
Abstract
Background
Studies reported that there is a relationship between volumetric bone mineral density (vBMD) and hemoglobin (HGB) in sickle cell anemia, chronic obstructive pulmonary disease, inflammatory bowel disease, and chronic kidney disease, it is not clear whether this association exists in normal populations or different genders. In order to further clarify the relationship between vBMD and HGB, and provide the basis for the diagnosis of related diseases, this study was conducted in the physical examination population.
Methods
A cross-sectional study was conducted on a health check-up population from Wannan area of China from January to December 2018. The study involved 1238 individuals aged 23 to 85 years. Linear regression analysis and smooth curve were applied to determine the relationship of HGB and vBMD.
Results
The average level of vBMD in the population was 130.11 ± 79.51 mg/cm3, after adjusting for age, body mass index (BMI), systolic blood pressure (SBP), diastolic blood pressure (DBP), total cholesterol (TC), triglycerides (TG), glucose (GLU), high-density lipoprotein (HDL) and low-density lipoprotein (LDL). A U-shape relationship was established between vBMD and HGB, the cut off value of HGB was 130 g/L. After gender stratification, the results showed a U-shaped curve relationship between vBMD and HGB in male group, and a linear relationship between vBMD and HGB in female group. The vBMD decreased with HGB when HGB < 120 g/L, and increased when HGB ≥ 120 g/L in male group.
Conclusion
The relationship between vBMD and HGB in the male physical examination population presents a U-shaped curve.
Similar content being viewed by others

Background
Osteoporosis (OP) is a systemic bone metabolic disease characterized by decreased bone mass, increased bone fragility, and susceptibility to fractures [1]. There are approximately 200 million osteoporotic patients worldwide, and about 8.9 million fractures occur every year globally [2,3,4]. Previous studies have identified the basic metabolic conditions and risk factors associated with osteoporosis, these factors include age, weight, dyslipidemia and hypertension [5] and so on. The most common diagnostic criterion for OP is bone mineral density (BMD) [2]. The strategies of treating osteoporosis are exercise and pharmacological treatments which involves drugs such as risedronate [6], alendronate [7], estrogens [8, 9], SERMs [10,11,12] and bisphosphonates [13,14,15,16]. However, there is no treatment method that is fast and effective enough to deal with OP [17, 18]. Thus, OP is still a major public health problem [19].
Studies have reported a positive correlation between BMD and hemoglobin (HGB) levels in patients with sickle cell anemia, chronic obstructive pulmonary disease, inflammatory bowel disease, and chronic kidney disease [20,21,22,23], while some other studies found that there was no significant correlation between BMD and HGB [24,25,26]. These two indicators correspond to the diagnosis of different systemic diseases, in addition to focusing on the correlation between them, other aspects of the research are limited. Whether there is a nonlinear relationship between them or does this correlation exist in normal people is not clear. Therefore, further clarify the relationship between them is still very necessary. This cross-sectional study is to investigate the relationship between volumetric bone mineral density (vBMD) and HGB in a relatively wide age range health check-up population.
Materials and methods
Study subjects
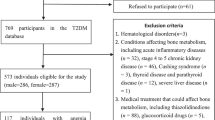
A cross-sectional study was conducted on 1238 health check-up participants aged 23 to 85 years in the Health Management Center at the First Affiliated Hospital of Wannan Medical College in Wuhu, China from January to December 2018. All protocols are carried out in accordance with relevant guidelines and regulations. Ethical approval was received from the Medical Ethics Committee of Wannan Medical College. Since the participants in this study are the people who came to the hospital for routine physical examinations, the Medical Ethics Committee of Wannan Medical College approved that the study only needs to obtain the participant’s verbal informed consent. Therefore, this study did not have the participants’ written informed consent. Before the survey, each participant provided verbal informed consent. In addition, data related to private information were deleted during analysis of the results. The participants were: (1) subjects within the age range of 20—90 years, and (2) subjects with available data on age, sex, HGB, SBP, DBP, TG, TC, GLU, low-density lipoprotein (LDL), high-density lipoprotein (HDL), and vBMD. All subjects completed physical examination and blood biochemical examination. The following categories of subjects were excluded from the study: (1) subjects with incomplete clinical data, duplicated cases, and missing data; (2) subjects who received drug interventions, and (3) patients who had cancer, severe cardiovascular disease or severe infections. The study involved a total of 1238 participants made up of 525 females (42.41%) and 713 males (57.59%). The mean ages of the female and male participants were 53.07 ± 12.94 and 52.38 ± 12.86 years, respectively.
Study questionnaire
A questionnaire was used to collect information with respect to demographic and behavioral characteristics, disease history and surgical history [27]. The demographic characteristics included age, sex, occupation and educational background, while the behavioral characteristics included smoking and drinking. The other information obtained were disease history, surgical history and history of severe infections.
Physical examination
Trained professionals measured height, weight, blood pressure and other variables using standard methods, based on the guidelines of World Health Organization (WHO) and International Society of Hypertension [28]. Height measurement required subjects to stand barefooted on the floor of the height meter, with their trunks naturally straight, heads straight, with eyes focused in front, upper limbs drooping naturally, and legs straight. The recorded data on height were accurate to 0.1 cm. Body weight measurement required barefooted subjects to wear shorts and stand naturally in the center of the weight pedal so as to keep their bodies stable. The recorded data were accurate to 0.1 kg. The BMI was calculated by dividing body weight (kg) with the square of the height (m) i.e., m2, to an accuracy of 0.01 kg/m2. Systolic blood pressure (SBP) and diastolic blood pressure (DBP) was measured with a mercury sphygmomanometer. The subjects were advised to sit still for 5 min before the BP measurement.
Blood parameters
Fasting venous blood (5 mL) was collected from each subject in the morning, and all samples were analyzed within 24 h. The indicators included TG, TC, GLU, LDL and HDL were measured using the Hitachi 7600 automatic biochemical analyzer.
Bone mineral density examination
The lumbar spine was scanned with quantitative CT (QCT) method [29]. The subject lay supine on a CT scanning bed, and a standard phantom and blue cushion was placed under the lumbar spine parallel to the body. The blue soft cushion was placed close to the lumbar spine without any gap during the period. The value of vBMD was defined as the mean value of vBMD of the lumbar spine from L1 to L4.
Statistical analyses
Statistical analyses were performed using SPSS 18.0 software and R-project 2.41. The continuous variables are all normal distribution and presented as mean ± standard deviation. Student’s t-test was used to compare the differences of demographics characteristic, and indicators of physical examination and blood biochemical examination between men and women. The relationship between vBMD and HGB was tested using generalized smoothing splines, and the knot locations was generated automatically in generalized additive models with R package MGCV [30]. Adjusted factors were age, BMI, GLU, TC, TG, SBP, DBP, HDL and LDL. According to the knot locations of HGB, the relationship between HGB and vBMD in different HGB segments was further analyzed with linear regression model, and adjusted age, BMI, GLU, TC, TG, SBP, DBP, HDL and LDL. On this basis, gender was stratified, and the relationship between HGB and vBMD was analyzed with generalized smoothing splines, then the linear regression was conducted to analyze the relationship between HGB and vBMD in different HGB segments according to the knot locations in different genders, and adjusted age, BMI, GLU, TC, TG, SBP, DBP, HDL and LDL. All p values were two-tailed, with a significance level of 0.05.
Results
General characteristics of male and female participants
Table 1 shows that HGB, BMI, SBP, DBP, TC, TG, GLU, HDL and LDL differed significantly between the male and female groups (p < 0.05).
Relationship between vBMD and HGB
Figure 1 shows a U-shaped curve relationship between vBMD and HGB, the cut off value of HGB was 130 g/L. vBMD decreased with HGB when HGB < 130 g/L, and increased when HGB ≥ 130 g/L, before and after adjustment for gender, age, BMI, TC, TG, SBP, DBP, GLU, HDL and LDL. These results are presented on Table 2.

Generalized smoothing splines for vBMD and HGB. Horizontal coordinates represent different components, while vertical coordinates represent residuals of vBMD. Solid line: no adjustment; dashed line: adjusted for gander, age, BMI, TC, TG, SBP, DBP, GLU, HDL and LDL. Shaded area shows the 95% confidence interval
Relationship between vBMD and HGB in different genders
Figure 2 shows that through gender stratification and before and after adjustment for age, BMI, TC, TG, SBP, DBP, GLU, HDL and LDL, a U-shaped curve relationship was established between vBMD and HGB in male group, vBMD decreased with HGB when HGB < 120 g/L, and increased when HBG ≥ 120 g/L; while a negative linear relationship between vBMD and HGB in female group. These data are shown on Table 3.

Generalized smoothing splines for vBMD and HGB in male group (A) and female group (B). Horizontal coordinates represent different components, while vertical coordinates represent residuals of vBMD. Solid line: no adjustment; dashed line: adjusted for age, BMI, TC, TG, SBP, DBP, GLU, HDL and LDL. Shaded area shows the 95% confidence interval
Discussion
A statistical survey has shown that the prevalence of osteoporotic fractures in women over 50 years old in China was 15%, with the prevalence of osteoporosis being significantly high among people over 60 years old, especially among female patients [29, 31, 32]. In recent years, epidemiological and clinical studies have found that HGB levels are associated with osteoporosis [33, 34]. It suggested that low oxygen environment may affect bone metabolism, while anemia may cause bone loss, reduce vBMD, and lead to osteoporosis [23].
The results of this study are not consistent with other studies. In this study, after adjusting the age and others factors, the relationship between vBMD and HGB in male population is presented a U-shaped curve, when HGB < 120 g/L, the vBMD decreases with HGB increasing, while when HGB ≥ 120 g/L, the vBMD increases with HGB increasing. The possible reason is that higher HGB level means that the body has a strong ability to provide oxygen feedback, indicating that the exercise amount of these people in daily life is higher, and the exercise is positively related to bone density. In clinical, low level of HGB is an important index of iron deficiency anemia when HGB was lower than 120 g/L [34]. There is a mechanism to promote bone formation in clinic, that is, iron deficiency anemia caused by blood loss can promote the proliferation of bone cells [35]. This negative feedback regulation may cause a negative correlation between vBMD and HGB at low HGB level (HGB < 120 g/L). Meanwhile, the HGB level is closely related to the content of red blood cells, and the production of red blood cells depends on the content of red marrow, with the increase of age, red marrow gradually changes to yellow marrow, and the decrease of red marrow leads to the decrease of RBC productivity, which finally results in the decrease of HGB. At the same time, with the increase of age, bone density level will also decrease [35]. Consistent with the results of this study is that Kri and Kim showed the positive correlation between vBMD and HGB in male population [24, 25]. And, different from the linear regression analysis method used in other studies, the smooth curve used in this study can further explore the quantitative relationship between vBMD and HGB. Furthe more, the subjects in these studies was only for the elderly (age > 50), and this study included a wider age group (age 20–85), so it can better show the role of age in the relationship between them. To further assess whether the age inclusion criteria are the reason why our results differ from other studies, we conducted age stratification analysis (supplementary Fig. 1–2 and supplementary Table 1–2), the results showed that the relationship between vBMD and HGB in the two age groups in male group was still a U-curve, but the decrease of HGB < 120 g/L was relatively slow in the participants under 50 years old.
In female participants, there was no significant association of vBMD and HGB after adjusted age and other factors. It indicated that the factors corrected by this study have a great influence on the relationship between BMD and HGB. The cause maybe related to the promotion of periodic menstrual loss on osteoblast proliferation in young women. Due to this regulation, vBMD in female is maintained at a relatively stable level in young age, and it does not begin to decrease until the elderly menopause [36, 37], which suggests that age has a greater impact on vBMD for women than HGB. Similar to this study, Yun’s study also found a negative correlation between vBMD and HGB without age and other factors adjustment in female population [33].
It is worth noting that most previous studies used dualenergy X-ray absorptiometry (DXA) method to measure BMD, which can not distinguish cancellous bone from cortical bone. In fact, the area and conversion rate of cancellous bone are much higher than cortical bone [38]. In addition, in the measurement of lumbar indicators, the measured value may be higher than the actual value due to bone hyperplasia, intervertebral disc degeneration, ligament ossification and abdominal aorta calcification, which may cause misdiagnosis and missed diagnosis [39]. In contrast, the QCT method used in this study will not be interfered by factors such as bone hyperplasia, so it has a high accuracy.
In conclusion, this further suggests that gender should not be ignored when hemoglobin is used as an early warning indicator of BMD related diseases.
Limitations of the study
There are some limitations in this study. Firstly, causal links in this study cannot be accounted by the cross-sectional study. Secondly, some important factors affecting BMD in this study were not investigated, such as menopausal or menopausal age, vitamin D intake and so on, which restricted the scientificity of the results. Thirdly, the study population is physical examination population, and its characteristics are different from the community population, so the representativeness of the research results is limited.
Conclusions
The relationship between vBMD and HGB in male population presents a U-shaped curve. and a linear relationship in female population. At present, vBMD is an important indicator of bone strength, and it is also an important diagnostic criterion for osteoporosis. In the absence of effective treatment, active prevention of osteoporosis is very important. It is of great significance to identify some indicators for evaluating the progress of osteoporosis, and for guiding its treatment. In the future, the scope of the study will be expanded, and a multi-center research will be carried out. Further studies are required to confirm these findings and determine the potential mechanisms underlying the observed associations.
Availability of data and materials
The data of participants are collected by the authors and uploaded to the database, which makes it easier for the authors to use the data in the process of analyzing data and writing manuscripts. This kind of database system can conveniently shield the data irrelevant to the experiment and effectively protect the privacy of participants. The data that support the findings of this study are available from the Health Management Center at the First Affiliated Hospital of Wannan Medical College in Wuhu, China but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of Health Management Center at the First Affiliated Hospital of Wannan Medical College in Wuhu, China. If someone wants to request the data from this study, they can contact Yufeng Wen (corresponding author).
Abbreviations
- OP:
-
Osteoporosis
- BMD:
-
Bone mineral density
- vBMD:
-
Volumetric bone mineral density
- HGB:
-
Hemoglobin
- BMI:
-
Body mass index
- SBP:
-
Systolic blood pressure
- DBP:
-
Diastolic blood pressure
- TC:
-
Total cholesterol
- TG:
-
Triglycerides
- GLU:
-
Glucose
- HDL:
-
High-density lipoprotein
- LDL:
-
Low-density lipoprotein
- WHO:
-
World Health Organization
- BP:
-
Blood pressure
- QCT:
-
Quantitative CT
References
Miller PD. Management of severe osteoporosis. Expert Opin Pharmacother. 2016;17(4):473–88. https://doi.org/10.1517/14656566.2016.1124856.
Lupsa BC, Insogna K. Bone Health and Osteoporosis. Endocrinol Metab Clin North Am. 2015;44(3):517–30. https://doi.org/10.1016/j.ecl.2015.05.002.
Johnell O, Kanis JA. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Int. 2006;17(12):1726–33. https://doi.org/10.1007/s00198-006-0172-4.
Jang EJ,Lee YK,Choi HJ,et al. Osteoporotic Fracture Risk Assessment Using Bone Mineral Density in Korean: A Community-based Cohort Study. J Bone Metab,2016,23 (1):34–39. https://doi.org/10.11005/jbm.2016.23.1.34.
Espallargues M, Sampietro-Colom L, Estrada MD, et al. Identifying bone-mass-related risk factors for fracture to guide bone densitometry measurements: a systematic review of the literature. Osteoporos Int. 2001;12(10):811–22. https://doi.org/10.1007/s001980170031.
Fogelman I,Ribot C,Smith R,et al. Risedronate reverses bone loss in postmenopausal women with low bone mass: results from a multinational, double-blind, placebo-controlled trial. BMD-MN Study Group. J Clin Endocrinol Metab. 2000,85 (5):1895–1900. https://doi.org/10.1210/jcem.85.5.6603.
Liberman UA,Weiss SR,Bröll J,et al. Effect of oral alendronate on bone mineral density and the incidence of fractures in postmenopausal osteoporosis. The Alendronate Phase III Osteoporosis Treatment Study Group. N Engl J Med. 1995,333 (22):1437–1443. https://doi.org/10.1056/NEJM199511303332201.
Khosla S, Amin S, Orwoll E. Osteoporosis in men. Endocr Rev. 2008;29(4):441–64. https://doi.org/10.1210/er.2008-0002.
Rossouw JE, Anderson GL, Prentice RL, et al. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results From the Women’s Health Initiative randomized controlled trial. JAMA. 2002;288(3):321–33. https://doi.org/10.1001/jama.288.3.321.
Chesnut CH 3rd, Silverman S, Andriano K, et al. A randomized trial of nasal spray salmon calcitonin in postmenopausal women with established osteoporosis: the prevent recurrence of osteoporotic fractures study. PROOF Study Group Am J Med. 2000;109(4):267–76. https://doi.org/10.1016/s0002-9343(00)00490-3.
Riggs BL, Hartmann LC. Selective estrogen-receptor modulators – mechanisms of action and application to clinical practice. N Engl J Med. 2003;348(7):618–29. https://doi.org/10.1056/NEJMra022219.
Vogel VG, Costantino JP, Wickerham DL, et al. Effects of tamoxifen vs raloxifene on the risk of developing invasive breast cancer and other disease outcomes: the NSABP Study of Tamoxifen and Raloxifene (STAR) P-2 trial. JAMA. 2006;295(23):2727–41. https://doi.org/10.1001/jama.295.23.joc60074.
Vahle JL, Long GG, Sandusky G, et al. Bone neoplasms in F344 rats given teriparatide [rhPTH(1–34)] are dependent on duration of treatment and dose. Toxicol Pathol. 2004;32(4):426–38. https://doi.org/10.1080/01926230490462138.
Khosla S, Hofbauer LC. Osteoporosis treatment: recent developments and ongoing challenges. Lancet Diabetes Endocrinol. 2017;5(11):898–907. https://doi.org/10.1016/S2213-8587(17)30188-2.
Lacey DL, Boyle WJ, Simonet WS, et al. Bench to bedside: elucidation of the OPG-RANK-RANKL pathway and the development of denosumab. Nat Rev Drug Discov. 2012;11(5):401–19. https://doi.org/10.1038/nrd3705.
Meunier PJ, Roux C, Seeman E, et al. The effects of strontium ranelate on the risk of vertebral fracture in women with postmenopausal osteoporosis. N Engl J Med. 2004;350(5):459–68. https://doi.org/10.1056/NEJMoa022436.
Thacker HL,Richmond B. In rebuttal: Osteopenia is a useful diagnosis. Cleve Clin J Med. 2006,73 (1):34–35, 38. https://doi.org/10.3949/ccjm.73.1.34.
Karaguzel G, Holick MF. Diagnosis and treatment of osteopenia. Rev Endocr Metab Disord. 2010;11(4):237–51. https://doi.org/10.1007/s11154-010-9154-0.
Srivastava M, Deal C. Osteoporosis in elderly: prevention and treatment. Clin Geriatr Med. 2002;18(3):529–55. https://doi.org/10.1016/s0749-0690(02)00022-8.
Fujimoto H, Fujimoto K, Ueda A, et al. Hypoxemia is a risk factor for bone mass loss. J Bone Miner Metab. 1999;17(3):211–6. https://doi.org/10.1007/s007740050087.
Karadag F, Cildag O, Yurekli Y, et al. Should COPD patients be routinely evaluated for bone mineral density? J Bone Miner Metab. 2003;21(4):242–6. https://doi.org/10.1007/s00774-002-0416-0.
Laudisio A, Marzetti E, Antonica L, et al. Association of left ventricular function with bone mineral density in older women: a population-based study. Calcif Tissue Int. 2008;82(1):27–33. https://doi.org/10.1007/s00223-007-9094-1.
Rutten EP, Franssen FM, Spruit MA, et al. Anemia is associated with bone mineral density in chronic obstructive pulmonary disease. COPD. 2013;10(3):286–92. https://doi.org/10.3109/15412555.2012.744390.
Kim HS, Park HM, Lee HS, et al. Hemoglobin levels and low bone mineral density in non-anemic older adults: Secondary analysis of the Korean National Health and Nutrition Examination Survey. Exp Gerontol. 2019;126: 110706. https://doi.org/10.1016/j.exger.2019.110706.
Kristjansdottir HL, Mellström D, Johansson P, et al. High platelet count is associated with low bone mineral density: The MrOS Sweden cohort. Osteoporos Int. 2021;32(5):865–71. https://doi.org/10.1007/s00198-020-05766-6.
Valderrábano RJ, Buzkova P, Chang PY, et al. Association of bone mineral density with hemoglobin and change in hemoglobin among older men and women: The Cardiovascular Health Study. Bone. 2019;120:321–6. https://doi.org/10.1016/j.bone.2018.11.010.
Jiang M, Zha X, Wu Z, et al. Inverted U-shaped curve relationship between red blood cell distribution width and hypertension in a large health checkup population in China [J]. J Am Soc Hypertens. 2018;12(5):327–34. https://doi.org/10.1016/j.jash.2018.03.003.
Chalmers J, MacMahon S, Mancia G, et al. 1999 world health Organization-International Society of hypertension guidelines for the management of hypertension. Guidelines sub-committee of the world health Organization. Clin Exp Hypertension (New York, NY: 1993) 1999;21(5–6):1009–1060. https://doi.org/10.3109/10641969909061028.
Li X, Li X, Li J, et al. The accuracy of bone mineral density measurement using dual-energy spectral CT and quantitative CT: a comparative phantom study. Clin Radiol. 2020;75(4):320.e9-320.e15. https://doi.org/10.1016/j.crad.2020.05.026.
Musio M, Sauleau EA, Augustin NH. Resources allocation in healthcare for cancer: a case study using generalised additive mixed models. Geospat Health. 2012;7(1):83–9. https://doi.org/10.4081/gh.2012.107.
Li N, Ou P, Zhu H, et al. Prevalence rate of osteoporosis in the mid - aged and elderly in selected parts of China. Chin Med J (Engl). 2002;115(5):773–5.
Bellver M, Del Rio L, Jovell E, et al. Bone mineral density and bone mineral content among female elite athletes. Bone. 2019;12:393–400. https://doi.org/10.1016/j.bone.2019.06.030.
Yun HO,Ji HM,Cho B. Association between Hemoglobin Level and Bone Mineral Density in Korean Adults. J Bone Metab. 2017,24 (3):161–173. https://doi.org/10.11005/jbm.2017.24.3.161.
McLean E, Cogswell M, Egli I, et al. Worldwide prevalence of anaemia, WHO Vitamin and Mineral Nutrition Information System, 1993–2005. Public Health Nutr. 2009;12:444–54. https://doi.org/10.1017/S1368980008002401.
Gurevitch O, Slavin S, Feldman AG. Conversion of red bone marrow into yellow - cause and mechanisms. Med Hypotheses. 2007;69:531–6. https://doi.org/10.1016/j.mehy.2007.01.052.
Diana M, Axel H, Kristina GD. A Review of Clinical Guidelines on the Management of Iron Deficiency and Iron-Deficiency Anemia in Women with Heavy Menstrual Bleeding. Adv Ther. 2021;38:201–25. https://doi.org/10.1007/s12325-020-01564-y.
Walkley CR. Erythropoiesis, anemia and the bone marrow microenvironment. Int J Hematol. 2011;93:10–3. https://doi.org/10.1007/s12185-010-0759-6.
Riggs BL, Melton LJ, Robb RA, et al. A population-based assess- ment of rates of bone loss at multiple skeletal sites:evidencefor sub- stantial trabecular bone loss in young adult women and men. J Bone Miner Res. 2008;23:205–41. https://doi.org/10.1359/jbmr.071020.
Christian G, Fernando M, Helmut P, et al. High resolution quantitative computed tomography-based assessment of trabecular microstructure and strength estimates by finite-element analysis of the spine, but not DXA, reflects vertebral fracture status in men with glucocorticoid-induced osteoporosis. Bone. 2013;52:568–77. https://doi.org/10.1016/j.bone.2012.10.036.
Acknowledgements
First of all, the authors would like to thank all the staff from the First Affiliated Hospital of Wannan Medical College who were involved in this work. Secondly, the authors would like to thank the study participants for their cooperation.
Funding
This work was supported by the Teaching Reform and Quality Improvement Plan of the Department of Education of Anhui Province-Teaching Teacher (grant number 2019jxms066); The Teaching Reform and Quality Improvement Plan of the Department of Education of Anhui Province-Teaching Team (grant number 2018jxtd153).
Author information
Authors and Affiliations
Contributions
YF Wen designed the research. YM Zhou, SJ Liu participated in data collection and analysis and drafted the manuscript. XM Wang, YH Fu, F Su, L Cao, XJ Zha helped analyze data and manuscript development. YF Wen provided research funding and software support. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All protocols are carried out in accordance with relevant guidelines and regulations. Ethical approval was received from the Medical Ethics Committee of Wannan Medical College. This study was based on data from Health Management Center at the First Affiliated Hospital of Wannan Medical College in Wuhu, China. Since the participants in this study are people who came to the hospital for routine physical examinations, the Medical Ethics Committee of Wannan Medical College approved that the study only needs to obtain the participant’s verbal informed consent. Therefore, this study did not have the participants’ written informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Supplementary table 1:
Association between vBMD and HGB by linear regression model in male group. Supplementary table 2: Association between vBMD and HGB by linear regression model in female group. Supplementary figure 1: Generalized smoothing splines for vBMD and HGB in male group, 20-50 years (A), 50-90 years (B). Horizontal coordinates represent different components, while vertical coordinates represent residuals of vBMD. Solid line: no adjustment; dashed line: adjusted for age, BMI, TC, TG, SBP, DBP, GLU, HDL and LDL. Shaded area shows the 95% confidence interval. Supplementary figure 2: Generalized smoothing splines for vBMD and HGB in female group, 20-50 years (A), 50-90 years (B). Horizontal coordinates represent different components, while vertical coordinates represent residuals of vBMD. Solid line: no adjustment; dashed line: adjusted for age, BMI, TC, TG, SBP, DBP, GLU, HDL and LDL. Shaded area shows the 95% confidence interval.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhou, Y., Liu, S., Wang, X. et al. Implications of gender-based variabilities in bone mineral density and hemoglobin levels. BMC Musculoskelet Disord 22, 645 (2021). https://doi.org/10.1186/s12891-021-04536-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-021-04536-7