
Abstract
Background
Obesity is a pressing public health risk issue worldwide. Women, in particular, face a higher risk of obesity. Recent research has highlighted the association between obesity and female sexual dysfunction. Therefore, the objective of this study is to investigate the global prevalence of sexual dysfunction in obese and overweight women through a systematic review and meta-analysis.
Methods
In this study, a systematic search was conducted across electronic databases, including PubMed, Scopus, Web of Science, Embase, ScienceDirect, and Google Scholar. The search aimed to identify studies published between December 2000 and August 2022 that reported metabolic syndrome's impact on female sexual dysfunction.
Results
The review included nine studies with a sample size of 1508 obese women. The I2 heterogeneity index indicated high heterogeneity (I2: 97.5). As a result, the random effects method was used to analyze the data. Based on this meta-analysis, the prevalence of sexual dysfunction in women with obesity was reported as 49.7% (95%CI: 35.8–63.5). Furthermore, the review comprised five studies involving 1411 overweight women. The I2 heterogeneity test demonstrated high heterogeneity (I2: 96.6). Consequently, the random effects model was used to analyze the results. According to the meta-analysis, the prevalence of sexual dysfunction in overweight women was 26.9% (95% CI: 13.5–46.5).
Conclusion
Based on the results of this study, it has been reported that being overweight and particularly obese is an important factor affecting women's sexual dysfunction. Therefore, health policymakers must acknowledge the significance of this issue in order to raise awareness in society about its detrimental effect on the female population.
Similar content being viewed by others


Background
Obesity and overweight refer to the excessive and abnormal accumulation of body fat, which leads to adverse health effects [1]. This condition represents a significant public health concern worldwide [2] and has detrimental health effects on individual well-being and society’s financial burden [3].
The increasing prevalence of high body mass index (BMI) and its associated mortality rates pose a significant threat to people's health in many countries [3]. However, there are distinct factors that contribute to the higher vulnerability of women compared to men in terms of being underweight, overweight, or obese, including variations in biological factors (such as hormones) and behavioural characteristics (such as childhood food deprivation and inadequate physical activity [4].
One possible explanation for this gender disparity is that women tend to experience more difficulties in long-term weight recovery and maintenance as they transition into adulthood and reproductive years [5].
Globally, approximately 40% of women are classified as overweight, while 15% are categorized as obese [6]. In the United States, the prevalence of obesity among adults aged 20–59 years is higher among women (38–41%) compared to men (34–38%) [7].
Epidemiological studies have identified obesity and overweight as significant risk factors for various diseases, including diabetes, certain cancers, cardiovascular diseases, and high blood pressure [3]. Moreover, women who are overweight or obese face a relatively higher risk of experiencing severe maternal complications and mortality [2]. These conditions can also lead to menstrual irregularity, reduced quality and quantity of ovulation, longer time to conceive, and the need for higher doses of medication to stimulate ovulation [8]. Furthermore, women's sexual response cycle is also a complex process influenced by multiple factors, including vascular, nervous, hormonal, and psychogenic factors. Any disruption in these factors can contribute to female sexual dysfunction (FSD) [9]. Additionally, certain treatments for these conditions, such as the use of certain anti-hypertensive drugs or antidepressants, can have negative effects on sexual performance [10].
Sexual dysfunction refers to any condition that hinders a person's ability to derive satisfaction from sexual activity [9]. In particular, female sexual dysfunction (FSD) is a complex disorder with multi-faceted causes rooted in biological and psychosocial factors [11]. FSD can have detrimental effects on an individual’s self-esteem, sense of wholeness, and interpersonal relationships, often leading to emotional discomfort [12].
The symptoms of FSD impact over 40% of adult women worldwide [11]. A comprehensive international clinical study revealed that 39% of sexually active women reported experiencing at least one form of sexual disorder. Notably, during menopause, the prevalence of this disorder ranges between 25 and 79% [13].
The symptoms of FSD impact over 40% of adult women worldwide [11]. A comprehensive international clinical study revealed that 39% of sexually active women reported experiencing at least one form of sexual disorder. Notably, during menopause, the prevalence of this disorder ranges between 25 and 79% [13].
In recent years, research has revealed a correlation between obesity and sexual dysfunction, with a significant number of obese women reporting that their primary sexual dysfunction is related to orgasmic difficulties [14].
Given the numerous complications associated with obesity and overweight and the significance of sexual dysfunction in women, we conducted a comprehensive review of studies in this field. Our objective was to perform a systematic review and meta-analysis to determine the global prevalence of sexual dysfunction among women who are obese or overweight. The findings of this study can provide crucial evidence to shed light on the issue of sexual dysfunction in obese and overweight women worldwide.
Methods
Our search was conducted from December 2020- August 2022 for this systematic review. Five databases, namely PubMed, Web of Science, Google Scholar, Scopus, ScienceDirect, and Embase, were searched to retrieve relevant articles using the keywords "Female Sexual Dysfunction" and “FSD”. To ensure the comprehensiveness of the search, no restrictions were placed on the publication year of the articles. The gathered information was subsequently organized and managed using the information management software EndNote.
Study selection
The inclusion criteria for the studies were as follows: cross-sectional studies, studies with accessible full-text versions, and studies that presented adequate data on sample size and prevalence. Conversely, the exclusion criteria encompassed case reports, case series studies, review and duplicate studies.
Data extraction
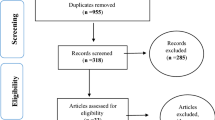
The selection of studies followed the guidelines outlined by PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses). Initially, duplicate studies found across different databases were excluded. To mitigate bias, two researchers independently conducted the review process and data extraction. In total, 505 articles were screened through database searches, and two potentially relevant articles were identified through manual searches. The selected articles were then imported into the information management software EndNote for further analysis. Following the PRISMA steps, the articles underwent thorough evaluation, resulting in the inclusion of 10 studies for the final review. The findings and relevant information from these 10 studies are presented in Table 1 and Fig. 1.

The flowchart on the stages of including the studies in the systematic review and meta-analysis (PRISMA 2009(
Quality evaluation and statistical analysis
To validate and assess the quality of articles, a STROBE checklist, designed for observational studies, was utilized. This checklist comprises 32 items. Articles that achieved a score of 16 or higher were categorized as having good or moderate methodological quality, whereas those scoring below 16 were deemed to exhibit poor methodological quality. As a result, articles characterized by poor methodological quality were excluded from the study. The extracted results of the selected studies were entered into Comprehensive Meta-Analysis, version 2 (Biostat Inc, New Jersey). To assess the heterogeneity of the studies, the I2 test was employed.
Results
In this systematic review and meta-analysis, most of the included studies were cross-sectional. Four studies were identified as case–control studies [17,18,19, 23], and one study was categorized as a case–control-cross-sectional study [15]. Moreover, most of the reviewed studies were conducted in Asian countries, with no studies identified from North America. Among the studies included, nine studies used the standard Female Sexual Function Index (FSFI) questionnaire to assess the presence of sexual dysfunction. One study employed a self-administered version of the FSFI questionnaire [20], while another study used face-to-face interviews [17].
Regarding the studies presented in Table 1, the highest reported prevalence of sexual dysfunction among obese women was 86% in a study conducted by Yaylali et al. in 2010 in Turkey [18]. In overweight women, the highest prevalence was reported as 57.1% in a study conducted by Silva et al. in 2019 in Brazil [21]. Conversely, the lowest prevalence of sexual dysfunction among obese women was reported as 12.8% in a study conducted by Erenel et al. in 2013 in Turkey [22]. For overweight women, the lowest prevalence was reported as 10.0% in a survey conducted by Karadag et al. in 2014 in Turkey [17].
In the review of 9 studies with a total sample size of 1508 obese women, a high level of heterogeneity was observed according to the I2 heterogeneity test (I2: 97.5). Consequently, the random effects method was employed to analyze the results. Based on the meta-analysis, the prevalence of sexual dysfunction among women with obesity was determined to be 49.7 (95% CI: 35.8–63.5) (Fig. 2). Additionally, a check for publication bias in the included studies was conducted using the Egger, which indicated the absence of publication bias in the studies (p = 0.187) (Fig. 3).

Forest plot of sexual dysfunction in women with obesity based on the random effects model

Funnel plot of the publication bias in the reviewed studies
In the review of 5 studies involving a total sample size of 1411 overweight women, the I2 heterogeneity test revealed a high-level heterogeneity (I2: 96.6). Based on this, the random effects method was used to analyze the results. Based on the meta-analysis, the prevalence of sexual dysfunction among overweight women was 26.9 (95%CI: 13.5–46.5) (Fig. 4). Furthermore, an assessment of publication bias in the included studies was conducted using the Egger test, which indicated the absence of publication bias in the studies (p = 0.120) (Fig. 5).

Forest plot of sexual dysfunction in overweight women based on random effects method

Funnel plot of the publication bias in the reviewed studies
Discussion
This study represents the first systematic review and meta-analysis focusing on the global prevalence of sexual dysfunction in obese and overweight women. To the best of our knowledge, no previous systematic review study has specifically examined this topic globally. The study employed rigorous secondary analysis methods, selecting and analyzing data from 10 high-quality primary studies.
Given that the prevalence of obesity is higher than that of underweight individuals, except in certain regions of sub-Saharan Africa and Asia, the issue of obesity has emerged as a significant social threat in contemporary times [25]. Female sexual dysfunction (FSD) can affect women of all ages and is often a complex issue with multiple contributing factors [26]. Interestingly, there has been relatively more research focusing on the relationship between obesity and sexual function in men to women, and the impact of obesity on women’s sexual lives remains less understood [27, 28].
Esposito et al. conducted a study comparing women with and without FSD, as well as women with Female Sexual Function Index (FSFI) scores of ≥ 23. Their findings revealed that age and BMI were the only factors associated with FSD [29]. Similarly, Kirchengast et al. (1996), in a study without a control group, reported that body weight and subcutaneous fat, particularly in areas such as the chest, waist, and hips, were associated with a decrease in sexual interest among postmenopausal women who were not undergoing hormone therapy [30]. Notably, these results align with the findings of the present study, further highlighting the association between obesity, overweight status and sexual dysfunction in women.
Several studies have provided insights into the relationship between weight loss and sexual function. It has been observed that lifestyle modifications or drug therapies resulting in weight loss of up to 10% are associated with improvements in sex hormone levels and sexual performance [31,32,33]. Another study compared the Female Sexual Function Index (FSFI) scores of 52 women with abnormal names? to those of 66 women in the control group. The study found a significant association between FSFI scores and BMI but not the waist-to-age ratio [34]. Similarly, another study found a negative correlation between BMI and female sexual dysfunction. The researcher suggested that individuals with higher BMI might face difficulties with body positioning during sexual activity, emphasizing the importance of early interventions to reduce BMI in healthcare settings [35].
Contrary to our study findings, one study reported no significant relationship between BMI and the improvement of FSFI scores following non-surgical weight loss interventions for obese women. In contrast, non-surgical weight loss in obese men demonstrated more pronounced improvements in sexual dysfunction [14]. Another study found no statistically significant difference in FSFI scores between obese and control groups. The prevalence of female sexual dysfunction was reported to be 50% and 41% in the obese and control groups, respectively [19]. Elofsson et al. also conducted a study involving a Swedish population that included 840 young women (18% overweight, 6% obese) and 426 older women (32% overweight and 11% obese). Their findings indicated no difference in sexual life satisfaction between obese and normal-weight women, contradicting the results of our study [36].
This meta-analysis had certain limitations that should be acknowledged. Firstly, the number of studies available from different countries was unequal, and the participants’ age distributions varied, which could contribute to the differences in the prevalence of obesity and overweight across countries. Additionally, the inclusion of studies was limited to those published in English, potentially leading to the oversight of studies published in other languages. It is important to consider these limitations when interpreting the findings of this meta-analysis.
Conclusion
The findings of this study reveal the significant prevalence of sexual dysfunction in overweight and obese women. It is crucial to recognize that sexual dysfunction adversely affects the quality of marital relationships and overall life satisfaction for women. Policymakers can use the outcomes of this meta-analysis to emphasize the importance of screening for obesity and overweight among women, as well as raising awareness within society about the detrimental effects of these conditions, including their impact on sexual performance. The results of this research can serve as a valuable research priority and guide interventions aimed at addressing the issue effectively.
Availability of data and materials
Datasets are available through the corresponding author upon reasonable request.
Abbreviations
- WoS:
-
Web of Science
- FSD:
-
Female sexual dysfunction
- BMI:
-
Body Mass Index
References
Abdelaal M, le Roux CW, Docherty NG. Morbidity and mortality associated with obesity. Ann Transl Med. 2017;5(7):161.
Chen C, Xu X, Yan Y. Estimated global overweight and obesity burden in pregnant women based on the panel data model. PLoS ONE. 2018;13(8): e0202183.
Okati-Aliabad H, Ansari-Moghaddam A, Kargar S, Jabbari N. Prevalence of obesity and overweight among adults in the Middle East Countries from 2000 to 2020: a systematic review and meta-analysis. J Obes. 2022;2022:8074837.
Al Kibria GM, Swasey K, Hasan MZ, Sharmeen A, Day B. Prevalence and factors associated with underweight, overweight and obesity among women of reproductive age in India. Global Health Res Pol. 2019;4(1):24.
Meldrum DR, Morris MA, Gambone JC. The obesity pandemic: causes, consequences, and solutions-but do we have the will? Fertil Steril. 2017;107(4):833–9.
World health organization. Obesity and overweight. 2018. Available at: https://www.who.int/news-room/factsheets/detail/obesity-and-overweight. 9 June 2021.
Downs DS, Savage JS, Rivera DE, Pauley AM, Leonard KS, Hohman EE, et al. Adaptive, behavioural intervention impact on weight gain, physical activity, energy intake, and motivational determinants: results of a feasibility trial in pregnant women with overweight/obesity. J Behav Med. 2021;44(5):605–21.
Hunter E, Avenell A, Maheshwari A, Stadler G, Best D. The effectiveness of weight-loss lifestyle interventions for improving fertility in women and men with overweight or obesity and infertility: A systematic review update of evidence from randomized controlled trials. Obes Rev. 2021;22(12): e13325.
Yoldemir T, Garibova N, Atasayan K. The association between sexual dysfunction and metabolic syndrome among Turkish postmenopausal women. Climacteric. 2019;22(5):472–7.
Sarwer DB, Hanson AJ, Voeller J, Steffen K. Obesity and sexual functioning. Curr Obes Rep. 2018;7(4):301–7.
Kim JI, Zhu D, Davila J, Lee J, Chubak BM, Melamed ML, et al. Female sexual dysfunction as measured by low sexual frequency is associated with lower socioeconomic status: an analysis of the National Health and Nutrition Examination Survey (NHANES), 2007–2016. J Sex Med. 2022;19(1):90–7.
Oksuz E, Malhan S. Prevalence and risk factors for female sexual dysfunction in Turkish women. J Urol. 2006;175(2):654–8.
Di Francesco S, Caruso M, Robuffo I, Militello A, Toniato E. The impact of metabolic syndrome and its components on female sexual dysfunction: a narrative mini-review. Curr Urol. 2018;12(2):57–63.
Loh HH, Shahar MA, Loh HS, Yee A. Female sexual dysfunction after bariatric surgery in women with obesity: A systematic review and meta-analysis. Scand J Surg. 2022;111(1):14574969211072396.
Shorub EM, Hussein H, El-Shafei A. Female sexual dysfunction and body image dissatisfaction in Egyptian obese patients. Middle East Curr Psychiatry. 2016;23(2):106–11.
Abu Ali RM, Al Hajeri RM, Khader YS, Ajlouni KM. Factors associated with sexual dysfunction in Jordanian women and their sexual attitudes. Ann Saudi Med. 2009;29(4):270–4.
Karadag H, Oner O, Karaoglan A, Orsel S, Demir AU, Firat H, et al. Body mass index and sexual dysfunction in males and females in a population study. Klin Psikofarmakol Bul. 2014;24(1):76–83.
Yaylali GF, Tekekoglu S, Akin F. Sexual dysfunction in obese and overweight women. Int J Impot Res. 2010;22(4):220–6.
Kadioglu P, Yetkin DO, Sanli O, Yalin AS, Onem K, Kadioglu A. Obesity might not be a risk factor for female sexual dysfunction. BJU Int. 2010;106(9):1357–61.
Mostafa AM, Khamis Y, Helmy HK, Arafa AE, Abbas AM. Prevalence and patterns of female sexual dysfunction among overweight and obese premenopausal women in Upper Egypt; a cross-sectional study. Middle East Fertil Soc J. 2018;23(1):68–71.
Silva G, Lima S, Reis BFD, Macruz CF, Postigo S. Evaluation of Obesity Influence in the Sexual Function of Postmenopausal Women: A Cross-Sectional Study. Rev Bras Ginecol Obstet. 2019;41(11):660–7.
Erenel AS, Kilinc FN. Does obesity increase sexual dysfunction in women? Sex Disabil. 2013;31(1):53–62.
Aba YA, Avcı D, Ozdilek R, Alp Yılmaz F, Acar BH. Prevalence of SEXUAL DYSFUNCTION IN WOMEN WITH OBESITY AND ASSOCIATED FACTORs. Sex Disabil. 2021;39(3):543–54.
Senobari M, Azmoude E, Mousavi M. The relationship between body mass index, body image, and sexual function: A survey on Iranian pregnant women. Int J Reprod Biomed. 2019;17(7):505–14.
Shodieva NU. Main risk factors for overweight and obesity in young people. Eurasian Medical Research Periodical. 2022;7:141–6.
Sood R, Kuhle CL, Thielen JM, Kapoor E, Vencill JA, Mara KC, et al. Association of mindfulness with female sexual dysfunction. Maturitas. 2022;161:27–32.
Mulhall J, Teloken P, Brock G, Kim E. Obesity, dyslipidemias and erectile dysfunction: a report of a subcommittee of the sexual medicine society of North America. J Sex Med. 2006;3(5):778–86.
Derby CA, Mohr BA, Goldstein I, Feldman HA, Johannes CB, McKinlay JB. Modifiable risk factors and erectile dysfunction: can lifestyle changes modify risk? Urology. 2000;56(2):302–6.
Esposito K, Ciotola M, Marfella R, Di Tommaso D, Cobellis L, Giugliano D. The metabolic syndrome: a cause of sexual dysfunction in women. Int J Impot Res. 2005;17(3):224–6.
Kirchengast S, Hartmann B, Gruber D, Huber J. Decreased sexual interest, and its relationship to body build in postmenopausal women. Maturitas. 1996;23(1):63–71.
Cabler S, Agarwal A, Flint M, du Plessis SS. Obesity: modern man’s fertility nemesis. Asian J Androl. 2010;12(4):480–9.
Brewer CJ, Balen AH. The adverse effects of obesity on conception and implantation. Reproduction. 2010;140(3):347–64.
Gosman GG, Katcher HI, Legro RS. Obesity and the role of gut and adipose hormones in female reproduction. Hum Reprod Update. 2006;12(5):585–601.
Esposito K, Ciotola M, Giugliano F, Bisogni C, Schisano B, Autorino R, et al. Association of body weight with sexual function in women. Int J Impotence Res. 2007;19(4):353–7.
Yilmaz H, Polat HA, Yilmaz SD, Erkin G, Kucuksen S, Salli A, et al. Evaluation of sexual dysfunction in women with rheumatoid arthritis: a controlled study. J Sex Med. 2012;9(10):2664–70.
Adolfsson B, Elofsson S, Rössner S, Undén AL. Are sexual dissatisfaction and sexual abuse associated with obesity? A population-based. Study Obes Res. 2004;12(10):1702–9.
Acknowledgements
The authors would like to thank the Student Research Committee of Kermanshah University of Medical Sciences.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
NS and RH and MM contributed to the design, MM statistical analysis, participated in most of the study steps. MM and RH and TS prepared the manuscript. HZ and SHSH and MM assisted in designing the study, and helped in the, interpretation of the study. All authors have read and approved the content of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Salari, N., Hasheminezhad, R., Sedighi, T. et al. The global prevalence of sexual dysfunction in obese and overweight women: a systematic review and meta-analysis. BMC Women's Health 23, 375 (2023). https://doi.org/10.1186/s12905-023-02544-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12905-023-02544-4