
Abstract
Background
This study aimed to compare the age-related positional and morphological characteristics of the temporomandibular joint (TMJ) between individuals with anterior openbite or crossbite and controls.
Methods
This multi-cross-sectional comparative study analysed cone-beam computed tomography images of 750 participants, equally divided into the openbite, crossbite, and control groups (OBG, CBG, and CG, respectively). Each group was further divided into five subgroups (8–11 years, 12–15 years, 16–19 years, 20–24 years, and 25–30 years). Measurements of the TMJ included the position of the condyles in their respective fossae and morphology of the condyles and fossae. Data were submitted to statistical analysis. The study adhered to the STROBE Statement checklist for reporting of cross-sectional studies.
Results
Condyles were positioned more posteriorly with increasing age in all groups, and the condylar position was more posterior in the OBG than in the CBG. The articular eminence inclination increased with age in all the groups. There were significant differences in the articular eminence inclination among the three major groups at the age of > 15 years, and the condylar path was flatter in the CBG than in the OBG.
Conclusions
Age-related morphological and positional characteristics of the TMJ differed considerably among OBG, CBG and CG. Contrary to CBG, OBG was found to have relatively posterior condylar position and steeper condylar path.
Similar content being viewed by others


Background
The temporomandibular joint (TMJ) with related anatomic structures is regarded as one of the most unique and essential components of the masticatory system, and its function is critical for maintaining proper occlusion and a stable stomatognathic system. It is well known that there is a significant correlation between the morphology of the TMJ and its function [1, 2]. Because the TMJ is capable of remodeling, morphologic and positional changes are thought to be an adaptive response to functional and mechanical requirements. Accumulating evidence indicates that various occlusal conditions cause functional adaptation in the neuromuscular system that is guided by proprioceptive feedback reflexes that originate in the teeth and this adaptation leads to structural and positional changes in the TMJ due to functional loads imposed on it [3].
Incisal guidance is among the occlusal factors and is essential for a harmonious and functional occlusion that can stabilise mandibular movement, reduce applied forces, and protect anatomical structures. Many researchers have emphasised that the incisal path must be coordinated with the condylar path and proposed that incisal guidance affects condylar guidance, which in turn influences condyle position and morphology [4, 5]. Interestingly, we previously reported that the relationships between the condyle and fossa are diverse in individuals with different incisor guiding angles, and incisal guidance is related to the growth and development of the TMJ [6]. Therefore, it is reasonable to suspect that no incisal guidance would affect the position and shape of the TMJ.
Individuals with anterior openbite or anterior crossbite have no incisal guidance, which has long-term effects on the masticatory movement. The aberrant movement of the lower jaw may put pressure on the TMJ, affecting its position and morphology. Abnormal external stress can readily result in TMJ structural degeneration in patients with limited compensating ability and slowed TMJ remodelling, generating detrimental effects on the TMJ and masticatory system. Some studies have revealed that patients with anterior openbite or crossbite have an increased risk of dysfunction of the TMJ, with more signs and symptoms such as muscle tiredness and orofacial pain [7,8,9,10]. Because condylar-fossa variation is strongly correlated with TMJ dysfunction [11, 12], altered TMJ position and morphology due to the lack of incisal path must be considered when planning orthodontic and prosthetic treatments in anterior openbite and crossbite cases.
To date, the relevant quantitative investigations remain insufficient. A few studies have investigated the TMJ configuration in individuals with anterior openbite or anterior crossbite. For example, Wohlberg et al. [13] concluded that anterior crossbite is associated with a reduced eminence height, causing a flatter condylar path; Koak et al. [14] suggested that the condyle inclination is smaller in openbite patients, and the function of the TMJ is more restricted due to poor incisal guidance. Notably, assessment of growth-related remodelling changes of the TMJ requires additional time. However, these aforementioned studies covered a small age range and involved fewer observations. In addition, age-related changes in the condyle and glenoid fossa can also affect TMJ and, if not taken into account, may lead to dysfunction [15, 16]. In general, there has been a lack of research on age-related variations in position and morphology of the TMJ in individuals with anterior openbite or those with anterior crossbite.
To our knowledge, despite a large amount of literature on the relationship between TMJ structures and different malocclusions, no study has compared age-related morphological and positional features of the TMJ between individuals with anterior openbite and those with anterior crossbite. Cone-beam computed tomography (CBCT) has recently been widely used to evaluate the TMJ region with a high level of reliability [17]. Hence, this study aimed to establish and compare normative and detailed data on the position and morphology of the TMJ among openbite, crossbite and unaffected individuals and to determine possible age-related adaptive changes in the TMJ using CBCT.
Methods
Sample-size calculation and sample selection
Ethical approval for this multi-cross-sectional comparative study was granted by the Stomatological Hospital of Chongqing Medical University Ethical Committee (No.2021-026). The sample size was calculated using an alpha value of 0.05 and a power of 90% based on a pilot experiment using PASS (Version 15.0, NCSS, LLC). A total of 750 participants participated in the study.
This retrospective study was conducted on individuals who had undergone CBCT examinations from February 2015 to July 2020 at the Stomatological Hospital of Chongqing Medical University. CBCT examinations were performed for several clinical purposes, e.g., orthodontic treatment, impacted teeth extraction, and third molar resolution. A total of 3785 untreated participants were screened for eligibility, and the criteria shown in Table 1 were used to select participants.
Following the application of inclusion and exclusion criteria, 750 non-TMD participants were selected and divided into three major groups (250 participants each): (1) openbite group (OBG) (81 males and 169 females; mean age: 18.18 ± 6.17 years), (2) crossbite group (CBG) (124 males and 126 females; mean age: 18.06 ± 6.90 years), and (3) control group (CG) (92 males and 158 females; mean age: 17.89 ± 5.66 years). Based on the characteristics of the TMJ’s growth and development, each major group was further divided by chronological age into five subgroups (50 participants each): groups I (8–11 years), II (12–15 years), III (16–19 years), IV (20–24 years), and V (25–30 years).
Right and left TMJs were examined separately, and a total of 1500 TMJ cases were measured and analysed.
CBCT assessment and analysis
All CBCT (KaVo 3D exam, USA) images were obtained at the Stomatological Hospital of Chongqing Medical University (radiological parameters: 120 kV; 5 mA; voxel size, 0.4 mm; exposure time, 8.9 s; field of view, 16 × 17 cm). According to the imaging protocol, the Frankfort plane was adjusted to be parallel to the ground, and when the patient bit into maximum dental intercuspation, the CBCT scans were obtained. All images were obtained by a single radiologist.
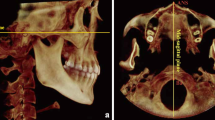
The CBCT data were analysed using the Dolphin11.9 software (Chatsworth, CA) by two investigators with experience in the evaluation of CBCT images. The Build X-Rays Tool was used to assess radiographically the anteroposterior and vertical skeletal characteristics of the participants by measuring the SNA, SNB, ANB, and FH-MP on constructed lateral images. The transverse skeletal characteristics were evaluated with the multiplanar CBCT images by measuring the maxillary basal width and the mandibular width, as described previously [19, 20]. Assessment of the TMJ position and morphology was performed in a manner similar to the studies by Chae et al. [21] and Ma et al. [22]. Initially, head-orientation images were standardised. When viewed from the front, the horizontal plane was parallel to the orbits. The skull was repositioned using the Frankfort horizontal plane, which was formed by the most superior point of the meatus acusticus externus on the right side and the most inferior point of the orbital rim on the left and right sides. To reconstruct the images of the sagittal and axial TMJ, the axial slice thickness was set to 0.5 mm to determine the largest and most pronounced condyle image on the left and right joints individually. Subsequently, the Standard Line (Fig. 1) was defined as a line tangent to the most superior point of the fossa and parallel to the Frankfort horizontal plane. Sagittal and axial measurements were performed based on the images as described as follows:

Measurements of the temporomandibular joints. a SS, superior space; AS, anterior space; PS, posterior space; b AIC, anterior inclination of the condyle; PIC, posterior inclination of the condyle; c HF, height of the fossa; WF, width of the fossa; AEH, articular eminence height; AEI, articular eminence inclination; d LAC, lateral inclination of the condyle; MAC, minor axis of the condyle
Assessments of joint spaces (Fig. 1a).
-
1.
Anterior joint space (AS), defined as the shortest distance between the most anterior point of the condyle and the posterior aspects of the articular tubercle;
-
2.
Posterior joint space (PS), defined as the shortest distance between the most posterior point of the condyle and the posterior aspects of the mandibular fossa;
-
3.
Superior joint space (SS), defined as the perpendicular distance between the most superior point of the condyle and the standard line.
Assessments of condylar morphology (Fig. 1b, d)
-
1.
Anterior inclination of the condyle (AIC), measured from the angle between the standard line and the line formed by the most superior point of the condyle to the point formed by the line drawn from the most superior point of the fossa tangent to the anterior aspects of the condylar head;
-
2.
Posterior inclination of the condyle (PIC), measured from the angle between the standard line and the line formed by the most superior point of the condyle to the point formed by the line drawn from the most superior point of the fossa tangent to the posterior aspects of the condylar head;
-
3.
Long axis of the condyle (LAC), the largest mediolateral diameter of the mandibular condylar processes;
-
4.
Minor axis of the condyle (MAC), the largest anteroposterior diameter of the mandibular condylar processes.
Assessment of fossa morphology (Fig. 1c).
-
1.
Height of the fossa (HF), defined as the perpendicular distance between the most superior point of the fossa and the line formed by the most inferior point of the articular tubercle to the most inferior point of the postglenoid process;
-
2.
Width of the fossa (WF), defined as the distance between the most inferior point of the articular tubercle and the most inferior point of the postglenoid process;
-
3.
Articular eminence height (AEH), defined as the perpendicular distance between the most inferior point of the articular tubercle and standard line;
-
4.
Articular eminence inclination (AEI), defined as the angle between the standard line and the best fit line on the posterior surface of the articular eminence.
Furthermore, according to Pullinger and Hollender [23], the anteroposterior condylar joint position (APCJP) was evaluated using the following formula: PS − AS/PS + AS × 100. A positive score indicates that the position is anterior, whereas a negative value indicates that the location is posterior.
Reliability/reproducibility of the method
To ensure intra- and inter-examiner reliability, 50 randomly selected samples were analysed twice by two different observers within 20-day intervals. Intraclass correlation coefficients (ICCs) were used to assess the reliability and reproducibility of the measurements. Both results showed excellent test–retest reliability (ICC = 0.97–1.00), indicating that the reproducibility of the evaluation method was statistically acceptable.
Statistical procedures
Data were analysed using the Statistical Package for the Social Sciences software, version 26 (IBM Corp, USA). The normality of data was confirmed using the Kolmogorov–Smirnov test, and all data were normally distributed. Quantitative data are presented as mean ± standard deviation (SD).
A paired t-test was performed to compare the left and right sides of the TMJ, and we found no statistical differences for any of the measurements (P > 0.1) (Additional file 1). The right and left TMJs were considered one unit, and the variables were averaged for subsequent analyses. The trend between age and TMJ characteristics was assessed using a linear trend test (P for trend). For intergroup comparisons, one-way analysis of variance (ANOVA) and Tukey’s post hoc test were used to determine statistically significant differences among various groups. A two-way multivariate ANOVA (two-way MANOVA) was performed to estimate the composite effect of age and occlusal characteristics of anterior teeth on the TMJ. Statistical significance was set at P < 0.05.
This study followed the STROBE statement for reports of observational studies (Additional file 2).
Results
Table 2 shows the anteroposterior, vertical, and transverse skeletal features of the selected sample, with matched groups in the anteroposterior, vertical, and transverse relation to rule out the influence of these factors on the condyle-fossa relationship.
Joint spaces and condylar position
Linear trend tests suggested a trend toward increased mean SS with age in each major group (P < 0.005). Regarding the AS, statistically significant trends were observed in the three major groups (P = 0.001, P = 0.021, and P = 0.001, respectively). At the age of 12–15 years, the AS of the OBG was the largest, and that of the CG was the smallest. Additionally, changes of the PS in the CG (P = 0.002) and CBG (P = 0.021) with increasing age were statistically significant (Tables 3 and 4).
The APCJP decreased with increasing age, and the condyles of all three major groups were positioned significantly more posteriorly (P < 0.001, P = 0.003, and P < 0.001, respectively). Moreover, the condyle position was mainly anterior and concentric in the CBG and was relatively posterior in the OBG (Fig. 2a; Tables 3 and 4).

Box-and-whisker plots showing the temporomandibular joint measurements of different age subgroups. Significant differences were defined by the means of the linear trend test (*P < .05. **P < .01. ***P < .001). a APCJP, anteroposterior condylar joint position; b HF, height of the fossa; c WF, width of the fossa; d AEI, articular eminence inclination; e AEH, articular eminence height; f AIC, anterior inclination of the condyle
Condylar morphology
The AIC significantly increased with increasing age in the three main groups (P < 0.001, P = 0.008, and P = 0.004, respectively). ANOVA indicated significant differences in the AIC among the three major groups, and the AIC of the OBG was smaller than that of the CG but greater than that of the CBG at the ages of 12–15 (P < 0.001), 16–19 (P = 0.006), and 20–24 (P = 0.008) years (Fig. 2f; Tables 3 and 4). However, there were no statistically significant trends in the PIC with age in each major group (Tables 3 and 4).
With the increase in age, the LAC increased (from 8–11 years to 25–30 years) (P < 0.001) and was significantly longer in the CBG than in the CG and OBG at the ages of 12–15 (P = 0.001), 20–24 (P = 0.017), and 25–30 (P = 0.004) years. The MAC tended to increase with age in the OBG (P = 0.027) and CBG (P < 0.001). The only significant MAC difference was detected among three major groups at 8–11 years of age (P = 0.048) (Tables 3 and 4).
Fossa morphology
The average HF increased first and then decreased with age in the CG (P = 0.031), OBG (P = 0.917), and CBG (P = 0.054). The turning point of the CG (20–24 years) was different from that of the other two major groups (16–19 years). No significant differences were found among the three major groups (Fig. 2b; Tables 3 and 4).
The WF tended to increase from 8–11 to 16–19 years, and then decreased with increasing age in all major groups. Significant differences were observed in WF among the three major groups at the ages of 8–11 (P = 0.001), 12–15 (P = 0.005), 16–19 (P = 0.018), and 25–30 (P < 0.001) years (Fig. 2c; Tables 3 and 4).
The AEH increased with age in all three major groups, but the trends were statistically significant only in the CG (P = 0.011) and CBG (P < 0.001). In the same age groups, the AEH of the OBG was smaller than that of the CG but greater than that of the CBG (Fig. 2e; Tables 3 and 4).
The AEI tended to increase with age in the OBG (P = 0.017), CBG (P = 0.047), and CG (P < 0.001). The AEI was flatter in the CBG than in the CG and OBG at the ages of 16–19(P = 0.031), 20–24(P = 0.002) and 25–30 (P = 0.001) years (Fig. 2d; Tables 3 and 4).
Effects of age or/and occlusal characteristics of anterior teeth on TMJ
Two-way MANOVA (Table 5) showed that age and occlusal characteristics of anterior teeth significantly affected the TMJ. However, no composite effect was observed in any of the measurements.
Discussion
The TMJ position and morphology varies among individuals and can be altered by a variety of factors, including the functional pressures exerted on it. This could be attributed to the close link between shape and function, which varies depending on occlusal characteristics [24]. Incisal guidance is one of the occlusal factors which can stabilise the movement of the condyle and maintain the health of the oral and craniofacial structures [25]. Therefore, abnormal movement of the lower jaw without incisor guidance may affect the shape, position, and function of the TMJs and masticatory system over time. Thus, understanding of the condyle-fossa relationships in anterior openbite and crossbite (no incisal guidance) could provide insights into the pathological effects of no incisal guidance on the TMJ. To the best of our knowledge, this study is the first to evaluate the TMJ characteristics in different age groups with anterior openbite or crossbite compared with their unaffected peers.
Investigating the effect of anterior openbite and crossbite on the position and shape of the TMJ anatomy was the primary objective of this study. Additionally, developmental and adaptive changes of the TMJ are age-related. The growth and development of the mandibular condyle are strongly linked to the growth and development of the mandible. It has been reported that there are two periods of increased growth of the TMJ: between the ages of 5 and 10 years and between the ages of 10 and 15, with the craniofacial growth stopping around the age of 20 [26, 27]. Katsavrias et al. [28] reported that the articular eminence height increases rapidly until the age of 7 years, then slows until the age of 11 years, regaining its full height by the age of 20 years. Sülün et al. [29] reported that the eminence inclination in healthy patients peaks between the ages of 21 and 30 years. Based on the TMJ’s growth and development characteristics, subjects were divided into five age groups to explore the age-related changes in the condyle and glenoid fossa, which was the second objective of this study.
In the present study, the condyles were more posteriorly positioned with age (P < 0.05); this finding aligns with the results obtained by Cohlmia et al. [30], indicating that the condyle-glenoid fossa relationship changes with increasing age. However, Liu et al. [31] failed to find a changing tendency in condylar position with increasing age, probably due to different age ranges in various age groups.
Moreover, we found that the condyle position was mainly anterior and concentric in the anterior crossbite. This finding contradicts that of Cohlmia et al. [30], who found no significant differences between patients with and without anterior crossbites in the condylar position. This discrepancy potentially results from the different inclusion criteria since patients with other types of malocclusions were also included in their study. Additionally, we observed that the position of the condyle in openbite was relatively posterior. The condyle position refers to the relative position of the condylar in the mandibular fossa in concentric occlusion and is the final product of many dynamic changes, which are related to growth, remodelling, and response to functional changes and so on [32, 33]. Different occlusal circumstances lead to different stress distributions in the TMJ, as described previously [34]. Thus, the position of the TMJ, which is affected by the pressures load on it, varies. The position of the lower incisors locating on the labial side of the opposing upper teeth, as an occlusal characteristic of the anterior crossbite, affects the mandibular movement guided by neuromuscular reflexes, which possibly changes the position of the condylar for functional adaptation. Furthermore, in anterior openbite individuals, no contact between the upper and lower teeth in the vertical direction might also influence the motion trajectory of the mandible; thus, the condyle position is relatively backward. To sum up, the position of the TMJ is subjected to a variety of functional and mechanical stresses during oral function, depending on the subject’ occlusal characteristics. Additionally, the sagittal position of the condyle is associated with TMJ dysfunction because the posterior position of the condyle may exert pressure on the retrodiscal tissues and sensory nerves, leading to TMD [35]. The higher incidence of the posterior condylar position suggests the anatomical preponderance of TMD and disk instability in anterior openbite; this finding is in line with the increased prevalence of clinical signs and symptoms of TMD in anterior openbite [9, 36].
Regarding the HF and WF, the trends of these data first increased and then decreased with increasing age in the three major groups, except that the turning point of the HF in the CG was different from that in the other two major groups. Different turning points might have been caused by the incisor guidance; the early increase may be the result of growth and development, while the late decrease is viewed as an adaptive response due to functional and mechanical constraints [6]. Except for the largest fossa width, the HF was lower in the CBG than in the other two groups; consistently, the AEH was lowest in the CBG. These results suggest that individuals with anterior crossbite have relatively shallow and wide glenoid fossa.
The orbit of the condyle, which moves out of the most superior and anterior position from the glenoid fossa, is guided by the posterior wall of the articular eminence and is commonly termed ‘condylar guidance’. Hence, the AEH and AEI influence the condylar path. In our study, AEH and AEI showed a sustained increase with ageing in each major group, and the AIC also increased with ageing; the findings are consistent with previous results [6, 37, 38]. Due to the coordination between AIC, AEI, and AEH in anatomical structure and jaw movement, their changing trends with age are similar. Moreover, some researchers [39] demonstrated that steeper articular eminences forced posterior disk rotation more prominently because of larger vertical movement upon opening as the condyle shifts anteriorly. Therefore, considering the peak age of TMD involvement, the steeper inclination of articular eminences at the ages of 20–30 years could be an anatomical aetiology. Because the aetiological and pathophysiological factors of TMD are complicated, factors such as psychoemotional stress may potentially influence the muscular endurance and masticatory system, consequently affecting the shape and position of the TMJ. Consistent with it, Wieckiewicz et al. [40] assessed the prevalence of TMD among Polish university students and demonstrated that emotional burden is a risk factor for muscular disorders which can impair the adaptive capacity of the masticatory system and may lead to a greater risk of TMD.
This study indicated significant differences in AEI among the three major groups at the age of > 15 years. Moreover, we found that the AEI of the CBG was significantly smaller than that of the CG, probably due to the flattening of the condylar path in the CBG; this finding is consistent with that of Wohlberg et al. [13]. The main reason for these results may be the occlusal characteristics in the CBG, which plays a role in the mastication pattern controlled by neuromuscular elements. The neuromuscular reflex changes the contractility of the masticatory muscles, thereby affecting the stress of the TMJ, which is the underlying cause of joint remodelling. Although no statistically significant differences were found between the CG and OBG, the condylar inclination of the OBG was flatter than that of the CG. This result agrees with those of previous studies regarding mandibular movement in patients with openbite and could be explained by the limitations of the effect of incisal guidance, as described by Koak et al. [14]. Moreover, the condylar path in the OBG was steeper than that in the CBG, suggesting that masticatory function in anterior openbite participants differed from that in anterior crossbite participants and mechanical force loaded on the TMJ was thus altered, thereby causing a difference in the condylar path. Consistently, Thorsten et al. [41] demonstrated that functional demands influence jaw muscles, which are able to modify their anatomical features, such as dimensions, cross-sectional area, and fibre phenotype. Taken together, the condylar path is affected by the incisal guidance; this result is in accordance with the conclusion of Hickey et al. [42] that incisal guidance has some influence on condylar guidance.
Accumulating evidence indicates that the condyle-fossa relationship is related to a variety of factors, such as age [15, 16], sex [21, 30] and occlusal factors (e.g., incisal guidance, tooth loss, and dental abrasion) [6, 38, 43]. Our results, similar to others, indicated that age and occlusal features of anterior teeth influenced the TMJ characteristics, but no composite effect of both was found. However, whether interactions between other correlative factors associated with TMJ exist and how they interact with each other should be further investigated in future studies considering the lack of previous related reports.
Functions and morphology are closely linked. It is widely recognized that pressure originating from the contractility of the masticatory muscles during chewing movements can affect the TMJ. This relationship implies that the position and morphology of the TMJ are somewhat determined by the forces pressing on it. Maeda et al. [44] suggested that the proliferation and matrix synthesis of condylar chondrocytes would be influenced by the pressure exerting on the TMJ, which is consistent with this assumption. Various occlusal conditions result in functional adaptation in the neuromuscular system which is guided by proprioceptive feedback reflexes that originate in the teeth [3]. This adaptation, in turn, influences the jaw muscles and causes structural and positional changes in the TMJ due to functional loads imposed on it. Thus, the TMJ loading differs between persons with specific occlusal conditions and those having other dentofacial morphologies, as does mechanical stress on the TMJ during oral function [34, 45, 46]. Taken together, incisor guidance has important implications for mandibular movement. The movement of the condyle, muscular contraction, neuromuscular health, TMJ, and associated structures in individuals with anterior openbite and crossbite will be disturbed without incisal guidance [47, 48], thus changing the condyle-fossa relationships, which the results of this study can support.
This study has some limitations. Longitudinal data could better explain the relationship between the shape and position of the TMJ and incisor guidance than multi-cross-sectional data. In addition, more detailed analyses of clinical data, such as muscle myoelectric activity and biting force, are required for further evaluation.
Conclusions
This study compared age-related variations in the position and morphology of the TMJ among the control, openbite, and crossbite groups. We found significant differences in condyle-fossa relationships and trends with age among the three groups. Contrary to the crossbite groups, individuals with anterior openbite were found to have relatively posterior condylar position and steeper condylar path. These findings can be clinically useful when evaluating the position and morphology of the TMJ with CBCT images in individuals with anterior openbite and crossbite.
Availability of data and materials
The data that support the findings of this study are available from the Stomatological Hospital of Chongqing Medical University, but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of the Stomatological Hospital of Chongqing Medical University.
Abbreviations
- AEH:
-
Articular eminence height
- AEI:
-
Articular eminence inclination
- AIC:
-
Anterior inclination of the condyle
- ANOVA:
-
Analysis of variance
- APCJP:
-
Anteroposterior condylar joint position
- AS:
-
Anterior joint space
- CBCT:
-
Cone-beam computed tomography
- CBG:
-
Crossbite group
- CG:
-
Control group
- HF:
-
Height of the fossa
- ICCs:
-
Intraclass correlation coefficients
- LAC:
-
Long axis of the condyle
- MAC:
-
Minor axis of the condyle
- OBG:
-
Openbite group
- PIC:
-
Posterior inclination of the condyle
- PS:
-
Posterior joint space
- SD:
-
Standard deviation
- SS:
-
Superior joint space
- TMJ:
-
Temporomandibular joint
- TMD:
-
Temporomandibular disorders
- WF:
-
Width of the fossa
References
Jiang H, Li C, Wang Z, Cao J, Shi X, Ma J, et al. Assessment of osseous morphology of temporomandibular joint in asymptomatic participants with chewing-side preference. J Oral Rehabil. 2015;42:105–12. https://doi.org/10.1111/joor.12240.
Fanghänel J, Gedrange T. On the development, morphology and function of the temporomandibular joint in the light of the orofacial system. Ann Anat. 2007;189:314–9. https://doi.org/10.1016/j.aanat.2007.02.024.
Slavicek R. Masticatory organ. Functions and dysfuncion. 1st ed. Kloster Neuenburg: Gamma; 2000.
Ogawa T, Koyano K, Suetsugu T. The influence of anterior guidance and condylar guidance on mandibular protrusive movement. J Oral Rehabil. 1997;24:303–9. https://doi.org/10.1046/j.1365-2842.1997.00479.x.
Zoghby AE, Ré JP, Perez C. Functional harmony between the sagittal condylar path inclination and the anterior guidance inclination. J Stomat Occ Med. 2009;2:131–6. https://doi.org/10.1007/s12548-009-0024-x.
Li Y, Zhou W, Wu Y, Dai H, Zhou J. The relation between incisal guidance angle and the growth and development of temporomandibular joint: a multi-cross-sectional retrospective study. BMC Oral Health. 2021;21:380. https://doi.org/10.1186/s12903-021-01716-8.
Pullinger AG, Seligman DA, Gornbein JA. A multiple logistic regression analysis of the risk and relative odds of temporomandibular disorders as a function of common occlusal features. J Dent Res. 1993;72:968–79. https://doi.org/10.1177/00220345930720061301.
Barrera-Mora JM, Espinar Escalona E, Abalos Labruzzi C, Llamas Carrera JM, Ballesteros EJ, Solano Reina E, et al. The relationship between malocclusion, benign joint hypermobility syndrome, condylar position and TMD symptoms. Cranio. 2012;30:121–30. https://doi.org/10.1179/crn.2012.018.
Schmitter M, Balke Z, Hassel A, Ohlmann B, Rammelsberg P. The prevalence of myofascial pain and its association with occlusal factors in a threshold country non-patient population. Clin Oral Investig. 2007;11:277–81. https://doi.org/10.1007/s00784-007-0116-1.
Pahkala RH, Laine-Alava MT. Do early signs of orofacial dysfunctions and occlusal variables predict development of TMD in adolescence? J Oral Rehabil. 2002;29:737–43. https://doi.org/10.1046/j.1365-2842.2002.00956.x.
Fernández Sanromán J, Gómez González JM, del Hoyo JA. Relationship between condylar position, dentofacial deformity and temporomandibular joint dysfunction: an MRI and CT prospective study. J Craniomaxillofac Surg. 1998;26:35–42. https://doi.org/10.1016/s1010-5182(98)80033-4.
Derwich M, Mitus-Kenig M, Pawlowska E. Temporomandibular joints’ morphology and osteoarthritic changes in cone-beam computed tomography images in patients with and without reciprocal clicking—a case control study. Int J Environ Res Public Health. 2020;17:3428. https://doi.org/10.3390/ijerph17103428.
Wohlberg V, Schwahn C, Gesch D, Meyer G, Kocher T, Bernhardt O. The association between anterior crossbite, deep bite and temporomandibular joint morphology validated by magnetic resonance imaging in an adult non-patient group. Ann Anat. 2012;194:339–44. https://doi.org/10.1016/j.aanat.2011.04.013.
Koak JY, Kim KN, Heo SJ. A study on the mandibular movement of anterior openbite patients. J Oral Rehabil. 2000;27:817–22. https://doi.org/10.1046/j.1365-2842.2000.00655.x.
Karlo CA, Stolzmann P, Habernig S, Müller L, Saurenmann T, Kellenberger CJ. Size, shape and age-related changes of the mandibular condyle during childhood. Eur Radiol. 2010;20:2512–7. https://doi.org/10.1007/s00330-010-1828-1.
Reicheneder C, Gedrange T, Baumert U, Faltermeier A, Proff P. Variations in the inclination of the condylar path in children and adults. Angle Orthod. 2009;79:958–63. https://doi.org/10.2319/081108-425.1.
Barghan S, Tetradis S, Mallya S. Application of cone beam computed tomography for assessment of the temporomandibular joints. Aust Dent J. 2012;57(Suppl 1):109–18. https://doi.org/10.1111/j.1834-7819.2011.01663.x.
Schiffman E, Ohrbach R, Truelove E, Look J, Anderson G, Goulet JP, et al. Diagnostic criteria for temporomandibular disorders (DC/TMD) for clinical and research applications: recommendations of the International RDC/TMD Consortium Network* and Orofacial Pain Special Interest Group†. J Oral Facial Pain Headache. 2014;28:6–27. https://doi.org/10.11607/jop.1151.
Simontacchi-Gbologah MSTR, Boucher NS, Vanarsdall RL, Secchi AG. Comparison of three methods to analyze the skeletal transverse dimension in orthodontic diagnosis [thesis]. University of Pennsylvania; 2010.
Shah SR, Fishel D, Tamburrino R. Periodontal rationale for transverse skeletal normalization. Orthod Pract. 2014;5:50–3.
Chae JM, Park JH, Tai K, Mizutani K, Uzuka S, Miyashita W, et al. Evaluation of condyle-fossa relationships in adolescents with various skeletal patterns using cone-beam computed tomography. Angle Orthod. 2020;90:224–32. https://doi.org/10.2319/052919-369.1.
Ma Q, Bimal P, Mei L, Olliver S, Farella M, Li H. Temporomandibular condylar morphology in diverse maxillary-mandibular skeletal patterns: a 3-dimensional cone-beam computed tomography study. J Am Dent Assoc. 2018;149:589–98. https://doi.org/10.1016/j.adaj.2018.02.016.
Pullinger A, Hollender L. Variation in condyle-fossa relationships according to different methods of evaluation in tomograms. Oral Surg Oral Med Oral Pathol. 1986;62:719–27. https://doi.org/10.1016/0030-4220(86)90270-7.
Alhammadi MS, Fayed MS, Labib A. Three-dimensional assessment of temporomandibular joints in skeletal Class I, Class II, and Class III malocclusions: cone beam computed tomography analysis. J World Fed Orthod. 2016;5:80–6.
Broderson SP. Anterior guidance—the key to successful occlusal treatment. J Prosthet Dent. 1978;39:396–400. https://doi.org/10.1016/s0022-3913(78)80155-3.
Smartt JM, Low DW, Bartlett SP. The pediatric mandible: I. A primer on growth and development. Plast Reconstr Surg. 2005;116:14e–23e.
Bender ME, Lipin RB, Goudy SL. Development of the pediatric temporomandibular joint. Oral Maxillofac Surg Clin North Am. 2018;30:1–9. https://doi.org/10.1016/j.coms.2017.09.002.
Katsavrias EG, Dibbets JM. The growth of articular eminence height during craniofacial growth period. Cranio. 2001;19:13–20. https://doi.org/10.1080/08869634.2001.11746146.
Sülün T, Cemgil T, Duc JM, Rammelsberg P, Jäger L, Gernet W. Morphology of the mandibular fossa and inclination of the articular eminence in patients with internal derangement and in symptom-free volunteers. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001;92:98–107. https://doi.org/10.1067/moe.2001.114621.
Cohlmia JT, Ghosh J, Sinha PK, Nanda RS, Currier GF. Tomographic assessment of temporomandibular joints in patients with malocclusion. Angle Orthod. 1996;66:27–35. https://doi.org/10.1043/0003-3219(1996)066%3c0027:TAOTJI%3e2.3.CO;2.
Liu Q, Wei X, Guan J, Wang R, Zou D, Yu L. Assessment of condylar morphology and position using MSCT in an Asian population. Clin Oral Investig. 2018;22:2653–61. https://doi.org/10.1007/s00784-018-2364-7.
Goldstein BH. Temporomandibular disorders: a review of current understanding. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999;88:379–85. https://doi.org/10.1016/s1079-2104(99)70048-x.
Abdel-Fattah RA. Optimum temporomandibular joint (TMJ) condylar position. Todays FDA. 1989;1:1C-3C.
Ueki K, Nakagawa K, Marukawa K, Takatsuka S, Yamamoto E. The relationship between temporomandibular joint disc morphology and stress angulation in skeletal Class III patients. Eur J Orthod. 2005;27:501–6. https://doi.org/10.1093/ejo/cji029.
Shokri A, Zarch HH, Hafezmaleki F, Khamechi R, Amini P, Ramezani L. Comparative assessment of condylar position in patients with temporomandibular disorder (TMD) and asymptomatic patients using cone-beam computed tomography. Dent Med Probl. 2019;56:81–7. https://doi.org/10.17219/dmp/102946.
Manfredini D, Vano M, Peretta R, Guarda-Nardini L. Jaw clenching effects in relation to two extreme occlusal features: patterns of diagnoses in a TMD patient population. Cranio. 2014;32:45–50. https://doi.org/10.1179/0886963413Z.0000000009.
Katsavrias EG. Changes in articular eminence inclination during the craniofacial growth period. Angle Orthod. 2002;72:258–64. https://doi.org/10.1043/0003-3219(2002)072%3c0258:CIAEID%3e2.0.CO;2.
Hinton RJ. Changes in articular eminence morphology with dental function. Am J Phys Anthropol. 1981;54:439–55. https://doi.org/10.1002/ajpa.1330540402.
Atkinson WB, Bates RE Jr. The effects of the angle of the articular eminence on anterior disk displacement. J Prosthet Dent. 1983;49:554–5. https://doi.org/10.1016/0022-3913(83)90321-9.
Wieckiewicz M, Grychowska N, Wojciechowski K, Pelc A, Augustyniak M, Sleboda A, et al. Prevalence and correlation between TMD based on RDC/TMD diagnoses, oral parafunctions and psychoemotional stress in Polish university students. BioMed Res Int. 2014;2014: 472346. https://doi.org/10.1155/2014/472346.
Grünheid T, Langenbach GE, Korfage JA, Zentner A, van Eijden TM. The adaptive response of jaw muscles to varying functional demands. Eur J Orthod. 2009;31:596–612. https://doi.org/10.1093/ejo/cjp093.
Hickey JC, Allison ML, Woelfel JB, Boucher CO, Stacy RW. Mandibular movements in three dimensions. J Prosthet Dent. 1963;13:72–92. https://doi.org/10.1016/0022-3913(63)90199-9.
Granados JI. The influence of the loss of teeth and attrition on the articular eminence. J Prosthet Dent. 1979;42:78–85. https://doi.org/10.1016/0022-3913(79)90333-0.
Maeda S, Nishida J, Sato T, Inomata Y, Shimamura T, Horiuchi S. Changes in microstructure and gene expression of articular chondrocytes cultured in a tube under mechanical stress. Osteoarthritis Cartil. 2005;13:154–61. https://doi.org/10.1016/j.joca.2004.10.019.
O’Ryan F, Epker BN. Temporomandibular joint function and morphology: observations on the spectra of normalcy. Oral Surg Oral Med Oral Pathol. 1984;58:272–9. https://doi.org/10.1016/0030-4220(84)90052-5.
Tanne K, Tanaka E, Sakuda M. Stress distributions in the TMJ during clenching in patients with vertical discrepancies of the craniofacial complex. J Orofac Pain. 1995;9:153–60.
Kerstein RB, Farrell S. Treatment of myofascial pain-dysfunction syndrome with occlusal equilibration. J Prosthet Dent. 1990;63:695–700. https://doi.org/10.1016/0022-3913(90)90328-a.
Williamson EH, Lundquist DO. Anterior guidance: its effect on electromyographic activity of the temporal and masseter muscles. J Prosthet Dent. 1983;49:816–23. https://doi.org/10.1016/0022-3913(83)90356-6.
Acknowledgements
We would like to acknowledge JZ in the promotion of this study.
Funding
This study was supported by the National Science Foundation for Young Scientists of China [Grant No. 31800818] and the Program for the Natural Science Foundation of Chongqing, China [cstc2020jcyj-msxmX0191].
Author information
Authors and Affiliations
Contributions
YC designed the work and drafted the manuscript. JW and YL were responsible for collecting the data. YL and LL performed the statistical analysis. NL, YW, and HD contributed to the approval of the final version of the manuscript. JZ was a project administrator and reviewed and edited the manuscript. All authors read and approved the final version of this manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval for this multi-cross-sectional comparative study was granted by the Stomatological Hospital of Chongqing Medical University Ethical Committee (NO.2021-026). All participants and their legal guardians or legally authorised representatives gave informed consent prior to participation. We confirm that all methods were performed in accordance with the relevant guidelines and regulations.
Consent for publication
All presentations of case reports must have consent for publication.
Competing interests
The authors declare no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1
. Side comparison of the measurements among three major groups.
Additional file 2
. STROBE Statement—checklist of items that should be included in reports of observational studies.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Chen, Y., Wang, J., Li, Y. et al. Age-related variations in position and morphology of the temporomandibular joint in individuals with anterior openbite and crossbite: a multi-cross-sectional comparative study. BMC Oral Health 22, 200 (2022). https://doi.org/10.1186/s12903-022-02236-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12903-022-02236-9