
Abstract
Background:
The use of cognitive-enhancing medications and supplements among healthy adults continues to rise. Limited data exists on their use among resident physicians. Given their highly competitive and stressful lifestyle, we sought to evaluate the prevalence, motivations, and side effects of using cognitive-enhancing supplements and medications among resident physicians at a large United States academic institution.
Methods:
An anonymous web-based survey was circulated to resident physicians inquiring about using cognitive-enhancing supplements and medications, as well as personal characteristics such as gender, marital and parental status, medical diagnoses, and medical specialty. Before circulation, we performed a pilot study. Weighted logistic regression analyses estimated the impact of personal characteristics on the probability of using both supplements and medications.
Results:
Survey response rate was 46.4%. Of respondents, 48.6% were female, 45.9% were married, 70.9% were without children, and 67.2% were in a non-surgical medical specialty. Few respondents had a related medical diagnosis, with attention deficit hyperactivity disorder being the most common (7.1%). Male, non-married, surgical residents were more likely to take supplements (odds ratio (OR) = 1.06, 1.05, and 1.05). Males, without children, and those who felt pressure to perform well, were afraid of being left behind, felt pressure because colleagues take them, or felt they could not reach their current level of training without medications were more likely to take medications (OR = 1.11, 1.04, 1.05, and 1.08). Adverse effects with medications were common.
Conclusion:
Supplement and medication use for cognitive enhancement was high among resident physicians at a single institution despite few having a related medical diagnosis. This study raises awareness of the growing pressure in competitive residency environments to use cognitive enhancement regardless of the potential side effects.
Similar content being viewed by others


Background
Prescription medications to enhance cognitive performance among healthy adults continues to gain popularity [1,2,3]. Cognitive enhancers are taken to improve memory, boost levels of energy and wakefulness, and increase mental alertness and concentration [4]. The mechanisms of action of these medications are often inconclusive, with some working to increase levels of circulating adrenalin to assist with wakefulness or modulate neurotransmitters such as dopamine. The most common medications include stimulants traditionally prescribed for attention deficit hyperactivity disorder (ADHD). Over 6% of healthy individuals use stimulants [5], with even higher rates among college students [6,7,8,9], medical students [10,11,12,13,14], and resident physicians [15]. Although the motivations may vary, common ones include a stressful lifestyle, a competitive environment, balancing the rigors of academic or professional obligations and social expectations, and a fear of being “left behind” by peers [15,16,17].
In addition to prescription medications, there is a growing list of over-the-counter supplements marketed as cognitive enhancers [4]. Collectively, these have been coined under the umbrella term, nootropics, which have gained popularity as international sales continue to climb and are expected to reach USD$5.32 billion by 2026 [18]. However, the use of medications and supplements for cognitive enhancement among resident physicians in the United States has been underexplored. Resident physicians are a unique population with a broad range of stressors that may influence their likelihood of using cognitive-enhancing medications and supplements. Stressors include long work hours, chronic sleep deprivation and fatigue, personal debt incurred from increasing medical education costs, decreasing confidence in the job market, and increasing efforts to master a rapidly expanding knowledge base in the more litigious medical landscape [19]. Furthermore, substance misuse, particularly illicit substance abuse has been associate with increased rates of suicide, an issue of significant concern among medical trainees and practicing physicians [20] . Therefore, we evaluated the prevalence, motivations, and side effects of cognitive-enhancing supplements and medications among resident physicians at a large United States academic institution.
Methods
We distributed an anonymous, cross-sectional, voluntary survey on the use of cognitive-enhancing supplements and medications to all 638 resident physicians at the University of Utah, a large public United States academic institution with over 23,700 employees and over 33,000 students. The institution is in the urban setting of Salt Lake City, Utah. A resident is a physician who has completed their medical degree and is undergoing additional training in a medical specialty of choice as part of a graduate medical education program. We distributed the survey using a web-based platform in January of 2022 via email on three separate occasions to all resident physicians at the University of Utah. There was no survey incentive provided. All respondents expressed written consent by completing the survey and were asked to complete the survey only once. The survey design included a pilot study of randomly selected residents from multiple specialties representing 5% of the study population (n = 30). Pilot study respondents completed the survey within approximately 5 minutes. The response rate of the pilot study was 43.3% (13 of 30 residents). Pilot survey respondents provided anonymous feedback about the survey. We incorporated all suggestions in revisions to the final survey.
Survey sections included demographic information; cognitive enhancing supplement information, including type, duration, frequency of use, side effects, and motivations; cognitive-enhancing medication information, including type, duration, frequency of use, side effects, and motivations. We limited the collection of demographic information to those variables previously shown to be associated with cognitive-enhancing medication use among resident physicians to ensure the anonymity of respondents [15]. Respondents were asked at what stage of their medical training did they start taking specific medications, including Amphetamine, Methylphenidate, and Modafinil, as well as particular supplements, including Noopept and Racetams. These medications and supplements were asked about because of their explicit use as cognitive enhancement. In addition, a follow-up question about the current frequency of use was utilized to determine whether respondents were currently using the medication or supplement or had simply used it in the past (Supplement).
Specific cognitive enhancing supplements measured included Noopept, Racetams (piracetam, pramiracetam, phenylpiracetam or phenotropil, aniracetam), Ashwagandha, Bacopa monnieri, Caffeine, Creatine, Ginkgo biloba, Lion’s Mane Mushroom, L-theanine, magnesium, Omega-3 fatty acids, Panax ginseng, and Rhodiola Rosea. Although many of the supplements, such as Omega-3 fatty acids, can be used for other purposes, respondents were asked explicitly about their use for cognitive enhancement. In addition, the form of caffeine consumption was not inquired about. Cognitive enhancing medications included Amphetamines (such as Adderall, Adzenys, Desoxyn, Dexedrine, Dyanavel, Evekeo, Mydayis, ProCentra, Vyvanse, or Zenzedi), Methylphenidates (such as Adhansia, Azstarys, Aptensio, Concerta, Contempla, Daytrana, Focalin, Journal, Metadate, Methylin, QuilliChew, Quillivant, or Ritalin), Modafinil (Provigil), Cholinesterase inhibitors [such as Donepezil (Aricept), Rivastigmine (Exelon), or Galantamine (Razadyne)], Glutamate regulator [Memantine (Namenda)], and Cholinesterase inhibitor + glutamate regulator [Donepezil and memantine (Namzaric)]. The survey also allowed participants to add ‘other’ cognitive enhancing supplements and medications.
We asked survey respondents about related medical diagnoses, including learning disorder or disability, ADHD, shift work sleep disorder, narcolepsy, sleep apnea with excessive daytime sleepiness, and neurodegenerative diseases such as Alzheimer’s disease or dementia. We also asked respondents about their motivations and perceptions of cognitive-enhancing supplements or medications. The University of Utah Institutional Review Board (IRB) approved the survey (Supplement). The study adhered to the Declaration of Helsinki.
We reported descriptive statistics of respondent demographics and stimulant use using counts and percentages out of the total for each question and out of the subset for nested questions. To evaluate the prevalence of using cognitive enhancing supplements or medications and the reasons, we used the raking procedure to weight our completed sample to represent the population of interest [21]. We only used gender for calibration due to the desire to keep the survey respondents anonymous. We present estimates and confidence intervals for the estimated prevalence of the population that uses the supplements and medications.
We used weighted multivariable logistic regression to estimate the impact of personal characteristics on the probability of using supplements and medications for improving cognitive performance. These characteristics included gender, marital status, parental status, and motivations and perceptions of use. Response variables included the use of supplements (either Noopept or Racetams) and the use of medications (Amphetamine, Methylphenidate, or Modafinil). We reported odds ratios (OR) and confidence intervals. A two-tailed alpha level of 0.05 was selected. We performed data analysis with R-4.1.3, using the R package ‘Survey’ for the raking procedure and the weighted logistic regression.
Results
According to institutional records of the resident demographics at the time of our study, our survey population consisted of 638 resident physicians with an average age of 31 years. The population consisted of 315 males (49.4%), 317 females (49.7%), and 6 unknown (0.9%). The most common ethnicity was White or Caucasian at 477 (74.8%), followed by Asian at 61 (9.6%), two or more races at 35 (5.5%), Hispanic/Latino/Spanish at 26 (4.1%), and unspecified at 26 (4.1%).
Of the 638 asked to participate, 296 (46.4%) residents completed the survey. Table 1 shows unweighted descriptive statistics summarizing the participant demographics. Among respondents, there were 144 females (48.6%), 120 males (40.5%), and 32 unknown (10.8%). One hundred and twenty-nine (45.9%) residents were married, and 54 (18.2%) had children. Most respondents (67.2%) were in a non-surgical medical specialty.
The most common medical specialty was Internal Medicine (16.6%), followed by Pediatrics (11.5%), and Anesthesiology (6.8%). Twenty-one (7.1%) respondents reported a history of ADHD, 23 (7.8%) shift work sleep disorder, 2 (0.7%) narcolepsy, and 4 (1.4%) sleep apnea with excessive daytime sleepiness.
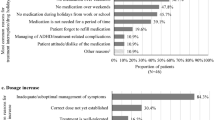
Using weighted analysis, we estimate the prevalence of caffeine use at 78.4%, the most among all the supplements (Table 2). Omega-3 fatty acids (9.9%), creatine (8.9%), and Lion’s Mane Mushroom (5.3%) were also common. Amphetamine and Modafinil were used the most among cognitive-enhancing medications at 19.2% and 11.1%, respectively. No residents used Glutamate regulators or Cholinesterase inhibitor + Glutamate regulators. To improve concentration, memory, or alertness and to increase studying or working time were the most common reasons for taking cognitive-enhancing supplements (82.1% and 58.9%) and medications (75.8% and 74.4%) (Fig. 1). Unfortunately, we observed a high non-response rate for questions asking when residents began taking supplements (97.3%) and medications (99.0%) and how frequently they use supplements (82.8%) and medications (82.8%) for cognitive enhancement.

Reasons for cognitive enhancing supplement (A) and medication (B) use (for those who used)
No residents reported side effects with supplement use, specifically with Noopept and Racetams. However, of those who reported taking cognitive-enhancing medications, 25 (49.0%) reported side effects with Amphetamine, including change in appetite (84.0%), sleeplessness (48.0%), euphoria or heightened sense of being (40.0%), anxiety or paranoia (36.0%), palpitations (28.0%), and headache (36.0%). Of the eight (50.0%) who reported taking Methylphenidate, sleeplessness (75.0%), change in appetite (37.5%), euphoria or heightened sense of being (37.5%), anxiety or paranoia (12.5%), and palpitations (12.5%) were the most common. Twelve (42.9%) residents reported adverse effects with Modafinil, including nausea or vomiting (66.7%), dizziness (16.7%), change in appetite (8.3%), euphoria or heightened sense of being (8.3%), palpitations (8.3%), and sleeplessness (8.3%).
Figure 2 shows the distribution of motivations and perceptions with the statement asked on the y-axis and the percentage of respondents on the x-axis. The percentage of respondents who agree with the statement is represented to the right of the zero line, while the percentage of respondents who disagree is shown to the left. The percentage of respondents who neither agree nor disagree is split down the middle and represented in a neutral color. The categories within each sector are ordered by the percentages who agree. Residents largely agreed (strongly agree and somewhat agree) with “I feel pressure to perform well professionally or academically,“ “I feel afraid that I will be left behind professionally or academically,“ and “It is possible to achieve the level of academic or professional performance expected of me without taking a cognitive enhancing supplement(s) or medication(s).“ Most disagreed (strongly disagree and somewhat disagree) with “I feel pressure to take cognitive-enhancing supplements or medications because my colleagues take them” and “I could not have reached my current level of training without taking a cognitive-enhancing supplement(s) or medication(s).“

Motivations and perceptions for cognitive enhancing supplement and/or medication use
Gender, marital status, medical specialty (surgical versus non-surgical), feeling nervous about the side effects of cognitive-enhancing supplements, and believing they could achieve the level of academic or professional performance without taking cognitive enhancing supplements had strong evidence of an association with using cognitive enhancing supplements (Fig. 3 A). Specifically, the odds for males were 1.06 times higher than females, p < 0.01. The odds for non-married residents were 1.05 times higher than married residents, p < 0.01. The odds for surgical residents were 1.05 times higher than non-surgical residents, p = 0.04. Residents who felt nervous about the side effects of cognitive-enhancing supplements or who believed they could achieve the level of academic or professional performance without taking them were less likely to take them, with OR of 0.99 and 0.96 (p-values of 0.03 and < 0.01), respectively.

Odds ratios (only for significant predictors) for use of cognitive enhancing supplements (A) and medications (B)
Gender, parental status, and all six motivation and perception survey items had strong evidence of an association with using cognitive-enhancing medications (Fig. 3B). Specifically, the odds for males were 1.21 times higher than females, p < 0.01. The odds for those without children were 1.11 times higher than those with children, p = 0.03. Residents who felt pressure to perform well, felt afraid of being left behind, felt pressure because their colleagues take them, felt nervous about getting into trouble if taking medications, or felt they could not reach their current level of training without taking medications were more likely to take cognitive enhancing medications with OR of 1.11, 1.04, 1.05, 1.07, and 1.08 (p-values of < 0.01, 0.01, 0.01, < 0.01, and < 0.01), respectively. Residents who felt nervous about the side effects, felt hesitant about the cost, or who believed they could achieve the level of academic or professional performance without taking cognitive-enhancing medications were less likely to take them, with OR of 0.9, 0.96, and 0.96 (p-values of < 0.01, 0.01, and 0.04).
Discussion
Cognitive-enhancing supplements and medications, also known as nootropics, to increase mental alertness, improve memory, and boost levels of energy and wakefulness in healthy individuals are on the rise [1,2,3]. With common motivations, including a stressful lifestyle, working in a competitive environment, and attempting to balance the rigors of academic or professional obligations and social expectations [15,16,17], the prevalence of cognitive-enhancing medication use among resident physicians is over 20% [15]. A prior study examining cognitive-enhancing medication use among resident physicians in Israel [15], focused on stimulants, specifically amphetamines and methylphenidate. However, other cognitive-enhancing medications, such as Modafinil and Glutamate regulators or Cholinesterase inhibitor + Glutamate regulators, have yet to be explored. In addition, our work represents the most comprehensive survey of cognitive enhancing supplement use among United States medical residents.
In our completed sample, supplements for cognitive enhancement were frequent with caffeine, omega-3 fatty acids, creatine, and Lion’s Mane Mushroom most reported. Interestingly, despite a robust list of possible supplements, residents added to these options with the most common ‘other’ supplement being nicotine. We surveyed multiple cognitive-enhancing medications and similar to other studies of resident physicians [15], prevalence of Amphetamine use was approximately 20% despite only 7% reporting a history of ADHD. Methylphenidate, another stimulant, was infrequently used, and unsurprisingly almost no respondents used cholinesterase inhibitors or glutamate regulators, commonly prescribed for Alzheimer’s disease and dementia. Newer medications, such as Modafinil which treats narcolepsy, sleep apnea, and shift work sleep disorder by promoting wakefulness and alertness was reported just over 11% use by residents. Unfortunately, over 95% of respondents did not indicate when they began using cognitive-enhancing supplements or medications and over 80% did not report how frequently they take them. It’s unclear why respondents did not complete these critical questions. It’s unlikely that respondents were confused by the questions given all pilot study respondents completed these questions. Potentially, the lack of response was due to fear of stigmata about onset and frequency of use.
Claims about the cognitive benefits of supplements and medications are poorly supported, and the health risks posed by their use may be significant. For example, a growing body of research supports the long-term alterations in brain plasticity and dependence on stimulants with frequent use [22]. In addition, the association of substance misuse and increased rates of suicide poses a serious concern as suicide continues to be a common cause of death for medical trainees, including residents [20]. Although no respondents reported side effects with supplements, we only focused on the side effects of Noopept and Racetams, which had a reasonably low prevalence. We chose to focus our queries on the side effects of these supplements because of their singular purpose of cognitive enhancement, as opposed to other supplements such as omega-3 fatty acids with other reported benefits. In addition, to maximize the survey response rate by minimizing survey duration, we were limited in the number and length of questions. However, a significant percentage of residents who reportedly used medications for cognitive enhancement experienced adverse effects. These ranged from a change in appetite, euphoria or heightened sense of being, anxiety or paranoia, headache, sleeplessness, nausea and vomiting, dizziness, and palpitations. Although it is unclear whether side effects directly influenced these medications, fear of medication side effects was associated with a lower likelihood of use.
Prior studies have examined several motivations for using cognitive-enhancing medications. In our completed sample, the two key motivations for using supplements and medications were to improve concentration, memory, or alertness and increase studying or working time. Residents who were male, not married, and were in surgical specialties were more likely to use supplements. Whereas residents who felt nervous about the side effects of supplements or who believed they could achieve the level of academic or professional performance without them were less likely to use them. Residents who were male or did not have children were more likely to take medications, as were those who felt pressure to perform well, felt afraid of being left behind, felt under the pressure of colleagues, or felt they could not have reached their current level training without taking the medication. Those who were nervous about the side effects, felt hesitant about the cost, and believed they could achieve the level of academic or professional performance without taking cognitive-enhancing medications were less likely to use them.
Male residents in our study were more likely to use cognitive-enhancing supplements and medications. Unfortunately, prior research on the use of cognitive-enhancing medications among resident physicians by Rubin-Kahana et al. does not shed light on the reason that males are more likely to use nootropics [15]; however, men are more likely to use illicit drugs and alcohol [23]. In addition, single male respondents without children were more likely to use cognitive-enhancing supplements and medications. Marriage and parenting seem to have a protective effect on using illicit drugs, alcohol, and tobacco, which may explain these data [24]. Given those critical motivations for using cognitive-enhancing supplements and medications were to improve concentration, memory, or alertness and to increase studying or working time; it makes sense that residents who were in surgical specialties, such as neurosurgery, were more likely to use cognitive enhancers when compared to non-surgical specialties, such as internal medicine. Surgical residencies tend to be among the most competitive specialties, according to the National Resident Matching Program (NRMP) results [25]. Surgical specialties also tend to have longer work hours and carry the additional demands of being on call, meaning residents are required to be available at any time in addition to regular working hours [26].
Comparing the incidence of cognitive-enhancing medication use in our population of resident physicians with a similarly demanding profession, law, demonstrates that rates of use are similar [27]. Specifically, between 9% and 18% of law students are reported to use cognitive-enhancing medications, most commonly Adderall and Ritalin, to improve academic performance. In addition to a similar incidence of use, motivations for use among law students were similar. Reasons listed by law students included improved concentration, increased studying and working time, increased mental alertness while studying, and preventing other students from having an academic edge over them.
Our study had several limitations. First, our survey was newly developed and could exhibit measurement errors. There is no existing, validated instrument to capture motivations for the use of cognitive-enhancing supplements and medications. However, we followed best practices in questionnaire development and performed a pilot study on approximately 5% of our target population. The feedback given by pilot study participants was incorporated into the final survey to improve accuracy. Second, this was a self-reported survey with the possibility of misreporting. However, the rates of misreporting sensitive behaviors in anonymous web-based surveys are reportedly low [28]. Our study population consisted of resident physicians at a single large urban United States academic institution, and results may not apply to other populations. In addition, our study did not inquire about ethnicity to protect respondents’ anonymity, therefore no sub-analysis was conducted due to this risk. Given the high degree of variability among residency program competitiveness, even at a single institution, it is difficult to draw conclusions about the competitive nature of the University of Utah and how it applies across residency programs throughout the United States. Although we surveyed resident physicians from multiple medical specialties, some specialties had a low number of respondents. Given that little is known about survey non-responders, we cannot rule out the presence of non-response bias. However, we did have a robust response rate of over 46%. Finally, although data suggests there may be cognitive benefits to stimulant and modafinil use [29, 30], we did not examine the benefits of cognitive-enhancing supplements and medications among resident physicians. Given modafinil has been shown to reduce cognitive errors in sleep-deprived residents [30], future research on the benefits and side effects of its use are needed. In addition to future research, the authors hope that residency programs can use the risk factors outlined in our study to create a screening protocol to identify residents at risk of abusing cognitive-enhancing medications and supplements. Screening protocols would allow programs to allocate additional resources to at risk residents, thereby minimize their use.
Conclusion
In conclusion, there was a high rate of supplement and medication use for cognitive enhancement among resident physicians at a single United States academic institution despite very few carrying a related medical diagnosis. Side effects of medications were not uncommon, and some had potentially serious health implications. Male residents in surgical specialties who were not married and did not have children were more likely to use cognitive enhancers. Those who used were more likely to feel pressure to perform well, feel afraid to be left behind, feel pressure from colleagues, or feel that they could not have reached their current level of training without them. Given the potential short- and long-term impact of their use, we need more research on the effects of cognitive-enhancing supplements and medications. This study raises awareness of the increasing pressure individuals feel in competitive residency environments to turn to cognitive enhancement, despite few having a related medical diagnosis. The motivations to use cognitive enhancers, regardless of the significant risk of potential adverse effects, legal ramifications, fairness, and ethics of use, must be addressed. Therefore, in an era of increasing burnout, suicide, and substance abuse, we recommend institutions use the risk factors identified in our study to create and implement screening protocols to identify residents at risk for cognitive-enhancing medication and supplement misuse and potential harm.
Data Availability
The dataset used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- ADHD:
-
Attention deficit hyperactivity disorder.
- IRB:
-
Institutional review board.
- NRMP:
-
National Resident Matching Program.
- OR:
-
Odds ratios.
References
Chen LY, Crum RM, Strain EC, Alexander GC, Kaufmann C, Mojtabai R. Prescriptions, nonmedical use, and emergency department visits involving prescription stimulants. J Clin Psychiatry. 2016 Mar;77(3):e297–304.
d’Angelo LSC, Savulich G, Sahakian BJ. Lifestyle use of drugs by healthy people for enhancing cognition, creativity, motivation and pleasure. Br J Pharmacol. 2017 Oct;174(19):3257–67.
Emanuel RM, Frellsen SL, Kashima KJ, Sanguino SM, Sierles FS, Lazarus CJ. Cognitive enhancement drug use among future physicians: findings from a multi-institutional census of medical students. J Gen Intern Med. 2013 Aug;28(8):1028–34.
Cognitive enhancers -. Alcohol and Drug Foundation [Internet]. [cited 2022 Apr 18]. Available from: https://adf.org.au/drug-facts/cognitive-enhancers/.
Compton WM, Han B, Blanco C, Johnson K, Jones CM. Prevalence and Correlates of Prescription Stimulant Use, Misuse, Use Disorders, and Motivations for Misuse Among Adults in the United States. Am J Psychiatry. 2018 Aug 1;175(8):741–55.
McCabe SE, Knight JR, Teter CJ, Wechsler H. Non-medical use of prescription stimulants among US college students: prevalence and correlates from a national survey. Addict Abingdon Engl. 2005 Jan;100(1):96–106.
Herman-Stahl MA, Krebs CP, Kroutil LA, Heller DC. Risk and protective factors for nonmedical use of prescription stimulants and methamphetamine among adolescents. J Adolesc Health Off Publ Soc Adolesc Med. 2006 Sep;39(3):374–80.
Advokat CD, Guidry D, Martino L. Licit and illicit use of medications for Attention-Deficit Hyperactivity Disorder in undergraduate college students. J Am Coll Health J ACH. 2008 Jun;56(6):601–6.
Benson K, Flory K, Humphreys KL, Lee SS. Misuse of stimulant medication among college students: a comprehensive review and meta-analysis. Clin Child Fam Psychol Rev. 2015 Mar;18(1):50–76.
Kudlow PA, Naylor KT, Xie B, McIntyre RS. Cognitive enhancement in Canadian medical students. J Psychoact Drugs. 2013 Oct;45(4):360–5.
Cohen YG, Segev RW, Shlafman N, Novack V, Ifergane G. Methylphenidate use among medical students at Ben-Gurion University of the Negev. J Neurosci Rural Pract. 2015 Sep;6(3):320–5.
Fond G, Gavaret M, Vidal C, Brunel L, Riveline JP, Micoulaud-Franchi JA, et al. (Mis)use of Prescribed Stimulants in the Medical Student Community: Motives and Behaviors: A Population-Based Cross-Sectional Study. Med (Baltimore). 2016 Apr;95(16):e3366.
Papazisis G, Tsakiridis I, Pourzitaki C, Apostolidou E, Spachos D, Kouvelas D. Nonmedical Use of Prescription Medications Among Medical Students in Greece: Prevalence of and Motivation for Use. Subst Use Misuse. 2018 Jan 2;53(1):77–85.
Franke AG, Bagusat C, Dietz P, Hoffmann I, Simon P, Ulrich R, et al. Use of illicit and prescription drugs for cognitive or mood enhancement among surgeons. BMC Med. 2013 Apr;9:11:102.
Rubin-Kahana DS, Rubin-Kahana Z, Kuperberg M, Stryjer R, Yodashkin-Porat D. Cognitive enhancement drug use among resident physicians: Prevalence and motivations for use - results from a survey. J Addict Dis. 2020 Sep;38(3):250–6.
Hildt E, Lieb K, Franke AG. Life context of pharmacological academic performance enhancement among university students–a qualitative approach. BMC Med Ethics. 2014 Mar;7:15:23.
Weyandt LL, Oster DR, Marraccini ME, Gudmundsdottir BG, Munro BA, Rathkey ES, et al. Prescription stimulant medication misuse: Where are we and where do we go from here? Exp Clin Psychopharmacol. 2016 Oct;24(5):400–14.
Data R. and. Nootropics Market To Reach USD 5.32 Billion By 2026 | Reports And Data [Internet]. GlobeNewswire News Room. 2020 [cited 2022 Apr 18]. Available from: https://www.globenewswire.com/news-release/2020/02/19/1987135/0/en/Nootropics-Market-To-Reach-USD-5-32-Billion-By-2026-Reports-And-Data.html.
Collier VU, McCue JD, Markus A, Smith L. Stress in medical residency: status quo after a decade of reform? Ann Intern Med. 2002 Mar;5(5):384–90. 136(.
Neeleman J, Farrell M. Suicide and substance misuse. Br J Psychiatry J Ment Sci. 1997 Oct;171:303–4.
Deville JC, Särndal CE. Calibration Estimators in Survey Sampling. J Am Stat Assoc. 1992 Jun;87(418)(1):376–82.
Urban KR, Gao WJ. Performance enhancement at the cost of potential brain plasticity: neural ramifications of nootropic drugs in the healthy developing brain. Front Syst Neurosci. 2014;8:38.
Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration. 2019. NSDUH Detailed Tables. September 11, 2020. Accessed July 23, 2022. https://www.samhsa.gov/data/report/2019-nsduh-detailed-tables.
Salvatore JE, Gardner CO, Kendler KS. Marriage and reductions in men’s alcohol, tobacco, and cannabis use. Psychol Med. 2020 Nov;50(15):2634–40.
National Resident Matching Program, Results and Data. 2022 Main Residency Match®. Washington, DC: National Resident Matching Program; 2022.
Leigh JP, Tancredi D, Jerant A, Kravitz RL. Annual work hours across physician specialties. Arch Intern Med. 2011 Jul;11(13):1211–3. 171(.
Organ J, Jaffe D, Bender K. Suffering in Silence: The Survey of Law Student Well-Being and the Reluctance of Law Students to Seek Help for Substance Use and Mental Health Concerns. J Leg Educ. 2016 Sep 1;66(1):116.
Gnambs T, Kaspar K. Disclosure of sensitive behaviors across self-administered survey modes: a meta-analysis. Behav Res Methods. 2015 Dec;47(4):1237–59.
Bagot KS, Kaminer Y. Efficacy of stimulants for cognitive enhancement in non-attention deficit hyperactivity disorder youth: a systematic review. Addict Abingdon Engl. 2014 Apr;109(4):547–57.
Sugden C, Housden CR, Aggarwal R, Sahakian BJ, Darzi A. Effect of pharmacological enhancement on the cognitive and clinical psychomotor performance of sleep-deprived doctors: a randomized controlled trial. Ann Surg. 2012 Feb;255(2):222–7.
Acknowledgements
The authors would like to acknowledge Elizabeth Nutall and Deborah Harrison for their assistance with the IRB approval.
Funding
Supported in part by an Unrestricted Grant from Research to Prevent Blindness, New York, NY, to the Department of Ophthalmology & Visual Sciences, University of Utah. This investigation was supported by the University of Utah Study Design and Biostatistics Center, with funding in part from the National Center for Research Resources and the National Center for Advancing Translational Sciences, National Institutes of Health, through Grant 8UL1TR000105 (formerly UL1RR025764).
Author information
Authors and Affiliations
Contributions
These authors contributed equally to this work: BK, MMM, BJB, CW, JP contributed to the design of the research, the development of instrument, and the conduct/analysis of qualitative survey results. TE developed the concept of this paper, assisted in the statistical analyses, and drafted the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the University of Utah Institutional Review Board (IRB) (Reference number 00140788). Informed consent was obtained from all participants. All methods were carried out in accordance with relevant guidelines and regulations. The study adhered to the Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests:
The authors have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Etheridge, T., Kennedy, B., Millar, M.M. et al. Cognitive enhancing supplements and medications in United States Resident Physicians. BMC Med Educ 22, 744 (2022). https://doi.org/10.1186/s12909-022-03778-w
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12909-022-03778-w