
Abstract
A substantial body of empirical evidence reveals that physical activity is associated with a wide range of positive physical and mental health outcomes. However, an absence of comprehensive syntheses is observed concerning the varying effects of different exercise intensities on the improvement of physical health among children and adolescents. The aim of this review is to systematically investigate the effects of different exercise intensities on the physical fitness of children and adolescents, to analyses the optimal exercise intensities for improving physical fitness, and to provide a relevant theoretical basis for optimizing school physical education curricula. A systematic search strategy was used in this study in four online databases (PubMed, Scopus, EBSCO and Web of Science). Intervention studies that met the inclusion criteria underwent a thorough screening process, and their methodological quality was assessed utilizing the PEDro scale. The selected literature was systematically analyzed and evaluated through induction, summary, analysis, and evaluation. These findings indicate that high-intensity exercise training exerts significant positive effects on body composition, cardiopulmonary function and muscle fitness in children and adolescents. Therefore, we suggest that schools should focus on high-intensity sports in their physical education curriculum, which can further improve the student's PHYSICAL FITNESS.
Similar content being viewed by others


Introduction
Overweight and obesity in children and adolescents have become a global public health problem1. The prevalence of obesity in children and adolescents has been reported to have increased from 0.7% to 5.6%2. The persistence of overweight and obesity into adulthood has the potential to lead to chronic diseases, including type 2 diabetes, cardiometabolic disorders, and a range of psychosocial problems3,4,5,6, Numerous studies have shown that physical activity is one of the most important interventions to reduce physical health and psychological problems in adolescents7,8,9. WHO recommends that children and adolescents should engage in an average of 60 min of moderate to high-intensity physical activity (MVPA) per day to obtain health benefits10, however, more than 80%of adolescents fail to reach the minimum recommended amount of physical activity11. Given that adolescents have difficulty starting and following recommended guidelines for 30–60 min of moderate-intensity training per day12,13, there is a need to explore and develop engaging alternatives for youth to achieve the many health benefits of regular physical activity. Traditionally, moderate-intensity continuous training (MICT) has been the most common type of exercise recommended to improve body composition and cardiorespiratory fitness (CRF)14,15. However, in recent years, a growing body of laboratory evidence has shown that high-intensity exercise training is less time-consuming than MICT in improving body composition and other health indicators in obese children and adolescents16,17,18. Whether high-intensity or low-intensity exercise training is more beneficial to the PHYSICAL FITNESS of children and adolescents is still highly debated. Therefore, there is a need to further explore differences in the effectiveness of different exercise intensity interventions in improving PHYSICAL FITNESS in children and adolescents.
PHYSICAL FITNESS is a multidimensional state of being. PHYSICAL FITNESS is the body’s ability to function efficiently and effectively. It is a state of being that consists of at least FIVE HEALTH-RELATED and SIX SKILL-RELATED PHYSICAL FITNESS COMPONENTS, each of which contributes to total quality of life. The five components of health-related PHYSICAL FITNESS are BODY COMPOSITION, CARDIOVASCULAR FITNESS, FLEXIBILITY, MUSCULAR ENDURANCE, AND STRENGTH19. A recent narrative and meta-analysis of 20 studies evaluated the efficacy of HIIT for improving HEALTH-RELATED FITNESS (ie, cardiorespiratory fitness, muscular fitness, body composition and flexibility). The results indicated significant improvements in cardiorespiratory fitness and body composition through HIIT, with notable effects observed in these areas13. Previous meta-analyses have weakened the interpretation of findings due to small sample sizes. Furthermore, there is less research on exercise interventions to treat PHYSICAL FITNESS in children and adolescents than in adults, particularly in terms of exploring exercise-related variables (intensity and duration).
Therefore, this systematic review aims to systematically summarized the effects of different exercise intensities on health-related fitness in children and adolescents and to analyze which exercise intensity is more conducive to improving health-related fitness in children and adolescents.
Methods
Protocol
This review was performed according to Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines20, and the Cochrane Handbook for systematic review21. The PRISMA checklist is presented in Additional File 1.
Search strategy
A comprehensive search was done systematically through PubMed, Scopus, EBSCO, and Web of Science up to the 5 of June 2024. Searching terms were based on adapted PICO questions to search through the aforementioned databases to access all the important articles. Free text words and medical subject heading (MeSH) terms were used. (1) children OR childhood OR pre*schooler OR schoolchildren OR preadolescent OR adolescent OR adolescence OR youth;(2) physical*activity OR physical*education OR exercise OR fitness OR sport;(3) strength OR flexibility OR motor OR endurance OR agility OR body composition OR anthropometry OR body mass index OR waist circumference OR overall adiposity OR central adiposity OR overweight OR obesity OR risk factors OR risk score cardiovascular disease OR metabolic syndrome OR blood glucose OR glucose tolerance OR insulin resistance OR insulin sensitivity OR blood lipids OR dyslipidemia OR diabetes OR blood pressure OR hypertension OR inflammatory markers OR bone mineral OR bone mineral content;(4) random OR random*controlled trial OR controlled trial OR trial. (The search strategy used for each database is provided in the supplementary material (table S2). At the same time, the reference lists of included articles and relevant reviews were retrospectively included to supplement the missing literature in the computer search. The systematic search process was conducted by XXZ and JYL. Any disagreement of an included/excluded study was resolved by the author PXJ.
Eligibility criteria of the selected studies
The inclusion criteria for articles were determined using the PICOS (Participants/Interventions/Comparisons/Outcomes/Study Design) principles, as follows. Participants (P): Children and adolescents (individuals in the 10–19 year age group22, including samples of overweight/obese children, but excluding samples of children with medical conditions); Interventions (I):interventions in the form of exercise, High-intensity aerobic exercise, Low-intensity aerobic training (LIT), Endurance training (ET), High-intensity interval exercise (HIIE), Moderate-intensity exercise (MIE),HIIT, moderate-intensity continuous (MICT); Comparisons (C): control group performed low to moderate intensity physical activity or no artificially designed physical exercise; Outcomes (O): assessment of at least one of the following indicators (i.e., body composition, cardiorespiratory fitness, muscular fitness, strength, flexibility, motor, endurance, agility, body composition, anthropometry, body mass index, waist circumference, overall adiposity , central adiposity , overweight , obesity ,risk factors , risk score cardiovascular disease, metabolic syndrome, blood glucose, glucose tolerance, insulin resistance, insulin sensitivity, blood lipids, dyslipidemia, diabetes, blood pressure, hypertension, inflammatory markers, bone mineral, bone mineral content); Study Design (S): controlled trial.
Exclusion criteria: (1) studies not related to the topic (non-physical activity, physical activity); (2) non-intervention studies (observational studies, systematic reviews) and studies that did not provide sufficient comparisons to compare; (3) Exclude other age groups other than 3–19 years old. The title, abstract and full text were independently assessed by two authors for eligibility. Finally, randomized controlled trials were limited to articles published in English.
Data extraction
Data extraction from the included studies was independently performed by two authors (XXZ and JYL). For each study, data were extracted for the characteristics of the study population. These include (1) first author’s surname; (2) year of publication; (3) purpose; (4) results; (5) the characteristics, sample size and age of the participants; (6) sampling type; (7) type of research; (8) Characteristics of physical exercise (type, frequency and duration). Any disagreement in data extraction was resolved by the third author PXJ (Table 1).
Quality assessment
Papers that met the inclusion criteria were independently assessed by two authors (XXZ and JYL). This review assessed the included literature using the Physiotherapy Evidence Database (PEDro) scale, a credit rating scale developed by the Australian Centre for Evidence-Based Practice. The PEDro scale is a valid measure of the methodological quality of clinical trial23. The scale consisted of randomized grouping (2 items), blinding (3 item), data reporting (3 item), data analysis (1 item), and follow-up (1 item), with a total of 10 criteria. Each item was recorded as 1 point when it appeared in the article and 0 points when it was not reflected, for a total score of 0 to 10 points. To avoid subjective opinions, two reviewers assessed the opinions, and the third judged the differences. It classifies papers into three levels: high quality above 8, medium quality 4–7, and low quality below 4 points. Disagreements were solved by a third party (PXJ) (Table 2).
Data synthesis and analysis
Due to the heterogeneity of the studies, no meta-analysis was performed. Instead, intervention characteristics for each study were summarized and analyzed and then recorded in a standardized form created by the authors. The effectiveness of the intervention was calculated using the formula: number of effective trials (post-intervention scores significantly higher than pre-intervention or control scores)/total number of trials. Data analysis was performed by the first author XXZ and then validated by the second author JYL.
Results
Literature screening process and results
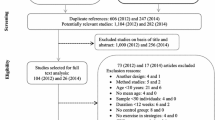
A preliminary search of the database yielded 10,030 relevant studies. We first imported the documents into the document management software Endnote, and after removing duplicate documents and screening titles and abstracts, we excluded 9990 articles. Of the remaining 40 articles, 30 articles were obtained after screening and checking the full text, and the irrelevant articles were eliminated. The reasons for the exclusion based on the full text were: (1) no intervention studies (3 articles); (2) The age does not meet (3 articles); (3) non-full text (2 articles); (4) non-English articles (2 articles). The PRISMA flowchart is shown in Fig. 1.

Flow chart of literature retrieval.
The systematic search of relevant literature published as of 5 June 2024 found 30 relevant articles, the earliest of which was published in 1999. The study included 30 related papers from the United States, Canada, Brazil, Denmark, Spain, China, Australia, the United Kingdom, Singapore, France, Portugal, Colombia, and Switzerland.
Study characteristics were summarized in Table 1, and the final analysis included 6494 children and adolescents with participants ranging in age from 5 to 18 years, with most studies including healthy children and adolescents, but nine studies including overweight or obese children. Study sizes ranged from 10 to 2166. Physical activity interventions mainly included HIIT (8/30; 27%), aerobic training (5/30; 17%), resistance training (2/30; 7%), physical education (1/30; 3%), endurance training (1/30; 3%), acute exercise (1/30; 3%) and other interventions. Outcome measures: body mass index, waist circumference, body fat, cardiorespiratory fitness, and muscle fitness (muscular endurance, muscle strength and muscular flexibility). Quality scores for 30 studies are shown in Table 2. The studies ranged in their scores from 3 to 10. Only two studies achieved high-quality scores (≥ 8) (Table 2). One study scored below 4. Blinding techniques ranged from 0 to 3 in this study, with only one study scoring 3 and four scoring 1; Fifteen studies scored 0.
Effects of different exercise intensity on BODY COMPOSITION in children and adolescents
A total of 11 studies in this study assessed the effects of different exercise intensities on body composition (weight, BMI, body fat, waist circumference, fat-free mass, and other relevant indicators), of which 9 showed that high-intensity exercise interventions had a positive effect on overweight or obese children and adolescents, but 2 had no positive effect.
Weight, BMI and body fat
A total of 8 of the 11 studies assessed changes in body weight, BMI, adiposity, or percentage of body fat measured. Six of the eight studies, reported positive effects of high-intensity exercise interventions on body weight, BMI, or body fat in overweight and obese child adolescents. However, 2 studies showed moderate or no positive effects of high-intensity exercise interventions on BMI, and body fat in overweight or obese children and adolescents.
Tadiotto et al. conducted a 12-week HIIT and MIIT intervention study and found significant reductions in (body mass index) BMI-z, (waist-to-height ratio) WHtR, and LDL-c in HIIT28. Benson et al. compared the effects of high-intensity progressive resistance training (PRT) on body composition in obese children and showed that an 8-week PRT intervention resulted in significant improvements in adiposity, percentage body fat, and body mass index34. Recent findings have shown that after 12 weeks of HIIT and MICT interventions, there was a significant reduction in BMI and body fat mass in the HIIT group compared to the control group, as well as a significant reduction in visceral adipose tissue (− 53 g vs. − 17 g, p < 0.01), LDL cholesterol was reduced only in the HIIT group, whereas in MICT only the body fat percentage was significantly reduced (− 17.2%, p < 0.05)31. In addition, Winn et al. compared the effects of HIIT on adolescents over a 6-month period and showed that after a 6-month school HIIT intervention, BMI was maintained in the HIIT group and significantly increased in the control group, and that HIIT was an effective tool for maintaining BMI47.
In a study assessing the effect of different exercise intensities on energy expenditure for spontaneous physical activity in adolescents, Paravidino et al. found that the mean energy expenditure was 82, 286 and 343 kcal in the control, moderate and vigorous exercise groups, respectively (p < 0.001), and the results suggest that high intensities are more conducive to an increase in energy expenditure, and thus to weight loss27. Saidi et al. studied the effect of vigorous exercise on subsequent dietary intake in obese adolescent girls and showed a significant reduction in adiposity in the exercise group compared to the control group (p < 0.02)45.
In the present study, 2 studies reported no significant effects of different intensities of exercise on body composition in overweight or obese children and adolescents. Gomes et al. compared the effects of different aerobic training intensities over a period of 12 on the body composition of obese adolescents, and showed a decrease in body weight, BMI, and body fat in both the intervention and control groups after a 12-week intervention (p < 0.001), but these results could not be attributed solely to aerobic training intensity due to the multidisciplinary intervention40. In another study, Costigan et al. conducted an 8-week study of aerobic training (AEP) and resistance and aerobic programming (RAP) with 68 secondary school students, and the results showed a moderate effect of the BMI intervention for participants in the AEP and RAP groups. It may be related to the small sample size43.
Waist circumference
Three randomized controlled trials assessed changes in waist circumference and all found beneficial effects. (Insert literature), a study conducted by Farah et al., showed that after 6 months of high-intensity aerobic training (HIT) and low-intensity aerobic training (LIT), significant beneficial changes in waist circumference were found only in the HIT group24. Benson et al. investigated the effects of 8 weeks of high-intensity progressive resistance training (PRT) on body composition in obese children and compared the effects between the experimental and control groups, showing that significant changes in waist circumference were obtained in the intervention group after 8 weeks of PRT training34. Costigan et al. conducted an 8-week study of aerobic training (AEP), resistance and aerobic programming (RAP) with 68 secondary school students and showed that participants in the AEP and RAP groups had significant changes in waist circumference (p = 0.024)43.
Fat-free mass
Only 1 study evaluated the effect of different exercise intensities on fat-free mass. Leppanen et al. investigated the effect of physical activity intensity and sedentary behaviours (ST) on body composition in 4 years old children. The results showed that the higher the intensity of moderate-to-vigorous exercise, the lower the percentage of fat (%FM, p = 0.015), the VPA (high intensity) and MVPA (moderate-to-vigorous exercise intensity) the higher the fat-free mass index (FFMI, p = 0.002 and p = 0.011) Time spent on VPA was associated with higher FFMI38.
Effects of different exercise intensities on CARDIOPULMONARY FUNCTION (CRF) in children and adolescents
A total of 16 studies investigated the effects of different exercise intensity interventions on cardiorespiratory fitness, and positive effects were found in all studies. In general, cardiorespiratory fitness improved with high-intensity exercise interventions. The included studies assessed vascularity, heart rate, lipids, insulin sensitivity, inflammatory markers, diabetes, and other relevant indicators.
Blood vessels
A total of 4 out of 16 studies investigated the effects of exercise intensity interventions on blood vessels in children and adolescents. Four studies demonstrated that high-intensity training interventions had a positive effect on blood vessels.
Bond et al. investigated the effect of exercise intensity on protecting the vascular system from high-fat diets in adolescents study by intervening with high-intensity interval exercise (HIIE) and moderate-intensity exercise (MIE) in 20 adolescents, and showed that exercise intensity plays an important role in protecting the vascular system from the deleterious effects of HFM, and that in the adolescent population, performing HIIE may be more effective than MIE in Provides better vascular benefits26. In a study examining the effects of sprint interval exercise on post-exercise metabolism and blood pressure in adolescents, it was shown that acute sprint interval exercise leads to an increase in short-term oxygen uptake and a decrease in blood pressure in adolescents37. Farpour-Lambert et al. investigated the effect of physical activity on systemic blood pressure in adolescent obese children, and after a 3-month intervention, significant changes in systolic and diastolic blood pressure were obtained in the intervention group compared to the control group51. Buchan et al. investigated whether a high-intensity training (HIT) intervention could improve the CVD risk profile of adolescents in a time-effective manner, and after a 7-week HIT intervention, a significant reduction in systolic blood pressure was obtained in the intervention group compared to the control group41.
Insulin sensitivity
Of the 16 studies, only 2 randomized controlled trials assessed the effect of exercise intensity on insulin sensitivity. Only one study showed that a high-intensity exercise intervention could have a positive effect on insulin sensitivity. In the first randomized controlled trial, the Davis study found that after the intervention, the high-dose aerobic training group had a greater reduction in insulin (AUC), which could be effective in reducing metabolic risk36. However, in another randomized trial of 106 overweight and obese adolescents who underwent high-intensity endurance training (ET) and moderate-intensity (ET) for 6 months, the results showed that ET significantly improved cardiorespiratory fitness in obese adolescents, but the effect of exercise intensity on insulin sensitivity and triglycerides remained unclear due to lack of compliance25.
Inflammation
A total of 3 out of 16 studies assessed the effect of exercise intensity interventions on inflammation, with only 2 showing a positive effect of high-intensity exercise interventions on the prevention of inflammation. The results of the study by Ramirez-Velez et al. suggest the utility of high-intensity aerobic and resistance training as a means of modulating the levels of certain pro-inflammatory interleukins in adolescent subjects, thereby playing an important role in the prevention of diseases associated with low-grade inflammation, such as cardiovascular disease and type 2 diabetes30. A study by Tadiotto et al. found that C-reactive protein (CRP) was significantly reduced in the HIIT group, promoting beneficial changes in obesity and inflammatory processes28. However, in a study conducted by Buchan et al. with 89 adolescent students to assess whether the HIIT intervention could improve the cardiovascular disease risk profile of secondary school students in a time-effective manner, after a 7-week intervention, the results showed no significant differences between groups for any of the nine biochemical risk markers for cardiovascular disease, but significantly improved cardiorespiratory fitness41.
Heart Rate
Two of the 16 studies showed that high-intensity exercise interventions had a positive effect on heart rate. In one study examining the effect of exercise intensity on blood pressure and heart rate in obese adolescents, after a 6-month period of HIT and LIT, beneficial changes in HR and HRV occurred only in the HIT group24. In a randomized controlled trial, Ketelhut et al. assessed the effect of implementing school-specific HIIT in a physical education curriculum on various hemodynamics parameters and heart rate variability, and after a 12-week intervention, the results showed that significant changes in heart rate were obtained in the intervention group (p = 0.010)52.
In addition, five other studies have all demonstrated the beneficial effects of high-intensity exercise interventions on cardiorespiratory fitness. Grasten et al. examined the effects of moderate-to-vigorous physical activity and ST with cardiorespiratory fitness in schoolchildren from 2017 to 2020, assessing accelerometer based MVPA by using waist-worn activity monitors and CRFs at four measurement points using the 20-m shuttle run test and ST, which showed a positive correlation between MVPA and CRF, and a negative correlation between ST and CRF42. Taber et al. conducted a moderate and vigorous exercise intervention with 1,029 eighth-grade girls and measured cardiorespiratory fitness using the Modified Physical Exercise Capacity Test (MPCT), which showed that vigorous exercise was positively associated with cardiorespiratory fitness35. Dias et al. showed that after 12 weeks of HIIT and MICT interventions, the HIIT group had a significant increase in relative peak VO2 compared to MICT, which was very effective in improving cardiorespiratory fitness32. Both studies by Gerber et al. and Leppanen et al. showed that higher levels of MVPA were associated with higher CRF scores39.
Effects of different exercise intensities on FLEXIBILITY in children and adolescents
Only two studies assessed changes in flexibility and no effects were found. The first study, conducted by Buchan et al., showed that after a 7-week period of high-intensity interval exercise, the intervention group showed an increase in vertical performance, and 10-m sprint speed (p < = 0.05), while the control group showed a significant decrease in both flexibility and vertical performance41. The most recent study, conducted by Juric et al. investigated the effects of a HIIT intervention lasting 12 weeks on balance, coordination, speed, flexibility, strength, and agility in 10- to 15-year-old students, and showed no significant effects. This may be because short-term HIIT interventions of only two 10-min sessions per week do not provide sufficient stimulation for fitness (muscular strength, muscular endurance, power, speed, flexibility, and balance) enhancement50.
Effects of different exercise intensities on MUSCLE FITNESS in children and adolescents
Five studies assessed changes in muscle fitness, and four showed that high-intensity exercise interventions had a positive impact on muscle fitness in children and adolescents. Larsen et al. explored whether the musculoskeletal fitness of 8–10 year old schoolchildren is affected by frequent high-intensity physical education classes, and showed that after a 10-month intervention of varying intensities, the intervention group had higher scores for changes in bone mineral content (BMC) and bone mineral density (aBMD) change scores were higher, suggesting that well organized high-intensity physical education sessions can promote the development of musculoskeletal fitness in young children29. A study of the effects of different resistance training programs on the development of muscular strength and endurance in children found a significant increase in leg extension muscular endurance with low repetition-heavy loads and high repetition-heavy loads, with high repetition-medium loads being significantly greater than low repetition-heavy loads training, and in the chest press exercise only the high repetition-medium loads exercise group had significantly greater muscular strength and muscular endurance than the control group33. Benson et al. found that an 8-week PRT (two sets of high-intensity exercises targeting major muscle groups) intervention resulted in significant increases in upper body strength and lower body strength compared to a control group34. Leppanen et al. investigated the effect of physical activity intensity on PHYSICAL FITNESS in children by using the PREFIT PHYSICAL FITNESS test to measure PHYSICAL FITNESS (that is, cardiorespiratory fitness, lower and upper body muscular strength and motor fitness), and the results showed that replacing sedentary, low- or moderate-intensity exercise with 5 min of high-intensity exercise per day promoted an increase in muscle strength38.
However, Videira-Silva et al. showed no significant improvement in muscular endurance in participants in the 12-week HIIT group49. That's because the study, which only had two 10-min short-term high-intensity interval exercise sessions per week, failed to provide enough stimulation for fitness enhancement. Therefore, long-term, high-intensity training may be necessary to effectively improve muscle fitness in children and adolescents.
Discussion
This review aimed to summarize the effects of physical activity of different exercise intensities on the PHYSICAL FITNESS of children and adolescents. The analysis included 30 interventional studies from 15 countries. 30 studies were assessed as above average, with good reason to believe that different exercise intensities had different effects on PHYSICAL FITNESS in children and adolescents. Based on strict restrictions on the nature of the intervention included in the studies, the studies included in the study span the years 1999 to 2024 (Table 1). It can be guessed that since 1999, researchers have gradually found differences in improving the PHYSICAL FITNESS of adolescents with different exercise intensities. In addition, from the perspective of regions and countries where the literature is published, relevant research is mainly concentrated in developed countries and some developing countries. This may be because, with the increase in material wealth, the PHYSICAL FITNESS of children and adolescents has received a high level of attention. Judging from the number of relevant published literature, there is still a lack of research on the effects of different exercise intensities on the PHYSICAL FITNESS of children and adolescents internationally. Therefore, this study aims to draw the attention of more draw the attention of more researchers from different regions and countries to this topic and encourage the conduction of controlled trials with high-quality evidence to further demonstrate the positive effects of different exercise intensities.
This study shows that high intensity exercise training has significant effects in improving body composition. It was mainly more effective in reducing visceral fat. These results align with a previous review by Batacan et al., which synthesized 65 studies and showed that HIIT can significantly improve waist circumference and body fat percentage in people who are overweight or obese54. A meta-analysis of adolescents found that exercise interventions of different intensities were differentially effective in reducing body weight and body mass index, and that high-intensity aerobic exercise and high-intensity aerobic exercise combined with high-intensity resistance training were more effective than low- and moderate-intensity exercise interventions55. We suspect that this may be due to the fact that high-intensity exercise leads to excessive post-exercise oxygen consumption and the substrate for this energy oxidation is fat, during high-intensity exercise the body needs to secrete more adrenaline and noradrenaline to control the muscles, and in addition the body has to maintain high metabolic levels for a longer period of time even after exercise. All of these effects lead to an increase in the body's resting metabolic levels, which further stimulates fat burning and leads to weight loss56,57. It is also interesting to note that Buchan and Kargarfard, when exploring the effects of HIIT on body composition in normal and obese adolescents, did not find any good changes in body composition or waist circumference in the intervention group. Both studies claimed that the lack of effect on body composition was due to the short duration of the training (duration of 7 and 8 weeks)58,59. Therefore, we suggest that relevant scholars pay more attention to the optimal training time when high-intensity exercise training can effectively improve the body composition of children and adolescents, and provide more effective training programs to reduce the obesity rate of children and adolescents at home and abroad.
This study showed that both high-intensity exercise training and moderate to low-level exercise training can improve cardiorespiratory fitness in children and adolescents, but high-intensity exercise training has a more significant effect on cardiorespiratory function. This finding coincides with previous conclusions60,61,62. A meta-analysis of adolescents aged 11–17 years found that high-intensity exercise training has a significant effect on improving cardiorespiratory fitness in adolescents compared to moderate-intensity exercise60, which is consistent with our findings. The mechanism by which this occurs may be due to the fact that high-intensity training increases the oxidative capacity of skeletal muscle more efficiently than conventional training methods. For example, in terms of the molecular adaptive mechanisms of skeletal muscle oxidative capacity, high-intensity exercise activates the activity of AMPK and MAPK exercise-responsive kinases63,64, while increasing the amount of mRNA for PGC-qα, a transcription factor that regulates the oxidative function of mitochondria. With the activation of the joints leading to increased transcription of mitochondrial substances, this allows the body's aerobic and anaerobic capacity to be enhanced, leading to improved cardiorespiratory fitness65. We therefore recommend that schools should incorporate high-intensity program in their physical education curricula so as to improve the cardiorespiratory fitness of children and adolescents and to reduce the probability of children and adolescents suffering from cardiovascular diseases in adulthood.
Muscle fitness is widely recognized as a key fitness component for maintaining overall health and is negatively correlated with obesity66.In this review, five studies confirmed the effects of different exercise intensities on muscle fitness function in children and adolescents. A systematic study of school-age children and adolescents suggests that high-intensity physical activity is more beneficial in building muscle67. Our findings are supported by Smith et al.'s study, where strenuous physical activity was positively associated with muscle fitness in children and adolescents68. In addition, only 1 study in this study showed that high-intensity training was effective in improving muscle flexibility. Muscle flexibility can be expressed as the normal physiological range of joint motion69. If adequate flexibility is lacking, daily activities will become difficult. In addition, reduced flexibility can also lead to musculoskeletal injuries70. Therefore, maintaining (or increasing) flexibility is essential as it maintains normal joint motion, thereby reducing the risk of injury71. A study of adolescents aged 14–17 years found that a 12-week, high-intensity training intervention resulted in adolescents displaying greater flexibility72, which is consistent with our findings. Furthermore, in the literature included in this review, only 1 study showed that high-intensity training improves muscle flexibility, but there was insufficient evidence that muscle flexibility is associated with high-intensity training. We speculate that on the one hand, this may be related to limitations in the assessment of muscle flexibility. The currently commonly used methods of assessing muscle flexibility (sitting and stretching) are unable to detect a lack of function due to muscle laxity73; the other side of the coin is that most of the current research on muscle flexibility has focused on the elderly population, with less attention paid to children and adolescents. This is due to the fact that muscle flexibility decreases with age, leading to increased joint stiffness and progressive loss of balance, which increases the risk of falls in older adults73. Overall, appropriate levels of flexibility have positive implications for the PHYSICAL FITNESS of children and adolescents, and exploring scientifically sound methods of assessing flexibility and research on flexibility in children and adolescents should receive more attention.
Research limitations and prospects
Although this review discusses the effects of different exercise intensities on the PHYSICAL FITNESS of children and adolescents from four aspects, its limitations should be properly examined. This review provides direction for further research on the effects of different exercise intensities on the PHYSICAL FITNESS of children and adolescents. Although an extensive literature search was conducted, including articles published before 2024, it is possible that some relevant literature may have been overlooked due to variations in keywords used in this study. Additionally, we conducted an extensive literature search in four major databases, but some published non-English foreign studies may have been missed in this review as our search was limited to English-language journal articles.
Despite these limitations, this review systematically collated the literature reports on the different effects of different exercise intensities on the PHYSICAL FITNESS of children and adolescents. Future research could explore higher-quality randomize controlled trials to provide more convincing evidence for optimal exercise intensity to improve the health of children and adolescents. Future research should also focus on the effect of different exercise intensities on muscle flexibility. At the same time, more comprehensive exercise evaluation is needed to support high-intensity exercise training as an effective exercise program to improve the PHYSICAL FITNESS of children and adolescents.
Conclusions
This systematic review demonstrates a positive association between high-intensity exercise training and PHYSICAL FITNESS in children and adolescents. High-intensity exercise training yields notable improvement in body composition (reduced body mass index, waist circumference, and body fat), cardiopulmonary function, and muscle strength in children and adolescents. Furthermore, the high-intensity training group outperforms both the moderate-intensity group and the control group in terms of improving physical fitness. Specifically, participation in HIIT exhibits a more significant effect on improving PHYSICAL FITNESS in children and adolescents. Based on the findings, we recommend that schools optimize their physical education programs by incorporating more high-intensity physical activities, thereby promoting the healthy growth of children and adolescents through effective exercise.
Moreover, the study highlights that the effects of high-intensity physical activity on the PHYSICAL FITNESS of children and adolescents may be influenced by factors such as average age, overweight or obesity of participants. Therefore, further refinement of the study design is necessary, along with additional high-quality research, particularly randomized controlled trials, to ensure the long-term reliability of the results. Additionally, in terms of measurement of related indicators, this study primarily relies on manual measurement and automated equipment, which may introduce measurement errors. Subsequent studies could consider using more advanced instruments to assess relevant indicators of the PHYSICAL FITNESS of children and adolescents.
Data availability
Data is provided within the manuscript or supplementary information files.
References
Jebeile, H., Kelly, A. S., O’Malley, G. & Baur, L. A. Obesity in children and adolescents: epidemiology, causes, assessment, and management. Lancet Diabetes Endocrinol. 10, 351–365. https://doi.org/10.1016/s2213-8587(22)00047-x (2022).
Ezzati, M. et al. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128.9 million children, adolescents, and adults. Lancet 390, 2627–2642. https://doi.org/10.1016/s0140-6736(17)32129-3 (2017).
Simmonds, M., Llewellyn, A., Owen, C. G. & Woolacott, N. Predicting adult obesity from childhood obesity: A systematic review and meta-analysis. Obesity Rev. 17, 95–107. https://doi.org/10.1111/obr.12334 (2016).
The, N. S., Suchindran, C., North, K. E., Popkin, B. M. & Gordon-Larsen, P. Association of adolescent obesity with risk of severe obesity in adulthood. Jama-J. Am. Med. Associat. 304, 2042–2047. https://doi.org/10.1001/jama.2010.1635 (2010).
Horesh, A., Tsur, A. M., Bardugo, A. & Twig, G. Adolescent and childhood obesity and excess morbidity and mortality in young adulthood-a systematic review. Curr. Obesity Rep. 10, 301–310. https://doi.org/10.1007/s13679-021-00439-9 (2021).
Jebeile, H., Cardel, M. I., Kyle, T. K. & Jastreboff, A. M. Addressing psychosocial health in the treatment and care of adolescents with obesity. Obesity 29, 1413–1422. https://doi.org/10.1002/oby.23194 (2021).
Weihrauch-Blueher, S., Schwarz, P. & Klusmann, J.-H. Childhood obesity: Increased risk for cardiometabolic disease and cancer in adulthood. Metabolism-Clin. Exp. 92, 147–152. https://doi.org/10.1016/j.metabol.2018.12.001 (2019).
Li, J., Zhou, X., Huang, Z. & Shao, T. Effect of exercise intervention on depression in children and adolescents: a systematic review and network meta-analysis. Bmc Public Health https://doi.org/10.1186/s12889-023-16824-z (2023).
Romero-Perez, E. M. et al. Influence of a physical exercise program in the anxiety and depression in children with obesity. Int. J. Environ. Res. Public Health https://doi.org/10.3390/ijerph17134655 (2020).
Martin, A. et al. Physical activity, diet and other behavioural interventions for improving cognition and school achievement in children and adolescents with obesity or overweight. Cochrane Database Systematic Rev. https://doi.org/10.1002/14651858.CD009728.pub3 (2018).
Cai, Y., Zhu, X. & Wu, X. Overweight, obesity, and screen-time viewing among Chinese school-aged children: National prevalence estimates from the 2016 Physical Activity and Fitness in China-The Youth Study. J. Sport Health Sci. 6, 404–409. https://doi.org/10.1016/j.jshs.2017.09.002 (2017).
Sedgwick, M. J., Morris, J. G., Nevill, M. E. & Barrett, L. A. Effect of repeated sprints on postprandial endothelial function and triacylglycerol concentrations in adolescent boys. J. Sports Sci. 33, 806–816. https://doi.org/10.1080/02640414.2014.964749 (2015).
Costigan, S. A., Eather, N., Plotnikoff, R. C., Taaffe, D. R. & Lubans, D. R. High-intensity interval training for improving health-related fitness in adolescents: A systematic review and meta-analysis. Br. J. Sports Med. https://doi.org/10.1136/bjsports-2014-094490 (2015).
Donnelly, J. E. et al. Appropriate physical activity intervention strategies for weight loss and prevention of weight regain for adults. Med. Sci. Sports Exercise 41, 459–471. https://doi.org/10.1249/MSS.0b013e3181949333 (2009).
Reilly, J. J. & Kelly, J. Long-term impact of overweight and obesity in childhood and adolescence on morbidity and premature mortality in adulthood: Systematic review. Int. J. Obesity 35, 891–898. https://doi.org/10.1038/ijo.2010.222 (2011).
Hopkins, N. D. et al. Relationships between measures of fitness, physical activity, body composition and vascular function in children. Atherosclerosis 204, 244–249. https://doi.org/10.1016/j.atherosclerosis.2008.09.004 (2009).
Chuensiri, N., Suksom, D. & Tanaka, H. Effects of high-intensity intermittent training on vascular function in obese preadolescent boys. Childhood Obesity 14, 41–49. https://doi.org/10.1089/chi.2017.002 (2018).
Weston, K. S., Wisloff, U. & Coombes, J. S. High-intensity interval training in patients with lifestyle-induced cardiometabolic disease: A systematic review and meta-analysis. Br. J. Sports Med. 48, 1227-U1252. https://doi.org/10.1136/bjsports-2013-092576 (2014).
Corbin, C. B., Welk, G. J., Corbin, W. R. & Welk, K. A. Concepts of Physical Fitness: Active Lifestyles for Wellness 14th edn. (William Glass, 2008).
Hutton, B., Caldwell, D. M., Chaimani, A., Schmid, C. H. & Cameron, C. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann. Internal Med. 162(11), 777–784. https://doi.org/10.7326/M14-2385 (2015).
Vrabel, M. Preferred reporting items for systematic reviews and meta-analyses. Oncol. Nursing Forum 42, 552–554. https://doi.org/10.1188/15.Onf.552-554 (2015).
Adolescent health in the South-East Asia Region, <https://www.who.int/southeastasia/health-topics/adolescent-health> (2022).
de Morton, N. A. The PEDro scale is a valid measure of the methodological quality of clinical trials: A demographic study. Aust. J. Physiother. 55, 129–133. https://doi.org/10.1016/s0004-9514(09)70043-1 (2009).
Farah, B. Q., Ritti-Dias, R. M., Balagopal, P., Hill, J. O. & Prado, W. L. Does exercise intensity affect blood pressure and heart rate in obese adolescents? A 6-month multidisciplinary randomized intervention study. Pediatric Obesity 9, 111–120. https://doi.org/10.1111/j.2047-6310.2012.00145.x (2014).
Hay, J. et al. Physical activity intensity and type 2 diabetes risk in overweight youth: a randomized trial. Int. J. Obesity 40, 607–614. https://doi.org/10.1038/ijo.2015.241 (2016).
Bond, B. et al. Exercise intensity and the protection from postprandial vascular dysfunction in adolescents. Am. J. Physiol. -Heart Circulatory Physiol. 308, H1443–H1450. https://doi.org/10.1152/ajpheart.00074.2015 (2015).
Paravidino, V. B., Felix Mediano, M. F., Hoffman, D. J. & Sichieri, R. Effect of exercise intensity on spontaneous physical activity energy expenditure in overweight boys: A crossover study. Plos One https://doi.org/10.1371/journal.pone.0147141 (2016).
Tadiotto, M. C. et al. Effects and individual response of continuous and interval training on adiponectin concentration, cardiometabolic risk factors, and physical fitness in overweight adolescents. Eur. J. Pediatr. 182, 2881–2889. https://doi.org/10.1007/s00431-023-04974-6 (2023).
Larsen, M. N. et al. Positive effects on bone mineralisation and muscular fitness after 10 months of intense school-based physical training for children aged 8–10 years: The FIT FIRST randomised controlled trial. Br. J. Sports Med. 52, 254. https://doi.org/10.1136/bjsports-2016-096219 (2018).
Ramirez-Velez, R. et al. Effects of different doses of exercise on inflammation markers among adolescents with overweight/obesity: HEPAFIT study. J. Clin. Endocrinol. Metabolism 107, E2619–E2627. https://doi.org/10.1210/clinem/dgac021 (2022).
Cao, M., Tang, Y., Li, S. & Zou, Y. Effects of school-based high-intensity interval training on body composition, cardiorespiratory fitness and cardiometabolic markers in adolescent boys with obesity: A randomized controlled trial. Bmc Pediatr. https://doi.org/10.1186/s12887-021-03079-z (2022).
Dias, K. A. et al. Effect of high-intensity interval training on fitness, fat mass and cardiometabolic biomarkers in children with obesity: A randomised controlled trial. Sports Med. 48, 733–746. https://doi.org/10.1007/s40279-017-0777-0 (2018).
Faigenbaum, A. D., Westcott, W. L., Loud, R. L. & Long, C. The effects of different resistance training protocols on muscular strength and endurance development in children. Pediatrics 104, e5–e5. https://doi.org/10.1542/peds.104.1.e5 (1999).
Benson, A. C., Torode, M. E. & Singh, M. A. F. The effect of high-intensity progressive resistance training on adiposity in children: A randomized controlled trial. Int. J. Obesity 32, 1016–1027. https://doi.org/10.1038/ijo.2008.5 (2008).
Taber, D. R. et al. Participation in vigorous sports, not moderate sports, is positively associated with cardiorespiratory fitness among adolescent girls. J. Phys. Activity Health 11, 596–603. https://doi.org/10.1123/jpah.2011-0280 (2014).
Davis, C. L. et al. Exercise dose and diabetes risk in overweight and obese children a randomized controlled trial. Jama-J. Am. Med. Associat. 308, 1103–1112. https://doi.org/10.1001/2012.jama.10762 (2012).
Burns, S. F., Oo, H. H. & Anh Thanh Thuy, T. Effect of sprint interval exercise on postexercise metabolism and blood pressure in adolescents. Int. J. Sport Nutr. Exerc. Metabolism 22, 47–54. https://doi.org/10.1123/ijsnem.22.1.47 (2012).
Leppanen, M. H. et al. Physical activity intensity, sedentary behavior, body composition and physical fitness in 4-year-old children: Results from the ministop trial. Int. J. Obesity 40, 1126–1133. https://doi.org/10.1038/ijo.2016.54 (2016).
Leppanen, M. H. et al. Longitudinal physical activity, body composition, and physical fitness in preschoolers. Med. Sci. Sports Exerc. 49, 2078–2085. https://doi.org/10.1249/mss.0000000000001313 (2017).
Gomes, P. P., Silva, H. J. G. D., Lira, C. T. C. D., Lofrano-Prado, M. C. & Prado, W. L. D. Efeitos de diferentes intensidades de treinamento aeróbio sobre a composição corporal em adolescentes obesos. Revista Brasileira de Cineantropometria Desempenho Humano 15, 594–603. https://doi.org/10.5007/1980-0037.2013v15n5p594 (2013).
Buchan, D. S. et al. High intensity interval running enhances measures of physical fitness but not metabolic measures of cardiovascular disease risk in healthy adolescents. BMC Public Health 13, 498–498. https://doi.org/10.1186/1471-2458-13-498 (2013).
Grasten, A., Huhtiniemi, M., Kolunsarka, I. & Jaakkola, T. Developmental associations of accelerometer measured moderate-to-vigorous physical activity and sedentary time with cardiorespiratory fitness in schoolchildren. J. Sci. Med. Sport 25, 884–889. https://doi.org/10.1016/j.jsams.2022.08.015 (2022).
Costigan, S. A. et al. Preliminary efficacy and feasibility of embedding high intensity interval training into the school day: A pilot randomized controlled trial. Prevent. Med. Rep. 2, 973–979. https://doi.org/10.1016/j.pmedr.2015.11.001 (2015).
Saidi, O. et al. Acute effect of an intensified exercise program on subsequent sleep, dietary intake, and performance in junior rugby players. Eur. J. Appl. Physiol. 119, 2075–2082. https://doi.org/10.1007/s00421-019-04196-5 (2019).
Saidi, O., Rochette, E., Bovet, M., Merlin, E. & Duche, P. Acute intense exercise improves sleep and decreases next morning consumption of energy-dense food in adolescent girls with obesity and evening chronotype. Pediatric Obesity https://doi.org/10.1111/ijpo.12613 (2020).
Gerber, M. et al. Moderate-to-vigorous physical activity is associated with cardiorespiratory fitness among primary schoolchildren living in cote D’ivoire, South Africa, and Tanzania. Front. Public Health https://doi.org/10.3389/fpubh.2021.671782 (2021).
Winn, C. O. N. et al. Effect of high-intensity interval training in adolescents with asthma: The exercise for asthma with Commando Joe’s (R) (X4ACJ) trial. J. Sport Health Sci. 10, 488–498. https://doi.org/10.1016/j.jshs.2019.05.009 (2021).
da Silva, P., Bento, A. F., Paez, L. C., de Mendonca, M. & Raimundo, A. High-intensity interval training in high-school physical education classes: Study protocol for a randomized controlled trial. Contemporary Clin. Trials Commun. 24, 100867–100867. https://doi.org/10.1016/j.conctc.2021.100867 (2021).
Videira-Silva, A., Sardinha, L. B. B. & Fonseca, H. Atherosclerosis prevention in adolescents with obesity: The role of moderate-vigorous physical activity. Int. J. Environ. Res. Public Health https://doi.org/10.3390/ijerph192315537 (2022).
Juric, P., Dudley, D. A. & Petocz, P. Does incorporating high intensity interval training in physical education classes improve fitness outcomes of students? A cluster randomized controlled trial. Prevent. Med. Rep. 32, 102127–102127. https://doi.org/10.1016/j.pmedr.2023.102127 (2023).
Farpour-Lambert, N. J. et al. Physical activity reduces systemic blood pressure and improves early markers of atherosclerosis in pre-pubertal obese children. J. Am. College Cardiol. 54, 2396–2406. https://doi.org/10.1016/j.jacc.2009.08.030 (2009).
Ketelhut, S., Ketelhut, K., Ketelhut, S. R. & Ketelhut, R. G. Effects of school-based high-intensity interval training on hemodynamic parameters and heart rate variability: A randomized controlled trial. J. Strength Cond. Res. https://doi.org/10.1519/jsc.0000000000004744 (2024).
Migueles, J. H. et al. Effects of an exercise program on cardiometabolic and mental health in children with overweight or obesity a secondary analysis of a randomized clinical trial. Jama Netw. Open https://doi.org/10.1001/jamanetworkopen.2023.24839 (2023).
Batacan, R. B. Jr., Duncan, M. J., Dalbo, V. J., Tucker, P. S. & Fenning, A. S. Effects of high-intensity interval training on cardiometabolic health: A systematic review and meta-analysis of intervention studies. Br. J. Sports Med. https://doi.org/10.1136/bjsports-2015-095841 (2017).
Hao, Z. et al. Which exercise interventions are more helpful in treating primary obesity in young adults? A systematic review and Bayesian network meta-analysis. Archiv. Med. Sci. 19, 865–883. https://doi.org/10.5114/aoms/153479 (2023).
Borsheim, E. & Bahr, R. Effect of exercise intensity, duration and mode on post-exercise oxygen consumption. Sports medicine (Auckland, NZ) 33, 1037–1060 (2003).
Sindorf, M. A. G. et al. Excess post-exercise oxygen consumption and substrate oxidation following high-intensity interval training: Effects of recovery manipulation. Int. J. Exerc. Sci. 14, 1151–1165 (2021).
Kargarfard, M. et al. Effects of endurance and high intensity training on ICAM-1 and VCAM-1 levels and arterial pressure in obese and normal weight adolescents. Physician Sportsmedicine 44, 208–216. https://doi.org/10.1080/00913847.2016.1200442 (2016).
Buchan, D. S. et al. The effects of time and intensity of exercise on novel and established markers of CVD in adolescent youth. Am. J. Hum. Biol. 23, 517–526. https://doi.org/10.1002/ajhb.21166 (2011).
Martin-Smith, R. et al. High intensity interval training (HIIT) improves cardiorespiratory fitness (CRF) in healthy, overweight and obese adolescents: A systematic review and meta-analysis of controlled studies. Int. J. Environ. Res. Public Health 17(8), 2955. https://doi.org/10.3390/ijerph17082955 (2020).
Cao, M., Tang, Y., Li, S. & Zou, Y. Effects of high-intensity interval training and moderate-intensity continuous training on cardiometabolic risk factors in overweight and obesity children and adolescents: A meta-analysis of randomized controlled trials. Int. J. Environ. Res. Public Health https://doi.org/10.3390/ijerph182211905 (2021).
Bond, B., Weston, K. L., Williams, C. A. & Barker, A. R. Perspectives on high-intensity interval exercise for health promotion in children and adolescents. Open Access J. Sports Med. 8, 243–265. https://doi.org/10.2147/oajsm.S127395 (2017).
Little, J. P. et al. Low-volume high-intensity interval training reduces hyperglycemia and increases muscle mitochondrial capacity in patients with type 2 diabetes. J. Appl. Physiol. 111, 1554–1560. https://doi.org/10.1152/japplphysiol.00921.2011 (2011).
Gibala, M. J. et al. Brief intense interval exercise activates AMPK and p38 MAPK signaling and increases the expression of PGC-1α in human skeletal muscle. J. Appl. Physiol. 106, 929–934. https://doi.org/10.1152/japplphysiol.90880.2008 (2009).
Little, J. P., Safdar, A., Bishop, D., Tarnopolsky, M. A. & Gibala, M. J. An acute bout of high-intensity interval training increases the nuclear abundance of PGC-1α and activates mitochondrial biogenesis in human skeletal muscle. Am. J. Physiol. -Regulatory Integrative Comparative Physiol. 300, R1303–R1310. https://doi.org/10.1152/ajpregu.00538.2010 (2011).
Wearing, S. C., Hennig, E. M., Byrne, N. M., Steele, J. R. & Hills, A. P. The impact of childhood obesity on musculoskeletal form. Obesity Rev.: Off. J. Int. Associat. Study Obesity 7, 209–218. https://doi.org/10.1111/j.1467-789X.2006.00216.x (2006).
Janssen, I. & LeBlanc, A. G. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int. J. Behav. Nutr. Phys. Activity https://doi.org/10.1186/1479-5868-7-40 (2010).
Smith, J. J. et al. Behavioral correlates of muscular fitness in children and adolescents: A systematic review. Sports Med. 49, 887–904. https://doi.org/10.1007/s40279-019-01089-7 (2019).
Holland, G. J., Tanaka, K., Shigematsu, R. & Nakagaichi, M. Flexibility and physical functions of older adults: A review. Aging Phys. Activity https://doi.org/10.1123/japa.10.2.169 (2002).
Badley, E. M., Wagstaff, S. & Wood, P. H. Measures of functional ability (disability) in arthritis in relation to impairment of range of joint movement. Ann. Rheumatic Diseases 43, 563–569. https://doi.org/10.1136/ard.43.4.563 (1984).
D’Onofrio, G., Kirschner, J., Prather, H., Goldman, D. & Rozanski, A. Musculoskeletal exercise: Its role in promoting health and longevity. Progr. Cardiovasc. Diseases 77, 25–36. https://doi.org/10.1016/j.pcad.2023.02.006 (2023).
Cvetkovic, N. et al. Exercise training in overweight and obese children: Recreational football and high-intensity interval training provide similar benefits to physical fitness. Scandinavian J. Med. Sci. Sports 28, 18–32. https://doi.org/10.1111/sms.13241 (2018).
Liu, C., Cao, Y., Zhang, Z., Gao, R. & Qu, G. Correlation of fundamental movement skills with health-related fitness elements in children and adolescents: A systematic review. Front. Public Health https://doi.org/10.3389/fpubh.2023.1129258 (2023).
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
X.X.Z. performed the methodological search on the research topic and helped write the draft manuscript. J.Y.L. contributed to the conception and design of the manuscript. X.P.J. critically wrote and revised the manuscript. All authors have read and approved the final version of this paper and agree with the other of its presentation.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Zhou, X., Li, J. & Jiang, X. Effects of different types of exercise intensity on improving health-related physical fitness in children and adolescents: a systematic review. Sci Rep 14, 14301 (2024). https://doi.org/10.1038/s41598-024-64830-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-64830-x
- Springer Nature Limited