
Abstract
Background
Inflammation exerts a critical role in the pathogenesis of infertility. The relationship between inflammatory parameters from peripheral blood and infertility remains unclear. Aim of this study was to investigate the association between inflammatory markers and infertility among women of reproductive age in the United States.
Methods
Women aged 20–45 were included from the National Health and Nutrition Examination Survey (NHANES) 2013–2020 for the present cross-sectional study. Data of reproductive status was collected from the Reproductive Health Questionnaire. Six inflammatory markers, systemic immune inflammation index (SII), lymphocyte count (LC), product of platelet and neutrophil count (PPN), platelet-lymphocyte ratio (PLR), neutrophil–lymphocyte ratio (NLR) and lymphocyte-monocyte ratio (LMR) were calculated from complete blood counts in mobile examination center. Survey-weighted multivariable logistic regression was employed to assess the association between inflammatory markers and infertility in four different models, then restricted cubic spline (RCS) plot was used to explore non-linearity association between inflammatory markers and infertility. Subgroup analyses were performed to further clarify effects of other covariates on association between inflammatory markers and infertility.
Results
A total of 3,105 women aged 20–45 was included in the final analysis, with 431 (13.88%) self-reported infertility. A negative association was found between log2-SII, log2-PLR and infertility, with an OR of 0.95 (95% CI: 0.78,1.15; p = 0.60), 0.80 (95% CI:0.60,1.05; p = 0.10), respectively. The results were similar in model 1, model 2, and model 3. Compared with the lowest quartile (Q1), the third quartile (Q3) of log2-SII was negatively correlation with infertility, with an OR (95% CI) of 0.56 (95% CI: 0.37,0.85; p = 0.01) in model 3. Similarly, the third quartile (Q3) of log2-PLR was negatively correlation with infertility, with an OR (95% CI) of 0.61 (95% CI: 0.43,0.88; p = 0.01) in model 3. No significant association was observed between log2-LC, log2-PPN, log2-NLR, log2-LMR and infertility in model 3. A similar U-shaped relationship between log2-SII and infertility was found (p for non-linear < 0.05). The results of subgroup analyses revealed that associations between the third quartile (Q3) of log2-SII, log2-PLR and infertility were nearly consistent.
Conclusion
The findings showed that SII and PLR were negatively associated with infertility. Further studies are needed to explore their association better and the underlying mechanisms.
Similar content being viewed by others


Introduction
Global disease burden of infertility has been increasing, as rate of female infertility increased by 14.962% throughout the period from 1990 to 2017 [1]. Among women diagnosed with infertility, up to 30% are considered unexplained infertility following standard investigation, which then would be advised to undergo cost prohibitive assisted reproductive technology with risks of adverse pregnancy and childbirth outcomes or laparoscopy combined with hysteroscopy based on age, ovarian reserve, infertility duration and other factors of women [2, 3]. Infertility should be regarded as more than reproductive health problem considering its public health economic burden and harmful influences on women’s psychological distress, as well as marital discord. Significant evidence has suggested that systemic or local inflammation and immune response are considered one of the most critical factors contributing to unexplained infertility [4]. Immune cells (including macrophages, natural killer cells, dendritic cells, and T cells) and immune regulatory molecules (such as IL-6, IL-10, TNF-α, and TGF-β1) maintaining homeostasis of endocrine display abnormal activity in women with diseases related to infertility [5, 6].
Systemic immune inflammation index (SII), lymphocyte count (LC), product of platelet and neutrophil count (PPN), platelet-lymphocyte ratio (PLR), neutrophil–lymphocyte ratio (NLR), and lymphocyte-monocyte ratio (LMR) calculated from peripheral blood cell counts are emerging inflammatory markers for diseases status or prognosis prediction. There is growing interest in research aimed at identifying value of complete blood cell counts derived inflammatory indicators because of their low cost-effective, rapid, and convenient process of blood draw and test. SII has been developed as an integrated and novel inflammatory indicator, while recent study confirmed the close relationship between SII and gynecological and breast cancers [7]. Earlier study demonstrated that the number of lymphocytes, the portion of CD4 + T lymphocytes, and NK cells were significantly elevated in women diagnosed with Polycystic Ovary Syndrome (PCOS) and that CD4 + T cells and NK cells were independent risk factors for PCOS [8], indicating peripheral blood inflammatory-immune cells as promising predictor of infertility among these patients. Aberrant function and frequency of lymphocytes have been accepted as partial pathogenesis of infertility and disturbed pregnancy [9], thus lymphocyte immunotherapy could be utilized to enhance maternal immune system against the paternal antigens with its promising effects on dysfunction of aberrant change of peripheral lymphocyte subsets. PPN is calculated as peripheral platelet count × neutrophil count. It has been reported that PPN was associated with female estradiol and bone mineral density. Researchers also found that SII, NLR was positively associated with female estradiol [10, 11].
Previous study demonstrated that NLR level increased in patients with PCOS and was positively correlated with insulin resistance. Furthermore, researchers considered that NLR might be a more sensitive marker to present low grade inflammation in patients with PCOS [12]. LMR has been introduced as an effective indicator for prognosis of patients with various carcinoma, acute ischemic stroke, and hypertension by recent studies [13,14,15,16,17,18]. PLR is ratio index calculated by inflammatory activators platelets and inflammatory regulators lymphocytes, which was positively associated with asthma prevalence [19] and adverse outcomes in acute exacerbations of chronic obstructive pulmonary disease [20].
Dysfunction and changed frequency of immune cells are closely related to infertility. However, association between SII, LC, PPN, PLR, NLR, LMR and infertility have not been reported yet. Therefore, this study aims to investigate association between inflammatory parameters and female infertility based on the National Health and Nutrition Examination Survey (NHANES) 2013–2020 data, hoping to provide new insights in inflammatory markers for female infertility.
Methods
Data source and population selection
NHANES, a continuous health and nutritional status program of adults and children in the United States, has been conducted as surveys including demographic, socioeconomic, dietary and health questions. NHANES was approved by the National Center for Health Statistics Institutional Review Board (https://www.cdc.gov/nchs/nhanes/irba98.htm), and informed consent of all individuals were obtained before participation in this program.
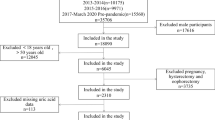
A total of 4,431 female participants aged 20–45 with finished Reproductive Health Questionnaire data was chosen from 35,706 individuals in the NHANES 2013–2020. Then, those with missing data to calculate inflammatory markers (n = 230), infertility information (n = 447), and other variables (n = 649) were excluded. Finally, 3,105 female participants were included in our analyses (Fig. 1).

Flowchart of participants selection. Legend: Abbreviations: NHANES, National Health and Nutrition Examination Survey
Definition of infertility and inflammatory markers
Self-reported infertility was determined according to answer to the specific two questions (question RHQ074 and question RHQ076) from the Reproductive Health Questionnaire. Question RHQ074: “Have you ever attempted to become pregnant over a period of at least a year without becoming pregnant?” Question RHQ076: “Have you ever been to a doctor or other medical provider because you have been unable to become pregnant?” Any woman who self-reported “Yes” to either of these questions was considered to have a history of infertility. Women who answered “Yes” were divided into the “infertility group”, while those who answered “No” were to the “non-infertility group”.
We collected lymphocyte count (LC), platelet count (PC), neutrophil count (NC) and monocyte count (MC) expressed in × 1000 cells/μ l from complete blood count to calculate the following inflammatory markers: SII was calculated as PC * NC/LC, PPN was the product of platelet and neutrophil, PLR was platelet to lymphocyte ratio, NLR was neutrophil to lymphocyte ratio, and LMR was lymphocyte to monocyte ratio.
Covariates
According to clinical practice, previous literature [21,22,23,24,25,26], and available in the NHANES database, we selected age, body mass index (BMI), race, marital status, education level, smoking status, alcohol user, income to poverty ratio (PIR), pelvic infection disease (PID), and age of menarche as covariates, aimed to control potential confounding bias in this study. Age was divided into two groups based on clinical significance (< 35, and ≥ 35 years). BMI was categorized into normal (< 25 kg/m2), overweight (25–30 kg/m2), and obesity (≥ 30 kg/m2) by clinical significance. Race was classified as “Mexican”, “Hispanic”, “White”, “Black”, and “Other race”. Marital status was classified as “Married/Living with partner”, and “Living alone”. Education level was divided into three groups as “Some college or AA degree above”, “High school/GED”, and “Less than 11th grade”. Smoking status was defined as “Yes” or “No” based on self-reported having smoked at least 100 cigarettes in their lifetime. The classification of alcohol user was determined through self-reporting as follows: heavy, self-reported ≥ 4 drinks every day; mild, self-reported ≤ 3 drinks every day; former, did not drink last year but drank ≥ 12 drinks in a lifetime or self-reported ≥ 12 drinks in 1 year and did not drink last year; never, self-reported < 12 drinks in a lifetime. The family PIR was categorized into three degrees (< 1.5, 1.5–3.5, and ≥ 3.5). PID was determined by the self-reported questions from Reproductive Health Questionnaire (RHQ078): Ever been treated for a pelvic infection/PID? The age of menarche was classified into two levels (< 15, and ≥ 15 years) by clinical practice.
Statistical analysis
Weight used for analysis was chosen based on instructions on the NHANES database. Weighting (2022), available at: https://wwwn.cdc.gov/nchs/nhanes/tutorials/Weighting.aspx, suggested that mobile examination center exam weight (WTMEC2YR) should be applied as complete blood count measured in the mobile examination center. Categorical variables were expressed as frequency (weighted proportion, %), and continuous variables were expressed as weighted mean (standard deviation, SD). Chi-square test (categorical variables) or Wilcoxon test (continuous variables) was used to compare significant differences between infertility and non-infertility groups.
As SII, LC, PPN, PLR, NLR and LMR from individuals included in the present study were right-skewed distribution (shown in Supplementary Fig. 1), SII, LC, PPN, PLR, NLR, and LMR were log2-transformed before data analysis (shown in Supplementary Fig. 2). Survey-weighted multivariable logistic regression was used to assess the association between inflammatory markers and infertility in four different models. No covariate was adjusted in crude model and age(continuous) was adjusted in model 1. Model 2 was adjusted for variables including age(continuous), BMI (continuous), race (Mexican, Hispanic, White, Black, and Other race), marital status (living alone, and married/living with partner), education (Some college or AA degree above, High school/GED, and Less than 11th grade), smoking status (No, Yes), alcohol user (never, former, mild, and heavy) and PIR (< 1.5, 1.5–3.5, and ≥ 3.5). Then based on model 2, we adjusted PID (No,Yes) and age of menarche (< 15 years or ≥ 15 years) in model 3. We then performed restricted cubic spline (RCS) plot to assess the potential non-linearity association between infertility and inflammatory markers. Furthermore, we performed subgroup and interaction analyses by all covariates to ensure the robustness of the result. R (version 4.3.1, http://www.R-project.org) was utilized to analyze data obtained from NHANES datasets, two-tailed P < 0.05 was of statistical significance.
Results
Baseline characteristics
A total sample of 3105 women represented a population of 40,670,393 women in the United States, with 431 (13.88%) self-reported infertility. Baseline characteristics of included women from NHANES 2013 to 2020 were shown in Table 1. The mean age of non-infertility and infertility women was 32.08 ± 0.22 and 35.18 ± 0.47 years, and the mean BMI was 29.19 ± 0.24 and 31.89 ± 0.63 kg/m2, respectively. Compared with non-infertility women, infertility women were more likely to be older, overweight, married or living with a partner, smoking, and history of pelvic infection disease (p < 0.05). No significant differences were found between the two groups in terms of race, education, alcohol user, PIR, and age of menarche. The mean log2-LC of infertility women was 1.22 (0.03) × 1000 cells/μl, significantly higher than those of non-infertility women. While no significant differences were found in log2-SII, log2-PPN, log2-PLR, log2-NLR, and log2-LMR between infertility women and non-infertility women.
Associations between inflammatory markers and infertility
The associations between inflammatory markers and infertility were shown in Table 2. In crude model, log2-LC was positively associated with infertility (OR 1.42; 95% CI: 1.00, 2.00; p = 0.05), and the results were stable in model 1, with OR of 1.51 (95% CI: 1.06, 2.16; p = 0.02). However, the results were not significantly stable in model 2 and model 3, with OR of 1.33 (95% CI: 0.93, 1.90; p = 0.12), 1.33 (95% CI: 0.93, 1.92; p = 0.12). No significant association was observed between log2-SII, log2-PPN, log2-PLR, log2-NLR, log2-LMR and infertility in crude model, with OR of 0.95 (95% CI: 0.78, 1.15; p = 0.60), 1.17 (95% CI: 0.94, 1.47; p = 0.15), 0.80 (95% CI: 0.60, 1.05; p = 0.10), 0.87 (95% CI: 0.58, 1.29; p = 0.48), and 1.05 (95% CI: 0.78, 1.41; p = 0.77), respectively. The results were similar in model 1, model 2, and model 3.
Furthermore, when these inflammatory markers were transformed from continuous variables to categorical variables by quartile, we found that women in the highest log2-LC quarter group (Q4) showed significantly highest risk of infertility compared with the lowest log2-LC quarter group (Q1) in both crude model (OR 1.46; 95% CI: 1.04, 2.03; p = 0.03) and model 1 (OR 1.55; 95% CI: 1.11, 2.18; p = 0.01). However, the highest quartile (Q4) of log2-LC were not significantly positively correlate with infertility in model 2 and model 3, with OR of 1.36 (95% CI: 0.95, 1.94; p = 0.09), 1.35 (95% CI: 0.94, 1.94; p = 0.10). The results of the association between log2-PPN by quartile and infertility were similar with log2-LC. Compared with the lowest quartile (Q1), the third quartile (Q3) of log2-SII was negatively correlation with infertility, with an OR (95% CI) of 0.71 (95% CI: 0.49, 1.03; p = 0.07) in crude model, 0.65 (95% CI: 0.44, 0.95; p = 0.03) in model 1, 0.57 (95% CI: 0.38, 0.85; p = 0.01) in model 2, and 0.56 (95% CI: 0.37, 0.85; p = 0.01) in model 3. While the ORs (95% CIs) for infertility with log2-SII levels in Q2 and Q4 in model 3 were 0.77 (95% CI: 0.52, 1.12; p = 0.17), and 0.83 (95% CI: 0.55, 1.27; p = 0.38), respectively. Similarly, the results of the association between log2-PLR by quartile and infertility were similar with log2-SII. No significant association was observed between log2-NLR, log2-LMR by quartile and infertility in model 3.
Restricted cubic spline (RCS) plot was performed to assess the potential non-linearity of the association between infertility and inflammatory markers. In Fig. 2, a similar U-shaped relationship between log2-SII and infertility was found (p for non-linear < 0.05). A non-linear relationship between log2-LC, log2-NLR and infertility was found (p for non-linear < 0.05), however, there were no significant association between log2-LC, log2-NLR by quartile and infertility in model 3 shown in Table 2. Of note, linear relationship could be observed between log2-PPN, log2-PLR, log2-LMR and infertility (p > 0.05).

Restricted cubic spline plot of the association between inflammatory markers and infertility. Legend: A log2-transformed SII; B log2-transformed LC; C log2-transformed PPN; D log2-transformed PLR; E log2-transformed NLR; F log2-transformed LMR. Abbreviation: SII, systemic immune inflammation index; LC, lymphocyte count; PPN, product of platelet and neutrophil count; PLR, platelet to lymphocyte ratio; NLR, neutrophil to lymphocyte ratio; LMR, lymphocyte to monocyte ratio
Subgroup analysis
We performed subgroup analyses to assess the stability of the association between log2-SII, log2-PLR by quartile and the risk of infertility in different populations based on age, BMI, race, marital status, education, smoking status, alcohol user, PIR, PID, and age of menarche (Tables 3 and 4). All covariates in each subgroup analysis model were adjusted, except the stratification variable itself. Compared with the lowest quartile (Q1), the third quartile (Q3) of log2-SII was associated with a decreased risk of infertility among those with BMI < 25 kg/m2 (OR, 0.43; 95% CI: 0.24, 0.79), Black (OR, 0.46; 95% CI: 0.24, 0.90), living alone (OR, 0.38; 95% CI: 0.21, 0.67), Some college or AA degree above (OR, 0.66; 95% CI: 0.46, 0.94), no history of PID (OR, 0.69; 95% CI: 0.50, 0.93). Significant interactions were observed in BMI, race, marital status, education, alcohol user, PIR, PID, and age of menarche (all p for interaction < 0.05), indicating that the negative correlation between log2-SII and infertility was also affected by the interaction among those different subgroups. Compared with the lowest quartile (Q1), the third quartile (Q3) of log2-PLR was consistently associated with a decreased risk of infertility among those aged < 35 years (OR, 0.59; 95% CI: 0.38, 0.91), BMI ≥ 30.0 kg/m2 (OR, 0.57; 95% CI: 0.38, 0.86), White (OR, 0.63; 95% CI: 0.40, 1.01), living alone (OR, 0.58; 95% CI: 0.34, 0.97), Some college or AA degree above (OR, 0.66; 95% CI: 0.46, 0.94), smoking(OR, 0.60; 95% CI: 0.36, 0.99), PIR among 1.5–3.5 (OR, 0.53; 95% CI: 0.32–0.88), no history of PID (OR, 0.71; 95% CI: 0.52, 0.96), and age of menarche < 15 years (OR, 0.70; 95% CI: 0.50, 0.97). Significant interactions were observed in BMI, race, education, PIR, and age of menarche (all p for interaction < 0.05), indicating that the negative correlation between log2-PLR and infertility was also affected by the interaction among those different subgroups. Furthermore, the association between log2-LC, log2-PPN, log2-NLR, log2-LMR by quartile and the risk of infertility in different subgroups were not significant (shown in Supplementary Tables 1, 2, 3 and 4).
Discussion
The findings showed that SII and PLR were negatively associated with infertility after adjusting for potential covariates. The increasing trend in SII, PLR were associated with a lower risk of infertility. No significant association was observed between LC, PPN, NLR, LMR and infertility.
It has been widely accepted that inflammation and immunity play critical role in many causes of female infertility, such as PCOS, endometriosis, genital and pelvic inflammatory diseases, as well as unexplained infertility. Moreover, immunological balance between tolerance of fetus and defense against infections is essential for successful pregnancy. Altered numbers or disturbed function of immune cells contribute to pathogenesis of reproductive adverse events, such as implantation failure, recurrent pregnancy loss and preterm birth [27]. Current diagnostic tests for causes of infertility are expensive, complicated and may cause discomfort to patients. However, several emerging parameters derived from peripheral blood, such as SII, LC, PPN, PLR, NLR and LMR have been accepted as inflammatory markers indicating inflammation and immune status and as possible predictors for immune related diseases with its cost-effective, rapid and convenient characteristics. Nevertheless, these indexes have become novel markers related to diverse pregnancy complications or neonatal outcomes, such as preeclampsia, gestational diabetes mellitus, spontaneous preterm birth, low placental and birth weights [28,29,30,31]. But limited direct evidence of link between these novel markers and infertility could be found.
One of our findings, consistent with earlier study demonstrating that imbalanced lymphocyte ratios or interaction between immune cells involve in the pathogenesis of infertility and disturbed pregnancy [9], was that LC level was elevated in the infertility group indicting LC might be associated with infertility. Higher level of CD19+ B lymphocytes was found in women with infertility and positive antiphospholipid antibodies when compared to healthy women or compared to women with a history of infertility without antiphospholipid antibodies [32]. Dysfunction of B lymphocytes with the production of antibodies among these women suggest that autoimmune process should be related to adverse obstetric outcomes.
For a more comprehensive assessment, we simultaneously assessed the associations between other inflammatory markers derived from PC, NC, MC, LC, and infertility. Interestingly, PPN, an emerging marker that has not been reported in literature about association between inflammatory markers and infertility, was positively related to risk of infertility in model adjusted for age in our study. It has been reported that PPN was associated positively with female estradiol [10]. Tang et al. found that PPN was negatively associated with BMD, indicating PPN may be a convenient marker that could be applied to predict the risk of osteoporosis for postmenopausal women [11]. Different findings of these two studies may be due to women included with different age. Thus, more investigations are needed to determine the association between PPN and reproductive function among women of reproductive age. Recently, a cross-sectional study revealed a significant positive correlation between NLR and PLR among infertility patients [33]. Jing X et al. reported that NLR was independent risk factors of endometriosis related infertility [34] based on a retrospective study comprising 662 women with endometriosis. Our study showed negative association between infertility and NLR, PLR based on a much larger sample size, but the relation between infertility and NLR had no statistical difference. Specific causes of infertility were not available in our study because they were not collected in NHANES datasets. Thus, we speculate that the difference between the two research findings may stem from different causes of infertility among the included population. Moreover, earlier studies have shown that LMR correlate with poor prognosis of patients with acute ischemic stroke and advanced soft tissue sarcoma [13, 14]. Previous cross-sectional study among Chinese women with normal pregnancy indicated that LMR level showed a gradual downward trend along with the trimesters of pregnancy [17]. We found positive association trend between LMR level and infertility in this study but without statistical significance for the first time. Thus, more researches are necessary to clarify the potential connection between LMR level and infertility.
Normal pregnancy is associated with a continuous systemic inflammatory response. The importance of SII has been emphasized because elevated SII has been considered as an effective blood indicator reflecting systemic inflammation conditions, such as increased risk of malignancy, depression, cognitive impairment, cardiopulmonary, rheumatic, and metabolic diseases [18, 35,36,37,38,39,40,41,42]. Nonetheless, the relationship between SII and infertility has not been reported yet. Findings on relationship between SII and reproductive health seemed to be controversial. Previous studies showed that clinical value of higher SII level for the prediction of miscarriage and adverse neonatal outcomes [43, 44], while SII showed dynamic changes during pregnant trimesters and the upper limit of SII in the second trimester showed the highest value [17]. The latter study supported the presumption that lower SII level may exert adverse influence on pregnancy, which is consistent with the negative relationship between SII and infertility in our study.
To our knowledge, this is the first study to assess the association between inflammatory markers including SII, LC, PPN, PLR, NLR, LMR and infertility based on the US NHANES data of women aged 20–45 years. We believe that this study is an important preliminary exploration of the relationship between inflammatory markers and infertility and has significant value for further research on the relationship and mechanism between inflammatory markers and infertility in the future. Findings from this study emphasized the clinical value of these markers, such as replacing current expensive standard tests for infertility diagnosis, predicting infertility prognosis and effects of assisted reproductive technology. Since these parameters are cheap, easy to apply and significantly associated with infertility prevalence, further study on the underlying mechanism of the relationship between these inflammatory markers and infertility should be performed.
There are several limitations in this study. First, the causality between risk of infertility and these inflammatory markers could not be established due to the cross-sectional design of this study. There may be intriguing interaction between infertility and inflammation immune response. Second, in the view of that some information was collected based on participants self-reported questionnaires, there might be recall bias in this study. Third, it is clear that male factors should be considered in infertility related research. However, semen analysis of the male partner and the specific causes of infertility were unavailable in this study, due to male related reproductive questionnaire was not collected in the NHANES database and female reproductive questionnaire also did not collect causes of infertility. In addition, prevalence of self-reported infertility in our study was 13.88%, which was similar to previous one [45], indicating sample in our study was representative for the US population. Finally, anti-Müllerian hormone (AMH) and basal sexual hormones have been regarded as essential measurements in the diagnosis and treatment of infertility. We failed to include AMH and basal sexual hormones as covariates in this study because they were unavailable in NHANES2013-2020 datasets. However, we did another analysis via collecting serum estradiol, total testosterone, and sex hormone binding globulin levels available in 2013–2016 NHANES datasets as parts of covariates and found the association between inflammatory markers and infertility remained consistent (results not shown).
Conclusion
Taken together, findings in this study showed that SII and PLR were negatively associated with infertility and infertile women should be aware of SII, PLR. Further studies are needed to explore their association better and the underlying mechanisms.
Availability of data and materials
The datasets supporting the conclusions of this article are available in the NHANES [https://www.cdc.gov/nchs/nhanes/].
References
Sun H, Gong TT, Jiang YT, Zhang S, Zhao YH, Wu QJ. Global, regional, and national prevalence and disability-adjusted life-years for infertility in 195 countries and territories, 1990–2017: results from a global burden of disease study, 2017. Aging (Albany NY). 2019;11(23):10952–91.
Practice Committee of the American Society for Reproductive Medicine. Evidence-based treatments for couples with unexplained infertility: a guideline. Fertil Steril. 2020;113(2):305–22.
Romualdi D, Ata B, Bhattacharya S, Bosch E, Costello M, Gersak K, et al. Evidence-based guideline: unexplained infertility†. Hum Reprod. 2023;38(10):1881–90.
Tola EN. The association between in vitro fertilization outcome and the inflammatory markers of complete blood count among nonobese unexplained infertile couples. Taiwan J Obstet Gynecol. 2018;57(2):289–94.
Luan YY, Zhang L, Peng YQ, Li YY, Liu RX, Yin CH. Immune regulation in polycystic ovary syndrome. Clin Chim Acta. 2022;531:265–72.
Vallvé-Juanico J, Houshdaran S, Giudice LC. The endometrial immune environment of women with endometriosis. Hum Reprod Update. 2019;25(5):564–91.
Ji Y, Wang H. Prognostic prediction of systemic immune-inflammation index for patients with gynecological and breast cancers: a meta-analysis. World J Surg Oncol. 2020;18(1):197.
He S, Mao X, Lei H, Dong B, Guo D, Zheng B, et al. Peripheral blood inflammatory-immune cells as a predictor of infertility in women with polycystic ovary syndrome. J Inflamm Res. 2020;13:441–50.
Jafarpour R, Pashangzadeh S, Mehdizadeh S, Bayatipoor H, Shojaei Z, Motallebnezhad M. Functional significance of lymphocytes in pregnancy and lymphocyte immunotherapy in infertility: a comprehensive review and update. Int Immunopharmacol. 2020;87:106776.
Wei C, Zhang W, Chen J, He Q, Cao L, Zhang P, et al. Systematic analysis between inflammation-related index and sex hormones in American adults: cross-sectional research based NHANES 2013–2016. Front Immunol. 2023;14:1175764.
Tang Y, Peng B, Liu J, Liu Z, Xia Y, Geng B. Systemic immune-inflammation index and bone mineral density in postmenopausal women: a cross-sectional study of the national health and nutrition examination survey (NHANES) 2007–2018. Front Immunol. 2022;13:975400.
Yilmaz MA, Duran C, Basaran M. The mean platelet volume and neutrophil to lymphocyte ratio in obese and lean patients with polycystic ovary syndrome. J Endocrinol Invest. 2016;39(1):45–53.
Zhang YX, Shen ZY, Jia YC, Guo X, Guo XS, Xing Y, et al. The Association of the neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, lymphocyte-to-monocyte ratio and systemic inflammation response index with short-term functional outcome in patients with acute ischemic stroke. J Inflamm Res. 2023;16:3619–30.
Watanabe S, Shimoi T, Nishikawa T, Kawachi A, Okuma HS, Tokura M, et al. Lymphocyte-to-monocyte ratio as a prognostic and potential tumor microenvironment indicator in advanced soft tissue sarcoma treated with first-line doxorubicin therapy. Sci Rep. 2023;13(1):10734.
Song Q, Xu SX, Wu JZ, Ling L, Wang S, Shu XH, et al. The preoperative platelet to neutrophil ratio and lymphocyte to monocyte ratio are superior prognostic indicators compared with other inflammatory biomarkers in ovarian cancer. Front Immunol. 2023;14:1177403.
Maloney S, Pavlakis N, Itchins M, Arena J, Mittal A, Hudson A, et al. The Prognostic and Predictive Role of the Neutrophil-to-Lymphocyte Ratio (NLR), Platelet-to-Lymphocyte Ratio (PLR), and Lymphocyte-to-Monocyte Ratio (LMR) as biomarkers in resected pancreatic cancer. J Clin Med. 2023;12(5):1989.
Bai YY, Xi Y, Yin BB, Zhang JH, Chen F, Zhu B. Reference intervals of systemic immune-inflammation index, neutrophil-to-lymphocyte ratio, lymphocyte-to-monocyte ratio, and platelet-to-lymphocyte ratio during normal pregnancy in China. Eur Rev Med Pharmacol Sci. 2023;27(3):1033–44.
Xu JP, Zeng RX, Zhang YZ, Lin SS, Tan JW, Zhu HY, et al. Systemic inflammation markers and the prevalence of hypertension: a NHANES cross-sectional study. Hypertens Res. 2023;46(4):1009–19.
Ke J, Qiu F, Fan W, Wei S. Associations of complete blood cell count-derived inflammatory biomarkers with asthma and mortality in adults: a population-based study. Front Immunol. 2023;14:1205687.
Zinellu A, Zinellu E, Mangoni AA, Pau MC, Carru C, Pirina P, et al. Clinical significance of the neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio in acute exacerbations of COPD: present and future. Eur Respir Rev. 2022;31(166):220095.
Guldbrandsen K, Håkonsen LB, Ernst A, Toft G, Lyngsø J, Olsen J, et al. Age of menarche and time to pregnancy. Hum Reprod. 2014;29(9):2058–64.
Practice Committee of the American Society for Reproductive Medicine. Smoking and infertility: a committee opinion. Fertil Steril. 2018;110(4):611–8.
Bala R, Singh V, Rajender S, Singh K. Environment, lifestyle, and female infertility. Reprod Sci. 2021;28(3):617–38.
Brunham RC, Gottlieb SL, Paavonen J. Pelvic inflammatory disease. N Engl J Med. 2015;372(21):2039–48.
Grodstein F, Goldman MB, Cramer DW. Infertility in women and moderate alcohol use. Am J Public Health. 1994;84(9):1429–32.
Rafael F, Rodrigues MD, Bellver J, Canelas-Pais M, Garrido N, Garcia-Velasco JA, et al. The combined effect of BMI and age on ART outcomes. Hum Reprod. 2023;38(5):886–94.
Robertson SA, Moldenhauer LM, Green ES, Care AS, Hull ML. Immune determinants of endometrial receptivity: a biological perspective. Fertil Steril. 2022;117(6):1107–20.
Hessami K, Tabrizi R, Homayoon N, Hashemi A, Heydari ST, Pourhoseini SA. Gestational diabetes mellitus and inflammatory biomarkers of neutrophil-lymphocyte ratio and platelet-lymphocyte ratio: a systematic review and meta-analysis. Biomarkers. 2021;26(6):491–8.
Elmaradny E, Alneel G, Alkhattaf N, AlGadri T, Albriakan N. Predictive values of combined platelet count, neutrophil-lymphocyte ratio, and platelet-lymphocyte ratio in preeclampsia. J Obstet Gynaecol. 2022;42(5):1011–7.
Zhang YH, Zhen MH, Zeng YF, Lao L, Ai W. Complete blood count during the first trimester predicting spontaneous preterm birth. Eur Rev Med Pharmacol Sci. 2022;26(15):5489–95.
de Moreuil C, Herry E, Lacut K, Chauvet J, Moineau MP, Lede F, et al. Correlation of biological parameters with placental parameters and pregnancy outcomes in pre-eclamptic women. Pregnancy Hypertens. 2020;19:61–6.
Krivonos MI, KhKhizroeva J, Zainulina MS, Eremeeva DR, Selkov SA, Chugunova A, et al. The role of lymphocytic cells in infertility and reproductive failures in women with antiphospholipid antibodies. J Matern Fetal Neonatal Med. 2022;35(5):871–7.
Duan Y, Zhou Y, Peng Y, Shi X, Peng C. Inflammatory markers in women with infertility: a cross-sectional study. Int J Gen Med. 2023;16:1113–21.
Jing X, Li C, Sun J, Peng J, Dou Y, Xu X, et al. Systemic inflammatory response markers associated with infertility and endometrioma or uterine leiomyoma in endometriosis. Ther Clin Risk Manag. 2020;16:403–12.
Luo Z, Wang W, Xiang L, Jin T. Association between the systemic immune-inflammation index and prostate cancer. Nutr Cancer. 2023;75(10):1918–25.
Xie R, Liu X, Wu H, Liu M, Zhang Y. Associations between systemic immune-inflammation index and abdominal aortic calcification: results of a nationwide survey. Nutr Metab Cardiovasc Dis. 2023;33(7):1437–43.
Ye C, Yuan L, Wu K, Shen B, Zhu C. Association between systemic immune-inflammation index and chronic obstructive pulmonary disease: a population-based study. BMC Pulm Med. 2023;23(1):295.
Zhao E, Cheng Y, Yu C, Li H, Fan X. The systemic immune-inflammation index was non-linear associated with all-cause mortality in individuals with nonalcoholic fatty liver disease. Ann Med. 2023;55(1):2197652.
Liu B, Wang J, Li YY, Li KP, Zhang Q. The association between systemic immune-inflammation index and rheumatoid arthritis: evidence from NHANES 1999–2018. Arthritis Res Ther. 2023;25(1):34.
Li X, Huan J, Lin L, Hu Y. Association of systemic inflammatory biomarkers with depression risk: results from national health and nutrition examination survey 2005–2018 analyses. Front Psychiatry. 2023;14:1097196.
Li W, Li S, Shang Y, Zhuang W, Yan G, Chen Z, et al. Associations between dietary and blood inflammatory indices and their effects on cognitive function in elderly Americans. Front Neurosci. 2023;17:1117056.
Xie R, Xiao M, Li L, Ma N, Liu M, Huang X, et al. Association between SII and hepatic steatosis and liver fibrosis: a population-based study. Front Immunol. 2022;13:925690.
Turgut E, Yildirim M, Sakcak B, Ayhan SG, Tekin OM, Sahin D. Predicting miscarriage using systemic immune-inflammation index. J Obstet Gynaecol Res. 2022;48(3):587–92.
Tanacan A, Uyanik E, Unal C, Beksac MS. A cut-off value for systemic immune-inflammation index in the prediction of adverse neonatal outcomes in preterm premature rupture of the membranes. J Obstet Gynaecol Res. 2020;46(8):1333–41.
Practice Committee of the American Society for Reproductive Medicine. Diagnostic evaluation of the infertile female: a committee opinion. Fertil Steril. 2015;103(6):e44.
Acknowledgements
We express our gratitude to all researchers and participants involved in the NHANES program.
Ethics statement
NHANES was approved by the National Center for Health Statistics Institutional Review Board and informed consent of individuals were obtained before participance in this program.
Funding
This study was funded by Basic and Applied Basic Research Foundation of Guangdong Province (No. 2022A1515220178), Science and Technology Innovation project of Foshan Science and Technology Bureau (No. 2016AG100531), and Guangdong TCM anti-aging Engineering Technology Research Center (No. 2022E040). Funders of the study play no role in the study design, data collection, data analysis, data interpretation, or writing of the report.
Author information
Authors and Affiliations
Contributions
CY: designed study, collected and analyzed data, wrote original draft. XY: designed study and analyzed data. YX: analyzed data and wrote original draft. WD, MJ, XN, XY, ZX, WJ: critically reviewed the study. WZ: examine and revise the article.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was conducted in accordance with the Declaration of Helsinki and was approved by the National Center for Health Statistics Research Ethics Review Committee (https://www.cdc.gov/nchs/nhanes/irba98.htm). All survey participants provided written informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Supplementary Figure 1.
Distribution of inflammatory markers among individuals included. Legend: (A) SII; (B) LC; (C) PPN; (D) PLR; (E) NLR; (F) LMR were measured in 1×103 cells/μL. SII, systemic immune inflammation index; LC, lymphocyte count; PPN, product of platelet and neutrophil count; PLR, platelet to lymphocyte ratio; NLR, neutrophil to lymphocyte ratio; LMR, lymphocyte to monocyte ratio.
Additional file 2: Supplementary Figure 2.
Distribution of log2-transformed inflammatory markers among individuals included. Legend: (A) log2-transformed SII; (B) log2-transformed LC; (C) log2-transformed PPN; (D)log2-transformed PLR; (E) log2-transformed NLR; (F) log2-transformed LMR. SII, systemic immune inflammation index; LC, lymphocyte count; PPN, product of platelet and neutrophil count; PLR, platelet to lymphocyte ratio; NLR, neutrophil to lymphocyte ratio; LMR, lymphocyte to monocyte ratio.
Additional file 3: Supplementary Table 1.
Subgroup analyses for the relationship between log2-LC and infertility. Legend: Note: The model was adjusted for age(categorical), BMI (categorical), race (Mexican, Hispanic, White, Black, and Other race), marital status (living alone, and married/living with partner), education (Some college or AA degree above, High school or GED, and Less than 11th grade), smoking status (No, Yes), alcohol user (never, former, mild, and heavy) and PIR (<1.5, 1.5-3.5, and ≥3.5), PID (No, Yes), and age of menarche (<15 years or ≥15 years). All covariates in the subgroup analysis models were adjusted, excepting the stratification variable itself (for example, “age” was not included as a covariate in the age subgroup). P value in bold indicates statistical significance. Abbreviation: BMI, body mass index; OR, odds ratios; CI, confidence interval; ref, reference group. LC, lymphocyte count; Q1, the first quartile; Q2, the second quartile; Q3, the third quartile; Q4, the highest quartile. Supplementary Table 2. Subgroup analyses for the relationship between log2-PPN and infertility. Legend: Note: The model was adjusted for age(categorical), BMI (categorical), race (Mexican, Hispanic, White, Black, and Other race), marital status (living alone, and married/living with partner), education (Some college or AA degree above, High school or GED, and Less than 11th grade), smoking status (No, Yes), alcohol user (never, former, mild, and heavy) and PIR (<1.5, 1.5-3.5, and ≥3.5), PID (No, Yes), and age of menarche (<15 years or ≥15 years). All covariates in the subgroup analysis models were adjusted, excepting the stratification variable itself (for example, “age” was not included as a covariate in the age subgroup). P value in bold indicates statistical significance. Abbreviation: BMI, body mass index; OR, odds ratios; CI, confidence interval; ref, reference group; PPN, product of platelet and neutrophil count; Q1, the first quartile; Q2, the second quartile; Q3, the third quartile; Q4, the highest quartile. Supplementary Table 3. Subgroup analyses for the relationship between log2-NLR and infertility. Legend: Note: The model was adjusted for age(categorical), BMI (categorical), race (Mexican, Hispanic, White, Black, and Other race), marital status (living alone, and married/living with partner), education (Some college or AA degree above, High school or GED, and Less than 11th grade), smoking status (No, Yes), alcohol user (never, former, mild, and heavy) and PIR (<1.5, 1.5-3.5, and ≥3.5), PID (No, Yes), and age of menarche (<15 years or ≥15 years). All covariates in the subgroup analysis models were adjusted, excepting the stratification variable itself (for example, “age” was not included as a covariate in the age subgroup). P value in bold indicates statistical significance. Abbreviation: BMI, body mass index; OR, odds ratios; CI, confidence interval; ref, reference group; NLR, neutrophil-lymphocyte ratio; Q1, the first quartile; Q2, the second quartile; Q3, the third quartile; Q4, the highest quartile. Supplementary Table 4. Subgroup analyses for the relationship between log2-LMR and infertility. Legend: Note: The model was adjusted for age(categorical), BMI (categorical), race (Mexican, Hispanic, White, Black, and Other race), marital status (living alone, and married/living with partner), education (Some college or AA degree above, High school or GED, and Less than 11th grade), smoking status (No, Yes), alcohol user (never, former, mild, and heavy) and PIR (<1.5, 1.5-3.5, and ≥3.5), PID (No, Yes), and age of menarche (<15 years or ≥15 years). All covariates in the subgroup analysis models were adjusted, excepting the stratification variable itself (for example, “age” was not included as a covariate in the age subgroup). P value in bold indicates statistical significance. Abbreviation: BMI, body mass index; OR, odds ratios; CI, confidence interval; ref, reference group; LMR, lymphocyte-monocyte ratio; Q1, the first quartile; Q2, the second quartile; Q3, the third quartile; Q4, the highest quartile.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Chen, Y., Xu, H., Yan, J. et al. Inflammatory markers are associated with infertility prevalence: a cross-sectional analysis of the NHANES 2013–2020. BMC Public Health 24, 221 (2024). https://doi.org/10.1186/s12889-024-17699-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-024-17699-4