
Abstract
Background
Early neonatal deaths, occurring within the first six days of life, remain a critical public health challenge. Understanding the trends and factors associated with this issue is crucial for designing effective interventions and achieving global health goals. This study aims to examine the trends in early neonatal mortality in Ethiopia and identify the key factors associated with changes in early neonatal mortality over time.
Methods
This study utilized five consecutive Ethiopian Demographic and Health Survey datasets from 2000 to 2019. To investigate the trends and identify factors influencing changes in early neonatal mortality over time, conducted a trend analysis and a logit-based multivariate decomposition analysis. Data management and analyses were performed using STATA version 17/MP software. All analyses were weighted to account for sampling probabilities and non-response. Statistical significance was determined at a two-sided p-value threshold of less than 0.05.
Result
The analysis included a total of 12,260 weighted women from the 2000 survey and 5,527 weighted women from the 2019 survey. Over the study period, there was an overall downward trend in early neonatal mortality, decreasing from 34 deaths per 1000 live births in 2000 to 27 deaths per 1000 live births in 2019. The annual rate of reduction was estimated to be 1.03%. Approximately 45% of the observed decline in early neonatal mortality rate can be attributed to changes in population characteristics or endowments (E) during the study period. Factors such as the mother’s age, maternal education, marital status, preceding birth interval, types of pregnancy, and the sex of the child significantly contributed to the compositional change in the early neonatal mortality rate.
Conclusion
Over the past two decades, Ethiopia has seen a modest decline in early neonatal mortality, but this progress falls short of the Sustainable Development Goal (SDGs) targets. To achieve the SDGs, the Ministry of Health and its partners should intensify efforts to reduce early neonatal mortality. Strategies like preventing early/late pregnancies, promoting appropriate marriage timing, and prioritizing education could help further reduce early neonatal deaths. Further research is also needed to explore the factors driving this issue.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Introduction
Neonatal mortality, defined as the number of deaths among live-born infants before 28 completed days, is a critical indicator of a country’s socioeconomic development and quality of life [1]. Within the neonatal period, early neonatal mortality specifically refers to the probability of dying during the first six days of life per 1000 live births [2].
Unfortunately, global estimates indicate that over 5.0 million children under the age of five and 2.4 million infants died in 2020, with newborns accounting for half of these deaths [1]. Alarmingly, nearly 3 million children worldwide die within the neonatal period, with a staggering 99% of these deaths occurring in low and middle-income countries [3]. Moreover, within the neonatal period, the majority of deaths (75%) occur within the first week of life, with a substantial proportion (25–45%) occurring within the first 24 h after birth [2].
While Ethiopia has made overall progress in reducing under-five and infant mortality rates, the country has experienced an unfortunate increase in neonatal deaths, with the neonatal mortality rate rising from 29 deaths per 1,000 live births in 2016 to 33 deaths per 1,000 live births in 2019. This reversal in the trend is a significant public health concern that requires urgent attention. However, the factors contributing to the rising neonatal mortality rates in Ethiopia are not well-understood [4].
The Sustainable Development Goals (SDGs) prioritize the reduction of under-five child mortality rates globally. To achieve this goal, it is crucial to address neonatal mortality rates, particularly in high-risk nations, where 98% of neonatal deaths occur (https://ethiopia.un.org/en/sdgs/3). The SDGs have set targets to lower newborn mortality to 25 and under-five mortality to 12 per 1,000 live births by 2030 [5]. Achieving these objectives necessitates a concerted effort to decrease early neonatal mortality rates, especially in developing nations.
Fortunately, evidence suggests that up to 50% of neonatal deaths can be prevented through cost-effective interventions that can be implemented before, during, and after delivery [6]. These interventions play a crucial role in reducing early neonatal mortality rates and improving the survival chances of newborns. However, the lack of understanding of the specific drivers of neonatal mortality in Ethiopia hampers the development of targeted policies and interventions.
Therefore, this study aims to investigate the trends and factors associated with neonatal mortality in Ethiopia. By identifying the contributing factors and understanding the underlying causes, policymakers and healthcare professionals can develop targeted interventions and strategies to effectively reduce early neonatal mortality rates and achieve the SDG targets. The findings of this study will fill an important research gap and provide critical insights to guide the efforts towards improving neonatal health and survival in Ethiopia.
Methods and materials
Study area, period, and design
Ethiopia is located in the horn of Africa, with its geographical coordinates ranging between latitude 3° and 14°N and longitude 33° and 48°E. The country spans a total area of 1,100,000 square kilometers (https://ethiopianembassy.org/overview-about-ethiopia/) and is divided into nine regional states, namely Tigray, Afar, Amhara, Gambela, Benishangul-Gumuz, Harari, Oromia, Somali, and Southern Nations Nationalities and Peoples of Region, along with two city administrations (Addis Ababa and Dire Dawa). The analysis utilized data from the Ethiopian Demographic and Health Surveys (EDHS) conducted in 2000, 2005, 2011, 2016, and 2019. The study employed a community-based cross-sectional study design.
Source and study population
The source population for this study consisted of all women of reproductive age who had given birth within five years before each survey. The study population included reproductive-age women who had given birth within five years preceding each survey in the selected enumeration areas (EAs). The surveys utilized nationally representative samples drawn from birth records, with the following weighted numbers of women participating: 12,260 in 2000, 11,163 in 2005, 11,872 in 2011, 11,022 in 2016, and 5,527 in 2019.
Data collection tools and procedures
The data collection process for each survey year involved two stages. Stratification was carried out based on urban and rural areas within each region of the country. In the first stage, a specific number of enumeration areas (EAs) were selected: 539 EAs in 2000, 535 EAs in 2005, 596 EAs in 2011, 643 EAs in 2016, and 305 EAs in 2019 for the EDHS. In the second stage, a fixed number of households were selected within each EA using systematic sampling. For the detailed sampling procedure, can refer to the EDHS reports available on the Measure DHS website (https://dhsprogram.com/Data/terms-of-use.cfm) for each specific survey.
Outcome variable
Dependent variables: Early neonatal mortality (Yes, No).
Early neonatal mortality refers to the mortality of newborn babies within the first six days of life. For regression analysis, newborn babies who experienced mortality within the first six days were coded as ‘1’, while newborn babies who survived beyond six days were coded as ‘0’.
Independent variables: Socio-demographic characteristics (age of the women, maternal educational status, marital status, place of residency and region), Maternal and Neonatal characteristics (high-risk fertility, antenatal care, place of delivery, mode of delivery, postnatal care, birth interval, birth order, types of pregnancy and sex of the baby).
Decomposing variable: Survey year was used to decompose (2000 labeled as “0” and 2019 labeled as “1”).
Operational definition
Early neonatal mortality refers to the deaths of newborn babies that occur within the first six days of their postnatal age, as recorded in the dataset.
Risk fertility behavior refers to the characteristics of mothers who exhibit behaviors associated with higher risks in terms of fertility. These behaviors include being too young (under the age of 18) or too old (over the age of 34), having short birth intervals (less than 24 months between the preceding birth and the current pregnancy), and having a high parity (having more than three children).
Data management and analysis
The data were extracted, edited, coded, and verified by using STATA version 17/MP software. Descriptive statistics were conducted to understand the variables. The trends were analyzed separately for each survey period. Before conducting statistical tests, the data was weighted using sampling weight, primary sampling unit, and strata to ensure the survey’s representativeness. The trend in early neonatal mortality rate was estimated by calculating the rate difference and annual rate of reduction. The annual rate of reduction (ARR) was used to describe the decrease in mortality rate per year. In this study, ARR was calculated as follows:
• r1 = mortality rate for the year of the survey used as a baseline
• r2 = mortality rate in the year of the final survey
• t = number of years between the first and second survey
A recently developed statistical technique called multivariate decomposition was employed in this study to analyze the differences in a distribution statistic between two groups or its change over time. This approach allows for the decomposition of the components of a group difference or change into various explanatory factors. The technique utilizes regression models to separate the factors contributing to the differences in a statistic, such as a mean or proportion, between groups. These factors include compositional differences between groups, differences in characteristics (endowments), and differences in the effects of characteristics (differences in coefficients). This analysis technique is also useful for examining changes over time, as it can partition the components of change into those attributable to changing composition and changing effects [7]. In this particular study, a non-linear multivariate logit decomposition model was used to assess the contribution of changes in proportion to the early neonatal mortality rate over the past two decades.
The proportion difference in early neonatal mortality rate between 2000 and 2019 EDHS surveys can be decomposed as:
For the log odds of early neonatal mortality rate, the proportion of the model is written as.
The component ‘E’ is the difference attributable to endowment change, usually called the explained component. The ‘C’ component is the difference attributable to coefficients (behavioral) change, usually called the unexplained component.
Result
Background characteristics of the study population
Table 1 provides information on the distribution of individual characteristics of women who gave birth in the five years preceding each survey conducted between 2000 and 2019. The average age of respondents was 29.5 years (+ 6.9) in 2000 and 28.6 years (+ 6.5) in 2019, indicating a slight decrease over the study period. In terms of maternal education, the percentage of uneducated mothers decreased from 82.07% in 2000 to 53.58% in 2019, showing a significant decline. This suggests an improvement in educational attainment among women over time.
These findings highlight several positive changes in individual characteristics and healthcare utilization among women giving birth in Ethiopia between 2000 and 2019. In both survey years, the proportion of males among the newborns was approximately 51%, indicating a relatively balanced sex ratio. Furthermore, there was a notable increase in the utilization of antenatal care services and institutional delivery. The proportion of women receiving the recommended fourth or more antenatal care visits increased by 4.2 times, indicating an improvement in access to prenatal care. Similarly, the percentage of women giving birth in a healthcare facility (institutional delivery) increased by nearly 10 times, reflecting an enhanced utilization of healthcare facilities during childbirth. The increase in educational attainment, antenatal care visits, institutional deliveries, and Cesarean section deliveries signifies progress in maternal and newborn health services (Table 2).
Trends of early neonatal mortality in the five survey years
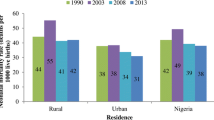
The early neonatal mortality rate in Ethiopia showed a significant decrease from 2000 to 2019. During Phase I (2000 to 2016) and Phase III (2000 to 2019), there was an overall decline in the early neonatal mortality rate, decreasing from 34 per 1000 live births in 2000 to 27 per 1000 live births in 2019 (Fig. 1), with an annual rate of reduction of 1.03%. However, in Phase II (2016 to 2019), there was a slight increase in the early neonatal mortality rate, rising from 22 to 27 per 1000 live births (Table 3).

Trends of early neonatal mortality in Ethiopia; 2000–2019
The rate of decline in early neonatal mortality varied among different background characteristics of the study participants. Among the eleven regions included in the analysis, only four regions (Tigray, Amhara, Oromia, and Southern nation nationality) showed a significant reduction in early neonatal mortality rates. The Southern nation nationality region exhibited the largest annual rate of reduction (ARR) in early neonatal mortality rates with the total reductions of 67 deaths per 1000 live births, respectively, from 2000 to 2019.
The rate of reduction was highest among participants who had home deliveries (2.4 per annum), received no antenatal care visits (2.29 per annum), had twin pregnancies (2.05 per annum), were uneducated (2.03 per annum), and were currently not married (1.93 per annum). Conversely, the lowest average annual rate of reduction was observed in the Somali region (-85.71% per annum), Dire Dawa (-12.5% per annum), and among mothers who gave birth in a healthcare institution and through cesarean section delivery (-49.6 and − 38.6 per annum, respectively) (Table 3).
Across all surveys, the early neonatal mortality rate showed a decline for mothers living in rural areas, uneducated women, those with a single high-risk fertility factor, women who delivered at home, and women with twin pregnancies. However, the Somali region recorded an increase of 119 deaths per 1000 live births in early neonatal mortality throughout 2000 to 2019.
These findings underscore the varying trends in early neonatal mortality rates across different regions and population groups in Ethiopia. It highlights the need to target interventions and resources to regions and populations where early neonatal mortality rates remain high or have experienced an increase. By addressing the factors contributing to these trends, further progress can be made in reducing early neonatal mortality and improving overall neonatal health in Ethiopia.
Decomposition analysis
The early neonatal mortality rate in Ethiopia has seen a significant reduction of 8 per 1000 live births from 2000 to 2019. A multivariate decomposition logistic regression analysis reveals that approximately 45% of the observed mortality difference can be attributed to the characteristics of the surveyed women, known as compositional factors (Table 4).
Several compositional factors were found to have a notable impact on the change in early neonatal mortality. These factors include the age of the mother, maternal education, marital status, preceding birth interval, types of pregnancy, and the sex of the child. The analysis indicates that certain changes in these factors positively or negatively contributed to the decline in early neonatal mortality rates.
The reduction in early neonatal mortality rates was significantly influenced by an increase in the proportion of women aged 20 to 34 years, married women, and those with primary or higher education. Conversely, compositional factors that remained relatively stable or unchanged exhibited a negative correlation with the decline in early neonatal mortality rates. These factors include birth intervals of 24 months or more, singleton pregnancies, and male infants.
After accounting for the effect of compositional factors, it was found that 55% of the change in early neonatal mortality between 2000 and 2019 in Ethiopia can be attributed to behavioral change factors or the effects of specific characteristics, rather than the structural composition of the two cohorts. However, this difference was not statistically significant (Table 4). These findings underscore the importance of considering various compositional factors (endowments) rather than coefficients when analyzing changes in early neonatal mortality rates. Understanding the specific contributions of these factors can provide valuable insights for designing effective interventions and policies to further reduce neonatal mortality rates in Ethiopia.
Discussion
Early neonatal mortality is a crucial measure of newborn health and has a strong association with neonatal and under-five mortality rates. It poses a significant challenge, especially in low-income countries such as Ethiopia, where efforts to reduce early neonatal mortality are of utmost importance. Therefore, this study aims to examine the pattern and multivariate decomposition of early neonatal mortality in Ethiopia over the past two decades.
The early neonatal mortality rate in Ethiopia has shown a significant decrease from 34 per 1000 live births in 2000 to 27 per 1000 live births in 2019. This decline is in line with Ethiopia’s commitment to achieving the Sustainable Development Goals (SDGs) and its efforts to reduce neonatal mortality (https://www.scribd.com/document/518384802/Annual-Performance-Report-2012-2019-2020). The Ethiopian government, along with development partners and organizations, has implemented several initiatives aimed at improving access to healthcare, enhancing maternal and child health services, and increasing community awareness of newborn care. These interventions have played a crucial role in addressing the factors contributing to early neonatal mortality [8]. However, despite the decline, the early neonatal mortality rate in Ethiopia remains high compared to global standards. To achieve the SDG targets for neonatal survival, further interventions are necessary. These include strengthening health systems, enhancing the capacity of healthcare professionals, promoting evidence-based practices, and addressing socio-cultural barriers [9].
Multivariate decomposition logistic regression analysis revealed that 45% of the observed early neonatal mortality difference is attributed to maternal characteristics (compositional factors) between the surveys. This highlights the importance of considering women’s characteristics when examining changes in early neonatal mortality rates. Specifically, the compositional change in maternal age, marital status, and education level have made important contributions to the decrease in early neonatal mortality rates in Ethiopia over the last twenty years.
Compositional change in maternal age makes an important contribution to the decrease in early neonatal mortality rate in Ethiopia over the last twenty years. Previous studies have shown that both younger and older maternal ages are associated with an increased risk of early neonatal mortality [10,11,12].
The compositional change in marital status has also been identified as a contributing factor for decrement in early neonatal mortality rate in Ethiopia. This finding highlights the protective role of marriage in early neonatal health outcomes. This might be because married women often have access to emotional and financial support from their spouses, which can contribute to improved health-seeking behavior and better utilization of healthcare services during pregnancy and childbirth. This supportive and stable environment reduces maternal stress which can lead to adverse pregnancy outcomes [13, 14]. Kebede et al. (2021) also found that married women had lower early neonatal mortality rates compared to unmarried or single women [15].
Additionally, the compositional change in the education level of mothers has significantly contributed to the decrease in early neonatal mortality. Educated individuals are more likely to adhere to healthcare recommendations, adopt healthier habits, have better access to media, and have greater decision-making power within their households, all of which contribute to improved neonatal health [16, 17]. Their enhanced financial capacity also plays a crucial role in ensuring adequate care for their newborn babies [18].
However, the data also revealed minimal changes in the composition of women’s birth intervals, which had a substantial negative effect on the rate of early neonatal mortality decline. Longer birth intervals may be associated with factors like delayed access to prenatal care, increased maternal age, or other underlying health conditions that increase the risk of early neonatal mortality [19]. Further research is needed to explore the underlying causes and mechanisms behind this negative impact.
Furthermore, slight decrements in the composition of women with singleton pregnancies and being female were also negatively associated with the change in early neonatal mortality rate. This may be due to women with singleton pregnancies and being female having a higher chance of survival compared to their counterparts [20, 21], potentially due to improved access to healthcare services, better prenatal care, or biological factors that confer a survival advantage [22].
Strengths and limitations
This study utilized a nationally representative dataset with a large sample size, providing robust statistical power to analyze the characteristics of the study population. The findings have implications for healthcare professionals and policymakers in identifying influential factors and designing interventions to reduce early neonatal mortality in Ethiopia. However, it is important to note that certain variables, such as gestational age, comorbidities, NICU admission history, treatment-related characteristics, and details about antenatal and postnatal care, were not included in the analysis due to limited availability or a high number of missing values in the data collected through the EDHS. This limitation restricts the comprehensive examination of these factors’ impact on early neonatal mortality. Moreover, the data collected through the DHS surveys rely on self-reported information, which may be subject to recall bias or social desirability bias. This potential for bias should be considered when interpreting the findings of the study.
Conclusion and recommendations
Over the past two decades, there has been a modest decline in early neonatal mortality in Ethiopia, but the rate remains unacceptably high. Approximately 45% of the overall reduction in early neonatal mortality can be attributed to changes in the characteristics of women during this period. Factors such as the age of the mother, maternal education, marital status, preceding birth interval, type of pregnancy, and the sex of the child have played a role, either positively or negatively, in influencing the change in early neonatal mortality in Ethiopia. To further reduce the early neonatal mortality rate, it is beneficial to encourage pregnancies among women between the ages of 20 and 34, promote marriage, and continue to prioritize education among the population. Additionally, interventions are needed to address the issue of short birth intervals, which has been identified as a significant barrier to delayed initiation of breastfeeding in Ethiopia over the past decade. Lastly, to achieve the Sustainable Development Goals, the Ministry of Health and other stakeholders should continue their efforts to decrease early neonatal mortality. Furthermore, further research is necessary to gain deeper insights into the underlying factors and mechanisms driving early neonatal mortality in Ethiopia.
Data availability
The datasets used during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- ARR:
-
Annual rate of reduction
- ANC:
-
Antenatal care
- C/S:
-
Cesarean section
- DHS:
-
Demographic health survey
- EAs:
-
Enumeration areas
- EDHS:
-
Ethiopian demographic and health survey
- ENMR:
-
Early neonatal mortality rate
- NICUs:
-
Neonatal intensive care units
- SDG:
-
Sustainable Development Goals
- SNNPR:
-
Southern nation’s nationalities and peoples
- UNICEF:
-
United Nations international children’s fund
- WHO:
-
World health organization
References
Sharrow D, Hug L, Sinae Lee YL and DY. Levels & trends in child mortality (UNICEF and UN IGME). 2021.
World Health Organization. Newborns: improving survival and well-being. World Health Organisation; 2019.
Moxon SG, Ruysen H, Kerber KJ, Amouzou A, Fournier S, Grove J et al. Count every newborn; a measurement improvement roadmap for coverage data. (special issue: every woman, every newborn). BMC Pregnancy Childbirth. 2015;15.
CSA. Ethiopia mini demographic and health survey. 2019.
Nations U. Agenda 2030. Encycl Sustain Manag. 2023;16301(October):95–95.
Lawn JE, Blencowe H, Oza S, You D, Lee ACC, Waiswa P et al. Every newborn 2 progress, priorities, and potential beyond survival. 2015;6736(14):7.
Powers DA. Multivariate decomposition for nonlinear response models. Stata J. 2011;4:556–76.
Birhanu BG, Mathibe-Neke JM. Interventions to enhance newborn care in north-west Ethiopia: the experiences of health care professionals. BMC Pregnancy Childbirth. 2022;22(1):1–10.
Ethiopian Public Health Institute E. Reducing neonatal mortality in Ethiopia: a call for urgent action! Full Report. 2021.
Kim YN, Choi DW, Kim DS, Park EC, Kwon JY. Maternal age and risk of early neonatal mortality: a national cohort study. Sci Rep. 2021;11(1):1–9.
Neal S, Channon AA, Chintsanya J. The impact of young maternal age at birth on neonatal mortality: evidence from 45 low and middle income countries. PLoS ONE. 2018;13(5):1–16.
Ganchimeg T, Ota E, Morisaki N, Laopaiboon M, Lumbiganon P, Zhang J, et al. Pregnancy and childbirth outcomes among adolescent mothers: a World Health Organization multicountry study. BJOG. 2014;121(Suppl 1):40–8.
Kane JB. Marriage advantages in perinatal health: evidence of marriage selection or marriage protection? J Marriage Fam. 2016;78(1):212–29.
Al-Mutawtah M, Campbell E, Kubis HP, Erjavec M. Women’s experiences of social support during pregnancy: a qualitative systematic review. BMC Pregnancy Childbirth. 2023;23(1). https://doi.org/10.1186/s12884-023-06089-0
Kebede AA, Cherkos EA, Taye EB, Eriku GA, Taye BT, Chanie WF. Married women’s decision-making autonomy in the household and maternal and neonatal healthcare utilization and associated factors in Debretabor, northwest Ethiopia. PLoS ONE. 2021;16.
Raghupathi V, Raghupathi W. The influence of education on health: an empirical assessment of OECD countries for the period 1995–2015. Arch Public Heal. 2020;78(1):1–18.
Kiross GT, Chojenta C, Barker D, Tiruye TY, Loxton D. The effect of maternal education on infant mortality in Ethiopia: a systematic review and meta-analysis. PLoS ONE. 2019;14(7):1–12.
Lin SJ. The effects of economic instability on infant, neonatal, and postneonatal mortality rates: evidence from Taiwan. Soc Sci Med. 2006;62(9):2137–50.
Rutstein SO. Effects of preceding birth intervals on neonatal, infant and under-five years mortality and nutritional status in developing countries: evidence from the demographic and health surveys. Int J Gynecol Obstet. 2005;89(SUPPL. 1).
Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the global burden of disease study 2010. Lancet. 2012;380(9859):2095–128.
Selemani M, Mwanyangala MA, Mrema S, Shamte A, Kajungu D, Mkopi A et al. The effect of mother’s age and other related factors on neonatal survival associated with first and second birth in rural, Tanzania: evidence from Ifakara health and demographic surveillance system in rural Tanzania. BMC Pregnancy Childbirth. 2014;14(1).
Mitiku HD. Neonatal mortality and associated factors in Ethiopia: a cross-sectional population-based study. BMC Womens Health. 2021;21(1):1–9.
Acknowledgements
We owe the DHS program for granting us access to the data.
Funding
The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
FSB, LA, AA, and AE were involved in this study from the inception to design, acquisition of data, data cleaning, and data analysis. AG, DM, AMH, and AM were involved in data analysis, interpretation, drafting, and revising of the manuscript. ET and FD were involved in supervising the final manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Under the ethical principles outlined in the Declaration of Helsinki, the authors took all necessary steps to adhere to guidelines for medical research. Due to the authors’ limited direct contact with neonates and their families, obtaining informed consent was not feasible. The data sets utilized in this study are accessible through the Ethiopian Statistical Agency and the Ministry of Health. The authors submitted the proposed title and study aim to the online DHS website to download and utilize the data. The EDHS program granted authorization for data access, which was then used in the current study.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Getaneh, F.B., Asmare, L., Endawkie, A. et al. Early neonatal mortality in Ethiopia from 2000 to 2019: an analysis of trends and a multivariate decomposition analysis of Ethiopian demographic and health survey. BMC Public Health 24, 2364 (2024). https://doi.org/10.1186/s12889-024-19880-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-024-19880-1