
Abstract
Background
The 6-min walk test (6MWT) and incremental shuttle walk test (ISWT) are valid and reliable measures to assess exercise capacity of patients with chronic obstructive pulmonary disease (COPD). However, the comparison of correlation between peak oxygen uptake (peak VO2) and 6MWT or ISWT distance has not been investigated. We aimed to investigate the correlation between peak VO2 and 6MWT and ISWT distances in COPD patients through a meta-analysis.
Methods
We systematically searched MEDLINE, Scopus, Embase, and the Cochrane Library up to June, 2020 for studies comparing the correlation of peak VO2 with either 6MWT or ISWT in COPD patients. Meta-analysis was performed with R software using a fixed-effect model. We compared the correlation coefficient and measured the heterogeneity using I2 statistics.
Results
We identified 12 studies involving 746 patients. Meta-analysis showed a significant correlation between peak VO2 and 6MWT and ISWT distances (6MWT: r = 0.65, 95% CI 0.61–0.70; ISWT: r = 0.81, 95% CI 0.74–0.85; p < 0.0001). The heterogeneity was lower in ISWT than in 6MWT (6MWT: I2 = 56%, p = 0.02; ISWT: I2 = 0%, p = 0.71). Subgroup analysis showed a higher correlation coefficient in the low exercise capacity group than in the high exercise capacity group in both field tests.
Conclusions
6MWT and ISWT significantly correlated with peak VO2. Our findings suggest that ISWT has a stronger correlation with peak VO2 than 6MWT. The exercise capacity in COPD patients may affect the strength of the relationship between peak VO2 and walking distance in both field tests, suggesting the importance of using various exercise tests.
Trial registration CRD 42020200139 at crd.york.ac.uk/prospero/
Similar content being viewed by others

Background
Chronic obstructive pulmonary disease (COPD) is characterized by airflow limitation that is not fully reversible and often progressive. The airflow limitation is associated with an inflammatory response of the lungs, mainly caused by smoking. Cough, sputum, and dyspnea (upon exertion or at rest) are chronic manifestation of COPD as the disease progresses. Exercise limitation is also a prominent complaint in patients with COPD [1]. Therefore, to assess the functional capacity of patients with chronic airway obstruction, cardiopulmonary exercise testing (CPET) and field tests have been used. CPET provides a global assessment of the integrative exercise response involving the pulmonary, cardiovascular, hematopoietic, neuropsychologic, and skeletal muscle systems; thus, it has been regarded as a gold standard test to assess exercise capacity and response to therapeutic interventions in patients with COPD [2]. However, CPET requires the use of costly exercise equipment, trained technicians, and specialists to interpret the results. Furthermore, some COPD patients with severe dyspnea are unable to undergo tests with equipment measuring expired gas, such as a mouthpiece. Field tests are practical and simple; they do not require complex equipment that can hardly be tolerated or have difficult interpretation. In this regard, field tests, such as the 6-min walk test (6MWT) and the incremental shuttle walk test (ISWT), and CPET are complementary. They play a key role in evaluating functional exercise capacity, assessing prognosis, and evaluating response to treatment [3, 4].
Walking distance during these field tests has been used to indicate the level of disability and cardiopulmonary capacity [5]. Peak oxygen uptake (peak VO2) is also regarded as an index of cardiopulmonary capacity, and air analysis during a maximal laboratory exercise test is the most precise method of measuring peak VO2 [6]. Previous studies showed a strong correlation between the distance of a field test and peak VO2 measured using CPET [7, 8].
6MWT is a practical and simple test that requires a patient to walk at the highest speed tolerated for 6 min. Therefore, 6MWT depends on individually adjusted characteristics, which are determined by patients who are even allowed to stop walking if they wish to [4]. By contrast, ISWT offers a different protocol from the 6MWT, which is incremental and externally paced. It is a 12-level test (1 min at each level) that imposes incremental acceleration through an auditory signal used to control the pace on a 10-m shuttle circuit delineated by two traffic cones. ISWT is also simple, has good reproducibility, and requires no specific ergometers [3, 9]. However, it has not been as widely accepted as 6MWT in clinical practice. We hypothesized that the ISWT would better assess the exercise capacity, and pondered whether the ISWT would better correlate with peak VO2 in the CPET than would the 6MWT in COPD patients. To our knowledge, no study has compared the correlation between peak VO2 and 6MWT or ISWT distance. Therefore, in this study, we aimed to investigate the correlation between peak VO2 and 6MWT and ISWT distances in patients with COPD through a meta-analysis and compared the correlation coefficient for assessing the validity of the 6MWT and ISWT to predict peak VO2.
Methods
Protocol and registration
This meta-analysis was reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [10]. The present study was registered in the PROSPERO international prospective register of systematic reviews (CRD 42020200139) and approved by the Institutional Review Board of Ulsan University Hospital (NON2020-001).
Search strategy and selection criteria
We systematically searched relevant studies published up to June 30, 2020 in MEDLINE, Scopus, Embase, and the Cochrane Library databases. The keywords were chosen by two physicians (GC and DP) and reviewed by keywords from other reviews and articles on similar topics. The following keywords were used to search the database: ‘incremental shuttle walk test’, ‘6 min walk test’, ‘cardiopulmonary exercise testing’, and ‘chronic obstructive pulmonary disease’. Citations of published relevant systematic reviews and meta-analyses were examined to identify further pertinent studies, if any [7, 8]. Two articles published in Japan (written in Japanese) were included [11, 12].
Studies including patients with COPD who underwent CPET and either 6MWT or ISWT were selected. The inclusion criteria were as follows: (1) full-text original article; (2) studies on patients with COPD; (3) studies measuring peak VO2 using CPET; and (4) studies investigating the correlation between 6MWT and CPET or between ISWT and CPET. The exclusion criteria were as follows: (1) case reports, case series, and review articles; (2) studies that do not report extractable data available for independent parameters; (3) studies investigating only the correlation between 6MWT and ISWT; and (4) studies on patients with other lung diseases.
Data extraction
Data from included studies were independently extracted and assessed by two independent reviewers (GC and DP) using a standardized data collection form. Discrepancies were resolved by rechecking the source paper and further discussion among all authors. To investigate the correlations between peak VO2 and 6MWT distance or between peak VO2 and ISWT distance in patients with COPD, we divided the data extracted according to field test type (6MWT and ISWT).
We extracted the following data from eligible studies: surname of the first author, publication year, number of patients, sex ratio, mean age, the results of 6MWT and ISWT distances (meter), peak VO2 (ml min−1 kg−1 or ml min−1), the measurement property of peak VO2 in CPET, and the correlation coefficient between peak VO2 and distance of field test (6MWT or ISWT).
Quality assessment
The quality of included studies was assessed using the Methodological Index for Non-Randomized Studies (MINORS) [13]. Each study was assessed using eight criteria (maximum score 16): a clearly stated aim, inclusion of consecutive patients, prospective collection of data, endpoints appropriate to the aim of the study, unbiased assessment of the study endpoint, follow-up period appropriate to the aim of the study, loss to follow up less than 5%, and prospective calculation of the study. The quality of each study was graded as not reported (0), reported but inadequate (1), and reported and adequate (2).
Statistical analysis
The R Statistics software version 4.0.2 (The R Foundation, Vienna, Austria) was used for statistical analysis of the pooled data. For the meta-analysis, the “meta” and “metafor” packages were used. We analysed the summary of correlation coefficient for validity assessment of 6MWT or ISWT to predict peak VO2. In each meta-analysis, I2 statistics was used to assess the heterogeneity, providing a measure of extent of inconsistency among results. Statistical significance was set at p value < 0.05, and a 95% confidence interval (CI) was used. The risk of publication bias was determined using a funnel plot and the Egger's test. Since the included studies were relatively homogenous patients and estimated that the effect size of the population would be consistent, a fixed-effect model was used. Sensitivity analysis was performed using a random-effects model to explore the effects of computational model. Further, studies that conducted each one of 6MWT, ISWT, and CPET were analysed.
As there was a substantial heterogeneity of correlation coefficiencies between peak VO2 and 6MWT distance, subgroup analysis using study-level characteristics was performed [14]. The exercise capacity of populations studied demonstrated a high between-study variability. We, therefore, divided the patients with COPD into low or high exercise capacity group using the cut-off of the peak VO2 of 15 ml ∙min−1 ∙kg−1 or 1000 ml ∙min−1 [15, 16].
Results
Identification of relevant studies
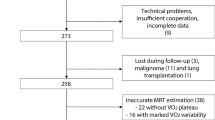
A total of 797 published studies were found after removing 358 duplicate articles from 1153 articles searched by keyword, and two additional articles were identified through other sources. Of the 797 retrieved articles, 12 studies were finally included in the meta-analysis after the inclusion and exclusion criteria were applied (Fig. 1) [5, 6, 11, 12, 17,18,19,20,21,22,23,24].

Preferred reporting items for systematic reviews and meta-analyses flow diagram for the identification of studies included in the meta-analysis about the correlation between peak VO2 and 6MWT and ISWT distances in patients with COPD. Abbreviations: peakVO2, peak oxygen uptake; 6MWT, 6-min walk test; ISWT, incremental shuttle walk test; COPD, chronic obstructive pulmonary disease
Study characteristics
Study characteristics and detailed methodologies of included studies are reported in Tables 1 and 2. Twelve studies included a total of 746 patients with COPD, with individual sample size ranging from 13 to 209. According to the type of field test, 10 studies reported correlation between peak VO2 and 6MWT distance and five studies reported correlation between peak VO2 and ISWT distance.
Quality assessment
In all included studies, ‘a clearly stated aim’, ‘inclusion of consecutive patients’, ‘endpoints appropriate to the aim of the study’, ‘unbiased assessment of the study endpoint’, and ‘follow-up period appropriate to the aim of the study’ were reported adequately. However, regarding ‘prospective collection of data’, only one study reported inappropriately. More than 5% loss to follow-up was reported in three studies. Any included studies did not calculate the appropriate sample size prior to the initiation of each study (Additional file 1: Table S1).
Meta-analysis results
In patients with COPD who underwent CPET and 6MWT (10 studies, n = 714), the 6MWT distance was a significant predictor of peak VO2 measured using CPET (r = 0.65, 95% CI 0.61 to 0.70). In patients with COPD who underwent CPET and ISWT (5 studies, n = 169), the ISWT distance was also a significant predictor of peak VO2 measured using CPET (r = 0.81, 95% CI 0.74 to 0.85). The heterogeneity was higher in 6MWT than in ISWT (6MWT: I2 = 56%; p = 0.02, ISWT: I2 = 0%; p = 0.69) (Fig. 2).

Forest plot of meta-analysis. Meta-analysis was performed in A 10 studies assessing the correlation coefficient between peak VO2 and distance of the 6MWT and in B five studies assessing the correlation coefficient between peak VO2 and ISWT distance. 6MWT, 6-min walk test; peak VO2, peak oxygen uptake; ISWT, incremental shuttle walk test
Sensitivity analysis was conducted to evaluate the effects of computational model. The heterogeneity, pooled correlation coefficients, and 95% CI of the indexes remained stable and were not significantly altered by the random-effects model (6MWT: r = 0.65, 95% CI 0.57–to 0.72, ISWT: r = 0.81, 95% CI 0.74– to 0.85; p < 0.0001) (Additional file 2: Fig. S1. We performed sensitivity analysis on three studies that conducted each one of 6MWT, ISWT, and CPET. The ISWT also showed a stronger correlation than 6MWT (6MWT: r = 0.75; 95% CI 0.66– to 0.82, ISWT: r = 0.80; 95% CI 0.73–to 0.85, p < 0.0001) (Additional file 3: Fig. S2).
We performed a subgroup analysis for exercise capacity of patients with COPD according to the mean of peak VO2: low exercise capacity group, peak VO2 < 15 ml ∙min−1 kg−1 or 1000 ml min−1; and high exercise capacity group, peak VO2 ≥ 15 ml min−1 kg−1 or 1000 ml min−1. In both field tests, the correlation coefficient was higher in the low exercise capacity group than in the high exercise capacity group (low exercise capacity group: r = 0.70 [6MWT], r = 0.81 [ISWT]; p = 0.017, high exercise capacity group: r = 0.63 [6MWT], r = 0.75 [ISWT]; p = 0.256). The heterogeneity of 6MWT in the high exercise capacity group was higher than in the low exercise capacity group (low exercise capacity group: I2 = 43%; p = 0.15, high exercise capacity group: I2 = 60%; p = 0.03). The heterogeneity of ISWT was very low and consistent regardless of peak VO2 (low exercise capacity group: I2 = 0%; p = 0.44, high exercise capacity group: I2 = 0%; p = 0.76) (Fig. 3).

Forest plot and bubble plot of subgroup analysis divided by exercise capacity. #: In this study, we used the cut-off of the peak VO2 for 1000 ml∙min−1. Abbreviations: 6MWT, 6-min walk test; peak VO2, peak oxygen uptake; ISWT, incremental shuttle walk test
Publication bias
A funnel plot was created to investigate the risk of publication bias. In patients with COPD who underwent CPET and 6MWT, a funnel plot between peak VO2 and 6MWT distance showed some asymmetry. However, the Egger's test showed no statistical significance (p = 0.73). These findings indicate that the asymmetry observations were not supported and that there may be no risk of publication bias. In patients with COPD who underwent CPET and ISWT, a funnel plot between peak VO2 and ISWT distance showed symmetry. The Egger's test showed no statistical significance (p = 0.62), indicating that there may be no risk of publication bias (Fig. 4).

Linear regression test of funnel plot asymmetry for identifying publication bias. Abbreviations: 6MWT, 6-min walk test; peak VO2, peak oxygen uptake; ISWT, incremental shuttle walk test
Discussion
Several studies have compared the correlation between peak VO2 and ISWT and 6MWT distances, but this study is the first to perform a meta-analysis of the correlation. This meta-analysis provided further evidence that the 6MWT and ISWT distances had significant correlations with peak VO2 measured using CPET in patients with COPD. When comparing the correlation coefficients with peak VO2, the ISWT showed a stronger correlation than the 6MWT. These results suggest that ISWT reflects a stronger correlation with peak VO2 measured using CPET than 6MWT in patients with COPD.
To date, many studies have confirmed that 6MWT and ISWT are valid, reliable, and responsive to therapeutic interventions [8, 25, 26]. However, the 6MWT and ISWT entail substantially different protocols. The 6MWT is a self-paced submaximal test and can be performed continuously or intermittently. This test is sensitive to methodological variations, such as encouragement, oxygen supplement, and circumstances (e.g., wheeled walking aid, circular/straight track, indoors/outdoors) [26]. By contrast, ISWT is an externally paced maximal exercise test [5, 8, 26]. This feature may be an advantage in circumstances where methodological variation is a concern if the test is performed by various sites or operators [8]. In addition, where the larger space requirements of 6MWT preclude its use, ISWT can be a useful alternative [8]. 6MWT requires a 30-m walking course, but ISWT only requires a short course of 10-m walking course. The protocol of ISWT is more standardized than that of 6MWT, and the proposal of incremental values is also clear in the shuttle walk test. In addition, ISWT shows a linear change of lung gas exchange including peak VO2, but 6MWT shows an exponential change [24]. Furthermore, the walking distance in ISWT has been reported to be reliable and a good indicator for predicting re-hospitalisations in patients with moderate to severe COPD [27]. Therefore, ISWT has better features than 6MWT.
Thus, we aimed to determine the correlation between peak VO2 and 6MWT and ISWT distances through a meta-analysis and to compare the correlation coefficient of both field tests. In this study, both field tests were confirmed to show a relatively strong correlation with peak VO2 through a meta-analysis. Notably, the correlation coefficient of ISWT was stronger than that of 6MWT. In a subgroup analysis, we found that both field tests had lower correlation coefficients in the high exercise capacity group. That is, when the exercise capacity was good, the correlation between the distance of field tests and peak VO2 decreased. This may be related to the “ceiling effect” that occurred in 6MWT. In a related study comparing bronchodilator-induced changes in exercise capacity with the 6MWT and the shuttle walk test, 6MWT showed less responsive for detecting changes in COPD patients with high exercise capacity [28]. In addition, the heterogeneity of ISWT was very low in all analyses. Although there was a limitation to the small number of the included ISWT studies, the low heterogeneity could support the good reproducibility of ISWT. On the contrary, 6MWT showed high heterogeneity, particularly in the high exercise capacity group. ISWT was proven superior to 6MWT for evaluating COPD patients with high exercise capacity.
The 6MWT is reported as a valid and reliable field test and reflects performance of more activities of daily life [4]. A previous study found that changes in dyspnea grade, patient-reported outcomes, 6-min walk distance (6MWD), and cycle endurance time (constant work-rate test), after pulmonary rehabilitation, did not show synchronous responses in patients with COPD, suggesting the need for various tests to evaluate the response in exercise intolerance [29]. Therefore, we proposed that 6MWT, ISWT, and CPET be used complementary to each other to evaluate the exercise capacity of patients with COPD. In our results, the correlation with peak VO2 and the heterogeneity of the ISWT were higher, and the heterogeneity of the 6MWT was higher especially in the high exercise capacity group. Therefore, we cautiously recommend performing the ISWT in patients with high exercise capacity and the 6MWT in those with low exercise capacity. The most appropriate exercise tests should be applied, depending on each COPD patient’s exercise capacity to evaluate their underlying pathophysiology of exercise intolerance.
Despite the advantages of the ISWT, it is underutilized to evaluate exercise capacity and effectiveness of treatment and respiratory rehabilitation and to predict prognosis in chronic respiratory diseases. Many studies have already demonstrated its superiority in preoperative evaluation, respiratory rehabilitation, and cardiopulmonary function evaluation. However, the ISWT has not been introduced in many countries, including South Korea. Thus, adoption of various complementary tests and evaluation of exercise capacity with an appropriate test will enable comprehensive assessment and provision of an individualized exercise program in patients with COPD nature.
This systematic review and meta-analysis have several limitations that should be mentioned. Firstly, we only included a small number of studies. Secondly, in the included studies, exercise modalities in CPET were heterogeneous. Peak VO2 was measured using a treadmill in three studies and a cycle ergometer in nine studies. Several studies have reported that the peak VO2 measured using a cycle ergometer is lower than that using a treadmill, but both peak VO2 measured with these devices show a significant correlation [30, 31]. In addition, the objective of this study was not to analyse the absolute value of the peak VO2, but to investigate the correlation between the peak VO2 and the field test results. Therefore, the difference in CPET exercise method is believed to not significantly affect the results of this study. Finally, for more convincing evidence with regard to the correlation between peak VO2 and field tests, more qualified prospective studies are required. In addition, future studies should verify whether the correlation coefficient of ISWT is superior to that of 6MWT as a primary outcome after calculating the sample size with the superiority study design.
Conclusions
The present study revealed further evidence that 6MWT and ISWT correlated significantly with peak VO2 measured using CPET in patients with COPD through a meta-analysis. Moreover, the ISWT distance showed a stronger correlation with peak VO2 than did the 6MWT distance as expected, suggesting that ISWT is more valid and reliable for assessing the maximal exercise capacity in patients with COPD. However, the strength of the relationship between peak VO2 and walking distance in the field tests was affected by the exercise capacity in COPD patients, suggesting the importance of using various exercise tests.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Celli BR, MacNee W. ATS/ERS task force standards for the diagnosis and treatment of patients with COPD: a summary of the ATS/ERS position paper. Eur Respir J. 2004;23:932–46.
American Thoracic Society, American College of Chest Physicians. ATS/ACCP Statement on cardiopulmonary exercise testing. Am J Respir Crit Care Med. 2003;167:211–77.
Singh SJ, Morgan MD, Scott S, Walters D, Hardman AE. Development of a shuttle walking test of disability in patients with chronic airways obstruction. Thorax. 1992;47:1019–24.
ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med. 2002;166:111–7.
Turner SE, Eastwood PR, Cecins NM, Hillman DR, Jenkins SC. Physiologic responses to incremental and self-paced exercise in COPD: a comparison of three tests. Chest. 2004;126:766–73.
Singh SJ, Morgan MD, Hardman AE, Rowe C, Bardsley PA. Comparison of oxygen uptake during a conventional treadmill test and the shuttle walking test in chronic airflow limitation. Eur Respir J. 1994;7:2016–20.
Parreira VF, Janaudis-Ferreira T, Evans RA, Mathur S, Goldstein RS, Brooks D. Measurement properties of the incremental shuttle walk test a systematic review. Chest. 2014;145:1357.
Singh SJ, Puhan MA, Andrianopoulos V, Hernandes NA, Mitchell KE, Hill CJ, et al. An official systematic review of the European Respiratory Society/American Thoracic Society: measurement properties of field walking tests in chronic respiratory disease. Eur Respir J. 2014;44:1447–78.
Elías Hernández MT, Fernández Guerra J, Toral Marín J, Ortega Ruiz F, Sánchez Riera H, Montemayor RT. Reproducibility of a shuttle walking test in patients with chronic obstructive pulmonary disease. Arch Bronconeumol. 1997;33:64–8.
Moher D, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6:e1000097.
Arizono S, Kitagawa C, Tanaka T, Oike T, Rikitomi N, Takahashi T, et al. Validity of incremental shuttle walking test as a measure of exercise tolerance in chronic obstructive pulmonary disease. J Jpn Soc Respir Care. 2002;11:414–9.
Arizono S, Ogawa T, Watanabe F, Homon R, Hirasawa J, Kondoh Y, et al. Prediction of peak V̇O2 using 6 minutes walk test and incremental shuttle walking test in COPD patients. J Jpn Soc Respir Care. 2008;18:160–5.
Slim K, Nini E, Forestier D, Kwiatkowski F, Panis Y, Chipponi J. Methodological index for non-randomized studies (MINORS): development and validation of a new instrument. ANZ J Surg. 2003;73:712–6.
Cordero CP, Dans AL. Key concepts in clinical epidemiology: detecting and dealing with heterogeneity in meta-analyses. J Clin Epidemiol. 2021;130:149–51.
Oga T, Nishimura K, Tsukino M, Sato S, Hajiro T. Analysis of the factors related to mortality in chronic obstructive pulmonary disease: role of exercise capacity and health status. Am J Respir Crit Care Med. 2003;167:544–9.
Hiraga T, Maekura R, Okuda Y, Okamoto T, Hirotani A, Kitada S, et al. Prognostic predictors for survival in patients with COPD using cardiopulmonary exercise testing. Clin Physiol Funct Imaging. 2003;23:324–31.
Rejeski WJ, Foley KO, Woodard CM, Zaccaro DJ, Berry MJ. Evaluating and understanding performance testing in COPD patients. J Cardiopulm Rehabil. 2000;20:79–88.
Chuang ML, Lin IF, Wasserman K. The body weight-walking distance product as related to lung function, anaerobic threshold and peak VO2 in COPD patients. Respir Med. 2001;95:618–26.
Oga T, Nishimura K, Tsukino M, Hajiro T, Ikeda A, Mishima M. Relationship between different indices of exercise capacity and clinical measures in patients with chronic obstructive pulmonary disease. Heart Lung. 2002;31:374–81.
Carter R, Holiday DB, Nwasuruba C, Stocks J, Grothues C, Tiep B. 6-minute walk work for assessment of functional capacity in patients with COPD. Chest. 2003;123:1408–15.
Starobin D, Kramer MR, Yarmolovsky A, Bendayan D, Rosenberg I, Sulkes J, et al. Assessment of functional capacity in patients with chronic obstructive pulmonary disease: correlation between cardiopulmonary exercise, 6 minute walk and 15 step exercise oximetry test. Isr Med Assoc J. 2006;8:460–3.
Hill K, Jenkins SC, Cecins N, Philippe DL, Hillman DR, Eastwood PR. Estimating maximum work rate during incremental cycle ergometry testing from six-minute walk distance in patients with chronic obstructive pulmonary disease. Arch Phys Med Rehabil. 2008;89:1782–7.
Díaz O, Morales A, Osses R, Klaassen J, Lisboa C. Six-minute-walk test and maximum exercise test in cycloergometer in chronic obstructive pulmonary disease. Are the physiological demands equivalent? Arch Bronconeumol. 2010;46:294–301.
Onorati P, Antonucci R, Valli G, Berton E, De Marco F, Serra P, et al. Non-invasive evaluation of gas exchange during a shuttle walking test vs a 6-min walking test to assess exercise tolerance in COPD patients. Eur J Appl Physiol. 2003;89:331–6.
Papathanasiou JV, Ilieva E, Marinov B. Six-minute walk test: an effective and necessary tool in modern cardiac rehabilitation. Hellenic J Cardiol. 2013;54:126–30.
Holland AE, Spruit MA, Troosters T, Puhan MA, Pepin V, Saey D, et al. An official European Respiratory Society/American Thoracic Society technical standard: field walking tests in chronic respiratory disease. Eur Respir J. 2014;44:1428–46.
Emtner MI, Arnardottir HR, Hallin R, Lindberg E, Janson C. Walking distance is a predictor of exacerbations in patients with chronic obstructive pulmonary disease. Respir Med. 2007;101:1037–40.
Pepin V, Brodeur J, Lacasse Y, Milot J, Leblanc P, Whittom F, et al. Six-minute walking versus shuttle walking: responsiveness to bronchodilation in chronic obstructive pulmonary disease. Thorax. 2007;62:291–8.
Mador MJ, Modi K. Comparing various exercise tests for assessing the response to pulmonary rehabilitation in patients with COPD. J Cardiopulm Rehabil Prev. 2016;36:132–9.
Mays RJ, Boér NF, Mealey LM, Kim KH, Goss FL. A comparison of practical assessment methods to determine treadmill, cycle, and elliptical ergometer V̇O2 peak. J Strength Cond Res. 2010;24:1325–31.
Loftin M, Sothern M, Warren B, Udall J. Comparison of VO2 peak during treadmill and cycle ergometry in severely overweight youth. J Sports Sci Med. 2004;3:554–60.
Acknowledgements
The authors would like to thank Yangjin Jegal, Taehoon Lee, Byung Ju Kang, and Jin Hyoung Kim (Ulsan University Hospital) for giving valuable comments at the research meeting.
Funding
None.
Author information
Authors and Affiliations
Contributions
GC enriched the conception, conducted literature search, assessed the studies, and wrote the first draft of the manuscript. EJK and SWL commented on the earlier drafts of the manuscript and approved the final manuscript. HJK and SGK commented the methodology. DP initiated the conception of this review, conducted literature search, assessed the studies, and revised the final manuscript. SWR initiated the conception of this review, directed the design, and approved the final manuscript. All the authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The present study was approved by the Institutional Review Board of Ulsan University Hospital (NON2020-001).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1. Table S1:
Results of quality assessment for included studies using the Methodological Index for Non-Randomized Studies.
Additional file 2. Figure S1:
Forest plot of sensitivity analysis performed using a random-effects model. 6MWT, 6-minute walk test; peak VO2, peak oxygen uptake; ISWT, incremental shuttle walk test.
Additional file 3. Figure S2:
Forest plot of sensitivity analysis performed on three studies that conducted each one of 6MWT, ISWT, and CPET. 6MWT, 6-minute walk test; ISWT, incremental shuttle walk test; CPET, cardiopulmonary exercise testing; peak VO2, peak oxygen uptake.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Chae, G., Ko, E.J., Lee, S.W. et al. Stronger correlation of peak oxygen uptake with distance of incremental shuttle walk test than 6-min walk test in patients with COPD: a systematic review and meta-analysis. BMC Pulm Med 22, 102 (2022). https://doi.org/10.1186/s12890-022-01897-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12890-022-01897-0