
Abstract
Objective
Rotator cuff tear is a common shoulder injury that often leads to serious limitations in daily life. Herein, a network Meta-analysis using frequency theory was performed to evaluate the clinical outcomes of five rotator cuff repair techniques, including single-row repair, double-row repair, suture bridge repair, platelet-rich plasma therapy, and bone marrow stimulation, thus guiding clinical decision-making on rotator cuff repair.
Methods
PubMed, EMbase, The Cochrane Library, and Web of Science were searched for randomized controlled trials and cohort studies comparing rotator cuff repair techniques published from inception to May 2022. Combined analysis and quality assessment were performed using software STATA15.1 and Review Manager5.3.
Results
A total of 51 articles were finally included, including 27 randomized controlled trials and 24 cohort studies. Results from the network Meta-analysis showed that: (1) In terms of the American Shoulder and Elbow Surgeons score, platelet-rich plasma therapy, double-row repair, bone marrow stimulation, and single-row repair were significantly better than suture bridge repair. (2) In terms of Constant score, bone marrow stimulation was significantly better than double-row repair, single-row repair, and suture bridge repair. (3) In terms of visual analog scale score, platelet-rich plasma therapy was significantly better than double-row repair and suture bridge repair. (4) In terms of the Shoulder Rating Scale of the University of California at Los Angeles score, platelet-rich plasma therapy and double-row repair were relatively better but not significantly different from the other treatments. (5) In terms of the risk of re-tear, the re-tear rate of platelet-rich plasma therapy and double-row repair was significantly lower than that of single-row repair and suture bridge repair.
Conclusion
Based on the results of network Meta-analysis and surface under the cumulative ranking, platelet-rich plasma therapy, bone marrow stimulation, and double-row repair have good overall rehabilitation effects. It is recommended to choose appropriate repair techniques as per the actual clinical situation.
Similar content being viewed by others


Introduction
The rotator cuff is an important organ that stabilizes the humeral head on the glenoid and plays an important role in maintaining shoulder flexion and abduction. Rotator cuff tear is a common rotator cuff injury, mostly in middle-aged and elderly patients, which is mainly manifested as shoulder pain and shoulder joint dysfunction [1, 2]. Long-term treatment will cause a huge economic burden to patients. Moreover, various complications caused by rotator cuff tears will seriously affect patients’ normal life. Rotator cuff injuries are a common form of sports injury. Conventionally, rehabilitation therapy is required for early mild injuries, while surgical treatment combined with rehabilitation is needed for severe injuries.
Arthroscopic rotator cuff repair has gradually replaced open repair as the major surgical procedure for rotator cuff repair due to its advantages of small incision [3]. Single-row repair has long been the standard approach used for rotator cuff tear repair, although some works have reported incomplete postoperative healing [4,5,6] or surgical failure [7] following single-row repair. To provide a better tendon-bone healing environment, double-row repair is preferred to increase the contact area of the tendon and bone, increase the maximum load of the suture site, and reduce the risk of re-tear [8], which is widely favored by doctors and patients. A biomechanical study reported better initial fixation strength with double-row fixation compared to single-row fixation [9]. However, there are also a series of randomized controlled studies that indicate no statistical difference in clinical outcomes between the two methods. The single-row repair is simple and time-saving and can eliminate certain potential risks, especially for patients with small tears. However, for medium and large injuries, the single-row repair often has no ideal prognostic outcomes. In another randomized controlled study, MRI results showed that double-row repair was significantly better than single-row repair for rotator cuff tears with a size of > 30 mm [10].
Suture bridge repair combines the merits and demerits of single-row repair and double-row repair [11]. On the basis of double-row repair, the outer-row mesh structure is used to fix the footprint area, and the rotator cuff tissue is squeezed and fixed through the thread bridge, to obtain a larger area of contact between the tendon and bone, thereby accelerating healing. Although existing studies have shown that suture bridge repair can achieve better biomechanical properties than double-row repair, there is no sufficient clinical evidence to confirm that it has better postoperative efficacy. Therefore, further exploration is needed.
For a better surgical prognosis in rotator cuff repair and reducing the risk of postoperative re-tear, the use of adjuvant biologics has been considered. Platelet-rich plasma (PRP), a biological preparation developed in recent years, is obtained by centrifugation of whole blood, containing a variety of growth factors, which can accelerate the formation of new blood vessels and the proliferation of stem cells, promote the formation of bone matrix, improve the metabolic rate, promote tendon repair, and effectively prevent the occurrence of re-tear [12]. PRP has been widely used in medical operations. Some scholars have proposed that the efficacy of PRP depends to a certain extent on the source, preparation method, dosage, and administration regimen [13]. Given this, a more complete preparation system can make it better exert its medicinal value. Bone marrow stimulation technologies such as multi-channel technology and microfracture technology are a group of new tendon repair technologies, which are simple and easy to operate, reduce the risk of in vitro infection caused by injection of growth factors such as PRP, and quickly provide sufficient mesenchymal stem cells for tendon healing. Compared with traditional arthroscopic repair, bone marrow stimulation has better biomechanical properties. A Meta-analysis [14] has shown that bone marrow stimulation can effectively reduce the risk of re-tear, but postoperatively, the rotator cuff function has not been significantly improved. In addition, there are few published studies on bone marrow stimulation, and its repair ability remains to be further verified.
In this study, the network Meta-analysis method was used to compare the efficacy of single-row repair, double-row repair, suture bridge repair, PRP therapy, and bone marrow stimulation for the treatment of rotator cuff tears. We attempted to provide evidence-based medicine support for the optimal therapeutic regimen for the clinical repair of rotator cuff tears.
Data and methods
Search strategy
Using “rotator cuff injuries, single-row, double-row, suture-bridge, platelet-rich plasma and bone marrow stimulation” as keywords, literature retrieval was performed in PubMed, Embase, The Cochrane Library, and Web of Science. The retrieval time was from inception to May 1, 2022.
Inclusion and exclusion criteria
Inclusion criteria for literature retrieval were (1) Type of study: randomized controlled trial or cohort study; (2) Subjects: patients diagnosed with rotator cuff tear and followed up for ≥ 6 months; (3) Interventions: at least any two of single-row repair, double-row repair, suture bridge repair, PRP therapy, and bone marrow stimulation; (4) Outcome indicators: at least any one of re-tear rate, Constant shoulder score (Constant) score [15], The Shoulder Rating Scale of the University of California at Los Angeles (UCLA) [16], the American Shoulder and Elbow Surgeons (ASES) score [17], and Visual Analog Scale (VAS).
Exclusion criteria included (1) retrospective studies, literature reviews, or conference papers with full text not available; (2) trials with no use of arthroscopy or suture anchoring techniques; (3) trials that did not involve imaging for structural assessment; and (4) animal or cell experiments.
Data extraction
Relevant literature was searched as per the PRISMA statement. To ensure the accuracy of the data and the rigor of the research, two researchers independently extracted relevant data and then cross-checked them according to the previously formulated standards. If disagreements occurred, the decision regarding data extraction was done by the third reviewer. The extracted baseline data included: the lead author’s name, publication time, number of patients, patient’s sex, mean age, interventions, follow-up time, and tear size.
Literature quality assessment
The Cochrane’s Risk of Bias tool was used to assess the risk of bias in the included randomized controlled trials, involving six domains: selection bias (random allocation sequence generation, allocation concealment), performance bias, detection bias, attrition bias, reporting bias, and other forms of bias. Each domain for assessing the risk of bias was assessed as low risk, high risk, or unclear risk, and then analyzed using Review Manager 5.3. The Newcastle–Ottawa Scale, which contains eight items, with a maximum score of 9, was used to evaluate the quality of the included cohort studies. A higher score indicates a lower risk of bias. If there was any disagreement, the third reviewer was consulted.
Outcome indicators
The outcome indicators included: AESE score, Constant score, VAS score, UCLA score, and re-tear rate.
Constant score is an important score for orthopedic surgeons to evaluate patients' shoulder function. It contains subjective and objective scores, involving eight aspects. The full score is 100 points. Higher scores indicate better recovery of shoulder function.
UCLA score acts as the final censoring score for shoulder repair, in which indicators such as pain and satisfaction are subjectively scored by patients, and indicators such as active forward elevation and strength are scored objectively by doctors, with a full score of 35 points. Higher scores indicate better outcomes and higher patient satisfaction.
AESE score is a patient-determined assessment scale for shoulder function and contains two dimensions of shoulder function: pain and performance in activities of daily living. It is a 100-point scale. Higher scores indicate better shoulder function.
VAS score is a commonly used quantitative index to measure the intensity of pain, usually providing a range of scores from 0–10. Lower scores indicate less pain intensity.
Statistical analysis
STATA15.1 and Review Manager5.3 were used for combined analysis and quality assessment, and a frequentist random-effects model was used for network Meta-analysis. The odds ratio (OR) was used as the effect size for dichotomous data (re-tear rate); mean difference (MD) was used as the effect size for continuous data such as the Constant score, UCLA score, and ASES score. The point estimates for each effect size and its 95% confidence interval (95% CI) were obtained. An inconsistency test was carried out by node splitting method on the outcome indicators containing closed loops in the evidence network graph. If a value of P > 0.05, the inconsistency was insignificant. The results of direct and indirect comparisons could be combined for analysis. On the contrary, the source of inconsistency was searched and eliminated, and the data were then merged and analyzed. As per the surface under the cumulative ranking (SUCRA) curve, the ranking results of the intervention measures were obtained. The larger area under the curve indicates better ranking and more effective intervention measures. Funnel plots were finally utilized to check for the existence of publication biases.
Results
Literature retrieval results
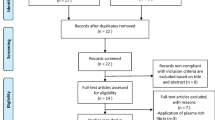
As shown in Fig. 1, a total of 3,793 related articles (908 in PubMed, 1,179 in Embase, 1,474 in Web of Science, and 232 in Cochrane Library) were initially retrieved. There were 2,423 articles after excluding duplicate articles. The 71 of 2,423 articles were screened out by reading the titles and abstracts. Of these 71 articles, 20 articles that did not meet the inclusion criteria were excluded after reading the full text and the remaining 51 articles were finally included for review [18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68]. There were 27 randomized controlled trials and 24 cohort studies included (Table 1).

Flow chart of document screening
Methodological quality of the included studies
Quality evaluation of the included studies indicated that of the 27 randomized controlled trials, 16 studies produced correct randomization sequences; 16 studies correctly concealed randomization sequences; 11 studies had no performance bias and 3 studies had performance bias; 19 studies had blinded assessments, with no detection bias; 17 studies reported complete outcome data, with no attrition bias; 20 studies made a statement about their findings; 21 studies had no other forms of bias (Fig. 2).

Risk of bias for randomized controlled trials
The quality of the included cohort studies was assessed using the Newcastle–Ottawa Scale. There are eight items in total, with a full score of 9 points. Higher scores indicate lower risks of bias. There were 19 studies with the total score of over 7 points. Therefore, the overall reliability of the included cohort studies was high.
Network met-analysis results
ASES score
Figure 3 shows the ASES score evaluation system. Figure 3A indicates the evidence network diagram of the ASES score. The outcome index involved five treatment measures, namely single-row, double-row, suture bridge, PRP therapy, and bone marrow stimulation, including 26 studies in total [18, 21,22,23,24,25, 27, 29,30,31, 34, 36, 42, 45, 46, 49, 51,52,53, 59, 62,63,64,65,66]. The included studies were first tested for inconsistency (P = 0.6350 > 0.05) and then for local inconsistency tests using the node-splitting method. Both the testing results were insignificant and therefore, the consistency model could be used for analysis. Figure 3B shows the SUCRA chart of ASES scores for five interventional measures. When both randomized controlled trials and cohort studies were included, the ASES scores of the five interventions were ranked as follows: PRP (SUCRA = 85.2), double-row (SUCRA = 71.0), bone marrow stimulation (SUCRA = 58.7), single-row (SUCRA = 34.4), and suture bridge (SUCRA = 0.7). Table 2 and Fig. 3C describe the trapezoidal comparison table of every two interventions and its intuitive forest diagram, respectively. Assessment of ASES scores indicated the efficacy of PRP therapy, double-row repair, bone marrow stimulation, and single-row repair was significantly better than that of suture bridge repair, and double-row repair, as well as the efficacy of double-row repair was significantly better than that of single-row repair, but there was no significant statistical difference among PRP therapy, double-row repair and bone marrow stimulation. A funnel plot was made for the obtained results to evaluate the possible publication bias of the ASES score (Fig. 1D), which is basically symmetrical, indicating no significant publication bias.

ASES scoring results (a Network Diagram; b Cumulative probability plot; c Forest map; d funnel chart)
Constant score
Figure 4 depicts the Constant score evaluation system, in which Fig. 4A is the evidence network diagram of the Constant score. This outcome index involved five treatment measures, namely single-row, double-row, suture bridge, PRP, and bone marrow stimulation, including a total of 36 studies [18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33, 35,36,37,38, 40, 42, 44,45,46, 48,49,50,51,52, 54,55,56,57,58,59, 61,62,63, 65, 67]. The obtained studies were first tested for inconsistency (P = 0.8267 > 0.05) and then for local inconsistency tests. Both of the testing results were insignificant and therefore, the consistency model was used for analysis. Figure 4B is the SUCRA chart of Constant scores for the five interventional measures. When both randomized controlled trials and cohort studies were included, the Constant scores of the five interventions were ordered: bone marrow stimulation (SUCRA = 92.4), single-row (SUCRA = 57.1), double-row (SUCRA = 44.3), PRP (SUCRA = 31.4), and suture bridge (SUCRA = 24.8) Fig. 4C is the forest plot for the comparison between every two measures, and Table 3 is the trapezoidal tale for the comparison between every two measures. There were no significant differences in the Constant score between the five treatment measures. As shown in Fig. 4D, the funnel plot is basically symmetrical, indicating no significant publication bias.

Constant scoring results (a Network Diagram; b Cumulative probability plot; c Forest map; d funnel chart)
VAS score
Figure 5 indicates the VAS score evaluation system, in which Fig. 5A is the evidence network diagram of the VAS score. This outcome index involved five treatment measures, namely single-row, double-row, suture bridge, PRP, and bone marrow stimulation, and a total of 21 studies were included [28,29,30,31,32,33, 35, 40, 41, 44, 48, 49, 54,55,56, 59, 61,62,63,64, 66]. The data extracted from the 21 studies were tested for inconsistency (P = 0.0000 < 0.05) and then for local inconsistency using the node-splitting method to seek the source of inconsistency. We found that the inconsistency originated from two studies, Li [54] and Martinelli [55]. After excluding these two studies, the value of P = 0.2125 > 0.05 indicated that consistency existed and then the consistency model could be used. Figure 5B is the SUCRA chart of VAS scores for the five interventional measures. When both randomized controlled trials and cohort studies were included, the VAS scores of the five interventions were ranked: bone marrow stimulation (SUCRA = 88.9), PRP (SUCRA = 81.7), single-row (SUCRA = 34.5), double-row (SUCRA = 25.5), and suture bridge (SUCRA = 19.3). Figure 5C and Table 4 are the forest plot and trapezoidal table for the comparison between every two treatment measures, respectively. In terms of VAS scores, the curative effect of PRP therapy was significantly better than that of single-row repair, double-row repair, and suture bridge repair (P < 0.05), and there was no significant difference between single-row repair, double-row repair, and suture bridge repair. A funnel plot was made for the obtained data to evaluate the possible publication bias of the VAS score. As shown in Fig. 5D, the funnel plot is basically symmetrical, indicating no obvious publication bias.

VAS scoring results (a Network Diagram; b Cumulative probability plot; c Forest map; d funnel chart)
UCLA score
Figure 6 shows the UCLA score evaluation system, in which Fig. 6D is the evidence network diagram of the UCLA score. This outcome index involved five treatment measures, namely single-row, double-row, suture bridge, PRP, and bone marrow stimulation, and a total of 25 studies were included [18, 21, 23, 24, 27, 28, 30,31,32,33, 36, 37, 40, 43, 48, 49, 51, 53,54,55, 58, 61,62,63, 65, 66]. The data extracted from the 25 studies were first tested for inconsistency (P = 0.4922 > 0.05) and then for local inconsistency using the node-splitting method. Results from both inconsistency tests were insignificant, indicating that the consistency model could be used for analysis. Figure 6B is the SUCRA chart of UCLA scores for the five interventional measures. When both randomized controlled trials and cohort studies were included, the UCLA score results of the five interventions were ranked: PRP (SUCRA = 77.4), double-row (SUCRA = 67.9), bone marrow stimulation (SUCRA = 45.3), suture bridge (SUCRA = 44.2), and single-row (SUCRA = 15.3). Figure 6C and Table 5 are the forest plot and trapezoid table for the comparison between every two measures. The curative effect of double-row repair was significantly better than that of single-row repair. Although the postoperative UCLA score of PRP therapy ranked in the forefront, there was no significant difference in the curative efficacy between PRP and the other measures. A funnel plot was made for the obtained data to evaluate the possible publication bias of the UCLA score. As shown in Fig. 6D, the funnel plot is basically symmetrical, indicating no significant publication bias.

UCLA scoring results (a Network Diagram; b Cumulative probability plot; c Forest map; d funnel chart)
Re-tear risk
Figure 7 describes the re-tear risk evaluation system, in which Fig. 7A is the evidence network diagram of re-tear risk. This outcome index involved five treatment measures, namely single-row, double-row, suture bridge, PRP, and bone marrow stimulation, and a total of 38 studies were included [18, 21, 23, 24, 26, 27, 29,30,31,32,33,34,35,36,37,38,39,40,41, 44,45,46,47, 49, 50, 53,54,55,56,57,58, 60,61,62,63,64,65]. Data extracted from these studies were used for inconsistency tests (P = 0.0097 < 0.05). As inconsistency existed, local inconsistency tests were performed using the node-splitting method, to find the source of inconsistency. After elimination of Pulatkan [54] and Hashiguchi [61], the inconsistency test indicated no significance (P = 0.0519 > 0.05), and then the consistency model could be used for analysis. Figure 7B is the SUCRA chart of re-tear rates for the five interventional measures. When both randomized controlled trials and cohort studies were included, the re-tear rates for the five interventions were ranked: PRP (SUCRA = 96.8), bone marrow stimulation (SUCRA = 67.8), double-row (SUCRA = 59.5), -suture bridge (SUCRA = 14.2), and single-row (SUCRA = 11.7). Figure 7C and Table 6 are the forest plot and trapezoidal table for the comparison between every two treatment measures. The re-tear rate of PRP therapy, bone marrow stimulation, and double-row repair was significantly lower than that of single-row repair and suture bridge repair (P < 0.05), and there was no significant difference between PRP therapy, bone marrow stimulation, and double-row repair. A funnel plot was made for the obtained data to evaluate the possible publication bias of the re-tear risk. As shown in Fig. 7D, the funnel plot is basically symmetrical, indicating no obvious publication bias.

Re-tear risk results (a Network Diagram; b Cumulative probability plot; c Forest map; d funnel chart)
Discussion
Rotator cuff injury is a common shoulder disease. Traditional open surgery can result in many postoperative complications and slow recovery. At present, arthroscopic repair has gradually become the mainstream trend. However, which treatment measure is the best under arthroscopy? There is no conclusive conclusion yet. Herein, a network Meta-analysis was carried out to focus on the prognostic efficacy of five rotator cuff repair techniques based on the data extracted from relevant randomized controlled trials and cohort studies. Five rotator cuff repair techniques, including single-row repair, double-row repair, suture bridge repair, PRP therapy, and bone marrow stimulation, were ranked based on their prognostic outcomes. The outcome indicators included ASES score, Constant score, VAS score, UCLA score, and re-tear rate.
For arthroscopic rotator cuff repair, double-row repair is significantly better than single-row repair in terms of ASES score, UCLA, and risk of re-tear. This may be because, compared with single-row repair, double-row repair increases the contact area between tendon and bone, increases the coverage area of rotator cuff "footprints", and improves the maximum load and fixation strength at the suture site, contributing to better restoring the rotator cuff structure. Compared with the other methods, single-row repair can get better Constant scores. The performance of suture bridge repair is not ideal in the five outcome indicators. Previous Meta-analysis [61] showed that suture bridge repair shows better biomechanical properties than single-row repair and obtains better footprint coverage in in vitro studies. However, suture bridge repair also makes the tension on the inner row too concentrated, weakens the connection at the tendon junction, and increases the risk of muscle atrophy and postoperative re-tear.
Meanwhile, the present study also found that PRP therapy had better performance in ASES score, VAS score, and risk of re-tea. Moreover, in terms of UCLA and Constant scores, there was no significant statistical difference between PRP therapy and the other interventions. This finding confirms the effectiveness of PRP therapy for rotator cuff injuries. To date, numerous studies have analyzed the effects of PRP in enhancing rotator cuff repair. A study by Li et al. [42] found that PRP therapy resulted in lower re-tear rates during 2-year follow-up after rotator cuff injury. Contrary to our conclusions, this study found no difference in UCLA scores at 3, 6, and 24 months after surgery. Another Meta-analysis regarding the use of PRP reviewed seven randomized controlled trials published between 2013 and 2018 and found that patients with PRP therapy had significantly lower re-tear rates and improved UCLA scores compared to those with no use of PRP [62]. Therefore, although PRP can improve the postoperative UCLA scores, there is no significant difference compared with the other surgical methods. However, it should be noted that in a relevant study, PRP has been divided into four categories: pure PRP, leukocyte and PRP, pure platelet-rich fibrin, and leukocyte-PRP and platelet-rich fibrin [63]. Different kinds of PRP may lead to inconsistent results.
As for bone marrow stimulation techniques, a recent meta-analysis [63] showed that bone marrow stimulation could reduce postoperative recurrence rates but not significantly improve functional outcomes compared with traditional repair methods. However, the present study found that bone marrow stimulation achieved the best Constant score in postoperative prognosis. And in terms of VAS score and risk of re-tear, after eliminating inconsistency, the bone marrow stimulation technique was also ranked top. Since mesenchymal stem cells generated in the foramen after microfracture may promote better histological healing of the repaired tendon [64], Beitzel conducted a retrospective analysis of the use of bone marrow mesenchymal stem cells to repair rotator cuff injuries. In the seven studies included, bone marrow mesenchymal stem cells were shown to promote healing but had no marked efficacy in one study. This is consistent with the results of our study [65, 66]. In addition, some basic and clinical studies have shown that PRP can stimulate local osteogenesis and promote the proliferation of mesenchymal stem cells, which is effective in the treatment of delayed healing or nonunion [67]. Chong found that at the early stage of tendon injury, injection of bone marrow mesenchymal stem cells could effectively promote tendon healing and improve its biomechanical properties.
The appropriate treatment regimen with effective rehabilitation can make patients achieve better outcomes [68]. Before implementing a rehabilitation regimen after rotator cuff repair, precautions should be given to the selection of surgical method, patient’s biological parameters, patient’s expectations for postoperative work, exercise, daily activities or recovery, and bone-to-tendon or tendon-to-tendon biological healing time. And based on these indicators, a personalized rehabilitation plan will be specified.
Based on the results of these five clinical outcome indicators, we concluded that PRP therapy is the most effective method for rotator cuff repair and double-row repair and bone marrow stimulation also have better prognostic outcomes. However, the overall therapeutic effect of single-row or suture bridge repair is relatively poor and both of them are not recommended for rotator cuff repair.
Availability of data and materials
All the data and materials were included within the manuscript.
References
Yamamoto A, Takagishi K, Osawa T, et al. Prevalence and risk factors of a rotator cuff tear in the general population. J Shoulder Elbow Surg. 2010;19(1):116–20.
Rizvi SMT, Bishop M, Lam PH, et al. Factors predicting frequency and severity of postoperative pain after arthroscopic rotator cuff repair surgery. Am J Sports Med. 2021;49(1):146–53.
Constant C, Murley A. A clinical method of functional assessment of the shoulder. Clin Orthop Relat Res. 1987;214:160–4.
Ellman H, Hanker G, Bayer M. Repair of the rotator cuff. End-result study of factors influencing reconstruction. J Bone Joint Surg Am. 1986;68(8):1136–44.
Tashjian RZ, Hollins AM, Kim HM, et al. Factors affecting healing rates after arthroscopic double-row rotator cuff repair[J]. Am J Sports Med. 2010;38(12):2435–42.
Burks RT, Crim J, Brown N, et al. A prospective randomized clinical trial comparing arthroscopic single-and double-row rotator cuff repair: magnetic resonance imaging and early clinical evaluation[J]. Am J Sports Med. 2009;37(4):674–82.
Grasso A, Milano G, Salvatore M, et al. Single-row versus double-row arthroscopic rotator cuff repair: a prospective randomized clinical study. Arthrosc J Arthrosc Relat Surg. 2009;25(1):4–12.
Aydin N, Kocaoglu B, Guven O. Single-row versus double-row arthroscopic rotator cuff repair in small-to medium-sized tears. J Shoulder Elbow Surg. 2010;19(5):722–5.
Koh KH, Kang KC, Lim TK, et al. Prospective randomized clinical trial of single-versus double-row suture anchor repair in 2-to 4-cm rotator cuff tears: clinical and magnetic resonance imaging results. Arthrosc J Arthrosc Relat Surg. 2011;27(4):453–62.
Lapner PL, Sabri E, Rakhra K, et al. A multicenter randomized controlled trial comparing single-row with double-row fixation in arthroscopic rotator cuff repair[J]. JBJS. 2012;94(14):1249–57.
Carbonel I, Martinez AA, Calvo A, et al. Single-row versus double-row arthroscopic repair in the treatment of rotator cuff tears: a prospective randomized clinical study. Int Orthop. 2012;36(9):1877–83.
Ma HL, Chiang ER, Wu HTH, et al. Clinical outcome and imaging of arthroscopic single-row and double-row rotator cuff repair: a prospective randomized trial. Arthrosc J Arthrosc Relat Surg. 2012;28(1):16–24.
Nicholas SJ, Lee SJ, Mullaney MJ, et al. Functional outcomes after double-row versus single-row rotator cuff repair: a prospective randomized trial. Orthop J Sports Med. 2016;4(10):2325967116667398.
Franceschi F, Papalia R, Franceschetti E, et al. Double-row repair lowers the retear risk after accelerated rehabilitation. Am J Sports Med. 2016;44(4):948–56.
Wade R, Salgar S. Clinico-radiological evaluation of retear rate in arthroscopic double row versus single row repair technique in full thickness rotator cuff tear[J]. J Orthop. 2017;14(2):313–8.
Imam M, Sallam A, Ernstbrunner L, et al. Three-year functional outcome of transosseous-equivalent double-row vs. single-row repair of small and large rotator cuff tears: a double-blinded randomized controlled trial. J Shoulder Elbow Surg. 2020;29(10):2015–26.
Zafra M, Uceda P, Muñoz-luna F, et al. Arthroscopic repair of partialthickness articular surface rotator cuff tears: single-row transtendon technique versus double-row suture bridge (transosseous equivalent) fixation: results from a prospective randomized study[J]. Arch Orthop Trauma Surg. 2020;140(8):1065–71.
Pandey V, Bandi A, Madi S, et al. Does application of moderately concentrated platelet-rich plasma improve clinical and structural outcome after arthroscopic repair of medium-sized to large rotator cuff tear? A randomized controlled trial. J Shoulder Elbow Surg. 2016;25(8):1312–22.
Jo CH, Shin JS, Shin WH, et al. Platelet-rich plasma for arthroscopic repair of medium to large rotator cuff tears: a randomized controlled trial. Am J Sports Med. 2015;43(9):2102–10.
Randelli P, Arrigoni P, Ragone V, et al. Platelet rich plasma in arthroscopic rotator cuff repair: a prospective RCT study, 2-year follow-up. J Shoulder Elbow Surg. 2011;20(4):518–28.
Malavolta EA, Gracitelli MEC, Ferreira neto AA, et al. Platelet-rich plasma in rotator cuff repair: a prospective randomized study. Am J Sports Med. 2014;42(10):2446–54.
Holtby R, Christakis M, Maman E, et al. Impact of platelet-rich plasma on arthroscopic repair of small-to medium-sized rotator cuff tears: a randomized controlled trial. Orthop J Sports Med. 2016;4(9):2325967116665595.
D’ambrosi R, Palumbo F, Paronzini A, et al. Platelet-rich plasma supplementation in arthroscopic repair of full-thickness rotator cuff tears: a randomized clinical trial. Musculoskelet Surg. 2016;100(1):25–32.
Jo CH, Shin JS, Lee YG, et al. Platelet-rich plasma for arthroscopic repair of large to massive rotator cuff tears: a randomized, single-blind, parallel-group trial. Am J Sports Med. 2013;41(10):2240–8.
Osti L, Del buono A, Maffulli N. Microfractures at the rotator cuff footprint: a randomised controlled study. Int Orthop. 2013;37(11):2165–71.
Milano G, Saccomanno MF, Careri S, et al. Efficacy of marrowstimulating technique in arthroscopic rotator cuff repair: a prospective randomized study. Arthrosc J Arthrosc Relat Surg. 2013;29(5):802–10.
Ebert JR, Wang A, Smith A, et al. A midterm evaluation of postoperative platelet-rich plasma injections on arthroscopic supraspinatus repair: a randomized controlled trial. Am J Sports Med. 2017;45(13):2965–74.
Malavolta EA, Gracitelli MEC, Assunção JH, et al. Clinical and structural evaluations of rotator cuff repair with and without added plateletrich plasma at 5-year follow-up: a prospective randomized study. Am J Sports Med. 2018;46(13):3134–41.
Wang A, Mccann P, Colliver J, et al. Do postoperative platelet-rich plasma injections accelerate early tendon healing and functional recovery after arthroscopic supraspinatus repair? A randomized controlled trial. Am J Sports Med. 2015;43(6):1430–7.
Flury M, Rickenbacher D, Schwyzer HK, et al. Does pure platelet-rich plasma affect postoperative clinical outcomes after arthroscopic rotator cuff repair? A randomized controlled trial. Am J Sports Med. 2016;44(8):2136–46.
Turan K, Çabuk H, Köroğlu C, et al. Increased acromiohumeral distance in a double-row arthroscopic rotator cuff surgery compared to a single-row surgery after 12 months. J Orthop Surg Res. 2021;16(1):1–7.
Pulatkan A, Anwar W, Tokdemir S, et al. The clinical and radiologic outcome of microfracture on arthroscopic repair for full-thickness rotator cuff tear. J Shoulder Elbow Surg. 2020;29(2):252–7.
Plachel F, Siegert P, Rüttershoff K, et al. Long-term results of arthroscopic rotator cuff repair: a follow-up study comparing single-row versus double-row fixation techniques. Am J Sports Med. 2020;48(7):1568–74.
Chen Y, Li H, Qiao Y, et al. Double-row rotator cuff repairs lead to more intensive pain during the early postoperative period but have a lower risk of residual pain than single-row repairs. Knee Surg Sports Traumatol Arthrosc. 2019;27(10):3180–7.
Hantes ME, Ono Y, Raoulis VA, et al. Arthroscopic single-row versus double-row suture bridge technique for rotator cuff tears in patients younger than 55 years: a prospective comparative study. Am J Sports Med. 2018;46(1):116–21.
Zhou XB, Liang JB, Chen ZY. Comparison of therapeutic effects of three repair methods for rotator cuff tears under arthroscopy. Zhongguo gu Shang China J Orthop Traumatol. 2017;30(8):689–94.
Wang E, Wang L, Gao P, et al. Single-versus double-row arthroscopic rotator cuff repair in massive tears. Med Sci Monit. 2015;21:1556.
Tudisco C, Bisicchia S, Savarese E, et al. Single-row vs. double-row arthroscopic rotator cuff repair: clinical and 3 Tesla MR arthrography results. BMC Musculoskelet Disord. 2013;14(1):1–10.
Denard PJ, Jiwani AZ, Lädermann A, et al. Long-term outcome of arthroscopic massive rotator cuff repair: the importance of double-row fixation. Arthrosc J Arthrosc Relat Surg. 2012;28(7):909–15.
Park JY, Lhee SH, Choi JH, et al. Comparison of the clinical outcomes of single-and double-row repairs in rotator cuff tears. Am J Sports Med. 2008;36(7):1310–6.
Sugaya H, Maeda K, Matsuki K, et al. Functional and structural outcome after arthroscopic full-thickness rotator cuff repair: single-row versus dual-row fixation. Arthrosc J Arthrosc Relat Surg. 2005;21(11):1307–16.
Li M, Wang K, Zhang H, et al. Clinical evaluations of intraoperative injection of platelet-rich plasma in arthroscopic single-row rotator cuff repair at 2-year follow-up[J]. BioMed Res Int. 2021;2021:1–9.
Martinelli D, Fornara P, Stecco A, et al. Does intraoperative plateletrich plasma improve clinical and structural outcomes after arthroscopic repair of isolated tears of the supraspinatus tendon? Indian Journal of Orthopaedics. 2019;53(1):77–81.
Zhang Z, Wang Y, Sun J. The effect of platelet-rich plasma on arthroscopic double-row rotator cuff repair: a clinical study with 12-month follow-up. Acta Orthop Traumatol Turc. 2016;50(2):191.
Gwinner C, Gerhardt C, Haneveld H, et al. Two-staged application of PRP in arthroscopic rotator cuff repair: a matched-pair analysis. Arch Orthop Trauma Surg. 2016;136(8):1165–71.
Panella A, Amati C, Moretti L, et al. Single-row and transosseous sutures for supraspinatus tendon tears: a retrospective comparative clinical and strength outcome at 2-year follow-up. Arch Orthop Trauma Surg. 2016;136(11):1507–11.
Park YE, Shon MS, Lim TK, et al. Knot impingement after rotator cuff repair: is it real? Arthrosc J Arthrosc Relat Surg. 2014;30(9):1055–60.
Kakoi H, Izumi T, Fujii Y, et al. Clinical outcomes of arthroscopic rotator cuff repair: a retrospective comparison of double-layer, double-row and suture bridge methods. BMC Musculoskelet Disord. 2018;19(1):1–7.
Hashiguchi H, Iwashita S, Sonoki K, et al. Clinical outcomes and structural integrity of arthroscopic double-row versus suture-bridge repair for rotator cuff tears. J Orthop. 2018;15(2):396–400.
Kim KC, Shin HD, Lee WY, et al. Repair integrity and functional outcome after arthroscopic rotator cuff repair: double-row versus suturebridge technique. Am J Sports Med. 2012;40(2):294–9.
Kim C, Lee YJ, Kim SJ, et al. Bone marrow stimulation in arthroscopic repair for large to massive rotator cuff tears with incomplete footprint coverage. Am J Sports Med. 2020;48(13):3322–7.
Yoon JP, Chung SW, Kim JY, et al. Outcomes of combined bone marrow stimulation and patch augmentation for massive rotator cuff tears. Am J Sports Med. 2016;44(4):963–71.
Liu B, Jeong HJ, Yeo JH, et al. Efficacy of intraoperative platelet-rich plasma augmentation and postoperative platelet-rich plasma booster injection for rotator cuff healing: a randomized controlled clinical trial. Orthop J Sports Med. 2021;9(6):23259671211006100.
Jo CH, Shin JS, Park IW, et al. Multiple channeling improves the structural integrity of rotator cuff repair. Am J Sports Med. 2013;41(11):2650–7.
Li C, Zhang H, Bo X, et al. Arthroscopic release combined with single-row fixation or double-row suture bridge fixation in patients with traumatic supraspinatus tear and adhesive capsulitis non-responsive to conservative management: a prospective randomized trial[J]. Orthop Traumatol Surg Res. 2021;107(4):102828.
Sánchez-Villacañas J R, Almoguera-Martinez A, Seoane G H, et al. No effect of intra-articular platelet-rich plasma injections after arthroscopic repair of rotator cuff tears: a prospective randomized study. Muscles Ligaments Tendons J. 2021;11(3):577–83.
Ying ZM, Lin T, Yan SG. Arthroscopic Single-row versus Double-row Technique for Repairing Rotator Cuff Tears: a Systematic Review and Meta-analysis. Orthop Surg. 2014;6(4):300–12.
Ryan J, Imbergamo C, Sudah S, et al. Platelet-rich product supplementation in rotator cuff repair reduces retear rates and improves clinical outcomes: a meta-analysis of randomized controlled trials. Arthrosc J Arthrosc Relat Surg. 2021;37(8):2608–24.
Malavolta EA, Gracitelli MEC, Assuncao JH, et al. Mid-term clinical and structural evaluation of platelet-rich plasma in rotator cuff repair—a prospective randomized study. J Shoulder Elbow Surg. 2019;28(6):e213.
Li Z, Zhang Y. Efficacy of bone marrow stimulation in arthroscopic repair of full thickness rotator cuff tears: a meta-analysis. J Orthop Surg Res. 2019;14(1):1–11.
Yamakado K. Two techniques for treating medium-sized supraspinatus tears: The medially based single-row technique and the suture bridge technique. JBJS Essent Surg Tech. 2021;11(2):e20.00004.
Yang F A, Liao C D, Wu C W, et al. Effects of applying platelet-rich plasma during arthroscopic rotator cuff repair: a systematic review and meta-analysis of randomised controlled trials[J]. Sci Rep. 2020;10(1):1–10.
Ehrenfest D M D, Andia I, Zumstein M A, et al. Classification of platelet concentrates (Platelet-Rich Plasma-PRP, Platelet-Rich Fibrin-PRF) for topical and infiltrative use in orthopedic and sports medicine: current consensus, clinical implications and perspectives[J]. Muscles Ligaments Tendons J. 2014;4(1):3.
Mazzocca A D, McCarthy M B R, Chowaniec D, et al. Bone marrow–derived mesenchymal stem cells obtained during arthroscopic rotator cuff repair surgery show potential for tendon cell differentiation after treatment with insulin[J]. Arthrosc: J Arthrosc Relat Surg. 2011;27(11):1459–71.
Chong AK, Ang AD, Goh JC, Hui JH, Lim AY, Lee EH, et al. Bone marrow-derived mesenchymal stem cells influence early tendon-healing in a rabbit achilles tendon model. J Bone Joint Surg Am. 2007;89(1):74–81.
Beitzel K, Solovyova O, Cote MP, Apostolakos J, Russell RP, McCarthy MB, et al. The future role of mesenchymal stem cells in the management of shoulder disorders. Arthroscopy. 2013;29(10):1702–11.
Osborne J D, Gowda A L, Wiater B, et al. Rotator cuff rehabilitation: current theories and practice[J]. Phys Sportsmed. 2016;44(1):85–92.
Conti M, Garofalo R, Delle Rose G, et al. Post-operative rehabilitation after surgical repair of the rotator cuff[J]. Musculoskelet Surg. 2009;93(1):55–63.
Acknowledgements
Not applicable.
Funding
There is no funding for this study.
Author information
Authors and Affiliations
Contributions
Tianshu You wrote the main manuscript, Siyu Wu and Xiaolan Ou performed data processing together, Ying Liu prepared the pictures and tables in the manuscript, and Xu Wang selected the topic of the article. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
You, T., Wu, S., Ou, X. et al. A network meta-analysis of arthroscopic rotator cuff repair. BMC Surg 23, 201 (2023). https://doi.org/10.1186/s12893-023-02078-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12893-023-02078-4