
Abstract
Background
Early- and mid-career academics in medicine, dentistry and health sciences are integral to research, education and advancement of clinical professions, yet experience significant illbeing, high attrition and limited advancement opportunities.
Objectives
Identify and synthesise published research investigating challenges and opportunities related to diversity and inclusion, as experienced by early and mid-career academics employed in medicine, dentistry and health sciences disciplines.
Design
Rapid review.
Data sources
OVID Medline, Embase, APA PsycInfo, CINAHL and Scopus.
Methods
We systematically searched for peer reviewed published articles within the last five years, investigating challenges and opportunities related to diversity and inclusion, as experienced by early and mid-career academics employed in medicine, dentistry and health sciences. We screened and appraised articles, then extracted and synthesised data.
Results
Database searches identified 1162 articles, 11 met inclusion criteria. Studies varied in quality, primarily reporting concepts encompassed by professional identity. There were limited findings relating to social identity, with sexual orientation and disability being a particularly notable absence, and few findings relating to inclusion. Job insecurity, limited opportunities for advancement or professional development, and a sense of being undervalued in the workplace were evident for these academics.
Conclusions
Our review identified overlap between academic models of wellbeing and key opportunities to foster inclusion. Challenges to professional identity such as job insecurity can contribute to development of illbeing. Future interventions to improve wellbeing in academia for early- and mid-career academics in these fields should consider addressing their social and professional identity, and foster their inclusion within the academic community.
Registration
Open Science Framework (https://doi.org/10.17605/OSF.IO/SA4HX).
Similar content being viewed by others

Key messages
-
1. Of the 11 included studies of early- and mid-career academics, most reported concepts encompassed by professional identity, few of the findings related to the topic of inclusion or social identity, with sexual orientation and disability being a particularly notable absence.
-
2. Job insecurity, limited opportunities for professional development, and a sense of being undervalued in the workplace were evident for these academics.
-
3. Systems-level targeted action is needed to strengthen inclusion, diversity and support opportunities for advancement among early and mid-career academics.
Background
The early- and mid-career academic (EMCA) workforce has experienced unprecedented challenges during the COVID-19 pandemic [1, 2], compounding pre-existing psychological illbeing associated with job insecurity [3], high workload [3, 4], and diversity of experience, discrimination, and sexism [2, 5]. Recruiting, maintaining, sustaining, and retaining these essential professionals is dependent on a range of factors including excellent leadership, management, workplace culture, support, promotion, and work-life balance [4, 6,7,8,9,10,11,12,13,14,15,16,17].
Work wellbeing is increasingly forefront in local [2], national [18] and international [19] recommendations for promoting mental health. Interventions to reduce illbeing (e.g., stress, anxiety, depressed mood, burnout) and promote flourishing and thriving in workplaces, including academia, have seen exponential growth [18, 20,21,22]. The experience of establishing a career in academia following completion of a Doctor of Philosophy degree is characterised by significant challenges such as limited support to navigate career progression, a problematic/dysfunctional workplace culture and unsustainable workloads affecting a sense of belonging and inclusion, and experiences of unacceptable workplace behaviours such as discrimination or bullying [2, 3, 23].
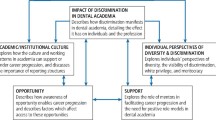
The Inclusion@Work Index [24] defines diversity as all the ways people differ in terms of their social and professional identities. When we consider this in the context of the workplace, diversity refers to the different social and professional identities of people in an organisation, such as, ethnicity, culture, age, gender, education and profession. Inclusion in the workplace is when this diverse mix of people are “respected, connected, progressing and contributing” [24] (p.7) to the success of an organisation; an individual’s identity will influence their views and experiences of inclusion.
In addition to the known pressures facing the EMCA workforce, recent research has identified a disproportionate impact of the COVID-19 pandemic upon early and mid-career researchers. Some identified impacts were relevant to diversity and inclusion issues, such as the greater impacts noted for females with caring responsibilities, or those working with reduced hours, and the noted loss of career prospects due to disrupted track records [2, 25, 26].
There is a large body of literature focusing on widening participation and mitigating diversity and inclusion challenges faced by postgraduate students at universities [27, 28]. Less is known about the experiences of academic staff in the same space [29]. Previous survey research that included clinician researchers indicates they may experience unique support needs compared to other STEM academics [30]. Findings from reviews and commentaries focused on science, technology, engineering and mathematics (STEM) disciplines [31,32,33] or academia generally [3, 29] may not have the same relevance to medicine, dentistry and health sciences fields.
The aim of this review was to identify and explore experiences and perceptions of diversity and inclusion, as experienced by early and mid-career academics employed in medicine, dentistry and health science disciplines. Synthesising primary research on these topics will inform future strategies and research to address challenges, capitalise on opportunities, and highlight successful initiatives.
There were three review questions (RQ), focused on the topic of experiences and perceptions of diversity and inclusion in early and mid-career academics employed in medicine, dentistry and health sciences: RQ1) what are the characteristics of studies about this topic? RQ2) what instruments have been used to investigate this topic? and RQ3) what are the reported experiences and perceptions in the included studies?
Methods
This rapid review [34] followed an a priori review protocol. The review protocol was not eligible for registration on the PROSPERO platform due to the focus on experiences of academics, and therefore was registered in the Open Science Framework (https://doi.org/10.17605/OSF.IO/SA4HX) on 20th July 2022. Registration occurred after searches and data extraction but before analysis. Reporting followed the updated guideline for reporting systematic reviews [35].
Search strategy
Information sources
To identify potentially relevant studies, the following electronic databases were searched on 9th November 2021: OVID Medline/Embase, APA PsycInfo, CINAHL and Scopus. Rapid review methodology guidance [36] suggests limiting to a single database – CINAHL was included due to our population including allied health academics, while APA PsycInfo and Scopus were included to ensure social sciences literature was considered, as publications relating to diversity and inclusion in the chosen context may be submitted to these journals rather than medical journals.
Search terms
The search strategy (reported in full in Supplementary File 1) was developed from the research questions and based on population, concepts, and context. A research librarian reviewed and advised on the final implemented search strategy.
Inclusion and exclusion criteria
Only primary research papers reported in English from January 2017 to September 2021 were included. Constraining searches to recent literature, e.g. last 5 years, is a strategy deployed in rapid reviews with constrained time frames [37], as in the case of this project, to manage scope and feasibility. A review of reviews was not possible for this topic as we were unable to identify any published systematic reviews focusing on, or presenting separate data, for this subgroup.
Population
Early and mid-career post-doctoral academics in medicine, dentistry and health sciences (e.g., biomedical science, nursing, optometry, physiotherapy, social work, audiology) were included. The definition of early and mid-career academic varies between universities, funders and countries. For example, the EURAXESS definition of an early-stage researcher encapsulates the PhD study period [38], whereas other funding bodies exclude the PhD period and focus on the years post-award [17, 39]. For teaching specialists and mid-career researchers, this becomes even less delineated [21, 40]. A previous Australian study demonstrated the importance of permitting self-definition of career stage, to bridge the gap between current university definitions and the increasingly diverse experiences of early career academics [41]. For this reason, we included any article that reported early or mid-career academics as participants, and we extracted and reported any definitions provided by article authors. Science, technology, engineering, and doctoral students were excluded due to the wide body of previous work focusing on graduate students and the difference in challenges experienced by this cohort.
Concepts
Articles reporting experiences, perceptions, themes of diversity and inclusion in early and mid-career academics employed in medicine, dentistry and health sciences. Diversity in the context of early and mid-career academic social and professional identity were included. Diversity was defined as: “…all the differences between people in how they identify in relation to social identity, that is their Aboriginal and/or Torres Strait Islander background, age, caring responsibilities, cultural background, disability, gender, faith/no religion, LGBTIQ + status, and social class, and their professional identity, that is their profession, education, work experiences, and organisational role.” [24]. Inclusion was defined as occurring when “…a diversity of people are respected, connected, progressing and contributing to organisational success.” [24].
Context
Articles focused on tertiary education setting including medicine, dentistry, health, and biomedical sciences were included.
Screening
The Cochrane Rapid Reviews Methods Group recommends dual screening at least 20% of abstracts with a single reviewer for the remainder after conflicts are resolved [36]. However, due to resourcing constraints it was not possible to have a single reviewer, therefore dual screening and extraction was applied to all abstracts to ensure consistency. Title and abstract screening was conducted by 7 reviewers, full text review by 3 reviewers, and data extraction by 3 reviewers. Conflicts arising during screening and full text review were resolved by consensus from members of the research team involved at each phase.
Assessment of methodological quality
The assessment of methodological quality was conducted by a single reviewer (MP) using a range of established quality assessment tools as appropriate to the study design, such as those from the Critical Appraisal Skills Programme (CASP) and the National Institute of Health. Quality ratings, where tools indicated them, and supporting statements for the choice of rating were reviewed by a second reviewer (RJ). The assessment was limited to the study methodology and outcomes relating specifically to diversity and inclusion topics. Regardless of any ratings of methodological quality, all studies proceeded to data extraction and findings from this quality assessment are reported separately from the synthesis of findings. This approach was adopted due to the variety of study designs included in the review.
Data extraction, analysis and reporting
Data extraction was limited to study characteristics (RQ1), outcome measures (RQ2), and findings (RQ3) specifically related to diversity and inclusion topics. The data extraction form was developed in Covidence by two reviewers and piloted on three papers to refine before full double extraction was undertaken. The Covidence platform highlighted conflicts in extraction which were resolved by consensus from members of the research team involved in this phase. The extracted data were tabulated, synthesised, and reported narratively to address each of the review questions.
Results
Study identification, screening and selection
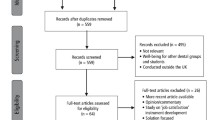
Database searches were executed in September 2021, identifying 1162 articles; 11 met inclusion criteria, were quality appraised, and progressed to data extraction and analysis. A flowchart of study identification, screening and selection is illustrated in Fig. 1.

Study identification, screening and selection flowchart
Characteristics of included studies (RQ1 & RQ2)
Characteristics of included studies are reported in Table 1.
Of the included studies, five were published before 2020, and four published in the last year (2021). Study designs were primarily qualitative (n = 7), using interview or survey methods to explore experiences. Two studies used mixed methods (quantitative survey with qualitative interviews/focus groups [49, 52]). Three studies used a survey methodology to measure purely quantitative outcomes for statistical analysis [44, 45, 48]. Three studies looked at outcomes over time, with the remainder cross-sectional in design. Studies were predominantly USA-based (n = 8) with the remainder conducted in Europe.
Definitions of early and/or mid-career academics ranged from describing time since completing PhD to specific academic ranks (and titles) of participant. Participant career stage varied across studies, with only two studies reporting range of years post-PhD for participants [51, 52], totalling 1–8 years. Three studies had majority assistant, associate or early professors as participants and could be considered to have a focus on mid-career researchers. Criteria to define an early or mid-career researcher were not reported for 5 studies, while two studies defined postdoctoral status by participation in USA-specific “T32 FIRST (Fellowships In Research and Science Teaching)” programme, a nationwide programme of funded, institution-based postdoctoral research training. One study allowed participation by self-identification of postdoctoral status [42].
Assessment of methodological quality
The methodological quality of included studies is tabulated in Supplementary File 2. Three studies were exploratory [45, 49, 52], assessing the impact of an established program. These studies did not report a research question or pre-determine a sample size and opted for mainly descriptive reporting. Most studies utilised participants within a single institution or were small sample, limiting transferability of findings to other program and institutions. Methods reporting was usually comprehensive. Only a limited proportion of the qualitative studies considered reflexivity. Some programs for early and mid-career academics were only accessible through a competitive selection process, therefore some biases cannot be ruled out when considering findings, such as candidates self-selecting based upon the criteria, and unconscious bias on part of those making the selection, potentially reinforcing traditional and conservative measures of performance. Many identified studies were US-based and may not necessarily generalise to other tertiary education systems in other countries.
Experiences and perceptions (RQ3)
Findings related to diversity and inclusion were primarily focused on professional identity, and to a lesser extent, social identity. Main findings are reported in Table 2.
With regard to social identity, only one study reported whether there were any transgender participants [51], and proportion speaking English as a second language [44]. Five studies reported ethnicity [42, 44, 49, 51], or race [46], while all but except Deane and Clunie [47] reported gender, with Chaudron et al.’s study [45] featuring all women participants. Five studies reported age [43, 44, 50,51,52]. Only two studies [51, 52] reported demographic information relating to marital status and dependents (i.e., children). None of the studies reported on living with disability or long-term health conditions.
Aspects of social identity were reported in five studies [42, 44, 49,50,51] including the topics of gender, family life, balance and children, ambition and success, and self-efficacy. Two studies reported differences in communication styles for males; finding males more vocal of career intentions [50] and more likely to perceive themselves as having high self-efficacy in informal speaking [44]. Academia impacted on having a family [51], as well as the amount of time spent with family [42]. All 11 studies reported findings related to professional identity. The main professional identity foci were relationships and connection, feeling valued and supported, and balancing clinical and research commitments.
Five studies reported interventions, comprising professional development [45, 49, 52], mentoring [43, 49, 52], or peer support/networking [45, 47]. Impact of these interventions was primarily reported positively, such as perceptions of enhanced development of professional identity and leadership skills, achieving set goals [45]. The USA-specific “T32 FIRST” postdoctoral research training program content was more tailored towards individuals, for example mentoring and having opportunities to work in an established laboratory [43, 49], although reported details of leadership education were limited. Those receiving mentoring found mentoring impactful upon their leadership skills, knowledge and competency [43, 44, 52]. Not all focused on these as specific outcome measures, for example, van Dongen et al. [52] considered research productivity as a measurable outcome. This was also the only intervention study to measure outcomes in a longitudinal manner.
From an inclusion perspective, findings from four studies [42, 47, 49, 50] emphasised value of feeling part of a community, for example as part of an intervention cohort, or peer support, or good line management, good connections, and networks. Online community supported this in lieu of an actual physical community [47]. Most findings related to inclusion explored experiences and perceptions [42, 43, 46,47,48, 50,51,52]. Studies reported challenges of heavy workloads [42, 46, 50], maintaining work-life balance [42, 46, 50, 51], imposter syndrome, and a lack of feeling supported and valued [42, 47, 48, 50], such as work not being appreciated by others [42]. A study by Duke et al. [48] exploring burnout in more depth, found the odds of experiencing burnout decreased if it was felt one’s contributions to a department were valued, and yet only half of participants felt their contributions were valued [48]. The authors did not speculate on reasons for this, instead highlighting steps taken at their institution to address these issues, such as creating opportunities to highlight faculty accomplishments, although the impact of these changes was not reported.
The lack of career support was particularly evident in the research and clinical environment for healthcare professionals [47] with challenges between wanting to progress but balancing roles as a clinician and a researcher [47, 50]. The complexity of heavy workloads in combination with high academic achievement [50] was also expressed as a warning to academics [42], suggesting work–life balance as essential. This striving for high academic achievement was also reported by Behar-Horenstein and Prikhidko [43], where the competition culture was felt to strain peer relationships. Opportunities for team science and multiple mentors were found to be beneficial [43], alongside relationships and connections in the form of networks [42, 49]. The included studies rarely had a direct focus on diversity and inclusion concepts, and subsequently did not go beyond reporting findings to interpret them and develop new concepts or theories. One exception was a study which examined mentoring experiences through the lens of team science [43], to understand the mechanisms by which mentoring may be beneficial.
In summary, the included studies largely focused on reporting a variety of experiences and perceptions relating to academic careers or participating in interventions to develop careers, a number of which related to diversity (social and professional identity) and inclusion.
Discussion
Our rapid review aimed to synthesise the experiences and perceptions of diversity and inclusion by early and mid-career academics employed in medicine, dentistry and health sciences, as reported in the primary research literature. We have reported these experiences and perceptions as a narrative synthesis, alongside the characteristics of these studies, including the methods by which these studies have explored this topic.
There were limited findings in the reviewed studies relating to social identity, with disability and LGBTQIA + being particularly notable absences. Included studies primarily focused on ethnicity, race, and gender. LGBTQIA + status was rarely reported in these studies, and we found no studies where exploring this was a specific aim. One paper incidentally reported transgender status alongside male and female genders [51]. By contrast, there are studies that have explored LGBTQIA + discrimination in STEM more generally, or from the student experience perspective [53, 54], with similar papers existing for students with disabilities [55,56,57]. None of the included studies focused on disability. It appears there is limited focus on certain aspects of social identity in both the EMCA space and overall fields of medicine, dentistry and health sciences.
Included studies frequently addressed concepts encompassed by professional identity, often echoing those in papers about other areas of academia [6, 7, 30], but very few of the findings relate to the topic of inclusion. These studies used data collected before COVID-19 introduced novel challenges to academia, such as physical distancing, altered education pathways and moving of programmes online. Surveys of EMCAs during the pandemic highlight the challenges of creating a sense of belonging and inclusion under such circumstances, e.g. feeling connected to colleagues, as well as opportunities to network and be involved in the workplace culture [2, 25, 26]. In clinical academia, COVID-19 also compounded challenges related to professional identity, such as high workloads, and work-life imbalance, and added to psychological illbeing, such as high stress and anxiety [20, 45, 51]. These impacts are also further accentuated by the social identity of EMCAs, such as feeling unable to start a family due to lack of job security or low pay, feeling unable to meet current family obligations, or having other caring responsibilities necessitating, for example, part-time working [2, 25, 26, 42, 51]. Overall, there are a number of work-based contributors to poor mental health for EMCAs that are inextricably linked to diversity and inclusion concepts.
Work plays an important role in mental health, and is forefront in the World Health Organization’s definition of mental health as “a state of wellbeing in which the individual realises his or her own abilities, can cope with the normal stresses of life, can work productively and fruitfully, and is able to make a contribution to his or her community” [58]. When considering findings related to inclusion, there are several similarities with models of workplace wellbeing developed through academic research [59] which typically include positive relationships and emotions, life purpose/meaning, personal growth, autonomy, engagement and self-acceptance. These components resonate with findings from studies in our review that demonstrate the value of mentoring relationships, a sense of community, and networking opportunities or interventions supporting the meeting of personal goals, or development of leadership skills. What is not evident in academic conceptualisations of workplace wellbeing [59], yet is evident in our review, was the importance of academics feeling supported, respected, and valued. It can therefore be argued that interventions to improve diversity and inclusion experiences of early and mid-career academics in the higher education space, with a particular focus on the less explored areas medicine, dentistry and health sciences, would be highly relevant to improve work wellbeing, and subsequently mental health.
With regard to interventions, we found a limited number for early and mid-career academics in medicine, dentistry and health sciences fields that reported an accompanying evaluation – papers that described programs but did not report outcomes were excluded. Intervention studies had varied aims and objectives but often sought to establish a cohort or community [43, 49], and thus a sense of belonging and inclusion. However, experiences and perceptions relating to diversity and inclusion were a ‘by-product’ of the research process, and the programmes described did not appear to have fostering inclusion as a primary aim, despite many reporting social identity characteristics. There was also no theoretical framework described for the foundations of these interventions, although one study retrospectively explored the “T32 FIRST” postdoctoral research training programme in the context of the team science framework [43]. Many interventions were limited in their description within the reviewed papers, for example the components of leadership programmes were not described in depth.
A future opportunity is to consider a systematic approach to the development, implementation and evaluation of programs to actively promote wellbeing of academics and enhance inclusivity. Interventions to enhance wellbeing could be informed by recognised academic models of wellbeing, such as the “Five Ways to Wellbeing” [60, 61], which includes: ‘Connect’, ‘Be active’, ‘Take notice’, ‘Keep learning’, and ‘Give’. Use of a systematic reporting template, appropriate to the intervention, may strengthen reporting of these interventions, in turn supporting their future reliable implementation and replication. One such example is the Template for Intervention Description and Replication (TIDieR [62]). Unifying definitions of diversity and inclusion, determining the best evidence to inform the development of these interventions, and accurately measuring the effectiveness of interventions are all crucial next steps.
A key point of interest in these intervention studies was the variety of definitions (or lack thereof) of early and mid-career researcher used to determine access to these interventions. In some countries membership of post-doctoral associations is simply by self-definition of being an EMCA. It is important to consider, from an inclusion perspective, whether the lack of consistent definition of what constitutes an early or mid-career researcher may in fact be a barrier to some individuals putting themselves forward for these programmes [40]. Further, unifying definitions globally would help to determine the transferability of some of these interventions to other locations.
Based on our review findings, including lack of clarity in definitions of EMCAs and limitations of the available evidence, we recommend strengthening the evidence base to inform future interventions and diversity and inclusion experiences of EMCAs through the development of:
-
1)
Global unified definitions of early career academic and mid-career academics.
-
2)
A planned, global approach to exploration and description of diversity and inclusion research for early- and mid-career academics.
-
3)
A planned, global approach to development and evaluation of interventions to improve diversity and inclusion experiences of early- and mid-career academics.
Limitations
Resourcing constraints necessitated some deviations from the Cochrane recommendations for rapid reviews, such as the use of multiple reviewers across different screening phases and data extraction. The impact of this was mitigated by applying dual screening, resolution of screening conflicts with the research team and double extraction of the included articles. The variation in definitions of early and mid-career academic across studies has been explicitly described in the tables but applying the findings of such studies to other countries with different definitions is more difficult. Similarly, there may be differences between countries in the way some groups of academics captured within our target population are treated, such as differing pay rates for clinical academics versus clinical practitioners [63], or clinical versus non-clinical academics. These differences could affect experiences and perceptions of certain topics such as job security and financial stability to support family.
The search terms and chosen databases are likely to bias towards research conducted in English-speaking countries, and will not capture, for example, project reports on websites for higher education organisations. While we endeavoured to capture a variety of search terms that describe early to mid-career academics, it’s possible that some articles may have been missed if the cohort was described in a way that did not refer directly to this career stage in the title or abstract. We have clearly reported the constrained timeframe of searches to the last 5 years of published primary research so the scope of our review is clear, thus older literature is not represented. Lastly, although data screening and extraction were performed in groups, we cannot rule out our respective social and professional identities impacting upon the narrative interpretation of the literature (see authors’ information).
Conclusions
Our review has identified that academic models of wellbeing overlap with key facilitators of inclusion, and key aspects of professional identity such as job insecurity can contribute to the development of illbeing. As such, wellbeing, illbeing, diversity and inclusion are linked. Therefore, to improve wellbeing in academia for early- and mid-career academics, future interventions, particularly in the relatively under-researched fields of medicine, dentistry and health sciences, should consider addressing their social and professional identity, and how they are included within the academic community. There is an opportunity to strengthen primary research on academic wellbeing through the inclusion of groups with certain social identities not currently represented within this research area, such as people who identify as LGBTQIA + and people with disabilities, who are absent from recent literature.
Availability of data and materials
All data generated or analysed during this study are included in this published article and supplementary information file. An example search string using the CINAHL database is archived at searchrxiv: https://doi.org/10.1079/searchRxiv.2022.00083.
References
Fisher JR, Tran TD, Hammarberg K, Sastry J, Nguyen H, Rowe H, et al. Mental health of people in Australia in the first month of COVID-19 restrictions: a national survey. Med J Aust. 2020;213(10):458–64.
Singh A, Marck C, Ayton D, Koay H, Wiley JF, Steward T. Early- and Mid-Career Researchers: A Workplace Culture, Career Development, and Mental Wellbeing Survey. Melbourne: University of Melbourne; Monash University; 2020.
Nicholls H, Nicholls M, Tekin S, Lamb D, Billings J. The impact of working in academia on researchers’ mental health and well-being: A systematic review and qualitative meta-synthesis. PLoS ONE. 2022;17(5):e0268890.
Hollywood A, McCarthy D, Spencely C, Winstone N. ‘Overwhelmed at first’: the experience of career development in early career academics. J Furth High Educ. 2019;44(7):998–1012.
Bourabain D. Everyday sexism and racism in the ivory tower: The experiences of early career researchers on the intersection of gender and ethnicity in the academic workplace. Gend Work Organ. 2021;28(1):248–67.
Dorenkamp I, Weiß E-E. What makes them leave? A path model of postdocs’ intentions to leave academia. High Educ. 2017;75(5):747–67.
Eleftheriades R, Fiala C, Pasic MD. The challenges and mental health issues of academic trainees. F1000Res. 2020;9:104.
Ghaffarzadegan N, Xu R, Larson RC, Hawley JD. Symptoms versus Root Causes: A Needed Structural Shift in Academia to Help Early Careers. Bioscience. 2018;68(10):744–5.
Guthrie S, Lichten C, van Belle J, Ball S, Knack A, Hofman J. Understanding mental health in the research environment: A Rapid Evidence Assessment. RAND Corporation; 2017.
Hardy MC, Carter A, Bowden N. What do postdocs need to succeed? A survey of current standing and future directions for Australian researchers. Palgrave Commun. 2016;2(1):1–9.
Lambert WM, Wells MT, Cipriano MF, Sneva JN, Morris JA, Golightly LM. Career choices of underrepresented and female postdocs in the biomedical sciences. Elife. 2020;9:e48774.
Lashuel HA. What about faculty? Elife. 2020;9:e54551.
Signoret C, Ng E, Da Silva S, Tack A, Voss U, Lidö HH, et al. Well-Being of Early-Career Researchers: Insights from a Swedish Survey. High Educ Pol. 2018;32(2):273–96.
Sohn E. How to handle the dark days of depression. Nature. 2018;557(7704):267–9.
Van Benthem K, NadimAdi M, Corkery CT, Inoue J, Jadavji NM. The changing postdoc and key predictors of satisfaction with professional training. Stud Grad Postdr Educ. 2020;11(1):123–42.
Ysseldyk R, Greenaway KH, Hassinger E, Zutrauen S, Lintz J, Bhatia MP, et al. A Leak in the Academic Pipeline: Identity and Health Among Postdoctoral Women. Front Psychol. 2019;10:1297.
EMCR Forum of the Australian Academy of Science, Australian Brain Alliance EMCR Network. Submission to the Productivity Commission’s inquiry into the effect of mental health. Canberra: Australian Academy of Science; 2020.
The Future of Work Institute. Thrive at Work Perth: The Future of Work Institute. 2021.
World Health Organisation. Guidelines on mental health at work. Geneva: World Health Organisation; 2022.
Gottlieb G, Smith S, Cole J, Clarke A. Research culture and environment toolkit. 2021. 2022.
Casci T, Adams E. Setting the right tone. Elife. 2020;9:e55543.
Jarden RJ, Jarden A. A systems pathway to self-care in academia: Me, We, and Us as avenues to integrated long-term self-care. Reflections on Valuing Wellbeing in Higher Education: Routledge; 2022. p. 95–110.
Moran H, Karlin L, Lauchlan E, Rappaport SJ, Bleasdale B, Wild L, et al. Understanding Research Culture: What researchers think about the culture they work in. Wellcome Open Res. 2020;5:201.
O’Leary J, D’Almada-Remedios R. DCA Inclusion@Work Index 2021–2022: Mapping the State of Inclusion in the Australian Workforce. Sydney: Diversity Council Australia; 2021.
EMCR Forum of the Australian Academy of Science. Impacts of COVID-19 for EMCRs: National Survey Report. Canberra: Australian Academy of Science; 2020.
Morin A, Helling BA, Krishnan S, Risner LE, Walker ND, Schwartz NB. Surveying the experience of postdocs in the United States before and during the COVID-19 pandemic. Elife. 2022;11:e75705.
Gale T, Parker S. Widening participation in australian higher education: Report submitted to HEFCE and OFFA. 2013.
Grant-Smith D, Irmer B, Mayes R. Equity in Postgraduate Education in Australia: Widening participation or widening the gap? National Centre for Student Equity in Higher Education (NCSEHE) Accessed at https://www.ncsehe.edu.au/publications/widening-participation-or-widening-the-gap-equity-in-postgraduate-study. 2020.
Urbina-Garcia A. What do we know about university academics’ mental health? A systematic literature review. Stress Health. 2020;36(5):563–85.
Christian K, Johnstone C, Larkins J-A, Wright W, Doran MR. A survey of early-career researchers in Australia. Elife. 2021;10:e60613.
Casad BJ, Franks JE, Garasky CE, Kittleman MM, Roesler AC, Hall DY, et al. Gender inequality in academia: Problems and solutions for women faculty in STEM. J Neurosci Res. 2021;99(1):13–23.
Weissmann GS, Ibarra RA, Howland-Davis M, Lammey MV. The multicontext path to redefining how we access and think about diversity, equity, and inclusion in STEM. J Geosci Educ. 2019;67(4):320–9.
Cardel MI, Dhurandhar E, Yarar-Fisher C, Foster M, Hidalgo B, McClure LA, et al. Turning Chutes into Ladders for Women Faculty: A Review and Roadmap for Equity in Academia. J Womens Health (Larchmt). 2020;29(5):721–33.
Khangura S, Konnyu K, Cushman R, Grimshaw J, Moher D. Evidence summaries: the evolution of a rapid review approach. Syst Rev. 2012;1:10.
Page MJ, McKenzie J, Bossuyt P, Boutron I, Hoffmann T, mulrow c, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Center for Open Science; 2020.
Garritty C, Gartlehner G, Nussbaumer-Streit B, King VJ, Hamel C, Kamel C, et al. Cochrane Rapid Reviews Methods Group offers evidence-informed guidance to conduct rapid reviews. J Clin Epidemiol. 2021;130:13–22.
Haby MM, Chapman E, Clark R, Barreto J, Reveiz L, Lavis JN. What are the best methodologies for rapid reviews of the research evidence for evidence-informed decision making in health policy and practice: a rapid review. Health Res Policy Syst. 2016;14(1):83.
EURAXESS. Research profiles descriptors Geneva: EURAXESS; 2022 Available from: https://euraxess.ec.europa.eu/europe/career-development/training-researchers/research-profiles-descriptors.
UK Research and Innovation. Early career researchers: career and skills development London: Arts and Humanities Research Council. 2022.
Gould J. Muddle of the middle: why mid-career scientists feel neglected [Internet]. London: Nature; 2022 21st September 2022. Podcast.
Bosanquet A, Mailey A, Matthews KE, Lodge JM. Redefining ‘early career’ in academia: a collective narrative approach. High Educ Res Dev. 2017;36(5):890–902.
Afonja S, Salmon DG, Quailey SI, Lambert WM. Postdocs’ advice on pursuing a research career in academia: A qualitative analysis of free-text survey responses. PLoS ONE. 2021;16(5):e0250662.
Behar-Horenstein LS, Prikhidko A. Exploring mentoring in the context of team science. Mentor Tutoring. 2017;25(4):430–54.
Cameron C, Lee HY, Anderson CB, Trachtenberg J, Chang S. The role of scientific communication in predicting science identity and research career intention. PLoS ONE. 2020;15(2):e0228197.
Chaudron LH, Anson E, Bryson Tolbert JM, Inoue S, Cerulli C. Meeting the Needs of Mid-Career Women in Academic Medicine: One Model Career Development Program. J Women’s Health. 2021;30(1):45–51.
Cumbler E, Rendón P, Yirdaw E, Kneeland P, Pierce R, Jones CD, et al. Keys to career success: resources and barriers identified by early career academic hospitalists. , <Blank>: Springer Nature; 2018. p. 588–9.
Deane JA, Clunie G. Healthcare professionals in research (HPiR) Facebook community: a survey of U.K. doctoral and postdoctoral healthcare professionals outside of medicine. BMC Med Educ. 2021;21(1):236.
Duke NN, Gross A, Moran A, Hodsdon J, Demirel N, Osterholm E, et al. Institutional Factors Associated With Burnout Among Assistant Professors. Teach Learn Med. 2020;32(1):61–70.
Eisen A, Eaton DC. A Model for Postdoctoral Education That Promotes Minority and Majority Success in the Biomedical Sciences. CBE Life Sci Educ. 2017;16(4):ar65.
Lange W, Kars MC, Poslawsky IE, Schuurmans MJ, Hafsteinsdóttir TB. Postdoctoral Nurses’ Experiences With Leadership and Career Development: A Qualitative Study. J Nurs Scholarsh. 2019;51(6):689–98.
Price RM, Kantrowitz-Gordon I, Gordon SE. Competing discourses of scientific identity among postdoctoral scholars in the biomedical sciences. CBE Life Sci Educ. 2018;17(2):ar29.
van Dongen L, Cardiff S, Kluijtmans M, Schoonhoven L, Hamers JPH, Schuurmans MJ, et al. Developing leadership in postdoctoral nurses: A longitudinal mixed-methods study. Nurs Outlook. 2021;69(4):550–64.
Gallardo-Nieto EM, Gómez A, Gairal-Casadó R, del Mar R-S. Sexual orientation, gender identity and gender expression-based violence in Catalan universities: qualitative findings from university students and staff. Arch Public Health. 2021;79(1):16.
Glazzard J, Jindal-Snape D, Stones S. Transitions Into, and Through, Higher Education: The Lived Experiences of Students Who Identify as LGBTQ+. Frontiers in Education. 2020;5.
Kimball EW, Wells RS, Ostiguy BJ, Manly CA, Lauterbach AA. Students with Disabilities in Higher Education: A Review of the Literature and an Agenda for Future Research. In: Paulsen MB, editor. Higher Education: Handbook of Theory and Research. Cham: Springer International Publishing; 2016. p. 91–156.
Miller RA, Downey M. Examining the STEM Climate for Queer Students with Disabilities. JPED. 2020;33(2):169–81.
Cech EA. The intersectional privilege of white able-bodied heterosexual men in STEM. Sci Adv. 2022;8(24):eabo1558.
World Health Organisation. Mental health action plan 2013–2020. Geneva: World Health Organisation; 2013.
Hone L, Schofield G, Jarden A. Conceptualizations of wellbeing: Insights from a prototype analysis on New Zealand workers. NZJHRM. 2015;15(2):97–118.
Aked J, Marks N, Cordon C, Thompson S. Five ways to well-being: The evidence. London: new economics foundation. 2008.
Dewe P, Kompier M. Wellbeing and Work: Future Challenges. PsycEXTRA Dataset: American Psychological Association (APA). 2008.
Hoffmann TC, Glasziou PP, Boutron I, Milne R, Perera R, Moher D, et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ. 2014;348(mar07 3):g1687.
Wise J. Medical academic workforce is under threat without urgent action on pay and pensions, say peers. BMJ. 2023;380:p220.
Acknowledgements
The authorship team are grateful to Jim Berryman, academic librarian, for assistance with developing the initial search terms, and to Associate Professor Kate Hayward for her helpful comments on the manuscript as well as support with literature screening.
Funding
This work was funded by a Diversity and Inclusion grant awarded by the University of Melbourne Faculty of Medicine, Dentistry and Health Sciences.
Author information
Authors and Affiliations
Contributions
All authors were involved in the study design and development of the protocol. MP conducted searches. All authors conducted title and abstract screening. Full text screening by EK, FH and RJ. Data extraction by MP, BL and RJ. Article preparation by MP and RJ. All authors read and approved the final manuscript.
Authors’ information
The research team is comprised of entirely women, early- or mid-career academics in health sciences, representing the following fields: Nursing, orthoptics, optometry, audiology and speech pathology, social work, physiotherapy.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Supplementary file 1.
Full search strategy. Supplementary file 2. Methodological quality of included studies.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Piano, M., Diemer, K., Hall, M. et al. A rapid review of challenges and opportunities related to diversity and inclusion as experienced by early and mid-career academics in the medicine, dentistry and health sciences fields. BMC Med Educ 23, 288 (2023). https://doi.org/10.1186/s12909-023-04252-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12909-023-04252-x