
Abstract
Background
Several systematic reviews have been published to investigate the effectiveness of high-intensity interval training (HIIT) in schools. However, there has been limited attention given to understanding the functioning of the intervention processes, which is of paramount importance for interpreting and translating the intervention effectiveness. The aim of this systematic review is to determine the extent to which process evaluation is measured in school-based HIIT interventions and to explore the effects of process evaluation and intervention characteristics on cardiorespiratory fitness (CRF), body composition, muscular strength, and blood pressure.
Methods
A comprehensive search was conducted in SPORT Discus (EBSCOhost), Web of Science, Scopus, Medline (Ovid) and Cochrane Central Register of Controlled Trials. The extent to which process evaluation is measured was narratively reported, alongside with the guidance of process evaluation of complex interventions by UK Medical Research Council. Meta-analyses and meta-regressions were conducted to determine the effects of process evaluation and intervention characteristics to the intervention outcomes.
Results
The literature search identified 77 studies reporting on 45 school-based HIIT interventions. In total, five interventions reported process evaluation in a section or in a separate study, and only one intervention adopted a process evaluation framework. On average, 6 out of 12 process evaluation measures were reported in all interventions. Subgroup analyses did not indicate any beneficial treatment effects for studies with process evaluation group, whereas all pooled data and studies without process evaluation group showed significant improvement for CRF and body composition.
Conclusion
Process evaluation is frequently omitted in the literature of school-based HIIT in children and adolescents. Although reporting of process evaluation measures may not directly associate with better intervention outcomes, it allows accurate interpretation of intervention outcomes, thereby enhancing the generalisability and dissemination of the interventions.
Similar content being viewed by others


Introduction
Physical activity (PA) is well documented in promoting physical fitness and health, including improvement in body composition, cardiorespiratory fitness (CRF), musculoskeletal function and psychological health in children and adolescents [1,2,3,4]. Despite the importance of PA, it is reported that less than 20% of adolescents meet the World Health Organization guideline of an average of 60 min moderate to vigorous PA (MVPA) per day [3]. In addition, recent studies have shown that the COVID-19 pandemic, local or international conflicts, and economic and climate changes, have further exacerbated global physical inactivity [5, 6].
Schools, where children and adolescents spend most of their waking time, play a fundamental role in promoting MVPA amongst children and adolescents [7]. Time in PA participation can be accumulated not only during physical education classes, but also throughout various breaks or even in academic classes [8]. However, the effectiveness of school-based interventions to increase engagement in MVPA is limited [1, 9, 10]. Commonly cited barriers for MVPA engagement are time constraints, lack of motivation and facilities [11, 12]. Consequently, adopting a time-efficient and engaging PA strategy may be a promising approach for health promotion within school settings.
Despite concerns for high-intensity interval training (HIIT) to be safely performed by inactive population, the elderly, or patients [13], emerging evidence suggests that HIIT is a form of exercise that is safe [14], time-efficient [11] and enjoyable [15] to be performed among healthy school-aged children and adolescents. Apart from these allures, HIIT provides young people with opportunities to engage in vigorous PA (VPA) [14], which is favourably associated with several cardiometabolic health markers (e.g., CRF) in youth [16, 17]. Therefore, the popularity of tailoring HIIT in school-based health-promoting interventions has grown in recent years. Indeed, several school-based HIIT reviews have been published [18,19,20,21,22,23], supporting beneficial effects of HIIT on health markers such as body composition, CRF and neuromuscular performance in comparison to a control group (e.g., maintaining daily living, attending regular physical education classes etc.).
However, the question remains as to how practitioners and researchers should accurately interpret and capitalise on these promising findings and whether the effectiveness of these interventions are transferable to different contexts. These important questions will not necessarily be addressed if an intervention is conducted in isolation, without reporting the implementation process [24]. Process evalution provides insights into how an intervention is conducted, drawing upon the causality underpinning the treatment effects [25]. By incorporating process evaluation with randomised controlled trials (RCTs), gold standard for establishing intervention effectiveness [26], the implementation fidelity and quality of the RCTs can be assessed and the causal mechanisms and contextual factors shaping the intervention effectiveness can be clarified [24]. Therefore, process evaluation is complementary to that of RCTs by not only assessing if the intervention works, but also why it works and if it works in other contexts [24], thereby informing future intervention maintenance, scaling up and transfer [25].
Recognising the growing importance of process evaluation, a cascade of frameworks emerged under the term ‘process evaluation’ [24, 27,28,29]. Among them, the Medical Research Council (MRC) guidance on the process evaluation of complex interventions, developed by Moore et al., stands out as particularly comprehensive [24]. This framework drew upon insights related to the existing definition of process evaluation and was developed by a group of researchers with expertise in complex interventions through a series of workshops, conferences, and seminars. The MRC guidance delineates three domains of process evaluation: implementation, mechanisms of impact and context. These domains encompass understandings of what and how the intervention is implemented; how the intervention brings changes to the intervention outcomes; and how the context shapes the implementation process and outcomes. Notably, the MRC guidance has been adopted in reviews of different areas [30, 31]. For example, Ma and colleagues adapted the framework to assess the extent to which process evaluation is reported in interventions aimed at improving gross motor competence in children and adolescents [30].
While process evaluation serves as an important complement to outcome assessment, its reporting remains infrequent and insufficient [32]. Among the six school-based HIIT reviews [18,19,20,21,22,23], none has primarily focused on process evaluation. Despite one study reported certain aspects of process evaluation measures, such as fidelity and attendance [18], comprehensive attention to this critical aspect is notably lacking. With more studies starting to report process evaluation in school-based HIIT RCTs [33,34,35,36,37], a systematic review assessing process evaluation is timely in synthesising the evidence and providing recommendations for future interventions. Therefore, the primary aim of this systematic review is to examine the extent of process evaluation reporting in school-based HIIT studies. The secondary aim is to determine the effects of process evaluation and intervention characteristics on CRF, body composition, muscular health, and blood pressure.
Methods
This review aligns with the guidelines of Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [38], see Additional File 1 for the PRISMA checklist, and Cochrane Handbook for Systematic Reviews of Interventions [39]. The protocol of the review was registered on PROSPERO (CRD42022314567).
Inclusion and exclusion criteria
Population
To be included in this review, participants needed to be 5–18-year-old school children or adolescents with no restrictions placed on weight status. However, studies which focused on specific sub-populations, such as youth athletes or paediatric disease/disability groups (e.g., diabetes mellitus) were excluded.
Intervention
Intervention duration ≥ 2 weeks was considered eligible, and the intervention must comprise at least one HIIT treatment group to be included in the review. HIIT in the current study was defined as repeating short (within 45 s) to long (up to 4 min) bouts of high-intensity exercises (e.g., 85% maximum heart rate (HRmax)), interspersed with rest or recovery periods [40].
Comparator
Any form of control or comparative groups were included for assessing the extent of process evaluation reporting. However, only the studies with a usual practice control group (e.g., continued with regular physical education session) were included in the subsequent meta-analyses and meta-regressions considering the heterogeneity among comparative exercise groups.
Outcome
The primary aim was to explore and report the extent of process evaluation in school-based HIIT interventions. Consequently, no restriction was made in terms of intervention outcomes. However, only the following outcomes were considered for meta-analysis and regression: CRF, body composition, muscular strength, and blood pressure. These variables were selected as they are the most frequently studied fitness parameters in the literature of school-based HIIT interventions [18, 22].
Study design
The interventions must be conducted on school premises, regardless of where the outcome data were collected. In addition, only RCTs were included in the current study since it is considered as the gold standard for establishing intervention effectiveness [26].
Search strategy and selection
A comprehensive search for the relevant literature was conducted in SPORTDiscus (EBSCOhost), Web of Science, Scopus, Medline (Ovid) and Cochrane Central Register of Controlled Trials from inception to March 2022. Search strategy was formulated based upon the guideline of Peer Review of Electronic Search Strategy (PRESS) [41] and was checked with an information specialist before commencement. The full search strategy is available in Additional File 2.
Upon removal of duplicates on Endnote (Clarivate Analytics, Philadelphia, USA), two reviewers (YL and CW) independently screened the titles and abstracts against the inclusion and exclusion criteria in a blinded manner on Rayyan [42]. Subsequently, a discussion was organised to compare and reconcile the independent screening results, reaching a consensus on the papers to undergo a full-text review. This process was reiterated via another round of independent screening and discussion to complete the selection. Disagreements were resolved by discussion with two additional authors (CAW and ARB). The references cited in the included studies were manually checked for identifying additional eligible studies and an updated search was made in November 2022. Whenever not enough information in the manuscript for deciding, an inquiry email was sent to the authors for clarification. If the authors did not reply, these studies were listed as awaiting classification and were excluded if no responses were received after a second inquiry attempt at least fourteen days apart. These excluded papers are presented in Additional File 3.
Data extraction
A data extraction sequential list (Table 1) was predefined in case multiple measurements of the same outcome emerged. The rationale for the prioritisation was based upon measurement properties (e.g., validity and reliability) and popularity of the measurements. Data extraction on process evaluation measures was guided by the Medical Research Council (MRC) process evaluation framework [24], including domains of implementation, mechanisms of impact, and context. The framework is elaborately conducted, providing a systematic, comprehensive, and exhaustive process evaluation review [25, 30]. A process evaluation framework by Ma et al. [30] was referred to adapt the framework into practice. The process evaluation measures were predefined in Table 2. Of note, although defined as session quality (e.g., attendance and dose received) and intensity in school-based HIIT studies [37, 43], fidelity was solely represented by intensity in the current review, as session quality was reported separately as other process evaluation measures (e.g., dose delivered).
The following data were extracted: (1) key study characteristics (e.g., author name, publication year, participant characteristics, intervention details, and sample size); (2) process evaluation measures (implementation, mechanisms of impact and context); (3) post intervention (the closest to intervention endpoint) outcomes and results, including sample size, mean and standard deviation (SD) in intervention and non-exercise control groups. Where trials reported 95% confidence intervals [33, 50] or median and interquartile range [53], these were converted to means and SDs using established methods [54]. In addition, mean change values [50, 55] were extracted when post-means and SDs were not reported, and data were extracted from figures, via GetData Graph Digitizer, when not reported numerically [35]. Data extraction forms were developed, piloted, and refined through discussions across the authorship team. The extraction was conducted by YL and partially (30%) checked by CW for accuracy.
Risk of bias assessment
The Cochrane risk-of-bias tool for randomized trials and revised Cochrane risk-of-bias tool for cluster-randomized trials [56] were adopted for quality assessment of RCTs and cluster-RCTs, respectively. Risk of bias for the outcomes of CRF, body composition and muscular strength were assessed separately from the following five domains: randomization process, intended interventions, missing outcome data, measurement of outcome and report of results by answering signalling questions. The judgments for each domain were summarised as “low risk of bias” “some concerns” or “high risk of bias”. An overall risk of bias judgement was reached through algorithms that map responses to signalling questions. The first author (YL) performed the risk of bias assessment, and the accuracy of the assessment was subsequently verified by a second author (CW) through a random sub-sample (30%) of studies, with less than 80% of consensus triggered a check for all the studies. Conflicts were discussed with consultation been made with either CAW or ARB whenever disputes occurred.
Data synthesis and meta-analyses
Process evaluation measures in relation to the included interventions were thematically assembled in line with the prescribed definition (Table 2) and were narratively reported. All the interventions were qualitatively synthesised. Random-effects meta-analyses were performed, incorporating subgroup analyses for studies with and without process evaluation, to determine the differences between the two groups concerning CRF, body composition, muscular strength and blood pressure. Where outcomes were reported using different measurement units, a standardised mean difference (SMD) effect size was reported. SMD was set as 0.2, 0.5 and 0.8, corresponding to small, medium and large effects [57]. Several sensitivity analyses were performed including a leave one out meta-analysis, the removal of high risk of bias studies, and studies that had a computed outcome score. A spectrum of intervention characteristics and process evaluation measures (Table 3) were selected and regressed to determine mediators of CRF, body composition, muscular strength and blood pressure. Heterogeneity was assessed via I2 and tau2 (τ2) statistic [39], publication bias was assessed via funnel plots and the Egger’s test [58]. The analyses were performed in STATA version 17 (College Station, Texas 77,845 USA) [59].
Results
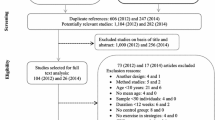
The initial search in March 2022 yielded 3,766 records, and an additional 320 records were identified in the updated search in November 2022. The PRISMA flowchart is shown in Fig. 1. The detailed reasons for the exclusion of the full text checked studies are presented in the Additional File 3. At length, 77 studies were included, covering 45 school-based HIIT interventions. All the interventions were included to determine the extent of process evaluation reporting. Of note, since only one study reported both blood pressure and process evaluation simultaneously [34], no further analysis was conducted for this outcome. Thus, 30, 22 and 13 interventions were included in meta-analyses and meta-regressions for CRF, body composition and muscular strength assessment, respectively.

Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram. PICO, population, intervention, comparison and outcomes; CRF, cardiorespiratory fitness
Study characteristics
In total, 15 interventions (33%) were cluster-RCTs. When combined, over 25,104 participants, across 17 Countries/regions, were included in this review. Twenty-one interventions (47%) were conducted in primary schools, while twenty-four interventions (53%) were delivered in secondary schools. The mean age was 12.2 years (n = 38), and 7 studies provided the age range of the participants only. There were 8 and 7 interventions targeted exclusively at female and male participants, respectively. Eleven interventions examined children living with overweight and obesity. The HIIT intervention duration ranged from 2 weeks to one academic year and was 12 weeks on average. The session frequency ranged from 1 to 5 times per week, with 3 (24 interventions, 53%) or 2 (14 interventions, 31%) sessions per week being most frequently reported. The HIIT sessions were as short as 4 min to as long as 43 min in total length. The work and rest intervals varied significantly, ranging from 10 s up to 240 s, with more than half of the interventions (n = 27) adopted a work interval less than 30 s. Additionally, the work-to-rest ratio was different from interventions, with the ratio = 1 (n = 17), < 1 (n = 5), > 1 (n = 9) or varied (n = 14). Twenty interventions (44%) adopted the traditional running or cycling modality. The details of all the intervention characteristics are summarised in the Additional File 4.
Risk of bias
No conflicts were found between the two authors regarding the risk of bias assessment of the 30% sub-sample. The details of risk of bias assessment for CRF, body composition and muscular strength are presented in Additional File 5 and 6, and are briefly displayed in Figs. 2, 3 and 4, respectively. Of the 30 studies reporting CRF, 5 (17%) studies were assessed as “low risk”, 11 (37%) “some concerns” and 14 (46%) “high risk”. For body composition outcome studies, 3 (14%) were rated as “low risk”, 8 (36%) “some concerns” and 11 (50%) “high risk”. For muscular strength outcome studies, 3 (23%) were assessed as “low risk”, 5 (38%) “some concerns” and 5 (39%) “high risk”. The major reasons for raising the concerns were: 1) lack of proper randomization; 2) no blinding; 3) not accounting for missing data; and 4) lack of pre-determined protocol.

Studies with versus without process evaluation on CRF in school-based HIIT interventions. SMD, stand mean difference; RoB, risk of bias; CI, confidence interval; S, some concern; H, high risk of bias; L, low risk of bias; YYIRT1, YO-YO Intermittent Recovery Test Level 1; PACER, Progressive Aerobic Cardiovascular Endurance Run; AEP, aerobic exercise programme; RAP, resistance and aerobic programme

Studies with versus without process evaluation on body composition in school-based HIIT interventions. SMD, stand mean difference; RoB, risk of bias; CI, confidence interval; S, some concern; H, high risk of bias; L, low risk of bias; BMI, body mass index; AEP, aerobic exercise programme; RAP, resistance and aerobic programme

Studies with versus without process evaluation on muscular strength in school-based HIIT interventions. SMD, stand mean difference; RoB, risk of bias; CI, confidence interval; S, some concern; H, high risk of bias; L, low risk of bias; AEP, aerobic exercise programme; RAP, resistance and aerobic programme
The extent of process evaluation reporting
Table 4 summaries the process evaluation measures across the included interventions. In total, 4 interventions labelled and nested process evaluation in a section of the paper [33,34,35,36] and one intervention reported process evaluation in a separate paper [37]. Although not labelled as “process evaluation”, two interventions published a separate paper to evaluate and reflect on the implementation process [60] and to identify the facilitators and barriers across the intervention delivery process [61]. On average, half of the process evaluation measures (n = 6) were reported upon, and most interventions (n = 43) reported on multiple process evaluation measures. Implementation was the most frequently reported domain (59%), followed by mechanism of impact (42%) and context (34%). The detailed information of how each process evaluation measures were met is presented in Table 5.
Implementation
In total, 38 out of 45 interventions (84%) reported fidelity using a variety of methods. Specifically, HR monitors were used in 22 interventions, with seventeen providing HR outcome data and five did not. Maximum aerobic speed (MAS) was adopted by eleven interventions. However, five of them did not articulate how MAS was used to quantify intensity (e.g., individualising interval distance according to participants’ MAS). Four interventions used rating of perceived exertion (RPE), with only two of them reporting outcome data (6.9/10 [78] and 17.3/20 [48]). Fidelity was also reported as accumulated VPA time via accelerometer by two interventions, with one demonstrating significantly higher VPA time in the intervention group compared to control [35]. Seven interventions did not monitor exercise intensity.
Reach was reported in 19 interventions (42%). All the interventions documented the number of participants recruited, despite five which did not provide information regarding retention. Of the 40 interventions that tracked retention, six recorded the number of dropped out participants but without specifying the reasons. Four interventions reported 100% attendance, while 31 reported both attritions and reasons, with lack of time, school transfer, illness and absence in testing days been most frequently documented. All the interventions provided information regarding dose delivered. Eleven interventions (22%) reported adaptation(s) to refine the implementation.
Mechanism of impact
While dose delivered was frequently reported, nearly half (22 interventions, 49%) did not track dose received. There were 16 interventions (36%) which investigated the mediators of the intervention outcomes, with baseline level, sex, maturity, and dose response explored. Adverse event (n = 24) was the most frequently reported unintended consequences. Apart from that, absence of deliverer (due to illness), poor compliance and inclement weather were documented. With regard to response, 12 interventions (27%) collected feedback from students, teachers, parents and/or school authorities, via questionnaires, interviews, focus groups and/or surveys.
Context
Barriers were reported in 12 interventions (27%). Among them, three interventions perceived the busy curriculum as a barrier, three mentioned the inconvenient use of equipment and six reported time constrains. Others were lack of space and perceived fitness improvement. By contrast, 20 interventions (44%) informed the facilitators of implementation. Of them, twelve interventions used different incentives to motivate participants, including offering choices (e.g., choose exercise modalities, partners or music), equipment (e.g., real-time HR on screen) and voucher/money upon completion of intervention; nine interventions provided pre-intervention training to students and/or teachers; five interventions adopted a theory model to guide the implementation; two interventions perceived their study design as facilitators, such as short, simple, low cost and equipment free; and three perceived the support from the schools or research team as facilitators. Lastly, 15 interventions (33%) reported the measurement of contamination. In detail, three interventions served the control groups with placebo (e.g., stretches); eleven blinded the outcome assessors to avoid bias in data collection; and one blinded the researchers for randomisation to ensure the quality of group allocation.
Effects of process evaluation and intervention characteristics on CRF, body composition and muscular strength
A total of 33 studies were included for pooled random-effects meta-analyses and meta-regressions, with subgroup comparison between studies with and without process evaluation. In total, eight studies were appraised as fulfilling implementation process (intended to report process evaluation measures) and were allocated to the studies with process evaluation subgroup.
CRF
Thirty studies reported CRF related outcomes, including VO2peak (n = 14), 20 m shuttle run (n = 13), Yo-Yo Intermittent Recovery Test Level 1 (n = 3), 6 min running (n = 2), and one study reported 15 m Progressive Aerobic Cardiovascular Endurance Run (Fig. 2). There was a small but significant overall improvement in CRF following HIIT compared to no exercise control group, with a SMD of 0.33 (95% CI 0.16 to 0.51; I2 = 90.90%; τ2 = 0.18). The subgroup analysis revealed a nonsignificant effect on CRF for studies with process evaluation (SMD 0.06; 95% CI -0.07 to 0.18; I2 = 54.18%; τ2 = 0.01), while a significant medium effect for studies without process evaluation (SMD 0.53; 95% CI 0.23 to 0.84; I2 = 89.87%; τ2 = 0.42) (Fig. 2).
Several sensitivity analyses were performed. By removing high risk of bias studies (n = 14), the overall effect for CRF remained significant (SMD 0.14; 95% CI 0.01 to 0.27; I2 = 77.19%; τ2 = 0.04). However, when accounting for risk of bias, both studies with and without process evaluation groups were not significant (SMD 0.03; 95% CI -0.09 to 0.15; I2 = 51.94%; τ2 = 0.01 and SMD 0.29; 95% CI -0.03 to 0.61; I2 = 83.98%; τ2 = 0.15, respectively). The removal of computed outcome scores [33, 35, 50, 53, 55] had no significant influence on the overall results. In addition, no individual study had a clinically or statistically meaningful effect on the overall SMD through leave-one-out analysis. The funnel plot indicated considerable asymmetry and Egger’s test (p < 0.01) showed significant publication bias for studies reporting CRF in school-based HIIT interventions. The sensitive analysis figures and funnel plot for CRF are presented in Additional File 7.
In total, 14 intervention characteristics and 15 process evaluation measures were regressed to examine mediators of CRF (Table 6). Altogether, seven intervention characteristics and four process evaluation measures significantly altered CRF. Specifically, the following characteristics elicited significantly greater CRF: 1) individual compared to cluster RCTs; 2) direct compared to indirect measurement of CRF; 3) overweight and/or obese cohort compared to not specified; 4) shorter compared to longer intervention duration; 5) running/cycling-based HIIT compared to other modalities; 6) higher compared to lower risk of bias studies; and 7) lower compared to higher reported % HRmax. In addition, studies reported adaptation, dose received, incentive strategy and pre-intervention training were associated with significantly lower CRF compared to studies did not report these process evaluation measures (Table 6).
Body composition
Data for body composition were available in 22 studies and five studies in the process evaluation subgroup (Fig. 3). Based on Table 2, data were presented as % body fat (n = 12), BMI (n = 8), BMI-z score (n = 1) and fat mass (n = 1). The pooled data showed significantly small effects on body composition in both overall (SMD = -0.24; 95% CI from -0.47 to -0.02; I2 = 88.58%; τ2 = 0.26) and studies without process evaluation group (SMD = -0.36; 95% CI from -0.70 to -0.03; I2 = 90.30%; τ2 = 0.45). By contrast, the studies with process evaluation showed no treatment effect (SMD = 0.02; 95% CI from -0.09 to 0.12; I2 = 0%; τ2 = 0).
When removing the high risk of bias studies (n = 11), neither overall nor studies with and without process evaluation subgroups were significant, whereas no significant change was observed by omitting the computed outcome scores. The results are listed in the Additional File 7. The funnel plot (Additional File 7) indicated slight asymmetry and Egger’s test (p = 0.09) suggested nonsignificant publication bias for studies measuring the outcome of body composition.
Meta-regression revealed that studies individually randomised, conducted among overweight and/or obese cohort, adopted running/cycling modality and without reporting incentive strategies induced significantly better effects on body composition compared to the counterparts (Table 7).
Muscular strength
Thirteen studies reported muscular strength related variables, with 6 studies allocated to the process evaluation subgroup (Fig. 4). In terms of measurement, three studies reported handgrip, one for leg muscle strength, four for standing long jump, three for push-ups and two for counter movement jump. The overall effect was not significant, with SMD = 0.26 (-0.16, 0.69), I2 = 94.44% and τ2 = 0.61. Similarly, no significant findings were observed in the subgroup analyses (Fig. 4) and sensitive analyses (Additional File 7). The funnel plot (Additional File 7) indicated asymmetry and Egger’s test (p = 0.01) suggested significant publication bias for studies measuring the outcome of muscular strength. Furthermore, leave-one-out analysis did not modify the overall result. However, reporting of reach and adverse event were negatively associated with muscular strength outcomes (Table 8).
Discussion
The present review is the first to scrutinise the extent of process evaluation reporting in school-based HIIT interventions while examining the influence of process evaluation and intervention characteristics on CRF, body composition, and muscular strength. Previous school-based HIIT reviews [18,19,20,21,22,23] exclusively focused on reporting intervention outcomes, overlooking the critical aspect of process evaluation. Our review timely addresses this gap by summarising the implementation process of included studies and determining the potential impact of process evaluation measures on intervention effectiveness for key outcomes including CRF, body composition and muscular strength.
Summary of findings
In total, 77 studies from 45 school-based HIIT interventions were identified, with an average of 6 out of 12 process evaluation measures being reported. Five interventions (11%) explicitly labelled and reported process evaluation in either a section of the paper or summarised in a separate publication. However, most of them were atheoretical except one intervention [37] adopted a framework by McKay et al. [121]. Overall, half (6/12) of the process evaluation measures were reported on average across all the interventions, with implementation being the most frequently reported domain (59%), followed by mechanism of impact (42%) and context (34%). The current study did not identify any favourable associations between studies intended to report process evaluation and the intervention outcomes in terms of CRF, body composition and muscular strength, and neither did reporting any of the process evaluation measures elicit better treatment effects for these health parameters. Rather, the overall pooled studies and those studies without deliberately reporting process evaluation were found to have beneficial effects for CRF, body composition and muscular strength, despite the studies without process evaluation group being characterised by higher heterogeneity and risk of bias. These findings indicate that process evaluation elicits no salient potentiation to the intervention effectiveness. However, it is undeniable that process evaluation completes the outcome-oriented RCTs of school-based HIIT interventions by providing sound implementation details, exploring potential mechanisms of impact and clarifying context factors. Hence, the understanding of the intervention effectiveness, generalizability and transferability are enhanced through the “lens” of process evaluation. Nevertheless, process evaluation has been largely neglected and under-reported, which may have potentially tempered the value of the existing school-based HIIT interventions.
How and to what extent process evaluation measures were reported and what can be used to inform future studies
Fidelity is the key to process evaluation and is defined as the degree of the intervention being delivered as intended by multiple frameworks [24, 121,122,123]. In the present review, it was represented solely by HIIT intensity. Of the 45 included interventions, the majority of studies (84%) monitored HIIT intensity. Notwithstanding, the prescribed intensity was monitored in various ways, and to some extent, in an incomplete or invalid manner. First, although HR monitors provide an objective measure of HIIT intensity, failing to report the actual HR data can compromise intervention fidelity and leave the mechanisms underlying intervention effectiveness ambiguous. Likewise, MAS is another way to prescribe intensity, however, not without the premise of articulating how to individualise the running speed. Second, RPE enables a simple and convenient way for intensity monitoring. Even so, notably, RPE is not yet validated in the context of school-based HIIT interventions. Interestingly, VPA (as measured via accelerometery) has emerged as a means of gaging HIIT intensity in two studies [35, 43], which ushered in a new direction and consideration for determining HIIT fidelity. Both studies aimed to assess intervention fidelity by comparing accelerometer determined VPA between the HIIT and control groups, with one study [35] reporting significantly greater amount of VPA time in the HIIT group, while the other [43] reported nonsignificant findings. However, neither study established a predetermined standard for ‘high intensity’ using VPA, despite fidelity being defined as intervention delivered as intended [24, 121,122,123,124]. Future studies are recommended to thoroughly consider the pros and cons of HIIT monitoring tools before incorporating into their study designs. These considerations should include factors such as precision, affordability, validity and time commitment. Additionally, the pursuit of more efficient tools for prescribing and monitoring HIIT could be a future research endeavour. Our research team has recently demonstrated the validity of utilising RPE, as evidenced by Liu et al. [125], and session RPE, as illustrated by Duncombe et al. [126], for monitoring HIIT in laboratory and school settings, respectively. Furthermore, a call is claimed to fully report the HIIT intensity data and to continuously working on developing convenient and feasible measurements for establishing HIIT fidelity, especially for large-scaled studies [18].
The current review found that the common reasons for dropping out were absence in testing days, illness, lack of time and school transfer. High level of attrition may lead to biased intervention effects [53], therefore, where possible, measures should be taken to motivate and retain participants or by using appropriate statistical analysis methods (e.g., intention-to-treat). Several strategies were applied to do so in the studies included in the present review, including providing a flexible intervention schedule [63], rescheduling the missed sessions or tests [47] and offering choices [35, 111] or rewards [36, 105, 119]. These are practical solutions for researchers to boost future “buy-in” of potential stakeholders. Since no “one size fits all” approach to the study design, adaptation(s) may be necessary at times. Yet, it was the least reported process evaluation measures. Findings suggested that the purposes for making the adaptation(s) were to: 1) adjust intensity (e.g., introduce new rules to avoid participants staying still [34]); 2) to ease implementation (e.g., substitute HR monitors with RPE for monitoring intensity [48]); and 3) to make a compromise (e.g., re-schedule sessions due to busy curriculum [47]). The current study demonstrated that HIIT is generally safe for children and adolescents in view of the fact that only minor injuries (bruises and strains) [86] and dizziness (due to blood sampling) [34] were reported. This was in accordance with previous reviews which demonstrated that HIIT is safe to be applied in children and adolescents [11, 127]. While dose delivered was reported by all the interventions, half of them (n = 23) were not clear on how many doses were received by participants, overshadowing the quality of implementation and the understanding of effectiveness. Although barriers and facilitators were underreported, the existing information sheds some light on future interventions. Based on the qualitative reporting of the included studies, it appears that busy curriculum [43, 50], lack of time [36, 111] and inconvenient equipment use [35, 105] were frequently reported as barriers to implementation, whereas training workshops [44, 48, 113], incentive strategies [105, 113] and theoretical instructions [37, 50] were reported as effective boosters. In addition, findings of the present review suggest that short, simple, enjoyable interventions that do not heavily rely on equipment may be better suited to meet the needs of stakeholders [48, 119].
Effects of process evaluation measures
Nesting process evaluation within RCTs enables a comprehensive and lucid description of both the process and outcome evaluations, thereby facilitating the replication and synthesis of evidence [24]. Nevertheless, it remains unclear whether process evaluation leads to better effects in school-based HIIT interventions. The current review revealed that better reporting of process evaluation posed no potentiation to the outcomes of CRF, body composition and muscular strength in school-based HIIT interventions. Despite the context differences (e.g., setting, outcomes), findings in this review were contrary to those of previous studies. Seral-Cortes et al. [31] found that reporting of process evaluation measures was associated with significantly decreased BMI. Similarly, Ma et al. [30] claimed that the inclusion of a process evaluation aim tended to benefit the overall effectiveness of motor competence programmes.
Several explanations have been proposed for a better understanding of the counter intuitive findings. First, both studies with and without process evaluation were no longer significant with respect to CRF and body composition improvement after removing high risk of bias studies. This observation suggests that some of the high risk of bias studies might have distorted the overall effectiveness. Indeed, previous work has shown that higher risk of bias is associated with exaggerated (approximately 10%) treatment effects [128]. Given that 21/23 and 17/19 interventions in studies without process evaluation group for CRF and body composition respectively were appraised as either high risk or some concerns (see Figs. 2 and 3), there is a possibility that the effect size of these two outcomes in studies without process evaluation may have been overestimated.
Second, the studies included in this review had a disproportionately larger number of participants in the studies with process evaluation group (n = 8, participants = 17,774) compared to the studies without process evaluation group (n = 25, participants = 2,552), which may have contributed to the discrepancy in intervention effectiveness. Indeed, it is reported that when interventions are conducted at larger scales, they may experience a 'scale-up penalty' or 'voltage drop', where the effectiveness of the intervention diminishes due to adaptations made to accommodate the contexts [129, 130]. In agreement with this, the current review revealed that reporting of adaptation is associated with lower improvement in CRF (β = -0.34, p = 0.05) compared to studies that did not report adaptation. Third, studies with process evaluation group were mostly cluster-RCTs and utilised exercise modalities other than running/cycling, which were associated with lower improvements in CRF and body composition compared to the studies without process evaluation (Tables 6 and 7). It is, therefore, conceivable that process evaluation is unlikely the only reason, or not responsible, for intervention ineffectiveness. Fourth, it is worth considering that process evaluation may be independent of outcome evaluation if the intervention is conducted without a prescribed process evaluation aim and without the support of a process evaluation framework. This is supported by Ma et al. [30], who found that including a process evaluation aim tended to benefit the overall effectiveness of motor competence programmes. Thus, it seems plausible that process evaluation did not contribute to the outcome assessments in the current review since only one study [37] adopted a process evaluation framework. Nevertheless, future studies are encouraged to further explore the relationship between process and outcome evaluation.
Effects of HIIT characteristics
The current review showed that studies conducted among overweight and obese cohort were associated with favourable intervention effects on CRF (β = 0.66, p = 0.01) and body composition (β = -0.93, p = 0.01) compared to studies without specifying weight status. This is in agreement with previous reviews [18, 22], which have demonstrated that overweight and obesity significantly mediates CRF, waist circumference, percentage body fat and BMI in school-based HIIT interventions targeting children and adolescents. Hence, HIIT may be a particular effective and beneficial form of exercise for this “at-risk” cohort [131, 132].
Previous school-based HIIT reviews have shown that running- or cycling-based HIIT was the most adopted modality [18, 20, 22]. Despite this, our review is the first to systematically compare the differences between the traditional running/cycling HIIT and other HIIT modalities (e.g., resistance-based HIIT). The pooled evidence suggested that running/cycling HIIT was superior in improving CRF and body composition, but not muscular strength, compared to other modalities. This finding corroborated the speculation made by Costigan et al. [11] that cycling/running-based HIIT was likely to improve CRF, rather than muscular strength, due to the lack of training specificity.
The current review found that shorter intervention duration elicited higher CRF improvement. This is consistent with Leahy et al. [133], where they concluded that shorter intervention duration emerged as a better predictor of well-being. In addition, Ma et al. [30] suggested that a shorter intervention duration led to greater effects on motor competence, proposing that longer interventions were more susceptible to interruptions and less supported. This assertion is supported by some of the studies included in the current review, indicating that extended interventions are associated with high drop-out rates and diminished implementation quality (e.g., inadequate exercise intensity monitoring and reduced dose delivery) [43, 53].
Interestingly, the pooled HR data revealed that lower HR was associated with significantly higher improvement in CRF, whereas no effects for body composition and muscular strength were observed. However, given the relatively low effect size (β = -0.01, p = 0.01), we speculate that HR induces no effects on the intervention outcomes once a certain level is reached (above 70% in the current review). This is supported by McKay et al. [134] and Schaun et al. [135] in which they stated that the magnitude of CRF would not be influenced by intensity once it is above 60% VO2max, despite their conclusion being based upon young adults.
Strengths and limitations
This is the first review exploring the implementation process of school-based HIIT interventions in children and adolescents. The comprehensive literature search and combination of all possible outcomes regarding CRF, body composition and muscular strength contribute to the complete and overarching findings of the current school-based HIIT review. There are some limitations within this review. Since few studies had specified the process evaluation measures, most of the measures are subjectively assessed by authors. Although a second author in our review has checked for the accuracy and consistency of the judgements, disagreements may still exist from a reader’s point of view. To minimise author bias, the current review adopted the MRC process evaluation framework [24], combined with study by Ma et al. [30] for process evaluation. However, currently there is no single definition of process evaluation. The results may be different if another framework is adopted. Nevertheless, the MRC framework is probably one of the most comprehensive process evaluation guidance in the literature [136]. In addition, the preferential orders of data extraction for outcome variables in Table 1 is based on the understanding of authors in the present review. Consequently, it is essential to admit that these decisions may involve nuanced considerations. Finally, the results for all the outcomes showed significant methodological and statistical heterogeneity and publication bias, therefore future studies should interpret these results with caution.
Conclusion
The extent of process evaluation in school-based HIIT interventions remains low, especially for the domains of adaptation, mediator, dose received, response, barriers, facilitators, and contamination. Even when interventions were conducted with the purpose of process evaluation, they generally lacked theoretical rigour. The present review suggests that process evaluation was not related to outcome evaluation and did not contribute to achieving better treatment effects. However, incorporating process evaluation into RCTs may be beneficial in providing comprehensive implementation details, which aids in interpreting intervention effectiveness and functioning. Ultimately, this will contribute to the scaling up and translation to other school-based HIIT interventions. Therefore, future school-based HIIT interventions are highly recommended to report process evaluation under the guidance of a theoretical framework.
Adaptations from protocol
The sentence “cardiorespiratory fitness (20 m shuttle run in laps finished), body composition (BMI), strength (push-ups in times and standing long jump in meters) and blood pressure (mmHg)” in the protocol was changed to “cardiorespiratory fitness (e.g., 20 m shuttle run in laps finished), body composition (e.g., BMI), strength (e.g., push-ups in times and standing long jump in meters) and blood pressure (mmHg)”. In addition, the initial process of risk of bias assessments, conducted by two independent authors (YL and CW), was modified. The first author (YL) performed the risk of bias assessment, and the accuracy of the assessment was subsequently verified by a second author (CW) through a random sub-sample (30%) of studies, with less than 80% of consensus triggered a check for all the studies.
Availability of data and materials
All data generated or analysed during this study are included in this article.
Abbreviations
- HIIT:
-
High-intensity interval training
- CRF:
-
Cardiorespiratory fitness
- PA:
-
Physical activity
- MVPA:
-
Moderate-to-vigorous physical activity
- VPA:
-
Vigorous physical activity
- RCT:
-
Randomised controlled trial
- HRmax:
-
Maximum heart rate
- VO2peak:
-
Peak oxygen uptake
- BMI:
-
Body mass index
- SD:
-
Standard deviation
- SMD:
-
Standard mean difference
- MAS:
-
Maximum aerobic fitness
- RPE:
-
Rating of perceived exertion
References
Neil-Sztramko SE, Caldwell H, Dobbins M. School-based physical activity programs for promoting physical activity and fitness in children and adolescents aged 6 to 18. Cochrane Database Syst Rev. 2021;9:CD007651.
He Z, Wu H, Yu F, Fu J, Sun S, Huang T, et al. Effects of Smartphone-Based Interventions on Physical Activity in Children and Adolescents: Systematic Review and Meta-analysis. JMIR Mhealth Uhealth. 2021;9(2):e22601.
Chaput JP, Willumsen J, Bull F, Chou R, Ekelund U, Firth J, et al. 2020 WHO guidelines on physical activity and sedentary behaviour for children and adolescents aged 5–17 years: summary of the evidence. Int J Behav Nutr Phys Act. 2020;17(1):141.
Carter T, Pascoe M, Bastounis A, Morres ID, Callaghan P, Parker AG. The effect of physical activity on anxiety in children and young people: a systematic review and meta-analysis. J Affect Disord. 2021;285:10–21.
Aubert S, Barnes JD, Demchenko I, Hawthorne M, Abdeta C, Abi Nader P, et al. Global Matrix 4.0 Physical Activity Report Card Grades for Children and Adolescents: Results and Analyses From 57 Countries. J Phys Act Health. 2022;19(11):700–28.
Stockwell S, Trott M, Tully M, Shin J, Barnett Y, Butler L, et al. Changes in physical activity and sedentary behaviours from before to during the COVID-19 pandemic lockdown: a systematic review. BMJ Open Sport Exerc Med. 2021;7(1):e000960.
Hollis JL, Williams AJ, Sutherland R, Campbell E, Nathan N, Wolfenden L, et al. A systematic review and meta-analysis of moderate-to-vigorous physical activity levels in elementary school physical education lessons. Prev Med. 2016;86:34–54.
Brazendale K, Beets MW, Weaver RG, Pate RR, Turner-McGrievy GM, Kaczynski AT, et al. Understanding differences between summer vs. school obesogenic behaviors of children: the structured days hypothesis. Int J Behav Nutr Phys Act. 2017;14(1):100.
Metcalf B, Henley W, Wilkin T. Effectiveness of intervention on physical activity of children: systematic review and meta-analysis of controlled trials with objectively measured outcomes (EarlyBird 54). BMJ. 2012;345:e5888.
Love R, Adams J, van Sluijs EMF. Are school-based physical activity interventions effective and equitable? A meta-analysis of cluster randomized controlled trials with accelerometer-assessed activity. Obes Rev. 2019;20(6):859–70.
Costigan SA, Eather N, Plotnikoff RC, Taaffe DR, Lubans DR. High-intensity interval training for improving health-related fitness in adolescents: a systematic review and meta-analysis. Br J Sports Med. 2015;49(19):1253–61.
Hall WJ, Schneider M, Thompson D, Volpe SL, Steckler A, Hall JM, et al. School factors as barriers to and facilitators of a preventive intervention for pediatric type 2 diabetes. Transl Behav Med. 2014;4(2):131–40.
Ekkekakis P, Vallance J, Wilson PM, Ewing Garber C. Extraordinary claims in the literature on high-intensity interval training (HIIT): III. Critical analysis of four foundational arguments from an interdisciplinary lens. Psychol Sport Exerc. 2023;66:102399.
Lubans DR, Eather N, Smith JJ, Beets MW, Harris NK. Scaling-up Adolescent High-Intensity Interval Training Programs for Population Health. Exerc Sport Sci Rev. 2022;50(3):128–36.
Malik, Williams CA, Weston KL, Barker AR. Perceptual Responses to High- and Moderate-Intensity Interval Exercise in Adolescents. Medicine & Science in Sports & Exercise. 2018;50(5):1021–30.
Hay J, Maximova K, Durksen A, Carson V, Rinaldi RL, Torrance B, et al. Physical Activity Intensity and Cardiometabolic Risk in Youth. ARCH PEDIATR ADOLESC MED. 2012;166(NO 11):1022–9.
Carson V, Rinaldi RL, Torrance B, Maximova K, Ball GDC, Majumdar SR, et al. Vigorous physical activity and longitudinal associations with cardiometabolic risk factors in youth. Int J Obes. 2014;38(1):16–21.
Duncombe SL, Barker AR, Bond B, Earle R, Varley-Campbell J, Vlachopoulos D, et al. School-based high-intensity interval training programs in children and adolescents: A systematic review and meta-analysis. PLoS One. 2022;17(5):e0266427.
Bauer N, Sperlich B, Holmberg HC, Engel FA. Effects of High-Intensity Interval Training in School on the Physical Performance and Health of Children and Adolescents: A Systematic Review with Meta-Analysis. Sports Med Open. 2022;8(1):50.
Zapata-Lamana R, Cigarroa Cuevas I, Fuentes V, Soto Espindola C, Parrado Romero E, Sepulveda C, et al. HIITing Health in School: Can High Intensity Interval Training Be a Useful and Reliable Tool for Health on a School-Based Enviroment? A Systematic Review. Int J School Health. 2019;6(3):1–10.
Delgado-Floody P, Latorre-Román P, Jerez-Mayorga D, Caamaño-Navarrete F, García-Pinillos F. Feasibility of incorporating high-intensity interval training into physical education programs to improve body composition and cardiorespiratory capacity of overweight and obese children: A systematic review. J Exerc Sci Fit. 2019;17(2):35–40.
da Silva Bento AF, Páez LC, de Mendonça Raimundo AM. School-based high-intensity interval training programs for promoting physical activity and fitness in adolescents: A systematic review. J Teach Phys Educ. 2021;41(2):288–300.
Bond B, Weston KL, Williams CA, Barker AR. Perspectives on high-intensity interval exercise for health promotion in children and adolescents. Open Access J Sports Med. 2017;8:243–65.
Moore GF, Audrey S, Barker M, Bond L, Bonell C, Hardeman W, et al. Process evaluation of complex interventions: Medical Research Council guidance. BMJ. 2015;350:h1258.
McIntyre SA, Francis JJ, Gould NJ, Lorencatto F. The use of theory in process evaluations conducted alongside randomized trials of implementation interventions: A systematic review. Transl Behav Med. 2020;10(1):168–78.
Hariton E, Locascio JJ. Randomised controlled trials - the gold standard for effectiveness research: Study design: randomised controlled trials. BJOG. 2018;125(13):1716.
Grant A, Treweek S, Dreischulte T, Foy R, Guthrie B. Process evaluations for cluster-randomised trials of complex interventions: a proposed framework for design and reporting. Trials. 2013;14:15.
Baranowski T, Stables G. Process Evaluations of the 5-a-Day Projects. Health Educ Behav. 2000;27(2):157–66.
Linnan L, Steckler A. Process Evaluation for Public Health Interventions and Research. Jossey-Bass. 2002:1–24.
Ma J, Lander N, Eyre ELJ, Barnett LM, Essiet IA, Duncan MJ. It’s Not Just What You Do but the Way You Do It: A Systematic Review of Process Evaluation of Interventions to Improve Gross Motor Competence. Sports Med. 2021;51(12):2547–69.
Seral-Cortes M, De Miguel-Etayo P, Zapata P, Miguel-Berges ML, Moreno LA. Effectiveness and process evaluation in obesity and type 2 diabetes prevention programs in children: a systematic review and meta-analysis. BMC Public Health. 2021;21(1):348.
Getachew-Smith H, King AJ, Marshall C, Scherr CL. Process Evaluation in Health Communication Media Campaigns: A Systematic Review. Am J Health Promot. 2022;36(2):367–78.
Costigan SA, Eather N, Plotnikoff RC, Taaffe DR, Pollock E, Kennedy SG, et al. Preliminary efficacy and feasibility of embedding high intensity interval training into the school day: A pilot randomized controlled trial. Prev Med Rep. 2015;2:973–9.
Martínez-Vizcaíno V, Soriano-Cano A, Garrido-Miguel M, Cavero-Redondo I, de Medio EP, Madrid VM, et al. The effectiveness of a high-intensity interval games intervention in schoolchildren: A cluster-randomized trial. Scand J Med Sci Sports. 2022;32(4):765–81.
Ricci JM, Currie KD, Astorino TA, Erickson K, Pfeiffer KA. Program Evaluation and Preliminary Efficacy of Fitness and Skill-Based High-Intensity Interval Training in Physical Education. Res Q Exerc Sport. 2023;94(4):1042–52.
Harris N, Warbrick I, Atkins D, Vandal A, Plank L, Lubans DR. Feasibility and Provisional Efficacy of Embedding High-Intensity Interval Training Into Physical Education Lessons: A Pilot Cluster-Randomized Controlled Trial. Pediatr Exerc Sci. 2021;33(4):186–95.
Kennedy SG, Leahy AA, Smith JJ, Eather N, Hillman CH, Morgan PJ, et al. Process Evaluation of a School-Based High-Intensity Interval Training Program for Older Adolescents: The Burn 2 Learn Cluster Randomised Controlled Trial. Children (Basel). 2020;7(12):299.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. PLoS Med. 2021;18(3):e1003583.
Higgins J, Thomas J, Chandler J, Cumpston M, Li TJ, Page M, et al. Cochrane Handbook for Systematic Reviews of Interventions: The Cochrane Collaboration and John Wiley & Sons Ltd; 2019.
Buchheit M, Laursen PB. High-intensity interval training, solutions to the programming puzzle. Part II: anaerobic energy, neuromuscular load and practical applications. Sports Med. 2013;43(10):927–54.
Sampson M, McGowan J, Cogo E, Grimshaw J, Moher D, Lefebvre C. An evidence-based practice guideline for the peer review of electronic search strategies. J Clin Epidemiol. 2009;62(9):944–52.
Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan—a web and mobile app for systematic reviews. Syst Rev. 2016;5(1):210.
Wassenaar TM, Wheatley CM, Beale N, Nichols T, Salvan P, Meaney A, et al. The effect of a one-year vigorous physical activity intervention on fitness, cognitive performance and mental health in young adolescents: the Fit to Study cluster randomised controlled trial. Int J Behav Nutr Phys Act. 2021;18(1):1–15.
Harris N, Warbrick I, Fleming T, Borotkanics R, Atkins D, Lubans D. Impact of high-intensity interval training including Indigenous narratives on adolescents’ mental health: a cluster-randomised controlled trial. Aust N Z J Public Health. 2022;46(6):794–9.
Oliveira RS, Barker AR, Kranen SH, Debras F, Williams CA. Effects of High-Intensity Interval Training on the Vascular and Autonomic Components of the Baroreflex at Rest in Adolescents. Pediatr Exerc Sci. 2021:1–7.
Martinez-Vizcaino V, Soriano-Cano A, Garrido-Miguel M, Cavero-Redondo I, de Medio EP, Madrid VM, et al. The effectiveness of a high-intensity interval games intervention in schoolchildren: a cluster randomized trial. Scand J Med Sci Sports. 2021.
Logan GR, Harris N, Duncan S, Plank LD, Merien F, Schofield G. Low-Active Male Adolescents: A Dose Response to High-Intensity Interval Training. Med Sci Sports Exerc. 2016;48(3):481–90.
Engel FA, Wagner MO, Schelhorn F, Deubert F, Leutzsch S, Stolz A, et al. Classroom-Based Micro-Sessions of Functional High-Intensity Circuit Training Enhances Functional Strength but Not Cardiorespiratory Fitness in School Children-A Feasibility Study. Front Public Health. 2019;7:291.
Ruiz-Ariza A, Suárez-Manzano S, López-Serrano S, Martínez-López EJ. The effect of cooperative high-intensity interval training on creativity and emotional intelligence in secondary school: A randomised controlled trial. Eur Phys Educ Rev. 2017;25(2):355–73.
Lubans DR, Smith JJ, Eather N, Leahy AA, Morgan PJ, Lonsdale C, et al. Time-efficient intervention to improve older adolescents’ cardiorespiratory fitness: findings from the “Burn 2 Learn” cluster randomised controlled trial. Br J Sports Med. 2020;55(13):751–8.
McNarry MA, Lewis MJ, Wade N, Davies GA, Winn C, Eddolls WTB, et al. Effect of asthma and six-months high-intensity interval training on heart rate variability during exercise in adolescents. J Sports Sci. 2019;37(19):2228–35.
Moreau D, Kirk IJ, Waldie KE. High-intensity training enhances executive function in children in a randomized, placebo-controlled trial. ELife. 2017;6.
Takehara K, Togoobaatar G, Kikuchi A, Lkhagvasuren G, Lkhagvasuren A, Aoki A, et al. Exercise Intervention for Academic Achievement Among Children: A Randomized Controlled Trial. Pediatrics. 2021;148(5):1–10.
Wan X, Wang W, Liu J, Tong T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol. 2014;14:135.
Popowczak M, Rokita A, Kozlenia D, Domaradzki J. The high-intensity interval training introduced in physical education lessons decrease systole in high blood pressure adolescents. Sci Rep. 2022;12(1):1974.
Sterne JAC, Savovic J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898.
Cohen J. Statistical power analysis for the behavioral sciences (2nd ed.): Hillsdale, NJ: Erlbaum; 1988.
Egger M, Smith GD, Schneider M. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315:629–34.
StataCorp. Stata Statistical Software: Release 17. College Station, TX: StataCorp LLC; 2021.
Wheatley C, Beale N, Wassenaar T, Graham M, Eldridge E, Dawes H, et al. Fit to Study: Reflections on designing and implementing a large-scale randomized controlled trial in secondary schools. Trends Neurosci Educ. 2020;20:100134.
Sharp CA, McNarry MA, Eddolls WTB, Koorts H, Winn CON, Mackintosh KA. Identifying facilitators and barriers for adolescents participating in a school-based HIIT intervention: the eXercise for asthma with commando Joe’s® (X4ACJ) programme. BMC Public Health. 2020;20(1):1–11.
Alberto A. 24 sessions of monitored cooperative high-intensity interval training improves attention-concentration and mathematical calculation in secondary school. J Phys Educ Sport. 2018;18(3):1572–82.
Winn CON, Mackintosh KA, Eddolls WTB, Stratton G, Wilson AM, McNarry MA, et al. Effect of high-intensity interval training in adolescents with asthma: The eXercise for Asthma with Commando Joe’s (R) (X4ACJ) trial. J Sport Health Sci. 2021;10(4):488–98.
McNarry MA, Lester L, Ellins EA, Halcox JP, Davies G, Winn CON, et al. Asthma and high-intensity interval training have no effect on clustered cardiometabolic risk or arterial stiffness in adolescents. Eur J Appl Physiol. 2021;121(7):1967–78.
McNarry MA, Winn CON, Davies GA, Eddolls WTB, Mackintosh KA. Effect of High-Intensity Training and Asthma on the V O2 Kinetics of Adolescents. Med Sci Sports Exerc. 2020;52(6):1322–9.
Winn CO, Mackintosh KA, Eddolls WT, Stratton G, Wilson AM, Rance JY, Doull IJ, McNarry MA, Davies GA. Perceptions of asthma and exercise in adolescents with and without asthma. J Asthma. 2018;55(8):868–76.
Williams AC, Armstrong N, Powell J. Aerobic responses of prepubertal boys to two modes of training. Br J Sports Med. 2000;34:168–73.
Martínez SR, Ríos LJC, Tamayo IM, Almeida LG, López-Gomez MA, Jara CC. An After-School, high-intensity, interval physical activity programme improves health-related fitness in children. Motriz Revista Educacao Fisica. 2016;22(4):359–67.
Leahy AA, Eather N, Smith JJ, Hillman CH, Morgan PJ, Plotnikoff RC, et al. Feasibility and Preliminary Efficacy of a Teacher-Facilitated High-Intensity Interval Training Intervention for Older Adolescents. Pediatr Exerc Sci. 2019;31(1):107–17.
Leahy AA, Eather N, Smith JJ, Hillman C, Morgan PJ, Nilsson M, et al. School-based physical activity intervention for older adolescents: rationale and study protocol for the Burn 2 Learn cluster randomised controlled trial. BMJ Open. 2019;9(5):e026029.
Leahy AA, Michels MFI, Eather N, Hillman CH, Shigeta TT, Lubans DR, et al. Feasibility of test administration and preliminary findings for cognitive control in the Burn 2 learn pilot randomised controlled trial. J Sports Sci. 2020;38(15):1708–16.
Mavilidi MF, Mason C, Leahy AA, Kennedy SG, Eather N, Hillman CH, et al. Effect of a Time-Efficient Physical Activity Intervention on Senior School Students’ On-Task Behaviour and Subjective Vitality: the “Burn 2 Learn” Cluster Randomised Controlled Trial. Educ Psychol Rev. 2021;33(1):299–323.
Valkenborghs SR, Hillman CH, Al-Iedani O, Nilsson M, Smith JJ, Leahy AA, et al. Effect of high-intensity interval training on hippocampal metabolism in older adolescents. Psychophysiology. 2022;59(11):e14090.
Mucci P, Baquet G, Nourry C, Deruelle F, Berthoin S, Fabre C. Exercise testing in children: comparison in ventilatory thresholds changes with interval-training. Pediatr Pulmonol. 2013;48(8):809–16.
Nourry C, Deruelle F, Guinhouya C, Baquet G, Fabre C, Bart F, et al. High-intensity intermittent running training improves pulmonary function and alters exercise breathing pattern in children. Eur J Appl Physiol. 2005;94(4):415–23.
Baquet G, Guinhouya C, Dupont G, Nourry C, Berthoin S. Effects of a short-term interval training program on physical fitness in prepubertal children. J Strength Cond Res. 2004;18(4):708–13.
Baquet G, Gamelin F, Mucci P, Thevenet D, Paraagh VE, Berthoin S. Continuous vs. interval aerobic training in 8-11-year-old children. J Strength Cond Res. 2010;24(5):1381–8.
Ángel Latorre-Román P, Berrios-Aguayo B, Aragón-Vela J, Pantoja-Vallejo A. Effects of a 10-week active recess program in school setting on physical fitness, school aptitudes, creativity and cognitive flexibility in elementary school children. A randomised-controlled trial. J Sports Sci. 2021;39(11):1277–86.
Chuensiri N, Suksom D, Tanaka H. Effects of High-Intensity Intermittent Training on Vascular Function in Obese Preadolescent Boys. Child Obes. 2018;14(1):41–9.
Camacho-Cardenosa A, Brazo-Sayavera J, Camacho-Cardenosa M, Marcos-Serrano M, Timón R, Olcina G. Effects of High Intensity Interval Training on Fat Mass Parameters in Adolescents. Rev Esp Salud Publica. 2016;90:e1–9.
Racil G, Ben Ounis O, Hammouda O, Kallel A, Zouhal H, Chamari K, et al. Effects of high vs. moderate exercise intensity during interval training on lipids and adiponectin levels in obese young females. Eur J Appl Physiol. 2013;113(10):2531–40.
Stenman M, Pesola AJ, Laukkanen A, Haapala EA. Effects of Two-Week High-Intensity Interval Training on Cognition in Adolescents – A Randomized Controlled Pilot Study. Hum Mov. 2017;18(2):15–20.
Costigan S, Eather N, Plotnikoff R, Hillman C, Lubans D. High intensity interval training on cognitive and mental health in adolescents. J Sci Med Sport. 2017;20:e108–9.
Costigan SA, Ridgers ND, Eather N, Plotnikoff RC, Harris N, Lubans DR. Exploring the impact of high intensity interval training on adolescents’ objectively measured physical activity: Findings from a randomized controlled trial. J Sports Sci. 2018;36(10):1087–94.
Takehara K, Ganchimeg T, Kikuchi A, Gundegmaa L, Altantsetseg L, Aoki A, et al. The effectiveness of exercise intervention for academic achievement, cognitive function, and physical health among children in Mongolia: a cluster RCT study protocol. BMC Public Health. 2019;19(1):697.
Larsen MN, Nielsen CM, Orntoft C, Randers MB, Helge EW, Madsen M, et al. Fitness Effects of 10-Month Frequent Low-Volume Ball Game Training or Interval Running for 8–10-Year-Old School Children. Biomed Res Int. 2017;2017:2719752.
Elbe A-M, Wikman JM, Zheng M, Larsen MN, Nielsen G, Krustrup P. The importance of cohesion and enjoyment for the fitness improvement of 8–10-year-old children participating in a team and individual sport school-based physical activity intervention. Eur J Sport Sci. 2017;17(3):343–50.
Larsen MN, Nielsen CM, Helge EW, Madsen M, Manniche V, Hansen L, et al. Positive effects on bone mineralisation and muscular fitness after 10 months of intense school-based physical training for children aged 8–10 years: the FIT FIRST randomised controlled trial. Br J Sports Med. 2016;52(4):254–60.
Alonso-Fernández D, Fernández-Rodríguez R, Taboada-Iglesias Y, Gutiérrez-Sánchez Á. Impact of a HIIT protocol on body composition and VO2max in adolescents. Sci Sports. 2019;34(5):341–7.
McManus AM, Cheng CH, Leung MP, Yung TC, Macfarlane DJ. Improving aerobic power in primary school boys: a comparison of continuous and interval training. Int J Sports Med. 2005;26(9):781–6.
Racil G, Zouhal H, Elmontassar W, Abderrahmane AB, De Sousa MV, Chamari K, et al. Plyometric exercise combined with high-intensity interval training improves metabolic abnormalities in young obese females more so than interval training alone. Appl Physiol Nutr Metab. 2016;41(1):103–9.
Lambrick D, Westrupp N, Kaufmann S, Stoner L, Faulkner J. The effectiveness of a high-intensity games intervention on improving indices of health in young children. J Sports Sci. 2016;34(3):190–8.
McNarry MA, Lambrick D, Westrupp N, Faulkner J. The influence of a six-week, high-intensity games intervention on the pulmonary oxygen uptake kinetics in prepubertal obese and normal-weight children. Appl Physiol Nutr Metab. 2015;40(10):1012–8.
Martínez-Vizcaíno V, Álvarez-Bueno C, Cavero-Redondo I, Pozuelo-Carrascosa DP, Garrido-Miguel M, Martínez-Hortelano JA, et al. MOVI-daFIT! Intervention: Rationale and design of a cluster randomized controlled trial testing the effects on improving adiposity, cognition, and subclinical atherosclerosis by increasing cardiorespiratory fitness in children. Medicine (Baltimore). 2019;98(9):e14737.
Haghshenas R, Jamshidi Z, Doaei S, Gholamalizadeh M. The Effect of a High-intensity Interval Training on Plasma Vitamin D Level in Obese Male Adolescents. Indian J Endocrinol Metab. 2019;23(1):72–5.
Wassenaar TM, Wheatley CM, Beale N, Salvan P, Meaney A, Possee JB, et al. Effects of a programme of vigorous physical activity during secondary school physical education on academic performance, fitness, cognition, mental health and the brain of adolescents (Fit to Study): study protocol for a cluster-randomised trial. Trials. 2019;20(1):189.
Tian X, Fu J, Tian J, Yang Y, Liang W, Fan W, et al. The Efficacy of Brief School-Based Exercise Programs in Improving Pubertal Bone Mass and Physical Fitness: A Randomized Controlled Trial. Int J Environ Res Public Health. 2021;18(18):9648.
Domaradzki J, Cichy I, Rokita A, Popowczak M. Effects of Tabata Training During Physical Education Classes on Body Composition, Aerobic Capacity, and Anaerobic Performance of Under-, Normal- and Overweight Adolescents. Int J Environ Res Public Health. 2020;17(3):876.
Domaradzki J, Rokita A, Koźlenia D, Popowczak M. Optimal Values of Body Composition for the Lowest Risk of Failure in Tabata Training's Effects in Adolescents: A Pilot Study. Biomed Res Int. 2021:1–7.
Domaradzki J, Koźlenia D, Popowczak M. Sex Moderated Mediation of the Musculoskeletal Fitness in Relationship between High-Intensive Interval Training Performing during Physical Education Classes and Cardiorespiratory Fitness in Healthy Boys and Girls. Biomed Res Int. 2022;2022:8760620.
Domaradzki J, Kozlenia D, Popowczak M. The Mediation Role of Fatness in Associations between Cardiorespiratory Fitness and Blood Pressure after High-Intensity Interval Training in Adolescents. Int J Environ Res Public Health. 2022;19(3):1–14.
Domaradzki J, Kozlenia D, Popowczak M. Prevalence of Positive Effects on Body Fat Percentage, Cardiovascular Parameters, and Cardiorespiratory Fitness after 10-Week High-Intensity Interval Training in Adolescents. Biology (Basel). 2022;11(3):424.
Domaradzki J, Kozlenia D, Popowczak M. The Relative Importance of Age at Peak Height Velocity and Fat Mass Index in High-Intensity Interval Training Effect on Cardiorespiratory Fitness in Adolescents: A Randomized Controlled Trial. Children (Basel). 2022;9(10):1554.
Domaradzki J, Kozlenia D, Popowczak M. Mediation effect of cardiorespiratory fitness on relationships between high-intensity interval training and body fat in overweight and obese adolescents. J Sports Med Phys Fitness. 2022;62(12):1735–41.
Boddy LM, Stratton G, Hackett AF, George KP. The effectiveness of a ‘short, sharp, shock’ high intensity exercise intervention in 11- and 12-year-old Liverpool schoolgirls. Arch Ex Health Dis. 2010;1:19–25.
McManus A, Armstrong N, William CA. Effect of training on the aerobic power and anaerobic performance of prepubertal girls. Acta Paediatr. 1997;86:456–9.
Reyes Amigo TR, Labisa-Palmeira A. Moderators of the effect of high-intensity and moderate-intensity games in schoolchildren on cardiorespiratory fitness and body composition. Motricidade. 2020;16(2):156–69.
Reyes-Amigo T, Molina JS, Martinez Mera G, De Souza LJ, Ibarra Mora J, Soto-SÁNchez J. Contribution of high and moderate-intensity physical education classes to the daily physical activity level in children. J Phys Educ Sport. 2021;21(1):29–35.
Cao M, Tang Y, Zou Y. Integrating High-Intensity Interval Training into a School Setting Improve Body Composition, Cardiorespiratory Fitness and Physical Activity in Children with Obesity: A Randomized Controlled Trial. J Clin Med. 2022;11(18):5436.
Meng C, Yucheng T, Shu L, Yu Z. Effects of school-based high-intensity interval training on body composition, cardiorespiratory fitness and cardiometabolic markers in adolescent boys with obesity: a randomized controlled trial. BMC Pediatr. 2022;22(1):112.
Bogataj S, Trajkovic N, Cadenas-Sanchez C, Sember V. Effects of School-Based Exercise and Nutrition Intervention on Body Composition and Physical Fitness in Overweight Adolescent Girls. Nutrients. 2021;13(1):238.
Gamelin F-X, Baquet G, Berthoin S, Thevenet D, Nourry C, Nottin S, et al. Effect of high intensity intermittent training on heart rate variability in prepubescent children. Eur J Appl Physiol. 2009;105(5):731–8.
Ketelhut S, Kircher E, Ketelhut SR, Wehlan E, Ketelhut K. Effectiveness of Multi-activity, High-intensity Interval Training in School-aged Children. Int J Sports Med. 2020;41(4):227–32.
Cvetković N, Stojanović E, Stojiljković N, Nikolić D, Milanović Z. Effects of a 12 Week Recreational Football and High-Intensity Interval Training on Physical Fitness in Overweight Children. Physical Education and Sport: Facta Universitatis, Series; 2018.
Cvetković N, Stojanović E, Stojiljković N, Nikolić D, Scanlan AT, Milanović Z. Exercise training in overweight and obese children: Recreational football and high-intensity interval training provide similar benefits to physical fitness. Scand J Med Sci Sports. 2018;28:18–32.
Racil G, Coquart JB, Elmontassar W, Haddad M, Goebel R, Chaouachi A, et al. Greater effects of high-compared with moderate-intensity interval training on cardio-metabolic variables, blood leptin concentration and ratings of perceived exertion in obese adolescent females. Biol Sport. 2016;33(2):145–52.
Abassi W, Ouerghi N, Nikolaidis PT, Hill L, Racil G, Knechtle B, Feki M, Bouassida A. Interval training with different intensities in overweight/obese adolescent females. Int J Sports Med. 2022;43(05):434–43.
Abassi W, Ouerghi N, Ghouili H, Haouami S, Bouassida A. Greater effects of high- compared with moderate-intensity interval training on thyroid hormones in overweight/obese adolescent girls. Horm Mol Biol Clin Investig. 2020;41(4).
Williams RA, Dring KJ, Morris JG, Sunderland C, Nevill ME, Cooper SB. Effect of two-weeks of school-based sprint training on physical fitness, risk factors for cardiometabolic diseases and cognitive function in adolescent girls: A randomized controlled pilot trial. Front Sports Act Living. 2022;4:884051.
Bossmann T, Woll A, Wagner I. Effects of Different Types of High-Intensity Interval Training (HIIT) on Endurance and Strength Parameters in Children and Adolescents. Int J Environ Res Public Health. 2022;19(11):6855.
McKay H, Naylor PJ, Lau E, Gray SM, Wolfenden L, Milat A, et al. Implementation and scale-up of physical activity and behavioural nutrition interventions: an evaluation roadmap. Int J Behav Nutr Phys Act. 2019;16(1):102.
Carroll C, Patterson M, Wood S, Booth A, Rick J, Balain S. A conceptual framework for implementation fidelity. Implement Sci. 2007;2:40.
Montgomery P, Underhill K, Gardner F, Operario D, Mayo-Wilson E. The Oxford Implementation Index: a new tool for incorporating implementation data into systematic reviews and meta-analyses. J Clin Epidemiol. 2013;66(8):874–82.
Coates AM, Joyner MJ, Little JP, Jones AM, Gibala MJ. A Perspective on High-Intensity Interval Training for Performance and Health. Sports Med. 2023;53(Suppl 1):85–96.
Liu Y, Williams CA, Weston KL, Duncombe SL, Malik AA, Barker AR. Validation and calibration for embedding rating of perceived exertion into high-intensity interval exercise in adolescents: a lab-based study. Pediatric Exercise Sci. 2024;1(aop):1–7.
Duncombe SL, Stylianou M, Price L, Walker JL, Barker AR. Making a HIIT: Methods for quantifying intensity in high-intensity interval training in schools and validity of session rating of perceived exertion. J Sports Sci. 2023;41(18):1678–86.
Eather N, Babic M, Riley N, Costigan SA, Lubans DR. Impact of Embedding High-Intensity Interval Training in Schools and Sports Training on Children and Adolescent’s Cardiometabolic Health and Health-Related Fitness: Systematic Review and Meta-Analysis. J Teach Phys Educ. 2022:1–13.
Savovic J, Turner RM, Mawdsley D, Jones HE, Beynon R, Higgins JPT, et al. Association Between Risk-of-Bias Assessments and Results of Randomized Trials in Cochrane Reviews: The ROBES Meta-Epidemiologic Study. Am J Epidemiol. 2018;187(5):1113–22.
Lane C, McCrabb S, Nathan N, Naylor PJ, Bauman A, Milat A, et al. How effective are physical activity interventions when they are scaled-up: a systematic review. Int J Behav Nutr Phys Act. 2021;18(1):16.
Kennedy SG, Sanders T, Estabrooks PA, Smith JJ, Lonsdale C, Foster C, et al. Implementation at-scale of school-based physical activity interventions: A systematic review utilizing the RE-AIM framework. Obes Rev. 2021;22(7):e13184.
García-Hermoso A, Cerrillo-Urbina AJ, Herrera-Valenzuela T, Cristi-Montero C, Saavedra JM, Martínez-Vizcaíno V. Is high-intensity interval training more effective on improving cardiometabolic risk and aerobic capacity than other forms of exercise in overweight and obese youth? A meta-analysis. Obesity Rev. 2016;17(6):531–40.
Liu J, Zhu L, Su Y. Comparative Effectiveness of High-Intensity Interval Training and Moderate-Intensity Continuous Training for Cardiometabolic Risk Factors and Cardiorespiratory Fitness in Childhood Obesity: A Meta-Analysis of Randomized Controlled Trials. Front Physiol. 2020;11:214.
Leahy AA, Mavilidi MF, Smith JJ, Hillman CH, Eather N, Barker D, et al. Review of High-Intensity Interval Training for Cognitive and Mental Health in Youth. Med Sci Sports Exerc. 2020;52(10):2224–34.
McKay BR, Paterson DH, Kowalchuk JM. Effect of short-term high-intensity interval training vs. continuous training on O2 uptake kinetics, muscle deoxygenation, and exercise performance. J Appl Physiol (1985). 2009;107(1):128–38.
Schaun GZ, Pinto SS, Silva MR, Dolinski DB, Alberton CL. Whole-Body High-Intensity Interval Training Induce Similar Cardiorespiratory Adaptations Compared With Traditional High-Intensity Interval Training and Moderate-Intensity Continuous Training in Healthy Men. J Strength Cond Res. 2018;32(10):2730–42.
McGill E, Marks D, Er V, Penney T, Petticrew M, Egan M. Qualitative process evaluation from a complex systems perspective: A systematic review and framework for public health evaluators. PLoS Med. 2020;17(11):e1003368.
Acknowledgements
The authors express their gratitude to Alison Bethel, an information specialist in University of Exeter, for her assistance in developing the search strategy. Special thanks are extended to Jiani Ma for her help in interpreting process evaluation measures. The authors would like to acknowledge the China Scholarship Council and the University of Exeter for providing funding for Yong Liu's PhD study. Additionally, Curtis A Wadey is funded by an industrial PhD scholarship by Canon Medical Systems UK Ltd. and the University of Exeter.
Funding
Not applicable.‘For the purpose of open access, the author has applied a Creative Commons Attribution (CC BY) licence to any Author Accepted Manuscript version arising from this submission’.
Author information
Authors and Affiliations
Contributions
Conceptualization: Yong Liu, Curtis Wadey, Alan R. Barker, Craig A. Williams. Data curation: Yong Liu, Curtis Wadey. Formal analysis: Yong Liu, Curtis Wadey. Methodology: Yong Liu, Curtis A. Wadey, Alan R. Barker, Craig A. Williams. Supervision: Alan R. Barker, Craig A. Williams. Visualization: Yong Liu. Writing of original draft: Yong Liu. Writing, review and editing: Yong Liu, Curtis Wadey, Alan R. Barker, Craig A. Williams.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table S1.
PRISMA 2020 Checklist.
Additional file 3:
Table S2. Exclusion details for the initial search and updated search.
Additional file 4:
Table S3. Study characteristics.
Additional file 5:
Fig S1. Risk of bias assessment for cardiorespiratory fitness. Fig S2. Risk of bias assessment for body composition. Fig S3. Risk of bias assessment for muscular fitness.
Additional file 7: Fig S4.
Sensitive analysis by removing high risk of bias studies for CRF. N, participant number; SD, standard deviation; SMD, standard mean difference; CI, confidence interval; AEP, aerobic exercise programme; RAP, resistance and aerobic programme. Fig S5. Sensitive analysis by removing studies with computed outcome scores for cardiorespiratory fitness. N, participant number; SD, standard deviation; SMD, standard mean difference; CI, confidence interval. Fig S6. Funnel plot for studies reported cardiorespiratory fitness. Fig S7. Sensitive analysis by removing high risk of bias studies for body composition. N, participant number; SD, standard deviation; SMD, standard mean difference; CI, confidence interval; AEP, aerobic exercise programme; RAP, resistance and aerobic programme. Fig S8. Sensitive analysis by removing studies with computed outcome scores for body composition. N, participant number; SD, standard deviation; SMD, standard mean difference; CI, confidence interval. Fig S9. Funnel plot for studies reported body composition. Fig S10. Sensitive analysis by removing high risk of bias studies for muscular strength. N, participant number; SD, standard deviation; SMD, standard mean difference; CI, confidence interval; AEP, aerobic exercise programme; RAP, resistance and aerobic programme. Fig S11. Sensitive analysis by removing studies with computed outcome scores for muscular strength. N, participant number; SD, standard deviation; SMD, standard mean difference; CI, confidence interval. Fig S12. Funnel plot for studies reported muscular strength.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Liu, Y., Wadey, C.A., Barker, A.R. et al. Process evaluation of school-based high-intensity interval training interventions for children and adolescents: a systematic review and meta-analysis of randomized controlled trials. BMC Public Health 24, 348 (2024). https://doi.org/10.1186/s12889-024-17786-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-024-17786-6