
Abstract
Background
Physical activity (PA) in older people is critically important in the prevention of disease, maintenance of independence and improvement of quality of life. Little is known about the physical activity of the older adults or their compliance with current physical activity guidelines.
Methods
A systematic literature search of the published literature was conducted. Included were published reports of original research that independently reported: the PA level of non-institutional older adults (aged 60 years and over); and the proportion of older adults in the different samples who met PA recommendations or guidelines. The review was restricted to studies published since 2000 to provide a current picture of older adults’ PA levels.
Results
Fifty three papers were included in the review. The percentage of older adults meeting recommended physical activity ranged from 2.4 – 83.0% across the studies. Definitions of “recommended” physical activity in older adults varied across the studies as did approaches to measurement which posed methodological challenges to data analysis. Older age groups were less likely than the reference group to be regularly active, and women were less likely than men to achieve regular physical activity, especially leisure time physical activity, when measured by both subjective and objective criteria.
Conclusion
The review highlights the need for studies which recruit representative random samples of community based older people and employ validated measurement methods consistently to enable comparison of PA levels over time and between countries.
Similar content being viewed by others

Background
Regular physical activity (PA) can bring significant health benefits to people of all ages and the need for PA does not end in later life with evidence increasingly indicating that PA can extend years of active independent living, reduce disability and improve the quality of life for older people [1]. Indeed a large scale longitudinal 8 year study found that every additional 15 minutes of daily PA up to 100 minutes per day resulted in a further 4% decrease in mortality from any cause [2]. Increasing PA will help minimise the burden on health and social care through enabling healthy ageing [3, 4].
There is no known review of PA among older people and it is not known whether active older people comply with recommended PA levels. Understanding the extent of PA will provide a global perspective of PA among older people within the context of an increasing desire to promote PA goals across all age groups. The aim of this review was to establish global levels of PA among older people as reported in the published literature. Establishing PA prevalence in older community dwelling people provides a baseline against which changes in PA can be measured, international comparisons drawn and the success or otherwise of public health interventions to increase PA evaluated.
Methods
Search strategy
The following methods were used to locate relevant published studies from January 2000 – 11 April 2011. Electronic searches of computerized databases were carried out on English language databases (The Cochrane Library, PubMed, MEDLINE, EMBASE, CINAHL, PsycINFO, British Nursing Index (BNI) and Scopus) and Chinese databases: Chinese Biomedical, VIP Chinese Science Journals and WANFANG DATA. Keyword combinations for electronic database searches are listed in Table 1. The search was limited to the English and Chinese languages.
Selection criteria
Papers were reviewed if they met the following criteria: (1) original research; (2) independently reported the PA level of non-institutional older people (adults aged 60 years and over); (3) reported the proportion of any of PA recommendation or guidelines achieved by the sample.
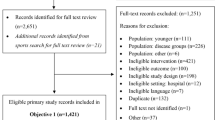
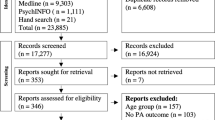
No attempt was made to access unpublished studies or other ‘grey’ literature. The study selection process is set out in Figure 1.

Literature identification process.
Data extraction and appraisal
All authors devised the research strategy. Initial screening was undertaken by one researcher (FS) and then checked by another (AEW). Disagreements about inclusion were discussed until agreement was reached. One researcher (FS) extracted the following data from the selected studies: country of study, study sample, measurements, recommendations and main results. Another researcher (AEW) verified the extracted data and made corrections where necessary. Disagreements were resolved by reference to the third researcher (IJN). All three researchers contributed to the synthesis of the data.
PA recommendations or guidelines
Definitions of “recommended” PA in older adults varied across the studies with some studies employing two or more guidelines. These guidelines are summarized in Table 2. The minimum recommended PA level in the guidelines in most studies was 150 minutes of moderate or vigorous PA per week and we adopted this standard as the desired PA level for the purpose of this review. We categorised the selected studies according to their underpinning PA guidelines, and identified studies as falling into one of two groups according to the detail provided by the study authors on the guidelines followed. Twenty six studies which stated only the total amount of PA per week were classified within the ‘less detailed guideline group’. Studies which stated the weekly frequency and daily dosage towards the total amount of weekly PA were classified as being in the ‘detailed guideline group’. According to the Physical Activity Guideline Advisory Committee’s report [5], detailed guidelines, such as 1995 CDC/ACSM guideline is too specific. In other words, the existing scientific evidence cannot distinguish the health benefits of 30 minutes of PA on 5 days a week from those gained through 50 minutes of PA on 3 days a week.
Results and discussion
An overview of selected papers
A total of 53 papers met the inclusion criteria. The main findings of the selected studies are reported in Tables 3 and 4.1
Most of the studies were conducted in the United States and Australia (USA n=19; Australia n=10; UK n=5; Brazil n=4; China n=4; Canada n=4; New Zealand n=1; Colombia n=1; South Africa n=1; Greece and Cyprus n=1; Cyprus n=1; Sweden n=1; Switzerland n=1). Forty nine papers reported cross-sectional studies and four reported longitudinal studies. The sample sizes ranged from 54 – 43,259. The number of studies conducted each year over the search period was not constant (1990–1994, n=2; 1995–1999, n=12; 2000–2004, n=32; 2005–2009, n=18; 2010–2011, n=2) with more than half being conducted between 2000 and 2004.
Forty seven studies measured PA intensity, duration, and frequency using subjective measures (interview or self-reported questionnaires) and six reported objective data gathered using an accelerometer. Two studies compared subjective and objective data measurements. While 39 studies recorded PA taken in periods of 10 minutes or more, other studies recorded all PA.
Physical activity comprises leisure-time PA, occupational PA, household PA and transportation PA. Leisure-time PA (LTPA) was most often measured and compared to the criterion for meeting PA recommendations. However, occupational, household and transportation PA were gathered in some studies. PA volume was calculated differently across the studies including: total metabolic equivalents (METs), minutes of weekly PA; minutes of participation in and frequency of PA during the week; kilocalories expended per kilogram of weight per day; and time in moderate to vigorous PA from accelerometers. To calculate minutes of weekly moderate to vigorous PA, some authors summed the duration of moderate and vigorous PA (MPA+VPA) while others doubled the time of vigorous PA because of its higher intensity (MPA+2VPA). The definition of moderate and vigorous PA also varied across the studies. For instance, the minimum cut off of moderate PA varied from 3 MET, 3.3 MET to 4 MET across the studies. Given the variety of methods of data collection and calculation of PA level, a meta-analysis was not attempted.
Levels of PA within recommendations or guidelines
Thirty two studies adopted the more detailed PA guidelines while 26 studies were in the less detailed group with some studies employing two or more guidelines. Although most of the PA guidelines stated the total PA amount which should be accumulated in bouts of at least 10 minutes, 14 of the 53 studies recorded all moderate or vigorous PA (see Table 2).
General PA prevalence in older adults
Tables 3 and 4 present a synopsis of the findings relating to older people’s PA levels from each country. Across the 53 papers, the percentage of older adults meeting the guidelines ranged from 2.4% [55] to 83% [49] with most studies reporting that 20-60% of the samples met the guideline. When LTPA was measured, 20 studies excluded household work with reported PA prevalence ranging from 6.23% [58] to 67.51 % [27], while 14 included household work with reported PA prevalence of 10.86% [31] to 66.7% [16]. Seventeen studies measured all domains of PA (including occupational, household, transportation and recreational PA) with reported PA prevalence of 11.67% [31] to 77.22% [51], and two studies reported that 31.7% [13] and 62.4% [45] of older people achieved sufficient PA through walking. In six papers PA prevalence was reported by age group, gender group, or residential area group (rural versus urban), but not for the sample overall.
Self-reported PA
In 48 subjectively measured PA studies, 29 studies adopted the more detailed PA guidelines and 21 studies adopted the less detailed PA guidelines (5 studies adopted 2 criteria). Studies that employed the more detailed guidelines reported PA prevalence ranging from 6.2% in the Health Survey for England [38] to 82.6% in an urban Chinese sample [47]. Using the less detailed guidelines (criteria), sufficient PA in the other studies increased from 21.3 % [34] to 83.0% [49] in a small older female sample.
Those studies that accumulated PA data by 10 minutes bouts reported a relatively lower PA prevalence. The two studies which only included PA data of more than 30 minute sessions reported the lowest PA prevalence (10.9% [30]; 6.23% [58]) across all the subjectively measured PA studies.
Objectively measured PA
Six studies used accelerometers and reported extractable data (i.e. proportion of the sample meeting the criterion of sufficient PA rather than measures of central tendency). The actigraph accelerometer was used in five studies and Actical in one study. When measured against the less detailed guidelines, the lowest prevalence (1.84%) was reported by Davis and Fox [3] based on an European sample and the highest was 17.2% from a US national survey, NHANES 2005–2006 [43]. Applying the more detailed guidelines, Davis and Fox [3] found nobody achieved sufficient PA and Colley [57] reported the highest proportion of 4.5% in this group with the exception of Hurtig-Wennlof et al.’s [51] exceptional finding of 87.04%.
However, there was a difference between the studies using self-report compared to the objective measurement of PA. In our review, two studies compared the subjective and objective data. Tucker et al.’s [43] analysis of the NHANES 2005–2006 data found that the sufficiently active group proportion defined by accelerometer measurement was 7.25% and 17.24% (using different guidelines); this increased to 54.2% when measured by questionnaire. Hurtig-Wennlof et al.’s Swedish study [51] reported a 87.04% objectively measured PA prevalence which was higher than the self-reported IPAQ data of 72.2%.
Gender differences in PA
Twenty two studies reported the recommended PA prevalence in males and females separately. In general, men’s PA levels were higher than women’s. In the self-reported data, gender differences of PA ranged from 0.8% [30] to 21.4% [15], while the differences measured by accerlerometer were significantly lower (0.2% and 1.5%). However, we noticed that in the self-reported total PA, increased participation in PA by women exceeded that of men in three studies [40, 53].
Residential differences in PA
Two Chinese papers reported the PA prevalence by place of residence and reported different results. Muntner et al. [22] reported sufficient all domain PA prevalence among 52.7% of their rural and 9.8% of their urban older people samples using the US CDC 1995 criterion from the InterASIAN Study. However, Xu et al. [47] reported that Guangdong province urban residents were more active than rural residents, with 82.6% of the urban and 60.9% of the rural samples attaining the HP 2010 goals measured by GPAQ.
PA prevalence across age groups
Eighteen studies measured PA subjectively and two studies measured PA objectively across different age groups, however, the majority divided the samples into two age groups and reported that the older old were more sedentary than the younger old. Only five studies divided the group by relatively narrow age bands. Patterns of participation in PA decreased progressively with age for both men and women although there was variation across the studies. In McGuire et al.’s study [36] PA declined from 23.0% in the 65–69 year group to 13.6% in 85+ year group but in Mummery et al.’s study [35], the difference between the 60–64 year group and 80+ year group was 24.2%. There was an unexpected rise in the 70–74 year age group in the Sims et al.’s [42] study although the general trends decreased with age. Although Hamdorf et al. [12] did not report the detailed percentage for each age group, we can see the same gradually declining trend from 50.8% in the 60–64 year age group to 15.4% in 85+ year age group in Figure 2.

Physical activity prevalence across age groups.
PA prevalence trends over time
A crucial aspect of investigating trends over time is the comparability of methods. Differences in instruments, cut-off points, PA definitions and domains of activity investigated posed significant challenges to our review. Although nine studies reported the results of the BRFSS, not all the studies included national representative samples making it difficult to assess trends. Therefore, we only included the results of longitudinal studies or the findings from the same surveillance evaluated by the same criterion to establish the trend from seven studies. In Australia between 1990–2000 the proportion LTPA of older people aged 60 years and over meeting the PA guideline decreased from 28% to 25.8% in Merom et al.’s report [13] while the NSW Population Health Survey [11] detected a small rise in the 65 + year age group from 36.2% in 1998 to 39.8% in 2005 with a dip to 34.0% in 2003. The trend of regular walking [13] was similar to Chau et al.’s [11] report. The USCDC compared the BRFSS data in 2001 and 2005 and reported that the US’ older population was more active, with a rising prevalence of 43.1% to 44.5% in men and 32.2% to 36.3% in women [21]. Another paper using the BRFSS 2001 and BRFSS 2007 reported the same overall trend from 37.5% to 39.3% [48]. Conversely, Knuth et al. [26] reported a clear drop in PA prevalence between 2002 and 2007 in Brazil. In 2002, the proportions of older people reaching the PAGA 2008 guideline were 56.2% and 35.3% in the 60–69 year and 70+ year age groups respectively and decreased to 42.7% and 23.7% in 2007.
Discussion
Demographic differences in PA prevalence
One of the challenges facing the development of disease prevention programmes is the lack of reliable data for PA levels and trends [59] and the data for PA levels in older people is no exception. Generally within the included studies, the older old age groups were less likely than those of younger age to be regularly active, and women were less likely than men to achieve regular PA, especially in LTPA across both the subjectively and objectively measured PA studies regardless of the PA guidelines adopted. The decline in PA with age may be the most consistent finding in PA epidemiology [60, 61] with the higher PA prevalence among males echoing the findings of previous studies [62] which may reflect increasing disability with age and cultural norms across the genders. However, one Australian study [42] found that the decline of LTPA across the age groups was not consistent with LTPA peaking in the 70–74 year group. Additionally three studies reported that women were more active than men in relation to total PA [25, 40, 53]. This pattern also appeared in other studies [63] which may reflect the inclusion of household activities and other non-leisure, non-sport activities [53] in the total PA, which, in many cases, are largely specific to women. However, this was not a consistent finding across the included studies regardless of the guidelines category, indicating the need to quantify household activities accurately to enable comparisons across genders.
PA trends by country and over time
In our review, there was a slightly increasing trend towards recommended PA levels in older people in Australia and the US over the last 10 years but a decrease in Brazil. Studies of time trends in PA have been conducted mostly in developed countries and their results indicate that LTPA levels appear to be increasing [31, 34, 64, 65]. Nevertheless, the data indicate that substantial numbers of older adults do not engage in sufficient PA to promote their health and there is considerable variation in the levels of PA reported across countries. Further, we found little data on time trends in PA in developing countries which was echoed in a recent systematic review [66]. However, the decline in PA in Brazil [26] is perhaps indicative of changes in occupational PA with the emergence of increasing sedentary work in developing countries which will present a future public health challenge especially when combined with dietary changes. Similarly Hallal et al. have also highlighted the lower proportions of adults who are physically active in south east Asia [59].
The difference between objectively and subjectively measured PA prevalence
The only two studies comparing self-reported PA to accelerometer measured PA in our review yielded contradictory results [43, 51] with Tucker et al.’s [43] findings being consistent with the majority of other similar studies [67]. It is likely that the subjective PA studies reflect social desirability, recall bias and that there is underestimation of PA using objective measurement; PA monitors are worn typically on the hip which means that they do not accurately assess upper body activities or account for movements that require extra effort, such as walking uphill or carrying loads. Hurtig-Wennlof et al.’s [51] contradictory findings were probably caused by the lower cut-off point of MPA at 760 counts per minute (contrasting with about 2000 counts/min in the other studies) and the inclusion of PA under 10 minute bouts. This highlights the need for well designed studies using objectively measured PA to generate the evidence base for public health initiatives.
Review limitations
Limitations of this review arise from the discrepancies and inconsistencies in instrumentation, PA type measured, guidelines or recommendations adopted by different researchers, algorithms, sample frames and other confounding factors. These made it difficult to make full use of the extracted data and impossible to compare the PA prevalence between different regions/countries or assess PA trends with certainty.
Conclusion
Dramatic global population ageing has brought new demands to improve older people’s health by adding “quality” to their extended lives [68]. The review was undertaken against the background of the WHO recommendations on PA for adults aged 65 years and older [69]. Despite these recommendations physical inactivity is an increasing global health burden [70] with PA surveillance emerging as one of the priorities of global public health for the development of effective non-communicable disease prevention programmes [59]. International efforts to increase PA have been reported within the adult or youth populations [38, 66, 71–73]. However, PA levels of older adults have attracted less interest so there are limited data regarding the prevalence of various types of PA in older adults and the proportion of older people whose PA meets PA guidelines. This review is the first of its kind and revealed many methodological challenges to data analysis across the selected studies. Robust studies which recruit representative random samples and consistently employ validated measurement instruments are needed to enable comparisons in PA levels to be drawn over time and between countries. More evidence of PA levels amongst older people is needed to inform public health strategies which could extend the health and quality of life of people into old age.
Authors’ information
FS is a doctoral student. AEW and IJN are established health service researchers. This review was conducted to understand the prevalence and measurement of physical activity in older people.
Abbreviations
- AAS:
-
Active Australia Survey
- BRFSS:
-
Behavioural Risk Factor Surveillance System
- CDC-ACSM:
-
Centers for Disease Control and Prevention and the American College of Sports Medicine
- CHMS:
-
Canadian Health Measures Survey
- CCHS:
-
Canadian Community Health Survey
- GPAQ:
-
Global Physical Activity Questionnaire
- IPAQ:
-
International Physical Activity Questionnaire
- LTPA:
-
Leisure-time physical activity
- MET:
-
Total metabolic equivalents
- MPA:
-
Moderate physical activity
- NHANES:
-
National Health and Nutritional Examination Survey
- NHIS:
-
National Health Interview Survey
- PA:
-
Physical activity
- PAGA:
-
Physical Activity Guidelines for Americans
- SGR:
-
US Surgeon General’s Report
- VPA:
-
Vigorous physical activity.
References
Division of Ageing and Seniors: Physical activity and older adults from Canada. 2011, Available at: [http://www.phac-aspc.gc.ca/seniors-aines/index-eng.php] Accessed Aug 1, 2011
Wen CP, Wai JP, Tsai MK, Yang YC, Cheng TY, Lee MC, Chan HT, Tsao CK, Tsai SP, Wu X: Minimum amount of physical activity for reduced mortality and extended life expectancy: a prospective cohort study. Lancet. 2011, 378: 1244-1253. 10.1016/S0140-6736(11)60749-6.
Davis MG, Fox KR: Physical activity patterns assessed by accelerometry in older people. Eur J Appl Physiol. 2007, 100: 581-589. 10.1007/s00421-006-0320-8.
Chodzko-zajko WJ, Proctor DN, Fiatarone Singh MA, Minson CT, Nigg CR, Salem GJ, Sinner JS: American College of Sports Medicine position stand. Exercise and physical activity for older adults. Med Sci Sports Exer. 2009, 41: 1510-1530. 10.1249/MSS.0b013e3181a0c95c.
U.S. Department of Health and Human Services: Physical Activity Guidelines for Americans. 2008, Available at: [http://www.health.gov/paguidelines/] Accessed Sep 11, 2011
Merom D, Phongsavan P, Chey T, Bauman A: Australian Bureau of Statistics.Long-term changes in leisure time walking, moderate and vigorous exercise: Were they influenced by the national physical activity guidelines. J Sci Med Sport. 2006, 9: 199-208. 10.1016/j.jsams.2006.03.021.
Jerome GJ, Glass TA, Mielke M, Xue QL, Andersen RE, Fried LP: Physical activity participation by presence and type of functional deficits inolder women: the Women's Health and Ageing Studies. J Gerontol A Biol Sci Med Sci. 2006, 61A: 1171-6.
Brownson RC, Jones DA, Pratt M, Blanton C, Heath GW: Measuring physical activity with the behavioral risk factor surveillance system. Med Sci Sports Exerc. 2000, 32 (11): 1913-8. 10.1097/00005768-200011000-00015.
Brach JS, Simonsick EM, Kritchevsky S, Yaffe K, Newman AB: Health gency and Body Composition Study Research Group. The association between physical function and lifestyle activity and exercise in the health, ageing and body composition study. J Am Geriatr Soc. 2004, 52: 502-509. 10.1111/j.1532-5415.2004.52154.x.
Phongsavan P, Merom D, Marshall A, Bauman A: Estimating physical activity level: the role of domestic activities. J Epidemiol Community Health. 2004, 58: 466-467. 10.1136/jech.2003.012096.
Chau J, Smith BJ, Bauman A, Merom D, Eyeson-Annan M, Chey T, Farrell L: Recent trends in physical activity in New South Wales. Is the tide of inactivity turning. Aust New Zealand Health. 2008, 32: 82-85. 10.1111/j.1753-6405.2008.00170.x.
Hammdorf P, Starr G, Williams MA: A survey of physical-activity levels and functional capacity in older adults in South Australia. J Aging Phys Act. 2002, 10: 281-289.
Merom D, Chey T, Chau J, Smith BJ, Barr M, Bauman AE: Are messages about lifestyle walking being heard? Trends in walking for all purposes in New South Wales (NSW), Australia. Prev Med. 2009, 48: 341-344. 10.1016/j.ypmed.2009.02.010.
Heesch KC, Brown WJ: Do walking and leisure-time physical activity protect against arthritis in older women. J Epidemiol Community Health. 2008, 62: 1086-1091. 10.1136/jech.2007.072215.
Lim K, Taylor L: Factors associated with physical activity among older people - a population-based study. Prev Med. 2005, 40: 33-40. 10.1016/j.ypmed.2004.04.046.
Lawlor DA, Taylor M, Bedford C, Ebrahim S: Is housework good for health? Levels of physical activity and factors associated with activity in elderly women. Results from the British Women's Heart and Health Study. J Epidemiol Community Health. 2002, 56: 473-78. 10.1136/jech.56.6.473.
Hillsdon M, Lawlor DA, Ebrahim S, Morris JN: Physical activity in older women: Associations with area deprivation and with socioeconomic position over the life course: Observations in the British Women's Heart and Health Study. J Epidemiol Community Health. 2008, 62: 344-350. 10.1136/jech.2006.058610.
Brown DW, Balluz LS, Heath GW, Moriarty DG, Ford ES, Giles WH, Mokdad AH: Associations between recommended levels of physical activity and health-related quality of life. Findings from the 2001 Behavioral Risk Factor Surveillance System (BRFSS) survey. Prev Med. 2003, 37: 520-528. 10.1016/S0091-7435(03)00179-8.
Brown DR, Yore MM, Ham SA, Macera CA: Physical activity among adults ≥50 yr with and without disabilities, BRFSS 2001. Med Sci Sports Exerc. 2005, 37: 620-629. 10.1249/01.MSS.0000158189.17546.ED.
Ashe MC, Miller WC, Eng JJ, Noreau L: Older adults, chronic disease and leisure-time physical activity. Gerontology. 2009, 55: 64-72. 10.1159/000141518.
CDC: Prevalence of regular physical activity among adults - United States, 2001 and 2005. Morb Mortal Wkly Rep. 2007, 56: 1209-1212.
Muntner P, Gu D, Wildman RP, Chen J, Qan W, Whelton PK, He J: Prevalence of physical activity among Chinese adults: results from the International Collaborative Study of Cardiovascular Disease in Asia. Am J Public Health. 2005, 95: 1631-1636. 10.2105/AJPH.2004.044743.
Benedetti T, Borges L, Petroski E, Gonçalves LH: Physical activity and mental health status among elderly people. Rev Saude Publica. 2008, 42: 302-307. 10.1590/S0034-89102008005000007.
Ding CC, Chen XR, Zhang Z, Li KJ: Exercise and walking intensity and level of Beijing adult residents. Chi J Sports Med. 2009, 28: 362-364.
Hallal PC, Victora CG, Wells JC, Lima RC: Physical Inactivity: prevalence and associated variables in Brazilian adults. Med Sci Sports Exerc. 2003, 35: 1894-1900. 10.1249/01.MSS.0000093615.33774.0E.
Knuth AG, Bacchieri G, Victora CG, Hallal PC: Changes in physical activity among Brazilian adults over a 5-year period. J Epidemiol Community Health. 2010, 64: 591-595. 10.1136/jech.2009.088526.
Meyer K, Rezny L, Breuer C, Lamprecht M, Stamm HP: Physical activity of adults aged 50 years and older in Switzerland. Soz Praventivmed. 2005, 50: 218-229. 10.1007/s00038-005-4093-3.
Frank L, Kerr J, Rosenberg D, King A: Healthy ageing and where you live: Community design relationships with physical activity and body weight in older Americans. J Phys Act Health. 2010, 7 (1): S82-S90.
Guinn B, Vincent V: Select physical activity determinants in independent-living elderly. Activ. Adapt. Aging. 2002, 26: 17-26. 10.1300/J016v26n04_02.
Taylor-Piliae RE, Norton LC, Haskell WL, Mahbouda MH, Fair JM, Iribarren C, Hlatky MA, Go AS, Fortmann SP: Validation of a new brief physical activity survey among men and women aged 60–69 years. Am J Epidemiol. 2006, 164 (6): 598-606. 10.1093/aje/kwj248.
Allender S, Foster C, Boxer A: Occupational and non-occupational physical activity and the social determinants of physical activity: results from the Health Survey for England. J Phys Act Health. 2008, 5: 104-16.
Florindo AA, Guimães VV, Cesar CL, Barros MB, Alves MC, Goldblaum M: Epidemiology of leisure, transportation, occupational, and household physical activity: prevalence and associated factors. J Phys Act Health. 2009, 6: 625-632.
Joubert J, Norman R, Lambert EV, Groenewald P, Schneider M, Bwi F, Bradshaw D, South African Comparative Risk Assessment Collaborating Group: Estimating the burden of disease attributable to physical inactivity in South Africa in 2000. SA Med J. 2007, 97 (8): 725-731.
Meisner BA, Dogra S, Logan AJ, Baker J, Weir PL: Do or decline? Comparing the effects of physical inactivity on biopsychosocial components of successful ageing. J Health Psychol. 2010, 15: 688-696. 10.1177/1359105310368184.
Mummery WK, Kolt G, Schofield G, McLean F: Associations between physical activity and other lifestyle behaviors in older New Zealanders. J Phys Act Health. 2007, 4: 411-422.
McGuire LC, Ahluwalia IB, Strine TW: Report from the CDC. Chronic disease-related behaviors in U.S. older women: Behavioral Risk Factor Surveillance System, 2003. J Womens Health (Larchmt). 2006, 15: 3-7. 10.1089/jwh.2006.15.3.
Pronk NP, Anderson LH, Crain AL, Martinson BC, O'Connor PJ, Sherwood NE, Whitebird RR: Meeting recommendations for multiple healthy lifestyle factors: Prevalence, clustering, and predictors among adolescent, adult, and senior health plan members. Am J Prev Med. 2004, 27 (2): 25-33. 10.1016/j.amepre.2004.04.022.
Stamatakis E, Ekelund U, Wareham N: Temporal trends in physical activity in England: The Health Survey for England 1991 to 2004. Prev Med. 2007, 45: 416-423. 10.1016/j.ypmed.2006.12.014.
DiSipio T, Rogers C, Newman B, Whiteman D, Eakin E, Fritschi L, Aitken J: The Queensland Cancer Risk Study: behavioural risk factor results. Aust N Z J Public Health. 2006, 30: 375-382. 10.1111/j.1467-842X.2006.tb00852.x.
Ready AE, Butcher JE, Dear JB, Fieldhouse P, Harlos S, Katz A, Moffatt M, Rodriguez M, Schmalenberg J, Gardiner PF: Canada's physical activity guide recommendations are a low benchmark for Manitoba adults. Appl Physiol Nutr Metab. 2009, 34: 172-181. 10.1139/H08-143.
Panagiotakos DB, Polystipioti A, Polychronopoulos E: Prevalence of type 2 diabetes and physical activity status in elderly men and women from Cyprus (the MEDIS Study). Asia Pac J Public Health. 2007, 19: 22-28. 10.1177/101053950701900305.
Sims J, Hill K, Davidson S, Gunn J, Huang N: A snapshot of the prevalence of physical activity amongst older, community dwelling people in Victoria, Australia: patterns across the ‘young-old’ and ‘old-old’. BMC Geriatr. 2007, 7: 4-10.1186/1471-2318-7-4.
Tucker JM, Welk GJ, Beyler NK: Adults: compliance with the physical activity guidelines for Americans. Am J Prev Med. 2011, 40: 454-461. 10.1016/j.amepre.2010.12.016.
Tyrovolas S, Zeimbekis A, Bountziouka V, Voutsa K, Pounis G, Papoutson S, Matallinos G, Ladsukaki E, Polychronopoulos E, Lionis C, Panagiotakos DB: Factors associated with the prevalence of diabetes mellitus among elderly men and women living in Mediterranean Islands: The MEDIS study. Rev Diabet Stud. 2009, 6: 54-63. 10.1900/RDS.2009.6.54.
Gómez LF, Parra DC, Buchner D, Sarmiento OL, Pinzón JD, Ardila M, Moreno J, Serrato M, Lobelo F: Built environment attributes and walking patterns among the elderly population in Bogotá. Am J Prev Med. 2010, 38: 592-599. 10.1016/j.amepre.2010.02.005.
McGuire L, Bouldin EL, Andresen EM, Anderson LA: Examining modifiable health behaviours, body weight, and use of preventive health services among caregivers and non-caregivers age 65 years and older in Hawaii, Kansas and Washington using 2007 BRFSS. J Health Aging. 2010, 14 (5): 373-379. 10.1007/s12603-010-0083-0.
Xu YJ, Mao WJ, Xu XJ, Cai QM, Song XL, Nie SP, Xu HF, Xia L: Patterns and influencing factors of physical activity among residents in guangdong province. South China. J Prev Med. 2009, 35: 5-
CDC USA: Prevalence of self-reported physically active adults--United States, 2007. MMWR Morb Mortal Wkly Rep. 2008, 57: 1297-300.
Bird S, Kurowski W, Feldman S, Browning C, Lau R, Radermacher H, Thomas S, Sims J: The influence of the built environment and other factors on the physical activity of older women from different ethnic communities. J Women Ageing. 2009, 21: 33-47. 10.1080/08952840802633669.
Carlson SA, Fulton JE, Schoenborn CA, Loustalot F: Trend and prevalence estimates based on the 2008 Physical Activity Guidelines for Americans. Am J Prev Med. 2010, 39: 305-313. 10.1016/j.amepre.2010.06.006.
Hurtig-Wennlof A, Hagstromer M, Olsson LA: The International Physical Activity Questionnaire modified for the elderly: aspects of validity and feasibility. Public Health Nutr. 2010, 13: 1847-1854. 10.1017/S1368980010000157.
Shores KA, West ST, Theriault DS, Davison EA: Extra-individual correlates of physical activity attainment in rural older adults. J Rural Health. 2009, 25: 8-10.1111/j.1748-0361.2009.00193.x.
Xue MY: Effects of daily physical activities on physical health and quality of life in elderly community residents in Jiangsu Province. J Clin Rehabilitative Tissue Eng Res. 2010, 14: 6-
Fleming LE, Lee DJ, Martinez AJC, Leblanc WG, McCollister KE, Bridges KC, Christ SL, Arheart KL, Pitman T: The health behaviors of the older US worker. Am J Ind Med. 2007, 50: 427-437. 10.1002/ajim.20468.
Troiano RP, Berrigan D, Dodd KW, Masse LC, Tilert T, McDowell M: Physical activity in the United States measured by accelerometer. Med Sci Sports Exerc. 2007, 40: 181-188.
Harris TJ, Owen CG, Victor CR, Adams R, Crook DG: What factors are associated with physical activity in older people, assessed objectively by accelerometry?. Br J Sports Med. 2009, 43: 442-450. 10.1136/bjsm.2008.048033.
Colley R, Garriguet D, Janssen I, Craig CL, Clarke J, Tremblay MS: Physical activity of Canadian children and youth: accelerometer results from the 2007 to 2009 Canadian Health Measures Survey. Health Rep. 2011, 22: 1-9.
Stamatakis E, Hillsdon M, Primatesta M: Domestic physical activity in relationship to multiple CVD risk factors. Am J Prev Med. 2007, 32: 320-327. 10.1016/j.amepre.2006.12.020.
Hallal PC, Andersen LB, Bull FC, Guthold R, Haskell W, Ekelund U: Global physical activity levels: surveillance progress, pitfalls, and prospects. Lancet. 2012, 380: 247-257. 10.1016/S0140-6736(12)60646-1.
Craig CL, Russel CJ, Cameron C, Bauman A: Twenty-year trends in physical activity among Canadian adults. C J Public Health. 2004, 95 (1): 59-63.
Caspersen CJ, Pereira MA, Curran KM: Changes in physical activity patterns in the United States, by sex and cross-sectional age. Med Sci Sports Exerc. 2000, 32: 1601-1609.
Curtis J, White P, McPherson B: Age and physical activity among Canadian women and men: findings from longitudinal national survey data. J Ageing Phys Act. 2000, 8: 1-19.
Weller I, Corey P: The impact of excluding non-leisure energy expenditure on the relation between physical activity and mortality in women. Epidemiology. 1998, 9: 632-635. 10.1097/00001648-199811000-00012.
Helkapori S, Uutela A, Prattala R: Health Behaviour and Health among FinnishPopulation, Spring 2000. 2000, Helsinki, Finland: National Public Health Institute
Sport and Recreation New Zealand: Results from the New Zealand Sport and PhysicalActivity Surveys (1997–2001). 2001, Available at: [http://www.activenzsurvey.org.nz/Results/SPARC-Trends-in-Participation-in-Sport-and-Active-Leisure-1997-2001/Trends-Participation/] Accessed Sep 11, 2011
Knuth AG, Hallal PC: Temporal trends in physical activity: a systematic review. J Phys Act Health. 2009, 6: 548-559.
Prince SA, Adamo KB, Hamel ME, Hardt J, Gorber SC, Tremblay M: A comparison of direct versus self-report measures for assessing physical activity in adults: a systematic review. Int J Behav Nutr Phys Act. 2008, 6: 5-56.
Bowling A: The psychometric properties of the older people’s quality of life questionnaire, compared with the CASP-19 and the WHOQOL-OLD. Curr Gerontol Geriatr Res. 2009, 10.1155/2009/298950.
World Health Organisation: Global Recommendations on Physical Activity for Health. 2010, Geneva: World Health Organisation
Lee I-M, Shiroma EJ, Lobelo F, Puska P, Blair SN, Katzmarzk PT: Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet. 2012, 380: 219-229. 10.1016/S0140-6736(12)61031-9.
Sisson SB, Katzmarzyk PT: International prevalence of physical activity in youth and adults. Obes Rev. 2008, 9: 606-614. 10.1111/j.1467-789X.2008.00506.x.
Vandelanotte C, Duncan MJ, Caperchione C, Hanley C, Mummery WK: Physical activity trends in Queensland (2002 to 2008): are women becoming more active than men?. Aust N Z J Public Health. 2010, 34: 248-254. 10.1111/j.1753-6405.2010.00521.x.
Macera CA, Pratt M: Public health surveillance of physical activity. Res Q Exerc Sport. 2000, 71 (2): S97-103.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2458/13/449/prepub
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
None declared by the authors. This review was unfunded.
Authors’ contributions
All authors devised the research strategy; initial screening was undertaken by FS and then checked by AEW. FS extracted the data which was checked by AEW. Disagreements were resolved by reference to IJN. All authors contributed to the data synthesis and production of the paper. All authors read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
{kind=link}
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Sun, F., Norman, I.J. & While, A.E. Physical activity in older people: a systematic review. BMC Public Health 13, 449 (2013). https://doi.org/10.1186/1471-2458-13-449
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2458-13-449