
Abstract
Background
Maintaining good functional ability is a key component of healthy ageing and a basic requirement for carrying out activities of daily living, staying independent, and delaying admission to a nursing home. Even though women have a higher life expectancy and slower age-related muscle mass loss than men, they often show a higher prevalence of limitations in physical functioning. However, the reasons behind these sex differences are still unclear. Therefore, the aims of this study were to investigate sex differences among older adults regarding physical functioning and to study which factors are explaining these sex differences.
Methods
Cross-sectional data from participants of the OUTDOOR ACTIVE study residing in Bremen, Germany, aged 65 to 75 years, were included in the analyses. Physical functioning was assessed via a self-administered questionnaire using the SF-36 10-item Physical Functioning Scale. Social, lifestyle, and health-related factors were also assessed using the questionnaire. Physical activity was measured objectively using wrist-worn accelerometers over seven consecutive days. Descriptive analyses with absolute and relative frequencies, means and standard deviations, as well as T-tests and chi-square tests were carried out. To test for associations between sex, physical functioning, and several individual factors, linear regressions were performed.
Results
Data of 2 141 participants (52.1% female) were included in the study. Women and men showed statistically significant differences in physical functioning, with men perceiving fewer limitations than women. On average, women had a physical functioning score of 81.4 ± 19.3 and men 86.7 ± 17.0. Linear regression showed a statistically significant negative association between physical functioning score and sex (β: -0.15, 95% CL: -0.19, -0.10). The association remained statistically significant when adding individual factors to the model. All factors together were only able to explain 51% of the physical functioning-sex association with health indicators and the presence of chronic diseases being the most influential factors.
Conclusions
We found sex differences in physical functioning, with older women having more limitations than older men. The results showed that health-related factors and chronic diseases played the biggest roles in the different physical functioning scores of women and men. These findings contribute to future longitudinal, more in-depth research.
Trial registration
German Clinical Trials Register DRKS00015117 (Date of registration 17-07-2018).
Similar content being viewed by others


Background
Maintaining functional ability into higher age is a key component of healthy ageing and has profound consequences on the individual, societal, and economic levels [1, 2]. Good physical functioning is a basic requirement for carrying out activities of daily living (ADL), staying independent, and delaying admission to a nursing home [3]. These are important goals not only for older adults but also for the health system [4].
Physical functioning declines with age, which in most cases leads to frailty and disability [5]. Furthermore, low physical functioning is associated with decreased quality of life [6], an increased risk of hospitalisation [7, 8] and mortality [9, 10]. It is believed, that the decrease of muscle mass, which usually starts during midlife, plays an important role in diminishing physical functioning [11]. The extent to which other factors influence the decline of physical functioning has not been fully investigated, but previous cross-sectional studies have found associations between physical functioning and social support [12], socioeconomic status [13], nutrition [14], and body mass index (BMI) [15]. Longitudinal research has also found physical functioning to be affected by BMI [16], as well as social isolation [17] and physical activity [18].
Even though women have a higher life expectancy, lower risks of several non-communicable diseases, and slower age-related muscle mass loss than men [19,20,21], they often show a higher prevalence of limitations in physical functioning. Hansen et al. [22] for example, found in their sample of 60 to 70-year-old Danes, that 16.8% of men and 20.4% of women displayed limitations in at least two out of three activities. Furthermore, women experience a faster decline in physical functioning and live longer with disabilities [23, 24]. Sex differences regarding limitations in physical functioning are already present among younger adults and broaden with increasing age [25]. Sialino et al. found in their Dutch study an average difference in the physical functioning score (possible 0 to 100 points) of 6 points at the age of 45 and 12 points at age 80, with women scoring lower points than men [25]. However, the reasons behind women having a higher prevalence of limitations in physical functioning are still unclear [11]. First studies have found work and family characteristics [24] as explanations for sex differences in physical functioning among working Japanese adults. Since health behaviours, biological factors, and reporting behaviour (i.e., willingness to report symptoms, recollection of minor health problems) are associated with sex differences in overall health [26,27,28], they are being discussed as potential explanations for sex differences in physical functioning [11, 25, 29].
Understanding the influences of physical functioning in women and men can help designing health-related interventions to maintain physical ability. Since women tend to get older and live alone for a longer period, it is important to investigate the reasons behind the physical functioning differences. Therefore, the study aims to (a) investigate sex differences among older adults regarding physical functioning and (b) to study whether social, lifestyle, and health-related factors are predicting these sex differences.
Methods
Study design and sample
This cross-sectional study is based on the OUTDOOR ACTIVE project, which was part of the prevention research network AEQUIPA in north-western Germany [30]. The project aimed to assess physical activity (PA) among older adults between 65 and 75 years and identify drivers and barriers of PA. Additionally, a community-based physical activity program for older adults was developed using participatory methods. The OUTDOOR ACTIVE study was divided into a pilot study (02/2015 to 01/2018) and a registered cluster-randomized controlled trial (c-RCT) (02/2018-12/2022) [31].
Participants and recruitment
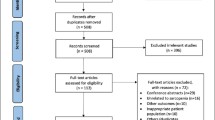
Eligibility criteria included living in pre-defined subdistricts of Bremen (pilot study: Arbergen, Hastedt, Hemelingen, Mahndorf, Sebaldsbrueck; c-RCT: Blumenthal, Burg-Grambke, Gete, Lehe, Lehesterdeich, Neustadt, Ohlenhof, Ostertor), being between 65 and 75 years old, and not being institutionalised. Exclusion criteria were moving out of the study region, language barriers, acute health problems (i.e., every illness or injury that prevented participation), and death. Address data were obtained from the Registration Office Bremen, which is authorized for scientific research. Initially, all potential participants (n = 10 928) were sent an invitation letter and later contacted by phone. Of these, 3 425 individuals were never reached, 4 247 refused participation, and 1 115 were excluded.
The ethics committee of the University of Bremen approved both study parts and all participants provided written informed consent.
Measures
Both the pilot study and the c-RCT consisted of a baseline survey and a follow-up survey, which comprised a self-administered paper-pencil questionnaire, a short physical examination followed by a fitness test, and seven-day accelerometry to objectively measure PA [31, 32]. All assessments were carried out by trained members of the study team, usually a research assistant and a student assistant. To ensure the assessments were done as standardized as possible and therefore minimizing the risks of potential biases, a survey manual was developed and handed to each member of the study team in addition to the training. Additionally, regular quality checks during the survey were carried out.
Social factors
Information on age, sex, marital status, and having a partner were assessed using a self-administered questionnaire. For socioeconomic status (SES), an additive social class index was calculated, consisting of education, income, and occupation (for more details see [32]), with a possible maximum of 100 points. Social support was assessed using the Oslo Social Support Scale [33] and calculating a score (3–14 points), with higher results indicating better social support. Using a modified question from the German Health Interview and Examination Survey [34] participants were asked if they lived alone and, if not, to state their household size (“How many people live in your household?”, response categories: “I live alone”, “We are _ people in the household”).
Physical functioning
Physical functioning was assessed via a self-administered paper-pencil questionnaire using the 10-item Physical Functioning Scale (items 3a-3j) from the MOS 36-Item Short Form Health Survey (Version 1.0) (SF-36) [35]. Participants were asked if they had any limitations regarding ten different activities. Possible answers were limited a lot, limited a little, and not limited at all. A score was calculated with a possible range of 0 to 100 points. Higher scores indicate better physical functioning.
Health-related factors
Self-rated health status and bodily pains in the past four weeks were assessed using questions from the SF-36 (items 1 and 7) [35]. A modified question from the German Health Interview and Examination Survey [34] on chronic diseases was used (“Do you have one or more long-term, chronic diseases?”). A list of chronic diseases was provided, where participants checked the ones they had. Using a self-developed question, participants were asked if they take medications daily (“Do you take medications daily?”) with the response categories “No” and “Yes, namely” followed by an open text field. Shortness of breath during light PA was assessed using a self-developed question (“Are you short of breath during light exertion, e.g. during short walks, light gardening or after climbing a few steps?”), with the response categories “Yes” and “No”.
During the short physical examination body weight and height were measured using a Kern MPC 250K100M personal floor scale (Kern & Sohn GmbH, Balingen, Germany) and a Seca 217 mobile stadiometer (Seca GmbH & Co. KG, Hamburg, Germany), respectively. Subsequently, body mass index (BMI) was calculated by dividing body weight (in kg) by the squared height (in m). The classification of underweight (< 18.5 kg/m2), normal weight (18.5 kg/m2-24.9 kg/m2), overweight (25 kg/m2-29.9 kg/m2), and obesity (≥ 30 kg/m2) by the World Health Organization was used [36].
The consumption of alcohol was assessed using a self-developed question on food frequency (“How often do you eat or drink the following foods?”) with six response categories (“never”, “once a month or less”, “two to three times a month”, “once a week”, “several times a week”, “(almost) daily”). In the questionnaire, more food items were included, but for this analysis, only alcohol as a potential health-compromising behaviour was included. For the analyses, response categories of “never” to “several times a week” were scored as 0 and “(almost) daily” as 1.
Physical activity
Physical activity was measured objectively and via self-report. For objective measurement, the ActiGraph GT3x-BTw (ActiGraph LLC, Pensacola, FL, USA) accelerometers were used. Acceleration and deceleration of the body are measured in three axes [37]. Sampling frequency was set to 30 Hz, data were downloaded and processed using ActiLife (Version 6.13.3 ActiGraph LLC, Pensacola, FL, USA). Participants were asked to wear the devices for seven consecutive days on their non-dominant wrist, if possible, for 24 h. Vector magnitude counts were calculated from the data of the three axes and non-wear time was defined as 90 consecutive minutes with zero counts [38]. Average daily counts per minute (CPM) reflect the total amount of PA and were included in the analyses. Active transport was assessed using a question based on the Neighbourhood Environment and Walkability Scale (NEWS) [39] using 12 common destinations. Participants stated their usual mode of transportation and the minutes spent on one trip (for further details see [40]). Transport via bike or on foot was combined for active transport for the present study.
Statistical analyses
The statistical analyses only comprise data from the baseline survey. Descriptive analyses with absolute and relative frequencies were carried out for sex, marital status, having a partner, SES, self-rated health, BMI, items of the physical functioning score, and the categories of physical functioning. Means and standard deviations were calculated for age and physical functioning score. T-tests and chi-square tests were carried out to test for statistically significant differences between women and men regarding the physical functioning score and physical functioning items.
To test whether the association between sex and physical functioning can be explained by other individual factors, we standardized the data using the SAS procedure PROC STDIZE (SAS Institute, Cary (NC), USA), where \({z}_{i}\) is the standardized value of \({x}_{i}\) given \({(x}_{i}-\bar{x})/s\) with \(\bar{x}\) being the variables’ mean and \(s\) the standard deviation. Then, the following approach was pursued: Firstly, we grouped the individual factors into the following groups: vertical social factors, horizontal social factors, lifestyle factors, health indicators and (presence of) chronic diseases. Secondly, we performed ordinary least squares (OLS) regressions (complete case analyses) with physical functioning as dependent and the individual factors and age as independent variables to check whether the variable has an association with physical functioning. Thirdly, for each group of individual factors with at least one statistically significant association with physical functioning, we performed an OLS regression (complete cases) with physical functioning as dependent and the statistically significant individual factors of that group and sex and age as independent variables to check if and to what extent the association between sex and physical functioning can be explained by including these individual factors. For the latter, we (a) performed an OLS regression with physical functioning as dependent and sex as independent variable and saved the residuals, and (b) performed OLS regressions (complete cases) with the calculated residuals as dependent and the individual factors of each group and age as the independent variables. For this last step, we reported the explained variance of the residuals R2. For all other OLS regressions we reported the standardized beta β with 95%-confidence limits. The number of missing data for each individual factor is being displayed in Additional file 1. A sensitivity analysis excluding participants with missing data was conducted. To check violations of regression model assumptions, studentized residuals were calculated for each of the models. Except for the standardization of variables, all statistical analyses were conducted with SPSS 22.0 (IBM Corp. Armonk (NY), USA). The threshold for statistical significance was set at p < 0.05.
Results
The characteristics of the 2 141 participants of both the pilot study and the c-RCT are displayed in Table 1. 52.1% of the participants were female and the mean age was 69.8 ± 3.0 years. The majority was married and had a partner. Women were mostly in the lower SES quintiles, while most of the men pertained to the higher SES quintiles. Both women and men mostly rated their health as good. Most participants were either overweight or obese.
Detailed information on physical functioning is shown in Table 2. Women and men showed statistically significant differences in nine out of ten physical functioning items, with men perceiving fewer limitations than women. Only the item bathing or dressing oneself showed no significant differences. The majority of the participants had no limitations when walking one hundred metres, bathing or dressing oneself, climbing one flight of stairs, and walking several hundred metres. Vigorous activities was the item where most participants showed limitations. Most limitations were reported regarding carrying out vigorous activities. The distribution of physical functioning categories showed statistically significant sex differences, with men having higher scores than women.
Figure 1 shows the cumulative percent of participants reaching the different physical functioning scores. For example, 90.3% of women and 94.3% of men scored at least 50 points in physical functioning, while 35.3% of women and 49.6% of men scored at least 90 points. Linear regression showed a statistically significant negative association between physical functioning score and sex (β: -0.15, 95% CL: -0.19, -0.10).

Sex differences in physical functioning score, cumulative percentages
Table 3 shows the results of the analyses which individual factors were able to predict the sex-physical functioning association. Linear regression results showed that a higher physical functioning score was statistically significantly positively associated with having a higher SES, having a partner, higher total amount of PA, higher amount of active transport per week, and drinking alcohol daily. Statistically significant negative associations with physical functioning were seen for poor social support, living alone, all health indicators, and all chronic diseases. The association between sex and physical functioning remained statistically significant when adding SES, horizontal social factors (i.e., poor social support, having a partner, living alone), lifestyle factors, health indicators, and chronic diseases. All factors together were only able to predict 51% of the physical functioning-sex association, with health indicators (R2: 0.46) and the presence of chronic diseases (R2: 0.22) being the most influential factors.
Discussion
This study investigated sex differences among older adults regarding physical functioning and whether social, lifestyle, and health-related factors predicted these. Results showed sex differences regarding physical functioning, with men perceiving fewer limitations than women. The statistically significant negative associations between physical functioning and sex remained after adding vertical social factors, horizontal social factors, lifestyle factors, health indicators, and chronic diseases, both individually and all together in a model. The physical functioning-sex association depended mostly on health indicators (R2: 0.46), followed by chronic diseases (R2: 0.22).
Our results regarding sex differences in physical functioning are in line with previous research, which found women to perceive more limitations and therefore a lower physical functioning score than men [24, 25, 41, 42]. Sialino et al. found a difference in physical functioning scores of 6.55 points on average [25] and von Bonsdorff et al. [43] found a mean difference of 6.67 points, with women having lower scores. While our results showed a slightly smaller difference of 5.3 points, the findings strengthen the evidence of sex differences regarding physical functioning, especially for German older adults.
We found SES to be statistically significantly positively associated with physical functioning and negatively with sex. However, SES predicted only little of the association between sex and physical functioning (R2: 0.06). Previous research found contrasting results. While Hansen et al. [44] found a statistically significant negative association between social class and physical functioning, they found no differences regarding this association between men and women. Their study sample, however, consisted of middle-aged adults between 50 and 60 years and they measured physical functioning objectively with a physical performance test. Park et al. [27], on the other hand, found SES to have an impact on the sex differences in physical functioning among older adults, although they defined physical functioning as having limitations in ADL (i.e., basic needs such as eating, getting dressed, hygiene [45]) and instrumental ADL (IADL, i.e., shopping, doing housework, financial tasks [46]). Pajak et al. [47] also found SES to be statistically significantly positively associated with physical functioning in their study of the 45 to 65-year-old Polish population. They also used the Physical Functioning Scale from SF-36 and showed that the social gradient regarding physical functioning was larger in women than in men.
Our results indicated that health indicators have one of the highest influences on sex differences in physical functioning. Though the sex difference remained statistically significant, health indicators decreased the association most. These findings are in line with previous research. Kuh et al. [41] found women to have poorer overall health, which leads to weakness and therefore worse physical functioning. Although that study only included participants aged 53 years and were therefore younger than our study sample, these findings can be applied to older women as well, since muscle mass and strength tend to start declining around midlife [11, 48]. Further, previous research showed bodily pain to be an important determinant of physical functioning. In the study by Sialino et al. [25], the intensity of bodily pain was reported as more severe among women and was associated with decreased physical functioning. They further found BMI to be negatively associated with physical functioning, however, a higher BMI was more prevalent among men. These findings could also be observed in our results, indicating that overweight and obesity should be considered when trying to improve physical functioning among older adults, especially men.
When looking at chronic diseases, the association between sex and physical functioning decreased but remained statistically significant. Sialino and colleagues [25] found chronic diseases to be one of the strongest determinants associated with physical functioning. Additionally, previous studies have shown that physical functioning decreases with an increasing number of chronic diseases [49, 50]. Especially chronic diseases, that can lead to disabilities, predicted significantly more problems and functional limitations, such as Parkinson’s disease, arthritis, past stroke, and kidney stones in the study by Koukouli et al. [12]. While some evidence suggests that men display higher prevalences of chronic diseases [51], previous research found that women more often suffer from disabling and non-lethal diseases, such as arthritis or depression, which can lead to limitations in physical functioning [52, 53].
In our study, lifestyle factors and horizontal social factors, such as poor social support, having a partner, and living alone, did not explain sex differences regarding physical functioning. Previous studies have shown higher physical activity to be related to better physical functioning among older adults [42, 54]. While in the study by Mosallanez and colleagues [42] women were less physically active and showed lower levels of physical functioning than men, our results differed with women being more physically active, but still showing lower physical functioning scores. A factor explaining these differences might be that we used objective measures of PA and the Swedish study used subjective measures. In our study, accelerometers were worn on the non-dominant wrist, which can detect more upper body movement than other placements, like the hip [55]. In a previous publication, we found that the women devoted more time than the men in our study sample to household activities, which include a lot of upper body movements [40]. This could lead to higher PA levels of women. Furthermore, when interpreting the subjective measures used in the Swedish study misreporting of PA in questionnaires has to be taken into account. Dyrstad et al. [56] found that men tend to report higher PA levels than women.
Câmara et al. [57] found associations between social interactions and better physical performance while living alone was associated with worse physical functioning in men but not in women. Previous research has shown that loneliness is a risk factor for frailty [58] and disability [59], which both result in lower physical functioning. Our results also indicated that living alone is associated with worse physical functioning.
Other possible explanations for sex differences in physical functioning have been discussed in the literature. One main topic is biological causes for different physical functioning among older adults. It is assumed that menopause can lead to loss of muscle mass, which in turn can lead to lower muscle strength compared to men [48]. Another possible explanation is a difference in response behaviour. There have been discussions that women tend to report more disability and limitations than men because they perceive their physical functioning to be dysfunctional more frequently [60]. Additionally, it is assumed that men are more likely to neglect pain and disease, because of social conditioning [60]. However, previous studies have found women’s physical functioning to also be more limited than men’s when using objective measures, such as fitness tests [61, 62]. Furthermore, when discussing physical functioning of older adults, it is important to take into account, that physical functioning seems to be a dynamic process that can be improved even when limitations have been reported [63].
When comparing research on physical functioning, the different understandings of what this term includes and how it is being measured pose a problem. The most common measures are assessing limitations in ADL or IADL [27, 64,65,66], conducting various fitness tests [11, 54, 57, 61, 62], or, as we did in our study, using the SF-36 physical functioning scale [18, 24, 25, 67, 68]. While there is some overlap in the assessment of the different measures, they could come to varying conclusions.
This study has some strengths and limitations that need to be discussed. Firstly, the analyses were only implemented cross-sectionally; therefore, no statements regarding causation can be made. Furthermore, we do not have any information on the mentioned biological factors, such as menopause and the resulting loss of muscle mass, which could be the main factors for sex differences in physical functioning. Since most of the variables used were self-reported data, the results have to be interpreted with caution. Social desirability, over- and underreporting could potentially distort the results and should be taken into account. A selection bias is possible, since participants could choose in which parts of the study they wanted to partake in. Furthermore, the data used in this study stem from older adults residing in Bremen, Germany, which is why the results cannot be generalized for all older adults. However, the findings give an indication which factors play a role in sex differences regarding physical functioning. The strength of this study is that we included a wide range of different possible factors. In many studies that investigated physical functioning, sex differences were found, but they were not further explored. The studies that investigated sex differences mostly focused on one specific dimension, such as social factors, but only very few included a variety of possible factors.
Conclusion
This study found sex differences regarding physical functioning among older adults, with women having more limitations than men. The results showed that health factors, such as poor self-rated health, overweight or obesity, pains, and shortness of breath as well as chronic diseases can predict sex differences regarding physical functioning of older adults. Longitudinal research and a more distinct definition of physical functioning and its measures are needed to get a better understanding of sex differences in physical functioning.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- ADL:
-
Activities of daily living
- BMI:
-
Body mass index
- c-RCT:
-
Cluster-randomized controlled trial
- CL:
-
Confidence limits
- COPD:
-
Chronic obstructive pulmonary disease
- IADL:
-
Instrumental activities of daily living
- PA:
-
Physical activity
- SES:
-
Socioeconomic status
References
Guralnik JM, LaCroix AZ, Abbott RD, Berkman LF, Satterfield S, Evans DA, et al. Maintaining mobility in late life. I. demographic characteristics and chronic conditions. Am J Epidemiol. 1993;137(8):845–57.
Ayis S, Gooberman-Hill R, Bowling A, Ebrahim S. Predicting catastrophic decline in mobility among older people. Age Ageing. 2006;35(4):382–7.
Luppa M, Luck T, Weyerer S, König H-H, Brähler E, Riedel-Heller SG. Prediction of institutionalization in the elderly. A systematic review. Age Ageing. 2010;39(1):31–8.
Rechel B, Grundy E, Robine J-M, Cylus J, Mackenbach JP, Knai C, et al. Ageing in the European union. Lancet. 2013;381(9874):1312–22.
Rudnicka E, Napierała P, Podfigurna A, Męczekalski B, Smolarczyk R, Grymowicz M. The world health organization (WHO) approach to healthy ageing. Maturitas. 2020;139:6–11.
Bjerk M, Brovold T, Skelton DA, Bergland A. Associations between health-related quality of life, physical function and fear of falling in older fallers receiving home care. BMC Geriatr. 2018;18(1):253.
Fisher S, Ottenbacher KJ, Goodwin JS, Graham JE, Ostir GV. Short physical performance battery in hospitalized older adults. Aging Clin Exp Res. 2009;21(6):445–52.
Penninx BW, Ferrucci L, Leveille SG, Rantanen T, Pahor M, Guralnik JM. Lower extremity performance in nondisabled older persons as a predictor of subsequent hospitalization. J Gerontol Biol Sci Med Sci. 2000;55(11):M691–7.
Minneci C, Mello AM, Mossello E, Baldasseroni S, Macchi L, Cipolletti S, et al. Comparative study of four physical performance measures as predictors of death, incident disability, and falls in unselected older persons: the insufficienza Cardiaca Negli Anziani Residenti a Dicomano Study. J Am Geriatr Soc. 2015;63(1):136–41.
Veronese N, Stubbs B, Fontana L, Trevisan C, Bolzetta F, Rui M, de, et al. A comparison of objective physical performance tests and future mortality in the elderly people. J Gerontol Biol Sci Med Sci. 2017;72(3):362–8.
Okabe T, Suzuki M, Goto H, Iso N, Cho K, Hirata K et al. Sex differences in age-related physical changes among Community-Dwelling adults. J Clin Med 2021; 10(20).
Koukouli S, Vlachonikolis IG, Philalithis A. Socio-demographic factors and self-reported functional status: the significance of social support. BMC Health Serv Res. 2002;2(1):20.
Noppert GA, Brown CS, Chanti-Ketterl M, Hall KS, Newby LK, Cohen HJ, et al. The impact of multiple dimensions of socioeconomic status on physical functioning across the life course. Gerontol Geriatr Med. 2018;4:2333721418794021.
Jyväkorpi SK, Urtamo A, Pitkälä KH, Strandberg TE, Nutrition. Daily walking and resilience are Associated with physical function in the oldest old men. J Nutr Health Aging. 2018;22(10):1176–82.
Kostadinovic M, Nikolic D, Petronic I, Cirovic D, Grajic M, Santric Milicevic M. Sociodemographic predictors of physical functioning in the elderly: a national health survey. Int J Environ Res Public Health 2018; 16(1).
Hu Y, Malyutina S, Pikhart H, Peasey A, Holmes MV, Hubacek J, et al. The relationship between body Mass Index and 10-Year trajectories of physical functioning in middle-aged and older russians: prospective results of the Russian HAPIEE study. J Nutr Health Aging. 2017;21(4):381–8.
Imamura K, Kamide N, Ando M, Sato H, Sakamoto M, Shiba Y. Social isolation is associated with future decline of physical performance in community-dwelling older adults: a 1-year longitudinal study. Aging Clin Exp Res. 2022;34(6):1391–8.
Peeters G, Beard JR, Deeg DJH, Tooth LR, Brown WJ, Dobson AJ. Longitudinal associations between lifestyle, socio-economic position and physical functioning in women at different life stages. Eur J Ageing. 2019;16(2):167–79.
Robert Koch-Institut. [Health in Germany. Federal Health Monitoring.] Gemeinsam getragen von RKI und Destatis. Berlin. 2015 [cited 2023 Sep 14]. Available from: https://www.rki.de/DE/Content/Gesundheitsmonitoring/Gesundheitsberichterstattung/GesInDtld/gesundheit_in_deutschland_2015.pdf?__blob=publicationFile.
Gallagher D, Visser M, de Meersman RE, Sepúlveda D, Baumgartner RN, Pierson RN, et al. Appendicular skeletal muscle mass: effects of age, gender, and ethnicity. J Appl Physiol. 1997;83(1):229–39.
Mitchell WK, Williams J, Atherton P, Larvin M, Lund J, Narici M. Sarcopenia, dynapenia, and the impact of advancing age on human skeletal muscle size and strength; a quantitative review. Front Physiol. 2012;3:260.
Hansen J, Hansen H, Nilsson C, Ekholm O, Molsted S. Association between educational level and self-reported musculoskeletal pain and physical functioning in Danes 60–70 years old from 2010 to 2017: a longitudinal analysis of trends over time on data from the Danish health and morbidity survey. BMJ Open. 2023;13(11):e073523.
Dugan SA, Gabriel KP, Lange-Maia BS, Karvonen-Gutierrez C. Physical activity and physical function: moving and aging. Obstet Gynecol Clin North Am. 2018;45(4):723–36.
Sekine M, Chandola T, Martikainen P, Marmot M, Kagamimori S. Sex differences in physical and mental functioning of Japanese civil servants: Explanations from work and family characteristics. Soc Sci Med. 2010; 71(12):2091–9. Available from: URL: https://www.sciencedirect.com/science/article/pii/S0277953610006957.
Sialino LD, Picavet HSJ, Wijnhoven HAH, Loyen A, Verschuren WMM, Visser M, et al. Exploring the difference between men and women in physical functioning: how do sociodemographic, lifestyle- and health-related determinants contribute? BMC Geriatr. 2022;22(1):610.
Verbrugge LM. Gender and health: an update on hypotheses and evidence. J Health Soc Behav. 1985;26(3):156.
Park S-M, Jang S-N, Kim D-H. Gender differences as factors in successful ageing: a focus on socioeconomic status. J Biosoc Sci. 2010;42(1):99–111.
Avis NE, Colvin A, Bromberger JT, Hess R, Matthews KA, Ory M, et al. Change in health-related quality of life over the menopausal transition in a multiethnic cohort of middle-aged women: study of women’s Health across the Nation. Menopause. 2009;16(5):860–9.
Louie GH, Ward MM. Sex disparities in self-reported physical functioning: true differences, reporting bias, or incomplete adjustment for confounding? J Am Geriatr Soc. 2010;58(6):1117–22.
Forberger S, Bammann K, Bauer J, Boll S, Bolte G, Brand T et al. How to Tackle Key challenges in the Promotion of Physical Activity among older adults (65+): the AEQUIPA Network Approach. Int J Environ Res Public Health 2017; 14(4).
Bammann K, Drell C, Lübs LL, Stalling I. Cluster-randomised trial on participatory community-based outdoor physical activity promotion programs in adults aged 65–75 years in Germany: protocol of the OUTDOOR ACTIVE intervention trial. BMC Public Health. 2018;18(1):1197.
Stalling I, Albrecht BM, Foettinger L, Recke C, Bammann K. Associations between socioeconomic status and physical activity among older adults: cross-sectional results from the OUTDOOR ACTIVE study. BMC Geriatr. 2022;22(1):396.
Dalgard OS, Dowrick C, Lehtinen V, Vazquez-Barquero JL, Casey P, Wilkinson G, et al. Negative life events, social support and gender difference in depression: a multinational community survey with data from the ODIN study. Soc Psychiatry Psychiatr Epidemiol. 2006;41(6):444–51.
Robert Koch-Institut. [Health questionnaire 65 + years. German Health Interview and Examination Survey]; 2009. [cited 2022 Feb 23].
Ware JE, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. conceptual framework and item selection. Med Care. 1992;30(6):473–83.
World Health Organization. Obesity: preventing and managing the global epidemic. Report of a WHO consultation; 2000.
Ndahimana D, Kim E-K. Measurement methods for physical activity and energy expenditure: a review. Clin Nutr Res. 2017;6(2):68–80.
Choi L, Liu Z, Matthews CE, Buchowski MS. Validation of accelerometer wear and nonwear time classification algorithm. Med Sci Sports Exerc. 2011;43(2):357–64.
Saelens BE, Sallis JF, Black JB, Chen D. Neighborhood-based differences in physical activity: an environment scale evaluation. Am J Public Health. 2003;93(9):1552–8.
Stalling I, Albrecht BM, Doerwald F, Bammann K. Time allocation to active domains, physical activity, and health indicators in older adults: cross-sectional results from the OUTDOOR ACTIVE study. BMC Public Health. 2020;20(1):1580.
Kuh D, Bassey EJ, Butterworth S, Hardy R, Wadsworth MEJ. Grip strength, postural control, and functional leg power in a representative cohort of British men and women: associations with physical activity, health status, and socioeconomic conditions. J Gerontol Biol Sci Med Sci. 2005;60(2):224–31.
Mosallanezhad Z, Hörder H, Salavati M, Nilsson-Wikmar L, Frändin K. Physical activity and physical functioning in Swedish and Iranian 75-year-olds - a comparison. Arch Gerontol Geriatr. 2012;55(2):422–30.
von Bonsdorff MB, Rantanen T, Sipilä S, Salonen MK, Kajantie E, Osmond C, et al. Birth size and childhood growth as determinants of physical functioning in older age: the Helsinki Birth Cohort Study. Am J Epidemiol. 2011;174(12):1336–44.
Hansen ÅM, Andersen LL, Skotte J, Christensen U, Mortensen OS, Molbo D, et al. Social class differences in physical functions in middle-aged men and women. J Aging Health. 2014;26(1):88–105.
Katz S, Ford AB, Moskowitz RW, Jackson BA, Jaffe MW. Studies of illness in the aged: the Index of ADL: a standardized measure of biological and psychosocial function. JAMA. 1963;185:914–9.
Lawton MP, Brody EM. Assessment of Older people: self-maintaining and instrumental activities of Daily Living. Gerontologist. 1969;9(3 Part 1):179–86.
Pająk A, Polak M, Kozela M, Doryńska A, Bobak M. Trajectories in physical functioning at older age in relation to childhood and adulthood SES and social mobility: a population-based cohort study. Front Public Health. 2023;11:1228920.
Danneskiold-Samsøe B, Bartels EM, Bülow PM, Lund H, Stockmarr A, Holm CC, et al. Isokinetic and isometric muscle strength in a healthy population with special reference to age and gender. Acta Physiol. 2009;197(Suppl 673):1–68.
Stenholm S, Westerlund H, Salo P, Hyde M, Pentti J, Head J, et al. Age-related trajectories of physical functioning in work and retirement: the role of sociodemographic factors, lifestyle and disease. J Epidemiol Community Health. 2014;68(6):503–9.
Bleijenberg N, Zuithoff NPA, Smith AK, de Wit NJ, Schuurmans MJ. Disability in the Individual ADL, IADL, and mobility among older adults: a prospective cohort study. J Nutr Health Aging. 2017;21(8):897–903.
Heidemann C, Scheidt-Nave C, Beyer A-K, Baumert J, Thamm R, Maier B et al. Gesundheitliche Lage von Erwachsenen in Deutschland – Ergebnisse zu ausgewählten Indikatoren der Studie GEDA 2019/2020-EHIS; 2021.
Avedano MMJ. Changes in Physical Health among older europeans. In: Boersch-Supan A, Alcser KH, editors. Health, ageing and retirement in Europe: first results from the survey of health, ageing and retirement in Europe (2004–2007): starting the longitudinal dimension. Mannheim: MEA; 2008. pp. 118–24.
Crimmins EM, Kim JK, Solé-Auró A. Gender differences in health: results from SHARE, ELSA and HRS. Eur J Public Health. 2011;21(1):81–91.
Veen J, Edholm P, Rodriguez-Zamora L, Folkesson M, Kadi F, Nilsson A. Adherence to the physical activity guideline beyond the recommended minimum weekly amount: impacts on indicators of physical function in older adults. Front Public Health. 2023;11:1197025.
Sun F, Norman IJ, While AE. Physical activity in older people: a systematic review. BMC Public Health. 2013;13:449.
Dyrstad SM, Hansen BH, Holme IM, Anderssen SA. Comparison of self-reported versus accelerometer-measured physical activity. Med Sci Sports Exerc. 2014;46(1):99–106.
Câmara SMA, Falvey JR, Orwig D, Gruber-Baldini AL, Auais M, Feng Z et al. Associations between living alone, social interactions, and physical performance differ by sex: results from the Baltimore Hip studies. J Am Geriatr Soc 2023.
Gale CR, Westbury L, Cooper C. Social isolation and loneliness as risk factors for the progression of frailty: the English Longitudinal Study of Ageing. Age Ageing. 2018;47(3):392–7.
Cabello M, Caballero FF, Chatterji S, Cieza A, Ayuso-Mateos JL. Risk factors for incidence and persistence of disability in chronic major depression and alcohol use disorders: longitudinal analyses of a population-based study. Health Qual Life Outcomes. 2014;12:186.
Mauvais-Jarvis F, Bairey Merz N, Barnes PJ, Brinton RD, Carrero J-J, DeMeo DL et al. Sex and gender: modifiers of health, disease, and medicine. Lancet. 2020; 396(10250):565–82. Available from: URL: https://pubmed.ncbi.nlm.nih.gov/32828189/.
Wiley E, Noguchi KS, Moncion K, Stratford PW, Tang A. Sex differences in functional capacity in older adults with stroke: an Analysis of Data from the National Health and Aging trends Study. Phys Ther 2022; 102(8).
Xu F, Cohen SA, Greaney ML, Earp JE, Delmonico MJ. Longitudinal sex-specific physical function trends by Age, Race/Ethnicity, and Weight Status. J Am Geriatr Soc. 2020;68(10):2270–8.
Ylitalo KR, Karvonen-Gutierrez CA, Fitzgerald N, Zheng H, Sternfeld B, El Khoudary SR et al. Relationship of race-ethnicity, body mass index, and economic strain with longitudinal self-report of physical functioning: the Study of Women’s Health Across the Nation. Ann Epidemiol. 2013; 23(7):401–8. Available from: URL: https://www.sciencedirect.com/science/article/pii/S1047279713000987.
Toyama M, Fuller HR, Owino J. Longitudinal Implications of Social Integration for age and gender differences in late-life physical functioning. Int J Aging Hum Dev. 2022;94(2):169–92.
Lai ETC, Ho HC, Ho SC, Woo J, Socioeconomic, Status. Physical functioning and mortality: results from a Cohort Study of older adults in Hong Kong. J Am Med Dir Assoc. 2022;23(5):858–e8645.
Yang L, Konttinen H, Martikainen P, Silventoinen K. Socioeconomic status and physical functioning: a longitudinal study of older Chinese people. J Gerontol B Psychol Sci Soc Sci. 2018;73(7):1315–29.
Ylitalo KR, Karvonen-Gutierrez CA, Sternfeld B, Pettee Gabriel K. Association of Physical Activity and physical functioning phenotypes with fall risk among women. J Aging Health. 2021;33(5–6):409–17.
van Dyck D, Cardon G, Deforche B, de Bourdeaudhuij I. The contribution of former work-related activity levels to predict physical activity and sedentary time during early retirement: moderating role of educational level and physical functioning. PLoS ONE. 2015;10(3):e0122522.
Acknowledgements
The authors would like to thank all participants of the OUTDOOR ACTIVE study.
Funding
Open Access funding enabled and organized by Projekt DEAL. The OUTDOOR ACTIVE study is funded by the German Federal Ministry of Education and Research (BMBF; grant numbers 01EL1422B and 01EL1822B). The funder had no role in the design of the study, data collection, or analysis, interpretation of data and in writing the manuscript. Open Access funding enabled and organized by the DEAL agreement.
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
IS performed statistical analyses and drafted the manuscript. KB contributed to the conception and design of the study as well as statistical analyses. KB and MG critically revised and reviewed the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The OUTDOOR ACTIVE study (German Clinical Trials Register DRKS00015117) was approved by the ethics committee of the University of Bremen (protocol codes No: 2018-06 and 2015−0910). We confirm that all methods were performed in accordance with relevant guidelines and regulations under ethical approval. All participants provided written informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Stalling, I., Gruber, M. & Bammann, K. Sex differences in physical functioning among older adults: cross-sectional results from the OUTDOOR ACTIVE study. BMC Public Health 24, 1766 (2024). https://doi.org/10.1186/s12889-024-19218-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-024-19218-x