
Abstract
Background
Surgical ward rounds are key element to point-of-care interprofessional postoperative treatment and technical and communicational aspects are relevant for the patient’s safety and satisfaction. Due to COVID-19 restrictions, the training opportunity of experiencing a face-to-face surgical ward round was massively hampered and thus, we developed a digital concept. This study aims to investigate the feasibility of video-transmitted ward rounds integrating surgical and communicational aspects with live streaming from wards. Further, medical students were asked for their satisfaction and their subjective learning success.
Methods
The proof-of-concept study consisted of self-reported subjective evaluation of competences in ward round skills. Qualitative feedback was collected to gain deeper insight and students’ empathy was rated by using the student version of the Jefferson Empathy Scale (JES).
Results
One hundred three medical students participated. The students were satisfied with the video-transmitted ward round (M = 3.54; SD = 1.22). In the subjective evaluation students’ ward round competencies rose significantly (p < .001, Mpre = 3.00, SD = 0.77; Mpost = 3.76, SD = 0.75). The surgeon was rated as empathic (M = 119.05; SD = 10.09). In the qualitative feedback they named helpful aspects like including an expert for communication. However, they preferred the face-to-face setting in comparison to the digital concept.
Conclusions
It was feasible to implement a video-transmitted ward round within a pandemic. The format worked technically, was well-accepted and also led to a subjective rise in the students’ competencies. Video-transmitted ward rounds may be integrated to support the medical education, though, they cannot replace the face-to-face setting.
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Introduction
Surgical ward rounds are key element to point-of-care interprofessional postoperative treatment of surgical patients, which warrants central importance in medical education, too [1]. Although ward round teaching is important in every clinical discipline, particularly in surgery specific training is needed to provide a well-structured and focused yet complete physical examination [2,3,4]. Besides the technical aspects a surgical ward round also contains aspects of communication and interaction pivotal to effective and safe patient care as well as patient satisfaction [5,6,7,8,9]. This is also mirrored in the surgical assessment tool (SWAT) that includes non-technical ward round skills like communication and teamwork as important pillars for effective ward rounds in surgery [10]. As consultants may be unaware of the communicational learning opportunities, efforts to explicitly integrate communication aspects into surgical ward round teaching should be made [11].
Due to COVID-19 restrictions, the training opportunity of experiencing a face-to-face surgical ward round was massively hampered since summer term 2020 as students were not allowed any direct patient contact in teaching [12, 13]. On the other hand, the pandemic was a massive catalyst for the development and implementation of digital learning resources worldwide [14]. Most of these relied heavily on digital communication methods enabled by IP-based tools like videoconferencing software or learning platforms [15]. Clinical educators tried to counterbalance the loss of direct patient contact by specific virtual teaching sessions including display of treatment of COVID-19 patients or correct handling of personal protective equipment (PPE) on wards [16,17,18]. Also, as several specialties were pretty strained with care for COVID-19 patients and couldn’t offer specific standalone teaching, students were integrated into regular telemedical treatment sessions and learned in kind of a virtual bedside teaching environment [19]. There have also been a variety of attempts to specifically create virtual ward round settings. Glasgow and colleagues for example modified a usual surgical multi-professional ward round: only the attending surgeon was in the room with the patient wearing a hands-free headset whilst the rest of the team were attending online [20]. The majority of the team members and the patients considered it a good substitute in a pandemic. However, as this study included no medical students such a setting might only work for persons already trained in and familiar with the subject. Another study group tried a mixed reality version of a surgical ward round with the physician wearing a HoloLens 2™ whilst in the patient’s room [21]. Although this concept was evaluated as feasible, well-accepted and effective, it only included 11 students in the study which limits generalisability. Also, via the HoloLens 2™ it only allowed an interaction with the surgeon but not with the patient, which might prevent successful active learner involvement deemed so necessary in effective workplace-based learning [22, 23]. Additionally, it didn’t use the normal ward round setting of a surgical ward but specifically taught two selected patients in 60 min making it more a profound kind of bedside teaching than an actual surgical ward round.
Thus, to the best of our knowledge, there hasn’t been any attempt to preserve the traditional surgical ward round to teach medical students this complex skill in a time where direct patient contact was prohibited.
At our surgical department, teaching started as a complete virtual course with asynchronous and synchronous elements but without any patient contact. In 2021, at least seminar teaching was allowed in presence although direct face-to-face patient contacts were still prohibited. We thus created a video-transmitted ward round concept including surgical and communicational aspects of ward rounds with live streaming from wards. With this study, we wanted to prove that such a setting was feasible to perform, worked in its hybrid form, was well-accepted by students, and showed a positive subjective learning effect regarding key elements of ward round competencies.
Materials
Study design
We conducted a proof-of-concept study with self-reported evaluation of the acquired competences in ward round skills as well as satisfaction with its implementation. Additionally, we collected qualitative feedback to gain deeper insight. Furthermore, we examined the physician–patient interaction using the Jefferson Empathy Scale.
Sample
In total, 103 Students participated in the study. Of these were 69.9% female and 30.1% male which corresponds to the general gender relation at the Medical Faculty of Tübingen. 92.9% of the students were in the 9. Semester forming the regular target group while 2.9% and 3.9% were in the 8th and 10th semester taking part in the course earlier or later than regularly scheduled. Eligibility criteria were being medical students attending courses of clinical examination and understanding German.
Teaching procedure
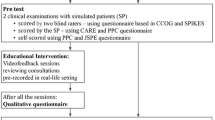
The ward round teaching took place within the regular surgical class in year 5 on a weekly basis. On the introductory day, there was a 45min seminar on theoretical background followed by the practical teaching on day 4. It lasted 150min and was taught as a face-to-face seminar by one surgeon and one liaison psychiatrist to reflect on technical as well as non-technical skills within a ward round. The corresponding ward round streamed to the students was performed on a regular ward of the department of visceral surgery, University Hospital Tübingen, Germany. The ward round team included the class surgeon and a nurse, as well as potentially other health care professionals and/or nurses in training or final-year medical students. The liaison psychiatrist stayed with the students in the seminar room the whole time. During the surgeon’s absence she discussed with the students topics regarding communication and interaction on the one hand and moderated the communication between the observing students group and the ward group (for a more comprehensive overview, please see Fig. 1). 16 students took part in the ward round per unit. 12 surgeons of the department of General, Visceral and Transplant Surgery taught the students. One patient was part of the ward round per unit. In total 14 Patients participated in the study course. The patients' diseases were in the field of general surgery.

Video-transmittedl ward round teaching elements
The technical setup comprised an Apple iPad mini for the actual ward round and a standard laptop with external monitor in the seminar room, both connected via an end-to-end encrypted “Zoom” connection approved by the hospital’s data security office for patient streaming. Due to the bidirectional audio-visual connection, all participants (ward and seminar room) could see and interact with each other. The Students could especially ask questions to the team and the patient.
Measurement
At the end of the face-to-face teaching seminar students filled in a questionnaire containing questions on their subjective rating of ward round competencies as well as satisfaction with and helpfulness of the course. Additionally, structural and technical aspects of the video-transmitted ward round (e.g. efficiency of the round itself, visibility of the patient or integration of nurse) were assessed. All items ranged on a Likert Scale from 1 (“not at all”) to 5 (“very”). An example item was “how satisfied were you with the general organization of the ward round.”. Furthermore, students rated the surgeon’s empathy in the observed ward round using the student version of the Jefferson Empathy Scale (JES). The JES is a standardizedquestionnaire and consists of 20 items ranging from 1 (“do not agree at all”) to 7 (“completely agree”) [24]. The JES is highly reliable and validated [25]. A value under 80 indicates little empathy while 140 is the highest score indicating a high level of empathy [25]. To cover for the digital aspect, we also asked for technical difficulties experienced in the session and students’ course preference (digital/in-person) using dichotomous answers (yes/no). Furthermore, students could made comments in the qualitative feedback section regarding the teaching course.
Statistical analysis
Quantitative data were evaluated by using IBM SPSS Statistics version 27. Frequencies, percentages, mean values (M) and standard deviations (SD) were calculated. Data was tested normally distributed by using Kolomogrow Smirnow-test. T-test for dependent samples were used to test for differences in the competencies before and after the course. The level of significance was set to p < 0.05. Qualitative feedback was evaluated in thematic content analysis based on Braun & Clark (2006) using Microsoft Excel, and themes in the dataset were identified, analysed and documented [26]. Based on the qualitative data codes and categories were inductively generated and after examining them topics were built [26].
Ethics
The study was approved by the Ethics Committee of the University Clinic of Tübingen, Project Nr. 272/2021BO2. It was conducted in accordance to the relevant guidelines and regulations and in accordance to the Declaration of Helsinki. Participation was voluntary, and all participants gave their informed written consent. All patients involved were thoroughly informed beforehand and gave their written consent. Patients below the age of 18 or with a limited understanding of German were excluded from participation in the study.
Results
Overall, students were satisfied with the video-transmitted ward round course rating it with M = 3.54 (SD = 1.22). The Helpfulness of the course was rated with M = 3.92 (SD = 1.01).
In the subjective evaluation students’ ward round competencies rose significantly (p < 0.001) from M = 3.0 (SD = 0.77) to M = 3.76 (SD = 0.75) in a pre-post comparison.
Students considered the teacher’s explanation of the lab results as very good (M = 4.73, SD = 0.64). The ward round itself was considered highly efficient (M = 4.64, SD = 0.58). They were also very happy with the explanation of the bedside examination within the ward round (M = 4.77, SD = 0.54). Regarding the interprofessional ward team, the involvement of the nurse was rated relatively high with M = 3.84 (SD = 0.93) reflecting standard operational procedures on the ward. The ward round surgeon was rated as highly empathic by the students with M = 119.05 (SD = 10.09).
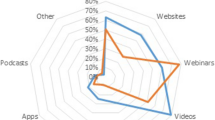
Also, the rating of technical aspects was generally positive (for further details, please see Fig. 2); only 8.7% of the students rated technical difficulties with disruptions of the visual connection, reduced sound quality or a break down of the connection as most commonly mentioned.

Rating of technical aspects of the video-transmitted ward round. Likert Scale 1–5
Rating of the video-transmitted ward round technical aspects.
In general, students appreciated aspects of structure and interprofessional teaching, though still were in favour of face-to-face ward rounds (87.4%) if allowed again. The following thematic topics could be found based on the qualitative analysis: helpful aspects of the video-transmitted ward round, room for improvement, content to be kept after the pandemic and reasons for preference of format (online versus face-to-face). Please see Table 1 for more details.
Discussion
With this study, we could show that it was feasible to implement a video-transmitted ward round into regular training of undergraduate medical students within a pandemic. The format worked technically, was well-accepted by the target group and also led to a subjective significant rise in surgical ward round competencies of medical students deemed necessary for adequate treatment of surgical inpatients [1].
Due to a structured educational model, explicit teaching of usually implicitly taught skills like communication aspects of a ward round, was implemented and appreciated by students. This was in line with literature stating the importance of communicational aspects of a ward round for patient care and safety as well as the surgeon’s role as a communicator [27,28,29,30,31]. The two-way interaction possibility with all participants involved (interprofessional healthcare team, patient, students) and here especially the possibility to ask questions also made the students feel fully integrated and part of the actual ward round preventing an otherwise commonly observed effect of disengagement all be it in a digital environment [16, 22, 23]. Their appreciation of a more immediate contact is in line with other findings and corroborates well-established concerns of usual surgical ward rounds [20, 21, 32].
The ward round is also a central point for interprofessional care, where crucial aspects of patients are discussed in the team of healthcare professionals [33]. Interprofessional collaboration has been labelled a crucial factor in reducing complications and mortality in patients [34]. In this study, students observed a full integration of the ward nurse and mentioned it as a pivotal learning effect of the session. Raising awareness for the interprofessional aspects within a surgical ward round is a fundamental component of patient-safety [3, 35].
Digital formats for teaching within the pandemic had so far focussed either on the care of actual COVID-19 patients, created specific designs for ward round teaching, or simply let students sit by routine telemedical encounters [17,18,19, 21]. Although these concepts offer a valuable teaching opportunities, our intention was specifically to preserve the skill of conducting a surgical ward round making use of digital concepts already proven helpful in general bedside teachings [36].
A well-known issue in ward round teaching is, that students lack a structure as also mirrored in our study. Although checklists have shown to be helpful for basic structure, its value to improve the actual communication and interaction on the ward is still unclear [1, 37,38,39]. We thus used a designated, structured teaching concept, explicitly covering all aspects and key competencies of the ward round cycle – as demanded by research in this field [40, 41]. Especially the interaction and the students’ willingness to ask questions can be improved by such targeted interventions [42].
In this study, the performing surgeon was rated as very empathic. This is particularly important in light of the fact that physicians are eagerly observed by students and act as role models [43]. Awareness to this fact should be risen to all teaching faculty stuff as it is well-proven that positive role models encourage interest in the subject and consequently positively influence career choice [44]. It is also well-known that patient subjectively rate their treatment outcome higher when they consider their surgeon as more empathic [45].
A big issue with digital teaching is the technical component and possible failure of devices or transmission [46]. In this study, the technical side worked pretty well with only a very small group (8.7%) reporting issues. Although most of these were rather minor, it is of utmost importance to guarantee high quality audio-visual set-ups to give a realistic impression and feeling of emersion when performing a video-transmitted ward round. Therefore, the help and support of specialized technical staff should be made available in the faculties particularly if even more digitally advanced elements like augmented or virtual element features are to be integrated [47, 48].
Understandably, students in our study were currently more inclined to have a face-to-face ward round than a digital one which is in line with other findings on bedside teaching settings [20, 49]. However, the dynamics driven by the COVID-19 pandemic may be the catalyst to meticulously scrutinize the positive effects of virtual ward rounds for transfer potential in face-to-face settings combining the best of two worlds and train competent surgeons of the future. Therefore it is relevant to stress that the Students mentioned a better visibility and comprehensibility of the clinical encounters which may be related to the fact that all viewers had the same perspective close to the Patient. In a real world patients room there is usually only a limited space with reduced visibility for some students. We will study this in the future with the help of 3D Videos of ward round situations.
Having one perspective on the situation enabled also a better postexposure discussion as all participants had watched the same footage this corresponds to the helpfulness of videos as a reflexive instrument [50]. Due to the nature of video streams this visualisation was transitory for the future a recorded version of the ward round could help this process even further.
There are some limitations to this study. First, it was within one semester and one medical faculty only which may limit generalisability. Second, we only measured the students’ subjective gain in competency. Future studies should evaluate skills acquired through video-transmitted ward rounds in either real war round settings or simulated sessions objectively. Finally, it was not possible to compare the digital concept to a face-to-face setting due to the Covid-19 restrictions, we only asked the medical students’ perspective. Further research should investigate this comparison to confirm our finding on students’ preference of a face-to-face setting. Furthermore, the patient’s perspective was not assessed in the study. So, we could not compare the patient’s and students’ perspective regarding the physician’ s empathy. Future research should also involve the patient’s perspective. In this study, we decided us against the patient’s perspective as we focused on the feasibility. However, despite these limitations we feel confident that this study contributes significantly to the insights of digital teaching concepts with regards to surgical ward rounds.
Conclusions
This study showed that it is possible to transfer the powerful tool of ward round teaching successfully into a digital format. Further studies should focus on more detailed and specific components of the ward round and the patients’ perception of such an offer as well as on the transfer potential of digitally helpful elements in a face-to-face ward round structure. Moreover, the communications aspects and the integration of ward nurses should be focused more specifically in future research as, in this study, they might be addressed as implicit manners.
Availability of data and materials
The datasets used and/or analysed during this study are available from the corresponding author on reasonable request.
References
Pucher PH, Aggarwal R. Improving ward-based patient care: prioritizing the ward round in training and practice. Ann Surg. 2016;263(6):1075–6.
Vietz E, März E, Lottspeich C, Wölfel T, Fischer MR, Schmidmaier R. Ward round competences in surgery and psychiatry - a comparative multidisciplinary interview study. BMC Med Educ. 2019;19(1):137.
Pucher PH, Aggarwal R, Darzi A. Surgical ward round quality and impact on variable patient outcomes. Ann Surg. 2014;259(2):222–6.
Shetty K, Poo SXW, Sriskandarajah K, Sideris M, Malietzis G, Darzi A, Athanasiou T. “The longest way round is the shortest way home”: an overhaul of surgical ward rounds. World J Surg. 2018;42(4):937–49.
Leonard M, Graham S, Bonacum D. The human factor: the critical importance of effective teamwork and communication in providing safe care. Qual Saf Health Care. 2004;13 Suppl 1(Suppl 1):i85-90.
Mast MS. On the importance of nonverbal communication in the physician-patient interaction. Patient Educ Couns. 2007;67(3):315–8.
Griffith CH 3rd, Wilson JF, Langer S, Haist SA. House staff nonverbal communication skills and standardized patient satisfaction. J Gen Intern Med. 2003;18(3):170–4.
Pucher PH, Aggarwal R, Singh P, Tahir M, Darzi A. Identifying quality markers and improvement measures for ward-based surgical care: a semistructured interview study. Am J Surg. 2015;210(2):211–8.
Leape LL, Berwick DM. Five years after To Err Is Human: what have we learned? JAMA. 2005;293(19):2384–90.
Ahmed K, Anderson O, Jawad M, Tierney T, Darzi A, Athanasiou T, Hanna GB. Design and validation of the surgical ward round assessment tool: a quantitative observational study. Am J Surg. 2015;209(4):682-688.e682.
Dewhurst G. Time for change: teaching and learning on busy post-take ward rounds. Clin Med (Lond). 2010;10(3):231–4.
Loda T, Löffler T, Erschens R, Zipfel S, Herrmann-Werner A. Medical education in times of COVID-19: German students’ expectations - a cross-sectional study. PLoS One. 2020;15(11):e0241660–e0241660.
Whelan A, Prescott J, Young G, Catanese V, McKinney R. Interim guidance on medical students' participation in direct patient contact activities: principles and guidelines. Washington, DC: Association of American Medical Colleges; 2020. p. 30. https://www.aamc.org/media/43311/download.
Rose S. Medical Student Education in the Time of COVID-19. JAMA. 2020;323(21):2131–2.
Hilburg R, Patel N, Ambruso S, Biewald MA, Farouk SS. Medical education during the Coronavirus disease-2019 pandemic: learning from a distance. Adv Chronic Kidney Dis. 2020;27(5):412–7.
Hofmann H, Harding C, Youm J, Wiechmann W. Virtual bedside teaching rounds with patients with COVID-19. Med Educ. 2020;54(10):959–60.
Runge A, Wray A, Harding C. Virtual COVID rounds: A curricular enrichment program for pre-clinical medical students. Med Educ. 2021;55(5):661–661.
Bavare AC, Goldman JR, Musick MA, Sembera KA, Sardual AA, Lam AK, Tume SC, Thammasitboon SX, Williams EA. Virtual communication embedded bedside ICU rounds: a hybrid rounds practice adapted to the coronavirus pandemic. Pediatr Crit Care Med. 2021;22(8):e427–36.
Safdieh JE, Lee JI, Prasad L, Mulcare M, Eiss B, Kang Y. Curricular response to COVID-19: real-time interactive telehealth experience (RITE) program. Med Educ Online. 2021;26(1):1918609–1918609.
Glasgow S, Saha P, Moore H, James B, Newsholme W, Zayed H. Perception and acceptability of virtual ward round reviews of vascular inpatients to preserve resources and reduce infection risk in the COVID-19 era. Eur J Vasc Endovasc Surg. 2021;61(3):527–8.
Bala L, Kinross J, Martin G, Koizia LJ, Kooner AS, Shimshon GJ, Hurkxkens TJ, Pratt PJ, Sam AH. A remote access mixed reality teaching ward round. Clin Teach. 2021;18(4):386–90.
Dornan T, Boshuizen H, King N, Scherpbier A. Experience-based learning: a model linking the processes and outcomes of medical students’ workplace learning. Med Educ. 2007;41(1):84–91.
van der Zwet J, Zwietering PJ, Teunissen PW, van der Vleuten CP, Scherpbier AJ. Workplace learning from a socio-cultural perspective: creating developmental space during the general practice clerkship. Adv Health Sci Educ Theory Pract. 2011;16(3):359–73.
Hojat M, Mangione S, Nasca TJ, Cohen MJM, Gonnella JS, Erdmann JB, Veloski J, Magee M. The Jefferson Scale of Physician Empathy: development and preliminary psychometric data. Educ Psychol Measur. 2001;61(2):349–65.
Hojat M, DeSantis J, Shannon SC, Mortensen LH, Speicher MR, Bragan L, LaNoue M, Calabrese LH. The Jefferson Scale of Empathy: a nationwide study of measurement properties, underlying components, latent variable structure, and national norms in medical students. Adv Health Sci Educ Theory Pract. 2018;23(5):899–920.
Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101.
Greenberg CC, Regenbogen SE, Studdert DM, Lipsitz SR, Rogers SO, Zinner MJ, Gawande AA. Patterns of communication breakdowns resulting in injury to surgical patients. J Am Coll Surg. 2007;204(4):533–40.
Frank JR, Danoff D. The CanMEDS initiative: implementing an outcomes-based framework of physician competencies. Med Teach. 2007;29(7):642–7.
Kulike K, Hilgers J, Störmann S, Hornung T, Dudziak J, Weinmann P, Johannink J: Kerncurriculum für die medizinische Ausbildung in Deutschland - Ein Vorschlag der Medizinstudierenden DeutschlandsBVMD. 2006;23:2006.
Arora S, Sevdalis N, Suliman I, Athanasiou T, Kneebone R, Darzi A. What makes a competent surgeon?: experts’ and trainees’ perceptions of the roles of a surgeon. Am J Surg. 2009;198(5):726–32.
Frank JR, Langer B. Collaboration, communication, management, and advocacy: teaching surgeons new skills through the CanMEDS Project. World J Surg. 2003;27(8):972–8; discussion 978.
White R. Patients’ views of the ward round: a survey. Psychiatr Bull. 2005;29:207–9.
Fischer MR, Wölfel T, Schmidmaier R. Interface ward round. Dtsch Med Wochenschr. 2016;141(1):28–31.
Organization WH. Framework for action on interprofessional education and collaborative practice. In. Geneva: World Health Organization; 2010. WHO REFERENCE NUMBER: WHO/HRH/HPN/10.3. https://www.who.int/publications/i/item/framework-for-action-on-interprofessional-education-collaborative-practice.
Reeves S, Rice K, Conn LG, Miller KL, Kenaszchuk C, Zwarenstein M. Interprofessional interaction, negotiation and non-negotiation on general internal medicine wards. J Interprof Care. 2009;23(6):633–45.
Adams RJ. Tele-attending can emulate and even improve bedside teaching and learning. Med Teach. 2018;40(10):1067–8.
Pucher PH, Aggarwal R, Qurashi M, Singh P, Darzi A. Randomized clinical trial of the impact of surgical ward-care checklists on postoperative care in a simulated environment. BJS (British Journal of Surgery). 2014;101(13):1666–73.
Pronovost P, Berenholtz S, Dorman T, Lipsett PA, Simmonds T, Haraden C. Improving communication in the ICU using daily goals. J Crit Care. 2003;18(2):71–5.
Ainsworth CR, Pamplin JC, Allen DA, Linfoot JA, Chung KK. A bedside communication tool did not improve the alignment of a multidisciplinary team’s goals for intensive care unit patients. J Crit Care. 2013;28(1):112.e117-112.e113.
Kadmon M, Ganschow P, Gillen S, Hofmann HS, Braune N, Johannink J, Kuhn P, Buhr HJ, Berberat PO. The competent surgeon : Bridging the gap between undergraduate final year and postgraduate surgery training. Chirurg. 2013;84(10):859–68.
Herrmann-Werner A, Nikendei C, Keifenheim K, Bosse HM, Lund F, Wagner R, Celebi N, Zipfel S, Weyrich P. “Best practice” skills lab training vs. a “see one, do one” approach in undergraduate medical education: an RCT on students’ long-term ability to perform procedural clinical skills. PLoS One. 2013;8(9):e76354.
Shields HM, Honan JP, Goldsmith JD, Madan R, Pelletier SR, Roy CL, Wu LC. Is asking questions on rounds a teachable skill? A randomized controlled trial to increase attendings’ asking questions. Adv Med Educ Pract. 2020;11:921–9.
Han JL, Pappas TN. A review of empathy, its importance, and its teaching in surgical training. J Surg Educ. 2018;75(1):88–94.
Ravindra P, Fitzgerald JE. Defining surgical role models and their influence on career choice. World J Surg. 2011;35(4):704–9.
Steinhausen S, Ommen O, Antoine SL, Koehler T, Pfaff H, Neugebauer E. Short- and long-term subjective medical treatment outcome of trauma surgery patients: the importance of physician empathy. Patient Prefer Adherence. 2014;8:1239–53.
Wilcha RJ. Effectiveness of virtual medical teaching during the COVID-19 crisis: systematic review. JMIR Med Educ. 2020;6(2):e20963.
Scott KM, Baur L, Barrett J. Evidence-based principles for using technology-enhanced learning in the continuing professional development of health professionals. J Contin Educ Health Prof. 2017;37(1):61–6.
Martin G, Koizia L, Kooner A, Cafferkey J, Ross C, Purkayastha S, Sivananthan A, Tanna A, Pratt P, Kinross J. Use of the HoloLens2 mixed reality headset for protecting health care workers during the COVID-19 pandemic: prospective, observational evaluation. J Med Internet Res. 2020;22(8):e21486.
Kidess M, Schmid SC, Pollak S, Gschwend JE, Berberat PO, Autenrieth ME. Virtual skills-training in urology: teaching at the Technical University of Munich during the COVID-19-pandemic. Urologe A. 2021;60(4):484–90.
Carroll K, Iedema R, Kerridge R. Reshaping ICU ward round practices using video-reflexive ethnography. Qual Health Res. 2008;18(3):380–90.
Acknowledgements
We highly appreciate the engagement of all surgical and liaison psychiatry physicians as well as ward nurses of the University Hospital Tübingen, who were passionately providing the teaching. We would also like to thank all patients willingly participating and Thomas Grabe for providing setup and technical support. We acknowledge support by Open Access Publishing Fund of University of Tübingen.
Funding
Open Access funding enabled and organized by Projekt DEAL. We acknowledge support by Open Access Publishing Fund of University of Tübingen.
Author information
Authors and Affiliations
Contributions
JJ and SA were responsible for the design and conduction the study, as well as acquisition, analysis and interpretation of data. JJ drafted the first version of the manuscript. TFW and AHW were involved in data analyses and interpretation. AK and SZ made substantial contributions to the study design. All authors revised the manuscript critically. All authors approved the final version of the manuscript and agreed to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Ethics Committee of the University Clinic of Tübingen, Project Nr. 272/2021BO2. It was conducted in accordance to the relevant guidelines and regulations and in accordance to the Declaration of Helsinki. Participation was voluntary, and all participants gave their informed written consent. All patients involved were thoroughly informed beforehand and gave their written consent. Patients below the age of 18 or with a limited understanding of German were excluded from participation in the study.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Johannink, J., Axt, S., Königsrainer, A. et al. Evaluation of the feasibility of a video-transmitted surgical ward round: a proof of concept study. BMC Med Educ 23, 685 (2023). https://doi.org/10.1186/s12909-023-04656-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12909-023-04656-9