
Abstract
Background
Despite the increasing longevity of the world’s population, with an unprecedented rise in the number of people who need palliative care (PC), there has been sparse research regarding palliative care for older people, especially when it comes to comparison of PC between healthcare systems and cultures. The aim of this systematic scoping review was to identify the characteristics of the body of literature and to examine the knowledge gaps concerning PC research for older people (> 60 years) in two healthcare systems and cultures, mainland China and Sweden.
Methods
The guidelines PRISMA (Preferred Reporting Items for Systematic Reviews), and PICOS (Patient/population, Intervention, Comparison/control, and Outcome) were used. Empirical studies on patients 60 years or older, next of kin or staff participating in a palliative care intervention or setting were included. They were conducted in mainland China or in Sweden during 2007–2019, were published in English and were extracted from seven databases: Embase, PubMed, Scopus, Cinahl, PsycInfo, Academic Search Complete and Cochrane Library. Two independent researchers conducted the selection of studies, data extraction and methodological evaluation. Any disagreements were resolved in consultation with a third researcher. The analysis was manifest directed content analysis based on PICOS domains.
Results
Of the 15 studies, four were from mainland China and 11 from Sweden. Both countries included older patients with cancer but also other end-stage diseases such as heart failure and dementia. The studies differed in design, method and the content of the interventions. The study in China based on traditional Chinese medicine concerns traditional Chinese folk music. The six qualitative studies from Sweden were evaluations of five interventions.
Conclusions
Despite the high age of the participating patients, there was no focus on an ageing perspective concerning palliative care. To adapt to the changes taking place in most societies, future research should have increased focus on older persons’ need for palliative care and should take account of issues concerning research ethics, ethnicity and culture.
Registered in Prospero
CRD42020078685, available from.
Similar content being viewed by others


Background
There is a speedily increasing need for palliative care (PC) in China and Sweden as a consequence of the fast-growing number of elderly in the population. This growth is a worldwide phenomenon, the estimate being that the global number of people aged 65 or more will have doubled to 1 in 6 by 2050, from 1 in 11 in 2019 [1]. The increased longevity means an increased need of PC since older people’s last years are commonly associated with such conditions as cardiovascular disease, chronic obstructive pulmonary disease, diabetes, cancer and dementia [2]. PC should be knowledge-based in order to meet the complex needs of older people, which is to say that it should be built on scientific research evidence, best clinical practice and the preferences of the patient, next of kin and healthcare professionals [2, 3].
At the same time the importance of local context and culture has increasingly been emphasised in healthcare, and this is highly relevant to end-of-life decision-making [3,4,5]. Chinese culture has developed from Taoism, Confucianism and Buddhism, which has influenced traditional Chinese medicine (TCM) [6]. However, Western medicine has had an increased influence on healthcare in China since the early twentieth century, although TCM still plays an important role and is planned to increase in the future [7, 8]. Swedish culture is based mainly on Christian traditions, even though Sweden today is relatively secular [9]. In a Western culture such as that of Sweden, embracing the TCM perspective with integration between mind and body is of increased interest in healthcare but involves cultural, legal and institutional challenges [10, 11]. To the best of our knowledge there has not been any research study that compares PC in the two healthcare systems and cultures, those of mainland China and Sweden.
Our research team has a long record of research collaboration between the two countries [12,13,14,15], and during this collaboration we have found that there is a lack of research comparing the different healthcare systems regarding PC. Such comparison, though, is of importance for staff competence and the provision of evidence-based care in these multicultural countries. To acquire a deeper understanding of the existing knowledge-gap we first consider systematic studies of PC in general (without focusing on ageing) published during 5 years and then, against this background, review empirical studies of PC interventions for older people, which is the focus of this research.
A summary of the general systematic review studies from China follows. One recently published review identified seven studies which together covered the following broad range of PC: home-based hospice (n = 1), inpatient hospice (n = 1), PC and nutrition support (n = 1), Advanced Care Plan (n = 1), family conferences in inpatient context (n = 1), music therapy (n = 1) and three-week review intervention (n = 1) [16]. This intervention for patients with terminal illness consisted of reviewing the person’s life and composing a life-review booklet. It was also identified in two systematic reviews of the effects of spiritual care on quality of life (QoL) and spiritual well-being. The main conclusion was that more rigorous designs should be used in future studies [17]. A meta-analysis of six randomised controlled trials (RCTs) from China revealed that music therapy improved the QoL of terminally ill patients, alleviating pain and psychological symptoms like anxiety and depression [18]. A review of 14 studies concerning Chinese herbal medicine (CHM) as a means of symptom management for people with cancer showed significantly reduced pain when conventional treatment was complemented by CHM [19]. A Cochrane review was based on 15 studies from China of people with severe or end-stage chronic kidney disease being provided with either haemodialysis or peritoneal dialysis. The effect of various types of acupuncture and related interventions was low and there was a high or unclear risk of bias in all these studies [20]. However, another review indicated that when conventional cancer care was complemented by acupuncture and related therapies there was an improvement in QoL, with reduced pain and fatigue [21]. In another review [22] a preliminary conclusion was that PC effectively relieves pain in patients with cancer. However, this review covered only a small number of studies (n = 18) with several methodological limitations and exhibited a high heterogeneity of both pharmacological and non-pharmacological treatments. In a review of six studies involving Qigong exercises for symptom management among cancer patients no form of Qigong was suggested as being superior to any another and the effectiveness was uncertain due to the limited number of Qigong trials, methodological problems and high risk of bias [23]. A systematic review concerning supervised walking 5 days a week during 3 weeks alleviated fatigue for patients with advanced-stage haematologic cancer [24]. To summarize, the identified studies were disparate in content and focus, which may illustrate the extremely limited access to palliative care for people living in China described in the literature [25, 26].
In Sweden, a broadly based literature review of PC research [27] found a large increase in the number of studies for the period 2007–2012 as compared with the period 1970–2006 (mean 44 per year for the six-year period as compared with four per year for the longer period). This review showed that still predominant were cross-sectional studies, qualitative and mono-disciplinary studies, with exclusion of ethnic minorities, nonverbally communicable people and the oldest people. Of the 263 studies for the period 2007–2012, only 4 % of the studies involved clinical interventions and only 1 % were implementation studies. This can be assessed as inadequacy when it comes to the development of knowledge-based PC. The interventions included palliative home care team, symptom management with pain treatment, soft tissue massage and non-pharmacological caregiving activities, artificial nutrition and hydration, creative activity, complementary and alternative medicine (CAM), [27]. To summarize, the number of intervention and implementation studies was unexpectedly small considering that PC was established in Sweden some 40 years ago and that the research has expanded steadily in volume [27].
The similarities found in the reviews from the two countries, not selected by age, were that PC studies mostly concern cancer, as the proportion of the non-cancer specific population was 8% in China [16] and 13% in Sweden [27]. However, studies from mainland China were somewhat more often included in systematic reviews of PC than those from Sweden. This is probably related to the fact that there were few intervention studies from Sweden [27].
There is an urgent need to acquire a more profound knowledge of PC for older people. The PC needs are increasing in the ageing populations worldwide, which means that professionals and researchers have to develop evidence-based PC. International collaboration may seem to be essential to enable healthcare professionals to better respond to cultural diversity in evidence-based practice [28]. The previous sparse research and the research group’s longstanding collaboration in practice and research [12,13,14,15] is the background to mapping the knowledge of PC for older people in China and Sweden. Therefore, the aim of this systematic scoping review was to identify the characteristics of the body of literature and to examine the knowledge gaps concerning PC research for older people (> 60 years) in two healthcare systems and cultures, mainland China and Sweden. With this in mind, the following three research questions were in focus; (1) What are the similarities and differences between the two countries regarding PC interventions for older people who are at the end of life?, (2) What does PC mean for older people from the perspective of different ethnic groups in each country?, and (3) What ethical questions were discussed in connection with palliative care for older people with incurable disease in each country?
Methods
This study was a systematic scoping review based on the guidelines provided by PRISMA (Preferred Reporting Items for Systematic Reviews) [29]. A scoping review is a particularly appropriate method for identifying the body of evidence and knowledge gap when the literature is complex and heterogeneous [30, 31].
The study is registered in Prospero, CRD42020078685. Available from: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42020078685
Eligibility criteria
A protocol including Patient/population, Intervention, Comparison/control, and Outcome (PICOS) was constructed (Table 1) in order to perform a systematic screening procedure in accordance with the aim of the study.
To decide the period for the literature search a pilot test according to the inclusion and exclusion criteria (Table 1) was carried out in PubMed, which was the database expected to provide the greatest number of hits (see Additional file 1). There were 22 hits from China and 88 from Sweden. None of the 22 from China met the inclusion criteria: 15 were from Hong Kong or Taiwan, or included Chinese people living in other countries, six did not concern palliative care and one was not an intervention study (Additional file 1). Therefore the period chosen for inclusion was 1 January 2007 - 31 May 2019, this in order to allow comparisons between the two countries and also acquire deeper knowledge of palliative care interventions.
Regarding the 88 articles/hits found in the pilot test from Sweden, these showed the same pattern as reported in the previous review by the National Board of Health and Welfare, which included 133 studies for the same period up to and including 2006 [27]. Articles during that period consisted of predominantly qualitative design, small studies, cross-sectional studies and very few intervention studies.
Both quantitative and qualitative studies were included since there was no similar comparison study to be found in the Prospero register at the start of the study. Inclusion criterion were that the study was conducted in mainland China or in Sweden and have a published abstract. Furthermore, it has to be empirical studies involving interventions in palliative care or palliative settings of relevance for one of the included countries, and to have been published in a peer-review indexed journal. The patients were to be 60 years or older and with limited life-expectancy, and/or their next of kin or staff were included. The language was limited to English as this was the language shared by the involved researchers. More details of the inclusion and exclusion criteria are shown in Table 1.
Databases and search strategy
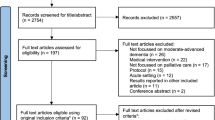
Two information specialists and librarians from Lund University conducted a systematic search and screening procedure for identifying and excluding double hits (Additional file 2, Fig. 1). The following databases were examined: Embase, PubMed, Scopus, Cinahl, PsycInfo, Academic Search Complete and Cochrane Library. A first search was performed in September 2017 and a second in May 2019. The search terms were modified according to the specific vocabulary of the particular database. MeSH was used and the following terms (with “and/or”) were sought: Palliative care, palliative nursing, palliative therapy, Palliative medicine, Palliative treatment, Terminal care, Terminal illness, End-of life care, End-of life treatment, Hospice, Hospice care, Aged, Elderly, Over 60 years. After removal of duplicates the librarian delivered the references as an EndNote database (Clarivate Analytics, Philadelphia, PA, USA). Grey literature was not identified and included.

Flow chart of the identification and selection procedure of the articles according to Prisma guideline
Study selection
All involved researchers had knowledge of the study aim and design before the start of the selection of studies, and the work was constantly discussed through Zoom online meetings (Zoom Video Communications, Inc.) or at face-to-face meetings chaired by the first author. The articles were stored and used in EndNote software. The steps for selection of the articles were based on PRISMA (Fig. 1) and PICOS. Two researchers independently reviewed the articles in each step. Any disagreements regarding study selection were resolved in consultation with a third or in some case fourth researchers. In the first step relevance was judged on the basis of abstract, thereafter on full text. The full text assessment was based on the selected EQUATOR guideline (Enhancing the QUAlity and Transparency Of health Research) [32] relevant to the design of the particular article. That means CONSORT for randomized trials, STROBE for observational studies, SRQR for qualitative research etc. The guidelines enabled the identification of the inclusion criteria in a similar manner independently of whether the researchers were from Sweden or China. The screening procedure resulted in 15 articles (Fig. 1).
Data analysis
The analysis of quantitative and/or qualitative data in each article was in the form of directed content analysis [33] based on PICOS domains, and it was geared to similarities and differences between China and Sweden with regard to palliative care for older people. This manifest analysis was used to describe the existing body of literature, identifying study characteristics, the scope of what has been studied, context, the available findings and gaps that need to be filled [34]. The analysis of the text for each domain was done by two reviewers, one from each country, in an iterative model between the researchers (GA, JH), and discussions with the other co-authors were used to validate the finding. First, both researchers read the articles several times and did the tabulation (Tables 2 and 3). Second, a summary of each article was written based on PICOS domains. Third, the text was condensed from each article without interpretation. Fourth, the different condensed texts from all 15 articles were put together. Fifth, the essence of the whole was identified and presented in the results section concerning similarities and differences between China and Sweden with regard to palliative care for older people. The scales of the instruments were reviewed only in an overall perspective, not in focus for deeper analysis with regard to assessing the risk of bias in the included studies.
Results
Design of the studies included
Of the 15 articles included, four were from mainland China and 11 in Sweden (Table 2). Nine had a quantitative design, all four from China and five from Sweden. The remaining six were qualitative studies from Sweden.
Two of the Chinese studies were RCT studies [35, 36] and two were questionnaire studies [37, 38]. Two of the Swedish quantitative studies were RCT studies [39, 40], two were quasi-experimental studies, one with control group [41] and one without control group [42], and the fifth was a cross-sectional questionnaire study [43].
All of the six qualitative studies involved evaluations of RCTs or interventions [44,45,46,47,48,49]. Five of them were interview studies [44,45,46,47,48], the other one was an ethnographic study with participant observations, field notes and follow-up interviews [49]. In Sweden two large RCT projects were represented by three [39, 45, 46] and two articles respectively [40, 47].
The quantitative and qualitative results are presented integrated in the text and in Table 2. In addition, the results of the qualitative studies are presented separately in Table 3.
Population
The number of participants varied greatly between the countries and study design (Table 2). Three of the four studies from China consisted of together 787 patients, whilst one included 2970 adult children of deceased older parents. Thus, the total number of participants from the Chinese studies were 3757 (range 170-2970). The 11 studies from Sweden involved 1811 participants (range 7-922): 1080 patients, 716 family members and 15 staff. Demographic data of the study groups such as mean age and sex were not comparable between the two countries.
Two of the studies from China focused on cancer [35, 36] while the other two did not focus on a specific disease. The respondents in the two non-cancer studies were the children of deceased older parents [38] and nursing home residents [37]. In Sweden only two of the 11 studies specifically involved patients with cancer [44, 47]. Three additional studies included patients in hospice care [42] and palliative home care [40, 43] without specific cancer focus even though that diagnosis is the most common in these types of care. Respondents in one of the studies concerning palliative home care were family members [40], while respondents in the other study were both patients and family members [43]. Three studies involved patients with chronic heart Failure (HF) [39, 45, 46]; in one of these studies the respondents were the family members [45]. Furthermore, one study used the handlers of therapy dogs as respondents and the patients were persons with dementia [48]. Finally, two studies concerned older patients without focus on specific diseases where the respondents were family members [39] and staff [49]. Both countries presented studies on older patients and cancer but Swedish studies have also included other end-stage diseases (HF and dementia), Table 2.
Perspectives on palliative care
Some differences between the two countries concerning theoretical concepts of palliative care was found. The three earliest studies from China used the terms Chinese medicine [35] and end-of-life care [37, 38] but then in 2018 Zhuang and colleagues [36] gave a description of palliative care which is much in agreement with the Swedish perspective. Palliative care is seen as being based on interdisciplinary collaboration between staff and is designed to alleviate symptoms, promoting the patient’s and the family’s QoL and facilitating the staff’s communication with the family. All studies from Sweden [39,40,41,42,43,44,45,46,47,48,49] used palliative care as the main concept and the term end-of-life only as a description of the late life phase. Some studies from Sweden focused on person-centred care and integrated care as new concepts for describing palliative care [39, 45, 46], but these concepts were not mentioned in the studies from China.
Another difference found between the countries was that Chinese culture was reported as influencing the development of palliative care in China, whilst no influence of culture was reported in the case of Sweden. The barriers mentioned in the Chinese studies were that death is a very sensitive issue, a topic people avoided speaking about, and that filial piety implies children’s fundamental responsibility for providing care for an ageing parent nearing the end of life [37, 38].
Interventions and exploration of palliative care
The RCT studies were not blinded for the participants or the health professionals. Two randomised intervention studies were from China, one evaluated the effect of the TCM five-element music on QoL for senior and non-senior patients with advanced cancer [35], the other the effect of early palliative care on QoL in patients with non-small-cell lung cancer (NSCLC) [36]. Of the two cross-sectional studies from China, one evaluated the family caregiving pattern at end-of-life [38], the other evaluated end-of-life care preferences in the form of the Advance Directive (AD) for nursing home residents [37].
One of the two randomised intervention studies from Sweden evaluated the intervention PREFER (Palliative advanced home caRE and heart failurE caRe). The target group were patients with HF and the intervention was based on key components in this cardiac care and specialised palliative care, person-centred, team-based, home-based and structured care [39]. This programme was evaluated by patients [39] and family members [45, 46]. The second randomised intervention study also concerned palliative home care but was a psycho-educational group intervention for family caregivers, evaluated on family caregivers and patients [40, 47].
The other interventions comprised massage [42, 44], the structured standard care plan known as the Liverpool Care Pathway (LCP) [41], palliative care education for the staff at nursing homes [49], multidisciplinary palliative home care teams [43], and use of therapy dog for patients with dementia [48]. These interventions were evaluated by patients [42,43,44], family members [41, 43], and staff [48, 49], Table 2.
Control groups in the studies
The two RCT studies in China were designed with randomised control groups and three of the RCT studies in Sweden involved control groups, as shown in Table 2.
Outcome measures
QoL and symptom assessment were the most common primary outcome measures when evaluating interventions. The interventions evaluated quantitatively (Table 2) use a number of different validated questionnaires (n = 16). Of these, the Hospital Anxiety and Depression Scale (HAD) was used in both countries [36, 40]. The Edmonton Symptom Assessment Scale (ESAS, which measures pain, tiredness, nausea, depression, anxiety, drowsiness, appetite, well-being, and shortness of breath) was used in three Swedish interventions [39, 41, 42], but none from China. Independently of which intervention programme was used, all evaluations showed enhanced QoL and decreased symptom burden in the intervention group post-intervention as compared with before and/or in comparison with a control group.
Table 3 shows the results from the six qualitative studies in terms of themes, sub-themes and categories. The qualitative studies are all from Sweden, none is from mainland China. The results provide greater understanding of each separate intervention in palliative care from the perspectives of patients (n = 3), family members (n = 1), assistant nurses and handlers of therapy dogs working in nursing homes (n = 2).
Discussion
The results show that palliative care interventions concerning older people were scarce since only 15 of totally 4194 identified articles at the start were included in this scoping review (the inclusion rate in China was 0.17% and in Sweden 0.59%). However, several studies in both countries were excluded because of not fulfilling the inclusion criteria. The main reasons for exclusion in China were that the interventions were medical palliative treatments (not palliative care, were not conducted in mainland China (the sample were instead Chinese immigrants living and receiving palliative care in other countries such as the USA) or were not focused on older people. The main reasons in Sweden were no intervention, not concerning older people or deficient information on the average age of the study group. The only TCM study in China was about music, whilst in Sweden there were two studies on massage but these were not reported as being based on a TCM perspective. In both countries symptom and QoL assessments were applied in the evaluations. However, the only instrument used in both countries was the HAD-scale for anxiety and depression. The six qualitative articles included the perspectives of patients, family and staff. To summarize, the included studies from each country differ from each other in respect of number of studies, designs and methods, and in the content of the interventions.
It is well-known that old age is strongly associated with a high risk of frailty and multimorbidity (two or more chronic health conditions in an individual) [50,51,52]. According to the WHO report on palliative care for older people [2], the specific needs in the end-of-life phase have received too little focus despite the fact that death is most common among older people. Palliative care should be provided more widely and become integrated into all relevant health care, not only offered to people with cancer in hospice or specialist units [2]. Despite an average age of 60 years or older in the included studies, only a few mentioned briefly the impact of age on the design of the palliative care intervention [48, 49]. There is a significant need to develop palliative care to meet the complex needs of older people due to multimorbidity and the sharply increased number of older people in the world including China and Sweden. One way is to broaden the competence within the palliative care team with a geriatrician and a nurse with special training in geriatric care to complement the oncology competence area [2, 53].
Research about palliative care produces various ethical concerns and methodological complexities since it involves vulnerable dying people. All studies in this review had been rigorously reviewed by the relevant ethical authority for each country. One common threat to the quality of the results in studies involving people with life-threatening conditions is high heterogeneity due to varied prognosis for different diseases, another is high attrition [2, 27, 54]. Development of new interventions or adaptation of established interventions for new groups such as older people presupposes evidence before implementation in daily palliative care. However, the need for new knowledge must be weighed against the risk of harm and the right not to be exposed to tiring research in a vulnerable situation without informed consent [54, 55]. A few studies from Sweden in this review reported ethical concerns; none from China did so. Cronfalk and colleagues [44] consider that the intervention with massage in the patient’s home involves a risk of intrusion upon integrity, whilst the human interaction in connection with massage can threaten the effect of this intervention. The decision to rely on proxy raters in research such as family members [41] and dog-handlers instead of the patients in the last phase of palliative care was taken in order to ensure nonmaleficence [48]. In contrast, Cronfalk and colleagues (2009) found that patients wanted to participate in the late phase of palliative care in order to contribute to the development of knowledge. Altruism was the main finding in a review of ten empirical studies concerned with dying persons’ attitudes to participating in research. It was meaningful for them to help others in a similar situation, to help society and to contribute to the progress of knowledge. However, the willingness to participate differed between designs and of study and in accordance with the degree of effort required of the patient [56]. Research ensures that palliative care provided for dying persons continues to become developed and evidence-based [2, 56]. Still, such research needs to be conducted with sensitivity, respecting the person’s autonomy and dignity [54, 55].
A systematic review of 50 articles demonstrates that older people had varied views concerning life and death, commonly involving a pragmatic acceptance of death’s inevitability [57]. Cultural beliefs and values are critical for people’s preferences and how they manage end-of-life. Culture can be described as a complex, multifaceted phenomenon shaped by interactions between socio-demographic factors and continuous processes of redefinition deriving from historical experiences and social realities [5]. In almost all developed and some developing countries, palliative care (like other forms of healthcare) has increased in complexity at the same time as the work of healthcare professionals is expected to be evidence-based. For evidence to be successfully implemented into practice, it is essential that the issues of context and cultural be considered. By critically reflecting on taken-for granted assumptions a greater understanding of both practice and the evidence available for use in practice can be acquired [58]. Knowledge and awareness of culture are therefore a necessity for professionals in palliative care who are to meet the needs of dying patients and their families of different cultural descent [5, 6]. In this review, three of the four Chinese studies described Chinese culture as a background to the study [35, 37, 38], but none of the Swedish studies takes account of cultural aspects.
Zuo and colleagues [38] investigated the children’s provision of the parents’ end-of-life care in rural areas. In the rural part of China end-of-life care is primarily provided by the family since there is little access to community-based palliative care. The results showed that the traditional shouldering of responsibility by the eldest sons and their spouses, based on the principles of Confucianism, was being transferred to eldest daughters, who increasingly provided the care of their parents. This fact was to be explained by the changing economy and culture in the context of the mass migration of young adults from rural areas [38]. In contrast to Swedish culture, the relatives’ power is more important than patient autonomy, which means that older Chinese people often prefer that their family make all care or treatment decisions [37].
Another cultural difference between the two countries concerns the patterns of communication with regard to dying and death [5]. The interventions from Sweden in respect of person-centred and integrated care [39, 45, 46] and in respect of education [40, 47, 49] indicate the vital role communication has in palliative care. The goal of this communication is to create sensitive, open and safe palliative care [43]. Studies from China show that death is a taboo subject that generates fear of bad luck [6, 25, 37]. The consequence is avoidance of communication about death by staff and family members [37], which may contribute to the concentration on striving to prolong the patient’s life as long as possible [6]. The problem is that patients may misunderstand their illness and prognosis and have no time to say goodbye, which is negative both for themselves and for their families [59]. There is need for further investigation of how cultural aspects shape meaning with regard to life and death and influence decision-making at the end of life.
This scoping review provides a basis for future research projects that can bridge the existing knowledge gap concerning PC, which is of considerable importance when it comes to meeting the needs of patients representing European and Chinese cultures. The identified areas could appropriately be the focus of future systematic reviews or other types of evidence synthesis.
Methodological considerations
This review has three limitations. Firstly, the studies had to be published in the English language. Even though palliative care has recently become an increasing area of healthcare in China [25, 26, 59], many studies on TCM are published in Chinese and therefore not included in this study. However, the literature reviews of palliative care interventions for patients of adult age (without focus on older people, summarized in the Introduction), indicate that these studies were small and without a control group and therefore did not fit the quality criteria for a systematic review. Scoping reviews are particularly helpful when the literature is complex and heterogeneous. It is also appropriate to assess and understand the extent of the knowledge in an emerging field or to identify, map, report or discuss the characteristics or concepts in that field [30, 31]. A recent scoping review of cohort studies in Chinese and English shows that TCM interventions have increased rapidly but the studies were of poor quality [60]. This limitation needs to be in mind when interpreting the results. A systematic review is to be recommended in the future to evaluate the evidence emerging from the steadily increasing number of intervention studies and to address any uncertainty or variation in their designs [30, 31].
Secondly, the studies included in this review revealed a significant variation in number, designs and focus of research questions and methods, when comparison was made within each country but especially when it was made between the countries. Given this diversity, no meta-analysis or meta-synthesis was undertaken. Instead, we used the PICO domains as the structure for the analysis. The final textual analysis was performed by two authors, one from each country (GA and JJ), and validated by the others. The selection of the studies was based on independent reviews of articles made according to Prisma by at least two researchers [29]. When there were conflicting results, three or sometimes four researchers reviewed the study in question until a final decision was made. The quality assessment was based on EQUATOR guidelines [32], and the guideline used was adapted to the particular design of the study. Furthermore this guideline is comprehensive and the disagreements were often caused by the reviewers’ varied focus in respect of quality criteria. From such disagreements there emerged the best possible judgement with an additional reviewer.
Thirdly, the intervention studies were so few in number that we had to broaden the design to include at least a few studies that contribute to knowledge about palliative care in the particular country. This weakness needs to be kept in mind when interpreting the results of this study. In the light of this we see the value of doing a follow-up study over the next decade to acquire more evidence-based knowledge and learn more from each other’s countries about palliative care.
A strength in this study was the pilot test of the literature search which resulted in a time limitation starting from 2007. This was a way of achieving reliability and efficiency and avoiding publication bias in the literature search by the information specialists/librarians [61].
Conclusions
This scoping review revealed very few palliative care interventions for people 60 years and above in both mainland China and Sweden. The differences were in the number of studies, in their perspective, design and method, and in the content of the interventions. It is therefore unclear whether the interventions are in line with the specific needs of older patients and their family members. Learning from each country regarding evidence-based interventions is limited in this step due to the small number of interventions, considerable variation and unsatisfactory scientific quality. This review represents an initial step in research about PC interventions in these two different healthcare systems and cultures. Palliative care is in an expansive phase, especially in China, making it of interest to carry out a systematic review in a follow-up study in the coming decade to evaluate whether the intervention research and practice is based on the established quality of evidence. Future research should have increased focus on older persons’ need for palliative care and should take account of issues concerning research ethics, ethnicity and culture.
Availability of data and materials
Abbreviations
- CAM :
-
Complementary and alternative medicine
- CHM :
-
Chinese herbal medicine
- EQUATOR guidelines :
-
Enhancing the QUAlity and Transparency Of health Research
- HAD :
-
The Hospital Anxiety and Depression Scale
- PC :
-
Palliative care
- PICOS :
-
Patient/population, intervention, comparison/control, and outcome
- PRISMA :
-
Preferred reporting items for systematic reviews
- QoL :
-
Quality of life
- RCT :
-
Randomised controlled trials
- TCM :
-
Traditional Chinese medicine
References
World Population Ageing 2019: Highlights (ST/ESA/SER.A/430). In.: United Nations; 2019.
Hall SPH, Tsouros A, Constantini M, Higginson I. Palliative care for older people : better practices. Copenhagen: World Health Organization, Regional Office for Europe; 2011.
Rycroft-Malone J, Seers K, Titchen A, Harvey G, Kitson A, McCormack B. What counts as evidence in evidence-based practice? J Adv Nurs. 2004;47(1):81–90.
Schein E. Organizational culture and leadership. San Francisco: Jossey-Bass; 2010.
Bullock K. The influence of culture on end-of-life decision making. J Soc Work End Life Palliat Care. 2011;7(1):83–98.
Hsu CY, O'Connor M, Lee S. Understandings of death and dying for people of Chinese origin. Death Stud. 2009;33(2):153–74.
Li ZG, Wei H. A Comprehensive Evaluation of China's TCM Medical Service System: An Empirical Research by Integrated Factor Analysis and TOPSIS. Front Public Health. 2020;8:532420.
Wang L, Suo S, Li J, Hu Y, Li P, Wang Y, et al. An investigation Into Traditional Chinese Medicine Hospitals in China: Development Trend and Medical Service Innovation. Int J Health Policy Manag. 2017;6(1):19–25.
History of Sweden. [https://sweden.se/society/history-of-sweden].
Liu Y, Yang Z, Cheng J, Fan D. Barriers and countermeasures in developing traditional Chinese medicine in Europe. Front Med. 2016;10(3):360–76.
Roberti di Sarsina P, Alivia M, Guadagni P. Traditional, complementary and alternative medical systems and their contribution to personalisation, prediction and prevention in medicine-person-centred medicine. EPMA J. 2012;3(1):15.
Le C, Ma K, Tang P, Edvardsson D, Behm L, Zhang J, et al. Psychometric evaluation of the Chinese version of the Person-Centred Care Assessment Tool. BMJ Open. 2020;10(7):e031580.
Cai L, Ahlstrom G, Tang P, Ma K, Edvardsson D, Behm L, et al. Psychometric evaluation of the Chinese version of the Person-centred Climate Questionnaire - Staff version (PCQ-S). BMJ Open. 2017;7(8):e017250.
Silen M, Tang PF, Ahlstrom G. Swedish and Chinese nurses' conceptions of ethical problems: a comparative study. J Clin Nurs. 2009;18(10):1470–9.
Wadensten B, Wenneberg S, Silen M, Ping Fen T, Ahlstrom G. A cross-cultural comparison of nurses' ethical concerns. Nurs Ethics. 2008;15(6):745–60.
Chung H, Harding R, Guo P. Palliative Care in the Greater China Region: A Systematic Review of Needs, Models, and Outcomes. J Pain Symptom Manag. 2021;61(3):585–612.
Chen J, Lin Y, Yan J, Wu Y, Hu R. The effects of spiritual care on quality of life and spiritual well-being among patients with terminal illness: A systematic review. Palliat Med. 2018;32(7):1167–79.
Gao Y, Wei Y, Yang W, Jiang L, Li X, Ding J, et al. The effectiveness of music therapy for terminally ill patients: a meta-analysis and systematic review. J Pain Symptom Manag. 2019;57(2):319–29.
Chung VCH, Wu X, Lu P, Hui EP, Zhang Y, Zhang AL, et al. Chinese herbal medicine for symptom management in cancer palliative care: systematic review and meta-analysis. Medicine (Baltimore). 2016;95(7):e2793.
Kim K-H, Lee MS, Kim TH, Kang JW, Choi T-Y, Lee JD. Acupuncture and related interventions for symptoms of chronic kidney disease. Cochrane Database Syst Rev. 2016;2016(6):CD009440. https://doi.org/10.1002/14651858.CD009440.pub2.
Lau CHY, Wu X, Chung VCH, Liu X, Hui EP, Cramer H, et al. Acupuncture and related therapies for symptom management in palliative cancer care: systematic review and meta-analysis. Medicine (Baltimore). 2016;95(9):e2901.
Zhao XX, Cui M, Geng YH, Yang YL. A systematic review and meta-analysis of randomized controlled trials of palliative care for pain among Chinese adults with cancer. BMC Palliat Care. 2019;18(1):69.
Van Vu D, Molassiotis A, Ching SSY, Le TT. Effects of Qigong on symptom management in cancer patients: A systematic review. Complement Ther Clin Pract. 2017;29:111–21.
Chen YJ, Li XX, Ma HK, Zhang X, Wang BW, Guo TT, et al. Exercise training for improving patient-reported outcomes in patients with advanced-stage cancer: a systematic review and meta-analysis. J Pain Symptom Manag. 2020;59(3):734–749 e710.
Yin Z, Li J, Ma K, Ning X, Chen H, Fu H, et al. Development of Palliative Care in China: A Tale of Three Cities. Oncologist. 2017;22(11):1362–7.
Wu Y, Li L, Su H, Yao X, Wen M. Hospice and Palliative Care: Development and Challenges in China. Clin J Oncol Nurs. 2016;20(1):E16–9.
Henoch I, Carlander I, Holm M, James I, Sarenmalm EK, Hagelin CL, et al. Palliative care research--a systematic review of foci, designs and methods of research conducted in Sweden between 2007 and 2012. Scand J Caring Sci. 2016;30(1):5–25.
Gysels M, Evans N, Menaca A, Andrew EV, Bausewein C, Gastmans C, et al. Culture is a priority for research in end-of-life care in Europe: a research agenda. J Pain Symptom Manag. 2012;44(2):285–94.
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gotzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. 2009;339:b2700.
Munn Z, Peters MDJ, Stern C, Tufanaru C, McArthur A, Aromataris E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med Res Methodol. 2018;18(1):143.
Peters MDJ, Marnie C, Tricco AC, Pollock D, Munn Z, Alexander L, et al. Updated methodological guidance for the conduct of scoping reviews. JBI Evid Synth. 2020;18(10):2119–26.
Enhancing the Quality and Transparency of health Research. Equator-network.org; 2021 [Available from: https://www.equator-network.org Accessed 24 April 2021. 2021.
Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15(9):1277–88.
Lucas PJ, Baird J, Arai L, Law C, Roberts HM. Worked examples of alternative methods for the synthesis of qualitative and quantitative research in systematic reviews. BMC Med Res Methodol. 2007;7:4.
Liao J, Yang YF, Cohen L, Zhao YC, Xu Y. Effects of Chinese medicine five-element music on the quality of life for advanced cancer patients: a randomized controlled trial. Chin J Integr Med. 2013;19(10):736–40.
Zhuang H, Ma Y, Wang L, Zhang H. Effect of early palliative care on quality of life in patients with non-small-cell lung cancer. Curr Oncol. 2018;25(1):e54–8.
Ni P, Zhou J, Wang ZX, Nie R, Phillips J, Mao J. Advance directive and end-of-life care preferences among nursing home residents in Wuhan, China: a cross-sectional study. J Am Med Dir Assoc. 2014;15(10):751–6.
Zuo D, Li S, Mao W, Chi I. End-of-life family caregiving for older parents in China's Rural Anhui province. Can J Aging. 2014;33(4):448–61.
Brannstrom M, Boman K. Effects of person-centred and integrated chronic heart failure and palliative home care. PREFER: a randomized controlled study. Eur J Heart Fail. 2014;16(10):1142–51.
Holm M, Arestedt K, Carlander I, Furst CJ, Wengstrom Y, Ohlen J, et al. Short-term and long-term effects of a psycho-educational group intervention for family caregivers in palliative home care - results from a randomized control trial. Psychooncology. 2016;25(7):795–802.
Brannstrom M, Furst CJ, Tishelman C, Petzold M, Lindqvist O. Effectiveness of the Liverpool care pathway for the dying in residential care homes: An exploratory, controlled before-and-after study. Palliat Med. 2016;30(1):54–63.
Pedersen K, Bjorkhem-Bergman L. Tactile massage reduces rescue doses for pain and anxiety: an observational study. BMJ Support Palliat Care. 2018;8(1):30–3.
Nordstrom M, Strang P. High Degree of Satisfaction With the Support Given by Multidisciplinary Palliative Home Care Teams in the County of Stockholm. J Palliat Care. 2018;33(2):109–14.
Cronfalk BS, Strang P, Ternestedt BM, Friedrichsen M. The existential experiences of receiving soft tissue massage in palliative home care--an intervention. Support Care Cancer. 2009;17(9):1203–11.
Alvariza A, Arestedt K, Boman K, Brannstrom M. Family members' experiences of integrated palliative advanced home and heart failure care: A qualitative study of the PREFER intervention. Palliat Support Care. 2018;16(3):278–85.
Talabani N, Angerud KH, Boman K, Brannstrom M. Patients' experiences of person-centred integrated heart failure care and palliative care at home: an interview study. BMJ Support Palliat Care. 2020;10(1):e9.
Norinder M, Goliath I, Alvariza A. Patients' experiences of care and support at home after a family member's participation in an intervention during palliative care. Palliat Support Care. 2017;15(3):305–12.
Swall A, Craftman A, Grundberg A, Wiklund E, Valiaho N, Hagelin CL. Dog handlers' experiences of therapy dogs' impact on life near death for persons with dementia. Int J Palliat Nurs. 2019;25(2):65–71.
Alftberg A, Ahlstrom G, Nilsen P, Behm L, Sandgren A, Benzein E, et al. Conversations about Death and Dying with Older People: An Ethnographic Study in Nursing Homes. Healthcare (Basel). 2018;6(2):63. https://doi.org/10.3390/healthcare6020063.
St John PD, Menec V, Tyas SL, Tate R, Griffith L. Multimorbidity in Canadians living in the community: Results from the Canadian Longitudinal Study of Aging. Can Fam Physician. 2021;67(3):187–97.
Zhang Y, Zhou L, Liu S, Qiao Y, Wu Y, Ke C, et al. Prevalence, correlates and outcomes of multimorbidity among the middle-aged and elderly: Findings from the China Health and Retirement Longitudinal Study. Arch Gerontol Geriatr. 2020;90:104135.
Zheng DD, Loewenstein DA, Christ SL, Feaster DJ, Lam BL, McCollister KE, et al. Multimorbidity patterns and their relationship to mortality in the US older adult population. PLoS One. 2021;16(1):e0245053.
Evans CJ, Ison L, Ellis-Smith C, Nicholson C, Costa A, Oluyase AO, et al. Service Delivery Models to Maximize Quality of Life for Older People at the End of Life: A Rapid Review. Milbank Q. 2019;97(1):113–75.
Oriani A, Fusi-Schmidhauser T, Guo P. Should end-of-life patients be enrolled as participants in clinical research? A best-fit framework synthesis. J Adv Nurs. 2021;77(4):1656–66.
World Medical Association. WMA Declaration of Helsinki – Ethical principles for medical research involving human subjects. Fortaleza: WMA General Assembly; 2013.
Bloomer MJ, Hutchinson AM, Brooks L, Botti M. Dying persons' perspectives on, or experiences of, participating in research: An integrative review. Palliat Med. 2018;32(4):851–60.
Ke LS, Huang X, Hu WY, O'Connor M, Lee S. Experiences and perspectives of older people regarding advance care planning: A meta-synthesis of qualitative studies. Palliat Med. 2017;31(5):394–405.
Kent B, McCormack B. Clinical context for evidence-based nursing practice. Chichester: Wiley-Blackwell; 2010.
Lu Y, Gu Y, Yu W. Hospice and Palliative Care in China: Development and Challenges. Asia Pac J Oncol Nurs. 2018;5(1):26–32.
Duan Y, Xu Z, Deng J, Lin Y, Zheng Y, Chen J, et al. A scoping review of cohort studies assessing traditional Chinese medicine interventions. BMC Complement Med Ther. 2020;20(1):361.
Lefebvre C, Glanville J, Briscoe S, Littlewood A, Marshall C, Metzendorf M-I, et al. Chapter 4: Searching for and selecting studies. In: JPT H, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA, editors. Cochrane Handbook for Systematic Reviews of Interventions version 6.2 (updated February 2021): Cochrane; 2021. Available from www.training.cochrane.org/handbook.
Acknowledgements
We would like to thank Matthias Bank and Carola Tilgman, information specialists and librarians at Library & ICT, the Faculty of Medicine of Lund University, for valuable work with the literature search process through systematic data curation of articles and screening procedures of double hits in the databases. We would also like to thank Lina Behm, who participated in the first step of reviewing the abstracts.
Funding
Open access funding provided by Lund University. The study was supported by grants from the National Natural Science Fund of China (Grant number: 81611130077), the Swedish Research Council (Grant number: 2015-06243), the Faculty of Medicine at Lund University, Sweden and the Third People’s Hospital of Kunming, Kunming City, China. The funders had no role in the design of the study, data collection, data analysis, interpretation of data, or writing of the manuscript.
Author information
Authors and Affiliations
Contributions
Conceptualization: GA, LC, PT, HH; Data curation: MB, CT, GA, MP; Reviewing articles: GA, JH, BHR, CB, EIP, MP; Formal analysis: GA, JH; Funding acquisition: GA, HH, LC; Methodology: GA; Writing – original draft: GA; Writing – review & editing: GA, HH, YL, LX, CB, BHR, EIP, LC, PT, MP, JH. The authors read and approved the final manuscript.
Authors’ information
Gerd Ahlström RN, PhD, Professor of Nursing and researcher in elderly care, Lund University, Lund.
Hongli Huang MD, Chief Physician at, and Vice-President of, the Third People’s Hospital of Kunming, Kunming City.
Yu Luo MD, MSc, Deputy Chief Physician, Director of Department of Hospice Care, the Third People’s Hospital of Kunming, Kunming City.
Christina Bökberg RN, PhD, researcher in elderly care, Lund University, Lund.
Birgit H Rasmussen RN, PhD, Professor of Palliative Care at the Institute for Palliative Care, Region Skåne and Lund University, Lund.
Eva I Persson RN, PhD, Associate Professor, Director of the Research Group Health-promoting Complex Interventions, Lund University, Lund.
Lian Xue RN, MSc, Deputy Chief Nurse, Head Nurse of the Department of Hospice Care, the Third People’s Hospital of Kunming, Kunming City.
Le Cai PhD, Professor of Public Health, Associate Dean at Kunming Medical University, Kunming.
Pingfen Tang RN, Professor of Nursing at Kunming Medical University and advisor at the Department of Hospice Care, the Third People’s Hospital of Kunming, Kunming City.
Magnus Persson PhD and research coordinator at the Department of Health Sciences, Faculty of Medicine, Lund University, Lund.
Jingjing Huang MSc, research coordinator at the Third People’s Hospital of Kunming, Kunming City.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable for this study design.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Identified articles from mainland China and reason of exclusion in the pilot test for all years up to 2007 before the main systematic literature.
Additional file 2.
Literature search for China and Sweden.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Ahlström, G., Huang, H., Luo, Y. et al. Similarities and differences between China and Sweden regarding the core features of palliative care for people aged 60 or older: a systematic scoping review. BMC Palliat Care 21, 35 (2022). https://doi.org/10.1186/s12904-022-00906-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12904-022-00906-7