
Abstract
Background
All orthopaedic procedures, comprising foot and ankle surgeries, seemed to show a positive trend, recently. Bone grafts are commonly employed to fix bone abnormalities resulting from trauma, disease, or other medical conditions. This study specifically focuses on reviewing the safety and efficacy of various bone substitutes used exclusively in foot and ankle surgeries, comparing them to autologous bone grafts.
Methods
The systematic search involved scanning electronic databases including PubMed, Scopus, Cochrane online library, and Web of Science, employing terms like 'Bone substitute,' 'synthetic bone graft,' 'Autograft,' and 'Ankle joint.' Inclusion criteria encompassed RCTs, case-control studies, and prospective/retrospective cohorts exploring different bone substitutes in foot and ankle surgeries. Meta-analysis was performed using R software, integrating odds ratios and 95% confidence intervals (CI). Cochrane's Q test assessed heterogeneity.
Results
This systematic review analyzed 8 articles involving a total of 894 patients. Out of these, 497 patients received synthetic bone grafts, while 397 patients received autologous bone grafts. Arthrodesis surgery was performed in five studies, and three studies used open reduction techniques. Among the synthetic bone grafts, three studies utilized a combination of recombinant human platelet-derived growth factor BB homodimer (rhPDGF-BB) and beta-tricalcium phosphate (β-TCP) collagen, while four studies used hydroxyapatite compounds. One study did not provide details in this regard. The meta-analysis revealed similar findings in the occurrence of complications, as well as in both radiological and clinical evaluations, when contrasting autografts with synthetic bone grafts.
Conclusion
Synthetic bone grafts show promise in achieving comparable outcomes in radiological, clinical, and quality-of-life aspects with fewer complications. However, additional research is necessary to identify the best scenarios for their use and to thoroughly confirm their effectiveness.
Levels of evidence
Level II.
Similar content being viewed by others

Introduction
Foot and ankle musculoskeletal issues accounts for an enormous part of annual orthopaedic surgical procedures performed all around the world [1,2,3,4,5,6,7]. All orthopaedic procedures, comprising foot and ankle surgeries, seemed to show a positive trend, recently [8, 9]. Globally, bone substitutes are needed in about 10% of all orthopedic surgeries. Autogenous bone is the preferred choice because it provides osteoconduction, osteoinduction, and osteogenesis, ensuring compatibility and reducing the risk of disease transmission or rejection. However, to overcome the limitations and scarcity of autogenous bone, recent advancements have introduced several alternative therapeutic approaches such as synthetic bone grafts, local growth factors, and composites [10].
In orthopaedic surgery, bone grafts are frequently used to fix bone abnormalities brought on by trauma, disease, or other medical issues. Due to its capacity to offer all biologic components necessary for a functioning graft, autograft is regarded as the gold standard for bone grafting [11, 12]. Autografts involve moving bone from a particular region of the body—the donor site—to another. Numerous foot and ankle treatments, such as medial ankle instability, osteochondral lesions, arthrodesis, and tibiotalocalcaneal fusion have been investigated with respect to the application of autologous bone transfers [12, 13]. Numerous studies have compared the safety and effectiveness of autologous bone grafts to those of other treatments. According to a comprehensive analysis, autologous bone transplants are safe and have a low incidence of surgical or medical complications [14]. However, there remains some major limitations about utilizing autografts in orthopaedic setting. Donor site challenges such as excessive pain, superficial infection, osteomyelitis, and nerve damage made surgeons think about finding other alternatives [15].
Because of their limitless supply and simplicity in sterilization, synthetic bone grafts have attracted a lot of attention [16, 17]. These alternatives can be divided into three groups: calcium sulfate, tricalcium phosphate, and hydroxyapatite [18]. In contrast to autologous grafts, which call for a second surgical site and might lead to source site complications, synthetic bone grafts allay these worries by requiring no extra surgery. Nonetheless, they have drawbacks like varying rates of resorption and inadequate efficacy in some therapeutic scenarios [17]. Recently, bone graft grafts have been evaluated alongside autografts or allografts in the setting of particular orthopedic operations, such as spinal fusion [19], maxillary sinus augmentation [20], tibial plateau fractures [21], and upper extremity surgery [22]. However, limited evidence exists discussing the application of synthetic bone grafts in foot and ankle surgery (mostly regarding ankle arthrodesis) [15]. A comprehensive systematic review and meta-analysis is definitely demanded to decide which substitute fulfils the criteria to be appropriate for filling bone defects during procedures related to foot or ankle. The present study aimed to systematically review safety and efficacy of different types of bone substitutes in foot and ankle surgeries exclusively compared to autologous bone grafts.
Materials and methods
The "preferred reporting items for systematic reviews and meta-analyses" (the "PRISMA" statement)" requirements were followed when conducting this meta-analysis [23]. The prospective register of systematic reviews (PROSPERO) records the predefined approach that this review followed (CRD42022372290).
Search strategy and screening
Electronic databases involving MEDLINE/PubMed, Scopus, Cochrane Central Register of Controlled Trials (CENTRAL), and Web of Science were searched by two independent authors (AG, AMS). A manual search was conducted among publications that were similar to the ones being searched, related articles, and Google Scholar citations. Citation search was updated prior to the final analysis, with the most recent data update occurring on December 20, 2023. The following MeSH headings (Medical Subject Headings) or keyword phrases were employed: Bone substitute, synthetic bone graft, artificial bone, Hydroxyapatite, rhPDGF-BB, Autograft, autologous bone graft, Ankle joint, Foot joints, etc. The search approach is further described in supplementary data, table S1. Using Rayyan, a web-based tool for systematic reviewing, studies were reviewed. Each study was reviewed separately by two reviewers (AG, AMS), who also checked the full-text and removed any duplicates after screening the title and abstract. Studies that met the inclusion-exclusion criteria were chosen. Consensus sessions presided over by the third author (AHH) helped settle any disputes that might have developed between reviewers. Finally, the references of the included articles were checked to ensure that no relevant articles were omitted.
Inclusion and exclusion criteria
The following inclusion criteria were used to find eligible studies: 1) Participants: Patients who underwent any surgical management needing bone graft due a foot or ankle-related issue; 2) Intervention: Synthetic bone grafts such as Recombinant human platelet-derived growth factor-BB (rhPDGF-BB) and hydroxyapatite-based grafts; 3) Comparison: Autologous bone graft; 4) Outcome: at least one of the following outcomes including postoperative complications, union rate, functional status, and quality of life; 5) Retrospective or prospective cohort studies, case-control studies, or randomized clinical trials (RCTs) were eligible for inclusion. The following exclusion standards were applied: 1) inadequate information to calculate odds ratios or standardized mean differences; 2) Letters, correspondents, pilot studies, reviews and commentaries, technique papers, conference abstracts, animal research, and cadaver studies; 3) Studies without a comparable control group; 4) Studies involving patients undergoing surgical care who required a bone graft in anatomical areas other than the foot and ankle
Data extraction and Quality assessment
Two researchers (SE, AGR) separately filled out the following data on a pre-created Microsoft Excel sheet before records screening. The information was gathered on demographic characteristics of the patients, such as year of publication, study design, number of participants in both comparison groups, mean age in years, Body mass index (BMI), as well as topic-specific information including bone graft type, mean length of follow-up, complications by detail, pain at the follow-up, functional outcomes including AOFAS score and ATRS score, union rate at the follow-up, and quality of life measures. By the third reviewer (AHH), conflicts were evaluated. Cochrane risk of bias 2 (RoB2) and the ROBINS-I risk assessment tool, respectively, were employed as the criteria for measuring the risk of bias in randomized clinical trials (RCT) and non-RCTs [24]. The following areas were evaluated for bias risk using the RoB2: the randomization process, deviations from intended interventions, missing outcome data, assessment of the outcome, and choice of the reported result. The authors assigned a score of "low," "some concerns," or "high" to each domain. Using the maximum risk associated to any one area as our basis, overall ROB was calculated for each trial [24].
The ROBINS-I tool was modified in accordance with a similarly modified version to better assess risk of bias (RoB) in exposure studies [25], but regardless, the authors adhered to the comprehensive instructions for the ROBINS-I tool [26]. Each study was evaluated in relation to a hypothetical target randomized trial, with differences from the target trial being viewed as bias. By responding to signaling questions and critically mirroring each domain against a set of predetermined criteria, seven bias domains, including confounding, selection of participants, classification of diet groups, departures from baseline diet groups, missing data, measurement of outcomes, and selection of the reported results were evaluated.
Each domain could receive a "low," "moderate," "serious," "critical," or "no information" RoB rating, or a "no information" RoB rating. After that, each study was given an overall RoB assessment (study-level assessment) based on a different set of criteria. According to ROBINS, the overall RoB for a study was determined by assigning the most severe RoB judgment to each domain.
Data analyses
The data analyses and the ensuing data synthesis were conducted using R software, version 4.2.2 (R Foundation for Statistical Computing, Vienna, Austria; http://www.R-project.org). By inverse-variance method, standardized mean differences (SMD) was computed to evaluate continuous outcomes [27]. The Mantel-Haenszel method was used to produce the odds ratio (OR) and associated 95% confidence intervals (CI) as the effect estimate for all categorical data. Depending on the level of heterogeneity, a fixed-effect model and a random-effects model was employed to pool study-specific effect estimates for high heterogeneity and low heterogeneity. The Q-test and I2 were used to assess statistical heterogeneity. Low, moderate, and high heterogeneity were deemed to be represented by I2 values of 25, 50, and 75%, respectively [28]. If P>0.1 and I2<50%, a fixed effect model was used; otherwise, a random-effect model was applied [29]. To assess the publication bias, Egger's test was employed [30]. For all data analyses, with the exception of heterogeneity, a value of P<0.05 was taken as showing statistical significance, and all tests were two-sided.
Results
Study selection
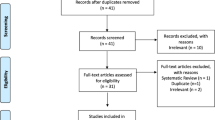
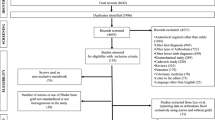
After collecting the search results from various databases and eliminating duplicate entries, a total of 224 articles were subjected to initial screening based on their titles and abstracts. Subsequently, the full text of 29 articles was assessed. Out of these, 21 articles were excluded due to issues such as the wrong design or comparison group, foreign language, absence of a control group, as well as similarity in the data. Eventually, eight articles were deemed unique and non-repetitive, and they were consequently incorporated into this systematic review (Fig. 1) [31,32,33,34,35,36,37,38]. Digiovanni et al. conducted a study in 2016 [39]. However, due to the similarity of the study population with their 2013 publication, and the 2013 study being more suitable for our current research, The authors have chosen to include the 2013 study in our systematic review.

PRISMA flow diagram
Risk of bias
Among the eight included articles, five of them are randomized clinical trials (RCTs), while the remaining studies are either retrospective or prospective cohorts. For the evaluation of the risk of bias, the ROBINs-I tool was used for cohorts, and the RoB 2 tool was employed for RCTs. The findings of the risk of bias assessment are summarized in supplementary data, Tables S2 and S3.
Bassline characteristics
A total of eight articles included in this review analyzed the data of 894 patients, 497 (55.6%) of them received synthetic bone grafts and 397 (44.4%) patients underwent surgical procedures using autologous bone grafts. Two studies were conducted collaboratively by researchers in the USA and Canada [31, 33]. One study was carried out in each of the USA [32], Canada [35], and Italy [34], while three studies were conducted in China [36,37,38]. The mean age ranged from 41.7 to 57.5 years, with a total of 484 males and 396 females included in the studies. Four articles reported body mass index (BMI), with a mean range of 20.26 to 31.4. Follow-up duration ranged from 9 to 145 months (Table 1).
In a total of eight studies, two different surgical techniques were utilized for various orthopedic purposes. Among these, arthrodesis surgery was employed in five studies [31,32,33, 35, 38], while three studies used open reduction [34, 36, 37]. In three of these studies, synthetic bone grafts consisting of a combination of recombinant human platelet-derived growth factor BB homodimer (rhPDGF-BB) and beta-tricalcium phosphate (β-TCP) collagen were employed [31,32,33]. The remaining four studies, except for Wan et al.'s study which did not specify details in this regard, employed hydroxyapatite compounds. All of these studies utilized entirely artificial grafts as synthetic bone substitutes. These surgical interventions targeted a range of bones and joints, including the ankle, calcaneus, subtalar, calcaneocuboid, and talonavicular (Table 2).
Arthrodesis
rhPDGF-BB/β-TCP bone graft
In three out of five studies, the rhPDGF-BB/β-TCP material was utilized as a synthetic bone graft [31,32,33]. In the studies, before patients received this synthetic graft material, the ingredients (rhPDGF-BB 0.3 mg/mL solution and β-TCP-collagen matrix) were combined and allowed at least 10 minutes to fully saturate before insertion at the fusion site using a cannula. A meta-analysis of these three studies revealed no significant difference between the synthetic and autologous groups in terms of CT fusion rate (OR [95%CI] = 0.95 [0.69-1.31], I2 = 0%) (Fig. 2). Regarding radiographic union rate, an analysis of all joints' three aspects union in Digiovanni et al.'s study indicated a significant difference between the two groups, favoring the synthetic bone graft (48.5% vs. 44.3%, P < 0.001) (Table 3) [33].

Forest plot illustrating the fusion rate assessed by CT scans in the synthetic (rhPDGF-BB/β-TCP bone graft) and autologous groups
Furthermore, no significant differences were observed in terms of American Orthopaedic Foot & Ankle Society (AOFAS) functional score (SMD [95%CI] = 0.03 [-0.13-0.18], I2 = 27%) (Fig. 3A), Foot Function Index (FFI) (SMD [95%CI] = 0.70 [-0.24-1.63], I2 = 97%) (Fig. 3B), and Short-Form 12 (SF-12) Physical Component Summary (PCS) (SMD [95%CI] = -1.41 [-3.13-0.31], I2 = 99%) (Fig. 3C). The visual analog scale (VAS) (pain) at the fusion site did not exhibit a significant difference (OR [95%CI] = 0.74 [-0.24-1.71], I2 = 98%) (Fig. 3D).

Forest plots illustrating A) American Orthopaedic Foot & Ankle Society (AOFAS) functional score, B) Foot Function Index (FFI), C) Short-Form 12 (SF-12) Physical Component Summary (PCS), and D) Visual Analog Scale (VAS) in the synthetic (rhPDGF-BB/β-TCP bone graft) and autologous groups
There were no significant differences in surgical complications between the two groups (OR [95%CI] = 1.03 [0.59-1.78], I2 = 60%) (Fig. 4). Additionally, Digiovanni et al. found no significant disparities in the occurrence of serious adverse events (P = 0.201), device-related adverse events (P = 0.354), or serious complications (P = 0.654) between the two groups [33]. similarly, Daniels et al. also reported no notable distinctions in the occurrence of serious adverse events (P = 1.00), device-related adverse events (P = 0.741), serious complications (P = 0.808), or infections (P = 0.127) between autologous or synthetic bone grafts (Table 5) [31].

Forest plot illustrating the surgical complications rate in the synthetic (rhPDGF-BB/β-TCP bone graft) and autologous groups
Other bone substitutes
Glazebrook et al. conducted a study on patients who underwent arthrodesis procedures, with 12 cases using B2A peptide-coated ceramic granules as a bone graft and 12 cases utilizing autologous grafts. They employed B2A peptide-coated ceramic granules in kit form, each containing a vial of lyophilized B2A peptide and porous granules composed of 80% tricalcium phosphate and 20% hydroxyapatite. They reported a 100% fusion success rate in the synthetic group compared to 66.7% in the autologous group, with an 83% complete union rate in the synthetic group and 58.3% in the autologous group (Table 3). At 6 months, 7 out of 12 subjects in both groups experienced a decrease in pain scores of at least 30%, while 1 out of 12 subjects in both groups had an increased pain score (Table 4). Graft site pain was reported by 2 patients at 6 months, and 2 patients in the synthetic group showed wound infections (Table 5) [35].
In a study led by Wan et al., they examined the outcomes of arthroscopy-assisted arthrodesis in two distinct groups, each consisting of 16 patients (not specified bone substitute type). Postoperative VAS and AOFAS scores did not show significant differences between the synthetic and autologous groups (P = 0.990 and 0.995, respectively) (Table 4) [38].
Open reduction and internal fixation (ORIF)
ORIF was the main surgical procedure in three papers [34, 36, 37]. In the study conducted by Lian et al., they utilized mineralized collagen as a synthetic bone graft, which was prepared in two main steps. Firstly, mineralized type I collagen fibrils were formed through the self-assembly of collagen triple helices and hydroxyapatite (HA). HA crystals nucleated and developed within collagen helices, a process regulated by collagen fibers. Secondly, mineralized type I collagen fibrils were combined with a polylactic acid solution to create mineralized collagen through comprehensive freeze-drying. The resulting product was then cut into small granules and sterilized. They discovered that there was no statistically significant difference in the time to union between the synthetic and autologous groups (8.3 and 7.9 weeks, respectively) (P > 0.05) [36]. Similarly, in Pan et al.'s study, no significant difference was observed, with values of 10.03 ± 1.73 and 9.80 ± 1.75 for the two groups, respectively (P = 0.606) (Table 3) [37]. The artificial mineralized collagen employed by them constituted a biomimetic bone graft, comprising arranged collagen and nano-sized hydroxyapatite.
Moreover, two of these studies also investigated radiographic angles, specifically Bohler and Gissane angles [34, 37]. The Bohler angle, discerned from a lateral foot radiograph, is determined by the angle formed between a line connecting the highest points of the anterior process of the calcaneus and the posterior articular facet, and another line linking the highest point of the posterior articular facet with the apex of the calcaneal tuberosity. Gissane angle is determined by tracing lines along the superior surfaces of the anterior process and the posterior facet of the calcaneus, culminating at the calcaneal sulcus. The Bohler angle is expected to range from 25° to 40°, while the Gissane angle typically falls between 125° and 145°, although there may be some variation about the standard normal range [40].
Both the Bohler and Gissane angles play pivotal roles in evaluating the severity of calcaneal fractures, with surgical intervention aiming to restore these angles to their standard values. Remarkably, both referenced studies found that post-surgery, these angles fell within the accepted normal range. Moreover, in Pan et al.'s investigation, no statistically significant distinction was observed between the two study groups in terms of postoperative angles (P < 0.05) (Table 3).
In Fortina et al.'s study, clinical examinations were carried out using the Creighton-Nebraska Health Foundation scoring system. The results showed no significant difference in residual pain levels between the synthetic and autologous groups, with values of 27.3 ± 2.6 and 29 ± 2.4, respectively (P > 0.05) [34]. Similarly, Lian et al. utilized the Maryland foot score to assess clinical outcomes, revealing a consistent absence of any notable difference between the two groups. Their findings indicated scores of 12 ± 90 and 10 ± 86 for the respective groups, with no statistically significant distinction evident (P > 0.05) [36]. Pan et al.'s study revealed similar findings, indicating that there was no statistically significant distinction in AOFAS scores (P = 0.071) between the synthetic group (88.37 ± 3.61) and the autologous group (88.37 ± 4.74) (Table 4) [37].
In Fortina et al.'s study, no instances of septic complications, reflex sympathetic dystrophies, or thrombophlebitis were reported [34]. In contrast, Lian et al. found that three out of 48 patients from both groups experienced wound infections in their study [36]. Conversely, Pan et al.'s investigation showed a comparable incidence of wound complications and rejections between the two groups, with eight out of 30 patients in the autologous group experiencing complications at the donor site [37] (Table 5).
Discussion
In the current systematic review, the authors found comparable complications, outcomes in radiological, and clinical measures between autograft and synthetic bone grafts. Autogenous bone graft has several advantages, including histocompatibility, osteogenecity, osteoconductive and osteoinductive properties, and no risk of disease transmission [41]. However, acquiring the autograft from the patient is an additional operation posing several complications related to the bone harvesting from donor site. Complications including blood loss, chronic pain at donor site, infection, nerve injury, and amplified surgical duration and expenses may occur due to autograft bone harvesting [41,42,43,44]. Furthermore, the patient's age, body mass index (BMI), gender, and overall health status can influence both the quality and quantity of accessible autograft materials [45]. On the other hand, synthetic bone grafts eliminate the potential risks associated with autografts. While synthetic bone grafts may not possess all the benefits of autografts, they have demonstrated favorable results in numerous instances, with potential for further enhancement.
Although the use of bone grafts in ankle arthrodesis is controversial, it is still widely used [46]. The authors found no differences when comparing the autograft with synthetic bone graft in terms of fusion, radiographic union, functional outcome, pain, and complications. As the most frequently used synthetic bone graft among included studies, rhPDGF-BB/β-TCP achieved comparable outcomes to autograft in arthrodesis. Since promoting osseous fusion is the primary goal of using grafts in arthrodesis [13], synthetic grafts can be considered as suitable alternatives based on our results.
Synthetic grafts typically consist of two components: a scaffold and a growth factor. β-TCP's calcium-to-phosphate ratio is similar to that of natural bone mineral, making it suitable for use as a scaffold. It is biocompatible and biodegradable, providing an osteoconductive matrix at the fusion site. Among various homodimers, PDGF-BB has been shown to be particularly important for bone regeneration, promoting mitogenesis, chemotaxis, extracellular matrix formation, and vascularization. Research has demonstrated that rhPDGF-BB can enhance the proliferation of various cell types and osteogenesis, further encouraging bone formation in fractures or defects. Recently, the combination of rhPDGF-BB and β-TCP has been used for ankle and foot fusion due to its exceptional bone healing properties [47,48,49,50,51]. Although, other types of synthetic grafts also achieved similar outcomes, further studies with larger sample sizes may reveal potential differences attributed to the additional osteoinductive properties. Nevertheless, achieving satisfactory results depends on using materials with properties closely resembling those of the autograft, including osteoconductivity, osteoinductivity, biocompatibility, and appropriate biomechanical properties. These grafts should mimic the structure of natural bone, support new bone growth, integrate well with existing tissues, and degrade at a rate that matches new bone formation [52, 53].
In foot and ankle procedures with ORIF, synthetic bone grafts also demonstrated similar outcomes to autografts. Bone grafts in ORIF of foot and ankle are usually used with aim of providing a mechanical support and to maintain alignment [54]. Two studies reporting Gissane and Bohler angles demonstrated restoration to standard values in both graft types. Moreover, time to union, as an important parameter in ORIF, was similar in both groups in 2 studies. Overall, no significant difference was found in radiographical, clinical, and pain-related outcomes and complications between the two groups. In fact, similarity of outcomes in terms of complications was regardless of the donor site morbidities and pain, which favors the use of synthetic bone grafts. Importantly, use of synthetic grafts aids surgeons in filling irregular defects in trauma surgeries, without the limitation posed by available autograft to be safely harvested [37].
A longer incorporation time for grafts which will be placed in anatomically weight-bearing sites demands higher structural stability, which in turn may limit the scaffold’s osteoconductive properties, further lengthening the incorporation time [55, 56]. Hence, the best option should be chosen considering this tradeoff.
Rapid incorporation of the graft to the host site, which is usually the case with foot and ankle surgeries, comes with a lack of durable structure to maintain osteoconductive and osteogenic properties of the graft. Cancellous bone grafts are therefore used most commonly in these surgeries [12]. Based on our review, procedures requiring grafts for the aforementioned purpose responded well to the use of synthetic bone grafts, highlighting the osteoconductive properties of these materials with minimal side effects. However, when structural stability (especially during the initial stages) becomes one of the main objectives, synthetic grafts are not functionally sufficient. Although outcomes such as pain and complications can still be similar, functional requirements of the procedure must be met in order to prevent revisions and validate the utilization of synthetic grafts. Newer synthetic grafts developed to overcome this drawback are necessary to replace autografts in procedures requiring structurally durable grafts.
Beyond assessing the risks and benefits, it is crucial for surgeons, hospitals, insurers, and patients to evaluate the economic impact of new technologies. Research has shown that using autografts incurs significant resource use, including extra operating room time, higher costs for supplies and personnel, additional medications, extended hospital stays, donor site complications, and both immediate and long-term side effects post-harvest [10, 57]. Moving forward, a critical comparison of the costs associated with autografts and synthetic bone grafts is necessary.
Our review was subject to certain limitations. While the majority of findings were in the same direction, the included studies were highly heterogenous, necessitating the use of random effects models in some of our analyses. Also, given the broad array of synthetic bone graft alternatives, the limited volume of research studies comparing their efficacy, either against autograft or within their category, necessitates cautious interpretation of our review's findings. Further prospective studies or RCTs are warranted to comprehensively evaluate and potentially improve synthetic bone grafts.
In conclusion, synthetic bone grafts show promise in achieving comparable outcomes to autografts in radiological, clinical, and quality-of-life measures, while also minimizing complications. Procedures requiring less structural support, such as those involving cancellous bone grafts, appear to benefit most from synthetic options. However, the variability in the data collected and the limited sample size and diversity of the studies underscore the need for further research to confirm these findings with greater certainty.
Availability of data and materials
The data used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Vosoughi AR, Hoveidaei AH, Roozbehi Z, Heydari Divkolaei SM, Zare S, Borazjani R. Patterns of Ankle Fractures Based on Radiographs and CT Images of 1000 Consecutive Patients. Arch Bone Jt Surg. 2024;12(2):128–35. https://doi.org/10.22038/ABJS.2023.71767.3350.
Hoveidaei AH, Nakhostin-Ansari A, Heckmann ND, et al. Increasing Burden of Lower-Extremity Fractures in the Middle East and North Africa (MENA): A 30-Year Epidemiological Analysis. J Bone Joint Surg Am. 2024;106(5):414–24. https://doi.org/10.2106/JBJS.23.00489.
Vosoughi AR, Borazjani R, Ghasemi N, Fathi S, Mashhadiagha A, Hoveidaei AH. Different types and epidemiological patterns of calcaneal fractures based on reviewing CT images of 957 fractures. Foot Ankle Surg. 2022;28(1):88–92.
Vosoughi AR, Fereidooni R, Shirzadi S, Zomorodian SA, Hoveidaei AH. Different patterns and characteristics of Talar injuries at two main orthopedic trauma centers in Shiraz, south of Iran. BMC Musculoskelet Disord. 2021;22(1):1–13.
Hoveidaei AH, Roshanshad A, Vosoughi AR. Clinical and radiological outcomes after arthrodesis of the first metatarsophalangeal joint. Int Orthop. 2021;45:711–9.
Vosoughi AR, Medhati P, Hosseini E, Labidi M, Hoveidaei AH. Clinical outcomes following treatment of deep surgical site infection after fixation of calcaneal fractures: a retrospective case-control study. Foot Ankle Surg. 2023;29(4):334–40.
Ghaseminejad-Raeini A, Azarboo A, Pirahesh K, Sharafi A, Hoveidaei AH, Nwankwo BO, et al. Antibiotic-coated intramedullary nailing managing long bone infected non-unions: a meta-analysis of comparative studies. Antibiotics. 2024;13(1):69.
Haralson RH 3rd, Zuckerman JD. Prevalence, health care expenditures, and orthopedic surgery workforce for musculoskeletal conditions. JAMA. 2009;302(14):1586–7.
Burton A, Aynardi MC, Aydogan U. Demographic Distribution of Foot and Ankle Surgeries Among Orthopaedic Surgeons and Podiatrists: A 10-Year Database Retrospective Study. Foot Ankle Specialist. 2021;14(3):206–12.
Lohmann H, Grass G, Rangger C, Mathiak G. Economic impact of cancellous bone grafting in trauma surgery. Arch Orthop Trauma Surg. 2007;127(5):345–8.
Baldwin P, Li DJ, Auston DA, Mir HS, Yoon RS, Koval KJ. Autograft, allograft, and bone graft substitutes: clinical evidence and indications for use in the setting of orthopaedic trauma surgery. J Orthop Trauma. 2019;33(4):203–13.
Miller CP, Chiodo CP. Autologous bone graft in foot and ankle surgery. Foot Ankle Clin. 2016;21(4):825–37.
Asomugha EU, Den Hartog BD, Junko JT, Alexander IJ. Tibiotalocalcaneal Fusion for Severe Deformity and Bone Loss. J Am Acad Orthop Surg. 2016;24(3):125–34.
Arner JW, Santrock RD. A historical review of common bone graft materials in foot and ankle surgery. Foot Ankle Specialist. 2014;7(2):143–51.
Sun H, Lu PP, Zhou PH, Sun SW, Zhang HT, Liu YJ, et al. Recombinant human platelet-derived growth factor-BB versus autologous bone graft in foot and ankle fusion: a systematic review and meta-analysis. Foot Ankle Surg. 2017;23(1):32–9.
Bhatt RA, Rozental TD. Bone graft substitutes. Hand Clin. 2012;28(4):457–68.
Valtanen RS, Yang YP, Gurtner GC, Maloney WJ, Lowenberg DW. Synthetic and Bone tissue engineering graft substitutes: What is the future? Injury. 2021;52(Suppl 2):S72-s7.
Campana V, Milano G, Pagano E, Barba M, Cicione C, Salonna G, et al. Bone substitutes in orthopaedic surgery: from basic science to clinical practice. J Mater Sci Mater Med. 2014;25(10):2445–61.
Buser Z, Brodke DS, Youssef JA, Meisel HJ, Myhre SL, Hashimoto R, et al. Synthetic bone graft versus autograft or allograft for spinal fusion: a systematic review. J Neurosurg Spine. 2016;25(4):509–16.
Al-Moraissi EA, Alkhutari AS, Abotaleb B, Altairi NH, Del Fabbro M. Do osteoconductive bone substitutes result in similar bone regeneration for maxillary sinus augmentation when compared to osteogenic and osteoinductive bone grafts? A systematic review and frequentist network meta-analysis. Int J Oral Maxillofac Surg. 2020;49(1):107–20.
Hofmann A, Gorbulev S, Guehring T, Schulz AP, Schupfner R, Raschke M, et al. Autologous Iliac bone graft compared with biphasic hydroxyapatite and calcium sulfate cement for the treatment of bone defects in tibial plateau fractures: a prospective, randomized, open-label, multicenter study. J Bone Joint Surg Am Vol. 2020;102(3):179–93.
Klifto CS, Gandi SD, Sapienza A. Bone graft options in upper-extremity surgery. J Hand Surg. 2018;43(8):755-61.e2.
Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097.
Minozzi S, Cinquini M, Gianola S, Gonzalez-Lorenzo M, Banzi R. The revised Cochrane risk of bias tool for randomized trials (RoB 2) showed low interrater reliability and challenges in its application. J Clin Epidemiol. 2020;126:37–44.
Morgan RL, Thayer KA, Santesso N, Holloway AC, Blain R, Eftim SE, et al. Evaluation of the risk of bias in non-randomized studies of interventions (ROBINS-I) and the “target experiment” concept in studies of exposures: Rationale and preliminary instrument development. Environ Int. 2018;120:382–7.
Sterne JA, Hernán MA, Reeves BC, Savović J, Berkman ND, Viswanathan M, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016;355:i4919.
Lin L, Aloe AM. Evaluation of various estimators for standardized mean difference in meta-analysis. Stat Med. 2021;40(2):403–26.
Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–60.
Nikolakopoulou A, Mavridis D, Salanti G. How to interpret meta-analysis models: fixed effect and random effects meta-analyses. Evid Based Ment Health. 2014;17(2):64.
Lin L, Chu H. Quantifying publication bias in meta-analysis. Biometrics. 2018;74(3):785–94.
Daniels TR, Anderson J, Swords MP, Maislin G, Donahue R, Pinsker E, et al. Recombinant Human Platelet-Derived Growth Factor BB in Combination With a Beta-Tricalcium Phosphate (rhPDGF-BB/β-TCP)-Collagen Matrix as an Alternative to Autograft. Foot Ankle Int. 2019;40(9):1068–78.
Digiovanni CW, Baumhauer J, Lin SS, Berberian WS, Flemister AS, Enna MJ, et al. Prospective, randomized, multi-center feasibility trial of rhPDGF-BB versus autologous bone graft in a foot and ankle fusion model. Foot Ankle Int. 2011;32(4):344–54.
DiGiovanni CW, Lin SS, Baumhauer JF, Daniels T, Younger A, Glazebrook M, et al. Recombinant human platelet-derived growth factor-BB and beta-tricalcium phosphate (rhPDGF-BB/β-TCP): an alternative to autogenous bone graft. J Bone Joint Surg Am. 2013;95(13):1184–92.
Fortina A, Bertone C, Rondini A. Reconstruction of calcaneal skeletal defects caused by trauma. J Foot Ankle Surg. 1998;37(5):386–90.
Glazebrook M, Younger A, Wing K, Lalonde KA. A prospective pilot study of B2A-coated ceramic granules (Amplex) compared to autograft for ankle and hindfoot arthrodesis. Foot Ankle Int. 2013;34(8):1055–63.
Lian K, Hong L, Xiaodong G, Fuzhai C, Zhiye Q, Shuyun X. The mineralized collagen for the reconstruction of intra-articular calcaneal fractures with trabecular defects. Biomatter. 2013;3(4):e27250-1-e27250-5. https://doi.org/10.4161/biom.27250.
Pan YX, Yang GG, Li ZW, Shi ZM, Sun ZD. Clinical observation of biomimetic mineralized collagen artificial bone putty for bone reconstruction of calcaneus fracture. Regen Biomater. 2018;5(2):61–7.
Wan J, Liu L, Zeng Y, Ren H, Zhang S. Comparison of different bone graft with arthroscopy-assisted arthrodesis for the treatment of traumatic arthritis of the subtalar joint. Int Orthop. 2020;44(12):2719–25.
DiGiovanni CW, Lin SS, Daniels TR, Glazebrook M, Evangelista P, Donahue R, et al. The importance of sufficient graft material in achieving foot or ankle fusion. J Bone Joint Surg Am. 2016;98(15):1260–7.
Lau BC, Allahabadi S, Palanca A, Oji DE. Understanding radiographic measurements used in foot and ankle surgery. J Am Acad Orthop Surg. 2022;30(2):e139–54.
Schmidt AH. Autologous bone graft: Is it still the gold standard? Injury. 2021;52(Suppl 2):S18-s22.
DeOrio JK, Farber DC. Morbidity associated with anterior iliac crest bone grafting in foot and ankle surgery. Foot Ankle Int. 2005;26(2):147–51.
Frohberg U, Mazock JB. A review of morbidity associated with bone harvest from the proximal tibial metaphysis. Mund Kiefer Gesichtschir. 2005;9(2):63–5.
Fillingham Y, Jacobs J. Bone grafts and their substitutes. Bone Joint J. 2016;98-b(1 Suppl A):6–9.
Cherukuri L, Kinninger A, Birudaraju D, Lakshmanan S, Li D, Flores F, et al. Effect of body mass index on bone mineral density is age-specific. Nutr Metab Cardiovasc Dis. 2021;31(6):1767–73.
Heifner JJ, Monir JG, Reb CW. Impact of bone graft on fusion rates in primary open ankle arthrodesis fixated with cannulated screws: a systematic review. J Foot Ankle Surg. 2021;60(4):802–6.
DiGiovanni CW, Lin S, Pinzur M. Recombinant human PDGF-BB in foot and ankle fusion. Expert Rev Med Devices. 2012;9(2):111–22.
Thaler M, Lechner R, Gstöttner M, Kobel C, Bach C. The use of beta-tricalcium phosphate and bone marrow aspirate as a bone graft substitute in posterior lumbar interbody fusion. Eur Spine J. 2013;22(5):1173–82.
Fiedler J, Etzel N, Brenner RE. To go or not to go: Migration of human mesenchymal progenitor cells stimulated by isoforms of PDGF. J Cell Biochem. 2004;93(5):990–8.
Caplan AI, Correa D. PDGF in bone formation and regeneration: new insights into a novel mechanism involving MSCs. J Orthop Res. 2011;29(12):1795–803.
Khojasteh A, Dashti SG, Dehghan MM, Behnia H, Abbasnia P, Morad G. The osteoregenerative effects of platelet-derived growth factor BB cotransplanted with mesenchymal stem cells, loaded on freeze-dried mineral bone block: a pilot study in dog mandible. J Biomed Mater Res B Appl Biomater. 2014;102(8):1771–8.
Georgeanu VA, Gingu O, Antoniac IV, Manolea HO. Current options and future perspectives on bone graft and biomaterials substitutes for bone repair, from clinical needs to advanced biomaterials research. Appl Sci. 2023;13(14):8471.
Sohn H-S, Oh J-K. Review of bone graft and bone substitutes with an emphasis on fracture surgeries. Biomater Res. 2019;23(1):9.
Panchbhavi VK. Synthetic bone grafting in foot and ankle surgery. Foot Ankle Clin. 2010;15(4):559–76.
Oryan A, Alidadi S, Moshiri A, Maffulli N. Bone regenerative medicine: classic options, novel strategies, and future directions. J Orthop Surg Res. 2014;9(1):18.
Griffin KS, Davis KM, McKinley TO, Anglen JO, Chu TMG, Boerckel JD, et al. Evolution of Bone Grafting: Bone Grafts and Tissue Engineering Strategies for Vascularized Bone Regeneration. Clin Rev Bone Mineral Metab. 2015;13(4):232–44.
Dahabreh Z, Calori GM, Kanakaris NK, Nikolaou VS, Giannoudis PV. A cost analysis of treatment of tibial fracture nonunion by bone grafting or bone morphogenetic protein-7. Int Orthop. 2009;33(5):1407–14.
Acknowledgements
None.
Funding
None.
Author information
Authors and Affiliations
Contributions
All the authors (Amir Human Hoveidaei, Amirhossein Ghaseminejad-Raeini, Sina Esmaeili, Amirmohammad Sharafi, Ali Ghaderi, Kasra Pirahesh, Alireza Azarboo, Basilia Onyinyechukwu Nwankwo, Janet D. Conway) have contributed to this research conceptualization and Manuscript drafting. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not Applicable (NA).
Consent for publication
NA.
Competing interests
JDC is a Consultant for Link and Resolute Med, Avitus, BoneSupport, Johnson and Johnson, and Orthofix - Not related to this work. JDC Receives Fellowship Support from Biocomposites and BoneSupport – Not related to this work.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Hoveidaei, A.H., Ghaseminejad-Raeini, A., Esmaeili, S. et al. Effectiveness of synthetic versus autologous bone grafts in foot and ankle surgery: a systematic review and meta-analysis. BMC Musculoskelet Disord 25, 539 (2024). https://doi.org/10.1186/s12891-024-07676-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-024-07676-8