
Abstract
Background
Self-regulated learning (SRL), which is learners’ ability to proactively select and use different strategies to reach learning goals, is associated with academic and clinical success and life-long learning. SRL does not develop automatically in the clinical environment and its development during the preclinical to clinical learning transition has not been quantitatively studied. Our study aims to fill this gap by measuring SRL in medical students during the transitional period and examining its contributing factors.
Methods
Medical students were invited to complete a questionnaire at the commencement of their first clinical year (T0), and 10 weeks later (T1). The questionnaire included the Motivated Strategies for Learning Questionnaire (MSLQ) and asked about previous clinical experience. Information about the student’s background, demographic characteristics and first clinical rotation were also gathered.
Results
Of 118 students invited to participate, complete paired responses were obtained from 72 medical students (response rate 61%). At T1, extrinsic goal orientation increased and was associated with gender (males were more likely to increase extrinsic goal orientation) and type of first attachment (critical care and community based attachments, compared to hospital ward based attachments). Metacognitive self-regulation decreased at T1 and was negatively associated with previous clinical experience.
Conclusions
Measurable changes in self-regulated learning occur during the transition from preclinical learning to clinical immersion, particularly in the domains of extrinsic goal orientation and metacognitive self–regulation. Self–determination theory offers possible explanations for this finding which have practical implications and point the way to future research. In addition, interventions to promote metacognition before the clinical immersion may assist in preserving SRL during the transition and thus promote life-long learning skills in preparation for real-world practice.
Similar content being viewed by others


Background
In the context of a constantly advancing medical world, the medical profession must consistently meet the high standards of optimal patient care [1, 2] and maintain their area of expertise throughout their careers [3, 4]. It is important that doctors become life-long learners who take control of their learning needs and activities through self-regulated learning [1, 2, 5]. Self-regulated learning (SRL) is defined as a process where the learner is motivationally, behaviourally and meta-cognitively proactive in the learning process [5]. In the clinical environment SRL has been associated with academic achievement [4, 6–8], success in clinical skills [9] and emotional health [10].
The initial transition from preclinical learning to clinical immersion is a significant and unique phase in a medical student’s education when students shift from spending more time learning in the classroom to experiential learning in the clinical setting [11–15]. In contrast to preclinical learning, students in immersive clinical rotations report the elements of adjusting to new environments with heavy workloads and long working hours [12, 16, 17], adapting to different expectations, forms of assessment and teaching styles [12, 18], feeling at times useless and uncertain about their role [12, 19, 20] and adapting to a more self–directed learning style [16, 20, 21]. Specifically, research suggests that despite the addition of clinical tutorials to the preclinical curriculum, students during the clinical transition face considerable challenges, ambiguity and uncertainty [12, 22, 23]. As well as opportunities, these experiences present potential disruptions to the development of the skills needed for life-long learning. However to our knowledge, no research has explored the changes in self -regulated learning that occur during the initial transition period from preclinical to clinical immersion using a quantitative approach.
We therefore aimed to measure the changes that occur in self-regulated learning during the critical transition from pre-clinical to immersive clinical learning and associated factors. We hypothesized that changes in SRL would occur, as the learning environment is a key factor affecting SRL in many theoretical models [2, 24, 25]. Our research questions were: “what are the changes in SRL during the transition to the clinical learning environment?” and “what factors are associated with that change?” Through these research questions we aimed to enhance our understanding of medical student motivation and learning during the clinical transitional period, which has implications on curricula and future research directions.
Method
Study setting
The study participants were 3rd year medical students at Western Sydney University, Australia. The curriculum is a 5-year undergraduate program. The first 2 years comprise of problem based learning in small groups with weekly clinical tutorials in hospital settings. The final 3 years are based on a model of clinical immersion in rural and metropolitan hospitals as well as community based attachments. In the first clinical year (3rd year of the course) there are seven rotations in a year, where each rotation is of a 5-week duration: two medical, two surgical, two community (consisting of community health service and general practice) and one critical care (consisting of emergency department and anaesthetics) attachments.
Study participants
This study was conducted in 2015 with a cohort of students (n = 118) at the beginning of first clinical year. Ethical approval was obtained from Western Sydney University (ID H9989).
Data collection
Consenting students were invited to complete a questionnaire at the introductory lectures prior to the commencement of their first clinical placement (Time 0, T0). The survey was repeated after the first 10 weeks of clinical placements (Time 1, T1). Only those who responded at both T0 and T1 and where paired responses could be identified were included in the analysis. The T1 time of 10 weeks was chosen as the organizational psychology literature suggests newcomers learn, adjust and adapt to the job, roles and culture of a workplace rapidly in the first 1–2 months post-entry period [26–29], that the resulting adjustments are relatively stable [30–32] and that early adaptations are related to important outcomes for both organizations and new employees [29, 30, 33, 34].
Motivated Strategies for Learning Questionnaire (MSLQ)
The MSLQ is a validated instrument based upon the social cognitive theory of learning to measure SRL [35, 36]. The instrument has been used in a wide range of population groups, from students in primary schools to those in higher education. Several studies have used the MSLQ as part of medical education research and have found associations between MSLQ scores and academic achievement [6, 37–39]. One preliminary study used the MSLQ to measure the changes in SRL of preclinical medical students that occurred between the first and second year of their course [40].
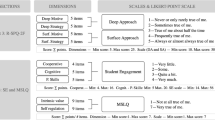
The MSLQ uses a 7-point Likert-type scale comprising of 2 sections, motivation and learning strategies. The motivation section contains 31 items assessing 3 domains: goal orientation, self-belief about learning, and test-provoked anxiety. The learning section contains 50 items assessing 3 domains: the use of cognitive strategies, metacognitive strategies and resource management (Additional file 1: Appendix 1).
First clinical rotation
Data was extracted from student records and included information about what the students’ first clinical attachment would be: medicine, surgery, critical care or the community attachment.
Participant background
Demographic data such as age, gender and entry status were extracted from student records. Entry status categories included school-leaver students who entered immediately after high school; non school-leaver students who started but have not finished another tertiary degree; graduate students who have completed another tertiary degree; and international students. As part of the T0 questionnaire, students were asked whether they had any prior clinical experience other than the compulsory clinical medicine tutorials during the first 2 years.
Data analysis
For each subscale of the MSLQ, the data were categorized into 3 categories: low scores (1.0 to <2.5), medium scores (2.5 to <5), and high scores (5 to <7). The Marginal Homogeneity Test was used to assess the significance of differences in each MSLQ subscale between T0 and T1. For subscales which were found to have a significant difference (p < 0.05), respondents’ scores were categorised as having increased, decreased or stayed in the same categories between T0 and T1. Ordinal Logistic Regression and Multiple Logistic Regression were then used to explore which dependent variables influenced the MSLQ subscale score changes between T0 and T1. As age reflects entry status, and entry status was considered more relevant to SRL than age, only entry status was entered into the regression analyses to avoid multi-collinearity. In the Ordinal Logistic Regression, the proportionality-of-odds assumption was evaluated by the likelihood-ratio test. All statistical analysis was performed with IBM SPSS Statistics 22.
For the purposes of analysis, medical and surgical first attachment groups were then combined. The rationale for this is that both medical and surgical attachments are similar in structure with 1–2 students being attached to relatively large ward-based teams and have the same clinical assessments. The critical care attachment does not involve ward round-based teaching but instead 1:1 shift-based clinical supervision with more formal tutorials. The community attachment also involves 1:1 supervision but focuses less on disease and treatment and more on the psychosocial, cultural, environmental and economic elements that can affect health.
Results
Of 118 students who were invited to participate, 94 responses were obtained at T0 (response rate 80%), and 75 responses were obtained at T1 (response rate 64%). Paired, complete responses were obtained from 72 medical students (response rate 61%).
Of the 72 respondents, most were female (61.1%), non-school leavers (44.4%), had previous clinical exposure (51.4%) and their first attachment was either medicine or surgery (58.3%). The mean age of respondents was 21.3 years (range 19–30, standard deviation, 1.7; Table 1). There were no statistically significant difference between the sample and the whole cohort with regard to gender, age, entry status or first rotation (all p > 0.05; data not shown).
Table 2 shows the change in SRL measured by the MSLQ between T0 and T1. Two scales (extrinsic goal orientation and metacognitive self-regulation) in the MSLQ showed significant differences between T0 and T1 (p < 0.033, p < 0.001 respectively). Extrinsic motivation increased and metacognitive self-regulation decreased. Domains of self-regulated learning that did not change in our study included the motivation scales of intrinsic goal orientation, task value, control beliefs, self-efficacy and test anxiety as well as the learning strategy scales of rehearsal, elaboration, organization, critical thinking, time and study environment regulation, effort regulation, peer learning and help-seeking behaviour.
The factors “entry status”, “gender”, “previous clinical experience” and “first clinical attachment” were entered into an ordinal logistic regression for extrinsic goal orientation. For metacognitive self-regulation as the data distribution was dichotomous, a binary logistic regression was used. Both regression analyses are summarized in Table 3. Regarding extrinsic goal orientation, two independent factors were identified: gender and first attachment. Male students were more likely to increase in extrinsic goal orientation (OR 4.1, 95% CI 1.2–13.5, p < 0.021) as were students on critical care (OR 8.7, 95% CI 1.6–48.5, p < 0.013) and students on the community attachment (OR 3.8, 95% CI 1.1–14.0, p < 0.042). Concerning metacognitive self-regulation the sole independent factor was previous clinical experience—students with extra previous clinical experience were more likely to have lower levels of metacognitive self-regulation (OR 5.0 95% CI 1.1–22.2, p < 0.035).
Discussion
This study has investigated the changes in SRL during the transition to clinical learning in the first clinical year and identified factors associated with that change. Our results indicated changes occurred in the two domains of extrinsic goal orientation and metacognitive self-regulation. Factors associated with an increase in extrinsic goal orientation were gender (male vs female) and first attachment (critical care and the community attachment vs medicine/surgery). The single factor associated with a decrease in metacognitive self-regulation was previous clinical experience (no experience vs experience).
Extrinsic motivation
According to the MSLQ, extrinsic goal orientation is defined as the degree to which a student perceives the importance of issues that are not directly related to participating in the task itself [41]. This includes grades, rewards and reputation. Studies from the transitions literature provide an explanation as to why transitioning clerkship students increase in extrinsic motivation, and how this may relate to their gender and first attachment.
As opposed to the preclinical years where students are assessed in formal examination settings, the literature suggests students in immersive clinical settings feel constantly informally assessed by their supervisors. [42–46]. These studies suggest clerkship students are more extrinsically motivated in their learning as impressing their supervisor may lead to further experiential learning opportunities, better evaluations and future career prospects [42–46]. This also explains why in our study, compared to the transitioning students on the ward-based attachments, the students whose first rotations involved 1:1 supervision (the critical care and the community attachments) were more likely to increase in extrinsic goal orientation.
In regards to gender, our study found that male students are more likely to develop an increase in extrinsic goal orientation with qualitative studies from the transitions literature supporting our finding [47, 48]. Supervisors may have gender-biased expectations of performance which lead to female medical students receiving less pressure [47].
A more nuanced explanation as to why students experience an increase in extrinsic goal orientation during the transition to the clinical environment can be provided by the self-determination theory (SDT) of Ryan and Deci, which is a more recent model of motivation to the MSLQ. Researchers widely agree that when possible, intrinsic motivation is preferred as it has been linked with more enjoyment [49], more engagement [50, 51] and better learning [52, 53]. According to Ryan and Deci, for extrinsic motivation to develop into intrinsic motivation, the student must be interested in the task at hand as well as have their needs of competence, autonomy and relatedness met [54]. According to SDT, competence refers to the experience of behaviour being effectively enacted. The feeling of competence is supported when activities are optimally challenging, thereby allowing students to test and expand their academic capabilities, or when feedback promotes feelings of efficacy or eventual mastery [49]. Autonomy occurs when a student’s behaviour is aligned with their authentic interests or integrated values and desires, and when the student fully endorses the actions they engaged in or the values they expressed [53, 55]. Autonomy is lost when the student feels they are compelled to behave in specific ways regardless of their own values or interests [55]. The need for relatedness refers to the tendency for people to internalise and adopt the values and the practices of those they feel connected to or desire a connection with, and from contexts where they feel belonging [49]. Relatedness is supported when a teacher genuinely likes, respects and values the student [49]. According to SDT, if the needs of competence, autonomy and relatedness are not met, any motivation will be extrinsic as opposed to intrinsic in nature.
When analysed through the frame of SDT, previous studies in the transitions literature suggests medical students in the transition period may experience a lack of all three needs: students feel they lack competence, autonomy and relatedness [11, 16, 46, 56–59]. Radcliffe and Lester found that during the transition students had experiences “of feeling useless [and] unable to contribute to patient care because they had insufficient knowledge or skills” [lack of competence] [11]. The lack of competence felt by medical students during the clinical transition is supported by other studies [58, 59]. In regards to autonomy, studies suggest that students feel they often complete tedious tasks such as paperwork at the request of their consultant physician instead of engaging in tasks more aligned with their interests and values, such as talking to patients [16, 46]. In regards to relatedness, students may feel they are neither being genuinely valued nor respected, with older studies suggesting that levels of abuse (verbal, physical, sexual and academic) experienced by medical students are high (50–93%) [56, 60–62].
Newer research suggest some forms of extrinsic motivation may be similar to intrinsic motivation [53]. It is important to state that there are—according to self-determination theory—4 types of extrinsic motivation (externally regulated, introjected, identified and integrated). Externally regulated motivation (where behaviours are enacted to obtain a reward or to avoid punishment) and introjected motivation (whereby behaviours are enacted in order to primarily protect one’s ego) are believed to be shallower forms of motivation whose behaviours are poorly maintained once the controlling extrinsic factors have been removed [54]. Identified motivation (where behaviours are enacted because of the perceived value of the task) and integrated motivation (where behaviours are enacted because they are aligned with other aspects of self) are believed to be deeper forms of motivation, whose behaviour stems from more autonomous motivation [53, 54]. The distinction between the former two and latter two types of motivations is critical because studies in educational psychology suggest that higher amounts of autonomous extrinsic motivation are linked with academic success, quicker adjustment, greater well-being, decreased anxiety and more intrinsic enjoyment [49, 63–65] which are all highly relevant to the transitions period. Thus it may be well worth for the MSLQ extrinsic motivation subscale to be revised so that it can distinguish between each of the different types of extrinsic motivation. Practically this is important, because if the increases in extrinsic motivation are not beneficial, then curriculum designers could structure first attachments so that transitioning students feel less monitored and more autonomous in their learning.
Metacognitive self-regulation
The MSLQ defines metacognition as the awareness and control of cognition that can be broken down into three general processes: planning, monitoring, and regulating [41]. Planning activities include goal setting and reflecting on prior knowledge that make organizing and comprehending the material easier. Monitoring activities include the tracking of attention and self-testing. Regulating activities include adjusting one’s cognitive and behavioural activities.
In our study, previous clinical experience was associated with a decrease in metacognitive self-regulation. This finding was surprising as we hypothesised that students with previous clinical experience would find the transition period less stressful and thus need to use less cognitive resources to adapt, spending more of their cognitive resources on metacognition. These hypotheses are consistent with previous transitions literature suggesting that prior clinical experience leads to a smoother transition [66–68] and potentially less cognitive load [69]. There is no clear reason for our findings from this research.
The decrease in metacognitive self-regulation has real-world importance. Studies suggest that metacognition has a positive association with academic performance [35] and surgical skills acquisition [70], a negative association with procrastination [4] and depression [9], and is important for clinical reasoning, decision making [71, 72] and the continuous process of life-long learning [73, 74]. Furthermore, positive metacognitive abilities have been associated with a decreased level of perceived stress [75]. On a conceptual level, because clerkships are based upon the principles of experiential learning, the success of clerkship depends in part on a student’s capacity for reflective practice and accurate self-assessment [76, 77]. Therefore metacognitive self-regulation is critical for students to be able to learn effectively, especially during the immersive clinical years as studies suggest that the student interactions with patients are rarely observed directly by clinical teachers [78, 79].
Fortunately, literature suggests that interventions can increase metacognitive processes. Chew showed a simple metacognitive checklist could facilitate metacognition in clinical decision-making [80], Sobral showed that a 30 h learning skills course for medical students could increase levels of reflection, one subset of metacognition [7] and Tanner suggests explicitly teaching metacognition may be efficacious [81]. Within the hospital, studies also suggest supervisors can increase the metacognition of their students by providing feedback [82], by “thinking-aloud”—which involves vocalizing their thought processes involved in clinical reasoning [83] and by emphasizing the importance of learning over outcome [84]. Our research suggests a metacognitive intervention before or during the transition may be valuable so that students can experience less stress and optimize their learning.
Limitations
Our study had several limitations. Due to the single-institution design of the study, care must be taken not to over interpret our findings particularly with respect to transitions in different medical schools. Furthermore our study focussed on a single transition and thus transferability to other cohorts is limited. However, as the clinical transition structure is the same across the years, it is possible that similar trends may exist in other cohorts. A questionnaire was our main data collection tool, therefore social desirability bias may be present. However the MSLQ has reasonable psychometric properties [34]. With our factor “first attachment” there is likely to be inherent differences within rotations. For example, two medical rotations could have different supervisor–student dynamics. Despite this likely diversity of experiences within the attachments, a significant effect of first attachment was still found for extrinsic motivation. The results of our study had wide confidence intervals and negative results and therefore a larger study should be conducted to get a clearer insight into the transitional period. Finally, due to the response rate we obtained, a possibility of selection bias and type 2 error exists.
Conclusion
Our study explored the changes in the SRL of medical students during the transition to immersive clinical learning using a quantitative approach. We found that 10 weeks after transitioning to clinical learning, students significantly increased in extrinsic goal orientation and significantly decreased in metacognitive self-regulation. Factors associated with the increase in extrinsic goal orientation were gender and first clinical attachment, with the style of clinical supervision being a possible explanation for the observed differences between attachments. The sole factor associated with the decrease in metacognitive self-regulation was previous clinical experience. Although a larger study with multiple cohorts from multiple institutions is necessary to improve the generalizability of our findings, our study suggests that future research could further explore the transition to clinical learning through the lens of SDT, as well as interventions to enhance metacognition and thus learning during the transition period.
Abbreviations
- MSLQ:
-
Motivated strategies for learning questionnaire
- SDT:
-
Self determination theory
- SRL:
-
Self-regulated learning
References
Lucieer SM, Jonker L, Visscher C, Rikers RMJP, Themmen APN. Self-regulated learning and academic performance in medical education. Med Teach. 2016;38(6):585–93.
Brydges R, Butler D. A reflective analysis of medical education research on self-regulation in learning and practice. Med Educ. 2012;46(1):71–9.
Greveson GC, Spencer JA. Self-directed learning--the importance of concepts and contexts. Med Educ. 2005;39(4):348–9.
Artino Jr AR, Dong T, DeZee KJ, Gilliland WR, Waechter DM, Cruess D, et al. Achievement goal structures and self-regulated learning: relationships and changes in medical school. Acad Med. 2012;87(10):1375–81.
Zimmerman BJ. Becoming a self-regulated learner: Which are the key subprocesses? Contemp Educ Psychol. 1986;11(4):307–13.
Turan S, Konan A. Self-regulated learning strategies used in surgical clerkship and the relationship with clinical achievement. J Surg Educ. 2012;69(2):218–25.
Song HS, Kalet AL, Plass JL. Assessing medical students’ self-regulation as aptitude in computer-based learning. Adv Health Sci Educ. 2011;16(1):97–107.
Sobral DT. An appraisal of medical students’ reflection-in-learning. Med Educ. 2000;34(3):182–7.
Cleary TJ, Sandars J. Assessing self-regulatory processes during clinical skill performance: A pilot study. Med Teach. 2011;33(7):e368–e74.
Van Nguyen H, Laohasiriwong W, Saengsuwan J, Thinkhamrop B, Wright P. The relationships between the use of self-regulated learning strategies and depression among medical students: An accelerated prospective cohort study. Psychol Health Med. 2015;20(1):59–70.
Dubé TV, Schinke RJ, Strasser R, Couper I, Lightfoot NE. Transition processes through a longitudinal integrated clerkship: a qualitative study of medical students’ experiences. Med Educ. 2015;49(10):1028–37.
Radcliffe C, Lester H. Perceived stress during undergraduate medical training: a qualitative study. Med Educ. 2003;37(1):32–8.
Haglund ME, aan het Rot M, Cooper NS, Nestadt PS, Muller D, Southwick SM, et al. Resilience in the third year of medical school: a prospective study of the associations between stressful events occurring during clinical rotations and student well-being. Acad Med. 2009;84(2):258–68.
Gaufberg EH, Batalden M, Sands R, Bell SK. The hidden curriculum: what can we learn from third-year medical student narrative reflections? Acad Med. 2010;85(11):1709–16.
Treadway K, Chatterjee N. Into the water--the clinical clerkships. New Engl J Med. 2011;364(13):1190–3.
Prince KJ, Boshuizen H, Van Der Vleuten CP, Scherpbier AJ. Students’ opinions about their preparation for clinical practice. Med Edu. 2005;39(7):704–12.
Prince KJAH, van de Wiel M, Scherpbier AJJA, Cess PM, Boshuizen HPA. A qualitative analysis of the transition from theory to practice in undergraduate training in a PBL-medical school. Adv Health Sci Educ. 2000;5(2):105–16.
Remmen R, Denekens J, Scherpbier A, Hermann I, Van Der Vleuten C, Royen PV, et al. An evaluation study of the didactic quality of clerkships. Med Educ. 2000;34(6):460–4.
Pitkala K, Mantyranta T. Professional socialization revised: medical students’ own conceptions related to adoption of the future physician’s role--a qualitative study. Med Teach. 2009;25(2):155-160
Seabrook MA. Clinical students’ initial reports of the educational climate in a single medical school. Med Educ. 2004;38(6):659–69.
White CB. Smoothing out transitions: How pedagogy influences medical students’ achievement of self-regulated learning goals. Adv Health Sci Educ. 2007;12(3):279–97.
Teunissen PW, Westerman M. Opportunity or threat: the ambiguity of the consequences of transitions in medical education. Med Educ. 2011;45(1):51–9.
O’Brien B, Cooke M, Irby DM. Perceptions and attributions of third-year student struggles in clerkships: do students and clerkship directors agree? Acad Med. 2007;82(10):970–8.
Zimmerman BJ, Schunk DH. Self-regulated learning and academic achievement: Theoretical perspectives. New York: Lawrence Erlbaum Associates; 2001.
Durning SJ, Cleary TJ, Sandars J, Hemmer P, Kokotailo P, Artino AR. Perspective: viewing “strugglers” through a different lens: How a self-regulated learning perspective can help medical educators with assessment and remediation. Acad Med. 2011;86(4):488–95.
Chan D, Schmitt N. Interindividual differences in intraindividual changes in proactivity during organizational entry: a latent growth modeling approach to understanding newcomer adaptation. J Appl Psychol. 2000;85(2):190.
Chen G, Klimoski RJ. The impact of expectations on newcomer performance in teams as mediated by work characteristics, social exchanges, and empowerment. Acad Manage J. 2003;46(5):591–607.
Cooper‐Thomas H, Anderson N. Newcomer adjustment: The relationship between organizational socialization tactics, information acquisition and attitudes. J Occup Organ Psychol. 2002;75(4):423–37.
Cooper‐Thomas HD, Anderson N. Organizational socialization: A field study into socialization success and rate. Int J Select Assess. 2005;13(2):116–28.
Morrison EW. Longitudinal study of the effects of information seeking on newcomer socialization. J Appl Psychol. 1993;78(2):173.
Ostroff C, Kozlowski SW. Organizational socialization as a learning process: The role of information acquisition. Pers Psychol. 1992;45(4):849–74.
Ashforth BE, Saks AM. Work-role transitions: A longitudinal examination of the Nicholson model. J Occup Organ Psychol. 1995;68(2):157–75.
Allen NJ, Meyer JP. The measurement and antecedents of affective, continuance and normative commitment to the organization. J Occup Psychol. 1990;63(1):1–18.
Saks AM, Ashforth BE. Organizational socialization: Making sense of the past and present as a prologue for the future. J Vocat Behav. 1997;51(2):234–79.
Pintrich PR, Smith DA, García T, McKeachie WJ. Reliability and predictive validity of the Motivated Strategies for Learning Questionnaire (MSLQ). Educ Psychol Meas. 1993;53(3):801–13.
Pintrich PR, De Groot EV. Motivational and self-regulated learning components of classroom academic performance. J Educ Psychol. 1990;82(1):33.
Stegers‐Jager KM, Cohen‐Schotanus J, Themmen AP. Motivation, learning strategies, participation and medical school performance. Med Educ. 2012;46(7):678–88.
Cook DA, Thompson WG, Thomas KG. The motivated strategies for learning questionnaire: score validity among medicine residents. Med Educ. 2011;45(12):1230–40.
Pizzimenti MA, Axelson RD. Assessing student engagement and self-regulated learning in a medical gross anatomy course. Anat Sci Educ. 2015;8(2):104–10.
Kim KJ, Jang HW. Changes in medical students’ motivation and self-regulated learning: a preliminary study. Int J Med Educ. 2015;6:213–5.
Pintrich PR. A manual for the use of the Motivated Strategies for Learning Questionnaire (MSLQ). 1991.
Al Kadri HM, Al-Moamary MS, Elzubair M, Magzoub ME, AlMutairi A, Roberts C, et al. Exploring factors affecting undergraduate medical students’ study strategies in the clinical years: a qualitative study. Adv Health Sci Educ. 2011;16(5):553–67.
Han H, Roberts NK, Korte R. Learning in the real place: medical students’ learning and socialization in clerkships at one medical school. Acad Med. 2015;90(2):231–9.
Al-Kadri HM, Al-Kadi MT, Van Der Vleuten CP. Workplace-based assessment and students’ approaches to learning: a qualitative inquiry. Med Teach. 2013;35 Suppl 1:S31–8.
Lempp H, Seale C. The hidden curriculum in undergraduate medical education: qualitative study of medical students’ perceptions of teaching. BMJ. 2004;329(7469):770–3.
White CB, Kumagai AK, Ross PT, Fantone JC. A qualitative exploration of how the conflict between the formal and informal curriculum influences student values and behaviors. Acad Med. 2009;84(5):597–603.
Babaria P, Abedin S, Nunez-Smith M. The effect of gender on the clinical clerkship experiences of female medical students: Results from a qualitative study. Acad Med. 2009;84(7):859–66.
Hill E, Vaughan S. The only girl in the room: how paradigmatic trajectories deter female students from surgical careers. Med Educ. 2013;47(6):547–56.
Niemiec CP, Ryan RM. Autonomy, competence, and relatedness in the classroom Applying self-determination theory to educational practice. Theor Res Educ. 2009;7(2):133–44.
Reeve J, Jang H, Carrell D, Jeon S, Barch J. Enhancing students’ engagement by increasing teachers’ autonomy support. Motiv Emotion. 2004;28(2):147–69.
Reeve J. Self-determination theory applied to educational settings. In: Deci EL, Ryan RM, editors. Handbook of self-determination research. Rochester: University of Rochester Press; 2002. p. 470.
Amabile TM. Creativity in context: Update to“the social psychology of creativity.” Boulder: Westview press; 1996.
Ryan RM, Deci EL. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am Psychol. 2000;55(1):68.
Ryan RM, Deci EL. Intrinsic and extrinsic motivations: Classic definitions and new directions. Contemp Educ Psychol. 2000;25(1):54–67.
Chirkov V, Ryan RM, Kim Y, Kaplan U. Differentiating autonomy from individualism and independence: a self-determination theory perspective on internalization of cultural orientations and well-being. J Pers Soc Psychol. 2003;84(1):97.
Lubitz RM, Nguyen DD. Medical student abuse during third-year clerkships. JAMA. 1996;275(5):414–6.
O’Sullivan M, Martin J, Murray E. Students’ perceptions of the relative advantages and disadvantages of community-based and hospital-based teaching: a qualitative study. Med Educ. 2000;34(8):648–55.
Dornan T, Tan N, Boshuizen H, Gick R, Isba R, Mann K, et al. How and what do medical students learn in clerkships? Experience based learning (ExBL). Adv Health Sci Educ. 2014;19(5):721–49.
Hayes K, Feather A, Hall A, Sedgwick P, Wannan G, Wessier-Smith A, et al. Anxiety in medical students: is preparation for full-time clinical attachments more dependent upon differences in maturity or on educational programmes for undergraduate and graduate entry students? Med Educ. 2004;38(11):1154–63.
Richman JA, Flaherty JA, Rospenda KM, Christensen ML. Mental health consequences and correlates of reported medical student abuse. JAMA. 1992;267(5):692–4.
Silver HK, Glicken AD. Medical student abuse: incidence, severity, and significance. JAMA. 1990;263(4):527–32.
Sheehan KH, Sheehan DV, White K, Leibowitz A, Baldwin DC. A pilot study of medical student’abuse’: student perceptions of mistreatment and misconduct in medical school. JAMA. 1990;263(4):533–7.
Grolnick WS, Ryan RM, Deci EL. Inner resources for school achievement: Motivational mediators of children’s perceptions of their parents. J Educ Psychol. 1991;83(4):508.
Black AE, Deci EL. The effects of instructors’ autonomy support and students’ autonomous motivation on learning organic chemistry: A self-determination theory perspective. Sci Educ. 2000;84(6):740–56.
Williams GC, Deci EL. Internalization of biopsychosocial values by medical students: a test of self-determination theory. J Pers Soc Psychol. 1996;70(4):767.
Godefrooij MB, Diemers AD, Scherpbier AJ. Students’ perceptions about the transition to the clinical phase of a medical curriculum with preclinical patient contacts; a focus group study. BMC Med Educ. 2010;10(1):28.
Littlewood S, Ypinazar V, Margolis SA, Scherpbier A, Spencer J, Dornan T. Early practical experience and the social responsiveness of clinical education: systematic review. BMJ. 2005;331(7513):387–91.
Windish DM, Paulman PM, Goroll AH, Bass EB. Do clerkship directors think medical students are prepared for the clerkship years? Acad Med. 2004;79(1):56–61.
Paas F, Renkl A, Sweller J. Cognitive load theory and instructional design: Recent developments. Educ Psychol. 2003;38(1):1–4.
Gardner AK, Jabbour IJ, Williams BH, Huerta S. Different goals, different pathways: the role of metacognition and task engagement in surgical skill acquisition. J Surg Educ. 2016;73(1):61–5.
Colbert CY, Graham L, West C, White BA, Arroliga AC, Myers JD, et al. Teaching metacognitive skills: helping your physician trainees in the quest to ‘Know What They Don’t Know’. Am J Med. 2015;128(3):318–24.
Dunphy BC, Cantwell R, Bourke S, Fleming M, Smith B, Joseph KS, et al. Cognitive elements in clinical decision-making: Toward a cognitive model for medical education and understanding clinical reasoning. Adv Health Sci Educ. 2010;15(2):229–50.
Quirk M. Intuition and metacognition in medical education: Keys to developing expertise. Springer Publishing Company; 2006.
Cornford IR. Learning-to-learn strategies as a basis for effective lifelong learning. Int J Lifelong Educ. 2002;21(4):357–68.
Beer N, Moneta GB. Coping and Perceived Stress as a Function of Positive Metacognitions and Positive Meta-Emotions.Indiv Dif Res. 2012;10(2): 105-116.
Schön DA. Educating the reflective practitioner: Toward a new design for teaching and learning in the professions. San Francisco; 1987.
Eva KW, Regehr G. Self-assessment in the health professions: a reformulation and research agenda. Acad Med. 2005;80(10):S46–54.
Holmboe ES. Faculty and the observation of trainees’ clinical skills: problems and opportunities. Acad Med. 2004;79(1):16–22.
Carney PA, Pipas CF, Eliassen MS, Donahue DA, Kollisch DO, Gephart D, et al. An encounter-based analysis of the nature of teaching and learning in a 3rd-year medical school clerkship. Teach Learn Med. 2000;12(1):21–7.
Chew K, Durning S, van Merriënboer J. Teaching metacognition in clinical decision-making using a novel mnemonic checklist: an exploratory study. Singapore Med J. 2016;57(12):694–700.
Tanner KD. Promoting student metacognition. CBE-Life Sci Educ. 2012;11(2):113–20.
Cutting MF, Saks NS. Twelve tips for utilizing principles of learning to support medical education. Med Teach. 2012;34(1):20–4.
Gonullu I, Artar M. Metacognition in medical education. Educ Health. 2014;27(2):225.
Schraw G. Promoting general metacognitive awareness. Instr Sci. 1998;26(1-2):113–25.
Funding
There was no funding for this research project.
Availability of data and materials
The datasets used in the current study is available from the corresponding author on reasonable request.
Authors’ contributions
All authors were involved in designing the study. BM and KC were involved in the data analysis of the project. WH, KC and VL were involved in interpreting the data. All authors were involved in the editing process and approved the final manuscript.
Competing interests
The authors declare that there are no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
Ethics approval and consent was obtained from Western Sydney University (ID H9989). Informed written consent for publication was obtained in writing from all participants in the study.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Author information
Authors and Affiliations
Corresponding author
Additional file
Additional file 1:
Appendix 1 The Motivated Strategies for Learning Questionnaire (MSLQ). Description: The MSLQ, a validated instrument based upon the social cognitive theory of learning to measure SRL. (DOCX 52 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Cho, K.K., Marjadi, B., Langendyk, V. et al. Medical student changes in self-regulated learning during the transition to the clinical environment. BMC Med Educ 17, 59 (2017). https://doi.org/10.1186/s12909-017-0902-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12909-017-0902-7