
Abstract
Background
Dyscalculia is defined as a specific learning difference or neurodiversity. Despite a move within postgraduate medical education (PGME) towards promoting inclusivity and addressing differential attainment, dyscalculia remains an unexplored area.
Methods
Using an interpretivist, constructivist, qualitative methodology, this scoping study explores PGME educators’ attitudes, understanding and perceived challenges of supporting doctors in training (DiT) with dyscalculia. Through purposive sampling, semi-structured interviews and reflexive thematic analysis, the stories of ten Wales-based PGME educators were explored.
Results
Multiple themes emerged relating to lack of educator knowledge, experience and identification of learners with dyscalculia. Participants’ roles as educators and clinicians were inextricably linked, with PGME seen as deeply embedded in social interactions. Overall, a positive attitude towards doctors with dyscalculia underpinned the strongly DiT-centred approach to supporting learning, tempered by uncertainty over potential patient safety-related risks. Perceiving themselves as learners, educators saw the educator-learner relationship as a major learning route given the lack of dyscalculia training available, with experience leading to confidence.
Conclusions
Overall, educators perceived a need for greater dyscalculia awareness, understanding and knowledge, pre-emptive training and evidence-based, feasible guidance introduction. Although methodological limitations are inherent, this study constructs novel, detailed understanding from educators relating to dyscalculia in PGME, providing a basis for future research.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
Dyscalculia is categorised as a specific learning difference or part of neurodiversity in the UK and a learning disability in North America. Learners with dyscalculia are said to have significant difficulties in numerical processing [1]. It is increasingly acknowledged that these relate to arithmetic, statistics, ordinance, number and code memorisation and recall, with other individual variance [2, 3]. Here, I chose to use “specific learning difference” (SpLD) to acknowledge that some feel SpLDs relate to a difference in learning needs but may not always result in learners identifying as disabled [4, 5]. Most contemporary definitions state that these challenges are out of keeping with learner age, intelligence level and educational background [1], evolve over time but persist during adulthood.
Dyscalculia is a comparatively recently recognised SpLD with a relatively low ‘diagnosed’ population prevalence, with estimates ranging between 3% and 7% [2]. Awareness of dyscalculia is lower than more highly ‘diagnosed’ SpLDs such as dyslexia, dyspraxia and Attention Deficit and Hyperactivity Disorder (ADHD) [3], with a paucity of research-based evidence, especially relating to adult learners [2]. Of the two studies exploring dyscalculia in Higher Education Institutions (HEI), from the perspective of learners, both Drew [3] and Lynn [6, 7] outlined poor understanding within adult learning environments and a lack of recognition of dyscalculia and of HEI learning support provision. Additionally, learner challenges were different to those described in dyslexia and dyspraxia studies, with understanding and perception of time, distance, finances, non-integer numbers, memorisation and recall of numerical codes and values being frequent issues. Potential complexity arose through possible coexistence of dyslexia or mathematical anxiety, varying learner-developed coping strategies effectiveness and learner coping mechanisms becoming ineffective during undergraduate or postgraduate education [3]. Drew’s [3] three healthcare learner participants had also experienced potential fitness to practice concerns either from themselves or educators.
Context for medical education
The number of DiT in postgraduate medical education (PGME) with dyscalculia remains unknown. Similarly, awareness levels of PGME educators, or what their experiences might be, of facilitating the learning of DiT with dyscalculia is unexplored. Indeed, there has been no published research to date relating to dyscalculia in PGME or undergraduate medical education.
This paucity of knowledge is set in the context of a presumed increasing proportion of UK PGME DiT learners with a disability resulting from increasing numbers of medical students in the UK reporting a disability [8, 9] and in other countries such as Australia [10]. Data collection via the statutory education bodies, and the medical regulator, the General Medical Council (GMC), is challenging given the voluntary nature of SpLD declaration and persisting concerns regarding discrimination and stigma [11]. My Freedom of Information request to the GMC in February 2022 revealed that 1.25% of registered doctors have declared a ‘learning disability’ (including SpLDs) such as dyslexia.
The impact of dyscalculia on DiT and their educators is unknown. The GMC defines differential attainment as the gap in assessment outcomes between learners grouped by protected characteristic [12]. It recently commissioned research into recommending education providers create more inclusive learning environments for disabled learners [13]. Other recent research indicates that differential attainment may persist from school-based examinations through to medical school exit ranking scores and onto PGME examinations [14].
Currently, there is no publicly available information addressing the support of PGME DiT with dyscalculia within the UK, and no known prospective screening in place. Support, including reasonable adjustments for PGME DiT with additional learning needs is accessed through, and coordinated by, education bodies’ Professional Support Units (PSU), including Health Educator and Improvement Wales’ (HEIW) PSU in Wales. More widely, HEIW, the education body in Wales, is responsible for delivery and quality management of PGME in accordance with UK-level standards set by the GMC and medical speciality Royal Colleges and Faculties. Reasonable adjustments are changes, additions, or the removal of learning environment elements to provide learners with additional support and remediate disadvantage [15]. They are frequently purported to enable learners with SpLDs to learn and perform to their potential, although evidence for this is variable [16, 17], with a marked lack of research relating to adult learners with dyscalculia.
Despite recent shifts from more teacher-centred to more student-centred learning approaches, with a range of andrological learning theories emphasising the learner being at the centre of learning [18], the educationalist remains a key element of many learning theories and PGME. Many PGME educators are practising doctors and, alongside this, must maintain a contemporaneous understanding of learning theory, training delivery, teaching, supervision and wider educational policies. However, how they approach, or would plan to approach, supporting learning for DiT with dyscalculia is unknown. Therefore, exploring the attitudes and perspectives of PGME DiT or educators regarding dyscalculia, both unresearched previously, through this paradigm could be valuable [19].
Educational challenges, learning needs and local context
For educators, a pivotal part of facilitating learning is understanding the learning needs of learners, felt to be a cornerstone of adult pedagogy [19, 20]. Davis et al. [20] define learning needs as ‘’any gap between what is and what should be”. These can be established subjectively, objectively or a combination approach. However, Grant [19] cautions against conducting limiting, formulaic learning need assessments.
Identifying attitudes and understanding
Furthermore, attitudes are said to frame educator approaches and thus the learning experiences learners will have [21]. Attitudes are defined as “a feeling or opinion about something or someone, or a way of behaving that is caused by this” [22]. Interpretivism offers a route to exploring such attitudes by outlining that there is no one universal truth or fact, but instead many equally valid realities constructed by different individuals, their meaning-making and their experiences.
Again, research is absent within medical education relating to educators’ attitudes and understanding of learners with dyscalculia and how these might influence their approach. Current research indicates attitudes of HEI educators are often formed through their past - or absent past - experiences, lack of legal obligations knowledge and, for healthcare educators, the patient-centred role of clinical learners [23]. These appeared to help form their approach to facilitating teaching [23,24,25,26,27,28,29]. Therefore, understanding PGME educationalist attitudes towards DiT with dyscalculia would be important in helping understand how learning is facilitated.
Thus, there exists a clear lack of published knowledge and understanding regarding dyscalculia set in a context of increasing awareness of the importance of inclusivity and addressing differential attainment within medical education. The importance of educators in facilitating learning of such PGME DiT suggests that exploring their perspectives and understanding could provide valuable insights into this understudied area. Such knowledge could provide benefit to learners and those designing and delivering programmes of learning for DiT and programmes of support for educators. This includes potentially exploring the attitudes and understanding of educators who have no direct experience of dyscalculia, given that this could be the context in which a DiT with dyscalculia finds themselves in a postgraduate learning environment. Assumptions, or perceptions generated without experience or knowledge of dyscalculia, are equally important to understand in a learning context when the awareness level and prevalence of dyscalculia within DiT is unknown. This allows understanding of how learning for DiT with dyscalculia may be facilitated in a knowledge and understanding-poor context, and furthermore, what educator needs exist and what further research is needed.
Consequently, the research question and aims below were constructed.
Research question:
What are the attitudes towards, understanding and perceived challenges of dyscalculia within postgraduate medical training by postgraduate medical educators?
Research aims:
-
To explore the awareness and understanding of dyscalculia that postgraduate medical educators may or may not have.
-
To determine the attitudes that postgraduate educators have towards dyscalculia and DiT with dyscalculia and how these might be formed.
-
To establish the challenges that postgraduate educators perceive they encounter or might encounter when facilitating the learning of a DiT who has dyscalculia.
-
To provide the basis for future research studies exploring how to facilitate the learning of DiT with dyscalculia during postgraduate training.
Methods
This scoping study was designed using an interpretivist, constructivist qualitative methodology to understand the phenomenon, in detail [30] as part of a Masters in Medical Education programme.
A literature review was undertaken to enable research question and aim construction. Firstly, a focused literature search ascertained the level, and lack, of evidence existing for the study phenomenon followed by four, progressively broader, searches to understand the wider context, between October 2021 and May 2022, revealing the lack of, or limited, literature existing.
The literature search was then performed by me using guidance [31, 32] and twenty-seven research search engines. Additionally, a spectrum of journals was searched directly. Literature was also identified through snowballing.
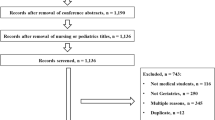
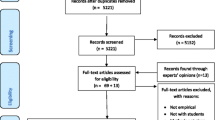
Keyword search terms were developed and refined during the literature search, with limits on further broadening the search based on relevance to the areas of interest: postgraduate learners, educators and SpLDs using different term combinations exploring dyscalculia and postgraduate education, SpLDs and postgraduate healthcare learners, postgraduate educators and attitudes or knowledge or experiences of facilitating learning (appendix 1, supplementary material). Broadening of search terms allowed for exploration of analogous phenomena (other SpLDs), in other postgraduate healthcare and learning contexts, and for further research question development, returning 2,638 items. Papers were initially screened using their titles and the inclusion/exclusion criteria (below) generating 182 articles, papers and theses, with abstracts and reference lists reviewed. 174 papers and eight PhD theses were appraised using guidance [32,33,34].
Inclusion criteria were:
-
Primary research or review.
-
International or UK-based research reported in English.
-
Postgraduate higher education (university-level, post Bachelor or equivalent degree) setting.
-
Relating to postgraduate or higher educationalists’ views from any discipline and knowledge of SpLDs.
Exclusion criteria were:
-
Literature published in non-English languages.
-
Opinion and commentary articles.
-
Undergraduate setting, unless mixed cohort/study with postgraduate learners.
Ultimately, 17 papers and one doctoral thesis were included. Whilst grey literature, this thesis [3] was included due to the dyscalculia-focused insights provided and limited adult-based dyscalculia research elsewhere. After literature appraisal, research aims and a research question were formed.
Semi-structured interviews were chosen to enable data collection and interpretation through a constructivist lens, via open enquiry rather than hypothesis testing [30, 35, 36]. Study participants were PGME educators, actively involved in DiT learning within any PGME programme within Wales whilst holding a Medical Trainer agreement with HEIW. Participants held a range of educationalist roles, from education supervisor to local speciality-specific Royal College tutor (local speciality training lead) to training programme director (responsible for delivery of speciality-specific training across a region).
Interview question and guide design (appendix 2, supplementary material) drew on the six qualitative and six quantitative research-based, validated published tools used to explore similar phenomena, particularly those of O’Hara [37], Ryder [38], L’Ecuyer [23] and Schabmann et al. [39]. Design also drew upon Cohen et al’s [40] recommendations of composing open, neutral questioning.
Interview format was piloted using a PGME educator from England (thus ineligible for study recruitment) with modifications resulting from participant feedback and through adopting reflexivity; as per Cohen et al. [41] and Malmqvist et al. [42]. Participant interviews took place between May and June 2022 and were recorded via the University-hosted Microsoft Teams platform, due to the pandemic-based situation and large geographical area involved, whilst maintaining interviewer-interviewee visibility during the dialogue [35]. Recruitment occurred via purposive sampling, through two HEIW gatekeepers, the national Directors of Postgraduate Secondary (hospital-based) and Primary (General Practice-based) Medical Training in Wales. An email-based invitation with project information was distributed to all postgraduate medical educators with a current HEIW Medical Trainer agreement, regularly engaging in the support of learners within PGME training, in Wales. In this case, the gatekeepers in HEIW were individuals who could grant permission and make contact with all potential eligible participants on behalf of myself, through their email databases, whilst adhering to UK data protection regulations [43, 44].
Ethical considerations
Formal ethics approval was gained from the Cardiff University School of Medicine Research Ethics Committee. Health Research Authority ethics approval was considered but deemed unnecessary. Informed written and verbal participant consent was obtained prior to, and at the point of, interview respectively. Additionally, verbal consent for video recording was sought, offering audio recording or notetaking alternatives; however, participant discomfort was not reported. Mitigation options to avoid selection bias included selecting alternative volunteers if significant relationships between the researcher and participant had existed.
Invitations to participate were circulated to approximately 2,400 to 2,500 postgraduate secondary care trainers and 600 primary care trainers. 18 individuals indicated interest in participating, one cancelled and seven did not respond to follow-up within the two-month timeframe the MSc project schedule allowed for. Subsequent reasons given for two out of seven who subsequently responded out of timeframe included clinical demands and unexpected personal matters. 10 postgraduate educators were interviewed and all allowed video-based interview recording. Interviews lasted between 40 and 60 min. Interviews were transcribed verbatim by me and checked twice for accuracy, with participants assigned pseudonyms. Data analysis was conducted using reflexive thematic analysis (RTA) and undertaken by me, the author, as the single coder and Masters student, with transcripts analysed three times.
RTA followed the six-step approach of Braun et al. [45], Braun and Clarke [46] and Braun and Clarke [47], with a primarily inductive approach [47, 48] through an iterative process. Both latent and semantic coding approaches were used, guided by meaning interpretation [49].
RTA allowed exploration through an interpretivist lens. Discussions persist regarding how RTA sample size sufficiency and ‘data saturation’ are determined, with RTA placing more emphasis on the analyst-based individualism of meaning-making. Therefore, mechanisms for determining thematic saturation are purportedly inconsistent and unreliable [50]. Consequently, sample size was based on the maximum number of participants recruited within the set project time limits.
Reflexivity
I strove to adopt reflexivity throughout, using a research diary and personal reflections, referring to Finlay [51] who stated that such subjectivity can evolve into an opportunity. My interest in the studied phenomenon resulted partially from my experiences as a DiT with SpLDs and from being a DiT representative. Acknowledging this was important given my perspective, as an intrinsic part of this research, could have affected data gathering, interpretation, and, ultimately, study findings through introducing insider status.
Additionally, holding an influential role within the research, with potential for ‘interviewer bias’ [52], I adopted Cohen et al.’s [53] recommendations, committing to conscious neutrality during interviews and use of an interview prompt list, whilst striving to maintain a reflexive approach. Alongside this, the impact on credibility of this study being part of a Masters project, limiting scale and timeframes were considered and mitigated by exploring these within the discussion and referring to this research as a scoping study.
Results
Educators with limited to no direct experience of learners with dyscalculia knew little to nothing about dyscalculia (Fig. 1).

Summary of themes and subthemes generated
Furthermore, of the participants who did, these educators cited close second-hand experiences with family members or past learners with dyscalculia which helped shape their understanding of dyscalculia. Those that had no direct experience drew on empathy and generalisation, extrapolating from the greater knowledge and confidence they had in their understanding regarding dyslexia or other SpLDs or even analysis of the term ‘dyscalculia’ to form definitions and perceptions.
“Absolutely nothing… I saw it, [dyscalculia in the study invitation] didn’t know what it was and Googled it so very, very little really. I suppose in my simplistic surgical sieve head, I would just sort of apply the bits and pieces I know around dyslexia.” P10.
All suggested dyscalculia represented a specific set of challenges and associated learning needs relating to numbers, numeracy or quantity where overall intelligence was preserved. Educators saw each learner as being an individual, therefore felt dyscalculia would present as a spectrum, with varying challenges and needs existing. Dyscalculia was seen as persisting lifelong, with the challenges and needs evolving with age and experiences. Common challenges suggested related to calculations, statistics, critical appraisal, awareness of time, organisation and recall of number-based information (such as job lists, blood results), spatial dimension quantification, prescribing, fast-paced tasks and emergencies, exams and learning-based fatigue or high cognitive load. Wellbeing issues relating to dyscalculia were also frequently perceived, with this potentially negatively affecting self-confidence and anxiety levels. All educators saw a key aspect of their role to be provision of pastoral support, in enabling effective learning.
Past educator experiences of dyscalculia were linked to perceived confidence in ability to support future DiT with dyscalculia. Educators felt their limited knowledge, with the primary source of information regarding dyscalculia being DiT with dyscalculia themselves, to be reflective of low levels of awareness, knowledge and identification within PGME, education systems and wider society. Some felt the proportion of PGME DiT with dyscalculia would be lower than for the general population, following challenging assessments during secondary school and undergraduate studies, but might be changing given widening participation initiatives within medicine. Others saw a potential hidden iceberg of later career stage doctors with unidentified dyscalculia who had completed training when speciality assessments relied less on numeracy.
“[It] was only because of my own experiences and my [relative] that I was able to kind of wheedle around and, you know, make them recognise that there was an issue and that, you know. But I - I think had I not had an awareness of it, I probably wouldn’t have recognised it, I think.” P7.
Educators frequently used empathy when attempting to understand dyscalculia. Educators had mixed feelings about ‘labelling’ DiT as having dyscalculia although all felt identification of additional learning needs was key. Some felt labels were necessary to enable and better support DiT with dyscalculia in the absence of effective, feasible, inclusive education approaches, others noted the potential for stigma or generalisations.
None of the participants had received dyscalculia training. Some felt widespread societal normalisation of mathematics challenges adversely impacted upon if, and at what educational stage, dyscalculia identification occurred and needs were recognised. Many felt assumptions might occur regarding dyscalculia through others making generalisations from better known SpLDs, including dyslexia and dyspraxia, in the absence of other knowledge sources but that these extrapolations could be inaccurate and unhelpful.
“And I think there’s a lot of ‘oh you’re just bad with numbers’ or ‘ohh, you just can’t do, you know people are just, I, I suspect there’s a lot of people who have just been told they’re not very good at maths, aren’t there? And it’s just, you know they can’t, can’t do it, which you know is not really very fair, is it?” P7.
Many felt PGME might represent a critical juncture for DiT with dyscalculia, where effective coping mechanisms developed in the past become ineffective. A variety of such coping mechanisms were suggested or hypothesised, often outlined as depending on the dyscalculia-based experience level of the educator, including checking work with others, calculator use and avoidance of numeracy-dense work or specialities.
Mechanisms were generally viewed positively except where perceived to reduce the likelihood of a DiT recognising dyscalculia themselves and seeking support.
Most felt positively towards learners with dyscalculia and their learning facilitation, especially those with greater experience of dyscalculia. Many balanced this positivity with potential concerns regarding patient safety. Concerns focused especially on heavily numeracy-based tasks, fast-paced situations, or when working independently in surgical or emergency prescription-based situations. Overall, concerns were heightened due to the clinical patient-based context to PGME learning. Two participants felt that not all DiT with dyscalculia should be supported to continue training in particular specialities where numeracy skills were seen as critical, such as ophthalmology.
“I am, and it just seemed really unfair that this one small thing could potentially have such a big impact and could potentially prevent [them] progressing and succeeding in the way that I think you know, [they, they] had the potential to.” P6.
Educators outlined a dependence on the bidirectionality of learner-educator relationships to best facilitate DiT learning per se, and it was felt all DiT had a responsibility to be honest with educators. Some cited potential barriers to this collaboration, including past negative learner experiences, felt stigma, limited educator time and frequent DiT rotations.
“It’s a wonderful opportunity for learning which I really enjoy, because I think that this is a two-way process. You know, I think the DiT gives you things that you reflect on and you should be giving the DiT things that they reflect on” P5.
Most felt they would take a one-to-one learning approach for DiT with dyscalculia. Group-based, fast-paced or numeracy-rich, higher risk clinical activity-based teaching would be more challenging to cater for.
For some, patient safety uncertainties abutted with the duality of being a clinician and educator, with perceived difficulty in quantifying clinical risks associated with learning and educators’ clinical workload demands limiting available time and resources. Thus, many felt that their educator roles always needed to be tempered with their duties as a doctor, prioritising patient safety and quality of care above all else.
“So, it’s not so much the learning, uh, issue that worries me. I think even if someone had dyscalculia the, uh, concepts of medicine could be understood and the basic outline of what we’re doing, but actually you’ve got to be quite precise in the vocational aspect of, of, of the training, and if you get it wrong, it’s a potential major clinical risk and obviously patient safety has to come first in everything that, that we do.” P4.
Educators wished strongly for pre-emptive support in facilitating the learning of DiT with dyscalculia, feeling great responsibility both for DiT learning but also for upholding clinical standards and safety. Many felt they would approach HEIW’s PSU for reactive support, including seeking learner ‘diagnosis’, although some predicted this support, and their knowledge, might be limited. However, two participants outlined positive experiences after seeking PSU support.
Most educator participants supported reasonable adjustment use if patient safety and quality of care remained prioritised and preserved. Other conditions for supporting reasonable adjustments included if they enabled without giving undue advantage and if educator-related workload was not overly burdensome. Those with experience of dyscalculia more confidently volunteered reasonable adjustments suggestions, ranging from calculation-table or App access to additional time for numeracy-rich activities. Some perceived a challenging divide between clinical educators and SpLD education experts who could make potentially unfeasible reasonable adjustment recommendations, with participants suggesting the importance of greater involvement of clinical educators in developing support processes.
“If I’m honest, I don’t think we do it very well…They’re [reasonable adjustments offered] very simplistic, … you know, they’re very much based on a sort of global ability rather than realising that processing and other things might be impacted… We’re, we’re probably behind the curve and not really doing what could be done” P8.
Further example quotes for each theme and subtheme can be found within appendix 3, supplementary material.
Discussion
Experience shapes educator knowledge, understanding and attitudes
This study reveals novel findings regarding dyscalculia in PGME within a vacuum of prior research. Notably, participants’ views towards PGME learners with dyscalculia, including DiT potential to learn, practise and develop effective coping strategies, were substantially more positive and empathetic than in the closest comparable healthcare studies of other SpLDs [23, 24, 27, 29, 54]. Furthermore, the potential impact of societal normalisation of numeracy challenges on awareness of, and attitudes towards, dyscalculia explored by some participants has only previously been noted by Drew [3].
Educators’ expressions of a sense of personal or healthcare-wide lack of awareness and understanding of dyscalculia aligns with the current UK position [2]. But they also built on this, outlining how generalisation from other SpLDs or disabilities was frequently used to bridge the dyscalculia knowledge gap with some not recognising this as potentially problematic. This suggests a need for enhanced awareness and understanding within the healthcare education community of the potential fallibility of using generalisation to support learners with poorly understood additional needs.
Moreover, no other studies have revealed that healthcare educators with personal experience of a learner relative with a SpLD displayed universally positive attitudes towards DiT with the same SpLD. Whilst this could reflect inter-study methodological differences, inter-professional differences or the increasing emphasis on compassionate clinical practice [55], it also suggests influence of educator experience in attitude formation.
In addition to their attitudes, the impact of prior experience of learners with dyscalculia on educators’ knowledge, understanding and confidence was often acknowledged as important by participants. This was seen to an extent in the closest comparable SpLD studies, [24, 54] and further shows the diverse influence of past educationalist experiences, particularly the establishment of deep, longitudinal relative-based relationships, aligning with social constructivism [56].
Unlike HEI lecturers in dyslexia studies [24, 54], who frequently questioned the needs of learners, educators saw DiT with dyscalculia as intelligent and high-functioning, having credible additional learning needs. Needs were seen as variable unlike elsewhere. Additionally, the level of detail constructed regarding educators’ perceptions of the needs, strengths and challenges of each DiT with dyscalculia, evolving over time and experience, is not seen in non-dyscalculia SpLD studies and only alluded to for dyscalculia [3]. These differences, which may be partially explained by varying methodologies or cultural norms regarding how different SpLDs are regarded, are important to better understand.
Furthermore, the preferred educator approach of individualising learning for DiT with dyscalculia is not seen elsewhere in the literature, although this aligns with supporting learning within their zone of proximal development (ZPD). Rather, Ryder and Norwich found HEI educators actually expressed negative attitudes towards individualising learning [24]. Methodological and SpLD-specific factors may contribute to these differences, with this study’s findings aligning more closely with Swanwick’s proposal that PGME often emulates apprenticeship-type learning [57]. It would be valuable to establish the efficacy of individualised PGME-based approaches to facilitating learning with dyscalculia from DiT and educator perspectives.
Greater educator support and training regarding dyscalculia is needed
Educators’ perceived need for wider awareness of dyscalculia, alongside greater pre-emptive training and guidance tailored towards dyscalculia within PGME learning environments has also been described for other SpLDs [23, 58, 59]. Greater research is needed to develop such awareness and evidence-based training, with similar needs identified more widely in HEI for dyscalculia [3] and for other SpLDs [23, 24, 27]. Akin to some participants, Swanwick and Morris [60] discuss the increasing expectations on clinical educationalists to deliver professional-level education and Sandhu [61] explores participants’ expressed need for greater faculty development whilst rectifying the deficit of evidence-base for PGME educators to use.
The crucial importance of the bidirectionality of the educator-learner relationship, with educators perceiving themselves as learners too, is only subtly alluded to elsewhere [3]. Given the bidirectional learning relationship was reportedly undermined by frequent DiT placement rotations, fast-paced clinical environments and shift-based training patterns, further exploration of the appropriateness of current UK PGME training design for DiT with dyscalculia could be important.
Coping strategies are important to better understand
As with this study, Drew’s research suggested coping strategies for learners with dyscalculia to be potentially important, effective and helpful but could have limitations [3]. However, this study provides the first examples of coping strategies, potential or already used, by DiT with dyscalculia. It is crucial that research to develop better understanding of both positive and negative dyscalculia-based coping mechanisms occurs in the future given the broad participant concerns.
Identification is key but not fully enabling
Educators perceived early identification of dyscalculia to be key, showing commonality with dyscalculia, dyslexia and dyspraxia-based studies [3, 25, 28]. That identification was not seen as an absolute solution reinforces the need for further research exploring other disabling factors. However, the witnessed or potential negatives of being ‘labelled’ following dyscalculia ‘diagnosis/identification’, outlined by some participants, have been found only minimally elsewhere within learner-based dyslexia and dyscalculia HEI studies [3, 25, 28]. Negative consequences to labelling included the attitudes learners encountered within the clinical community, suggesting a need to understand cultural norm-related impacts. In contrast, the far greater positives to identification, and the necessity of labelling perceived by educators, were also seen in other SpLD studies [3, 25, 28], enabling self-understanding and access to support. Certainly, the need for improved dyscalculia identification approaches and training is highlighted by the lack of educator confidence in identifying dyscalculia where they had no relative-based experience.
Within the UK, voluntary dyslexia ‘screening’ processes are now offered to some medical students and DiT and similar opportunities could be offered for dyscalculia in the future. Moreover, accumulating evidence indicates an ever-greater importance of establishing equity of learning opportunity and that identification has a positive performance effect for DiT with dyslexia [16, 62, 63].
The PGME clinical context may limit support
Whilst educators clearly adopted a strongly student-centred approach to supporting learning with dyscalculia, addressing the influence of the duality of clinical educator roles on this approach is important. Educator supportive intent was twinned with tension between balancing effective DiT learning with guaranteeing patient safety within diverse, predominantly clinical learning PGME environments, sharing commonalty with L’Ecuyer’s nursing study [23]. Swanwick and Morris [60] note this influence on delivering training, with Sandhu [61] exploring general concerns regarding risk and clinical learning.
Even more pronounced perceived patient safety concerns were expressed in other nursing SpLD studies [23, 29, 54, 64], and further post-qualification independent working concerns emerged [23, 65, 66], which limited educators’ willingness to support learning. Together, these tensions appear to set learning facilitation for those with dyscalculia within healthcare apart from non-healthcare settings. Therefore, healthcare-specific education research and training is needed to address this, especially given thus far, analogous concerns regarding dyslexia and clinical risk remain unproven.
The influence of educator-reported increasing clinical workload and resource limitations on approach towards supporting DiT with dyscalculia was similarly seen within nursing studies [23, 29]. Whilst the impact of clinical demands on UK-based educators are broadly known [67], greater recognition of the potentially disproportionately negative impact on DiT with dyscalculia needs to be made by those overseeing training delivery.
Uncertainty regarding reasonable adjustments need addressing
Additionally, whilst educators were generally supportive of RAs for DiT with dyscalculia, most intending these to be enabling, caveats to RA introduction were substantial for some. Concerns regarding RA implementation for DiT with dyscalculia were similar to nursing and wider HEI SpLD studies [24, 66], but less common or absolute, most relating to feasibility, fairness and adverse impact on educators. These are important to explore if inclusivity in PGME is to be further embraced. Furthermore, and similarly to HEI findings [24], participant concerns about externally-mandated RAs derived from distant SpLD experts suggest that harnessing coproduction, with greater involvement of clinical educators in RA design, could be important for future endorsement. Additionally, whilst the scale of potential RA suggestions for dyscalculia made in this study is novel, it is important that the experiences of DiT with dyscalculia themselves are captured and used to ensure adjustments are truly enabling.
Therefore, whilst this study reveals important and novel discoveries relating to educators, PGME and dyscalculia, establishing DiT experiences of dyscalculia and PGME is the most crucial avenue of future research to next undertake to better understand and enable both DiT and educators to fulfil their roles effectively and inclusively.
Limitations
As a small, qualitative scoping study undertaken in Wales, study findings cannot and should not be generalisable. Seemingly the first study in this area, transferability should also be considered carefully. Due to purposive sampling, those volunteering may have been more interested in this topic; therefore, findings may not reflect the range of knowledge, attitudes, and experiences of all PGME educators.
Furthermore, use of interviews for data collection and the resultant lack of anonymity may have altered participant contributions. Moreover, despite adopting reflexivity, as a relatively inexperienced, sole researcher, I will have engaged in interviews and analysed data with intrinsic unconscious biases, introducing variability and affecting finding credibility. Despite methodological limitations within this small scoping study, my intention was to construct detailed understanding, providing a basis for future research.
Conclusions
This study reveals, seemingly for the first time, the attitudes, understanding and perceptions of PGME educators relating to DiT with dyscalculia. It highlights that lack of awareness and understanding of dyscalculia exists within the PGME educator community, especially in the absence of relatives with dyscalculia, and that widely accessible, evidence-based approaches to identification, support, teaching approaches and RA provisions are needed and wanted by PGME educators.
The rich stories of participants illuminate the emphasis educators place on experiential learning in informing their perceptions and training approaches, especially in the absence of prospective dyscalculia training or evidence base to draw upon. Given this, including the impact of limited or complete lack of dyscalculia experience and the substitution of generalisation to fill knowledge gaps found in this study, there is a real need for greater PGME-focused research to pre-emptively inform and support all educators.
Furthermore, greater acknowledgement and understanding of the seminal influence that clinical context has on educators, their attitudes towards supporting DiT with dyscalculia and the highly prized bidirectional learning relationships, as revealed in this study, are needed. It highlights the need for greater research to better understand the impact that specific nuances of PGME might have on educators’ support of DiT with dyscalculia and further characterise unmet needs. Future research must begin to address educator uncertainties revealed in this study around potential concerns relating to patient safety and care and differential approaches for dyscalculia and unfairness to other learners to move PGME forward in an effective, inclusive and enabling way.
Notable in this study is the lack of the learner voice, and future research needs to begin to better understand the perceptions and experiences of DiT with dyscalculia of PGME across a wide range of aspects. These could involve those suggested by participants, including DiT PGME learning and assessment experiences, coping strategies, reasonable adjustments and cultural norm impact. Furthermore, clarifying the wider awareness and knowledge levels of PGME educators regarding dyscalculia via more quantitative approaches could help build breadth to the understanding of this poorly understood phenomenon alongside the depth provided by this study.
Data availability
No datasets were generated or analysed during the current study.
Abbreviations
- ADHD:
-
Attention Deficit and Hyperactivity Disorder
- DiT:
-
Doctors in Training
- GMC:
-
General Medical Council
- HEI:
-
Higher Education Institution
- HEIW:
-
Health Education and Improvement Wales
- PGME:
-
Postgraduate Medical Education
- PSU:
-
Professional Support Unit
- RA:
-
Reasonable Adjustment
- RTA:
-
Reflexive Thematic Analysis
- SpLD:
-
Specific Learning Difference
- UK:
-
United Kingdom
- ZPD:
-
Zone of Proximal Development
References
Laurillard D, Butterworth B. Review 4: The role of science and technology in improving outcomes for the case of dyscalculia. In: Current Understanding, Support Systems, and Technology-led Interventions for Specific Learning Difficulties: evidence reviews commissioned for work by the Council for Science and Technology. Council for Science and Technology, Government Office for Science; 2020. https://assets.publishing.service.gov.uk/media/5f849afa8fa8f504594d4b84/specific-learning-difficulties-spld-cst-report.pdf. Accessed 24th November 2023.
Parliamentary Office for Science and Technology (POST). Postnote: Dyslexia and dyscalculia. London: Parliamentary Office for Science and Technology. 2014. https://www.parliament.uk/globalassets/documents/post/postpn226.pdf. Accessed 9th October 2023.
Drew S. Dyscalculia in higher education. PhD Thesis, Loughborough University, UK; 2016.
Walker E, Shaw S. Specific learning difficulties in healthcare education: the meaning in the nomenclature. Nurse Educ Pract. 2018;32:97–8.
Shaw S. The impacts of dyslexia and dyspraxia on medical education. PhD Thesis, University of Brighton and the University of Sussex; 2021. p. 16.
Lewis K, Lynn D. Against the odds: insights from a statistician with dyscalculia. Educ Sci. 2017;8:63. https://doi.org/10.3390/educsci8020063.
Lewis K, Lynn D. An insider’s view of a mathematics learning disability: compensating to gain access to fractions. Investig Math Learn. 2018;10(3):159–72. https://doi.org/10.1080/19477503.2018.1444927.
Shrewsbury D. State of play: supporting students with specific learning difficulties. Med Teach. 2011;33(3):254–5.
Murphy M, Dowell J, Smith D. Factors associated with declaration of disability in medical students and junior doctors, and the association of declared disability with academic performance: observational study using data from the UK Medical Education Database, 2002–2018 (UKMED54). BMJ Open. 2022;12:e059179. https://doi.org/10.1136/bmjopen-2021-059179.
Mogensen L, Hu W. ‘A doctor who really knows...’: a survey of community perspectives on medical students and practitioners with disability. BMC Med Educ. 2019;19:288. doi: 10.1186/s12909-019-1715-7
British Medical Association. Disability in the Medical Profession: Survey Findings 2020. 2021. https://www.bma.org.uk/media/2923/bma-disability-in-the-medical-profession.pdf. Accessed 9th October 2023.
General Medical Council. What is differential attainment? 2021. Available from: https://www.gmc-uk.org/education/standards-guidance-and-curricula/projects/differential-attainment/what-is-differential-attainment. Accessed 9th October 2023.
General Medial Council. Welcomed and valued: Supporting disabled learners in medical education and training. 2019. https://www.gmc-uk.org/-/media/documents/welcomed-and-valued-2021-english_pdf-86053468.pdf. Accessed 9th October 2023.
Ellis R, Cleland J, Scrimgeour D, Lee A, Brennan P. The impact of disability on performance in a high-stakes postgraduate surgical examination: a retrospective cohort study. J Royal Soc Med. 2022;115(2):58–68.
Equality Act. 2010. c. 15. [Internet.] 2010. https://www.legislation.gov.uk/ukpga/2010/15. Accessed 9th October 2023.
Asghar Z, et al. Performance of candidates disclosing dyslexia with other candidates in a UK medical licensing examination: cross-sectional study. Postgrad Med J. 2018;94(1110):198–203.
Botan V, Williams N, Law G, Siriwardena A. How is performance at selection to general practice related to performance at the endpoint of GP training? Report to Health Education England. 2022. https://eprints.lincoln.ac.uk/id/eprint/48920/. Accessed 9th October 2023.
Taylor D, Hamdy H. Adult learning theories: implications for learning and teaching in medical education: AMEE Guide 83. Med Teach. 2013. https://doi.org/10.3109/0142159X.2013.828153.
Grant J. Learning needs assessment: assessing the need. BMJ. 2002;324:156–9. https://doi.org/10.1136/bmj.324.7330.156.
Davis N, Davis D, Bloch R. Continuing medical education: AMEE Education Guide 35. Med Teach. 2008;30(7):652–66.
Pit-Ten Cate I, Glock S. Teachers’ implicit attitudes toward students from different Social groups: a Meta-analysis. Front Psychol. 2019. https://doi.org/10.3389/fpsyg.2019.02832.
Cambridge Dictionary. Meaning of attitude in English. [Internet.] 2022. https://dictionary.cambridge.org/dictionary/english/attitude. Accessed 9th October 2023.
L’Ecuyer K. Perceptions of nurse preceptors of students and new graduates with learning difficulties and their willingness to precept them in clinical practice (part 2). Nurse Educ Pract. 2019;34:210–7. https://doi.org/10.1016/j.nepr.2018.12.004.
Ryder D, Norwich B. UK higher education lecturers’ perspectives of dyslexia, dyslexic students and related disability provision. J Res Spec Educ Needs. 2019;19:161–72.
Newlands F, Shrewsbury D, Robson J. Foundation doctors and dyslexia: a qualitative study of their experiences and coping strategies. Postgrad Med J. 2015;91(1073):121–6. https://doi.org/10.1136/postgradmedj-2014-132573.
Shaw S, Anderson J. The experiences of medical students with dyslexia: an interpretive phenomenological study. Dyslexia. 2018;24(3):220–33.
L’Ecuyer K. Clinical education of nursing students with learning difficulties: an integrative review (part 1). Nurse Educ Pract. 2019;234:173–84. https://doi.org/10.1016/j.nepr.2018.11.015.
Walker E, Shaw S, Reed M, Anderson J. The experiences of foundation doctors with dyspraxia: a phenomenological study. Adv Health Sci Educ Theory Pract. 2021;26(3):959–74.
Evans W. If they can’t tell the difference between duphalac and digoxin you’ve got patient safety issues. Nurse lecturers’ constructions of students’ dyslexic identities in nurse education. Nurse Educ Today. 2014;34(6):41–6. https://doi.org/10.1016/j.nedt.2013.11.004.
Illing J, Carter M. Chapter 27: philosophical research perspectives and planning your research. In: Swanwick T, Forrest K, O’Brien B, editors. Understanding medical education: evidence, theory and practice. 3rd ed. Oxford: Wiley; 2019. pp. 393–6.
Atkinson K, Koenka A, Sanchez C, Moshontz H, Cooper H. Reporting standards for literature searches and report inclusion criteria: making research syntheses more transparent and easy to replicate. Res Synth Methods. 2015;6(1):87–95.
Cohen L, Manion L, Morrison K. Research methods in education. 8th ed. London: Routledge; 2017. pp. 171–86.
Critical Skills Appraisal Programme (CASP): Qualitative checklist. In: Critical Appraisal Checklist. Critical appraisal skills programme. [Internet]. 2018. https://casp-uk.net/casp-tools-checklists/. Accessed 9th October 2023.
O’Brien BC, Harris IB, Beckman TJ, Reed DA, Cook DA. Standards for reporting qualitative research: a synthesis of recommendations. Acad Med. 2014;89(9):1245–51.
Cohen L, Manion L, Morrison K. Research methods in education. 8th ed. London: Routledge; 2017. pp. 334–5.
DeJonckheere M, Vaughn L. Semistructured interviewing in primary care research: a balance of relationship and rigour. Fam Med Com Health. 2019. https://doi.org/10.1136/fmch-2018-000057.
O’Hara C. To Teach or Not to Teach? A study of Dyslexia in Teacher Education. Cardiff Metropolitan University, UK;2013 p. 240.
Ryder D. Dyslexia assessment practice within the UK higher education sector: Assessor, lecturer and student perspectives. University of Exeter; 2016.
Schabmann A, Eichert H-C, Schmidt B, Hennes A-K, Ramacher-Faasen N. Knowledge, awareness of problems, and support: university instructors’ perspectives on dyslexia in higher education. Eur J Spec Needs Educ. 2020;35(2):273–82.
Cohen L, Manion L, Morrison K. Research methods in education. 8th ed. London: Routledge; 2017. pp. 507–24.
Cohen L, Manion L, Morrison K. Research methods in education. 8th ed. London: Routledge; 2017. ;523.
Malmqvist J, Hellberg K, Möllås G, Rose R, Shevlin M. Conducting the pilot study: a neglected part of the research process? Methodological findings supporting the importance of piloting in qualitative Research studies. Int J Qual Methods. 2019;18. https://doi.org/10.1177/1609406919878341.
Miller T, Bell L. Consenting to what? Issues of access, gate-keeping and ‘informed’ consent. In: Mauthner M, Birch M, Jessop J, Miller T, editors. Ethics in qualitative research. London: Sage; 2002. pp. 53–5.
Cohen L, Manion L, Morrison K. Research methods in education. 8th ed. London: Routledge. 2017.;523.
Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101.
Braun V, Clarke V. Can I use TA? Should I use TA? Should I not use TA? Comparing reflexive thematic analysis and other pattern-based qualitative analytic approaches. Couns Psychother Res. 2020;21(2):37–47.
Braun V, Clarke V. Thematic analysis. In: Cooper H, Camic P, Long D, Panter A, Rindskopf D, Sher K, editors. APA handbook of research methods in psychology, vol. 2: Research designs: quantitative, qualitative, neuropsychological, and biological. Washington, DC: American Psychological Association; 2012. pp. 57–71.
Braun V, Clarke V. Reflecting on reflexive thematic analysis. Qual Res Sport Exerc Health. 2019;11(4):589–97.
Byrne DA. Worked example of Braun and Clarke’s approach to reflexive thematic analysis. Qual Quant. 2021;56:1391–412.
Braun V, Clarke V. One size fits all? What counts as quality practice in (reflexive) thematic analysis? Qual. Res Psychol. 2021;18(3):328–52.
Finlay L. Outing the researcher: the provenance, process, and practice of reflexivity. Qual Health Res. 2002;12(4):531–45. https://doi.org/10.1177/104973202129120052.
Beer O. There’s a certain slant of light’: the experience of discovery in qualitative interviewing. OTJR. 1997;17(2):127.
Cohen L, Manion L, Morrison K. Research methods in education. 8th ed. London: Routledge; 2017. ;112.
Cameron H, Nunkoosing K. Lecturer perspectives on dyslexia and dyslexic students within one faculty at one university in England. Teach High Educ. 2012;17(3):341–52.
West M, Coia D. Caring for doctors, caring for patients. London:General Medical Council. 2019. https://www.gmc-uk.org/-/media/documents/caring-for-doctors-caring-for-patients_pdf-80706341.pdf. Accessed 8th October 2023.
Kaufman DM. Teaching and learning in Medical Education: how theory can inform practice. In: Swanwick T, Forrest K, O’Brien BC, editors. Understanding Medical Education evidence theory and practice. New Jersey: Wiley Blackwell; 2019. pp. 58–9.
Swanwick T. Postgraduate medical education: the same, but different. Postgrad Med J. 2015;91:179–81.
Farmer M, Riddick B, Sterling C. Dyslexia and inclusion: assessment and support in higher education. London: Whurr; 2002. pp. 175–81.
Mortimore T. Dyslexia in higher education: creating a fully inclusive institution. J Res Spec Educ Needs. 2013;13:38–47. https://doi.org/10.1111/j.1471-3802.2012.01231.x.
Morris C. Chapter 12: Work-based learning. In: Swanwick T, Forrest K, O’Brien B, editors. Understanding medical education: Evidence, theory and practice. 3rd ed. Oxford: Wiley; 2019. p.168.
Sandhu D. Postgraduate medical education – challenges and innovative solutions. Med Teach. 2018;40(6):607–9.
Ricketts C, Brice J, Coombes L. Are multiple choice tests fair to medical students with specific learning disabilities? Adv Health Sci Educ Theory Pract. 2010;15:265–75. https://doi.org/10.1007/s10459-009-9197-8.
Asghar Z, Williams N, Denney M, Siriwardena A. Performance in candidates declaring versus those not declaring dyslexia in a licensing clinical examination. Med Educ. 2019;53(12):1243–52.
Riddell S, Weedon E. What counts as a reasonable adjustment? Dyslexic students and the concept of fair assessment. Int Stud Sociol Educ. 2006;16(1):57–73. https://doi.org/10.1080/19620210600804301.
Riddick R, English E. Meeting the standards? Dyslexic students and the selection process for initial teacher training. Eur J Teach Educ. 2006;29(2):203–22. https://doi.org/10.1080/02619760600617383.
Morris D, Turnbull P. Clinical experiences of students with dyslexia. J Adv Nurs. 2006;54(2):238–47. https://doi.org/10.1111/j.1365-2648.2006.03806.x.
General Medical Council. National Training Survey 2024 results. [Internet]. 2024 p. 4–5, 24–25, 28–32. https://www.gmc-uk.org/-/media/documents/national-training-survey-summary-report-2024_pdf-107834344.pdf. Accessed 26/7/2024.
Acknowledgements
LJC would like to thank her academic supervisor Ms Helen Pugsley, Centre for Medical Education at Cardiff University, for her guidance and encouragement during LJC’s Masters project. LJC would also like to thank all the interview participants who took an active part in shaping this project. LJC is extremely grateful for their time, honesty and for providing such vivid and illuminating windows into their roles as educators. LJC would also like to thank Dr Colette McNulty, Dr Helen Baker and wider staff members at HEIW for their support in circulating her study invitation to trainers across Wales.
Funding
LJC did not receive any funding for, or as part of, the research project described in this paper.
Author information
Authors and Affiliations
Contributions
LJC designed and undertook the entirety of the research project described in this paper. She also wrote this paper in entirety.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study received ethical approval from Cardiff University’s Medical Ethics Committee. After discussions, it was felt that NHS Research Ethics Committee approval was not needed. Written and verbally informed consent to participate was obtained, with prospective participants being provided with information regarding the study and their rights at least three weeks before interviews took place.
Consent for publication
Research participants gave written and verbal consent for the contents of their interviews to be analysed and reported as part of this study.
Competing interests
The authors declare no competing interests.
Author’s information
LJC is currently a final year GP registrar working in Wales with keen interests in differential attainment, inclusivity within education and civil learning environments. This paper is borne from a project she designed and undertook as part of her Masters in Medical Education at Cardiff University.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Cheetham, L.J. “Because people don’t know what it is, they don’t really know it exists”: a qualitative study of postgraduate medical educators’ perceptions of dyscalculia. BMC Med Educ 24, 896 (2024). https://doi.org/10.1186/s12909-024-05912-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12909-024-05912-2