
Abstract
Background
Vaccination of healthcare workers (HCWs) is pivotal in decreasing the incidence of contagious infections in hospital settings. In this study, we assessed the knowledge, attitude, and practice regarding HCWs’ recommended vaccines among medical students and interns in Egypt.
Methods
A multicenter, cross-sectional study was conducted using a structured, pilot-tested, and self-administered questionnaire among Egyptian medical students and interns. We invited 1332 participants to our survey using a systematic random sampling that included participants across nine medical schools in Egypt during the 2021–2022 academic year.
Results
Out of 1332 participants, 1141 completed our questionnaire with a response rate of 85.7%. Overall, 43% of the participants had intermediate knowledge (knew 2–3 HCWs’ recommended vaccines). Furthermore, 36.7% had received a booster dose of at least one of the HCWs’ recommended vaccines over the last 10 years, with only 6.1% having received all recommended vaccines. Hepatitis B vaccine was the most widely known (71%) and received (66.7%). Interns were more likely to know, receive, and recommend HCWs’ recommended vaccines. The majority (> 90%) agreed that vaccination is beneficial and safe, with a median score of eight (interquartile range [IQR: Q25-Q75]: 7–9) out of ten for vaccine efficacy and eight (IQR: 7–8) for safety. However, the median score for hesitancy was five (IQR: 2–7). The most common influential and limiting factors for vaccination were scientific facts (60.1%) and fear of vaccine side effects (44.9%).
Conclusion
Although medical students in Egypt have good knowledge of and attitudes towards vaccination, there is a gap in their practices. Interventions are needed to improve vaccination uptake among medical students in Egypt.
Similar content being viewed by others


Introduction
Vaccination plays a crucial role in preventing infections in communities and healthcare settings, particularly among high-risk individuals. World Health Organization (WHO) and Center for Disease Control (CDC) prioritize vaccination coverage for children and high-risk groups including healthcare workers (HCWs) [1]. The CDC strongly recommends that HCWs receive vaccines such as Hepatitis B, MMR (Measles, Mumps, Rubella), Varicella (Chickenpox), Influenza, and DTaP (Diphtheria, Tetanus, Pertussis) [1, 2]. Moreover, it recommends that microbiologists and HCWs who come into contact with Neisseria meningitidis-infected individuals should receive meningococcal vaccine [1]. Additionally, due to the gap between childhood vaccinations and working as an HCW, booster doses or revaccination may be necessary to maintain high levels of immunity.
Ensuring high vaccination rates among HCWs is critical to prevent the transmission of infections to patients and maintain the integrity of the healthcare system. This is particularly relevant in the context of the COVID-19 pandemic, which highlights the importance of vaccination in preventing the spread of COVID-19 [3, 4]. However, there is an increasing rate of vaccine hesitancy, not only in general population but also among HCWs which has impacted vaccine-related behavior and uptake [5,6,7]. This is concerning as HCWs are considered to be the most influential for patients regarding vaccinations [8]. Patient decision about vaccination is usually associated with their trust in their HCWs [9].
Medical students are the future of the healthcare system and their attitude and practice towards vaccines will shape the future of vaccine uptake among HCWs and patients. Internationally, multiple studies have evaluated the knowledge and attitude of medical students towards vaccines. However, most of these studies included only one or a limited number of vaccines, such as influenza, HBV, and COVID-19 [10,11,12]. Generally, medical students are aware of the importance of vaccination, however there is a gap between knowledge and practice. Rostkwoska et al. reported that 99.2% of European medical students were aware of booster vaccinations; however, only 68% had taken any [13], which could be attributed to vaccine hesitancy.
In low- and middle-income countries, it is estimated that vaccination coverage for HCWs is lower than high-income countries. For example, WHO has estimated that only 18–39% of HCWs in low- and middle-income countries have HBV vaccination coverage compared to 67–79% in high-income countries [14]. In Egypt, most of the available studies have evaluated the attitudes of medical students towards only COVID-19 vaccination. Saied et al. explored the beliefs and barriers of medical students towards COVID-19 vaccines and found that 46% of Egyptian medical students were hesitant to receive COVID-19 vaccines [15]. Another study evaluated vaccination rates and found that 83.2% of Egyptian medical students were vaccinated [16]. However, to our knowledge, there is no or limited data regarding the other HCWs’ recommended vaccines.
This study is underpinned by the Health Belief Model (HBM) and the Theory of Planned Behavior (TPB), which provide a theoretical basis for understanding health behaviors, including vaccination uptake [17]. The HBM posits that individuals are more likely to engage in health-promoting behaviors if they perceive a higher susceptibility to a health issue, believe the health issue has serious consequences, think taking a specific action would reduce their susceptibility or severity, and perceive fewer barriers to taking that action [18]. The TPB, on the other hand, suggests that an individual’s behavior is influenced by their intentions, which are shaped by their attitudes towards the behavior, subjective norms, and perceived behavioral control [19]. Understanding the current knowledge and attitude of medical students and interns towards HCWs’ recommended vaccines will help to develop strategies to improve vaccination rates and protect the health of both HCWs and the population.
This study aims to assess the prevalence, knowledge, and attitudes towards HCWs’ recommended vaccinations among medical students and interns in Egypt. Furthermore, being shortly after the pandemic, it has special focus on COVID-19 and flu vaccines as they were highly recommended. Additionally, it examines the factors influencing the use of booster doses.
The specific research questions are:
-
1.
What is the prevalence of uptake of HCWs’ recommended vaccinations among medical students and interns in Egypt?
-
2.
What is the level of knowledge and what are the attitudes of medical students and interns towards these vaccinations?
-
3.
What factors influence the uptake of booster doses among medical students and interns?
Materials and methods
We conducted a multicenter, cross-sectional study using a structured, pilot-tested, and self-administered questionnaire to evaluate the knowledge, attitude, and practice of medical students regarding HCWs’ recommended vaccines. This study was approved by the institutional review board of Benha University.
Study population and sample size
Our population included undergraduate medical students and interns from Egyptian universities during the 2021–2022 academic year, regardless of nationality. Universities that recently opened without students in all study years were excluded. Of the 26 eligible Egyptian universities in the seven regions, 10 were randomly selected using stratified random sampling based on the number of eligible universities in each region. The selected universities were Cairo University, Benha University, Helwan University (Cairo region), Alexandria University (Alexandria region), Menoufia University, Damietta Branch of Al-Azhar University (Delta region), Zagazig University (Canal region), South Valley University (South Upper Egypt region), Assiut Branch of Al-Azhar University (Middle-Upper Egypt region), and Fayoum University, which were later excluded due to communication difficulties.
Using Raosoft online calculator (https://www.raosoft.com/samplesize.html), we calculated the sample size to achieve a 99% confidence interval, a 4% margin of error, and a 50% response rate to increase the power and accuracy to capture the diversity across medical universities throughout Egypt. This yielded a sample size of 1024. To account for a 30% non-response rate, the total required sample was 1332 which was divided proportionately among universities based on the overall number of students. Within each university, we used a simple random sampling technique, and the sample was divided equally between academic, clinical, and internship years. The first three years were considered academic, the next three years were clinical, and the last year was the internship year. We randomly selected participants from the students’ lists for each class using random.org.
Data collection
University teams were formed with local coordinators, who obtained student lists from official sources. Invitations to participate were sent to the selected individuals between September and November 2022 via email and social media platforms, with a unique code provided to each participant. A voluntary consent form was required for participation.
Questionnaire development
The questionnaire was developed by the principal investigators through a literature review and reviewed by two experts for clarity and relevance. A pilot study was conducted among seven universities to gather feedback on the questionnaire’s format, clarity, and completion time. Changes were made based on this feedback to improve question clarity. Pilot study responses were not included in the final analysis. The questionnaire, consisting of 29 questions divided into four sections, was administered in English using Google Forms. It included a cover letter, sociodemographic questions, practice and knowledge questions, attitudes towards vaccination questions, and attitudes towards specific vaccines (COVID-19 and flu). The questionnaire can be found in the supplementary files.
Statistical analysis
Descriptive statistics are presented as numbers and percentages for qualitative data and median and interquartile range (IQR) [Q25-Q75] for quantitative data. We used the chi-square test to assess the associations between categorical variables. Wilcoxon rank sum test (Mann Whitney) and Kruskal Wallis test were used to assess the association between gender, educational level, and attitudes regarding efficacy, safety, and hesitancy. Knowledge about recommended vaccines was divided into three categories: low knowledge (0–1 vaccines), intermediate knowledge (2–3 vaccines), and high knowledge (4–6 vaccines). A p-value of 0.05 was used as the limit for statistical significance. Statistical analyses were performed using the SAS statistical software (version 9.4; SAS Institute Inc., Cary, NC, USA).
Results
We collected data from nine of the ten selected universities. A total of 1,321 individuals were randomly selected from nine universities located across six regions of Egypt. Of these, 1,141 students completed the survey, resulting in a response rate of 86.4%. The demographic characteristics of the participants are summarized in Table 1. Most of the respondents were Egyptian (89.4%), male (51.9%), first-generation medical students (65.6%), and living in urban areas (63.6%). Furthermore, 95% of the participants had received vaccinations as part of a national campaign during infancy, and 78% reported having access to a vaccination center at their institution or governorate.
Knowledge of booster vaccinations
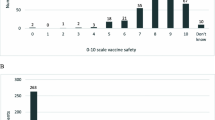
Approximately 85% of participants reported knowing at least one HCW-recommended vaccine, while only 3.8% were knowledgeable about all six recommended vaccines. Moreover, 43% and 25% of the participants had intermediate and high knowledge, respectively (Table 2). The most commonly recognized vaccine was HBV vaccine (Fig. 1A). Interns and clinical-year students were more likely to have intermediate knowledge than academic-year students (49.7% and 49.1% vs. 32.4%, P < 0.001). Moreover, males were more likely to have higher knowledge than females (27.7% vs. 22.6%, P = 0.003) and were more likely to have intermediate knowledge (Table 2). Additionally, Egyptian nationality (44.6% vs. 33.1% for non-Egyptians, P = 0.0457) and geographical region (P = 0.0329) significantly influenced intermediate knowledge. Other sociodemographic factors, including type of residence and generation, were not significantly associated with knowledge (P > 0.05).

Knowledge (A) and prevalence (B) of different HCWs’ recommended vaccines
Booster vaccination practice
About 36.7% of the participants reported receiving booster doses of at least one HCW-recommended over the past ten years. However, a small proportion (6.1%) reported receiving all recommended vaccine boosters, whereas 8.1% reported receiving 2–3 vaccine boosters. The most commonly reported vaccines among those who received booster doses were HBV (66.7%) and influenza (42.1%) (Fig. 1B). Educational grade (interns: 56.1% vs. academic: 30% vs. clinical: 26.3%; P < 0.0001), and geographical region (South Upper region: 56%; P = 0.0153) were significantly associated with higher prevalence. Interestingly, the presence of a vaccination center was significantly associated with receiving at least one HCW-recommended vaccine (yes: 39.3%, no: 28%, not sure: 26.9%; P = 0.0018). No significant associations were found for gender, residence, nationality, or generation (P > 0.05).
Attitudes towards booster vaccination
More than 90% of the participants agreed that vaccination is useful and safe and that everyone should be vaccinated. Additionally, 92.2% of participants recognized the necessity of booster doses to ensure adequate protection (Table 3). Interns demonstrated higher awareness of revaccination importance and compliance (37%) compared to clinical and academic students (28.1% and 31.7%, respectively; P < 0.001). Conversely, clinical students exhibited awareness but uncertainty regarding full vaccination, while academic students were more likely to encounter this information for the first time compared to interns and clinical students. Type of residence (urban: 34.4% vs. rural: 28%; P = 0.0116), presence of a vaccination center (yes: 34.7%, no: 22%, not sure: 22.9%; P = 0.0038), and nationality (Egyptian: 31% vs. non-Egyptians: 41.3%; P = 0.0009) were also significantly associated with awareness of the need for revaccination. Interestingly, over 50% of the participants reported an intention to take booster doses or at least perform a blood analysis to ensure immunity.
Regarding the mandatory nature of booster vaccination, approximately 88% and 67% of the participants believed that these vaccines should be mandatory for medical staff and medical students, respectively. Interns were more likely to support mandatory vaccination than academic students (72% vs. 62.6%, P = 0.01). Additionally, females were more likely than males to endorse mandatory vaccination for medical students (71% vs. 63.5%, P = 0.002). Furthermore, 74% of participants indicated that they would advise their colleagues, friends, and family to receive booster vaccinations. Educational grade (Table 3) and type of residence (urban: 75.6% vs. rural: 70.8%; P = 0.044) were significantly associated with the intention to recommend booster vaccination. Moreover, the presence of a vaccination center at the participants’ institutions or governorates was significantly associated with the intention to recommend booster vaccination (yes: 38%, no: 15.6%, not sure: 15.4%; P = 0.0008). However, other sociodemographic characteristics, including gender, region, generation, and nationality, were not associated with this recommendation (P > 0.05).
Out of ten, our participants reported a median score of eight (IQR: 7–9) for efficacy, a median score of eight (IQR: 7–8) for safety, and a median score of five (IQR: 2–7) for hesitancy. Regarding efficacy, interns (median [IQR] score = 8 [7–9]) and clinical students (median [IQR] score = 8 [7–9]) were more likely (P < 0.0001) to have higher median scores than academic students (median [IQR] score = 7 [6–8]). In addition, Egyptian students had higher median efficacy scores than non-Egyptian students (median [IQR] = 8 [7–9] vs. 7 [6–8]; P < 0.0001). The presence of a vaccination center was also associated with higher efficacy scores (median [IQR] score = 8 [7–9] vs. 7 [5–8] for no; P < 0.0001).
Regarding safety, males (median [IQR] score = 8 [7–9] vs. 8 [7–8] for females; P = 0.0095), Egyptian students (median [IQR] score = 8 [7–9] vs. 7 [6–8] for non-Egyptians; P = 0.0157), and interns and clinical-year students (median [IQR] score = 8 [7–9] and 8 [7–9] vs. 8 [6–8] for academic-year; P < 0.0001] were more likely to have higher median scores (Table 4). The presence of a vaccination center was also associated with higher median scores (median [IQR] score = 8 [7–9] vs. 7 [6–8]; P = 0.005] for safety. Neither the type of residence nor region was associated with safety or efficacy (P > 0.05). Additionally, no significant association was found with hesitancy in any of the demographic data.
Factors affecting students’ opinions towards booster vaccination
The most influential factors in students’ opinions regarding the booster vaccination were scientific facts (60.1%) and senior physicians or professors (15%) (Fig. 2A). There was a significant association between the factors affecting students’ opinions and gender (P = 0.01), educational grade (P = 0.01), and nationality (P = 0.002). Academic students were more likely to be influenced by social media than interns (14.6% vs. 7.8%, P = 0.01). However, there was no significant association with other demographic factors (P > 0.05).

Factors influencing (A) and limitations (B) of vaccination with HCWs? recommended vaccines
Limitations of receiving booster doses
The main factors that prevented students from receiving vaccines were fear of vaccine side effects (44.9%) and lack of time (37%) (Fig. 2B). There was a significant association between students who chose fear of vaccine effects and gender (female: 51.9% vs. male: 38.3%; P < 0.0001), educational level (academic: 52.9% vs. clinical: 44.8% vs. interns: 35.6%; P < 0.0001), and residence type (urban: 47.1% vs. rural: 41%; P = 0.0447). Regarding students who cited a lack of time, there was a significant association with gender (males: 40% vs. females: 33.7%; P = 0.0268), educational grade (interns: 41.9% vs. clinical: 40.9% vs. academic: 29%; P = 0.0002), and nationality (Egyptian: 38.3% vs. non-Egyptian: 25.6%; P = 0.0062). Delta region (27.5%; P = 0.0126) was less likely to choose a lack of time. Participants residing in urban areas significantly reported lack of time (39.9% vs. 31.8%, P = 0.01) as the main factor limiting vaccination uptake, whereas rural residents reported high vaccination costs as the primary limitation (18.8% vs. 13.9%, P = 0.03).
Flu vaccine
Approximately 35% of participants were aware that influenza vaccination is one of the HCW-recommended vaccinations. Regarding vaccination rates, 17.6% reported receiving a seasonal flu vaccine in the past year and approximately 49.4% reported having been vaccinated at least once before. However, only 5.1% of students reported receiving a booster vaccine every season. Gender (males: 31.3% vs. females: 21.9%, P = 0.002), generation (non-first-generation: 31.6% vs. first-generation: 24.2%, P = 0.002), and educational grade (academic: 35.9% vs. clinical: 21.5%; P = 0.001) were significantly associated with receiving the flu vaccine multiple times, but not seasonally. In contrast, the type of residence and region did not affect the rate of influenza vaccination (P > 0.05).
COVID-19 vaccine
Notably, about 92% of the participants received at least one dose of COVID-19, and 79.4% received at least two doses of COVID-19 vaccine. Among those who received COVID-19 vaccination, the most commonly received COVID-19 vaccines were Oxford/AstraZeneca (27%) and Sinovac (25.9%). Regarding booster doses, 66.3% of our participants received at least one booster dose of the COVID-19 vaccine. Oxford/AstraZeneca (26%), Sinovac (25.4%), and Pfizer (21%) were the most commonly reported boosters. More than 75% of the participants expressed a willingness to receive a yearly booster if recommended. Gender (male: 60.5% vs. female: 39.5%; P = 0.028) and educational level (academic: 63.4% vs. clinical: 59.6% vs. interns: 47.4%; P < 0.001) were significantly associated with receiving two doses of COVID-19 vaccine (P = 0.03), whereas no significant associations were observed with other demographic factors.
Discussion
To the best of our knowledge, this is the first study from Egypt to examine the knowledge, attitude, and practice of medical students towards HCWs’ recommended vaccines across various educational levels, including interns. Overall, there was a positive attitude towards HCWs’ recommended vaccination. However, most participants had moderate knowledge with a gap in the actual practice of receiving vaccines.
Knowledge of HCWs’ recommended vaccines
Approximately 43% and 25% of the students showed moderate and high knowledge levels, respectively. Notably, knowledge increased with educational grade, particularly among interns and clinical-level students, compared to academic-year students. This difference in knowledge likely stems from the greater exposure of these students to clinical settings, which enables them to witness the impact of vaccination in real-world scenarios. Moreover, a more rigorous curriculum for clinical-level students encompasses comprehensive information about vaccinations, facilitating the accumulation of knowledge over time [20, 21]. These findings align with those of previous studies conducted in the United States and Europe [13, 22,23,24]. Similarly, gender showed a significant association with knowledge about HCWs’ recommended vaccines, with females being more likely to have higher knowledge than males which is inconsistent with previous studies from Europe that showed no difference [13].
Practice of participants towards HCWs’ recommended vaccines
Our study found a notable disparity between medical students’ knowledge and practice, as only 8.1% of participants reported receiving two or three recommended vaccines in the past decade. Consistent with literature, HBV vaccine had the highest rates of both knowledge (70.9%) and practice (66.7%), likely due to the high prevalence of HBV infection in Egypt [25]. Previous studies have reported similar findings in Vienna, and Pakistan, where the rate of HBV vaccination reached 80% [26, 27]. Conversely, varicella and meningococcal vaccines are the least known and received vaccines. In our study, the MMR vaccination rate was 29.2%, which is lower than the average vaccination rates reported in several European countries which was about 80% [13].
Similar to knowledge, interns were more likely to receive booster vaccination which is consistent with findings from previous studies [13]. However, there was no significant difference in booster vaccination rates between academic- and clinical-year students or between male and female students. Having a vaccination center at the participants’ institutions or in their respective regions was positively correlated with increased knowledge and vaccine uptake. This underscores the potential of these centers to raise awareness and promote adherence to the recommended vaccines among healthcare students.
Attitude of participants towards HCWs’ recommended vaccines
The participants expressed positive views on vaccine safety and effectiveness, with little variation. Consistent with the literature, the majority (91%) of participants believed that vaccines were safe and effective [26, 28]. Attitudes towards booster vaccines were also positive due to awareness of the need for revaccination. Medical training and clinical exposure influenced attitudes, with interns and clinical year students reporting higher scores. Although 90% of the participants agreed that vaccination was safe and that everyone should be vaccinated, only 74% would recommend booster vaccinations to their colleagues, friends, and family. This discrepancy may reflect vaccine hesitancy among the participants. Our study found a median hesitancy score of 5/10, with 7.2% of the participants expressing uncertainty or unwillingness to receive booster vaccines. Similar hesitancy patterns are observed among medical students regarding influenza, COVID-19, and HBV vaccines [13, 24,25,26].
Factors that limit vaccine uptake
When participants were asked about reasons that might prevent them from receiving booster vaccinations, 44.9% reported their fear of side effects as a major concern. This fear could be influenced by misinformation regarding the side effects of COVID-19 vaccines that circulated just before this study was conducted [29, 30]. Interestingly, most of those who reported fear as a limitation were students in their academic years. Meanwhile, interns and students in their clinical years cited a lack of time as the main limitation. Additionally, participants from urban areas were more likely to cite lack of time as a limitation.
Factors that influence vaccine uptake
The most influential factors shaping medical students’ opinions on vaccination were scientific facts (60.1%), and senior physicians or professors (15%). Interns (63%) and clinical students (62.7%) were more likely to form opinions based on scientific facts. Interestingly, participants who reported social media as an influencing factor had less positive attitudes towards vaccine safety and efficacy than those influenced by scientific facts or senior physicians. These observations highlight the need for evidence-based and accurate information regarding the dissemination of vaccines among healthcare students.
Flu vaccine
Our study found that only 35% of the participants were aware that the flu vaccine is recommended for HCWs, ranking fourth on the list. Additionally, while 49.4% reported receiving at least one influenza vaccine shot, only 17.6% had received a shot within the previous year, which is similar to the results of a previous study [12]. Surprisingly, academic students were more likely to have received the seasonal flu vaccine in the past year than clinical students and interns, in contrast to the findings of Walker et al. [12] but consistent with Rostkowska et al. and Gray et al. [13, 31]. This may be due to academic students’ greater exposure to vaccination opportunities on university campuses and their compliance with vaccination requirements for attending classes or clinical placements [32].
COVID-19 vaccine
Approximately 80% of the participants in our study received at least two doses of the COVID-19 vaccine, consistent with findings in Egypt, and nearly double the rate of the general population (44.3%) [16, 33]. This high vaccination rate may be attributed to the government’s requirement for all university students to be vaccinated before returning to campus, after the lockdown measures were lifted. Notably, this trend aligns with the higher coverage rates among healthcare workers in Germany (91.7%), Italy (82%), Portugal (87%), and Greece (81.9%). Similar to the pattern observed for influenza vaccination, academic students were more likely to receive the COVID-19 vaccine than clinical students and interns.
Limitations of our study
Although our study has several strengths, including having participants from all study years in nine institutions, with a high response rate of 86.4%, some limitations should be considered. First, we were unable to collect data from the Fayoum geographic region, which represents less than 5% of all Egyptian medical students. Second, the timing of our questionnaire, conducted shortly after the onset of the COVID-19 pandemic, may have influenced some results, particularly the attitudes toward vaccination. Additionally, due to questionnaire length constraints, we could not include sections on other vaccines beyond flu and COVID-19, which were prioritized given the ongoing pandemic.
Conclusions
Overall, medical students showed intermediate knowledge of HCWs’ recommended vaccines with a positive attitude towards vaccination. The participants expressed strong agreement on the safety and efficacy of the vaccines with neutral hesitancy. Additionally, the students supported the implementation of mandatory booster vaccines for both the staff and students. However, there is still a gap in vaccination practices. Therefore, we recommend initiating vaccination campaigns to raise awareness and enhance vaccination practices, particularly for medical education and training.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- CDC:
-
Center for Disease Control
- COVID-19:
-
Coronavirus Disease of 2019
- DTaP:
-
Diphtheria, Tetanus, Pertussis
- HBV:
-
Hepatitis B Virus
- HCWs:
-
Healthcare care workers
- IQR:
-
Interquartile range
- MMR:
-
Measles, Mumps, Rubella
- WHO:
-
World Health Organization
References
Recommended Vaccines for Healthcare Workers | CDC. [https://www.cdc.gov/vaccines/adults/rec-vac/hcw.html].
Immunization of Health-Care Workers. Recommendations of the Advisory Committee on Immunization Practices (ACIP) and the hospital infection control Practices Advisory Committee (HICPAC) [https://www.cdc.gov/mmwr/preview/mmwrhtml/00050577.htm].
Zhu Y, Liu S, Zhang D. Effectiveness of COVID-19 vaccine Booster Shot compared with Non-booster: a Meta-analysis. Vaccines (Basel) 2022, 10(9).
Andrews N, Stowe J, Kirsebom F, Toffa S, Sachdeva R, Gower C, Ramsay M, Lopez Bernal J. Effectiveness of COVID-19 booster vaccines against COVID-19-related symptoms, hospitalization and death in England. Nat Med. 2022;28(4):831–7.
Siddiqui M, Salmon DA, Omer SB. Epidemiology of vaccine hesitancy in the United States. Hum Vaccin Immunother. 2013;9(12):2643–8.
Suryadevara M, Handel A, Bonville CA, Cibula DA, Domachowske JB. Pediatric provider vaccine hesitancy: an under-recognized obstacle to immunizing children. Vaccine. 2015;33(48):6629–34.
Paterson P, Meurice F, Stanberry LR, Glismann S, Rosenthal SL, Larson HJ. Vaccine hesitancy and healthcare providers. Vaccine. 2016;34(52):6700–6.
Freed GL, Clark SJ, Butchart AT, Singer DC, Davis MM. Sources and perceived credibility of vaccine-safety information for parents. Pediatrics. 2011;127(Suppl 1):S107–112.
Kasting ML, Wilson S, Dixon BE, Downs SM, Kulkarni A, Zimet GD. A qualitative study of healthcare provider awareness and informational needs regarding the nine-valent HPV vaccine. Vaccine. 2016;34(11):1331–4.
Afonso N, Kavanagh M, Swanberg S. Improvement in attitudes toward influenza vaccination in medical students following an integrated curricular intervention. Vaccine. 2014;32(4):502–6.
Loulergue P, Fonteneau L, Armengaud JB, Momcilovic S, Levy-Bruhl D, Launay O, Guthmann JP. Studyvax survey g: vaccine coverage of healthcare students in hospitals of the Paris region in 2009: the Studyvax survey. Vaccine. 2013;31(26):2835–8.
Walker L, Newall A, Heywood AE. Knowledge, attitudes and practices of Australian medical students towards influenza vaccination. Vaccine. 2016;34(50):6193–9.
Rostkowska OM, Peters A, Montvidas J, Magdas TM, Rensen L, Zgliczyński WS, Durlik M, Pelzer BW. Attitudes and Knowledge of European Medical Students and early graduates about vaccination and self-reported Vaccination Coverage-multinational cross-sectional survey. Int J Environ Res Public Health 2021, 18(7).
Prüss-Ustün A, Rapiti E, Hutin Y. Estimation of the global burden of disease attributable to contaminated sharps injuries among health-care workers. Am J Ind Med. 2005;48(6):482–90.
Saied SM, Saied EM, Kabbash IA, Abdo SAE. Vaccine hesitancy: beliefs and barriers associated with COVID-19 vaccination among Egyptian medical students. J Med Virol. 2021;93(7):4280–91.
Hamad AA, Selim R, Amer BE, Diab RA, Elazb M, Elbanna EH, Mrge Collaborative G, Negida A. COVID-19 Risk Perception and Adherence to Preventive Measures among Medical Students after Receiving COVID-19 Vaccination: A Multicenter Cross-Sectional Study in Egypt. Vaccines (Basel) 2022, 11(1).
Barattucci M, Pagliaro S, Ballone C, Teresi M, Consoli C, Garofalo A, De Giorgio A, Ramaci T. Trust in Science as a possible mediator between different antecedents and COVID-19 booster vaccination intention: an integration of Health Belief Model (HBM) and theory of planned behavior (TPB). Vaccines (Basel) 2022, 10(7).
Champion VLaS CS. The Health Belief Model. In: Glanz, K., Rimer, B.K. and Viswanath, K. Eds.Theory, research, and practice. 4th Edition, Jossey-Bass, San Francisco, 189–193. Health behavior and health education 2008.
Ajzen I. The theory of planned behavior: frequently asked questions. Hum Behav Emerg Technol 2020, 2.
Kimberly MDB. Medical Student Knowledge, attitudes, and practices regarding immunization. J Vaccines Vaccination 2012, 06(01).
Sanftenberg L, Roggendorf H, Babucke M, Breckwoldt J, Gaertner B, Hetzer B, Lendeckel A, Riemenschneider H, Voigt K, Keplinger A, et al. Medical students’ knowledge and attitudes regarding vaccination against measles, influenza and HPV. An international multicenter study. J Prev Med Hyg. 2020;61(2):E181–5.
Banaszkiewicz A, Talarek E, Śliwka J, Kazubski F, Małecka I, Stryczyńska-Kazubska J, Dziubak W, Kuchar E. Awareness of influenza and attitude toward influenza vaccination among medical students. Adv Exp Med Biol. 2016;934:83–8.
Dybsand LL, Hall KJ, Carson PJ. Immunization attitudes, opinions, and knowledge of healthcare professional students at two midwestern universities in the United States. BMC Med Educ. 2019;19(1):242.
Berera D, Thompson KM. Medical Student knowledge, attitudes, and practices regarding immunization. J Vaccines Vaccin. 2015;6(268):2.
Azzam A, Khaled H, Elbohy OA, Mohamed SA, Mohamed SMH, Abdelkader AH, Ezzat AA, Elmowafy AOI, El-Emam OA, Awadalla M, et al. Seroprevalence of hepatitis B virus surface antigen (HBsAg) in Egypt (2000–2022): a systematic review with meta-analysis. BMC Infect Dis. 2023;23(1):151.
Kunze U, Schweinzer H. Self-reported vaccination status and attitudes towards mandatory vaccinations for health care workers among medical students. Vaccine. 2020;38(35):5695–9.
Soomar SM, Siddiqui AR, Azam SI, Shah M. Determinants of hepatitis B vaccination status in health care workers of two secondary care hospitals of Sindh, Pakistan: a cross-sectional study. Hum Vaccin Immunother. 2021;17(12):5579–84.
Arlt J, Flaegel K, Goetz K, Steinhaeuser J. Regional differences in general practitioners’ behaviours regarding influenza vaccination: a cross-sectional study. BMC Health Serv Res. 2021;21(1):197.
Lucia VC, Kelekar A, Afonso NM. COVID-19 vaccine hesitancy among medical students. J Public Health (Oxf). 2021;43(3):445–9.
Strouthou E, Karageorgos SA, Christaki E, Agouridis AP, Tsioutis C. Medical students’ attitudes and perceptions of influenza and SARS-CoV-2 vaccination in Cyprus. Germs. 2022;12(2):180–94.
Gray G, Cooper J. An evaluation of influenza vaccine uptake in UK medical students. Occup Med (Lond). 2021;71(2):105–8.
Abdelkader FA, Alkubati SA, Alsabri M, McClean C, Albagawi B, Alsaqri SH, Al-Areefi M, Abo Seada AI. COVID-19 vaccination knowledge, perception, and reason for adherence and nonadherence among nursing students in Egypt. SAGE Open Nurs. 2022;8:23779608221141234.
Kandeel A, Eldeyahy I, Abu ElSood H, Fahim M, Afifi S, Abu Kamar S, BahaaEldin H, Ahmed E, Mohsen A, Abdelghaffar K. COVID-19 vaccination coverage in Egypt: a large-scale national survey - to help achieving vaccination target, March-May, 2022. BMC Public Health. 2023;23(1):397.
Acknowledgements
The authors acknowledge Amr Mahmoud, Enas Sherif, Ibrahim Al-Kurd, Nourhan Omar, Rawda M. Shehab, Seham Faried, Youssef Gouda (Benha University), Abdelrahman Hendawy, Hanan Zakaria, Marwa Ewis, Mohamed Basyouni, Salma Yahia, Zyad Shafik (Menoufia University), Ahmed Ismail, Ali Alsous, Canny Salah, Eiman Abd-Elaziz, Eman Gamal, Haneen Ibrahim, Khaled Elsebaei, Mahmoud Lotfy, Menna Borg, Mohamed Ashraf, Nada Mahdy, Osama Elzankaly, Rowan Khaled, Sara AlaaEldin, Seif Yameny, Shahd Radwan, Touqa Qotb, Yehia Orabi (Alexandria University), Abdelrahman Ouda, Ahmed Mutasim, Karem Hatem, Menna Rashad, Nagham Abdelhalim, Nour Khaled, Nouran Saffan, Rawan Elsayed, Rudayna Mahgoub, Shehab Moawad, Yasmin Elsayed, Youssef Mamdouh (Cairo University), Ahmed Sofyan, Ahmed Tantawy, Amany Refaat, Arwa Anwar, Esraa Mahmoud, Mohamed Elmasry (Helwan University), Mansour Algazar, Mohammed Refaat, Mohamed Nasser, Muhammad Ragab (Al-Azhar University), Ahmed Mahmoud, Esraa Abdelbaset, Mahmoud Shahat, Mayar Madny, Mervat Shehata, Mostafa Abo-elwafa, Sameh El-Hawary, Zahra Mahmoud (South Valley University), and Ahmed Faek, Esraa Soliman, Mohamed Eladl, Mohamed Abdallah, Mohamed Elmahdy, Mohamed Salah, Mostafa Salem, Nada Khaled, Omar Abu-El-Nasr, Samar Abdel-Rahim, Yasmin Abdel-Aziz, Yassmin Amir, (Zagazig University) for their highly-valued assistance in data collection.
Funding
No funds, grants, or other support were received.
Open access funding provided by The Science, Technology & Innovation Funding Authority (STDF) in cooperation with The Egyptian Knowledge Bank (EKB).
Author information
Authors and Affiliations
Contributions
MMS, YME, MBB, and OAA have generated the idea and participated in methodology and manuscript writing. MMS, MBB, and OAA analyzed the data. AA, ESI, AE, MAK, ASG, AN, MM, TE, and MMN participated in data collection and revised the manuscript. ARA, AHA, AAB, MIE, MAE, LS, MTK, and MAG participated in the methodology. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study protocol was approved by the Institutional Review Board at Faculty of Medicine, Benha University. The methods were carried out in accordance with relevant guidelines and regulations. Prior to data collection, we obtained informed consent from all participants after explaining their rights and duties in accordance with the Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Mohamed Shawqi, M., El-Said, Y.M., Behery, M.B. et al. Knowledge, attitude, and practice of Egyptian medical students towards healthcare workers’ recommended vaccines: a nationwide cross-sectional survey. BMC Med Educ 24, 876 (2024). https://doi.org/10.1186/s12909-024-05712-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12909-024-05712-8