
Abstract
Background
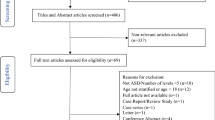
Pediatric spinal fusion may be associated with significant intraoperative blood loss, leading to complications from transfusion, hypoperfusion and coagulopathy. One emerging strategy to mediate these risks is by utilization of the anti-fibrinolytic agent tranexamic acid (TXA). However, concerns regarding potential adverse reactions, specifically postoperative seizures and thrombotic events, still exist. To assess these risks, we examined the perioperative morbidity of TXA use in a large national database.
Methods
Retrospective data from pediatric patients (age 18 years or younger), discharged between January 2013 to December 2015, who underwent primary or revision posterior spinal fusions, was collected from the Premier Perspective database (Premier, Charlotte, NC). Patients were stratified by TXA use and records were assessed for complications of new onset seizures, strokes, pulmonary embolisms (PE) or deep vein thromboses (DVT) occurring during the perioperative period.
Results
In this cohort of 2,633 pediatric patients undergoing posterior spinal fusions, most often to treat adolescent idiopathic scoliosis, 15% received TXA. Overall, adverse events were rare in this patient population. The incidence of seizure, stoke, PE, or DVT in the control group was 0.54% (95% CI, 0.31% to 0.94%) and not significantly different from the TXA group. There was no significant difference in the incidence of DVTs, and no incidences of stroke in either group. There were no new-onset seizures or PEs in patients who received TXA.
Conclusions
The use of TXA was not associated with an increased risk of adverse events including seizure, stroke, PE, and DVT. Our findings support the safety of TXA use in pediatric patients undergoing spinal fusion surgery.
Similar content being viewed by others

Background
Significant intraoperative blood loss occurring during pediatric spinal fusion may lead to complications associated with transfusion, hypoperfusion, and coagulopathy [1, 2]. One way to effectively decrease intraoperative blood loss is through the use of tranexamic acid (TXA), an antifibrinolytic agent [3,4,5]. This medication has been extensively used in cardiac surgery [6,7,8] and other types of orthopedic surgery [9,10,11,12,13], including spine surgery [14, 15]. Two studies, with large sample sizes of 1,769 and 4,269 pediatric patients undergoing spinal surgery assessed TXA use, but their findings were limited to TXA efficiency in decreasing blood loss without an analysis of adverse events associated with the drug [16, 17]. A few smaller studies, with sample sizes ranging from 44 to 166 patients, reported on the safety of TXA use in this population and did not find any associated adverse events [18,19,20,21,22,23,24,25]. However, concerns remain that rare, yet serious side effects, may not be adequately captured in a small sample.
Due to similarity in molecular structure, TXA may act as a competitive inhibitor of glycine (Fig. 1), and studies in animal models have demonstrated that competitive inhibition of glycine receptors by TXA could lead to excitation of neural tissues and result in seizure [26,27,28]. Some studies have found a link between TXA use and seizures in non-primate model organisms [29], and a few case reports have demonstrated this epileptic potential in humans [30,31,32]. Perhaps most importantly, multiple studies in adult patients found an increased risk of seizure after TXA use in cardiac surgery [33, 34]. However, the risk of this adverse event after TXA use in pediatric spine surgery is still unclear [6, 35, 36]. Additionally, due to its function as an anti-fibrinolytic agent, one concern of TXA use is the possibility of increased major thrombotic events such as pulmonary embolism (PE), deep vein thrombosis (DVT), and stroke. This is more frequently explored in the literature.

Chemical structures of glycine, an excitatory neurotransmitter and TXA
To address these concerns of TXA safety in pediatric spine fusion patients, we used a large national database to evaluate the association between TXA use and new-onset postoperative thrombotic events or seizures.
Methods
Data source
This study was a retrospective cohort analysis of the Premier Perspective Database (Premier, Charlotte, NC), which sources data from approximately 600 hospitals across the United States. This database is anonymized and contains encrypted identifiers to link longitudinal data from a single patient. Other data available include patient demographics, diagnostic/procedural coding information, including distinct codes for new onset diagnoses and those prior to admission, and drug administration during inpatient stays. The institutional review board at Weill Cornell Medicine approved this study and exempted the need for informed consent.
Patient cohort
Our study included patients 18 years or younger who were undergoing primary or revision posterior spinal fusions (ICD-9-CM procedure codes 81.0X or 81.3X) with discharge dates between January 1, 2013 to December 31, 2015. We identified all patients who had received TXA by searching for the term “tranexamic” in the list of the administered pharmaceuticals linked to their admission. Patients receiving any dose of TXA were categorized into the TXA group, and those without a note of the term “tranexamic” in their medication administration record were categorized into the non-TXA group. Charlson Comorbidity Index (CCI) was calculated for patients based on ICD-9-CM diagnosis codes using a previously reported algorithm [37].
Outcomes
We tracked the major complications of deep vein thromboses (451.X), pulmonary embolisms (415.1X), and seizures (780.39, 345.X), all of which were identified as new onset code identifiers associated with previously published codes for these diagnoses. We also examined a less commonly discussed complication of stroke (433.X1, 436). Additionally, for any patients with a documented history of seizure in a prior hospitalization, a diagnosis of seizure during the posterior spinal fusion admission was not considered “new onset”, even if it was identified with a new onset code modifier as such. Finally, we also examined the rate of mortality during the index hospitalization. For large dataset individual privacy protection, the exact rates of adverse events with fewer than 11 incidences were supressed.
Statistical analysis
Categorical variable differences were measured by Fisher’s Exact test or Chi-Squared as noted. Continuous variable differences were assessed by the 2-tailed Student t test or the Mann–Whitney test of nonnormally distributed data. Confidence intervals for fractions were calculated using the Wilson/Brown method. Odds ratios were calculated using the Baptista-Pike method. Statistical analysis was performed using Stata v14.2 (StataCorp, College Station, TX) and GraphPad Prism v9.0.2 (GraphPad Software, San Diego, California).
Results
Of the 2,633 pediatric patients who underwent spine fusion in our cohort, 96.2% underwent a primary fusion. The average age in the cohort was 14 ± 3 years; 64.5% were female, and 65.7% were white (Table 1). The most common reason for spinal fusion was a diagnosis of adolescent idiopathic scoliosis (AIS) which was present in 57.5% of patients, followed by traumatic injuries requiring fusion (12.8%). Less frequent (< 5%) primary diagnoses associated with posterior spinal fusion included congenital scoliosis, spondylolisthesis, neuromuscular scoliosis, and neoplastic causes as detailed in Fig. 2.

Diagnoses of pediatric spine fusion patients associated with surgical admission
A fraction of pediatric patients (15.3%, 402 patients) received TXA during their admission for posterior spinal fusion. There was no significant difference in the demographics, including age, sex, and race, or frequency of primary fusion between the two patient populations (Table 1). Patients in both groups had a low Charlton comorbidity index of 0.17.
There were no reported new onset seizures or PE in patients who received TXA perioperatively, and no statistically significant difference in incidence of DVT (Table 2). No strokes were reported in either cohort. There were also no cases of in-hospital mortality.
Overall, new diagnosis of DVT, PE, stroke, and seizure were rare, with no statistically significant difference between the two groups (p = 0.71, Table 2). The rate of any complication for patients not receiving TXA was 0.54% (95% CI, 0.31% to 0.94%). The odds ratio of complications in the group that received TXA compared to the group that did not was 0.46 (95% CI, 0.04 to 2.9).
Discussion
In this national sample of 2,633 pediatric patients undergoing posterior spinal fusion, thrombotic events (DVTs, PEs or strokes) were rare, and not associated with TXA use. Additionally, despite concerns that TXA could lead to excitation of neural tissues and prior reports showing seizures resulting from TXA use [30, 31], we did not find evidence of increased seizures in patients who received the drug. Overall, this data supports the safety of TXA in this pediatric population.
The reporting on TXA use in pediatric spine cases is increasing, including studies examining safety [18,19,20,21, 38,39,40,41,42,43]. While our literature search revealed multiple studies on TXA use in pediatric spine surgery, the majority of these, including two large retrospective cohort studies (N > 1,500), limited their findings to TXA efficacy in decreasing blood loss without analyzing adverse events [16, 17]. Out of the trials with a focus on safety of TXA use, all had limited sample sizes which ranged from 44 to 166 patients [18, 20,21,22, 24]. Meanwhile, research supporting TXA efficacy and safety in adult spine surgery has also been increasing [44, 45]. Multiple recent studies, including one randomized control trial of 68 thoracic spine stenosis patients and a retrospective analysis of 122 patients undergoing lumbar fusion, did not find any associated side effects with TXA use including the incidence of DVTs [46, 47]. Our findings are in line with this growing body of work demonstrating safety of TXA use in spine surgery.
The strength of our study is its large sample size, sampling of data from generalizable everyday practice, and focus on pediatric spine fusion patients. Our large sample size, multiple times larger than prior trials, allowed us to observe even rare side effects which may have been missed in smaller studies and demonstrate that TXA does not increase these risks.
Our findings must be interpreted with limitations. First, this work relied upon administrative data, which can have errors in the coding of diagnoses and procedures. We used previously published or validated code algorithms whenever possible to identify procedures, primary diagnoses, and adverse events in an attempt to mitigate this. However, the code for seizures has not been previously validated for sensitivity and specificity. Second, the new onset diagnosis code modifiers, used to determine if the adverse event occurred perioperatively instead of being a pre-existing condition, have not been specifically validated. As a result, it is possible that adverse events during the admission were undercounted for all patients. Additionally, the baseline and outcome measures which we were able to compare between the control and treatment groups were limited by the database, which did not include data such as the duration of surgery or surgeon experience. These effects may be confounders to our results.
Another surprising finding is that only a minority of patients received TXA in our study. However, this is in line with other large retrospective pediatric studies of TXA efficacy in spinal surgery, where 7% to 30% of the 4,269 and 1,769 patients received TXA respectively [16, 17]. Furthermore, in the context of trauma, this discrepancy was even more pronounced in our data, suggesting hesitation in TXA administration for this patient population. Other studies including a survey of pediatric trauma centers and a study of pediatric patients injured in a combat setting demonstrated similar findings where only a minority of the patients, 35% and 10% respectively were given TXA [48, 49]. This is despite previous research including the CRASH-2 trial demonstrating benefits of TXA use for adult trauma patients [50].
Despite these limitations, we feel that this work provides reassurance to surgeons and perioperative care teams incorporating TXA for the minimization of blood loss during posterior spinal fusion in pediatric patients.
Conclusions
In this study, TXA use was not associated with an increased risk of thrombotic events (pulmonary embolism, deep vein thrombosis or stroke) and did not precipitate any seizures. Our work demonstrates that the drug is relatively safe to use in the pediatric population for spinal surgery.
Availability of data and materials
The dataset analysed during the current study is not able to be shared by the authors, due to terms specified by the organization providing the data in a data use agreement. However, the data are available for purchase by the public from Premier Inc. (www.premierinc.com).
Abbreviations
- TXA:
-
Tranexamic acid
- PE:
-
Pulmonary embolism
- DVT:
-
Deep venous thrombosis
- AIS:
-
Adolescent idiopathic scoliosis
- CCI:
-
Charlson comorbidity index
References
Oetgen ME, Litrenta J. Perioperative Blood Management in Pediatric Spine Surgery: J Am Acad Orthop Surg. 2017;25(7):480–8. https://doi.org/10.5435/JAAOS-D-16-00035.
Fletcher ND, Marks MC, Asghar JK, Hwang SW, Sponseller PD, Newton PO. Development of Consensus Based Best Practice Guidelines for Perioperative Management of Blood Loss in Patients Undergoing Posterior Spinal Fusion for Adolescent Idiopathic Scoliosis*. Spine Deform. 2018;6(4):424–9. https://doi.org/10.1016/j.jspd.2018.01.001.
Hoylaerts M, Lijnen HR, Collen D. Studies on the mechanism of the antifibrinolytic action of tranexamic acid. Biochim Biophys Acta. 1981;673(1):75–85.
Dunn CJ, Goa KL. Tranexamic Acid: A Review of its Use in Surgery and Other Indications. Drugs. 1999;57(6):1005–32. https://doi.org/10.2165/00003495-199957060-00017.
Ker K, Prieto-Merino D, Roberts I. Systematic review, meta-analysis and meta-regression of the effect of tranexamic acid on surgical blood loss. Br J Surg. 2013;100(10):1271–9. https://doi.org/10.1002/bjs.9193.
Faraoni D, Rahe C, Cybulski KA. Use of antifibrinolytics in pediatric cardiac surgery: Where are we now? Pediatr Anesth. 2019;29(5):435–40. https://doi.org/10.1111/pan.13533.
Hardy JF, Desroches J. Natural and synthetic antifibrinolytics in cardiac surgery. Can J Anaesth J Can Anesth. 1992;39(4):353–65. https://doi.org/10.1007/BF03009046.
Barrons RW, Jahr JS. A REVIEW OF POST-CARDIOPULMONARY BYPASS BLEEDING, AMINOCAPROIC ACID, TRANEXAMIC ACID, AND APROTININ. Am J Ther. 1996;3(12):821–38. https://doi.org/10.1097/00045391-199612000-00007.
Porter SB, White LJ, Osagiede O, Robards CB, Spaulding AC. Tranexamic Acid Administration Is Not Associated With an Increase in Complications in High-Risk Patients Undergoing Primary Total Knee or Total Hip Arthroplasty: A Retrospective Case-Control Study of 38,220 Patients. J Arthroplasty. 2020;35(1):45-51.e3. https://doi.org/10.1016/j.arth.2019.08.015.
Veien M, Sørensen JV, Madsen F, Juelsgaard P. Tranexamic acid given intraoperatively reduces blood loss after total knee replacement: a randomized, controlled study. Acta Anaesthesiol Scand. 2002;46(10):1206–11. https://doi.org/10.1034/j.1399-6576.2002.461007.x.
Huang F, Wu D, Ma G, Yin Z, Wang Q. The use of tranexamic acid to reduce blood loss and transfusion in major orthopedic surgery: a meta-analysis. J Surg Res. 2014;186(1):318–27. https://doi.org/10.1016/j.jss.2013.08.020.
Iwai T, Tsuji S, Tomita T, Sugamoto K, Hideki Y, Hamada M. Repeat-dose intravenous tranexamic acid further decreases blood loss in total knee arthroplasty. Int Orthop. 2013;37(3):441–5. https://doi.org/10.1007/s00264-013-1787-7.
Friedman RJ, Gordon E, Butler RB, Mock L, Dumas B. Tranexamic acid decreases blood loss after total shoulder arthroplasty. J Shoulder Elbow Surg. 2016;25(4):614–8. https://doi.org/10.1016/j.jse.2015.09.014.
Shapiro F, Zurakowski D, Sethna NF. Tranexamic acid diminishes intraoperative blood loss and transfusion in spinal fusions for duchenne muscular dystrophy scoliosis. Spine. 2007;32(20):2278–83. https://doi.org/10.1097/BRS.0b013e31814cf139.
Zhao Y, Xi C, Xu W, Yan J. Role of tranexamic acid in blood loss control and blood transfusion management of patients undergoing multilevel spine surgery: A meta-analysis. Medicine (Baltimore). 2021;100(7): e24678. https://doi.org/10.1097/MD.0000000000024678.
Lonner BS, Ren Y, Asghar J, Shah SA, Samdani AF, Newton PO. Antifibrinolytic Therapy in Surgery for Adolescent Idiopathic Scoliosis Does the Level 1 Evidence Translate to Practice? Bull Hosp Jt Dis 2013. 2018;76(3):165–170.
McLeod LM, French B, Flynn JM, Dormans JP, Keren R. Antifibrinolytic Use and Blood Transfusions in Pediatric Scoliosis Surgeries Performed at US Children’s Hospitals. J Spinal Disord Tech. 2015;28(8):E460–6. https://doi.org/10.1097/BSD.0b013e3182a22a54.
Hasan MS, Yunus SN, Ng CC, Chan CYW, Chiu CK, Kwan MK. Tranexamic Acid in Pediatric Scoliosis Surgery: A Prospective Randomized Trial Comparing High-dose and Low-dose Tranexamic Acid in Adolescent Idiopathic Scoliosis Undergoing Posterior Spinal Fusion Surgery. Spine. 2021;46(22):E1170–7. https://doi.org/10.1097/BRS.0000000000004076.
Zhang Z, Wang LN, Yang X, et al. The effect of multiple-dose oral versus intravenous tranexamic acid in reducing postoperative blood loss and transfusion rate after adolescent scoliosis surgery: a randomized controlled trial. Spine J. 2021;21(2):312–20. https://doi.org/10.1016/j.spinee.2020.10.011.
Sethna NF, Zurakowski D, Brustowicz RM, Bacsik J, Sullivan LJ, Shapiro F. Tranexamic acid reduces intraoperative blood loss in pediatric patients undergoing scoliosis surgery. Anesthesiology. 2005;102(4):727–32. https://doi.org/10.1097/00000542-200504000-00006.
Dong Y, Liang J, Tong B, Shen J, Zhao H, Li Q. Combined topical and intravenous administration of tranexamic acid further reduces postoperative blood loss in adolescent idiopathic scoliosis patients undergoing spinal fusion surgery: a randomized controlled trial. BMC Musculoskelet Disord. 2021;22(1):663. https://doi.org/10.1186/s12891-021-04562-5.
Sui W yuan, Ye F, Yang J lin. Efficacy of tranexamic acid in reducing allogeneic blood products in adolescent idiopathic scoliosis surgery. BMC Musculoskelet Disord. 2016;17(1):187. doi:https://doi.org/10.1186/s12891-016-1006-y
Goobie SM, Zurakowski D, Glotzbecker MP, et al. Tranexamic Acid Is Efficacious at Decreasing the Rate of Blood Loss in Adolescent Scoliosis Surgery: A Randomized Placebo-Controlled Trial. J Bone Joint Surg Am. 2018;100(23):2024–32. https://doi.org/10.2106/JBJS.18.00314.
Yagi M, Hasegawa J, Nagoshi N, et al. Does the Intraoperative Tranexamic Acid Decrease Operative Blood Loss During Posterior Spinal Fusion for Treatment of Adolescent Idiopathic Scoliosis?: Spine. 2012;37(21):E1336-E1342. doi:https://doi.org/10.1097/BRS.0b013e318266b6e5
George S, Ramchandran S, Mihas A, George K, Mansour A, Errico T. Topical tranexemic acid reduces intra-operative blood loss and transfusion requirements in spinal deformity correction in patients with adolescent idiopathic scoliosis. Spine Deform. 2021;9(5):1387–93. https://doi.org/10.1007/s43390-021-00337-z.
Lecker I, Wang DS, Kaneshwaran K, Mazer CD, Orser BA. High Concentrations of Tranexamic Acid Inhibit Ionotropic Glutamate Receptors. Anesthesiology. 2017;127(1):89–97. https://doi.org/10.1097/ALN.0000000000001665.
Lecker I, Wang DS, Romaschin AD, Peterson M, Mazer CD, Orser BA. Tranexamic acid concentrations associated with human seizures inhibit glycine receptors. J Clin Invest. 2012;122(12):4654–66. https://doi.org/10.1172/JCI63375.
Kratzer S, Irl H, Mattusch C, et al. Tranexamic Acid Impairs γ-Aminobutyric Acid Receptor Type A–mediated Synaptic Transmission in the Murine Amygdala. Anesthesiology. 2014;120(3):639–49. https://doi.org/10.1097/ALN.0000000000000103.
Pellegrini A, Giaretta D, Chemello R, Zanotto L, Testa G. Feline Generalized Epilepsy Induced by Tranexamic Acid (AMCA). Epilepsia. 1982;23(1):35–45. https://doi.org/10.1111/j.1528-1157.1982.tb05051.x.
Garcha PS, Mohan CVR, Sharma RM. Death After an Inadvertent Intrathecal Injection of Tranexamic Acid: Anesth Analg. 2007;104(1):241–2. https://doi.org/10.1213/01.ane.0000250436.17786.72.
de Leede-van der Maarl MGJ, Hilkens P, Bosch F. The epileptogenic effect of tranexamic acid. J Neurol. 1999;246(9):843–843. doi:https://doi.org/10.1007/s004150050466
Yeh HM, Lau HP, Lin PL, Sun WZ, Mok MS. Convulsions and Refractory Ventricular Fibrillation after Intrathecal Injection of a Massive Dose of Tranexamic Acid. Anesthesiology. 2003;98(1):270–2. https://doi.org/10.1097/00000542-200301000-00042.
Manji RA, Grocott HP, Leake J, et al. Seizures following cardiac surgery: the impact of tranexamic acid and other risk factors. Can J Anesth Can Anesth. 2012;59(1):6–13. https://doi.org/10.1007/s12630-011-9618-z.
Martin K, Knorr J, Breuer T, et al. Seizures After Open Heart Surgery: Comparison of ε-Aminocaproic Acid and Tranexamic Acid. J Cardiothorac Vasc Anesth. 2011;25(1):20–5. https://doi.org/10.1053/j.jvca.2010.10.007.
Maeda T, Sasabuchi Y, Matsui H, Ohnishi Y, Miyata S, Yasunaga H. Safety of Tranexamic Acid in Pediatric Cardiac Surgery: A Nationwide Database Study. J Cardiothorac Vasc Anesth. 2017;31(2):549–53. https://doi.org/10.1053/j.jvca.2016.10.001.
Lecker I, Wang D, Whissell PD, Avramescu S, Mazer CD, Orser BA. Tranexamic acid–associated seizures: Causes and treatment. Ann Neurol. 2016;79(1):18–26. https://doi.org/10.1002/ana.24558.
Deyo R. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol. 1992;45(6):613–9. https://doi.org/10.1016/0895-4356(92)90133-8.
Neilipovitz DT, Murto K, Hall L, Barrowman NJ, Splinter WM. A randomized trial of tranexamic acid to reduce blood transfusion for scoliosis surgery. Anesth Analg. 2001;93(1):82–7. https://doi.org/10.1097/00000539-200107000-00018.
Grant JA, Howard J, Luntley J, Harder J, Aleissa S, Parsons D. Perioperative blood transfusion requirements in pediatric scoliosis surgery: the efficacy of tranexamic acid. J Pediatr Orthop. 2009;29(3):300–4. https://doi.org/10.1097/BPO.0b013e31819a85de.
Ng BKW, Chau W, Hung ALH, Hui AC, Lam TP, Cheng JCY. Use of Tranexamic Acid (TXA) on reducing blood loss during scoliosis surgery in Chinese adolescents. Scoliosis. 2015;10(1):28. https://doi.org/10.1186/s13013-015-0052-9.
Johnson DJ, Johnson CC, Goobie SM, et al. High-dose Versus Low-dose Tranexamic Acid to Reduce Transfusion Requirements in Pediatric Scoliosis Surgery. J Pediatr Orthop. 2017;37(8):e552–7. https://doi.org/10.1097/BPO.0000000000000820.
Jones KE, Butler EK, Barrack T, et al. Tranexamic Acid Reduced the Percent of Total Blood Volume Lost During Adolescent Idiopathic Scoliosis Surgery. Int J Spine Surg. 2017;11(4):27. https://doi.org/10.14444/4027.
Ohashi N, Ohashi M, Endo N, Kohno T. Administration of tranexamic acid to patients undergoing surgery for adolescent idiopathic scoliosis evokes pain and increases the infusion rate of remifentanil during the surgery. Sumitani M, ed. PLOS ONE. 2017;12(3):e0173622. doi:https://doi.org/10.1371/journal.pone.0173622
Yang B, Li H, Wang D, He X, Zhang C, Yang P. Systematic Review and Meta-Analysis of Perioperative Intravenous Tranexamic Acid Use in Spinal Surgery. Landoni G, ed. PLoS ONE. 2013;8(2):e55436. doi:https://doi.org/10.1371/journal.pone.0055436
Soroceanu A, Oren JH, Smith JS, et al. Effect of Antifibrinolytic Therapy on Complications, Thromboembolic Events, Blood Product Utilization, and Fusion in Adult Spinal Deformity Surgery. Spine. 2016;41(14):E879–86. https://doi.org/10.1097/BRS.0000000000001454.
Lei T, Bingtao W, Zhaoqing G, Zhongqiang C, Xin L. The efficacy and safety of intravenous tranexamic acid in patients with posterior operation of multilevel thoracic spine stenosis: a prospective randomized controlled trial. BMC Musculoskelet Disord. 2022;23(1):410. https://doi.org/10.1186/s12891-022-05361-2.
Ko BS, Cho KJ, Kim YT, Park JW, Kim NC. Does Tranexamic Acid Increase the Incidence of Thromboembolism After Spinal Fusion Surgery? Clin Spine Surg Spine Publ. 2020;33(2):E71–5. https://doi.org/10.1097/BSD.0000000000000860.
Cornelius B, Cummings Q, Assercq M, Rizzo E, Gennuso S, Cornelius A. Current Practices in Tranexamic Acid Administration for Pediatric Trauma Patients in the United States. J Trauma Nurs. 2021;28(1):21–5. https://doi.org/10.1097/JTN.0000000000000553.
Eckert MJ, Wertin TM, Tyner SD, Nelson DW, Izenberg S, Martin MJ. Tranexamic acid administration to pediatric trauma patients in a combat setting: The pediatric trauma and tranexamic acid study (PED-TRAX). J Trauma Acute Care Surg. 2014;77(6):852–8. https://doi.org/10.1097/TA.0000000000000443.
Roberts I, Shakur H, Coats T, et al. The CRASH-2 trial: a randomised controlled trial and economic evaluation of the effects of tranexamic acid on death, vascular occlusive events and transfusion requirement in bleeding trauma patients. Health Technol Assess. 2013;17(10). doi:https://doi.org/10.3310/hta17100
Acknowledgements
Not applicable.
Funding
Ms. Ivasyk was supported by a Medical Scientist Training Program grant from the National Institute of General Medical Sciences of the National Institutes of Health under award number T32GM007739 to the Weill Cornell/Rockefeller/Sloan-Kettering Tri-Institutional MD- PhD Program.
Author information
Authors and Affiliations
Contributions
Iryna Ivasyk, BS (Contribution: Analyzed and interpreted results, drafted the manuscript, approved the final draft to be submitted for publication, agreed to be accountable for all aspects of the work), Abhinaba Chatterjee BS (Contribution: substantial contributions to study design, analyzed and interpreted results, critically revised the manuscript for statistical accuracy/statistical analysis, approved of the final draft to be submitted for publication, agreed to be accountable for all aspects of the work), Catherine Jordan BS (Contribution: analyzed and interpreted results in the context of existing literature, assisted in drafting the manuscript, edited the manuscript, approved of the final draft to be submitted for publication, agreed to be accountable for all aspects of the work), Matthew T. Geiselmann, BS (Contribution: substantial contribution to data acquisition, edited the manuscript, approved of the final draft to be submitted for publication, agreed to be accountable for all aspects of the work), Peter S. Chang, MD (Contribution: analyzed and interpreted results, critically edited the manuscript, approved of the final draft to be submitted for publication, agreed to be accountable for all aspects of the work), Hooman Kamel, MD (Contribution: provided feedback on study design, critically revised the interpretation of data for the work, edited the manuscript, approved of the final draft to be submitted for publication, agreed to be accountable for all aspects of the work), Sariah Khormaee, MD PhD (Contribution: conceived and designed the study, data acquisition from the database, analyzed and interpreted results, drafted the manuscript, edited the manuscript, approved of the final draft to be submitted for publication, agreed to be accountable for all aspects of the work).
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was conducted and reported in accordance with the Declaration of Helsinki. The institutional review board and ethical committee at Weill Cornell Medicine gave approval to conduct this study with a waiver of informed consent due to the deidentified nature of the data source.
Consent for publication
Not applicable.
Competing interests
Ms. Ivasyk has no disclosures, Mr. Chatterjee has no disclosures, Ms. Jordan has no disclosures, Mr. Geiselmann has no disclosures, Dr. Chang has no disclosures, Dr. Kamel serves as a PI for the NIH-funded ARCADIA trial (NINDS U01NS095869) which receives in-kind study drug from the BMS-Pfizer Alliance for Eliquis® and ancillary study support from Roche Diagnostics, serves as Deputy Editor for JAMA Neurology, serves as a steering committee member of Medtronic’s Stroke AF trial (uncompensated), and serves on an endpoint adjudication committee for a trial of empagliflozin for Boehringer-Ingelheim, Dr. Khormaee has no disclosures.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Ivasyk, I., Chatterjee, A., Jordan, C. et al. Evaluation of the safety of tranexamic acid use in pediatric patients undergoing spinal fusion surgery: a retrospective comparative cohort study. BMC Musculoskelet Disord 23, 651 (2022). https://doi.org/10.1186/s12891-022-05604-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-022-05604-2