
Abstract
Background
Local treatment remains the best option for recurrent colorectal liver metastasis (CRLM). The current study aimed to investigate predictive factors of survival outcomes and select candidates for local treatment for CRLM at first recurrence.
Methods
Data were collected retrospectively from CRLM patients who underwent hepatic resection and developed first recurrence between 2000 and 2019 at our institution. A nomogram predicting overall survival was established based on a multivariable Cox model of clinicopathologic factors. The predictive accuracy and discriminative ability of the nomogram were determined by the concordance index and calibration curve.
Results
Among 867 patients who underwent curative hepatic resection, 549 patients developed recurrence. Three hundred patients were evaluated and had resectable and liver-limited disease. Among them, repeat liver resection and percutaneous radiofrequency ablation were performed in 88 and 85 patients, respectively. The other 127 patients received only systemic chemotherapy. Multivariable analysis identified primary lymph node positivity, tumor size > 3 cm, early recurrence, RAS gene mutation and no local treatment as independent risk factors for survival outcomes. Integrating these five variables, the nomogram presented a good concordance index of 0.707. Compared with patients who received only systemic chemotherapy, radical local treatment did not significantly improve survival outcomes (median OS: 21 vs. 15 months, p = 0.126) in the high-risk group (total score ≥ 13).
Conclusion
Radical local treatment improved the survival of recurrent CRLM patients. The proposed model facilitates personalized assessments of prognosis for patients who develop first recurrence in the liver.
Similar content being viewed by others


Key summary
More than half of CRLM patients develop recurrence after hepatic resection. The feasibility and safety of repeat local treatment have been tested. The present study created a nomogram to select recurrent CRLM patients who would benefit from repeat local treatment. This tool will help to design a personalized treatment regimen for recurrent CRLM.
Background
The liver is the most common site of colorectal cancer metastasis, and approximately 50% of patients develop liver metastasis at some point during their disease course [1]. Hepatic resection is a potentially curative treatment for colorectal cancer liver metastasis (CRLM) patients with 5-year survival rates of 30–50% [2]. Unfortunately, more than half of CRLM patients recur after hepatic resection, and the majority of such recurrences occur within 2 years [3].
Recent advances in surgical approaches have dramatically changed the treatment strategy for recurrent CRLM patients, which has allowed the description of risk factors for survival after a second round of local treatment. Previous studies have provided evidence that repeat hepatic resection is feasible in selected patients with intrahepatic recurrence [4, 5]. However, which individuals would yield maximum benefit from aggressive treatment following first recurrence is not clear, as there is a paucity of data on the risk factors for survival in this patient population. There has been no consensus introduced on how to select candidates.
The present study aimed to investigate prognostic factors for survival and select candidates for the local treatment of CRLM after first recurrence.
Methods
Study population
From January 2000 to September 2019, a total of 1027 patients underwent curative hepatic resection for CRLM at the Hepatopancreatobiliary Surgery Department I of Peking University Cancer Hospital. The demographic and clinical data were retrospectively obtained from a prospectively collected patient database. Patients were enrolled in the study based on the following criteria: (1) first recurrence developed after initial radical resection of both the liver metastasis and primary tumor; (2) the initial recurrence was considered resectable and liver-limited by a multidisciplinary team (MDT); (3) no extrahepatic metastasis had occurred since the first hepatic resection; and (4) there were no other simultaneous malignancies. The technical criteria of resectability related to the liver remnant after resection were as follows: (a) anticipated ability to preserve two contiguous segments; (b) anticipated ability to preserve adequate vascular inflow, outflow and biliary drainage; and (c) anticipated ability to preserve an adequate future liver remnant volume (30% in normal livers and 40% in livers pretreated with chemotherapy) [6]. The present study was approved by an Institutional Review Board.
Preoperative management for first recurrence
At first recurrence, all patients underwent routine laboratory tests, including serum carcinoembryonic antigen (CEA) and carbohydrate antigen (CA) 19–9 levels and liver function tests. Routine imaging modalities, including enhanced computed tomography (CT) scans of the abdominal, thoracic and pelvic regions and hepatic magnetic resonance imaging (MRI), were used to determine the disease stage. Strict criteria were used to detect evidence of cancer recurrence (local, metastatic or secondary colorectal cancer). Recurrence was diagnosed by CT scans, MRI, PET‐CT, or pathology (biopsy or specimen). All imaging reports that suggested recurrence were reviewed carefully and compared to baseline imaging reports to confirm that disease was not present at the time of liver resection. Preoperative chemotherapy was recommended for patients who presented a heavy tumor burden (CRS > 2) and/or recurred within a short period (disease-free survival time of less than 6 months) after the first hepatic resection. The response to chemotherapy was evaluated by MRI according to the Response Evaluation Criteria in Solid Tumors (RECIST 1.1) [7].
Indications for local treatment
The treatment strategy at first recurrence after hepatic resection was basically the same as that at first hepatic resection; that is, recurrent disease was treated locally only when the overall strategy was considered curative, and all detectable lesions had a tumor-free margin. The resectability was discussed, and clinical treatment decisions were made by an MDT. Systemic chemotherapy was recommended if the patient refused secondary local treatment. Resection of three or more segments was considered major hepatic resection. Percutaneous radiofrequency ablation (RFA) was performed using a CELON system (Teltow, Germany). The bipolar electrode needles were 16G, and guidance ultrasonography was performed using Aloka α-10 (Tokyo, Japan) and GE Logiq E9 (Connecticut, USA) devices. In general, RFA was recommended for deeply located tumors that would require extended resection of the normal parenchyma. RFA was contraindicated when (1) the diameter of the largest tumor exceeded 3 cm and (2) the tumor was adjacent to major bile ducts or large blood vessels or the colon/gallbladder were strictly restricted.
Postoperative work-up
After completing treatment, all patients underwent regular follow-up examinations with hepatic MRI and CT scans of the abdominal/thoracic/pelvic region, and levels of tumor markers were measured every three months. Adjuvant chemotherapy was usually recommended [8].
Statistical analysis
Continuous variables are summarized as the means, and categorical variables are summarized as frequencies and percentages. The means of variables were compared with chi square analysis or Fischer’s exact test (depending on the sample size) or with the independent Student’s t test or Mann–Whitney U test, as appropriate. The optimal cutoff points for the definition of early recurrence were determined using the minimum p value approach, which was calculated using the log-rank test for OS after first recurrence. Survival analyses were carried out using the Kaplan–Meier method with the log-rank test. OS was calculated from the date of local treatment or the date of systemic chemotherapy after first recurrence until death or the last follow-up. OS was the primary endpoint for studies with repeat hepatic resection [3, 9]. Cutoff values for continuous variables were determined based on the C-statistic, with a Cox regression model for survival data including censored patients. The estimated cutoff values for each variable were tumor number, 1–5; tumor size, 20–550 mm; CEA level, 5 (upper limit of the normal range), 10, 20, 50, 100, 200 ng/ml; and CA19-9, 37 (upper limit of the normal range), 50, 100 units/ml7. All statistical analyses were performed using SPSS 26.0 and R version 3.2.6 (http://www.r-project.org), and p values < 0.05 were considered statistically significant.
Establishment of nomogram
Univariable and multivariable analyses of various clinicopathological factors by Cox’s proportional hazard model were used to identify independent risk factors for OS in 300 patients. The results of multivariable analysis were used to develop an OS prediction nomogram with 1-, 3-, and 5-year OS as the endpoints. The C-index was calculated to assess the degree of discrimination, and calibration plots were generated to visualize the agreement between the predicted and actual 1-, 3- and 5-year OS with bootstrapped samples. Using all categorical risk factors, we found the best separation in terms of survival by permutation and created two risk groups, a high‐risk and a low‐risk group.
Results
Patient characteristics
A total of 867 patients were eligible for study enrollment (Additional file 1: Figure S1). Recurrence was observed in 549 patients (64.1%). Among them, 523 patients (95.3%) developed single-site recurrence [liver (n = 384), lung (n = 86), lymph node (n = 39), and other organ (n = 14)], while 26 patients developed recurrence in multiple organs. Among the patients with single-site recurrence of the liver, 300 were considered to be resectable by an MDT. Repeat hepatic resection and percutaneous radiofrequency ablation were performed in 88 and 85 patients, respectively. The incidence of 90-day mortality was 0% in the repeat resection group. Eight patients underwent intraoperative RFA, and 11 patients underwent R1 resection. There were 66 and 62 patients who received adjuvant chemotherapy in the repeat resection and RFA groups, respectively. The other 127 patients refused local treatment and received only systemic chemotherapy (Table 1). In patients who experienced recurrence, the optimal cutoff point for defining early recurrence was 6 months after hepatic resection based on the results of the minimum p value approach for survival after first recurrence (p = 7.57 × 10–17) (Additional file 2: Figure S2).
Survival analysis
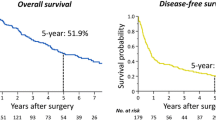
The median follow-up was 39 months after first recurrence (95% CI: 35–43 months). The 1-, 3- and 5-year OS and DFS rates were 92.3%, 59.3%, and 46.2% and 46.8%, 28.4%, and 25.4%, respectively, for 867 CRLM patients (Additional file 3: Figure S3). The 1-, 3- and 5-year OS rates for the local treatment group were 86.3%, 54.1% and 38.9%, respectively, and those for the systemic chemotherapy group were 64.8%, 16.3% and 2.7%, respectively. The difference between the two groups was significant (p < 0.001) (Fig. 1). Of the 173 patients who underwent local treatment, the 5-year OS and DFS rates were 38.9% and 22.2%, respectively (Additional file 4: Figure S4). Among them, 97 patients (56.1%) developed recurrence after local treatment.

The OS of local treatment and chemotherapy was shown by a Kaplan-Meier curve
Prognostic factors for OS after first recurrence
In univariable analysis, primary N + , tumor number > 1, largest tumor size > 3 cm, RAS mutation, early recurrence, bilateral distribution at first recurrence and no local treatment were related to decreased OS (p < 0.05). Five independent prognostic factors for OS were identified in multivariable analysis: node-positive primary (HR = 1.857, 95% CI: 1.227–2.809; p = 0.003), tumor size > 3 cm (HR = 1.707, 95% CI: 1.037–2.810; p = 0.036), early recurrence (HR = 1.693, 95% CI: 1.142–2.511; p = 0.009), RAS mutation (HR = 1.553, 95% CI: 1.080–2.234; p = 0.017) and local treatment (HR = 0.322, 95% CI: 0.222–0.467; p < 0.001) (Table 2).
Prognostic nomogram and calibration for OS
We developed a point-based prognostic nomogram to predict OS at first recurrence based on the five independent prognostic factors (Fig. 2). The sum of each score is presented in Additional file 5: Table S1. The C-index of the prognostic nomogram was 0.707 for predicting OS. The calibration plot suggested that the accuracy of the predicted 1-, 3-, and 5-year OS was excellent (Fig. 3a–c).

Colorectal liver metastasis nomogram for OS after first recurrence

a The predicted OS at 1 year by a calibration curve. b The predicted OS at 3 years by a calibration curve. c The predicted OS at 5 years by a calibration curve
Performance of the nomogram for predicting OS
In the development cohort, the AUCs of the nomogram score for predicting OS at 1, 3, and 5 years were higher than those of the algorithms recommended by Hof [10], Neal [11], and Serrano[12] (Additional file 6: Figure S5 and Additional file 7: Table S2).
Stratification by nomogram and indications for repeat local treatment
The survival curves stratified by quartiles of the nomogram-predicted score are shown in Additional file 8: Figure S6. Compared with patients (total score ≥ 13) who received systemic chemotherapy, radical local treatment did not significantly improve survival outcomes compared to those before treatment (median OS: 21 vs. 15 months, p = 0.126) (Additional file 9: Figure S7).
Discussion
Curative resection for CRLM improves survival outcomes and curative opportunities; however, the majority of patients will develop recurrence [13]. It has been suggested that secondary hepatic resection is a safe and feasible procedure for recurrent CRLM patients. However, repeat hepatic resection may not be possible due to anatomical or functional restraints [9, 10]. RFA is a useful alternative in this situation. The indications for repeat hepatic resection were believed to be the same as those for initial resection [4, 14]. However, the disease characteristics were not exactly compared between the initial and recurrent resection time points.
The indication and concerning prognostic factors for the local treatment of first recurrence have not been well studied or defined. Previous analyses have been limited by small and single cohorts of patients [4, 14]. In the present study, 173 patients who underwent local treatment at first recurrence for CRLM and had significantly better survival outcomes than those who only received systemic chemotherapy. Rumor size > 3 cm, node-positive primary, early recurrence, and RAS mutation have been identified to be risk factors for survival outcomes CRLM patients at first recurrence. Furthermore, in the high-risk group (total score ≥ 13), local treatment did not significantly improve OS (median OS: 21 vs. 15 months, p = 0.126). The present model might facilitate the identification of patients who may benefit most from repeat local treatment before an individualized treatment decision is made.
Recurrence occurs in 60–84% of CRLM patients after initial hepatic resection [15, 16]. The recent expansion of indications for surgery has led to an increase in the number of patients with potentially resectable disease, while these factors can also lead to an increased risk of early recurrence. Early recurrence has been reported to adversely influence survival after hepatic resection and therefore remains a concern for repeat hepatic resection because of worse patient prognosis [17, 18]. The present study investigated whether the optimal cutoff point for early recurrence was 6 months. Although it remained an independent prognostic risk factor, aggressive treatment should therefore be proactively considered even for patients with early recurrence. If the patient was determined to have unresectable early recurrence, systemic chemotherapy should be recommended. For patients with resectable disease, radical resection should be performed as often as possible. Two cycles of neoadjuvant chemotherapy should be recommended, followed by local treatment. If there is a risk of removing liver metastases, the patient should undergo upfront resection directly. RFA should be performed if the tumor is located deep in the liver.
The liver and lungs are the predominant sites of secondary recurrence, of which liver metastases are especially common [3, 19]. Therefore, the present study enrolled only patients with resectable, liver-limited disease at first recurrence. Repeat hepatic resection for recurrence has been reported to be associated with an equivalent long-term outcome to first hepatic resection, with a similarly low surgical risk, and the 5-year OS rate ranged from 27 to 45% [20,21,22,23]. RFA has emerged as an alternative radical treatment with lower invasiveness and a lower complication rate and is effective for patients with comorbidities and recurrent liver disease [24, 25]. Previous studies of percutaneous RFA for recurrent CRLM yield similar results [26, 27]. It has been suggested that tumor diameter and number are the most important factors that influence the efficacy [28, 29]. In our study, RFA was recommended in deeply located tumors that would require extensive resection of the normal parenchyma.
Given that the survival of patients who undergo liver resection for colorectal cancer metastases is long, surgeons and medical oncologists are now dealing with a “chronic disease” that should be treated differently depending on its presentation upon recurrence [30]. In the modern era, in addition to the current disease state of CRLM patients, recurrence should be considered when determining the treatment strategy. Preoperative chemotherapy might shrink tumors and increase resectability. In particular, it also likely selected individuals with recurrence who would benefit from resection. Therefore, this treatment might be recommended for patients who develop early recurrence or have a heavy disease burden in the liver.
Limitations
The limitations of the present study included its retrospective design and the gradual change in indications for resection and RFA over the course of the study. First, although the enrolled patients were determined to have resectable disease, bias could still have existed from patient selection in the three groups. Therefore, these results should be validated with further better quality studies. Second, it is possible that other unknown factors could affect the accuracy of the nomogram model and that a higher number of cases might be required to be detect them. This type of study is difficult to perform prospectively, and any trials must be very carefully performed. Moreover, there was no external validation cohort in the present study. Finally, all data were collected from a limited number of institutions.
Conclusion
Radical treatment remains the gold-standard for recurrent colorectal liver metastasis. The proposed model may help to predict the possibility of radical interventions (score < 13) and provide optimal individualized treatment.
Availability of data and materials
The datasets generated and/or analyzed during the current study are not publicly available to protect individual patient privacy but are available from the corresponding author upon reasonable request.
Abbreviations
- CRLM:
-
Colorectal liver metastasis
- RFA:
-
Radiofrequency ablation
- OS:
-
Overall survival
- DFS:
-
Disease-free survival
- MDT:
-
Multidisciplinary team
- CEA:
-
Carcinoembryonic antigen
- HR:
-
Hazard ratio
- MRI:
-
Magnetic resonance imaging
- CT:
-
Computed tomography
References
Leung U, Gonen M, Allen PJ, Kingham TP, DeMatteo RP, Jarnagin WR, D’Angelica MI. Colorectal cancer liver metastases and concurrent extrahepatic disease treated with resection. Ann Surg. 2017;265(1):158–65.
Kopetz S, Chang GJ, Overman MJ, Eng C, Sargent DJ, Larson DW, Grothey A, Vauthey JN, Nagorney DM, McWilliams RR. Improved survival in metastatic colorectal cancer is associated with adoption of hepatic resection and improved chemotherapy. J Clin Oncol. 2009;27(22):3677–83.
Imai K, Allard MA, Benitez CC, Vibert E, Sa Cunha A, Cherqui D, Castaing D, Bismuth H, Baba H, Adam R. Early recurrence after hepatectomy for colorectal liver metastases: what optimal definition and what predictive factors? Oncologist. 2016;21(7):887–94.
Wicherts DA, de Haas RJ, Salloum C, Andreani P, Pascal G, Sotirov D, Adam R, Castaing D, Azoulay D. Repeat hepatectomy for recurrent colorectal metastases. Br J Surg. 2013;100(6):808–18.
Butte JM, Gonen M, Allen PJ, Peter Kingham T, Sofocleous CT, DeMatteo RP, Fong Y, Kemeny NE, Jarnagin WR, D’Angelica MI. Recurrence after partial hepatectomy for metastatic colorectal cancer: potentially curative role of salvage repeat resection. Ann Surg Oncol. 2015;22(8):2761–71.
Adams RB, Aloia TA, Loyer E, Pawlik TM, Taouli B, Vauthey JN, Americas Hepato-Pancreato-Biliary A, Society of Surgical O, Society for Surgery of the Alimentary T. Selection for hepatic resection of colorectal liver metastases: expert consensus statement. HPB (Oxford). 2013;15(2):91–103.
Therasse P, Arbuck SG, Eisenhauer EA, Wanders J, Kaplan RS, Rubinstein L, Verweij J, Van Glabbeke M, van Oosterom AT, Christian MC, et al. New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J Natl Cancer Inst. 2000;92(3):205–16.
Nordlinger B, Sorbye H, Glimelius B, Poston GJ, Schlag PM, Rougier P, Bechstein WO, Primrose JN, Walpole ET, Finch-Jones M, et al. Perioperative FOLFOX4 chemotherapy and surgery versus surgery alone for resectable liver metastases from colorectal cancer (EORTC 40983): long-term results of a randomised, controlled, phase 3 trial. Lancet Oncol. 2013;14(12):1208–15.
Yan TD, Sim J, Black D, Niu R, Morris DL. Systematic review on safety and efficacy of repeat hepatectomy for recurrent liver metastases from colorectal carcinoma. Ann Surg Oncol. 2007;14(7):2069–77.
Hof J, Wertenbroek MW, Peeters PM, Widder J, Sieders E, de Jong KP. Outcomes after resection and/or radiofrequency ablation for recurrence after treatment of colorectal liver metastases. Br J Surg. 2016;103(8):1055–62.
Neal CP, Nana GR, Jones M, Cairns V, Ngu W, Isherwood J, Dennison AR, Garcea G. Repeat hepatectomy is independently associated with favorable long-term outcome in patients with colorectal liver metastases. Cancer Med. 2017;6(2):331–8.
Serrano PE, Gu CS, Husien M, Jalink D, Ritter A, Martel G, Tsang ME, Law CH, Hallet J, McAlister V, et al. Risk factors for survival following recurrence after first liver resection for colorectal cancer liver metastases. J Surg Oncol. 2019;120(8):1420–6.
Imai K, Allard MA, Castro Benitez C, Vibert E, Sa Cunha A, Cherqui D, Castaing D, Bismuth H, Baba H, Adam R. Nomogram for prediction of prognosis in patients with initially unresectable colorectal liver metastases. Br J Surg. 2016;103(5):590–9.
Luo LX, Yu ZY, Huang JW, Wu H. Selecting patients for a second hepatectomy for colorectal metastases: an systemic review and meta-analysis. Eur J Surg Oncol. 2014;40(9):1036–48.
de Jong MC, Pulitano C, Ribero D, Strub J, Mentha G, Schulick RD, Choti MA, Aldrighetti L, Capussotti L, Pawlik TM. Rates and patterns of recurrence following curative intent surgery for colorectal liver metastasis: an international multi-institutional analysis of 1669 patients. Ann Surg. 2009;250(3):440–8.
Vigano L, Capussotti L, Lapointe R, Barroso E, Hubert C, Giuliante F, Ijzermans JN, Mirza DF, Elias D, Adam R. Early recurrence after liver resection for colorectal metastases: risk factors, prognosis, and treatment. A LiverMetSurvey-based study of 6,025 patients. Ann Surg Oncol. 2014;21(4):1276–86.
Takahashi S, Konishi M, Kinoshita T, Gotohda N, Kato Y, Saito N, Sugito M, Yoshino T. Predictors for early recurrence after hepatectomy for initially unresectable colorectal liver metastasis. J Gastrointest Surg. 2013;17(5):939–48.
Tan MC, Butte JM, Gonen M, Kemeny N, Fong Y, Allen PJ, Kingham TP, Dematteo RP, Jarnagin WR, D’Angelica MI. Prognostic significance of early recurrence: a conditional survival analysis in patients with resected colorectal liver metastasis. HPB (Oxford). 2013;15(10):803–13.
Imai K, Yamashita YI, Miyamoto Y, Nakagawa S, Okabe H, Hashimoto D, Chikamoto A, Baba H. The predictors and oncological outcomes of repeat surgery for recurrence after hepatectomy for colorectal liver metastases. Int J Clin Oncol. 2018;23(5):908–16.
Kulik U, Bektas H, Klempnauer J, Lehner F. Repeat liver resection for colorectal metastases. Br J Surg. 2013;100(7):926–32.
Andreou A, Brouquet A, Abdalla EK, Aloia TA, Curley SA, Vauthey JN. Repeat hepatectomy for recurrent colorectal liver metastases is associated with a high survival rate. HPB (Oxford). 2011;13(11):774–82.
Battula N, Tsapralis D, Mayer D, Isaac J, Muiesan P, Sutcliffe RP, Bramhall S, Mirza D, Marudanayagam R. Repeat liver resection for recurrent colorectal metastases: a single-centre, 13-year experience. HPB (Oxford). 2014;16(2):157–63.
Ali MA, Di Sandro S, Lauterio A, Concone G, Mangoni I, Ferla F, Rotiroti V, Cusumano C, Giacomoni A, De Carlis L. Repeat hepatectomy for recurrent colorectal liver metastases: is it worth the challenge? J Gastrointest Surg. 2015;19(12):2192–8.
Oshowo A, Gillams AR, Lees WR, Taylor I. Radiofrequency ablation extends the scope of surgery in colorectal liver metastases. Eur J Surg Oncol. 2003;29(3):244–7.
Evrard S, Becouarn Y, Fonck M, Brunet R, Mathoulin-Pelissier S, Picot V. Surgical treatment of liver metastases by radiofrequency ablation, resection, or in combination. Eur J Surg Oncol. 2004;30(4):399–406.
Valls C, Ramos E, Leiva D, Ruiz S, Martinez L, Rafecas A. Safety and efficacy of ultrasound-guided radiofrequency ablation of recurrent colorectal cancer liver metastases after hepatectomy. Scand J Surg. 2015;104(3):169–75.
Solbiati L, Ahmed M, Cova L, Ierace T, Brioschi M, Goldberg SN. Small liver colorectal metastases treated with percutaneous radiofrequency ablation: local response rate and long-term survival with up to 10-year follow-up. Radiology. 2012;265(3):958–68.
Veltri A, Sacchetto P, Tosetti I, Pagano E, Fava C, Gandini G. Radiofrequency ablation of colorectal liver metastases: small size favorably predicts technique effectiveness and survival. Cardiovasc Intervent Radiol. 2008;31(5):948–56.
Hamada A, Yamakado K, Nakatsuka A, Uraki J, Kashima M, Takaki H, Yamanaka T, Inoue Y, Kusunoki M, Takeda K. Radiofrequency ablation for colorectal liver metastases: prognostic factors in non-surgical candidates. Jpn J Radiol. 2012;30(7):567–74.
Chua TC, Liauw W, Chu F, Morris DL. Viewing metastatic colorectal cancer as a curable chronic disease. Am J Clin Oncol. 2012;35(1):77–80.
Acknowledgements
No preregistration was performed for the reported studies reported in this article. We acknowledge QB, who contributed to the study by making substantial contributions to the acquisition of the data, and KMJ, who made substantial contributions to the analysis and interpretation of the data. They were involved in drafting the manuscript but did not meet the criteria for authorship.
Funding
This study was supported by Grants (No. 81874143 and No. 31971192) from the National Nature Science Foundation of China, the Beijing Natural Science Foundation (Grant No. 7192035) and the Beijing Hospitals Authority Youth Program (code: QMS20201105). The funding body financed the costs of the study and contributed to the design of the study, interpretation of data, and revision of the manuscript.
Author information
Authors and Affiliations
Contributions
BCX contributed to the conception and design. KW and HWW were responsible for the provision of the study materials and data collection. WL and JML contributed equally to the data analysis, interpretation and draft writing. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The present study was a retrospective study, and all subjects provided written informed consent. The investigation project was examined and certified by the Ethics Committee of Beijing Cancer Hospital. The study was performed in accordance with the Declaration of Helsinki.
Consent for publication
The manuscript does not contain any individual person's data.
Competing interests
The manuscript has not been presented at a talk or poster meeting. We declare that we have no financial and personal relationships with other people or organizations that could have inappropriately influenced our work, and there are no professional or other personal interests of any nature or kind in any product, service and/or company that could be construed.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Figure S1.
Flowchart of the enrolled cohorts.
Additional file 2: Figure S2.
The definition of early recurrence using the minimum p value approach by an optimal cutoff point regarding the time to first recurrence.
Additional file 3: Figure S3.
Kaplan-Meier curve showing the OS and DFS of 867 patients.
Additional file 4: Figure S4.
Kaplan-Meier curve showing the OS and DFS of local treatment.
Additional file 5: Table S1.
Prognostic factors.
Additional file 6: Figure S5.
The OS of the high-risk (score ≥ 13) and low-risk groups (score < 13) by a Kaplan-Meier curve.
Additional file 7: Table S2.
Comparison of different models for predicting OS.
Additional file 8: Figure S6.
The OS of local treatment and chemotherapy in the high-risk group by a Kaplan-Meier curve.
Additional file 9: Figure S7.
Kaplan-Meier curve showing the OS of local treatment and chemotherapy in the high-risk group.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Liu, W., Liu, JM., Wang, K. et al. Recurrent colorectal liver metastasis patients could benefit from repeat hepatic resection. BMC Surg 21, 327 (2021). https://doi.org/10.1186/s12893-021-01323-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12893-021-01323-y