
Abstract
Introduction
This study aims to compare cup inclination achieved (1) Using two orientation guides, whilst using the same 3-point pelvic positioner and (2) Using two types of pelvic positioners, whilst measuring intra-operative cup inclination with an inclinometer.
Materials and methods
This is a prospective, diagnostic cohort study of a consecutive series of 150 THAs performed through a posterior approach. Two types of 3-point pelvic positioners were used (Stulberg and modified Capello Hip Positioners) and the cup was positioned freehand using one of two orientation guides (mechanical guide or digital inclinometer). Intra-operative inclination was recorded, radiographic cup inclination and anteversion were measured from radiographs. The differences in inclination due to pelvic position (ΔPelvicPosition) and orientation definitions (ΔDefinition) were calculated. Target radiographic inclination and anteversion was 40/20° ± 10°.
Results
There was no difference in radiographic cup inclination/ (p = 0.63) using a mechanical guide or digital inclinometer. However, differences were seen in ΔPelvicPosition between the positioners ((Stulberg: 0° ± 5 vs. Capello: 3° ± 6); p = 0.011). Intra-operative inclination at implantation was different between positioners and this led to equivalent cases within inclination/anteversion targets (Stulberg:84%, Capello:80%; p = 0.48).
Conclusions
With the pelvis securely positioned with 3-point supports, optimum cup orientation can be achieved with both alignment guides and inclinometer. Non-optimal cup inclinations were seen when intra-operative inclinations were above 40° and below 32°, or the ΔPelvicPosition was excessive (> 15°; n = 2). We would thus recommend that the intra-operative cup inclination should be centered strictly between 30° and 35° relative to the floor. Small differences exist between different type of pelvic positioners that surgeons need to be aware off and account for.
Similar content being viewed by others


Introduction
Acetabular component (cup) orientation is associated with outcome following hip arthroplasty [1,2,3]. The resultant cup orientation is dependent upon (a) the pelvic position at time of cup impaction; and (b) the orientation of the cup provided by surgeon during impaction [4,5,6,7]. When operating in the lateral position, great variability in the use of pelvic support exists [8, 9]. The utilization of positioners with 3-point support is associated with less intra-operative movement [6]. However, 3-point support may be achieved with a number of commercially available supports [8]; whether all provide similar degrees of constraint is unknown.
The ability of surgeons to judge inclination angles in the lateral decubitus position varies significantly [10]. To aid surgeons, the use of mechanical aids has been advocated. However, these aids vary by implant and may lead to high inclination values [11]. As such many have advocated the use of an inclinometer to better quantify intra-operative inclination and improve radiographic cup inclinations [7, 12, 13].
The aims of this study were to compare radiographic cup inclination achieved (1) Using two types of orientation guides (inclinometer or alignment guide), whilst using the same 3-point pelvic positioner; and (2) Using two types of pelvic positioners, whilst measuring intra-operative cup inclination with an inclinometer. In doing so, factors leading to cup mal-orientation were identified.
Materials and methods
This is a prospective, institutional review board (IRB)-approved, single-surgeon, consecutive, case-series from a tertiary center. The study was conducted according to the Helsinki Declaration of 2008 and all patients gave informed consent.
One hundred and fifty consecutive primary total hip arthroplasties (THAs) performed through the posterior approach that had an uncemented acetabular component fixation, were studied between 2018 and 2020. Most patients were female (n = 88, 59%) and mean age at arthroplasty was 61 (±15) years old. The mean BMI was 30.9 ± 6.2 and the average adipose tissue depth (thickness of adipose tissue measured between skin and fascia lata at the level of the greater trochanter measured with a sterile ruler) was 6.7 ± 2.7 cm. Uncemented THAs were implanted in 116 cases and hybrid fixation in 34. The mean cup size was 50 ± 4 mm. Patient demographics and diagnoses are included in Table 1.
Pelvic position & support used
Two different types of pelvic positioners were used as per availability which depended on the hospital site the surgery was performed at. There were no demographic differences (including diagnosis and thickness of fat) between groups. The 2 pelvic positioners used were the Stulberg Hip Positionerand the Capello Hip Positioner (both Innomed Inc., Savannah, GA, USA). As the Capello Hip Positioner may not provide enough support on the anterior superior iliac spine (ASIS) on the operated side, an additional bolster was used as illustrated (Fig. 1) in all cases. Of the 150 cases; 100 were performed with the Stulberg and 50 were performed with the Capello Hip Positioner. All cases were positioned in the lateral decubitus position with the aim of having the operated hemi-pelvis as close to a neutral position, i.e. ‘perpendicular’, relative to the table in all planes at the time of cup impaction as possible. Given that the pelvis moves during surgery with the operated hemi-pelvis typically rotating internally during the posterior approach, the pelvis was aimed to be set with a slight externally rotated position of the operated hemi-pelvis (e.g. achieved with placing 2 blocks on the operated ASIS and 1 on the non-operated ASIS with the Stulberg Hip Positioner and visually with the Capello Positioner) [6, 7, 14, 15].

A Photograph illustrating pelvic positioning with the Capello Hip Positioner (pegboard with a modification, which is a single extra support over the operated Anterior Superior Iliac Spine). B Photograph illustrating pelvic positioning with the Stulberg Hip Positioner (no pegboard and three-point positioning system)
Acetabular preparation & impaction
It was ensured that the patient was securely positioned and that the operating table was level. A posterior approach was performed in all procedures. The acetabular component anteversion was placed taking into consideration, the orientation of the transverse acetabular ligament (TAL), the version of the femoral component and the combined anteversion value as femoral preparation proceeded that of the acetabulum. The acetabular component inclination was positioned freehand using one of 2 visual aids; a mechanical guide as per manufacturer set at inclination/anteversion: 45/20° in 50 consecutive THAs, or an inclinometer device (Digital Protractor Angle Gauge Finder, TEKCOPLUS, ASIN: B01HBIANG4) in the remaining 100 consecutive THAs [12, 16] (Fig. 2A&B). For all cases, it was aimed that the intra-operative inclination was less than 45° (i.e. guide not parallel to floor but pointing towards ceiling or measured inclination with inclinometer ≤45°) as this has been shown to lead to higher post-operative radiographic inclinations [17]; furthermore, a strict inclinometer reading target range was not utilized as in previous studies [7, 12, 13]. The inclination angle was not adjusted as per adipose tissue thickness or BMI [12]; however, whenever a varus femoral stem was used (n = 6), low inclination values were avoided as best as possible to reduce incidence of impingement in flexion and abduction as per technical guide [16]. Target cup orientation zone was defined as a radiographic inclination/anteversion of 40/20° ±10° [3, 18].

A & B Photograph illustrating the two visual cues used in this study (alignment guide – A and inclinometer – B) aligned with the impaction handle of the acetabular component
Parameters measured
The measured intra-operative inclination (IOI) angle was recorded from the inclinometer reading prior to disengaging the cup introducing handle, having ensured good cup fixation [12]. The IOI is the acetabular inclination of the cup/impactor relative to the operating table/floor. Radiographic cup inclination (RI) and anteversion (RA) was measured from post-operative, supine, anteroposterior (AP) pelvis radiographs obtained at the 6-week follow-up appointment, using the EBRA software (EBRA-cup; University of Innsbruck, Innsbruck, Austria) by an independent observer not involved with the care of these patients. The cup orientations of 15 cases (10%) were measured twice by the same reader and by a second reader to test intra- and inter- observer reliability. Average-measure correlation coefficients with a two-way random effects model for absolute agreement were calculated, showing excellent intra- and inter-observer reliabilities for radiographic measurements (range: 0.901 (95% CI; 0.705–0.969) to 0.932 (95% CI; 0.796–0.979).
Parameters calculated
Having established the radiographic cup orientation from the post-operative AP pelvic radiograph using the pelvic co-ordinate system, the true operative cup inclination (TOI) was determined using Murray’s nomograms [4]. The TOI is the operative inclination relative to the native pelvis that the surgeon impacted the cup at (Sin (operative inclination) = Sin (radiographic inclination) * Cos (radiographic anteversion), therefore TOI = ArcSin (Sin (RI) * Cos (RA)). The difference between the true operative inclination and the intra-operative inclination reflects the deviation of the pelvic position at the time of impaction from the desired position, as defined by the radiographic assessment, (ΔPelvicPosition = TOI – IOI). The inherent difference between the radiographic and true operative inclination has been described by Murray’s definitions and is dependent on the cosine function of operative anteversion (ΔDefinition = RI – TOI).
Analyses performed
Measurements of interest were the radiographic cup orientations achieved, the percentage of cases within target orientation, ΔPelvicPosition and ΔDefinition. We tested for potential differences in these measurements between cases with different types of pelvic positioner and different types of visual aids. To account for pelvic support and visual aids, the effect of visual aid used was only tested in cases that the Stulberg positioner was used for (n = 100). Similarly, the effect of positioner was only tested for cases that IOI was measured with the inclinometer (n = 100).
Statistics
We wanted to be able to detect a minimum difference in pelvic movement for abduction or adduction in the coronal plane of 5° between the two different positioner systems. We therefore performed a sample size calculation a priori, based upon previously published data on intraoperative pelvic movement with different supports, resulting in a minimum cohort size of 41 patients per group (α = 0.05, 1-β = 0.95, mean difference of 5° between groups (SD6°) [6, 19]. Furthermore, a ΔPelvicPosition greater than 10° was considered significant as the size of most safe zone described are of a ± 10° margin [1, 18, 20]. Variability was defined as 2 × standard deviations (SD). Non-parametric tests (Mann–Whitney U test, Spearman’s rho) were used. The chi-squared test was used for cross-tabulated data. Statistical significance was defined as a p ≤ 0.05. Analyses were performed with SPSS Statistics version 26 (IBM Corp., Armonk, New York).
Results
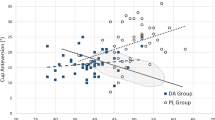
The cohort’s mean radiographic inclination was 41° ± 7 (range: 23–59). Optimum inclination was achieved in 138 THAs (92%) (Table 2 and Fig. 3). For cases that the inclinometer was used; the mean IOI was 35° ± 4 (range: 24–46) and the mean TOI was 7° ± 5 (range: 21–50). The mean ΔPelvicPosition was 2° ± 5 (range: − 13 to 16). The mean ΔDefinition was 4° ± 2 (range: 0–13) (Fig. 3).

Scatterplot illustrating the cup orientations achieved (as measured with the EBRA software for inclination and anteversion (green area indicating the target cup orientation zone of inclination/anteversion of 40/20° ±10°). The graph is color coded for the two pelvic positioners used in the study
Accounting for the pelvic positioner used (Stulberg), there appeared to be no clinically significant difference in the radiographic cup inclination (42° ± 6 vs. 42° ± 6; p = 0.63) or anteversion (23° ± 5 vs. 22° ± 5; p = 0.32) obtained for the two visual aids used. The TOI was similar whether the mechanical alignment guide (38° ± 5) or inclinometer (37° ± 5) was used (p = 0.9). There was no difference for the distribution of cups with optimum orientation for the two different visual aids used (44/50 vs. 42/50; p = 0.56) (Table 3).
Account for the visual aid used, differences in the pelvic positioners were identified (Table 3). Although, ΔDefinition was similar between positioners the Stulberg Group (4° ± 2) compared to the Capello (4° ± 2) (p = 0.355), there was a significant difference in ΔPelvicPosition (Stulberg: 0° ± 5 vs. Capello: 3° ± 6; p = 0.011). There were less cases with significant ΔPelvicPosition in the Stulberg (3/50) compared to the Capello group (10/50) (p = 0.037).
There were 8 out of the 100 inclinometer cases with sub-optimal inclinations. Four THAs had high inclinations (54°, 56°, 56°, 57°), with intra-operative inclinations that were 37°, 27°, 40° and 46°, respectively. Four THAs had low inclinations (23°, 26, 27°, 27°); with intra-operative inclinations that were 26°, 30°, 32° and 32°, respectively (Fig. 4 and Table 4). Cup mal-orientation were associated with both ΔPelvicPosition (− 7° ± 4 vs. 2° ± 5 vs. 10° ± 5; p < 0.001) and ΔDefinition (2° ± 5 vs. 4° ± 2 vs. 8° ± 4; p < 0.001) but the effect of ΔPelvicPosition was greater (Fig. 5).

Multiple line, color-coded, diagram illustrating the intra-operative, radiographic and true operative cup inclination values for each hip arthroplasty performed with the use of an inclinometer. Data provided can be used to identify underlying cause for inclination being out of target for each of the 100 cases in the group. Identifying the difference in value for each of the cases in the study. By assessing the angular differences between TOI (orange line) and IOI (blue line) (i.e. measure of ΔPelvicPosition) and the differences between RI (green line) and TOI (orange line) (i.e. measure of ΔDefinition), one can determine what was the underlying cause for each of the outliers seen in this study

Box and whisker plot illustrating the difference ΔPelvicPosition and ΔDefinition for the three cup inclination groups (Unacceptable – low; Acceptable and Unacceptable – High). The range of ΔPelvicPosition is much greater (−13° to + 16°) than the range of ΔDefinition as seen in graph (0 to + 13°) amongst all groups
Discussion
In this prospective study, the mean radiographic inclination (41°) achieved were as per target of 40° and the variability was in line with previous reports (12°). By standardizing factors that have been shown to influence resultant cup orientation (surgeon, approach, and 3-point supports) we illustrated that differences exist between different pelvic supports that surgeons should be aware off. Furthermore, we tested whether the inclinometer use was associated with improved chances of obtaining target cup orientation when the pelvic is well supported. Contrary to previous reports, highlighting the beneficial effect of the inclinometer, in this study the chances of obtaining optimum orientation was similar regardless of visual aid used; however, this is likely to be the case because the inclinometer did not strictly dictate IOI as in previous studies [7, 12, 13]. Non-optimal cup inclinations were seen in cases that the intra-operative inclinations were above 40° and below 32°, or the ΔPelvicPosition was excessive (> 15°; n = 2). We would thus recommend that the intra-operative cup inclination should be centered about 35°, when using 3-point pelvic supports.
Operating in the lateral decubitus position is associated with greater variability in pelvic position at impaction and an associated increased variability in the cup orientations achieved [19]. In the lateral decubitus position, it is primarily the pelvic position at impaction that is the cause of the great variability seen [7, 12, 13]. Type of pelvic support is associated with degree of intra-operative movement and 3-point positioners are associated with the least intra-operative movement during a THA [6]. However, not all 3-point of pelvic positioners provide similar support. In this study, the Stulberg positioner was associated with smaller ΔPelvicPosition (0° Vs. 3°) compared to the Capello one. This led to significantly closer orientations between the intra-operative (37° vs. 32°) and the resultant radiographic (41° vs. 39°). The resultant orientations were not as different as the ΔPelvicPosition and this was due to the intra-operative orientation differences between positioners; illustrating the surgeon likely accommodated for this effect probably due to anatomical clues used in his practice (e.g. TAL). This led to equivalent chances of achieving the radiographic cup orientation target.
The orientation of the cup at impaction and the ‘offset’ due to angular projections (Murray’s definitions) are also important in determining orientation. Two commonly described methods to assess cup inclination angle at impaction, relative to the horizontal, are mechanical alignment guides and the use of an inclinometer. Contrary to previous reports that only reported on the relationship between the intra-operative and resultant radiographic inclination [7, 12, 13], the current study also took into accounted for the resultant radiographic anteversion as this has a significant effect on the difference in cup inclinations between operative and radiographic values (ΔDefinition). There was no difference in any of the parameters measured (inclination/version/chances of reaching cup orientation targets) between the visual aid groups. This likely occurred because there was no fixed narrow target of IOI with the inclinometer, contrary to previous study [3, 4, 7, 12, 18]. Overall, an intra-operative orientation < 45° was aimed for, as radiographic inclination is greater than operative inclination, but the cups were not impacted within a narrow range as evident by the measured IOI (24–46°) post-implantation. This allowed us to study what contributes to cup mal-orientation and whether too high or too low intra-operative inclination was the primary reason for most of the mal-orientated cases. The proportion of cases with cup orientations within the pre-determined target (84%), seem to be comparable to other large series (50–88%) [3, 20,21,22,23,24]. Several studies have investigated freehand cup-positioning, reporting a high variability of cups within the save zone for inclianation and anteversion ranging from 26 to 71% [25]. However, whether by reducing the intraoperative range would lead to less variability akin to that reported in navigated- (87–93%) [23, 24, 26] and robotically-assisted (98–100%) [24, 27] THA requires further study.
During a posterior approach to the hip, the operated hemi-pelvis at the time of impaction is adducted and internally rotated [5, 14, 15]. Thus, in order to achieve a desired radiographic inclination, the intra-operative inclination (relative to the floor) must be reduced more than the Murray definition differences(3–4°) [3, 4, 7, 12, 18]. Non-optimal cup inclinations were seen in cases that the intra-operative inclinations were above 40° and below 32°, or the ΔPelvicPosition was excessive (> 15°; n = 2). All patients with low inclinations, had higher IOIs recorded; this is likely to have occurred because the operated hemi-pelvis was external rotated (or abducted) at impaction. As radiographic cup orientation is very rarely less than the intra-operative but is commonly greater (5–10°: 40%) and occasionally significantly greater (> 10°: 30%), we would recommend an intra-operative cup inclination of 35°, which is in line with other recommendations [28]. Contemporary alignment guides should therefore be redesigned [17]. Until then, inclinometers should be used as the ability to judge a 5–10° reduction in inclination angle with a rod can significantly vary [10].
This study has several limitations. Firstly, it is a single surgeon series and thus suffers from operator-related biases. However, by assessing a single surgeon we were able to account for surgical-related biases which may relate to defined optimum target, ability to judge a three-dimensional angle, cup preparation and impaction techniques and pelvic set-up [1, 6, 10, 12, 18, 20, 29]. Secondly, cases were randomly assigned to the different types of pelvic supports used according to the hospital site that the operation took place, which was not associated with any patient-related bias. This is a pragmatic situation likely to be encountered by surgeons practicing in different institutions with different resources available. Thirdly, the Capello positioner was further reinforced with additional bolster and hence the results do not apply to those that use simply the pegboard, which is therefore likely to be associated with much greater ΔPelvicPosition as it cannot easily, or securely, support both ASIS. Fourthly, we could not detect a significant difference for optimally positioned cups between the two cup orientation aids or two different positioners, which might have been due to the small study cohort size. Lastly, we did not assess for any spinal pathology (e.g. scoliosis) or degree of pelvic obliquity influencing inclination angles at impaction.
In conclusion, when the pelvis is securely positioned with 3-point supports, optimum cup orientation can be achieved with both alignment guides and inclinometer. Non-optimal cup inclinations were seen when intra-operative inclinations were above 40° and below 32°, or the ΔPelvicPosition was excessive (> 15°; n = 2). We would thus recommend that the intra-operative cup inclination should be centered strictly between 30° and 35° relative to the floor [7, 12]. Small differences exist between different type of pelvic positioners that surgeons need to be aware off and account for when impacting the cup.
Availability of data and materials
The datasets used and/or analysed during the current study is available from the corresponding author on reasonable request.
Abbreviations
- THA:
-
Total Hip Arthroplasty
- IRB:
-
Institutional review board
- BMI:
-
Body Mass Index
- SD:
-
Standard Deviation
- ORIF:
-
Open Reduction and Internal Fixation
- ASIS:
-
Anterior superior iliac spine
- TAL:
-
Transverse acetabular ligament
- IOI:
-
Intra-operative inclination
- RI:
-
Radiographic cup inclination
- RA:
-
Radiographic cup anteversion
- AP:
-
Anteroposterior
- TOI:
-
True operative cup inclination
References
Lewinnek GE, Lewis JL, Tarr R, Compere CL, Zimmerman JR. Dislocations after total hip-replacement arthroplasties. J Bone Joint Surg Am. 1978;60(2):217–20.
Dorr LD, Wan Z. Causes of and treatment protocol for instability of total hip replacement. Clin Orthop Relat Res. 1998;355:144–51.
Grammatopoulos G, Thomas GE, Pandit H, Beard DJ, Gill HS, Murray DW. The effect of orientation of the acetabular component on outcome following total hip arthroplasty with small diameter hard-on-soft bearings. Bone Joint J. 2015;97-B(2):164–72.
Murray DW. The definition and measurement of acetabular orientation. J Bone Joint Surg Br. 1993;75(2):228–32.
Grammatopoulos G, Pandit HG, da Assuncao R, McLardy-Smith P, De Smet KA, Gill HS, et al. The relationship between operative and radiographic acetabular component orientation: which factors influence resultant cup orientation? Bone Joint J. 2014;96-B(10):1290–7.
Grammatopoulos G, Pandit HG, da Assuncao R, Taylor A, McLardy-Smith P, De Smet KA, et al. Pelvic position and movement during hip replacement. Bone Joint J. 2014;96-B(7):876–83.
Beverland DE, O'Neill CK, Rutherford M, Molloy D, Hill JC. Placement of the acetabular component. Bone Joint J. 2016;98-B(1 Suppl A):37–43.
Rutherford M, O'Connor JD, Hill JC, Beverland DE, Lennon AB, Dunne NJ. Patient positioning and cup orientation during total hip arthroplasty: assessment of current UK practice. Hip Int. 2019;29(1):89–95.
Milone MT, Schwarzkopf R, Meere PA, Carroll KM, Jerabek SA, Vigdorchik J. Rigid patient positioning is unreliable in Total hip Arthroplasty. J Arthroplast. 2017;32(6):1890–3.
Grammatopoulos G, Alvand A, Monk AP, Mellon S, Pandit H, Rees J, et al. Surgeons’ accuracy in achieving their desired Acetabular component orientation. J Bone Joint Surg Am. 2016;98(17):e72.
van Duren BH, Royeca JM, Cunningham CM, Lamb JN, Brew CJ, Pandit H. Can the use of an inclinometer improve acetabular cup inclination in total hip arthroplasty? A review of the literature. HIP Int. 2020;0(0):1120700020946716.
Meermans G, Goetheer-Smits I, Lim RF, Van Doorn WJ, Kats J. The difference between the radiographic and the operative angle of inclination of the acetabular component in total hip arthroplasty: use of a digital protractor and the circumference of the hip to improve orientation. Bone Joint J. 2015;97-B(5):603–10.
Darrith B, Bell JA, Culvern C, Della Valle CJ. Can the use of an inclinometer improve the positioning of the acetabular component in total hip arthroplasty? Bone Joint J. 2018;100-B(7):862–6.
Asayama I, Akiyoshi Y, Naito M, Ezoe M. Intraoperative pelvic motion in total hip arthroplasty. J Arthroplast. 2004;19(8):992–7.
Ezoe M, Naito M, Asayama I, Ishiko T, Fujisawa M. Pelvic motion during total hip arthroplasty with translateral and posterolateral approaches. J Orthop Sci. 2005;10(2):167–72.
JRI: https://www.scp.no/media/documents/Furlong_Evolution_Operative_technique.pdf. Last accessed 18 Sep 2022.
Minoda Y, Ohzono K, Aihara M, Umeda N, Tomita M, Hayakawa K. Are acetabular component alignment guides for total hip arthroplasty accurate? J Arthroplast. 2010;25(6):986–9.
Grammatopoulos G, Pandit H, Glyn-Jones S, McLardy-Smith P, Gundle R, Whitwell D, et al. Optimal acetabular orientation for hip resurfacing. J Bone Joint Surg Br. 2010;92(8):1072–8.
Grammatopoulos G, Gofton W, Cochran M, Dobransky J, Carli A, Abdelbary H, et al. Pelvic positioning in the supine position leads to more consistent orientation of the acetabular component after total hip arthroplasty. Bone Joint J. 2018;100-B(10):1280–8.
Danoff JR, Bobman JT, Cunn G, Murtaugh T, Gorroochurn P, Geller JA, et al. Redefining the Acetabular component safe zone for posterior approach Total hip Arthroplasty. J Arthroplast. 2016;31(2):506–11.
Callanan MC, Jarrett B, Bragdon CR, Zurakowski D, Rubash HE, Freiberg AA, et al. The John Charnley award: risk factors for cup malpositioning: quality improvement through a joint registry at a tertiary hospital. Clin Orthop Relat Res. 2011;469(2):319–29.
Barrack RL, Krempec JA, Clohisy JC, McDonald DJ, Ricci WM, Ruh EL, et al. Accuracy of acetabular component position in hip arthroplasty. J Bone Joint Surg Am. 2013;95(19):1760–8.
Xu K, Li YM, Zhang HF, Wang CG, Xu YQ, Li ZJ. Computer navigation in total hip arthroplasty: a meta-analysis of randomized controlled trials. Int J Surg. 2014;12(5):528–33.
Domb BG, Redmond JM, Louis SS, Alden KJ, Daley RJ, LaReau JM, et al. Accuracy of component positioning in 1980 Total hip Arthroplasties: a comparative analysis by surgical technique and mode of guidance. J Arthroplast. 2015;30(12):2208–18.
Meermans G, Grammatopoulos G, Innmann M, Beverland D. Cup placement in primary total hip arthroplasty: how to get it right without navigation or robotics. EFORT Open Rev. 2022;7(6):365–74.
Hohmann E, Bryant A, Tetsworth K. A comparison between imageless navigated and manual freehand technique acetabular cup placement in total hip arthroplasty. J Arthroplast. 2011;26(7):1078–82.
Domb BG, El Bitar YF, Sadik AY, Stake CE, Botser IB. Comparison of robotic-assisted and conventional acetabular cup placement in THA: a matched-pair controlled study. Clin Orthop Relat Res. 2014;472(1):329–36.
O'Neill CKJ, Hill JC, Patterson CC, Molloy DO, Gill HS, Beverland DE. Reducing variability in apparent operative inclination during total hip arthroplasty: findings of a randomised controlled trial. Hip Int. 2018;28(3):234–9.
Merle C, Innmann MM, Waldstein W, Pegg EC, Aldinger PR, Gill HS, et al. High variability of Acetabular offset in primary hip osteoarthritis influences Acetabular reaming-a computed tomography-based anatomic study. J Arthroplast. 2019;34(8):1808–14.
Acknowledgements
None.
Funding
Open Access funding enabled and organized by Projekt DEAL. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. For the publication fee we acknowledge financial support by Deutsche Forschungsgemeinschaft within the funding programme “Open Access Publikationskosten“ as well as by Heidelberg University.
Author information
Authors and Affiliations
Contributions
Moritz Innmann designed the study, acquired the data, performed the statistical analysis, interpreted the data, wrote and revised the manuscript. Jeroen Verhaegen designed the study, wrote and revised the manuscript. Christian Merle designed the study, wrote and revised the manuscript. Paul Beaulé designed the study, wrote and revised the manuscript. Geert Meermans designed the study, interpreted the data, wrote and revised the manuscript. George Grammatopoulos designed the study, performed the statistical analysis, interpreted the data, wrote and revised the manuscript. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was conducted according to the Helsinki Declaration of 2008 and all patients gave informed consent. Ethics approval was obtained from the Ottawa Health Science Network Research Ethics Board prior to data collection and we have complied with ethical principles regarding research with human participants.
Consent for publication
Not applicable.
Competing interests
The authors report no competing interests being relevant for this study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Innmann, M.M., Verhaegen, J., Merle, C. et al. Cup orientation following posterior approach THA – the effect of different visual aids and pelvic supports. BMC Musculoskelet Disord 23, 881 (2022). https://doi.org/10.1186/s12891-022-05820-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-022-05820-w