
Abstract
Background
Globally, Human Immunodeficiency Virus (HIV) is the leading cause of death in women of reproductive age and accountable for a quarter of deaths during pregnancy in sub-Saharan Africa including Ethiopia. Introduction of antiretroviral therapy to women living with HIV highly improves lifestyle and the desire to have children. A comprehensive understanding of baseline predictors of pregnancy among women receiving ART essential to reduces unintended pregnancies, appropriate care, and preventing transmission from mother to child.
Objective
To determine the effect of baseline predictors on incidence rate of pregnancy among reproductive age women on antiretroviral therapy at public hospitals of Jigjiga and Harar town, Eastern Ethiopia from February 15 to march 15, 2020.
Methods
Retrospective cohort study was conducted on randomly selected 420 HIV-infected women using data recorded from September 11, 2014, to September 10, 2019 in Jigjiga and Harar town in Eastern Ethiopia. Simple random sampling was used to select study subjects from each hospital. Data were entered to Epi data version 3.2 and exported to Stata version 14.2 for analysis. Kaplan–Meier failure, and Cox proportional hazards model were used to estimate the incidence, and to identify predictors of pregnancy respectively. Variables which were significant (P value < 0.05) in the multivariate analysis were considered independent predictors of pregnancy.
Results
The overall incidence rate of pregnancy was 9.1 per 100 person-years (95% CI 7.19, 11.76). Being unadvanced HIV disease stage (AHR: 2.50; 95% CI 1.46, 4.19), having less than two children (AHR: 2.93; 95% CI 1.59, 5.40), and disclosed HIV status (AHR: 2.25; 95% CI 1.34, 3.79) were independent predictors of pregnancy.
Conclusion
The incidence rate of pregnancy among reproductive age women on ART was found to be considerable. Being unadvanced HIV disease stage, having less than two children, and disclosed HIV status were independent predictors of pregnancy. Thus, tailoring counseling have to be designed to enhance better pregnancy planning and consecutive health outcomes.
Similar content being viewed by others

Introduction
The Human Immunodeficiency Virus/Acquired Immunodeficiency Syndrome (HIV/AIDS) remains a serious public health challenge, as well as a social dilemma especially among women of reproductive age [1]. In 2018, around 18.8 million women of reproductive age globally, living with HIV [2]. Of these, 61% were residing in sub-Saharan Africa [2]. In Ethiopia, the prevalence of HIV/AIDS among women of reproductive age was 1.2% and the prevalence increases with increasing women’s age [3].
Introduction of antiretroviral therapy to women living with HIV highly improves lifestyle and the desire to have children [4]. Women who have HIV should seek treatment in accordance with WHO treatment guidelines because the virus can be passed on to their babies during pregnancy, childbirth, and breastfeeding [4]. Despite the fact that providing antiretroviral treatment to women living with HIV/AIDS has a tremendous effect on a mother's health and can virtually eliminate the risk of passing on the virus to a newborn, a birth from an HIV positive mother may result not only in an HIV positive baby but also in maternal death [5]. If proper care for the mothers is not in place, maternal death due to complications related to HIV and pregnancy can be very high [6]. Reports have shown that even in the presence of ART maternal mortality rates have been reported to be five times higher in HIV infected women than in uninfected women [7], and it is responsible for at least 20% of all deaths, a figure that is higher than any direct obstetric cause [8]. In Ethiopia, pregnancy related complications among women on ART are among the many health problems. Even if the country is constructing and equipping health facilities with staff and equipment, still morbidity and mortality due to complications related to pregnancy among women on ART are very high [9].
Evidence indicates that HIV-positive women continue to desire more children in the future, though to differing degrees in different contexts. According to studies from Canada and Tanzania, 69% and 37% of HIV-positive mothers want to have more children, respectively [10, 11]. Various studies in Ethiopia have found varying levels of fertility desire among HIV-positive women. According to research conducted in North Wollo [12], Addis Ababa [13], and Tigray region [14], the majority of HIV positive women desired to have more children.
Successful translation of HIV-prevention strategies requires a comprehensive understanding of the magnitude and baseline predictors of pregnancy among HIV positive women. This knowledge essential to reduce unintended pregnancies, appropriate care, and preventing transmission from mother to child. Therefore, this study aimed to determine effect of baseline predictors on incidence rate of pregnancy among reproductive age women receiving antiretroviral therapy at public hospitals of Jigjiga and Harar town, Eastern Ethiopia.
Methods
Study setting and period
This study was conducted at public hospitals of Jigjiga and Harar town, Eastern Ethiopia: Four hospitals, namely; Karamara general hospital, Sheikh Hassan Yabare Jigjiga university referral hospital (SHY-JURH), Hiwot Fana specialized university hospital, and Jugol hospital were included in the study conducted from February 15 to March 15, 2020.
Karamara general hospital and Sheikh Hassan Yabare Jigjiga university referral hospitals are located in Jigjiga town. Jigjiga, the administrative capital of the Somali region, is located 628 km east of Ethiopia's capital, Addis Ababa. Five governmental health institutions (3 health centers and 2 Hospitals) provide ART service for the catchment area population. Karamara general hospital and SHY-JURH are selected for the study. Karamara general hospital has been providing ART services for more than 17 years. As of 2020, 2907 and 179 HIV/AIDS patients have utilized ART services at the Karamara general hospital and SHY-JURH respectively, of whom 781 and 105 are reproductive age women, were on ART [15].
Hiwot Fana specialized Haramaya university hospital and Jugol hospitals are located in Harar town, 525 km from Ethiopia's capital, Addis Ababa. Hiwot Fana specialized Haramaya university hospital is the region's high load hospital, treating more than 50% of HIV patients. Both hospitals have been providing ART services for more than 18 years, and as of 2020, 1179 and 259 women of reproductive age are receiving ART at the two hospitals, respectively [15].
Study design
Retrospective cohort study was used.
Source population
The source population was all women on ART at public hospitals of Jigjiga and Harar town.
Study population
The study population was all reproductive age women who received antiretroviral treatment at public hospitals of Jigjiga and Harar town, between September 11, 2014, to September 10, 2019.
Inclusion and exclusion criteria
Inclusion criteria
All reproductive age women, who were getting antiretroviral treatment in the hospitals of Jigjiga and Harar town, between September 11, 2014, to September 10, 2019 were included in the study.
Exclusion criteria
Women who were getting pre-ART care and started ART based on option B+. Women with incomplete data on exposure and outcome were excluded from the study.
Sample size determination
Objective one: The required sample size for objective one was determined by using formula for event, based on the following assumptions: the significance level of 5%, 80% power, hazard ratio = 2.05, and π1 and π2 are the proportions to be allocated to group1 and 2 and for equal allocation π1 = π2 = \(\frac{1}{2}\). The incidence rate of pregnancy = 4.92 per 100 person years that converted to five years gives 0.246 person years in the study conducted in northwest Ethiopia [9].
-
Event (Pregnancy) = 4(Zα/2 + Zβ)2)/ (lnHR)2) = 60 [16]
-
Where Zα/2 and Zβ are standard percentiles which give 1.96 (95% CI) and 0.84 (80%)
-
n = Pregnancy/Pr (Pregnancy), Pr is the probability of Pregnancy and it is calculated by
-
Pr (Pregnancy) = 1-(π1 S1(T) + π2 S2(T)) = 1-\(\frac{1}{2}\) (S1(T) + S2(T)) where S(T) = exp(-λt), IR = λt
-
and S1 (t5) = exp(-0.246) = 0.782, S2(t5) = exp(-0.246 *HR) = 0.604
-
Pr (Pregnancy) = 1-(π1 S1 (T) + π2 S2 (T)) = 1- \(\frac{1}{2}\) (0.782 + 0.604) = 0.307
-
n = Pregnancy/Pr (Pregnancy) = \(\frac{60}{0.307}\) = 195 (adding 10% for incomplete data) = 215
Objective two: Sample size for specific objective two was calculated using stpower Cox in Stata version 14.2 software packages. The estimation was based on assumptions with the power of 80%, α (type I) error of 5%, and the hazard ratio of 2.3 for educational status of patients with unable to read & write vs. formal education [9]. By considering, 10% for incomplete data during follow up period and in adjusting for censoring taking the overall probability of event 0.12 with 1:1 allocation ratio, and 0.5 of standard deviation. By having all the above parameters, the Stata command estimated sample sizes for the second specific objective was 420.
Finally, sample size for first and second objectives was compared, and the larger of two sample sizes was used to determine a minimum required sample size. Thus, the sample size for objective two 420 was selected as final sample size for the study.
Sampling procedure
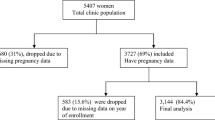
Four public hospitals from Jigjiga and Harar city were included. Cards of 1168 women living with HIV from September 11, 2014, to September 10, 2019, was reviewed according to the date of ART initiation. Due to eligibility criteria, 105 patient cards were excluded, and 1063 patients were eligible for study. Eligible cards were from Karamara general hospital (37.6%), SHY-JURH (11%), Hiwot Fana specialized Haramaya university hospital (36.2%), and Jugol hospital (15.2%). Finally, each hospital's study subjects were selected using proportional allocation followed by simple random sampling (Fig. 1).

Schematic presentation of sampling procedure on the effect of predictors on incidence rate of pregnancy among reproductive age women on antiretroviral therapy at public hospitals of Jigjiga and Harar town, Eastern Ethiopia. KGH: Karamara general hospital; SRS: simple random sampling; SHYJURH: Sheikh Hassan Yabare Jigjiga university referral hospital; HFSUH: Hiwot Fana Specialized Haramaya university hospital; JH: Jugol hospital
Data collection tools and procedure
A structured data collection checklist was prepared in English to extract data from the records. Data was extracted from the hospital's main excel record. Data elements which were not included in the excel sheet were collected from ART intake forms and cards. The most recent laboratory results before starting ART were used as a baseline. If there were no pre-treatment laboratory tests, results obtained within one month of ART initiation were used as baseline. The data was extracted by eight nurses who work in ART clinics and supervised by two experienced BSc nurses. The patients̕ date of pregnancy was extracted from ART follow up registration form.
Variables
Dependent variable
Time to pregnancy in months.
Independent variables
Socio-demographic factors: Age, Place of residence, marital status, educational status, main occupation, number of children, and religion.
Clinical, laboratory, and treatment related factors: WHO clinical stages, CD4 count level, BMI, functional status, hemoglobin level, ARVs medication adherence, ART regimen given, opportunistic infection, cotrimoxazole prophylactic status, and disclosure of HIV status.
Operational definitions
Incidence of Pregnancy: Incidence of pregnancy was considered as the first pregnancy after ART enrollment within the follow-up time [9].
Time scale: The time to event was calculated in months using the time between the dates of treatment initiation and the date of the event (pregnancy) or date of censoring. Thus, the minimum and the maximum follow up were 6 months and 60 months respectively.
Censored: If the exact time at which the event occurs is not observed, or if their last visit is any one of the following events; if lost to follow-up, transferred to another health facility, dead, and if not pregnant at the end of follow up [9].
Lost to follow up: A patient who has not attended the ART clinic for more than 90 days since the last scheduled appointment and whose whereabouts are unknown to the ART clinic staff [17].
Transferred-out: If the patients have moved to another health facility with confirmed written documentation of transfer out [17].
Not pregnant: If the patient does not experience the events at the end of the study.
WHO clinical stages (See Additional file 1).
Advanced HIV disease stage: Advanced HIV disease stage for adults is defined as having WHO clinical stage III or IV events [18].
Unadvanced HIV disease stage: Unadvanced HIV disease stage for adults is defined as having WHO clinical stage I or II events [18].
Data quality control
Data quality was ensured during data collection, coding, entry, cleaning, and analysis. The data collectors and the supervisor were trained on the data collection procedures for two days and supervisor supervised the data collection process. The principal investigator oversaw the overall process. Completeness of data was checked in each day of activity and the necessary feedback was offered to data collectors the next morning. Moreover, double data entry was performed to prevent data entry error.
Method of data analysis
Following the accomplishment of data collection activities, the data were entered to Epi data version 3.2 and exported to Stata version 14 for analysis. Mean with standard deviation, and median with inter quartile range for continuous variables, and frequencies with percentage for categorical variables were computed to describe a baseline characteristic of the participants. Incidence rate of pregnancy was determined from date of ART initiation to date of pregnancy recorded. The cumulative probability of pregnancy at every twelve months was estimated using Life table. Kaplan–Meier failure was used to estimate the probability of pregnancy after ART initiation. Crude hazard ratio test was carried out to identify candidate variables for the multivariable Cox regression model at P value < 0.25. Cox proportional hazards model was used to identify predictors of pregnancy and Variables which were significant (P value < 0.05) in the multivariate analysis were considered as independent predictors of pregnancy.
Results
Socio-demographic characteristics of the participants
A total of 420 HIV positive women from the record reviews were analyzed having a mean age of 31 (± 7 SD) years. About half; 232(55.2%) of the study subject were orthodox. About two-third of the study subject were urban by residence, less than two children by number of children with a magnitude of 329(78.3%), and 277(66.0%), respectively. Nearly half; of the study subjects were married and have no formal education with a magnitude of 192(45.7%), and 185(44.0%), respectively. About 155(36.9%) of study subjects were jobless (Table 1).
Clinical, Laboratory, and Treatment related characteristics
In terms of baseline clinical and laboratory characteristics, about 90% of patients, 381 (90.7 percent), had begun ART with TDF + 3TC + EFV. About two-thirds of the study subjects were working by functional status, and good by ARVs medication adherence with a magnitude of 314(74.8%), and 333(79.3%), respectively. The median Hemoglobin level and CD4 cell counts of the study subjects was 11.5(4.5), and 223(258) respectively. Furthermore, the average body mass index (BMI) of the study subjects was 19.7 (3.6) kg/m2. Above half of the study subjects were yes by OIs and cotrimoxazole Prophylaxis status, and disclosed by HIV disclosure status with a magnitude of 238(56.7%), 244(58.1%), and 250(59.5%), respectively (Table 2).
Incidence rate of pregnancy among HIV-infected women on ART care
In this study, there were 72 pregnancies, with the majority of them (69.4%) occurring in the first year of ART initiation. All of the study subjects (420) had contributed 9440 person month’s observations. The overall incidence rate of pregnancy was 9.1 per 100 person-years (95% CI 7.19, 11.76). The incidence rate of pregnancy in the entire cohort was 1.23, 0.59, 0.25, 0.33, and 0.000 per 100 person-year at 12, 24, 36, 48, and 60 months of ART initiation, respectively, indicating that as the year of follow up increases, the incidence rate of pregnancy decreases (Table 3). The Kaplan Meier failure curve depicts the probabilities of becoming pregnant at 20, 40, and 60 months of follow up, with the probability increasing over time (Fig. 2).

Kaplan–Meier failure curve estimate overall risk of having pregnancy among reproductive age women on ART at public hospital of Jigjiga and Harar town, 2020. From September 11, 2014 to September 10, 2019
Predictors of Pregnancy among HIV-infected women on ART care
In crude analysis; Age, Marital status, Level of education, Functional status, Number of children, BMI, Disease stage, Hemoglobin level, CD4 count level, OIs, ARVs medication adherence, Cotrimoxazole Prophylaxis, and disclosure of HIV status were variable candidate for multivariable Cox regression at P value < 0.25. Hence, place of residence was not included (Table 4).
In multivariable Cox regression analysis, women with unadvanced HIV disease stage at baseline has increased risk of pregnancy by more than two-fold (AHR: 2.50; 95% CI 1.46, 4.19) compared to women with advanced HIV disease stage, after adjusting the number of children, and disclosure of HIV status. The risk of pregnancy was almost three (AHR: 2.93; 95% CI 1.59, 5.40) times higher among mothers who had less than two children compared to those who had two and above children. Women who had disclosed their HIV status was increase the risk of pregnancy by two folds (AHR: 2.25; 95% CI 1.34, 3.79) when compared to Women who had not disclosed their HIV status (Table 5).
Discussion
The overall incidence of pregnancy was 9.1 per 100 person-years. Being unadvanced HIV disease stage, having less than two children, and disclosed HIV status were independent predictors of pregnancy.
The incidence of pregnancy was 9.1 per 100 person-years in the entire follow up period. This finding is consistent with research conducted in western Uganda (90.7/1000 person-years) [19], Uganda (9.4/100 person-years) [20], and sub-Saharan Africa (9/100 person-years) [21].
This finding is lower than the studies done in Tanzania (12/100 person-years) [22], and Uganda (24.6/100 person-years) [23]. This disparity could be attributed to differences in access and quality of services, as well as differences in pregnancy diagnosis criteria. This result is also lower than that of a prospective population-based cohort study conducted in eastern Ethiopia [24], in which the incidence of pregnancy was 22.7/100 person-years. This difference could be explained by the fact that in Assefa et al.'s prospective cohort study, the study subjects were free HIV/AIDS people, whereas in this study, the study subjects were women with HIV/AIDS.
This finding is higher than that of studies conducted in London (13/1000 person-years) [25], Korea (3.57/100 person-years) [26], Canada (2.91/100 person-years) [27], Eight west African countries (2.9/100 person-years), Burkina Faso (5/100 person-years) [28], and studies from Ethiopia: Addis Ababa (6.5/100 person-years) [29], and Debre Markos (4.92/100 person-years) [9]. This difference may be due to differences in; inclusion and exclusion criteria, the size of records reviewed, the study period, and difference in baseline exposure to ART.
Being unadvanced HIV disease stage at the time of ART initiation has increased risk of pregnancy by more than two-fold, after controlling potential baseline confounders. This finding is in line with the findings of the studies conducted in eight west African countries and Ethiopia [29, 30]. Women with advanced HIV disease stage were less likely to be pregnant compared with unadvanced stage. This could be because being in advanced HIV disease stage leads to decreased general health and well-being, which may be associated with decreased sexual activity. Being unadvanced, on the other hand, implies good health and a lower risk of complications, which probably influences both the fertility and the fertility desire.
Women with fewer than two children were nearly three times more likely to become pregnant than women with two or more children. This finding is consistent with the findings of an Ethiopian studies [9, 29]. Women who had less than two children might have high fertility desire compared to those having two or more children. This might be due to the fact that, women who had two or more children more likely to utilize family planning services.
Women who had disclosed their HIV status had a twofold increase in the risk of pregnancy when compared to women who had not disclosed their HIV status. This finding is in line with the finding of a studies done in Uganda [20], and Ethiopia [31]. Communication between partners may play an important role in pre-conception planning behaviors. Additionally, disclosing an HIV-positive status to a sexual partner leads to safer sexual practices, social and emotional, and financial supports, which probably increase their fertility desire.
Strength and limitations
This is one of the few studies in Ethiopia that explored effect of predictors on incidence rate of pregnancy among HIV infected women in ART era. Since this study was time to event analysis it enables us to consider contribution of censored study subjects. Due to a large number of missing data points, interesting variables such as family planning use, fertility desire, and intended and unintended pregnancies were not included. Thus, this finding should be interpreted with this limitation in mind.
Conclusion and recommendation
The incidence of pregnancy among reproductive age women on ART is found to be considerable. Being unadvanced HIV disease stage, having fewer than two children, and disclosing HIV status were all independent predictors of pregnancy. Thus, tailoring counseling has to be designed to improve pregnancy planning and subsequent health outcomes. Beside this, health officers and data clerks working with recording HIV-positive patient’s data either in chart or database need training to improve quality of medical data especially in keeping dataset from missingness.
Availability of data and materials
Almost all data are included in this study. However, additional data will be available from the corresponding author upon reasonable request.
References
Cooper D, Harries J, Myer L, Orner P, Bracken H. “Life is still going on”: reproductive intentions among HIV-positive women and men in South Africa. Soc Sci Med. 2007;65:274–83.
UNAIDS. Global AIDS Update 2018. Geneva, Switzerland. Available from: https://www.unaids.org/en/resources/documents/2018/Global-AIDSupdate-2018. Accessed Nov13, 2019. 2018 Report No.
EDHS. Ethiopia Demographic and Health Survey. HIV prevalence report. Central Statistical Authority. 2016.
Litwin LE, Makumbi FE, Gray R, Wawer M, Kigozi G, Kagaayi J, et al. Impact of availability and use of ART/PMTCT services on fertility desires of previously pregnant women in Rakai, Uganda: a retrospective cohort study. J Acquired Immune Deficiency Syndrom (1999). 2015;69(3):377.
Marston M, Nakiyingi-Miiro J, Hosegood V, Lutalo T, Mtenga B, Zaba B. Measuring the Impact of antiretroviral therapy roll-out on population level fertility in three African countries. 2016.
Reynolds H, Janowitz B, Wilcher R, Cates W. Contraception to prevent HIV-positive births: current contribution and potential cost savings in PEPFAR countries. Sex Transm Infect. 2008;84:49–53.
Gray GE, McIntyre JA. HIV and pregnancy. BMJ. 2007;334(7600):950–3.
Lathrop E, Jamieson DJ, Danel I. HIV and maternal mortality. Int J Gynecol Obstet. 2014;127(2):213–5.
Meseret M, Shimeka A, Bekele A. Incidence and predictors of pregnancy among women on ART in Debre Markos Referral Hospital, Northwest Ethiopia: a five-year retrospective cohort study. AIDS Res Treat. 2017;2017.
Loutfy M, Hart T. A., Mohammed SS. Fertility desires and intentions of HIV-positive women of reproductive age in Ontario, Canada: a cross-sectional study. PLoS ONE 4(12), article e7925 (2009).
Mmbaga EJ, Leyna GH, Ezekiel MJ, Kakoko DC. Fertility desire and intention of people living with HIV/AIDS in Tanzania: a call for restructuring care and treatment services. BMC Public Health. 2013;13(1):86.
Getachew M, Alemseged F, Abera M, Deribew A. Factors affecting fertility decisions of married men and women living with HIV in South Wollo Zone, Northeast Ethiopia. Ethiopian J Health Dev. 2010;24(3):204–20.
Asfaw HM, Gashe FE. Fertility intentions among HIV positive women aged 18–49 years in Addis Ababa Ethiopia: a cross sectional study. Reprod Health. 2014;11(1):36.
Melaku YA, Zeleke EG. Contraceptive utilization and associated factors among HIV positive women on chronic follow up care in Tigray Region, Northern Ethiopia: a cross sectional study. PLoS ONE. 2014;9(4): e94682.
HMIS HJ. HMIS Annual report. 2019.
Collett D. Modelling survival data in medical research third edition. 2013.
Seifu W, Ali W, Meresa B. Predictors of loss to follow up among adult clients attending antiretroviral treatment at Karamara general hospital, Jigjiga town, Eastern Ethiopia, 2015: a retrospective cohort study. BMC Infect Dis. 2018;18(1):280.
WHO. Guidelines for managing advanced HIV disease and rapid initiation of antiretroviral therapy. Geneva, Switzerland. Available at: http://www.who.int/hiv/pub/toolkits/advanced-HIV-disease-policy/en/. Accessed 25 December, 2019. 2017.
Kabami J, Turyakira E, Biraro S, Bajunirwe F. Increasing incidence of pregnancy among women receiving HIV care and treatment at a large urban facility in western Uganda. Reprod Health. 2014;11(1):81.
Kaida A, Matthews LT, Kanters S, Kabakyenga J, Muzoora C, Mocello AR, et al. Incidence and predictors of pregnancy among a cohort of HIV-positive women initiating antiretroviral therapy in Mbarara, Uganda. PLoS ONE. 2013;8(5):e63411.
Myer L, Carter RJ, Katyal M, Toro P, El-Sadr WM, Abrams EJ. Impact of antiretroviral therapy on incidence of pregnancy among HIV-infected women in Sub-Saharan Africa: a cohort study. PLoS Med. 2010;7(2):e1000229.
Odutola A, Baisley K, Hayes RJ, Rusizoka M, Tanton C, Weiss HA, et al. Pregnancy and contraceptive use among women participating in an HIV prevention trial in Tanzania. Sex Transm Infect. 2012;88(6):436–43.
Fredrick E, Makumbi, Gertrude N, J. S, Reynolds, Anthony N, et al. Associations between HIV antiretroviral therapy and the prevalence and incidence of pregnancy in Rakai, Uganda. 2010.
Assefa N, Berhane Y, Worku A. Pregnancy rates and pregnancy loss in Eastern Ethiopia. 2013.
Byrne L, Sconza R, Foster C, Tookey PA, Cortina-Borja M, Thorne C. Pregnancy incidence and outcomes in women with perinatal HIV infection. AIDS (London, England). 2017;31(12):1745.
Choi H, Kim MH, Lee SJ, Kim EJ, Lee W, Jeong W, et al. Pregnancy rates and outcomes of HIV-infected women in Korea. J Korean Med Sci. 2018;33(47):e296.
Salters K, Loutfy M, de Pokomandy A, Money D, Pick N, Wang L, et al. Pregnancy incidence and intention after HIV diagnosis among women living with HIV in Canada. PLoS ONE. 2017;12(7):e0180524.
Poda A, Hema A, Konaté A, Kaboré F, Zoungrana J, Kamboulé E, et al. Pregnancy rate and birth outcomes among women receiving antiretroviral therapy in Burkina Faso: a retrospective cohort study. Pan Afr Med J. 2016;23(1):105.
Degife M, Degu G, Molla M. Assessment of incidence and predictors of pregnancy among patients on antiretroviral therapy (ART) and pre-ART: a retrospective cohort study. Lancet. 2013;381:S34.
Burgos-Soto J, Balestre E, Minga A, Ajayi S, Sawadogo A, Zannou MD, et al. Incidence of pregnancy following antiretroviral therapy initiation and associated factors in eight West African countries. J Acquired Immune Deficiency Syndrom (1999). 2014;67(2):e45.
Melaku YA, Zeleke EG, Kinsman J, Abraha AK. Fertility desire among HIV-positive women in Tigray region, Ethiopia: implications for the provision of reproductive health and prevention of mother-to-child HIV transmission services. BMC Womens Health. 2014;14(1):137.
Acknowledgements
The authors are pleased to acknowledge the study participants who participated in this work and Haramaya University and its staff for their support throughout this study by providing all necessary materials and technical support. The authors are grateful to Karamara general hospital, Sheikh Hassan Yabare Jigjiga university referral hospital (SHY-JURH), Hiwot Fana specialized university hospital, and Jugol hospital for overall guidance and support. Special thanks to Dr. Tariku Dingeta (Haramaya University) to his immense support and advice.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship: This work was supported by Jigjiga University.
Author information
Authors and Affiliations
Contributions
AW conceived the idea, collected the data, and played a major role in this research. The authors (AW, LO, WG, and GD) contributed to data analysis, writing, and editing the document. AW, LO, WG, and GD gave valuable ideas for the manuscript and revised it. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical clearance was obtained from Institutional Health Research Ethics Review Committee (IHRERC) of Haramaya University College of health and medical sciences (Reference number: IHRERC/029/2020). Following the approval, official letter of cooperation was written to public hospitals of Jigjiga and Harar town. An official support letter was obtained from the medical directors of the Karamara general hospital, SHY-JURH, Hiwot Fana specialized Haramaya university hospital, and Jugol hospital, and the ART departments as well. Written informed consent from study participants were not feasible. Since this was analysis of secondary data retrieved from the patient cards/database, participant consent was waved by Institutional Health Research Ethics Review Committee (IHRERC) of Haramaya University College of health and medical sciences. All experimental protocols were approved by the ethics committee stated above. Each hospital’s management and ethics committee also judged the project as health research with no ethical risk. Besides, no personal identifiers were used on the data collection form. The authors confirm that all methods were performed in accordance with the relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors declares that there is no competing interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1
. WHO clinical stage of HIV and detailed description of clinical stages.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wariyo, A., Oljira, L., Golicha, W. et al. Effect of predictors on incidence rate of pregnancy among reproductive age women on antiretroviral therapy at public hospitals of Jigjiga and Harar Towns, Eastern Ethiopia: a retrospective cohort study. BMC Women's Health 22, 548 (2022). https://doi.org/10.1186/s12905-022-02135-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12905-022-02135-9