
Abstract
Background
Non-pharmacological interventions are the first line of Gestational diabetes mellitus (GDM) management. Community-based interventions are cheaper, more accessible, with higher patient satisfaction.
Objectives
To systematically review community-based non-pharmacological interventions and evaluate their effectiveness for GDM.
Search strategy
Twelve bibliographic databases and reference list of related studies from inception until January 2022.
Selection criteria
All primary studies of community-based non-pharmacological interventions for GDM reported in English which investigated any behavioural or clinical outcome(s).
Data collection and analysis
Data were extracted using modified Cochrane’s data extraction template. Studies were evaluated using Cochrane Collaboration’s risk of bias tool. Narrative synthesis was used to summarise findings. This study is registered with PROSPERO (CRD42021257634).
Main results
Twenty-seven studies involving 6,242 pregnant women with GDM investigated self-management programmes, medical nutrition/diet therapy, exercise/physical activity, combined diet and exercise, calcium plus vitamin D supplementation, and continuous glucose monitoring. Self-management programmes were more effective than routine care in improving self-efficacy, two-hour postprandial blood glucose, and lifestyle behaviours but were as effective as routine care in improving infant birth weight. Self-management programmes were superior to or as effective as usual care in improving fasting blood glucose, blood glucose control, glycated haemoglobin, macrosomia, and preterm delivery. Medical nutrition/diet therapy was more effective than usual care in improving postprandial blood glucose levels. Postprandial blood glucose levels were better improved by regular supervised exercise plus daily brisk walks or a daily walking intervention than routine obstetric care or no treatment. The effects of exercise/physical activity programmes were mostly inconsistent for other outcomes. Diet and exercise were superior to diet alone in reducing maternal weight gain although there were similar outcomes for other pregnancy and foetal outcomes. Limited or conflicting evidence was found for other outcomes and interventions including calcium and vitamin D supplementation and continuous glucose monitoring intervention.
Conclusions
Community-based non-pharmacological interventions are more effective than placebo; and are more or as effective as usual care. Self-management programmes and medical nutrition/diet therapy had the most promising GDM outcomes.
Funding
There was no funding for this study. The study design, data collection, data analysis and interpretation, and writing of this manuscript were not influenced externally by any funder.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Introduction
Gestational diabetes mellitus (GDM) is diagnosed by the detection of hyperglycaemia during pregnancy. This can convert a natural process to one fraught with increased risk for foetal and maternal mortality and morbidity, an increased need for surveillance, increased emotional distress, and reduced quality of life [1, 2]. Five percent of women develop type 2 diabetes within 10 years following first onset of GDM [3,4,5]. The prevalence of GDM is 1% – 30% globally. The burden is greatest in the Middle East and some North African countries (8.8–20.0%), followed by South- East Asia (9.6–18.3%), the Western Pacific (4.5–20.3%), South and Central America (7.1–16.6%), sub-Saharan Africa (8.5–13.1%) and North America and the Caribbean (6.5–11.9%). The lowest burden of GDM is found in Europe, and this region also has the widest variation in prevalence (1.8–31.0%) [2, 6].
GDM results from carbohydrate intolerance or hyperglycemia with first onset occurring in a present pregnancy. Most GDM are detected in late second trimester (13–26 completed weeks of gestation) or early in the third trimester (27–40 weeks). It appears that women who developed GDM in late gestation had decreased peripheral insulin sensitivity (insulin sensitivity – ability of insulin to increase glucose uptake in skeletal muscle and adipose tissues) even before conception. There is defect in the pancreatic β- cell function such that as pregnancy progresses, insulin resistance increases, the insulin response subsequently becomes inadequate resulting in hyperglycaemia. Inflammation, which has been linked to obesity, is also important in the pathophysiology of GDM as it disrupts insulin signaling. Pancreatic β- cell dysfunction can progress after the first GDM pregnancy and appear to be linked with retention of excessive gestational weight gain and increases in insulin resistance. Decreased insulin sensitivity affect maternal amino acid and lipid metabolism, which increases foetal growth and adiposity, and this can be associated with complications during delivery. Other complications in the offspring include congenital malformations, shoulder dystocia, respiratory distress syndrome, neonatal hypoglycemia, hyperbilirubinaemia, and hypocalcaemia [2, 7, 8].
Risk factors for GDM include body mass index (BMI) greater than 25kg/m2, advanced maternal age, non-white ancestry, family history of type 2 diabetes mellitus, previous history of GDM, parity, male foetus, multiple pregnancy, genetic factors, polycystic ovarian syndrome, cigarette smoking, psychosocial factors such as depression during pregnancy, unhealthy dietary behaviour (‘western diet style – high sugar consumption including sweets, sweetened beverages, potatoes; increased dietary fat consumption including fried foods and animal fat; and protein including red/processed meat; refined grain products e.g., French fries and pizza) before and during pregnancy, and physical inactivity before and during pregnancy. Furthermore, environmental (e.g., persistent organic pollutants and endocrine disruptors), and psychosocial (e.g., depression in the first and second trimester) factors increase the risk of developing GDM. Together with genetic susceptibility, these factors may explain the global differences in GDM burden. Nearly half of all GDM cases can be prevented by adopting a healthy diet prior to pregnancy (large uptake of fibre, nuts, fruits, green leafy vegetables, poultry and fish, an overall ‘Mediterranean’ diet), maintaining a BMI <25 kg/m2, doing exercise ≥30 minutes per day, and avoiding smoking [2, 3, 6]. Improvement in the metabolic processes associated with GDM occurs in women who return to pre-pregnancy body weight; which can be facilitated by engagement in physical activity and adoption of healthy diet [2].
Treatment of GDM aims to prevent foetal overgrowth and pregnancy complications and involves non-pharmacological and pharmacological modalities. Pharmacological treatments are utilized when non-pharmacological interventions do not achieve glycaemic control. Insulin therapy is the main pharmacological intervention, but it is associated with discomfort, increased cost, and risk of hypoglycaemia, requiring regular hospital visits and dose adjustments. Hence, glucose lowering oral medications such as metformin are becoming popular. Non-pharmacological interventions include mainly diet and physical activity [2] and are often sufficient to achieve glycaemic control [9, 10]. Indeed, lifestyle interventions which promote healthy diet and physical activity are also effective in the prevention of GDM. Furthermore, 70-90% of pregnant women with GDM can be effectively managed with lifestyle interventions alone [11]. Psychological and health education interventions may be relevant where they promote health behaviour changes such as self-monitoring of blood glucose levels [12,13,14]. A randomised controlled trial (RCT) showed improvements in 1-hour postprandial blood glucose after an educational intervention. The study reported no statistically significant differences amongst four groups of nutrition therapy only, nutrition therapy plus education, insulin therapy only, and insulin therapy plus education in other outcomes such as fasting blood glucose, 2-hour postprandial blood glucose, glycated haemoglobin and quality of life [15]. However, this study may have been underpowered to detect statistical significance. Self-management programmes usually contain psychological and health education components, and systematic reviews have suggested that they can be effective in the management of GDM [16,17,18].
Community-based treatment is associated with lower costs, higher patient satisfaction, fewer hospitalizations and emergency department visits, and lower mortality [19, 20]. Community-based interventions are often outside large health institutions such as primary health care and general community settings, can involve non-medical personnel, have behavioural expectations and active participation, are culturally sensitive rather than routine, and are usually not intrusive [21]. Community-based interventions can be seen as multicomponent interventions that combine individual and environmental change strategies across multiple settings aiming to prevent diseases and to promote well-being among population groups outside of mainstream secondary and tertiary health facilities [22].
There is no synthesized evidence on community-based non-pharmacological interventions for GDM. Therefore, we aimed to systematically summarise the evidence regarding community-based non-pharmacological interventions for GDM, including intervention content and effectiveness. We reported this systematic review in line with the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) 2020 and the Synthesis without meta-analysis (SWiM) in systematic reviews reporting guidelines [23, 24].
Methods
Eligibility criteria, information sources, selection process, data items, assessment of reporting bias and certainty assessment are detailed in Table 1.
Search strategy
Search strategies for the twelve databases were informed by the Cochrane handbook for systematic reviews of interventions [25]. In line with the PRISMA 2020 guidelines [23, 26], searches involved several combinations of MeSH and free text terms and word variants for pregnant, gestational diabetes, community-based and non-pharmacological interventions. Search strategies were developed for the different databases and was piloted to establish sensitivity prior to searching (appendix 1).
Data collection process
Data were collected using a data extraction form that was adapted from the Cochrane Group’s Data Extraction Template [27]. Three reviewers (CNI-C, PCO, GNE) independently piloted the form on a random sample of 5 articles. Final amendments were made to the form prior to data extraction. PCO and GNE independently extracted data from studies. Inconsistencies in extracted data were resolved by discussion with CNI-C. A maximum of three email requests were made to corresponding authors of studies with missing or unclear information.
Study risk of bias assessment
Two reviewers (CNI-C, PCO) independently assessed the risk of bias in all RCTs. Other study designs were regarded as high risk of bias. The risk of bias in RCTs were assessed using the Cochrane’s risk of bias tool including selection bias, performance bias, detection bias, attrition bias, reporting bias and other potential threats to validity [28]. For each RCT, low risk of bias in all domains was classified as low risk of bias overall. High risk of bias or unclear risk of bias in only one item was classified as minimal risk of bias overall. High risk of bias or unclear risk of bias in two to three items was classified as moderate risk of bias overall. High risk of bias or unclear risk of bias in four items and above was classified as high risk of bias overall.
Synthesis methods
Narrative synthesis was used due to clinical, methodological, and statistical heterogeneity arising from diverse interventions, study designs, methods, and outcomes, respectively.
This systematic review is registered with PROSPERO (CRD42021257634) and the protocol is available online.
Results
Study selection
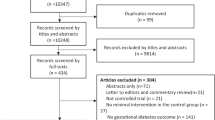
One thousand eight hundred sixteen duplicates were removed from the initial search yield of 9 162. 7 346 titles and abstracts were screened, and 109 full text articles were screened. 25 articles were eligible. Two RCTs were included from the update search. A total of 27 articles were included in this review: 16 RCTs and 11 quasi-experimental studies (Fig. 1).

Flow diagram of the study selection process
Study characteristics
Included study characteristics are illustrated in Table 2. Identified studies were published between 2004 and 2021; and involved 6,242 pregnant women with gestational diabetes mellitus in China (6), Iran (5), United State of America (3), Canada (2), Australia (1), Brazil (1), Croatia (1), Egypt (1), Ireland (1), Japan (1), Mexico (1), Nigeria (1), Oman (1), Thailand (1), and Turkey (1). The community-based non-pharmacological interventions were delivered in primary health care centres (antenatal/maternal clinics) (8), private community clinics (5), obstetric community clinics (3), gestational diabetes mellitus community clinics (3), perinatology community clinics (2), outpatient community clinics (2), medical centre (1), and urban community clinic (1) by researchers (9), dieticians/nutritionists (4), physicians and researchers (2), physicians (2), nurses (2), physiotherapists (1), educators (1), physician and nurses (1), educator and physicians (1), exercise physiologist and nurse (1), midwives and nurses (1), dietician and nurse (1), not specified (1). The control interventions were delivered in the same facilities.
Risk of bias in studies
Table 3 highlights the risk of bias in individual RCTs. Overall, two RCTs were low risk of bias, two RCTs were minimal risk of bias, eight RCTs were moderate risk of bias, and three RCTs were high risk of bias. All eleven quasi-experimental studies were regarded as high risk of bias.
Results of individual studies
Table 4 presents the description of the community-based non-pharmacological interventions and the control group interventions as well as the results of each study.
Summary of individual study outcomes
Majority (25) of the studies showed that community-based non-pharmacological interventions were more effective than control interventions which included routine/standard prenatal care, placebo, or no treatment in improving the greatest number of maternal and new-born outcomes. 15 studies reported similar effectiveness in comparatively fewer number of outcomes in the intervention and control groups. Only one study reported a superior improvement in a neonatal outcome (neonatal body mass index), and only one study reported a superior improvement in a maternal outcome (reduced caesarean section use), both when compared with control (routine/standard prenatal care).
Summary of community-based non-pharmacological interventions
Self-management programmes
Nine studies investigated self-management programmes which involved face-to-face educational sessions and self-care guide package [47], health education and lifestyle management delivered using social media (WeChat) plus motivational briefing to promote self-care in relation to diet, exercise, and blood glucose control [53], self-management education programme involving goal setting, motivational interviewing to increase self-efficacy, social support, self-monitoring of blood glucose, plus phone call reminder of education [32], self-efficacy enhancing intervention involving individualised health education comprising motivational messages, role modelling, goal-setting and mastery experience to facilitate healthy behaviours [48], cell phone–internet technology (CIT) for self-management (monitoring) of hyperglycemia during pregnancy [35], supplementary 1-hour education session for diabetes education [45], health-promoting lifestyle education programme [46], continuous health education using a smartphone-based telemedicine system [33], group educational programme enhancing health-related knowledge and facilitating self-care [34].
Medical nutrition/diet therapy interventions
Nine studies examined medical nutrition/diet therapy programmes which involved low–glycaemic index (LGI) diet [38, 39, 41], oat bran plus routine diet for gestational diabetes [54], dietary approaches to stop hypertension (DASH) diet that is rich in fruits, vegetables, whole grains and low-fat diary products [40], 3-day intensive diet therapy [37], medical nutrition therapy counselling [49,50,51].
Exercise/physical activity programmes
Five studies investigated exercise/physical activity programmes which involved resistance exercise [30], regular supervised exercise plus daily brisk walking [31], aerobic dance exercise [29], physical activity lifestyle programme [44], and daily walking programme [4].
Combined diet and exercise interventions
Two studies investigated combined exercise and diet therapy programmes which involved exercise equivalent to a 60% symptom-limited VO2 max and diabetic diet [42], and consultation with a dietician plus individually tailored exercise [43].
Calcium and vitamin D supplement therapy
One study examined the use of combined 1000 mg of Calcium and two pearls containing 1250 μg (50 000 IU) of cholecalciferol [52].
Continuous glucose monitoring intervention
One study investigated the use of continuous glucose monitoring which involved the use of continuous glucose monitoring system to assess 24-hour glucose fluctuations (every 10 seconds and an average value stored every 5 minutes. This provides up to 288 measurements per day, and offers a complete view of glucose profile about the direction, magnitude, duration, frequency, and causes of fluctuations in blood glucose levels [36].
Results of syntheses
Effectiveness of community-based non-pharmacological interventions
Meta-analysis was precluded due to different intervention content in experimental and control groups, study designs, and outcomes (Tables 2 and 4).
Effectiveness of self-management programmes
Self-management programmes consistently improved most health behaviour-related outcomes such as self-efficacy [32, 47, 48], lifestyle behaviours [46, 48], self-management behaviour [32], self-monitoring of blood glucose [35], adherence to recommended healthy health promoting behaviours [45], cues to action [32], perceived benefits [32], perceived barriers [32], perceived severity [32], perceived susceptibility [32], and satisfactory knowledge [34] better than routine obstetric care.
Two-hour postprandial blood glucose was also consistently better improved by self-management programmes than routine care [33, 35, 47].
Only one clinical trial each measured quality of life [46] and satisfaction [35], pregnancy-induced hypertension [33] with all reporting better improvements in the self-management programmes.
No differences between self-management programmes and routine care were found for infant birth weight [47, 53] and age of neonate at delivery [47], premature rupture of membranes [53], postpartum haemorrhage [53], days of maternal/neonatal hospitalisation [45].
Other maternal and neonatal clinical outcomes were conflicting. Two clinical trials (one cross-over trial) reported no difference in fasting blood glucose in the routine care and self-management programmes [35, 47]; but one non-RCT reported superior improvements in fasting blood glucose in the self-management programmes than routine care [33]. One study each reported superior effects of self-management programmes on blood glucose control (glycaemic qualification rate) [53], glycated haemoglobin [32], but another study reported no significant differences in glycaemic control [45] compared with routine care. No differences were found in macrosomia [45] in one study whereas another study reported lower rates of macrosomia in the self-management programmes compared with routine care [46]. One study reported no differences in preterm birth [53] but another study showed lower rates of premature delivery in the self-management programme compared with routine care [33]. Two studies reported no differences in the type of delivery [47, 53], whereas one study reported that caesarean section was less in the routine care group compared with self-management [33].
Effectiveness of medical nutrition/diet therapy interventions
Medical nutrition/diet therapy interventions consistently improved postprandial blood glucose levels more than routine diabetic diet [38, 41, 49, 50, 54].
One study showed that small group nutritional counselling saved 27 dietitian hours compared to individual nutritional counselling, with knowledge levels being similar in both treatment groups [51].
Fasting blood glucose was better improved by the addition of 30 grams oat bran daily to routine diabetic diet for 4 weeks than routine diabetic diet alone [54]. Superior improvements in fasting blood glucose was produced by a medical nutrition therapy (MNT) counselling compared with a no MNT group [49]. Another MNT programme produced similar improvements in fasting blood glucose as routine obstetric care [50].
Similar glycaemic control was observed between a low glycaemic index diet and a routine diabetic diet consisting of conventional high fibre diet [41]. However, a three-day intensive diet therapy produced superior glycaemic control than routine diabetic care such that fewer people required insulin therapy [37].
Similar outcomes between a low glycaemic index and a conventional high fibre diet were produced for infant birth weight, ponderal index (within normal), maternal weight, foetal abdominal circumference [54]. Likewise, similar outcomes were produced by an intensive MNT programme and routine obstetric care in insulin use, prematurity, macrosomia, low birth weight, and intrauterine death [50]. MNT counselling produced superior outcomes in maternal weight, rates of adverse events, and exclusive breast feeding than a no MNT control [49]. Similarly, an intensive MNT programme produced better outcomes in rates of perinatal complications, preeclampsia, maternal hospitalisations, neonatal intensive care unit admissions, and had no neonatal deaths compared with routine obstetric care [50]. Dietary approaches to stop hypertension (DASH) diet that is rich in fruits, vegetables, whole grains and low-fat diary products produced superior pregnancy outcomes (lower caesarean delivery and insulin therapy), lower rates of macrosomia, lower birth weight and head circumference, and lower ponderal index; but similar outcomes in gestational age, polyhydramnios, newborn length, and Apgar score compared to a control diet (45-55% carbohydrate, 15-20% protein, 25-30% total fat) given as routine care [40].
Effectiveness of exercise/physical activity programmes
Postprandial blood glucose levels were better improved by regular supervised exercise plus daily brisk walks than routine obstetric care [31]. Similarly, postprandial blood glucose levels were improved by a daily walking intervention in a pre-post-test study with no control group [4]. The effects of exercise/physical activity programmes were mostly inconsistent for other outcomes.
Fasting blood glucose was better improved by an aerobic dance exercise intervention than routine obstetric care [29]. In contrast, a regular supervised exercise plus daily brisk walking intervention and routine obstetric care produced similar improvements in fasting blood glucose [31]. Resistance exercise produced greater improvements in glycaemic control (weeks within target blood glucose range) than routine obstetric care but resistance exercise and routine obstetric care produced similar mean glucose levels [30].
Resistance exercise produced greater reduction in people requiring insulin, new-born birthweight but similar outcomes in quantity of insulin required by patients, time interval between patient inclusion in study and insulin use, rates of caesarean section, rates of preterm when compared with routine obstetric care [30]. Physical activity lifestyle programme produced better improvements in maternal body mass index, rates of preterm birth, rates of low birth weight, and macrosomia than a control group without such intervention [44]. Regular supervised exercise plus daily brisk walks produced similar outcomes as routine obstetric care on rates of pregnancy and birth complications, need for pharmacological therapy, maternal body mass and body fat percentage, neonatal Apgar scores, ponderal index. However, neonatal body mass index was better in the routine obstetric care group than the exercise/physical activity group [31].
Effectiveness of combined diet and exercise interventions
Diet and exercise was superior to diet alone in reducing maternal weight gain per week but similar outcomes were observed for other pregnancy and foetal outcomes including complications, gestational age at delivery, and rate of caesarean delivery [42]. Diet and exercise were better in improving the rates of large for gestational age and macrosomia compared with pregnant women with normal glucose tolerance placed on routine obstetric care, although other adverse outcomes were similar between the two groups [43].
Effectiveness of calcium and vitamin D supplement therapy
Significant decrease in the rates of caesarean delivery, maternal hospitalisation, hyperbilirubinaemia, newborn hospitalisation were observed with combined 1000 mg of Calcium and 1250 μg of cholecalciferol compared with placebo. No case of macrosomia was seen with the vitamin supplementation, in contrast to placebo [52].
Effectiveness of continuous glucose monitoring intervention
Better glycaemic control, reduced risk of pre-eclampsia and caesarean delivery, and reduced birth weight and neonatal complications were produced with continuous glucose monitoring plus routine obstetric care compared to routine obstetric care alone [36].
Reporting bias in overall results
There were no systematic differences in the consistent and inconsistent outcomes based on study rating of bias, study design and the size of individual studies.
Certainty of overall results
Strong evidence showed that the community-based self-management programmes improved self-efficacy [32, 47, 48], and 2-hour postprandial blood glucose [33, 35, 47], better than routine care. Moderate evidence suggests that the self-management programmes improved life style behaviours [46, 48], better than routine care. Moderate evidence indicated that the self-management programmes produced similar outcomes on infant birth weight as routine care [47, 53].
The strength of evidence for the effectiveness of the self-management programmes for some outcomes was conflicting. Moderate evidence suggests that the self-management programmes produced similar outcomes as routine care for fasting blood glucose [35, 47] but very low evidence suggest that they are superior to routine care [33] for fasting blood glucose. There is very low evidence that the self-management programmes were superior or as effective as routine care in improving blood glucose control [32, 45], macrosomia [45, 46], and preterm delivery [33, 53]. There is moderate evidence that the self-management programmes produced similar outcomes as routine care in reducing the rates of caesarean delivery [47, 53], but very low strength of evidence that they are inferior to routine care [33] in reducing the rates of caesarean delivery.
There is moderate evidence that community-based medical nutrition/diet therapy interventions were more effective than usual care in improving postprandial blood glucose levels [38, 41, 49, 50, 54].
The strength of evidence for the other outcomes and the effectiveness of the other community-based non-pharmacological interventions was uncertain because only one study examined them.
Discussion
This systematic review of community-based non-pharmacological interventions for pregnant women with gestational diabetes mellitus indicate that these interventions were more effective than routine care in improving health behaviour related outcomes and two-hour postprandial blood glucose. Other outcomes of these programmes were less consistent. Community-based self-management programmes were superior to or as effective as routine care in improving fasting blood glucose, blood glucose control, glycated haemoglobin, macrosomia/infant birth weight, and preterm delivery. There was a trend towards community-based self-management programmes being superior to routine care in improving self-management behaviour, self-monitoring of blood glucose, adherence to recommended health promoting behaviours, quality of life, satisfaction, pregnancy-induced hypertension, cues to action, perceived benefits, perceived barriers, perceived severity, perceived susceptibility, and satisfactory knowledge. However, there was a trend towards the self-management programmes being similar to usual care in improving age of neonate at delivery, premature rupture of membranes, postpartum haemorrhage, and days of maternal and neonatal hospitalisation. The impact on the rates of caesarean delivery is conflicting.
These findings align with the reviews of self-management programmes for other diabetic populations including adults, adolescents and/or children with type 1 or type 2 diabetes mellitus. Self-management programmes were efficacious and cost effective for facilitation of self-management, improvements in patients' knowledge, skills, and motivation, and improved biomedical, behavioural, and psychosocial outcomes [55]. Self-management programmes had a greater impact on glycaemic outcomes than on mental health outcomes which were rarely assessed [56]. Blood glucose control, diabetes knowledge, body weight, blood pressure, low density lipoprotein cholesterol, mean arterial pressure, anxiety and depression, diabetes distress, sedentary behaviours, quality of life, self-efficacy, self-care, self-management skills, and treatment satisfaction were improved following diabetes self-management programmes [57]. Self-management produced better improvements in glycated haemoglobin, diabetes knowledge, self-efficacy, self-management behaviours, depression, quality of life and patient satisfaction compared with routine care [58]. Self-management programmes were better than routine care for fasting blood glucose, blood pressure, body mass index, self-efficacy, diabetes knowledge; but were similar for self-management practices, physical activity, diabetes distress, and depression [59].
The conflicting results of the impact of self-management programmes for some outcomes in our review could be due to the different content, intensity, and delivery of the self-management programmes in few studies. Other reviews of diabetes self-management programmes have made similar observations and reported very few and differing studies of diverse diabetes self-management programmes which make interpretation and generalisation of findings difficult [57, 59]. The recommendation that diabetes self-management programmes be tailored acknowledging individual and cultural needs [60] might increase effectiveness and consistency of findings. Determining and utilising active components and core outcomes of diabetes self-management programmes could enhance effectiveness and consistency of findings. Self-management programmes focus on lifestyle changes, health behaviour change, and daily self-management of conditions [61,62,63,64] which could explain the consistent superior effectiveness of the community-based self-management programmes on health behaviour related outcomes when compared with routine care in our review.
Our results show that community-based medical nutrition/diet therapy interventions were more effective than routine care in improving postprandial blood glucose levels; which can be a proxy for good adherence to nutritional therapy [65]. The effectiveness of the interventions was less certain for the other outcomes because only one study reported each of them. Overall, there was a trend towards community-based medical nutrition/diet therapy interventions being superior to or as effective as usual care in the other maternal outcomes and all neonatal outcomes. Intensive nutritional interventions tended to be more effective than usual care in the greatest number of outcomes. Although group nutritional counselling was as effective as individual nutritional counselling in improving diabetes knowledge, group counselling had an additional advantage of saving dietitian hours.
Overall, our review found no evidence that any specific community-based nutritional therapy was superior to the other. This could be because any diet based on low glycaemic index diet, high in complex carbohydrate and fibre, low in simple sugar and low in saturated fat produce positive outcomes in GDM including reduction in blood glucose, prevention of insulin resistance, and attenuating excess foetal fat accretion [65,66,67,68,69,70]. Low glycaemic index diet is known to reduce two hour post prandial glucose, fasting blood glucose, and lipid profile in patients with GDM [71]. This aligns with our review which found that glycaemic control was similar between low glycaemic index and conventional high fibre diets. Low carbohydrate diet is not better than high complex carbohydrate diet [72]. Low carbohydrate diet can stimulate higher fat intake exacerbating maternal insulin resistance due to increased free fatty acids [70, 73, 74]. High fibre and low-fat intake increase gut microbiota diversity and richness which reduce insulin resistance and inflammatory response [75]. Caloric restriction is generally advised only for overweight and obese pregnant women with GDM [65, 66]. However, there is no consensus on specific diet characteristics including carbohydrate distribution and quantity due to the limited number of high quality clinical trials and the complexity that such interventions and studies will warrant [65, 66, 70, 76].
The strength of evidence for the effectiveness of community-based exercise/physical activity was limited due to the paucity of studies (less than two studies for each outcome). There was a trend for physical activity/exercise interventions being superior in improving postprandial blood glucose levels than routine care and no treatment. Other outcomes were less consistent but overall physical activity/exercise interventions tended to be better than or as effective as routine care in improving fasting blood glucose, glycaemic control, mean glucose levels, proportion requiring insulin, quantity of insulin required, time to insulin use, new-born birthweight, rates of caesarean section, rates of preterm birth, maternal body mass index, rates of low birth weight, macrosomia, rates of pregnancy and birth complications, need for pharmacological therapy, maternal body mass and body fat percentage, neonatal Apgar scores, ponderal index. Neonatal body mass index was the only outcome reported to be better with routine obstetric care in one study. There is limited direct evidence with which to compare these findings. A systematic review which shows that physical activity during pregnancy improves fasting and postprandial glucose, as well as glycated haemoglobin in pregnant women with GDM, had four of the included six studies combining exercise with diet [77].
Most reviews have focused on the prevention of GDM using exercise/physical activity. Although previous reviews found insufficient evidence that exercise/physical activity during pregnancy is effective in reducing the development of GDM [78, 79], more recent systematic reviews have found that exercise during pregnancy reduces the risk of developing GDM [80,81,82]. The greatest benefit of physical activity in reducing the risk of GDM occurs before pregnancy [83]. Findings from our review and previous reviews have not shown any evidence for the superiority of any exercise type. However, guidelines recommend both aerobic and resistance exercise at a moderate intensity, a minimum of three times per week for 30-60 minutes each time [84]. The exercise/physical activity interventions in our review were aerobic, resistance, or combined aerobic and resistance exercise which may align with this recommendation. Exercise/physical activity provides an alternative pathway of glucose uptake to insulin activated transport via muscular contraction that ultimately stimulates glucose transport; directly increases the biogenesis of GLUT4 which is an insulin-regulated glucose transporter that is responsible for insulin-regulated glucose uptake into fat and muscle cells; and can strengthen and compensate for defects in insulin signalling; which improve glycaemic control [85].
Our review found very limited evidence that community-based diet and exercise was better than diet alone or routine obstetric care in improving maternal and neonatal outcomes particularly maternal and neonatal weight. Evidence suggest that dietary improvements and physical activity are effective in managing hyperglycaemia and the associated sequelae [86].
Similarly, our review found very limited evidence that combined calcium and vitamin D supplement therapy was better than placebo in reducing the rates of caesarean delivery, maternal hospitalisation, hyperbilirubinaemia, newborn hospitalisation, and preventing macrosomia. Evidence suggests that multivitamins containing vitamin D reduce the risk of preeclampsia which was not found with administering only vitamins C and E [66, 87]. There is some evidence that vitamin D supplements improve insulin sensitivity in women with GDM, and an intake of 900-1000mg of calcium per day is recommended for all pregnant women [66, 87]. Calcium is considered important because the hyperglycaemia resulting from GDM is associated with neonatal hypocalcaemia, hypoglycaemia, hyperbilirubinemia, polycythaemia and respiratory distress syndrome [88].
We found very limited evidence that continuous glucose monitoring added to routine obstetric care reduced risk of pre-eclampsia and caesarean delivery, and reduced birth weight and neonatal complications better than routine obstetric care only. A recent meta-analysis of six RCTs found that continuous glucose monitoring was associated with lower glycated haemoglobin, less gestational weight gain, lower birth weight compared to standard blood glucose monitoring. However, there were no differences between continuous glucose monitoring and standard blood glucose monitoring for gestational age newborns, gestational age at birth, preterm deliveries, shoulder dystocia, neonatal hypoglycaemia, Apgar at five minutes, admission to neonatal intensive care unit, neonatal jaundice, and neonatal mortality [89].
Strengths and limitations
To the authors’ knowledge, this systematic review is the first to investigate community-based non-pharmacological interventions for pregnant women with GDM. Moreover, the concept of community-based interventions is evolving and can be diverse since ‘community’ can be conceptualised as the setting, target, agent, or the resource [90]. The inclusion of all relevant primary studies on GDM regardless of study design and publication date; plus, the grading of the strength of each outcome strengthens the evidence-base on which the findings of this review are based.
This review is limited by the lack of a consensus definition and diagnostic criteria for GDM in individual studies. This review used the most widely accepted definition of GDM as hyperglycaemia during pregnancy. This implies all cases of hyperglycaemia during pregnancy including true GDM (which develops later during pregnancy) and previously undetected pre-existing diabetes (which is also referred to as ‘overt diabetes’ and is often identified in early pregnancy, and comprises both pre-gestational type 2 diabetes mellitus and type 1 diabetes mellitus) [11]. Therefore, the findings from this systematic review may not be exclusive to GDM. This may not be a limitation per se since preventive strategies for type 2 diabetes may also be successful in the prevention of GDM [11]. The inclusion of observational studies alongside RCTs is a limitation which was addressed by the grading of the overall quality of evidence for each outcome. The heterogeneity in intervention content, study design and settings prohibit the endorsement of any specific components of the community-based non-pharmacological interventions.
Conclusions
Community-based non-pharmacological interventions were more effective or as effective as routine obstetric care in improving the most maternal and neonatal outcomes; and could be delivered by a broad range of health professionals. Of the six interventions identified, self-management programmes and medical nutrition/diet therapy had the strongest evidence for the most promising outcomes – on postprandial blood glucose levels and health behaviour related outcomes. There is need for more research on the effectiveness of these interventions whilst focusing on core GDM outcomes [91,92,93,94] and the active components of these interventions. There may be need to compare the clinical and cost-effectiveness of these interventions with hospital-based interventions.
Availability of data and materials
The review protocol is freely available on PROSPERO. Further information can be obtained via request to the corresponding author.
Abbreviations
- GDM:
-
Gestational Diabetes Mellitus
- PRISMA:
-
Preferred Reporting Items for Systematic reviews and Meta-Analyses
- SWiM:
-
Synthesis without meta-analysis in systematic reviews
- MeSH:
-
Medical Subject Heading
- RCT:
-
Randomised Controlled Trial
- CIT:
-
Cell phone–Internet Technology
- LGI:
-
Low–Glycaemic Index
- DASH:
-
Dietary Approaches to Stop Hypertension
- MNT:
-
Medical Nutrition Therapy
References
Craig L, Sims R, Glasziou P, Thomas R. Women’s experiences of a diagnosis of gestational diabetes mellitus: a systematic review. BMC Pregnancy Childbirth. 2020;20(1):1–15.
McIntyre HD, Catalano P, Zhang C, Desoye G, Mathiesen ER, Damm P. Gestational diabetes mellitus. Nat Rev Dis Prim. 2019;5(1):1–19.
Damm P, Houshmand-Oeregaard A, Kelstrup L, Lauenborg J, Mathiesen ER, Clausen TD. Gestational diabetes mellitus and long-term consequences for mother and offspring: a view from Denmark. Diabetologia. 2016;59(7):1396–9.
Hayashi A, Oguchi H, Kozawa Y, Ban Y, Shinoda J, Suganuma N. Daily walking is effective for the management of pregnant women with gestational diabetes mellitus. J Obstet Gynaecol Res. 2018;44(9):1731–8.
Dirar AM, Doupis J. Gestational diabetes from A to Z. World J Diabetes. 2017;8(12):489.
Zhu Y, Zhang C. Prevalence of gestational diabetes and risk of progression to type 2 diabetes: a global perspective. Curr Diab Rep. 2016;16(1):1–11.
Hall D, Du Toit M, Mason D, Conradie M. Diabetes mellitus in pregnancy, still changing. J Endocrinol Metab Diabetes South Africa. 2015;20(3):108–14.
Grzelak T, Janicka E, Kramkowska M, Walczak M, Czyżewska K. Cukrzyca ciążowa–skutki niewyrównania i podstawy regulacji glikemii. Now Lek. 2013;82(8):163–9.
Di Guardo F, Currò JM, Valenti G, Rossetti P, Di Gregorio LM, Conway F, et al. Non-pharmacological management of gestational diabetes: The role of myo-inositol. J Complement Integr Med. 2020;17(2). https://doi.org/10.1515/jcim-2019-0111.
Guo X, Shu J, Fu X, Chen X, Zhang L, Ji M, et al. Improving the effectiveness of lifestyle interventions for gestational diabetes prevention: a meta-analysis and meta-regression. BJOG An Int J Obstet Gynaecol. 2019;126(3):311–20.
Zito G, Della Corte L, Giampaolino P, Terzic M, Terzic S, Di Guardo F, et al. Gestational diabetes mellitus: Prevention, diagnosis and treatment. A fresh look to a busy corner. J Neonatal Perinatal Med. 2020;13(4):529–41.
Gilbert L, Gross J, Lanzi S, Quansah DY, Puder J, Horsch A. How diet, physical activity and psychosocial well-being interact in women with gestational diabetes mellitus: an integrative review. BMC Pregnancy Childbirth. 2019;19(1):1–16.
Moisés ECD. Multidisciplinary Care of Pregnant Women with Gestational Diabetes Mellitus: Non-Pharmacological Strategies to Improve Maternal and Perinatal Outcomes. In: Gestation Diabetes-Causes, Diagnosis Treat. 2013. p. 17.
Mariani HS, Layden BT, Aleppo G. Continuous glucose monitoring: a perspective on its past, present, and future applications for diabetes management. Clin Diabetes. 2017;35(1):60–5.
Mirfeizi M, Mehdizadeh Tourzani Z, Asghari Jafarabadi M, Moghimi Hanjani S, Hasanzad M. Health education in gestational diabetes mellitus and quality of life. J Midwifery Reprod Heal. 2017;5(4):1066–74.
Adesina N, Dogan H, Green S, Tsofliou F. Effectiveness and Usability of Digital Tools to Support Dietary Self-Management of Gestational Diabetes Mellitus: A Systematic Review. Nutrients. 2021;14(1):10.
Karavasileiadou S, Almegewly W, Alanazi A, Alyami H, Chatzimichailidou S. Self-management and self-efficacy of women with gestational diabetes mellitus: a systematic review. Glob Health Action. 2022;15(1):2087298.
Carolan-Olah MC. Educational and intervention programmes for gestational diabetes mellitus (GDM) management: An integrative review. Collegian. 2016;23(1):103–14.
Nielsen KK, de Courten M, Kapur A. Health system and societal barriers for gestational diabetes mellitus (GDM) services-lessons from World Diabetes Foundation supported GDM projects. BMC Int Health Hum Rights. 2012;12(1):1–10.
Kolu P, Raitanen J, Rissanen P, Luoto R. Health care costs associated with gestational diabetes mellitus among high-risk women–results from a randomised trial. BMC Pregnancy Childbirth. 2012;12(1):1–8.
Murphy JW. Community-based interventions: Philosophy and action. Springer; 2014.
Igwesi-Chidobe CN, Emmanuel GN, Okezue OC. Community-based non-pharmacological interventions for improving pain, disability and quality of life in pregnant women with musculoskeletal conditions: protocol for a systematic review with meta-analyses. BMJ Open. 2021;11(2):e042107.
Page MJ, Moher D, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ. 2021;372:n160.
Campbell M, McKenzie JE, Sowden A, Katikireddi SV, Brennan SE, Ellis S, et al. Synthesis without meta-analysis (SWiM) in systematic reviews: reporting guideline. BMJ. 2020;368:l6890.
Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al. Cochrane handbook for systematic reviews of interventions. John Wiley & Sons; 2019.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
Cochrane Consumers and Communication Review Group. data extraction template for Cochrane reviews. Cochrane Collaboration; 2016.
Higgins JPT, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928.
Daniel JA, Dikki CE. Aerobic dance exercise improves blood glucose level in pregnant women with gestational diabetes mellitus science. African J Phys Heal Educ Recreat Danc. 2014;20(21):273–81.
de Barros MC, Lopes MAB, Francisco RPV, Sapienza AD, Zugaib M. Resistance exercise and glycemic control in women with gestational diabetes mellitus. Am J Obstet Gynecol. 2010;203(6):556-e1.
Kokic IS, Ivanisevic M, Biolo G, Simunic B, Kokic T, Pisot R. Combination of a structured aerobic and resistance exercise improves glycaemic control in pregnant women diagnosed with gestational diabetes mellitus. A randomised controlled trial. Women Birth. 2018;31(4):e232-8.
Mohebbi B, Tol A, Sadeghi R, Mohtarami SF, Shamshiri A. Self-management Intervention Program Based on the Health Belief Model (HBM) among Women with Gestational Diabetes Mellitus: A Quazi-Experimental Study. Arch Iran Med. 2019;22(4):168–73.
Yang P, Lo W, He Z, Xiao X. Medical nutrition treatment of women with gestational diabetes mellitus by a telemedicine system based on smartphones. J Obstet Gynaecol Res. 2018;44(7):1228–34.
El Sayed Ibrahim R, Mousa Saber N. Impact of self-care program for gestational diabetic women on pregnancy outcomes. Am J Nurs Res. 2019;8(1):122–31.
Bartholomew ML, Soules K, Church K, Shaha S, Burlingame J, Graham G, et al. Managing diabetes in pregnancy using cell phone/internet technology. Clin Diabetes. 2015;33(4):169–74.
Yu F, Lv L, Liang Z, Wang Y, Wen J, Lin X, et al. Continuous glucose monitoring effects on maternal glycemic control and pregnancy outcomes in patients with gestational diabetes mellitus: a prospective cohort study. J Clin Endocrinol Metab. 2014;99(12):4674–82.
Sunsaneevithayakul P, Ruangvutilert P, Sutanthavibul A, Kanokpongsakdi S, Boriboohirunsarn D, Raengpetch Y, et al. Effect of 3-day intensive dietary therapy during admission in women after diagnosis of gestational diabetes mellitus. J Med Assoc Thail. 2004;87(9):1022–8.
Hu Z-G, Tan R-S, Jin D, Li W, Zhou X-Y. A low glycemic index staple diet reduces postprandial glucose values in Asian women with gestational diabetes mellitus. J Investig Med. 2014;62(8):975–9.
Louie JCY, Markovic TP, Perera N, Foote D, Petocz P, Ross GP, et al. A randomized controlled trial investigating the effects of a low–glycemic index diet on pregnancy outcomes in gestational diabetes mellitus. Diabetes Care. 2011;34(11):2341–6.
Asemi Z, Samimi M, Tabassi Z, Esmaillzadeh A. The effect of DASH diet on pregnancy outcomes in gestational diabetes: a randomized controlled clinical trial. Eur J Clin Nutr. 2014;68(4):490–5.
Grant SM, Wolever TMS, O’Connor DL, Nisenbaum R, Josse RG. Effect of a low glycaemic index diet on blood glucose in women with gestational hyperglycaemia. Diabetes Res Clin Pract. 2011;91(1):15–22.
Artal R, Catanzaro RB, Gavard JA, Mostello DJ, Friganza JC. A lifestyle intervention of weight-gain restriction: diet and exercise in obese women with gestational diabetes mellitus. Appl Physiol Nutr Metab. 2007;32(3):596–601.
Kgosidialwa O, Egan AM, Carmody L, Kirwan B, Gunning P, Dunne FP. Treatment with diet and exercise for women with gestational diabetes mellitus diagnosed using IADPSG criteria. J Clin Endocrinol Metab. 2015;100(12):4629–36.
Wang C, Zhu W, Wei Y, Feng H, Su R, Yang H. Exercise intervention during pregnancy can be used to manage weight gain and improve pregnancy outcomes in women with gestational diabetes mellitus. BMC Pregnancy Childbirth. 2015;15(1):1–8.
Mendelson SG, Mcneese-Smith D, Koniak-Griffin D, Nyamathi A, Lu MC. A community-based parish nurse intervention program for Mexican American Women with gestational diabetes. JOGNN J Obstet Gynecol Neonatal Nurs. 2008;37(4):415–25.
Ural A, Kizilkaya Beji N. The effect of health-promoting lifestyle education program provided to women with gestational diabetes mellitus on maternal and neonatal health: a randomized controlled trial. Psychol Health Med. 2021;26(6):657–70.
Kolivand M, Rahimi MA, Keramat A, Shariati M, Emamian MH. Effect of a new self-care guide package on maternal and neonatal outcomes in gestational diabetes: A randomized control trial. J Diabetes. 2019;11(2):139–47.
Al-Hashmi I, Hodge F, Nandy K, Thomas E, Brecht M-L. The effect of a self-efficacy-enhancing intervention on perceived self-efficacy and actual adherence to healthy behaviours among women with gestational diabetes mellitus. Sultan Qaboos Univ Med J. 2018;18(4):e513.
Shi M, Liu Z-L, Steinmann P, Chen J, Chen C, Ma X-T, et al. Medical nutrition therapy for pregnant women with gestational diabetes mellitus—a retrospective cohort study. Taiwan J Obstet Gynecol. 2016;55(5):666–71.
Perichart-Perera O, Balas-Nakash M, Parra-Covarrubias A, Rodriguez-Cano A, Ramirez-Torres A, Ortega-González C, et al. A medical nutrition therapy program improves perinatal outcomes in Mexican pregnant women with gestational diabetes and type 2 diabetes mellitus. Diabetes Educ. 2009;35(6):1004–13.
Murphy A, Guilar A, Donat D. Nutrition education for women with newly diagnosed gestational diabetes mellitus: small-group vs. individual counselling. Can J diabetes. 2004;28(2):0.
Karamali M, Asemi Z, Ahmadi-Dastjerdi M, Esmaillzadeh A. Calcium plus vitamin D supplementation affects pregnancy outcomes in gestational diabetes: randomized, double-blind, placebo-controlled trial. Public Health Nutr. 2016;19(1):156–63. Available from: http://www.ncbi.nlm.nih.gov/pubmed/25790761 cited 2020 Jul 31.
Tian Y, Zhang S, Huang F, Ma L. Comparing the Efficacies of Telemedicine and Standard Prenatal Care on Blood Glucose Control in Women With Gestational Diabetes Mellitus: Randomized Controlled Trial. JMIR mHealth uHealth. 2021;9(5):e22881.
Barati Z, Iravani M, Karandish M, Haghighizadeh MH, Masihi S. The effect of oat bran consumption on gestational diabetes: A randomized controlled clinical trial. BMC Endocr Disord. 2021;21(1):1–8.
Chatterjee S, Davies MJ, Heller S, Speight J, Snoek FJ, Khunti K. Diabetes structured self-management education programmes: a narrative review and current innovations. Lancet Diabetes Endocrinol. 2018;6(2):130–42.
Hermanns N, Ehrmann D, Finke-Groene K, Kulzer B. Trends in diabetes self-management education: where are we coming from and where are we going? A narrative review. Diabet Med. 2020;37(3):436–47.
Vas A, Devi ES, Vidyasagar S, Acharya R, Rau NR, George A, et al. Effectiveness of self-management programmes in diabetes management: A systematic review. Int J Nurs Pract. 2017;23(5): e12571.
Amagyei A, Meal A, Shaw I, Adams GG. Effectiveness of Community Health Worker-led Diabetes Self-Management Education on Type 2 diabetes patients: A Systematic Review and Meta-Analysis. Int J Diabetes. 2020;1(2):40-50.
Werfalli M, Raubenheimer PJ, Engel M, Musekiwa A, Bobrow K, Peer N, et al. The effectiveness of peer and community health worker-led self-management support programs for improving diabetes health-related outcomes in adults in low-and-middle-income countries: a systematic review. Syst Rev. 2020;9(1):1–19.
Haas L, Maryniuk M, Beck J, Cox CE, Duker P, Edwards L, et al. National standards for diabetes self-management education and support. Diabetes Care. 2014;37(Supplement_1):S144-53.
Barlow J, Wright C, Sheasby J, Turner A, Hainsworth J. Self-management approaches for people with chronic conditions: a review. Patient Educ Couns. 2002;48(2):177–87.
Grady PA, Gough LL. Self-management: a comprehensive approach to management of chronic conditions. Am J Public Health. 2014;104(8):e25-31.
Allegrante JP, Wells MT, Peterson JC. Interventions to support behavioral self-management of chronic diseases. Annu Rev Public Health. 2019;40:127–46.
Newman S, Steed L, Mulligan K. Self-management interventions for chronic illness. Lancet. 2004;364(9444):1523–37.
Moreno-Castilla C, Mauricio D, Hernandez M. Role of medical nutrition therapy in the management of gestational diabetes mellitus. Curr Diab Rep. 2016;16(4):1–9.
Vasile FC, Preda A, Ștefan AG, Vladu MI, Forțofoiu M-C, Clenciu D, et al. An Update of Medical Nutrition Therapy in Gestational Diabetes Mellitus. J Diabetes Res. 2021;2021:5266919.
Mahajan A, Donovan LE, Vallee R, Yamamoto JM. Evidenced-based nutrition for gestational diabetes mellitus. Curr Diab Rep. 2019;19(10):1–10.
Wang H-K, Cheng D-C, Yang Y-M, Wang X-H, Chen Y, Zhang L, et al. The Role of High-Content Complex Dietary Fiber in Medical Nutrition Therapy for Gestational Diabetes Mellitus. Front Pharmacol. 2021;12:1509.
Tsirou E, Grammatikopoulou MG, Theodoridis X, Gkiouras K, Petalidou A, Taousani E, et al. Guidelines for medical nutrition therapy in gestational diabetes mellitus: systematic review and critical appraisal. J Acad Nutr Diet. 2019;119(8):1320–39.
Hernandez TL, Anderson MA, Chartier-Logan C, Friedman JE, Barbour LA. Strategies in the nutritional management of gestational diabetes. Clin Obstet Gynecol. 2013;56(4):803.
Filardi T, Panimolle F, Crescioli C, Lenzi A, Morano S. Gestational diabetes mellitus: The impact of carbohydrate quality in diet. Nutrients. 2019;11(7):1549.
Moreno-Castilla C, Hernandez M, Bergua M, Alvarez MC, Arce MA, Rodriguez K, et al. Low-carbohydrate diet for the treatment of gestational diabetes mellitus: a randomized controlled trial. Diabetes Care. 2013;36(8):2233–8.
Hernandez TL, Brand-Miller JC. Nutrition therapy in gestational diabetes mellitus: time to move forward. Diabetes Care. 2018;41(7):1343–5.
Hernandez TL, Mande A, Barbour LA. Nutrition therapy within and beyond gestational diabetes. Diabetes Res Clin Pract. 2018;145:39–50.
Ponzo V, Fedele D, Goitre I, Leone F, Lezo A, Monzeglio C, et al. Diet-gut microbiota interactions and gestational diabetes mellitus (GDM). Nutrients. 2019;11(2):330.
Meloncelli N, Wilkinson SA, de Jersey S. Searching for utopia, the challenge of standardized medical nutrition therapy prescription in gestational diabetes mellitus management: a critical review. In: Seminars in reproductive medicine. Thieme Medical Publishers, Inc.; 2020. p. 389–97.
Laredo-Aguilera JA, Gallardo-Bravo M, Rabanales-Sotos JA, Cobo-Cuenca AI, Carmona-Torres JM. Physical activity programs during pregnancy are effective for the control of gestational diabetes mellitus. Int J Environ Res Public Health. 2020;17(17):6151.
Yin Y, Li X, Tao T, Luo B, Liao S. Physical activity during pregnancy and the risk of gestational diabetes mellitus: a systematic review and meta-analysis of randomised controlled trials. Br J Sports Med. 2014;48(4):290–5.
Ruchat S, Mottola MF. The important role of physical activity in the prevention and management of gestational diabetes mellitus. Diabetes Metab Res Rev. 2013;29(5):334–46.
Sanabria-Martínez G, García-Hermoso A, Poyatos-León R, Álvarez-Bueno C, Sánchez-López M, Martínez-Vizcaíno V. Effectiveness of physical activity interventions on preventing gestational diabetes mellitus and excessive maternal weight gain: a meta-analysis. BJOG An Int J Obstet Gynaecol. 2015;122(9):1167–74.
Russo LM, Nobles C, Ertel KA, Chasan-Taber L, Whitcomb BW. Physical activity interventions in pregnancy and risk of gestational diabetes mellitus: a systematic review and meta-analysis. Obstet Gynecol. 2015;125(3):576–82.
Suhail ARD, Furuya-Kanamori L, Toft E, Musa OAH, Mohamed AM, Clark J, et al. Physical activity in pregnancy prevents gestational diabetes: A meta-analysis. 2020.
Tobias DK, Zhang C, Van Dam RM, Bowers K, Hu FB. Physical activity before and during pregnancy and risk of gestational diabetes mellitus: a meta-analysis. Diabetes Care. 2011;34(1):223–9.
Padayachee C, Coombes JS. Exercise guidelines for gestational diabetes mellitus. World J Diabetes. 2015;6(8):1033.
Wang C, Guelfi KJ, Yang H-X. Exercise and its role in gestational diabetes mellitus. Chronic Dis Transl Med. 2016;2:208–14. Available from: https://doi.org/10.1016/j.cdtm.2016.11.006.
Bain E, Crane M, Tieu J, Han S, Crowther CA, Middleton P. Diet and exercise interventions for preventing gestational diabetes mellitus. Cochrane database Syst Rev. 2015;4(CD010443). https://doi.org/10.1002/14651858.CD010443.pub2.
Dolatkhah N, Hajifaraji M, Shakouri SK. Nutrition therapy in managing pregnant women with gestational diabetes mellitus: a literature review. J Fam Reprod Heal. 2018;12(2):57.
Carreiro MP, Nogueira AI, Ribeiro-Oliveira A. Controversies and advances in gestational diabetes—an update in the era of continuous glucose monitoring. J Clin Med. 2018;7(2):11.
García-Moreno RM, Benítez-Valderrama P, Barquiel B, González Pérez-de-Villar N, Hillman N, Lora Pablos D, et al. Efficacy of continuous glucose monitoring on maternal and neonatal outcomes in gestational diabetes mellitus: a systematic review and meta-analysis of randomized clinical trials. Diabet Med. 2022;39(1):e14703.
McLeroy KR, Norton BL, Kegler MC, Burdine JN, Sumaya CV. Community-based interventions. Am J Public Health. 2003;93(4):529–33.
Egan AM, Bogdanet D, Griffin TP, Kgosidialwa O, Cervar-Zivkovic M, Dempsey E, et al. A core outcome set for studies of gestational diabetes mellitus prevention and treatment. Diabetologia. 2020;63(6):1120–7.
Bashir M, Syed A, Furuya-Kanamori L, Musa OAH, Mohamed AM, Skarulis M, et al. Core outcomes in gestational diabetes for treatment trials: the Gestational Metabolic Group treatment set. Obes Sci Pract. 2021;7(3):251–9.
Bain E, Middleton P, Crowther CA. Progressing towards standard outcomes in gestational diabetes Cochrane reviews and randomised trials. Aust New Zeal J Obstet Gynaecol. 2016;56(1):113–6.
O’Reilly SL, Leonard Y, Dasgupta K, Terkildsen Maindal H. Diabetes after pregnancy prevention trials: systematic review for core outcome set development. Matern Child Nutr. 2020;16(3):e12947.
Acknowledgements
Not applicable.
Funding
None.
Author information
Authors and Affiliations
Contributions
CNI-C conceptualised the study, developed the review protocol, synthesized, and interpreted results, coordinated all review activities, and wrote the manuscript versions. PCO and GNE collaborated on database searching, screening, data extraction, and quality appraisal. CNI-C, PCO and BCO were responsible for results synthesis. PCO contributed to writing the initial manuscript draft. CNI-C, PCO, BCO and GNE critically revised the article for intellectual content and approved the final version. All authors had full access to all study data and jointly made the decision to submit the manuscript for publication.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Igwesi-Chidobe, C.N., Okechi, P.C., Emmanuel, G.N. et al. Community-based non-pharmacological interventions for pregnant women with gestational diabetes mellitus: a systematic review. BMC Women's Health 22, 482 (2022). https://doi.org/10.1186/s12905-022-02038-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12905-022-02038-9