one reviewer (HLP for PRISMS; LD for update; MP for RECURSIVE). Second reviewers undertook a 10% check for PRISMS (HP) and a 30% check for RECURSIVE (PB or NS), achieving 83% and 85% agreement, respectively. Disagreements were because unclear papers were included by the reviewer pending discussion with a lead investigator. Uncertainties and disagreements were resolved by full team discussion.
Assessment of methodological quality
We used the R-AMSTAR (Revised Assessment of Multiple Systematic Reviews [17]) quality appraisal tool to assess the methodological quality of the systematic reviews included in the PRISMS study. This reflects both the quality of the review process and the rigour with which the review assessed the quality of the studies it included. We used the Cochrane Risk of Bias tool to assess the quality of RCTs included in the updated search [15]. Quality assessment was undertaken by HLP or LD and independently by a second reviewer (HP) with disagreements resolved by discussion within the team (EE, GP, HLP, ST and HP).
To reflect both quality and size of the review, we developed a star weighting system based on (a) the R-AMSTAR score (≥31 was defined as ‘high-quality’) and (b) the number of participants (≥1000 participants was defined as ‘large’):
-
*** Large high-quality review
-
** Either small high-quality review or large low-quality review
-
* Small low-quality review
In the RECURSIVE study, quality assessment of formal economic evaluations was undertaken using the Drummond checklist [18, 19]; RCTs reporting healthcare utilisation were assessed by judging allocation concealment (the quality component most associated with treatment effect [20]) as adequate or inadequate according to the Cochrane Risk of Bias tool [15].
Outcomes
The primary outcome in the PRISMS meta-review was unscheduled use of healthcare resources (specifically unscheduled consultations, accident and emergency (A&E) department attendances and hospital admissions). Other outcomes of interest were asthma control, asthma-related quality of life and process outcomes (specifically, ownership of action plans). Healthcare utilisation rates and costs were the primary focus of the RECURSIVE review, especially major cost drivers (i.e. hospitalisation rates and costs) and comprehensive summaries including multiple sources of cost. The results of formal cost-effectiveness, cost-utility and cost–benefit analyses were also of interest.
Extraction of data
Data for the PRISMS review were extracted by HLP and LD (update) using a piloted data extraction form, and checked independently by HP for integrity and accuracy. Disagreements were resolved by team discussion. We extracted data on review rationale, the self-management intervention under review, review methodology, summary details of included RCTs (participant demographics, comparison groups, settings, service arrangements, components, duration/intensity of the intervention, follow-up arrangements) and the results of meta-analyses and narrative syntheses. We extracted the findings and conclusions as synthesised by the authors of the systematic reviews, specifically avoiding going back to the individual primary studies. The RCTs in the update review were extracted using similar headings.
A piloted data extraction sheet was devised for RECURSIVE that included descriptive data (characteristics of studies, populations and interventions) and quantitative data (for use in meta-analyses). All the descriptive data and approximately 40% of the quantitative data were double-extracted by two members of the research team working independently.
Data analysis
Meta-analysis is inappropriate at the meta-review level owing to the overlap of included RCTs between reviews. However, for the primary outcome, where two or more systematic reviews (including the RECURSIVE meta-analyses) present pooled statistics, we displayed the results graphically by creating ‘meta-Forest plots’. We undertook narrative syntheses to answer our key questions: Does supported self-management reduce use of healthcare resources and improve asthma control? For which target groups does it work? Which components contribute to effectiveness? and In what contexts does supported self-management work? We categorised the reviews and RCTs included in the PRISMS meta-review according to the question(s) that they answered (see Tables 3 and 4: column 3) and synthesised the findings within these categories.
The final question (What is the effect of self-management on healthcare utilisation and costs?) was answered by a meta-analysis of the RECURSIVE RCT data. The primary analysis explored whether self-management support could reduce utilisation without compromising outcomes. Standardised mean differences (SMD) were computed using a random effects model meta-analysis due to anticipated heterogeneity. Four meta-analyses examined the effects of self-management support interventions on hospitalisation rates, A&E attendances, quality of life and total costs, respectively. We then constructed permutation plots of the data from the subset of trials reporting both utilisation (hospitalisation rates, A&E attendances or total costs) and health outcomes (quality of life). Further details about the analytic approach are described in the RECURSIVE report [14]. Forest plots and permutation plots [21] for the subset of studies reporting both health outcomes and utilisation outcomes were constructed in STATA version 14.
Interpretation and end-of-project workshop
The PRISMS and RECURSIVE teams worked independently, but held regular teleconferences to enable synergies between the findings of the parallel reviews to be developed. Frequent meetings of the multidisciplinary teams aided interpretation of the emerging findings. Finally, we held an end-of-project stakeholder conference at which the findings and over-arching conclusions from PRISMS and RECURSIVE were presented to 34 multidisciplinary stakeholders, including people with LTCs, clinicians, commissioners, providers of healthcare services and policy-makers. Small discussion groups discussed and advised on practical implications for commissioning and providing services for people with LTCs.
Lay involvement
The PRISMS project (which reviewed evidence from 14 LTCs) benefited from a lay collaborator who was involved from the inception of the project. She and other lay representatives from a range of LTC interest groups (including Asthma UK) contributed to an initial stakeholder workshop at which the choice of LTCs studied in the project and self-management interventions of interest were discussed. Lay members also participated in the end-of-project workshop (described above), which aided interpretation and guided dissemination. The PRIMER patient and public involvement group at the University of Manchester, UK, collaborated with the RECURSIVE project.
Updating of searches prior to publication
We updated our PRISMS searches in January 2017 by undertaking forward citation of the original included reviews using Web of Science. Forward citation has been shown to be an efficient and effective method of identifying relevant papers in systematic reviews of complex and heterogeneous evidence [22]. We considered it was very unlikely that a subsequent systematic review or RCT would be published without citing at least one of the previously published reviews. One reviewer (HP) undertook focused data extraction of key findings, which were checked by MP. The additional data were added into the syntheses as appropriate. Had we identified studies that substantially changed our conclusions we planned to undertake full duplicate data extraction, quality assessment and revise our synthesis.
Results
Description of the studies in the meta-review
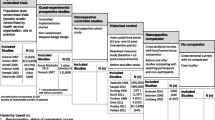
Figure 1 illustrates the PRISMA flow chart for both reviews. After removal of duplicates, 9633 references were identified from the initial PRISMS search and an additional 6321 from the update search. From these, 25 systematic reviews [23–47] were included in the PRISMS meta-review, representing data from 240 unique RCTs. The year of review publication ranged from 1995 to 2013, and included RCTs dated from 1979 to 2013. In addition we included 13 RCTs published since the last search dates of the included reviews (2010 for children, 2012 for adults and 2011 for ethnic groups; see Additional file 2 for details) [48–60]. (For clarity we refer to these as “update RCTs”.) A further two systematic reviews (which included a further four RCTs) [61, 62] and six RCTs [63–68] were added after the pre-publication update. The RECURSIVE study included 24 RCTs with publication dates from 1993 to 2015 [49, 69–91].

PRISMA flowchart. Note: The initial RECURSIVE search included all long-term conditions: papers reporting asthma randomised controlled trials (RCTs) were identified from 184 studies included in the full RECURSIVE report [14]
After excluding overlap, this represents 270 unique trials undertaken in at least 29 high- or middle-income countries: Argentina, Australia, Belgium, Brazil, Canada, Chile, Denmark, Finland, France, Germany, India, Israel, Italy, Jordan, Malaysia, Malta, Netherlands, New Zealand, Norway, Russia, Spain, Sweden, Switzerland, Taiwan, Trinidad, Turkey, UK, USA and Venezuela.
In the 18 systematic reviews that reported the duration of follow-up in their included RCTs [23–25, 27–29, 33, 35, 38–40, 42–47, 61], the modal duration (in 10 of the reviews) was 12 months, with only 3% of reported RCTs falling outside the range of 3–24 months. The update RCTs had a similar profile, with 6 of 13 update RCTs having a duration of 12 months (range 3–30 months).
Study quality and weight of evidence
Taking into consideration both study quality and total population size, 10 PRISMS reviews received an evidence weighting of three stars [27, 31, 32, 36–38, 40, 41, 43, 46], 13 were weighted two star [23–26, 29, 30, 33–35, 39, 42, 44, 45] and two were weighted one star [28, 47]. Of the PRISMS update RCTs, four were judged to be at low risk of bias [50–52, 58], five at high risk of bias [48, 49, 55, 59, 60] and in four the risk of bias was unclear [53, 54, 56, 57]. Allocation concealment was judged as adequate in six of the 24 asthma studies included in the RECURSIVE review [74, 76, 80, 83–85]. Study quality is indicated in the first columns of Tables 3, 4 and 5, with details of the quality assessments in Additional file 4.
Overview of presentation of results
Tables 3, 4, 5 and 6 provide summaries of the studies included in the PRISMS meta-review, update RCTs, the RECURSIVE review and pre-publication update with more detailed tables in Additional file 5.
Can supported self-management reduce the use of healthcare resources and improve asthma control?
Use of healthcare resources
Figure 2 is a meta-Forest plot illustrating the meta-analyses (including three PRISMS 3* reviews and RECURSIVE) that report relative risks of admissions, A&E attendances and/or unscheduled consultations [27, 31, 38]. Treatment event rates from the meta-analyses are in Table 7. These results suggest similar effects in adults [38], children [27] and mixed populations [31].

Meta-Forest plot of healthcare resource use from meta-analyses. This meta-Forest plot displays the summary data from the PRISMS systematic reviews that reported relative risk (RR). Note that meta-analysis is inappropriate at meta-review level owing to the overlap of included randomised controlled trials between reviews
Hospitalisations were reported in 12 reviews [25–29, 31, 35, 38, 40, 41, 44, 46]. Six meta-analyses (four 3*, two 2*) showed that self-management support interventions led to fewer hospital admissions [25–27, 31, 38, 41]. Six narrative reviews of variable quality, reporting heterogeneous interventions, showed inconsistent effects on hospitalisations [28, 29, 35, 40, 44, 46].
Ten reviews reported A&E attendances [25–27, 29, 31, 35, 38, 40, 44, 46]. Four meta-analyses (three 3* [27, 31, 38], one 2* [26]) reported a reduction in A&E attendances in the self-management intervention compared to control groups. Four narrative reviews (one 3* [46], three 2* [25, 35, 44]) showed a reduction in A&E attendances in at least half of their included RCTs; one 3* review showed inconsistent results [40], and one 2* review showed no benefit on A&E attendances [29].
Of the eight reviews that reported unscheduled care [24, 27, 28, 31, 34, 35, 43, 44], three 3* meta-analyses reported fewer unscheduled consultations in participants who received a self-management intervention when compared to control [27, 31, 43]. Furthermore, three 2* narrative reviews reported that self-management reduced unscheduled care in at least half their included trials [34, 35, 44]. The remaining two small or poor quality reviews had inconsistent results [24, 28].
Asthma control
Of the 10 reviews that reported measures of control [24, 28, 30, 31, 34, 35, 38, 41, 44, 46], three meta-analyses (two 3* [31, 41], one 2* [24]) and three narrative reviews [28, 35, 44] reported a reduction in symptoms in participants who received self-management interventions compared to control groups. The other four narrative reviews (two 3* [30, 34], two 2* [38, 46]) had inconsistent results [30, 34, 38] or showed no benefit on symptom control [46]. The broader concept of quality of life was reported as improved in some reviews [25, 30, 34, 46], but not others [27, 29, 40, 44].
Six reviews reported a reduction in days missed from school or work [24, 29–31, 38, 41]. Two 3* meta-analyses [31, 41], two small reviews each with only one RCT [24, 29] and five of the 13 RCTs in a 2* narrative synthesis of school-based interventions [30] concluded that self-management interventions reduced absenteeism. A single RCT reported in a 3* narrative review in adults concluded that asthma education following A&E attendance had no effect on absenteeism [38].
In which target groups has supported self-management been shown to work?
The systematic reviews encompassed a broad range of populations in diverse healthcare and demographic settings with consistently positive findings. For example, the reviews included all ages [28, 31] or only children [24, 26, 27, 29, 30, 35, 40, 41] or adults [34, 38, 43, 46]. Some focused on lower socioeconomic groups [35, 40] or ethnic minority communities [25, 29, 35]. The reviews and RCTs identified in the PRISMS update typically built on this extensive generic evidence base and investigated interventions targeting specific groups such as urban [52, 54], rural [53], deprived communities [46, 52, 54], cultural groups [46, 54, 55, 60], adolescents [48, 54, 56, 57] or older adults [49, 51]. Table 8 summarises the key strategies used in trials to tailor interventions, or their mode of delivery, to different groups.
Cultural groups
Four reviews explored the impact of self-management in cultural groups [25, 29, 35, 46]. A 2* meta-analysis reported that culture-specific programmes reduced hospitalisations in children and improved quality of life in adults compared to generic interventions [25]. A 3* narrative synthesis found only two RCTs testing culturally tailored interventions, one of which improved quality of life [46]. The involvement of community health workers reduced use of healthcare resources in two thirds, and improved symptoms in all seven RCTs included in a 2* narrative review [35]. An inpatient visit from a lay educator to Black or Latino children improved self-efficacy and action plan ownership 1 month post-discharge [66]. In contrast, three generic interventions in US minority populations showed no improvement [46]. Update RCTs, some underpowered, in indigenous populations had inconsistent outcomes [29, 48, 55, 60].
A&E attendees
Two 3* meta-analyses demonstrated reduced use of healthcare resources (admissions, A&E attendances and unscheduled consultations) in adults recruited during A&E attendance (13 RCTs) [38] and in children with a history of A&E attendance in the previous 12 months (38 RCTs) [27]. Neither review found improved markers of asthma control [27, 38], though an update RCT in paediatric A&E attendees (low risk of bias) found that children discharged with an action plan had fewer symptoms at 28 days compared with usual care [50].
Specific age groups
School-based interventions [30], often using information technology-based programmes [30] or delivered by peers [48, 56], improved quality of life and, in some cases, reduced absenteeism [30, 48, 56, 61]. Generic parenting skills initiatives improved self-efficacy in families struggling to manage young children with asthma, with inconsistent effect on asthma outcomes [64, 67].
Two update RCTs reported interventions in older people that improved control and quality of life [49, 51], and one reduced use of unscheduled care [49]. A key feature of both complex interventions was a structured approach to tailoring in order to meet personal goals or address individual problems.
Which components of supported self-management are important?
A 3* meta-analysis (36 RCTs; 6090 participants of all ages recruited from primary and secondary care settings) defined optimal self-management as education including advice on self-monitoring and a written action plan that was supported by regular professional review [31]. There is evidence that reducing the intensity of self-management education or level of clinical review may reduce its effectiveness [36].
Components of an action plan
The components of an action plan were further defined in two 3* and three 2* reviews [23, 24, 32, 36, 39]. In adults, self-monitoring based on peak flow or symptoms is equally effective [32, 36, 39]. In a comparison in children, symptom-based plans were more effective at reducing unscheduled healthcare [23], and equally effective at improving most measures of asthma control; the exception was days with symptoms, which were reduced more by peak-flow-based than symptom-based plans [23]. A 3* review concluded that action plans with between two and four action points, including recommendations on increasing inhaled corticosteroids and initiating oral corticosteroids, were consistently effective in reducing admissions and A&E attendances [32].
Behavioural change techniques
One 3* meta-analysis demonstrated that self-management interventions that incorporated specific behaviour change techniques reduced unscheduled care and improved control [43]. Meta-regression of the data from the 38 RCTs (7883 participants) concluded that active involvement of participants in the intervention was a key factor in reducing unscheduled healthcare [43]. More specifically, identifying individual behavioural traits (e.g. rebelliousness, low perceived emotional support) in adolescents enabled targeted use of behavioural change techniques [54]. A goal-setting approach proved challenging to implement in primary care settings [63].
Technology
Two 1* narrative reviews investigated computer- or internet-based interactive self-management programmes [28, 47]. The effect on healthcare utilisation was inconsistent, confirmed by a recent review identified in the pre-publication update [62], though both showed improvement in symptoms [28] and/or quality of life [28, 47]. Two update RCTs of web-based self-management programmes for adolescents also showed improved asthma control [54, 57], and an extended follow-up of RCT participants concluded that these effects could be sustained 18 months after conclusion of the trial [59]. Several school-based programmes used technology-based interventions to improve control and reduce absenteeism [30]. Supported self-management using mobile phone technology currently has a limited and inconclusive evidence base [42, 45], though a recent RCT in pregnancy demonstrated improved asthma control and quality of life [68].
Which contextual factors influence effectiveness?
Resonating with the concept of ‘optimal’ self-management (education, an action plan and regular review) [31], a 3* meta-analysis identified that omitting regular review (1 RCT) or reducing intensity of education (1 RCT) was associated with a smaller reduction in unscheduled consultations [36]. A 2* meta-analysis analysed the findings of 18 RCTs (3006 participants) according to the components of the Chronic Care Model [92]. Interventions that included all four components had a greater effect on adherence to inhaled corticosteroids compared to trials including self-management unsupported by the organisational components [33].
Organisational role in promoting supported self-management
A 3* narrative review of 14 RCTs (4588 participants) concluded that proactive organisational systems can increase action plan ownership by promoting uptake of asthma reviews and implementing (and monitoring) structured management systems for asthma care [37]. A recent RCT of a structured approach to self-management education in both primary care and specialist units improved asthma control and reduced unscheduled care [65], and a large cluster RCT at low risk of bias showed an increased adherence to guidelines and reduced asthma symptoms by systematically providing individualised prompts to general practitioners and parents of children with asthma [52]. Automatically linking an action plan to prescriptions given to patients being discharged from A&E improved clinician management and patient uptake of steroid courses [50].
What is the effect of supported self-management on healthcare utilisation and costs?
The RECURSIVE meta-analysis confirmed that self-management support interventions for people with asthma are associated with significant improvements in quality-of-life outcomes (SMD 0.26, 95% CI 0.12–0.39), significant small decreases in hospitalisation rates and costs (SMD −0.21, 95% CI −0.40 to −0.01), significant small decreases in A&E visits (SMD −0.25, 95% CI −0.49 to −0.01), and non-significant small increases in total healthcare costs (SMD 0.13, 95% CI −0.09 to 0.34). Figure 3 shows a Forest plot of the total costs.

Meta-analysis of total costs. CI confidence interval, ES effect size
What is the evidence that supported self-management for asthma can reduce costs without compromising outcomes?
Figure 4 shows the overall permutation plot of the studies (n = 21) reporting data on both quality of life and healthcare utilisation. The majority of the studies on quality of life versus costs related to hospitalisations and A&E attendances were in the right-down quadrant, indicating cost-effectiveness (reduced healthcare utilisation and improved quality of life). However, in terms of total costs (n = 7), the picture was mixed with more studies around zero and the right-up quadrant, indicating that similar costs or small cost increases are necessary to achieve better quality of life.

Permutation plot. Quality of life (x-axis), hospitalisations (y-axis blue) and total costs (y-axis red). In this permutation plot, the effects of self-management interventions on outcomes (quality of life) and utilisation (hospitalisations and total costs) can be visualised simultaneously by placing them in quadrants of the cost-effectiveness plane depending on the pattern of outcomes. Such plots identify studies in the appropriate quadrant (i.e. those that reduce costs without compromising outcomes) and those in problematic quadrants (i.e. those that reduce costs but also compromise outcomes, or those that compromise both outcomes and costs).
What is the evidence that supported self-management for asthma is cost-effective?
Four studies applied formal economic analyses; two showed that self-management support interventions were dominant (i.e. significantly better health outcomes with significantly lower costs) [72, 86], and two produced non-significant ratios between costs and benefits at levels likely to appeal to decision-makers (better outcomes with non-significant increases in costs) [75, 89] (see Additional file 5 for more details).
Thus, the benefits derived by supported self-management interventions are associated with reductions in key areas of healthcare utilisation such as hospitalisations and A&E attendances and can be delivered at similar levels of total costs to usual care.
Discussion
Summary of findings
Extensive evidence (n = 270 RCTs) derived from a broad range of demographic and healthcare settings reveals that supported self-management can reduce hospitalisations, A&E attendances and unscheduled consultations, and improve markers of control and quality of life for people with asthma. Core components of effective self-management are education, provision of an action plan and the support of regular professional review. Effectiveness has been demonstrated in diverse cultural, clinical and demographic groups, with evidence that tailored programmes have greater impact than generic interventions. A range of modes of delivery (including telehealthcare) may be employed to suit preferences and context. The cost of providing self-management support is offset by a reduction in hospitalisations and unscheduled healthcare.
Interpretation of findings
The literature on asthma self-management is particularly well developed and may thus be an exemplar for other LTCs [13, 14]. The 16 systematic reviews reporting effectiveness were typically large (five included data from >5000 participants [27, 30, 31, 41, 43]) and had consistently positive results, suggesting a mature evidence base, unlikely to be influenced by further trials. Outcomes in subgroups were more often the subject of the update RCTs as the field moves on from demonstrating overall effectiveness to investigating the impact in specific target groups [48–58, 60, 61, 72], demographic contexts [52–54, 66], or mode of delivery [54, 59, 62, 72].
Self-management support for asthma is a complex intervention and successful interventions were multi-component, including education, trigger avoidance, teaching self-monitoring, optimal treatment strategies, promotion of adherence and behaviour change techniques, many of which are common to self-management in other LTCs [6]. Appropriately in a variable condition [4], the hallmark of asthma self-management is the provision of an action plan with advice on recognising and responding to deterioration in control [4, 32]. People with asthma, however, have broader concerns as they accommodate the condition within their lives and the action plan needs to be embedded in support for ‘living with asthma’ [93].
Individuals with LTCs adjust medical regimes and self-management strategies to fit into their own lives and health beliefs [13]. Meta-reviews, for example in type 2 diabetes [94, 95], hypertension [96] and asthma [25], have emphasised the importance of culturally tailored interventions. Self-management support can be provided by many different professionals, often specialist nurses [38, 63] or LTC educators [25, 27, 95], but in some contexts the key personnel were community health workers [35, 97] or peer counsellors [30, 56, 66]. Traditionally education is delivered face-to-face, but increasingly technology-based interventions are being developed as alternatives [27, 28, 30, 42, 45, 47, 54, 57, 59, 62, 68].
Self-management support interventions are an integral component of high-quality care for people with LTCs [8–10]. Several of the systematic reviews demonstrated the synergy between self-management education and regular clinical review [31, 33, 36], and supported self-management is most effective when delivered within a proactive asthma management programme [33, 37, 65], or integrated within organisational routines [50, 52]. Only a minority of trials had follow-up periods over 12 months, and studies are needed to confirm long-term sustainability. Costs associated with self-management interventions are similar to usual care.
Strengths and limitations
Meta-reviews have some intrinsic strengths and limitations. The methodology enables the efficient review of a large body of evidence and thus provision of a comprehensive overview to inform policy and practice. However, it relies on the quality of the included systematic reviews (e.g. comprehensive search strategies, accurate data extraction and synthesis). We used the validated R-AMSTAR instrument to assess the quality of included systematic reviews [17]. In contrast to GRADE [98] (now recommended by the Cochrane Handbook [15]), R-AMSTAR assesses the overall quality of the review, rather than assessing the quality of evidence individually for each outcome.
Re-synthesising materials that have already been synthesised risks further loss of detail and has the potential for erroneous assumptions, especially if the primary focus of the review did not directly align with the questions of the meta-review. Overlap between the RCTs included in the systematic reviews may result in undue emphasis on commonly cited papers.
Whilst some reviews and update RCTs directly compared interventions with or without specific components [23–25, 32, 36, 39, 43], or a specific mode of delivery [28, 29, 41, 45], often the different interventions were compared to usual care, allowing only indirect comparison [31, 33, 35, 37, 42, 46, 47]. A further limitation is that ‘usual care’ is rarely defined in RCTs [99], and the definition is even more unclear at meta-review level. Typically usual care is enhanced in the context of a trial, reducing the apparent impact of an intervention [100].
Systematic reviews are only as current as their most-recent search, and meta-reviews add an additional time delay. In the PRISMS meta-review we therefore not only updated our search for systematic reviews, but also searched for RCTs published after the date of the last search used by the included systematic reviews. In addition, prior to publication we undertook forward citation on all the included systematic reviews, which identified two recent systematic reviews and six RCTs [61–68]. None of these changed our conclusions, confirming the maturity of the evidence base.
The two reviewers who undertook the screening and data extraction were not working independently; however, both projects ensured all the reviewers were fully trained and instituted random checks at every stage. Restricting inclusion to reviews with extractable RCT data maintained the quality of evidence, but may have resulted in some lower-grade but useful evidence being rejected.
RECURSIVE was not restricted to formal cost-effectiveness studies – it had a broader focus and included studies reporting data on healthcare utilisation only, without a full effectiveness analysis including costs and quality of life. Some of the RCTs in the RECURSIVE meta-analysis used a more comprehensive definition of ‘total costs’ (e.g. based on societal perspective) compared to others; to account for this inconsistency, we also present the results on key sources of costs such as hospitalisation and A&E attendance rates.
The PRISMS and RECURSIVE teams worked independently, but met regularly throughout the studies to optimise synergies. A further strength was the multidisciplinary team, including backgrounds in public health, general practice, epidemiology and health psychology, enabling a balanced interpretation.
Conclusions
Supported self-management for asthma can reduce unscheduled care, improve asthma control and quality of life, and does not lead to significant increases in total healthcare costs. Effective self-management should be tailored to cultural, clinical and demographic characteristics and is most effective when delivered in the context of proactive LTC management. Healthcare organisations should prioritise and promote the provision of supported self-management for people with asthma.
Abbreviations
- A&E:
-
Accident and emergency
- LTC:
-
Long-term condition
- RCTs:
-
Randomised controlled trials
- SMD:
-
Standardised mean difference
References
Global Asthma Network. The global asthma report 2014. Global Asthma Network. 2014. http://www.globalasthmareport.org/resources/Global_Asthma_Report_2014.pdf. Accessed 22 Dec 2016
Mukherjee M, Stoddart A, Gupta RP, Nwaru BI, Farr A, Heaven M, et al. The epidemiology, healthcare and societal burden and costs of asthma in the UK and its member nations: analyses of standalone and linked national databases. BMC Med. 2016;14:113.
British Thoracic Society, Research Unit of the Royal College of Physicians of London, King’s Fund Centre. National Asthma Campaign. Guidelines for management of asthma in adults: I-chronic persistent asthma. BMJ. 1990;301:651–3.
British Thoracic Society/Scottish Intercollegiate Guideline Network. British guideline on the management of asthma. 2016 update. http://sign.ac.uk/guidelines/fulltext/153/index.html. Accessed 22 Dec 2016.
Global Initiative for Asthma. Global strategy for asthma management and prevention 2015 update. http://www.ginasthma.org. Accessed 22 Dec 2016.
Pearce G, Parke H, Pinnock H, et al. The PRISMS taxonomy of self-management support: derivation of a novel taxonomy and initial testing of utility. J Health Serv Res Policy. 2016;21:73–82.
Royal College of Physicians. Why asthma still kills: the National Review of Asthma Deaths (NRAD) Confidential Enquiry report. London: Royal College of Physicians; 2014.
Singh D, Ham C. Improving care for people with long-term conditions: a review of UK and international frameworks. NHS Institute for Innovation and Improvement. Department of Health: Birmingham; 2006.
World Health Organization. Innovative care for chronic conditions. Building blocks for action. Global report. Geneva: WHO; 2002.
Department of Health. The Mandate. A mandate from the Government to the NHS Commissioning Board: April 2013 to March 2015. London: Department of Health; 2012.
Asthma UK. Time to take action on asthma. London: Asthma UK; 2014.
Pinnock H, Epiphaniou E, Pearce G, et al. Implementing supported self-management for asthma: a systematic review of implementation studies. BMC Med. 2015;13:127.
Taylor SJC, Pinnock H, Epiphaniou E, Pearce G, Parke H. A rapid synthesis of the evidence on interventions supporting self-management for people with long-term conditions. (PRISMS Practical Systematic Review of Self-Management Support for long-term conditions). Health Serv Deliv Res. 2014;2:54.
Panagioti M, Richardson G, Murray E, Rogers A, Kennedy A, Newman S, et al. Reducing care utilisation through self-management interventions (RECURSIVE): a systematic review and meta-analysis. Health Serv Deliv Res. 2014;2:54.
Higgins JPT, Green S. Cochrane handbook for systematic reviews of interventions version 5.1.0 http://handbook.cochrane.org. Accessed 22 Dec 2016.
Adams K, Greiner AC, Corrigan JM, editors. The 1st annual crossing the quality chasm summit – a focus on communities. Washington, D.C: The National Academic Press; 2004. p. 57.
Kung J, Chiappelli F, Cajulis OO, Avezova R, Kossan G, Chew L, et al. From systematic reviews to clinical recommendations for evidence-based health care: validation of Revised Assessment of Multiple Systematic Reviews (R-AMSTAR) for grading of clinical relevance. Open Dent J. 2010;4:84–91.
Drummond MF, O’Brien, Stoddart LG, Torrance GW. Methods for the economic evaluation of health care programmes. 2nd ed. Oxford: Oxford University Press; 1997.
Drummond MF, Sculpher MJ, Torrance GW, O’Brien BJ, Stoddart GL. Methods for the economic evaluation of health care programmes. 3rd ed. Oxford: Oxford University Press; 2005.
Pildal J, Hrobjartsson A, Jorgensen KJ, Hilden J, Altman DG, Gotzsche PC. Impact of allocation concealment on conclusions drawn from meta-analyses of randomized trials. Int J Epidemiol. 2007;36:847–57.
Nixon J, Khan K, Kleijnen J. Summarising economic evaluations in systematic reviews: a new approach. BMJ. 2001;322:1596–8.
Greenhalgh T, Peacock R. Effectiveness and efficiency of search methods in systematic reviews of complex evidence: audit of primary sources. BMJ. 2005;331:1064–5.
Bhogal SK, Zemek RL, Ducharme F. Written action plans for asthma in children. Cochrane Database Syst Rev. 2006;3, CD005306. doi:10.1002/14651858.CD005306.pub2.
Zemek RL, Bhogal SK, Ducharme FM. Systematic review of randomized controlled trials examining written action plans in children. What is the plan? Arch Pediatr Adolesc Med. 2008;162:157–63.
Bailey EJ, Cates CJ, Kruske SG, Morris PS, Brown N, Chang AB. Culture-specific programs for children and adults from minority groups who have asthma. Cochrane Database Syst Rev. 2009;2, CD006580. doi:10.1002/14651858.CD006580.pub4.
Bernard-Bonnin AC, Stachenko S, Bonin D, Charette C, Rousseau E. Self-management teaching programs and morbidity of pediatric asthma: a meta-analysis. J Allergy Clin Immunol. 1995;95:34–41.
Boyd M, Lasserson TJ, McKean MC, Gibson PG, Ducharme FM, Haby M. Interventions for educating children who are at risk of asthma-related emergency department attendance. Cochrane Database Syst Rev. 2009;2, CD001290. doi:10.1002/14651858.CD001290.pub2.
Bussey-Smith KL, Rossen RD. A systematic review of randomized control trials evaluating the effectiveness of interactive computerized asthma patient education programs. Ann Allergy Asthma Immunol. 2007;98:507–16.
Chang AB, Taylor B, Masters IB, Laifoo Y, Brown ADH. Indigenous healthcare worker involvement for Indigenous adults and children with asthma. Cochrane Database Syst Rev. 2010;5, CD006344. doi:10.1002/14651858.CD006344.pub3.
Coffman JM, Cabana MD, Yelin EH. Do school-based asthma education programs improve self-management and health outcomes? Pediatrics. 2009;124:729–42.
Gibson PG, Powell H, Wilson A, Abramson MJ, Haywood P, Bauman A, et al. Self management education and regular practitioner review for adults with asthma. Cochrane Database Syst Rev. 2002;3, CD001117. doi:10.1002/14651858.CD001117.
Gibson PG, Powell H. Written action plans for asthma: an evidence-based review of the key components. Thorax. 2004;59:94–9. doi:10.1136/thorax.2003.011858.
Moullec G, Gour-Provencal G, Bacon SL, Campbell TS, Lavoie KL. Efficacy of interventions to improve adherence to inhaled corticosteroids in adult asthmatics: impact of using components of the chronic care model. Respir Med. 2012;106:1211–25.
Newman S, Steed L, Mulligan K. Self-management interventions for chronic illness. Lancet. 2004;364:1523–37.
Postma J, Karr C, Kieckhefer G. Community health workers and environmental interventions for children with asthma: a systematic review. J Asthma. 2009;46:564–76.
Powell H, Gibson PG. Options for self-management education for adults with asthma. Cochrane Database Syst Rev. 2002;3, CD004107. doi:10.1002/14651858.CD004107.
Ring N, Malcolm C, Wyke S, et al. Promoting the use of personal asthma action plans: a systematic review. Prim Care Respir J. 2007;16:271–83.
Tapp S, Lasserson TJ, Rowe BH. Education interventions for adults who attend the emergency room for acute asthma. Cochrane Database Syst Rev. 2007;3:CD003000. doi:10.1002/14651858.CD003000.pub2.
Toelle B, Ram FSF. Written individualised management plans for asthma in children and adults. Cochrane Database Syst Rev. 2004;1, CD002171. doi:10.1002/14651858.CD002171.pub2.
Welsh EJ, Hasan M, Li P. Home-based educational interventions for children with asthma. Cochrane Database Syst Rev. 2011;10, CD008469. doi:10.1002/14651858.CD008469.pub2.
Bravata DM, Gienger AL, Holty JE, Sundaram V, Khazeni N, Wise PH, et al. Quality improvement strategies for children with asthma: a systematic review. Arch Pediatr Adolesc Med. 2009;163:572–81.
de Jongh T, Gurol-Urganci I, Vodopivec-Jamsek V, Car J, Atun R. Mobile phone messaging for facilitating self-management of long-term illnesses. Cochrane Database Syst Rev. 2012;12, CD007459. doi:10.1002/14651858.CD007459.pub2.
Denford S, Taylor RS, Campbell JL, Greaves CJ. Effective behavior change techniques in asthma self-care interventions: systematic review and meta-regression. Health Psychol. 2014;33:577–87.
Kirk S, Beatty S, Callery P, Gellatly J, Milnes L, Pryjmachuk S. The effectiveness of self-care support interventions for children and young people with long-term conditions: a systematic review. Child Care Health Dev. 2012;39:305–24.
Marcano Belisario JS, Huckvale K, Greenfield G, Car J, Gunn LH. Smartphone and tablet self management apps for asthma. Cochrane Database Syst Rev. 2013;11, CD010013. doi:10.1002/14651858.CD010013.pub2.
Press VG, Pappalardo AA, Conwell WD, Pincavage AT, Prochaska MH, Arora VM. Interventions to improve outcomes for minority adults with asthma: a systematic review. J Gen Int Med. 2012;27:1001–15.
Stinson J, Wilson R, Gill N, Yamada J, Holt J. A systematic review of internet-based self-management interventions for youth with health conditions. J Pediatr Psychol. 2009;34:495–510.
Al-sheyab N, Gallagher R, Crisp J, Shah S. Peer-led education for adolescents with asthma in Jordan: a cluster-randomized controlled trial. Pediatrics. 2012;129:e106–12.
Baptist AP, Ross JA, Yang Y, Song PXK, Clark NM. A randomized controlled trial of a self-regulation intervention for older adults with asthma. J Am Geriatrics Soc. 2013;61:747–53.
Ducharme FM, Zemek RL, Chalut D, McGillivray D, Noya FJ, Resendes S, et al. Written action plan in pediatric emergency room improves asthma prescribing, adherence, and control. Am J Respir Crit Care Med. 2011;183:195–203.
Goeman D, Jenkins C, Crane M, Paul E, Douglass J. Educational intervention for older people with asthma: a randomised controlled trial. Pat Ed Counsel. 2013;93:586–95.
Halterman JS, Szilagyi PG, Fisher SG, Fagnano M, Tremblay P, Conn KM, et al. Randomized controlled trial to improve care for urban children with asthma: results of the school-based asthma therapy trial. Arch Pediatric Adolesc Med. 2011;165:262–8.
Horner SD, Brown A. Evaluating the effect of an asthma self-management intervention for rural families. J Asthma. 2013;51:168–77.
Joseph CL, Ownby DR, Havstad SL, Saltzgaber J, Considine S, Johnson D, Research team members. Evaluation of a web-based asthma management intervention program for urban teenagers: reaching the hard to reach. J Adolesc Health. 2013;52:419–26.
Khan R, Maharaj R, Seerattan N, Babwah F. Effectiveness of personalized written asthma action plans in the management of children with partly controlled asthma in Trinidad: a randomized controlled trial. J Trop Pediatr. 2014;60:17–26.
Rhee H, Belyea MJ, Hunt JF, Brasch J. Effects of a peer-led asthma self-management program for adolescents. Arch Pediatr Adolesc Med. 2011;165:513–9.
Rikkers‐Mutsaerts ER, Winters AE, Bakker MJ, van Stel HF, van der Meer V, de Jongste JC, Smashing Study Group. Internet-based self-management compared with usual care in adolescents with asthma: a randomized controlled trial. Pediatr Pulmonol. 2012;47:1170–9.
Shah S, Sawyer SM, Toelle BG, Mellis CM, Peat JK, Lagleva M, et al. Improving paediatric asthma outcomes in primary health care: a randomised controlled trial. Med J Aust. 2011;195:405–9.
Van Gaalen JL, Beerthuizen T, van der Meer V, van Reisen P, Redelijkheid GW, Snoeck-Stroband JB, Smashing Study Group. Long-term outcomes of internet-based self-management support in adults with asthma: randomized controlled trial. J Med Internet Res. 2013;15, e188.
Wong SS, Nathan AM, de Bruyne J, Zaki R, Tahir SZM. Does a written asthma action plan reduce unscheduled doctor visits in children? Indian J Pediatr. 2011;80:590–5.
Coelho AC, Cardoso LS, Machado CS, Machado AS. The impacts of educational asthma interventions in schools: a systematic review of the literature. Can Respir J. 2016;2016:8476206.
McLean G, Murray E, Band R, Moffat KR, Hanlon P, Bruton A, et al. Interactive digital interventions to promote self-management in adults with asthma: systematic review and meta-analysis. BMC Pulm Med. 2016;16:83.
Morawska A, Mitchell AE, Burgess S, Fraser J. Effects of Triple P parenting intervention on child health outcomes for childhood asthma and eczema: randomised controlled trial. Behav Res Ther. 2016;83:35–44.
Yeh HY, Ma WF, Huang JL, Hsueh KC, Chiang LC. Evaluating the effectiveness of a family empowerment program on family function and pulmonary function of children with asthma: a randomized control trial. Int J Nurs Stud. 2016;60:133–44.
Hoskins G, Williams B, Abhyankar P, Donnan P, Duncan E, Pinnock H, et al. Achieving Good Outcomes for Asthma Living (GOAL): mixed methods feasibility and pilot cluster randomised controlled trial of a practical intervention for eliciting, setting and achieving goals for adults with asthma. Trials. 2016;17:584.
Rice JL, Matlack KM, Simmons MD, Steinfeld J, Laws MA, Dovey ME, et al. LEAP: A randomized-controlled trial of a lay-educator inpatient asthma education program. Pat Ed Counsel. 2015;98:1585–91.
Plaza V, Peiró M, Torrejón M, Fletcher M, López-Viña A, Ignacio JM, et al. A repeated short educational intervention improves asthma control and quality of life. Eur Respir J. 2015;46:1298–307.
Zairina E, Abramson MJ, McDonald CF, Li J, Dharmasiri T, Stewart K, et al. Telehealth to improve asthma control in pregnancy: a randomized controlled trial. Respirology. 2016;21:867–74.
Castro M, Zimmermann NA, Crocker S, Bradley J, Leven C, Schechtman KB. Asthma intervention program prevents readmissions in high healthcare users. Am J Respir Crit Care Med. 2003;168:1095–9.
Clark NM, Gong ZM, Wang SJ, Lin X, Bria WF, Johnson TR. A randomized trial of a self-regulation intervention for women with asthma. Chest. 2007;132:88–97.
de Oliveira M, Faresin S, Bruno V, de Bittencourt A, Fernandes A. Evaluation of an educational programme for socially deprived asthma patients. Eur Respir J. 1999;14:908–14.
Gallefoss F, Bakke PS. Cost-effectiveness of self-management in asthmatics: a 1-yr follow-up randomized, controlled trial. Eur Respir J. 2001;17:206–13.
Gruffydd-Jones K, Hollinghurst S, Ward S, Taylor G. Targeted routine asthma care in general practice using telephone triage. Br J Gen Pract. 2005;55:918–23.
Honkoop PJ, Loijmans RJ, Termeer EH, Snoeck-Stroband JB, van den Hout WB, Bakker MJ, et al. Symptom-and fraction of exhaled nitric oxide–driven strategies for asthma control: a cluster-randomized trial in primary care. J Allergy Clin Immunol. 2015;135:682–8.
Kauppinen R, Sintonen H, Tukiainen H. One-year economic evaluation of intensive vs conventional patient education and supervision for self-management of new asthmatic patients. Respir Med. 1998;92:300–7.
Krieger J, Song L, Philby M. Community health worker home visits for adults with uncontrolled asthma: the HomeBASE Trial randomized clinical trial. JAMA Intern Med. 2015;175:109–17.
Lahdensuo A, Haahtela T, Herrala J, Kava T, Kiviranta K, Kuusisto P, et al. Randomised comparison of guided self management and traditional treatment of asthma over one year. BMJ. 1996;312:748–52.
Levy ML, Robb M, Allen J, Doherty C, Bland JM, Winter RJ. A randomized controlled evaluation of specialist nurse education following accident and emergency department attendance for acute asthma. Respir Med. 2000;94:900–8.
Mancuso CA, Peterson MG, Gaeta TJ, Fernández JL, Birkhahn RH, Melniker LA, et al. A randomized controlled trial of self-management education for asthma patients in the emergency department. Ann Emerg Med. 2011;57:603–12.
McLean W, Gillis J, Waller R. The BC Community Pharmacy Asthma Study: a study of clinical, economic and holistic outcomes influenced by an asthma care protocol provided by specially trained community pharmacists in British Columbia. Canadian Respir J. 2003;10:195–202.
Moudgil H, Marshall T, Honeybourne D. Asthma education and quality of life in the community: a randomised controlled study to evaluate the impact on white European and Indian subcontinent ethnic groups from socioeconomically deprived areas in Birmingham. UK Thorax. 2000;55:177–83.
Pilotto LS, Smith BJ, Heard AR, McElroy HJ, Weekley J, Bennett P. Trial of nurse-run asthma clinics based in general practice versus usual medical care. Respirology. 2004;9:356–62.
Pinnock H, Bawden R, Proctor S, Wolfe S, Scullion J, Price D, et al. Accessibility, acceptability and effectiveness of telephone reviews for asthma in primary care: randomised controlled trial. BMJ. 2003;326:477–9.
Price D, Haughney J, Lloyd A, Hutchinson J, Plumb J. An economic evaluation of adjustable and fixed dosing with budesonide/formoterol via a single inhaler in asthma patients: the ASSURE study. Curr Med Res Opin. 2004;20:1671–9.
Ryan D, Price D, Musgrave SD, Malhotra S, Lee AJ, Ayansina D, et al. Clinical and cost effectiveness of mobile phone supported self monitoring of asthma: multicentre randomised controlled trial. BMJ. 2012;344, e1756.
Schermer TR, Thoonen BP, van den Boom G, Akkermans RP, Grol RP, Folgering HT, et al. Randomized controlled economic evaluation of asthma self-management in primary health care. Am J Respir Crit Care Med. 2002;166:1062–72.
Shelledy DC, Legrand TS, Gardner DD, Peters JI. A randomized, controlled study to evaluate the role of an in-home asthma disease management program provided by respiratory therapists in improving outcomes and reducing the cost of care. J Asthma. 2009;46:194–201.
Sundberg R, Tunsater A, Palmqvist M, Ellbjar S, Lowhagen O, Toren K. A randomized controlled study of a computerized limited education program among young adults with asthma. Respir Med. 2005;99:321–8.
van der Meer V, van den Hout WB, Bakker MJ, Rabe KF, Sterk PJ, Assendelft WJ, et al. Cost-effectiveness of Internet-based self-management compared with usual care in asthma. PLoS One. 2011;6, e27108.
Yilmaz A, Akkaya E. Evaluation of long-term efficacy of an asthma education programme in an out-patient clinic. Respir Med. 2002;96:519–24.
Yoon R, McKenzie DK, Bauman A, Miles DA. Controlled trial evaluation of an asthma education programme for adults. Thorax. 1993;48:1110–6.
Bodenheimer T, Wagner E, Grumbach K. Improving primary care for patients with chronic illness: the chronic care model. JAMA. 2002;288:1775–9.
Ring N, Jepson R, Hoskins G, Wilson C, Pinnock H, Sheikh A, et al. Understanding what helps or hinders asthma action plan use: a systematic review and synthesis of the qualitative literature. Pat Ed Counsel. 2011;85:e131–43.
Fleming E, Gillibrand W. An exploration of culture, diabetes, and nursing in the South Asian community: a metasynthesis of qualitative studies. J Transcult Nurs. 2009;20:146.
Nam S, Janson SL, Stotts NA, Chesla C, Kroon L. Effect of culturally tailored diabetes education in ethnic minorities with type 2 diabetes: a meta-analysis. J Cardiovasc Nurs. 2012;27:505–18.
Marshall IJ, Wolfe CDA, McKevitt C. Lay perspectives on hypertension and drug adherence: systematic review of qualitative research. BMJ. 2012;344, e3953.
Pérez-Escamilla R, Hromi-Fiedler A, Vega-López S, Bermúdez-Millán A, Segura-Pérez S. Impact of peer nutrition education on dietary behaviors and health outcomes among Latinos: a systematic literature review. J Nutr Educ Behav. 2008;40:208–26.
GRADE Working Group. Grading quality of evidence and strength of recommendations. BMJ. 2004;328:1490–4.
Ayling K, Brierley S, Johnson B, Heller S, Eiser C. How standard is standard care? Exploring control group outcomes in behaviour change interventions for young people with type 1 diabetes. Psychol Health. 2015;3:85–103.
de Bruin M, Viechtbauer W, Schaalma HP, Kok G, Abraham C, Hospers HJ. Standard care impact on effects of highly active antiretroviral therapy adherence interventions: a meta-analysis of randomized controlled trials. Arch Intern Med. 2010;170:240–50.
Acknowledgements
We thank Ms Christine Hunter, lay collaborator to the PRISMS project; the PRIMER patient and public involvement group at the University of Manchester; representatives from Asthma UK; and other stakeholder groups who contributed to the development of the project and the project workshops.
The following are members of the PRISMS group:
Stephanie JC Taylor, Hilary Pinnock, Chris J Griffiths, Trisha Greenhalgh, Aziz Sheikh, Eleni Epiphaniou, Gemma Pearce, Hannah L Parke, Anna Schwappach, Neetha Purushotham, Sadhana Jacob.
The following are members of the RECURSIVE group:
Peter Bower, Maria Panagioti, Gerry Richardson, Elizabeth Murray, Anne Rogers, Anne Kennedy, Stanton Newman, Nicola Small.
Funding
PRISMS and RECURSIVE were funded by the National Institute for Health Research Health Services and Delivery Research Programme (project numbers 11/1014/04 and 11/1014/06. The funding body had no role in the design of the study, collection, analysis, nor interpretation of data, nor in writing the manuscript. HP was supported by a Primary Care Research Career Award from the Chief Scientist’s Office of the Scottish Government at the time of the study. LD is supported by an Academic Fellowship in General Practice from the Scottish School of Primary Care.
Availability of data and materials
Not applicable: all data used in this meta-review are derived from published studies and thus already available.
Authors’ contributions
ST and HP initiated the idea for the PRISMS study, led the development of the protocol, securing of funding, study administration, data analysis, interpretation of results and writing of the paper. CG and AS were grant holders on the PRISMS review who contributed to the development of the protocol, the securing of funding, the interpretation of results and the writing of the paper. EE, HLP and GP were systematic reviewers who undertook searching, selection of papers and data extraction with ST and HP. LD updated the PRISMS review. PB developed the idea for the RECURISVE study, secured funding and had primary responsibility for the interpretation of the results and writing the paper. MP and PB reviewed articles, extracted the data, undertook the data analysis and wrote the RECURSIVE paper. MP performed the RECURSIVE update for this meta-review. All authors had full access to all the data, and were involved in interpretation of the data. HP wrote the initial draft of the paper with HLP, LD, MP and ST to which all the authors contributed. ST and HP are study guarantors for PRISMS; PB and MP are study guarantors for RECURSIVE. All authors read and approved the final manuscript.
Competing interests
The submitted work was funded by a grant from the National Institute for Health Research Health Services and Delivery Research Programme. None of the authors have financial relationships with any organisations that might have an interest in the submitted work. HP chairs the self-management evidence review group for the British Thoracic Society/Scottish Intercollegiate Guideline Network Asthma guideline; the authors declare that they have no other relationships or activities that could appear to have influenced the submitted work.
Consent for publications
Not applicable: no individual person’s data.
Ethics approval and consent to participate
Not applicable: meta-review of published data.
Department of Health disclaimer
The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the HS&DR programme, NIHR, NHS or the Department of Health.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional files
Additional file 1:
Detailed search terms: PRISMS and RECURSIVE (all databases). (DOCX 88 kb)
Additional file 2:
Dates of initial and update searches. (DOCX 21 kb)
Additional file 3:
Detailed PICOS table and inclusion/exclusion criteria. (DOCX 22 kb)
Additional file 4:
Quality assessment and weighting. (DOCX 43 kb)
Additional file 5:
Characteristics of included studies and key outcomes. (DOCX 169 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Pinnock, H., Parke, H.L., Panagioti, M. et al. Systematic meta-review of supported self-management for asthma: a healthcare perspective. BMC Med 15, 64 (2017). https://doi.org/10.1186/s12916-017-0823-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12916-017-0823-7