
Abstract
Background
Hypertension caused by air pollution exposure is a growing concern in China. The association between air pollutant exposure and hypertension has been found to be potentiated by obesity, however, little is known about the processes mediating this association. This study investigated the association between fine particulate matter (aerodynamic equivalent diameter ≤ 2.5 microns, PM2.5) exposure and the prevalence of hypertension in a representative population in southern China and tested whether obesity mediated this association.
Methods
A total of 14,308 adults from 48 communities/villages in southern China were selected from January 2015 to December 2015 using a stratified multistage random sampling method. Hourly PM2.5 measurements were collected from the China National Environmental Monitoring Centre. Restricted cubic splines were used to analyze the nonlinear dose-response relationship between PM2.5 exposure and hypertension risk. The mediating effect mechanism of obesity on PM2.5-associated hypertension was tested in a causal inference framework following the approach proposed by Imai and Keele.
Results
A total of 20.7% (2966/14,308) of participants in the present study were diagnosed with hypertension. Nonlinear exposure-response analysis revealed that exposure to an annual mean PM2.5 concentration above 41.8 µg/m3 was associated with increased hypertension risk at an incremental gradient. 9.1% of the hypertension burden could be attributed to exposure to elevated annual average concentrations of PM2.5. It is noteworthy that an increased body fat percentage positively mediated 59.3% of the association between PM2.5 exposure and hypertension risk, whereas body mass index mediated 34.3% of this association.
Conclusions
This study suggests that a significant portion of the estimated effect of exposure to PM2.5 on the risk of hypertension appears to be attributed to its effect on alterations in body composition and the development of obesity. These findings could inform intersectoral actions in future studies to protect populations with excessive fine particle exposure from developing hypertension.
Similar content being viewed by others

Introduction
Hypertension is a globally prevalent condition and contributes to millions of deaths from cardiovascular and renal diseases worldwide [1]. Over the past 30 years, new cases of hypertension have mainly been distributed in East Asia, the Pacific, and sub-Saharan Africa, according to surveillance data from 200 countries worldwide [1]. With the number of hypertensive individuals doubling over the past 20 years, China has the highest absolute burden of hypertension in the world, with over 240 million people affected [2, 3]. Furthermore, China is one of the regions worldwide with a great increase in average systolic and diastolic blood pressure over the past 40 years [4]. The increasing burden of hypertension has led to excessive mortality in the Chinese population [5,6,7]. Therefore, identifying and addressing controllable risk factors for hypertension is a priority.
Air quality in China poses serious challenges. A national survey showed that exposure to atmospheric emissions, especially fine particulate matter (aerodynamic diameter ≤ 2.5 μm, PM2.5), was strongly related to an increased risk of hospitalization for 7 major disease categories during 2013–2017 [8]. In addition, abundant epidemiological evidence suggests that long- or short-term exposure to high concentrations of ambient PM2.5 has increased the risk of hypertension in the past decade [9,10,11,12,13,14]. Possible reasons include the following: (a) the impact of PM2.5 exposure on vascular dysfunction and remodeling [15,16,17]; (b) possible systemic inflammation, oxidative stress, and altered neuroendocrine factors caused by PM2.5 exposure [18, 19]; and (c) other unclear drivers.
Inconsistent results have been shown for the dose-effect relationship between PM2.5 exposure and the risk of hypertension, as observed and measured in different surveys. For instance, based on a survey involving 43,745 7–18-year-old individuals seeking treatment in China, Zhang and his colleagues found that each 10 µg/m3 increase in environmental PM2.5 levels was associated with a 1.46-mmHg increase in systolic blood pressure (SBP) or a 45% higher risk of hypertension [14]. Xie et al. reported that an increase of 10 µg/m3 of PM2.5 was associated with an odds ratio (OR) of 1.010 for hypertension and a 0.569-mmHg increase in SBP in reproductive-age adults [20]. This inconsistent result may be related to the demographic characteristics or geographic heterogeneity of the subjects. More critically, potential mediators or modifiers of PM2.5-associated hypertension are important but still not fully recognized regarding the occurrence of hypertension.
Overweight and obesity have been observed to enhance susceptibility to air pollutant-related cardiovascular disease [21, 22]. Previous studies have found that obesity may mediate the relationship between air pollution and hypertension [21]. Unfortunately, these studies mainly focused on the traditional parameters of obesity, such as body mass index (BMI) and waist circumference; however, BMI does not distinguish between lean body mass and fat body mass, while adipose tissue is an important source of vasoconstrictor activators induced by air pollutants [23], suggesting that BMI may be insufficient for assessing the effects of air pollution on hypertension risk [24]. In this study, we focused on whether body fat percentage (BF%), an indicator that provides information on cardiovascular risk in low BMI conditions [25, 26], mediates the association between air pollution exposure and hypertension risk. The selection of potential mediators was based on the following evidence: (a) a prospective cohort study showing that exposure to air pollutants strongly affects BF% [27]; and (b) epidemiological evidence indicating that BF% is an independent risk factor for the onset of hypertension in postmenopausal women [28] and elderly individuals [29].
The purpose of this study was to assess the exposure-response relationship, population-attributable risk fraction, and potential mediators of the relationship between ambient PM2.5 exposure and hypertension risk in multiethnic adults in South China. Our research provides clinically accessible and optimized indicators for large-scale community health surveillance aimed at assessing the impact of air pollution exposure on hypertension risk and provides new insights into the development of public health policies to ameliorate the burden of hypertension in regions with high air pollution exposure.
Materials and methods
Study population
This population-based cross-sectional survey was part of The China Hypertension Survey [2, 30]. In this study, a nationally representative sample of Chinese community residents aged ≥ 15 years was obtained using a multistage stratified random sampling method.
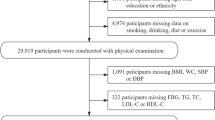
Given that environmental and biological differences among regions may corrode the association between air pollutant exposure and hypertension risk [3, 4], the inclusion of a homogeneous population from the same region as the study population was beneficial in minimizing this effect. We selected residents of the Guangxi Zhuang Autonomous Region as the major population to improve the robustness and scientific replicability of results for future investigations. A total of 17 100 residents (defined as individuals residing for 12 months or longer) from 48 communities or villages in this region were enrolled in this subset analysis. After exclusion (n = 262) due to missing information on blood pressure (BP) value or address, 16,838 individuals were eligible and completed the questionnaire. Participants aged ≥ 18 years (n = 14,308) were included in the final analysis. The participant recruitment and screening process is presented in Fig. 1. For each participant, the process of the survey was well-communicated and written informed consent was obtained. The Ethics Committee of The First Affiliated Hospital of Guangxi Medical University (Guangxi, China) approved the study (approval number: 2012[KY-E-017]). This study was conducted in strict accordance with the Declaration of Helsinki. This study has been registered on the Chinese Clinical Trials Registry (ChiCTR-ECS-14,004,641).

The flow chart of the study population selection
Data collection
A standardized questionnaire was utilized to obtain information on demographic and socioeconomic characteristics. BMI was derived by dividing weight by the square of height (kg/m2). BF% was measured by a weight and body fat measurement device (V-Body HBF-371; OMRON Corporation, Tokyo, Japan), which was calibrated by the manufacturer. Participants underwent 3 times BP measurements using a professional BP monitor (HBP-1300, OMRON Corporation, Tokyo, Japan). Subsequently, the average value of the 3 BP measurements was utilized for analysis, as documented in a previous report [2].
Outcome definitions
Hypertension was defined as meeting at least one of the following criteria: (a) an SBP ≥ 140 mmHg and/or a diastolic blood pressure (DBP) ≥ 90 mmHg; and (b) taking medication to lower BP within 2 weeks [31]. Overweight was defined as a BMI ≥ 24 kg/m2. The remaining variables not mentioned were defined in detail in a previous article [30].
Assessment of PM2.5 exposure
In this study, 8 air quality monitoring stations located in Nanning (station code 1401-1408 A), 7 stations located in Liuzhou (station code 1870-1875 A), 4 stations located in Guilin (station code 1862-1865 A), 3 stations located in Yulin (station code 2509-2511 A), 3 stations located in Qinzhou (station code 2502-2504 A), 3 stations located in Hechi (station code 2516-2518 A) and 2 stations located in Laibin (station code 2519-2520 A) were selected for data collection, and hourly PM2.5 measurements from January 1, 2013, to December 31, 2015, were obtained from open source data on the Ministry of Ecology and Environment of the People’s Republic of China website (http://www.mee.gov.cn/).
The 24-hour average PM2.5 concentration was calculated based on hourly measurements, with at least 18 h of available measurements required for a natural day. The geographic locations of the 48 communities or villages were obtained by questionnaire. We matched places of residence with PM2.5 data from the nearest air quality monitoring station according to distance on the Auto Navi Map.
Statistical analysis
SPSS 22.0 (IBM Corp., Armonk, N.Y., USA) and R software 4.1.3 (R Foundation for Statistical Computing, Vienna, Austria) were utilized to perform statistical analysis, and a two-tailed p value < 0.05 was considered statistically significant. Continuous variables are expressed as the mean (± standard deviation) or median (interquartile range). Categorical variables were presented as numbers and percentages. Student’s t tests or Wilcoxon rank tests for continuous variables, and chi-square tests for categorical variables were applied to perform intergroup comparisons. Contemporaneous national census data were employed to establish an age-standardized prevalence of hypertension.
To determine the potential nonlinear association between PM2.5 exposure and hypertension risk, we built restricted cubic splines with knots calculated on the basis of the minimum Akaike information criterion (AIC) value as the previous report [32]. Owing to the multistage random sampling resulting in the clustering of participants with a multilevel structure, we conducted a two-level logistic regression model to estimate the association between 12-month average PM2.5 exposure and the risk of hypertension in adults in southern China, where individuals were defined as first-level groups and communities and villages were defined as second-level groups, as described in previous research [33]. In addition, the following baseline variables were considered potential confounding variables for the occurrence of hypertension: demographic, socioeconomic, and lifestyle characteristics, such as sex, age, race, smoking status, family history of hypertension, BMI, alcohol consumption, education level, and residence type. PM2.5 exposure was categorized into quartiles (Q1: ≤ 25th percentile, Q2: [between the 25th and 50th percentile], Q3: [between the 50th and 75th percentile] and Q4: > 75th percentile), and the minimal PM2.5 exposure group (Q1) was used as a reference to assess the association between exposure and hypertension risk. In the sensitivity analysis, we explored the mean PM2.5 exposure levels at 1, 2, and 3 years and their associations with the risk of hypertension. We further matched identifiable variables (age, sex, and BMI) using the propensity score matching method.
Estimation of the attributable hypertension burden
Population-attributed risk fraction (PAR%) and attributable cases were used to estimate the increased hypertension burden attributable to environmental PM2.5 exposure. The PAR% was calculated using the following equation: PAR% = P (OR-1) / [1 + P (OR-1)] *100%, where P is the hypertension prevalence among individuals exposed to high annual average PM2.5 concentrations. The standard error of the PAR% was calculated using the delta method. Cases of hypertension attributed to PM2.5 exposure were estimated as follows: Attributable cases = Overall cases * PAR%.
Mediation analysis
Experimental and epidemiological findings indicate that obesity and metabolic pathways that are perturbed by air pollution exposure may lead to hypertension [34,35,36,37,38]; thus, they could be considered mediators in the causal pathways. Obesity indicators such as BMI have been used to explain the biological mechanisms linking air pollution exposure and dyslipidemia risk [39]; and glucose homeostasis [40]. The mediating effects of obesity in the relationship between air pollution exposure and hypertension risk, particularly the indicators with the strongest mediating effects, are still poorly understood. Causal mediation analysis is a typical technique used to evaluate mediating effects in recognizing causal effects [41, 42]. Compared to classical methods, the modified causal mediation analysis approach of Imai and Keele is considered more appropriate for use in conditions where the independent variable is nonlinearly associated with the dependent variable [43, 44].
In the present study, we treated obesity parameters, including BMI, BF%, waist circumference, and weight as potential mediators of the pathway from air pollutant exposure to hypertension. We followed a standard procedure for mediation analyses [45] involving three main steps to perform a series of linear and multivariable logistic regressions adjusted for sex, age (regarded as a categorical variable), ethnicity, current smoking status, BMI, alcohol consumption, education, urbanity, locations, and family history of hypertension. In the initial step, we conducted an evaluation to examine the associations between exposure (ambient PM2.5 concentration over a period of 1–3 years) and the outcome (hypertension). Subsequently, we assessed the association of exposure with mediators and mediators with outcomes separately. In the third step, the potential mediators and exposure were included in a linear regression to examine the direct or indirect effects of PM2.5 exposure on hypertension risk. Mediation models were fitted using a mediation package in the R software.
Results
Descriptive statistics
A total of 14,308 adults (7516 females and 6792 males, 57.6% from urban areas and 42.4% from rural areas) in South China were included in the final analysis. The detailed baseline characteristics of the participants are presented in Table 1. The spatial distribution of the participants and their average annual PM2.5 exposure levels are shown in Fig. 2.

Geographic location and 12-month average PM2.5 exposure levels of 14 308 participants from 48 communities or villages in south China in 2015. The blue dot represented a single selected community or village
In the present study, the participants had a mean SBP of 126.9 mmHg and a mean DBP of 74.4 mmHg, with a crude hypertension prevalence of 20.7% (Table 1). Patients with hypertension were more likely to be older than 60 years, have been exposed to higher 12-month average ambient PM2.5 levels, and had higher BMI, BF%, waist circumference, and weight compared to controls.
The nonlinear relationship between ambient PM2.5 exposure and hypertension risk
As shown in Fig. 3, we used restricted cubic splines to flexibly model and visualize the relationship between annual PM2.5 exposure, age, and BMI and the risk of hypertension in the southern Chinese population. As presented in Fig. 3A, we observed a nonlinear relationship between the average annual PM2.5 concentration and the risk of hypertension (nonlinear p = 0.018). The relationship between PM2.5 exposure and the risk of hypertension exhibited an amplified slope when the concentration exceeded 41.8 µg/m3 (Fig. 3A). In addition, when considered as a continuous variable, age and BMI were significantly and nonlinearly associated with the risk of hypertension (nonlinear p < 0.001, Fig. 3B C).

Concentration-response curves for the effects of ambient PM2.5(A), age (B), and body mass index (C) on hypertension. OR means odds ratio. Distribution of Propensity score (D) of participants before and after matching
Impact of annual PM2.5 exposure on the risk of hypertension in South China
For the assessment of the effect size of ambient PM2.5 exposure affecting the risk of hypertension, logistic regression analyses were performed with a minimum 25% PM2.5 exposure or an annual average below 41.8 µg/m3 as references, adjusting for potential confounders including sex, age (considered as a categorical variable), race, current smoking status, BMI, alcohol consumption, educational level, urbanization, location, and family history of hypertension. The results showed that each 5 µg/m3 increase in annual mean PM2.5 exposure was associated with a 4% higher risk of hypertension (OR = 1.040, 95% confidence interval (CI) = 1.007–1.062). Furthermore, individuals exposed to annual average PM2.5 concentrations above 41.8 µg/m3 was associated with an 18.3% increased risk of hypertension compared to those with lower average exposure (OR = 1.183, 95%CI = 1.165–1.212). As mentioned previously, exposure to higher mean annual PM2.5 concentration was associated with an increased risk of individual hypertension in a nonlinear pattern with ORs of 1.038 (95%CI = 1.006–1.058) (Q2 vs. Q1), 1.084 (95%CI = 1.071–1.102) (Q3 vs. Q1), and 1.421 (95%CI = 1.308–1.561) (Q4 vs. Q1), respectively (Table 2). Sensitivity analyses demonstrated that the estimates of hypertension risk associated with exposure to high ambient PM2.5 concentrations remained robust after propensity score matching for age, sex, and BMI (see Table S1 and Fig. 3D), consistent with previous reports [46]. Alternative analyses using 1-, 2-, and 3-year mean air pollution exposures consistently generated similar estimates (Table S2).
As presented in Table 3, in 9.1% (95% CI = 8.3-10.4%) or 270 patients (95% CI = 245–308) out of a total of 2966 patients, hypertension could be attributed to exposure at annual average PM2.5 concentrations higher than 41.8 µg/m3. Similar effects on the burden of hypertensive disease attributable to PM2.5 exposure were observed in the sex and age subgroups. Only 6% of participants with a BMI < 24 kg/m2 had hypertension that could be attributed to PM2.5 exposure, while this percentage was as high as 14.4% in those with a BMI ≥ 24 kg/m2.
Association between body composition, obesity, and PM2.5 exposure
Partial correlation coefficients were estimated to examine the correction among obesity parameters with annual mean PM2.5 concentrations and high blood pressure, as shown in Table S3. Furthermore, we evaluated the eligibility of 4 obesity indicators that should serve as mediators of the association between PM2.5 exposure and hypertension risk by multivariate linear and logistic regression. As shown in Table 4, increased PM2.5 levels per standard deviation (SD) were associated with higher SBP (β = 0.198, 95% CI = 0.102–0.294) and DBP (β = 0.250, 95% CI = 0.202–0.299). Higher PM2.5 was significantly associated with increased BMI (β = 0.173, 95% CI = 0.075–0.271), BF% (β = 0.242, 95% CI = 0.189–0.294), WC (β = 0.155, 95% CI = 0.134–0.177), and weight (β = 0.146, 95% CI = 0.125–0.167) in residents.
Association between body composition, obesity, and hypertension
In the models assessing the association between mediators and hypertension risk, we observed that exposure to each 1 SD of higher BMI (OR = 1.130, 95% CI = 0.075–0.271), BF% (OR = 1.145, 95% CI = 1.138–1.151), WC (OR = 1.102, 95% CI = 1.092–1.113), and weight (OR = 1.086, 95% CI = 1.076–1.096) was significantly associated with an increased hypertension risk, after adjusting for covariates mentioned in the previous section (Table 4). Moreover, consistent associations were observed between the mediators and both SBP and DBP measurements.
Furthermore, all 4 obesity parameters were associated with exposure to high annual mean PM2.5 concentrations and an increased risk of hypertension and corroded the association between PM2.5 exposure and the risk of hypertension when included in the model, as shown in Table 5.
Mediation analysis
We further conducted a mediation analysis to explore the potential mediating effects of obesity and body composition indicators on the association between PM2.5 exposure and hypertension risk. Mediation analyses adjusting for potential confounders showed that 59.3% (95% CI = 52.4-68.0%, p < 0.001) of the excess risk of hypertension associated with exposure to high annual average PM2.5 concentrations was attributed to elevated BF% (Fig. 4A), while 34.3% (95% CI = 29.5-41.3%, p < 0.001) of the excess risk was mediated by elevated BMI, 15.7% (95% CI = 8.1-20.0%, p < 0.001) was mediated by elevated waist circumference and 12.4% (95% CI = 6.7-17.2%, p < 0.001) was mediated by elevated weight (Fig. 4B and D).

It was estimated that body fat percentage (A) mediated the highest association between PM2.5 concentration and hypertension, over body mass index (B), waist circumference (C), and weight (D). ACME, average causal mediation effects. ADE, average direct effects
Discussion
The study findings revealed a non-linear association between high ambient concentrations of PM2.5 and an increased risk of hypertension. Additionally, it was estimated that 9.1% of the burden of hypertension could be attributed to exposure to an annual average PM2.5 concentration exceeding 41.8 µg/m3. Importantly, this effect appeared to be largely mediated by an increase in body fat percentage (BF%).
The results of this study were consistent with those of previous studies. A prospective cohort study that included 74,880 registered nurses in 11 states in the United States demonstrated a 4% higher risk of hypertension for every 5 µg/m3 increase in the 24-month average PM2.5 concentration [22]. In addition, an increase of 10 µg/m3 in the PM2.5 concentration was observed to be associated with an 11% increased risk of hypertension in a large-scale cross-sectional study in China [47]. A similar result was found in another cohort study including 59,456 adults in China (HR = 1.11; 95% CI = 1.05–1.17) [48].
However, other studies reported different findings. A study that included 7 European air pollution effect cohorts totaling 41,072 participants who did not report hypertension at baseline indicated that each 5 µg/m3 increase in the PM2.5 exposure level resulted in a 22% increased risk of hypertension [11]. Moreover, Trenton Honda et al. reported a 13% increased risk of hypertension for every interquartile range (equal to 3.98 µg/m3) increase in the ambient PM2.5 concentration [49]. These controversial results, although explainable or partially explainable by differences in atmospheric pollutant composition [50] and population demographic characteristics [51], indicate that the hypothesis that the exposure-response relationship between PM2.5 exposure and hypertension risk may be affected by mediators remains reasonable, and the direct and mediating effects of PM2.5 exposure and hypertension risk warrant further exploration.
Moreover, we conducted an assessment of the hypertension burden that could be attributed to PM2.5 exposure in the overall population and specific populations. Compared with many previous studies that used ORs or relative risks to demonstrate the relationship between PM2.5 exposure and hypertension risk, we combined the OR of PM2.5 exposure and hypertension risk with the percentage of the population exposed to high PM2.5 concentrations to provide a more comprehensive and understandable perspective. It was estimated that 9.1% of the hypertension burden could be attributed to exposure at an annual average PM2.5 concentration over 41.8 µg/m3. Similar results were observed in the subgroup analysis stratified by sex and age. However, we found that 14.4% of the hypertension burden could be attributed to exposure to high PM2.5 concentration in individuals with a BMI ≥ 24 kg/m2, whereas only 6.0% of the hypertension burden could be attributable to exposure to high PM2.5 concentration in those with a BMI < 24 kg/m2. BMI, a traditional indicator of obesity, is thought to be associated with PM2.5 exposure [35, 52]. More importantly, obesity is likewise considered an independent risk factor for hypertension; thus, we hypothesized that obesity may mediate the association between PM2.5 exposure and hypertension risk. To assess the potential mediating effect in a multidimensional manner, we used different obesity parameters, including BF%, BMI, waist circumference, and weight. The results of the mediation analysis demonstrated that BF%, rather than BMI, appeared the strongest mediating effect, explaining approximately 60% of the total effect of PM2.5 exposure on hypertension risk.
BMI has been criticized as an indicator of obesity for not reflecting body composition characteristics and therefore providing insufficient warning of disease risk. BF% represents a sensitive indicator of metabolic characteristics and is associated with lower insulin sensitivity, a larger subcutaneous adipocyte size, and central fat distribution in obese patients, with this effect considered independent of BMI [53, 54]. A clinical trial aiming to evaluate the effects of dietary interventions on the mobilization of fat storage pools found that a Mediterranean low-carbohydrate dietary pattern reduced the BF% and the total amount of visceral adiposity, with this change in lipid traits being independent of a given BMI [55]. An elevated BF% was observed in individuals with exposure to ambient fine particulate matter [56, 57]. A cross-sectional study of people aged ≥ 65 years in Taiwan showed that increased PM2.5 exposure was strongly associated with higher BF% and lower skeletal muscle mass [58]. Cai and his colleagues examined the significant positive associations between ambient air pollutant exposure and elevated BF% in participants from the UK Biobank, with the strongest associations between PM2.5 concentrations and the amount of fat at the trunk and viscera [59]. Evidence from experimental and interventional studies suggests that BF%, indicative of adipose tissue distribution, appears to possess the potential to better reflect PM2.5 exposure-associated hypertension risk than BMI. However, its mediating effect on PM2.5 exposure-associated hypertension and its potential biological mechanisms remain unknown. Limited evidence suggests that a high BF% may be a consequence of environmental and genetic susceptibility and their interaction-driven systemic inflammatory state, adipokine imbalance, and proinflammatory transformation of the gut microbial profile [60, 61], which appears to explain its mediating effect on air pollutant-induced blood pressure elevation since recent metabolomic, epigenetic, and toxicological studies from obese humans or other mammals have supported air pollutants as a critical environmental trigger for the mechanisms mentioned above [62,63,64,65]. Moreover, PM2.5 exposure experimentally attenuated compensatory antioxidant reserves [66], and enhanced intense vasoactive lipid release [67], which may partially explain the direct causation of hypertension. Additionally, exposure to fine particulate matter enhances physiological contractile mechanisms mediated by perivascular adipose tissue and corrodes the sensitivity of the vessel to diastolic agents. Zhou et al. reported that mice exposed to high concentrations of PM2.5 had upregulated expression of adipokines and oxidative stress-related molecules in aortic perivascular adipose tissue. Isolated aortic ring diastolic experiments showed that exposure to air pollutants inhibited the response of the aorta to relaxation agonists (acetylcholine and sodium nitroprusside). Overexpression of extracellular superoxide dismutase reversed this effect, highlighting the possibility of targeting excessive adipose tissue-mediated oxidative stress to prevent air pollutant exposure-induced hypertension [68].
The mediation analysis we performed provide new insights for understanding the mechanisms linking air pollutant exposure and hypertension risk and for proposing new health policies. First, our findings provide early warning indicators available to community-based large-scale health surveillance programs for monitoring intermediate processes between air pollution exposure and hypertension risk. Second, our findings support the rationale of BF% assessments for seeking population-level solutions for hypertension. Finally, these results support the hypothesis that targeting the improvement of unhealthy body compositions will reduce the average blood pressure of residents living in regions with severe air pollution. Further studies are needed to identify the potential effects of mutual interactions among ambient fine particulate matter exposure, body composition, and blood pressure.
Some limitations in this study should be acknowledged. Firstly, as a cross-sectional study, it is unable to establish a causal association between PM2.5 exposure and the risk of hypertension, as well as the mediating role of body composition and obesity in this association. Further study with a long-term follow-up is urgently warranted to confirm our findings. Second, we did not assess longer-term PM2.5 exposure beyond 3 years because no national air pollution detection system was established in China before 2013; however, previous studies have found that 1-year average PM2.5 exposure levels have reliable predictive efficacy for hypertension risk [69, 70]. Third, we failed to assess individual PM2.5 exposure, which could lead to an inability to measure individual health hazards; however, we collected measurements from all monitors at regional air quality monitoring stations and selected values from the nearest monitor, and this approach could reflect and compliment the spatial variability of individual-level exposure. Finally, our results were analyzed from a population in southern China, which may limit their applicability in other regions.
In conclusion, we find a nonlinear relationship between mean annual PM2.5 exposure levels and the risk of hypertension in a representative population sampled by multistage stratified randomization. Moreover, 9.1% of the burden of hypertension could be attributed to exposure to annual mean PM2.5 concentrations above 41.8 µg/m3 in the population dimension. Importantly, the observed association between PM2.5 exposure and hypertension appears to be predominantly mediated by alterations in body composition and obesity, adding information to support public health policy development and personal protection planning to reduce potentially harmful exposures.
Data Availability
The full datasets used in this analysis are available from the corresponding author upon reasonable request.
Abbreviations
- PM2.5:
-
Particulate matter with aerodynamic equivalent diameter ≤ 2.5 μm
- BP:
-
Blood pressure
- SBP:
-
Systolic blood pressure
- DBP:
-
Diastolic blood pressure
- PAR%:
-
Population attributable risk fraction
- PSUs:
-
Primary sampling units
- PPS:
-
Probability Proportional to Size
- BMI:
-
Body mass index
- BF%:
-
Body fat percentage
References
(NCD-RisC) NRFC. Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: a pooled analysis of 1201 population-representative studies with 104 million participants. Lancet (London England). 2021;398(10304):957–80.
Wang Z, Chen Z, Zhang L, Wang X, Hao G, Zhang Z, et al. Status of hypertension in China: results from the China Hypertension Survey, 2012–2015. Circulation. 2018;137(22):2344–56.
Wang J-G, Zhang W, Li Y, Liu L. Hypertension in China: epidemiology and treatment initiatives. Nat Rev Cardiol. 20;8:531–45.
Mills KT, Stefanescu A, He J. The global epidemiology of hypertension. Nat Rev Nephrol. 2020;16(4):223–37.
Wang W, Jiang B, Sun H, Ru X, Sun D, Wang L, et al. Prevalence, incidence, and mortality of stroke in China: results from a Nationwide Population-Based survey of 480 687 adults. Circulation. 2017;135(8):759–71.
Yang Z, Liu J, Ge J, Chen L, Zhao Z, Yang W. Prevalence of cardiovascular disease risk factor in the chinese population: the 2007–2008 China National Diabetes and Metabolic Disorders Study. Eur Heart J. 2012;33(2):213–20.
Du X, Patel A, Anderson C, Dong J, Ma C. Epidemiology of Cardiovascular Disease in China and Opportunities for Improvement: JACC International. J Am Coll Cardiol. 2019;73(24):3135–47.
Gu J, Shi Y, Zhu Y, Chen N, Wang H, Zhang Z, et al. Ambient air pollution and cause-specific risk of hospital admission in China: a nationwide time-series study. PLoS Med. 2020;17(8):e1003188.
Warembourg C, Maitre L, Tamayo-Uria I, Fossati S, Roumeliotaki T, Aasvang G, et al. Early-Life Environmental Exposures and blood pressure in children. J Am Coll Cardiol. 2019;74(10):1317–28.
Rajagopalan S, Al-Kindi S, Brook R. Air Pollution and Cardiovascular Disease: JACC State-of-the-art review. J Am Coll Cardiol. 2018;72(17):2054–70.
Fuks K, Weinmayr G, Basagaña X, Gruzieva O, Hampel R, Oftedal B, et al. Long-term exposure to ambient air pollution and traffic noise and incident hypertension in seven cohorts of the european study of cohorts for air pollution effects (ESCAPE). Eur Heart J. 2017;38(13):983–90.
Chen H, Burnett R, Kwong J, Villeneuve P, Goldberg M, Brook R, et al. Spatial association between ambient fine particulate matter and incident hypertension. Circulation. 2014;129(5):562–9.
Xu J, Zhang Y, Yao M, Wu G, Duan Z, Zhao X, et al. Long-term effects of ambient PM2.5 on hypertension in multi-ethnic population from Sichuan province, China: a study based on 2013 and 2018 health service surveys. Environ Sci Pollut Res Int. 2021;28(5):5991–6004.
Zhang Z, Dong B, Li S, Chen G, Yang Z, Dong Y, et al. Exposure to ambient particulate matter air pollution, blood pressure and hypertension in children and adolescents: a national cross-sectional study in China. Environ Int. 2019;128:103–8.
Münzel T, Gori T, Al-Kindi S, Deanfield J, Lelieveld J, Daiber A, et al. Effects of gaseous and solid constituents of air pollution on endothelial function. Eur Heart J. 2018;39(38):3543–50.
Krishnan R, Adar S, Szpiro A, Jorgensen N, Van Hee V, Barr R, et al. Vascular responses to long- and short-term exposure to fine particulate matter: MESA Air (multi-ethnic study of atherosclerosis and Air Pollution). J Am Coll Cardiol. 2012;60(21):2158–66.
Zhang J, Chen R, Zhang G, Wang Y, Peng J, Hu R, et al. PM increases mouse blood pressure by activating toll-like receptor 3. Ecotoxicol Environ Saf. 2022;234:113368.
Wang J, Wu S, Cui J, Ding Z, Meng Q, Sun H, et al. The influences of ambient fine particulate matter constituents on plasma hormones, circulating TMAO levels and blood pressure: a panel study in China. Environ Pollution (Barking Essex: 1987). 2022;296:118746.
Hu C, Tao Y, Deng Y, Cai Q, Ren H, Yu C et al. Paternal long-term PM2.5 exposure causes hypertension via increased renal AT1R expression and function in male offspring. Clinical science (London, England: 1979). 2021;135(22):2575-88.
Xie X, Wang Y, Yang Y, Xu J, Zhang Y, Tang W et al. Long-Term Effects of ambient particulate matter (with an aerodynamic diameter ≤ 2.5 µm) on hypertension and blood pressure and attributable risk among Reproductive-Age adults in China. J Am Heart Association. 2018;7(9).
Yang BY, Guo Y, Markevych I, Qian ZM, Bloom MS, Heinrich J, et al. Association of Long-term exposure to Ambient Air Pollutants with Risk factors for Cardiovascular Disease in China. JAMA Netw open. 2019;2(3):e190318.
Zhang Z, Laden F, Forman JP, Hart JE. Long-term exposure to Particulate Matter and Self-Reported hypertension: a prospective analysis in the Nurses’ Health Study. Environ Health Perspect. 2016;124(9):1414–20.
Jiang M, Li D, Piao J, Li J, Sun H, Chen L et al. Real-ambient exposure to air pollution exaggerates excessive growth of adipose tissue modulated by Nrf2 signal. The Science of the total environment.730:138652.
Salmón-Gómez L, Catalán V, Frühbeck G, Gómez-Ambrosi J. Relevance of body composition in phenotyping the obesities. Reviews in endocrine & metabolic disorders. 2023.
Deurenberg-Yap M, Chew SK, Deurenberg P. Elevated body fat percentage and cardiovascular risks at low body mass index levels among singaporean chinese, Malays and Indians. Obes Reviews: Official J Int Association Study Obes. 2002;3(3):209–15.
Carter JL, Abdullah N, Bragg F, Murad NAA, Taylor H, Fong CS et al. Body composition and risk factors for cardiovascular disease in global multi-ethnic populations. International journal of obesity (2005). 2023.
Wang X, Karvonen-Gutierrez CA, Gold EB, Derby C, Greendale G, Wu X, et al. Longitudinal Associations of Air Pollution with body size and composition in midlife women: the study of women’s Health across the Nation. Diabetes Care. 2022;45(11):2577–84.
Du S, Hong X, Yang Y, Ding Z, Yu T. Association between body fat percentage and H-type hypertension in pos tmenopausal women. Front Public Health.10:950805.
Han P, Zhang Y, Chen X, Liang Z, Yu X, Liu Y et al. Poor physical Capacity Combined with High Body Fat percentage as an in dependent risk factor for Incident Hypertension in Chinese Suburb-Dwel ling older adults. Front Public Health.10:875041.
Wang Z, Zhang L, Chen Z, Wang X, Shao L, Guo M, et al. Survey on prevalence of hypertension in China: background, aim, method and design. Int J Cardiol. 2014;174(3):721–3.
Liu LS. [2010 chinese guidelines for the management of hypertension]. Zhonghua xin xue guan bing za zhi. 2011;39(7):579–615.
Roshani D, Ghaderi E. Comparing smoothing techniques for fitting the Nonlinear Effect of Cov ariate in Cox Models. Acta Inf Med.24(1):38–41.
Dong GH, Qian ZM, Xaverius PK, Trevathan E, Maalouf S, Parker J, Association between long-term air pollution and increased blood pressure and hypertension in China., Hypertension et al. (Dallas, Tex: 1979). 2013;61(3):578 – 84.
Yusuf S, Joseph P, Rangarajan S, Islam S, Mente A, Hystad P, et al. Modifiable risk factors, cardiovascular disease, and mortality in 155 722 individuals from 21 high-income, middle-income, and low-income countries (PURE): a prospective cohort study. Lancet. 2020;395(10226):795–808.
Hou J, Gu J, Liu X, Tu R, Dong X, Li R, et al. Long-term exposure to air pollutants enhanced associations of obesity with blood pressure and hypertension. Clinical nutrition (Edinburgh. Scotland). 2021;40(4):1442–50.
Wang T, Han Y, Li H, Fang Y, Liang P, Wang Y et al. Fine particulate matter and vasoactive 20-hydroxyeicosatetraenoic acid: insights into the mechanisms of the prohypertensive effects of parti culate air pollution. The Science of the total environment.806(Pt 3):151298.
Xu X, Yavar Z, Verdin M, Ying Z, Mihai G, Kampfrath T et al. Effect of early particulate air pollution exposure on obesity in mice: role of p47phox. Arteriosclerosis, thrombosis, and vascular biology.30(12):2518–27.
Sun Q, Yue P, Deiuliis JA, Lumeng CN, Kampfrath T, Mikolaj MB et al. Ambient air pollution exaggerates adipose inflammation and insulin res istance in a mouse model of diet-induced obesity. Circulation.119(4):538–46.
Wang Q, Li X, Zhong W, Liu H, Feng C, Song C et al. Residential greenness and dyslipidemia risk: dose-response relations a nd mediation through BMI and air pollution. Environ Res.217:114810.
Yu W, Li X, Zhong W, Dong S, Feng C, Yu B et al. Rural-urban disparities in the associations of residential greenness w ith diabetes and prediabetes among adults in southeastern China. Sci Total Environ.860:160492.
Rijnhart JJM, Lamp SJ, Valente MJ, MacKinnon DP, Twisk JWR, Heymans MW. Mediation analysis methods used in observational research: a scoping review and recommendations. BMC Med Res Methodol. 2021;21(1):226.
Zhang Z, Zheng C, Kim C, Van Poucke S, Lin S, Lan P. Causal mediation analysis in the context of clinical research. Annals of Translational Medicine. 2016;4(21):425.
Imai K, Keele L, Tingley D. A general approach to causal mediation analysis. Psychol Methods. 2010;15(4):309–34.
Rene L, Linero AR, Slate E. Causal mediation and sensitivity analysis for mixed-scale data. Statistical methods in medical research. 2023:9622802231173491.
Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. J Personal Soc Psychol. 1986;51(6):1173–82.
Yang L, Zhang Y, Qi W, Zhao T, Zhang L, Zhou L, et al. Adverse effects of PM(2.5) on cardiovascular diseases. Rev Environ Health. 2022;37(1):71–80.
Yang S, Liang X, Dou Q, La Y, Cai J, Yang J, et al. Ethnic disparities in the association between ambient air pollution and risk for cardiometabolic abnormalities in China. Sci Total Environ. 2022;838(Pt 1):155940.
Huang K, Yang X, Liang F, Liu F, Li J, Xiao Q, Long-Term Exposure to Fine Particulate Matter and Hypertension Incidence in China., Hypertension et al. (Dallas, Tex: 1979). 2019;73(6):1195 – 201.
Honda T, Eliot MN, Eaton CB, Whitsel E, Stewart JD, Mu L, et al. Long-term exposure to residential ambient fine and coarse particulate matter and incident hypertension in post-menopausal women. Environ Int. 2017;105:79–85.
Daellenbach KR, Uzu G, Jiang J, Cassagnes LE, Leni Z, Vlachou A, et al. Sources of particulate-matter air pollution and its oxidative potential in Europe. Nature. 2020;587(7834):414–9.
Weng Z, Liu Q, Yan Q, Liang J, Zhang X, Xu J, et al. Associations of genetic risk factors and air pollution with incident hypertension among participants in the UK Biobank study. Chemosphere. 2022;299:134398.
Yan M, Hou F, Xu J, Liu H, Liu H, Zhang Y, et al. The impact of prolonged exposure to air pollution on the incidence of chronic non-communicable disease based on a cohort in Tianjin. Environ Res. 2022;215(Pt 1):114251.
Eriksson Hogling D, Bäckdahl J, Thorell A, Rydén M, Andersson DP. Metabolic impact of body Fat percentage Independent of Body Mass Index in women with obesity Remission after gastric bypass. Obes Surg.30(3):1086–92.
Garufi G, Seyhan AA, Pasarica M. Elevated secreted frizzled-related protein 4 in obesity: a potential role in adipose tissue dysfunction. Obes (Silver Spring Md). 2015;23(1):24–7.
Gepner Y, Shelef I, Schwarzfuchs D, Zelicha H, Tene L, Yaskolka Meir A, et al. Effect of distinct lifestyle interventions on mobilization of Fat Storage pools: CENTRAL magnetic resonance imaging Randomized Controlled Trial. Circulation. 2018;137(11):1143–57.
Tu R, Hou J, Liu X, Li R, Dong X, Pan M et al. Low socioeconomic status aggravated associations of exposure to mixtur e of air pollutants with obesity in rural chinese adults: a cross-sect ional study. Environ Res.194:110632.
Liu X, Tu R, Qiao D, Niu M, Li R, Mao Z, et al. Association between long-term exposure to ambient air pollution and ob esity in a chinese rural population: the Henan Rural Cohort Study. Volume 260. Essex: Environmental pollution (Barking; 1987. p. 114077.
Chen CH, Huang LY, Lee KY, Wu CD, Chiang HC, Chen BY, et al. Effects of PM(2.5) on skeletal muscle Mass and Body Fat Mass of the Elderly in Taipei, Taiwan. Sci Rep. 2019;9(1):11176.
Cai M, Li H, Wu Y, Zhang S, Wang X, Zhang Z, et al. Ambient air Pollution Associated with Body Fat Percentages at different body compartments: a cohort study of UK Biobank participants. Environ Health Perspect. 2022;130(6):67702.
Haapala EA, Kuronen E, Ihalainen JK, Lintu N, Leppänen MH, Tompuri T et al. Cross-sectional associations between physical fitness and biomarkers o f inflammation in children-the PANIC study. Scand J Med Sci Sports.33(6):1000–9.
Salazar-Tortosa DF, Labayen I, González-Gross M, Seral-Cortes M, Moreno LA. A GZ, Association between PTPN1 polymorphisms and obesity-related phenotypes in european adolescents: influence of physical activity. Pediatr Res. 2022.
Furlong MA, Klimentidis YC. Associations of air pollution with obesity and body fat percentage, and modification by polygenic risk score for BMI in the UK Biobank. Environ Res. 2020;185:109364.
Gruzieva O, Xu CJ, Breton CV, Annesi-Maesano I, Antó JM, Auffray C, et al. Epigenome-Wide Meta-analysis of methylation in children related to prenatal NO2 Air Pollution exposure. Environ Health Perspect. 2017;125(1):104–10.
Panni T, Mehta AJ, Schwartz JD, Baccarelli AA, Just AC, Wolf K, et al. Genome-wide analysis of DNA methylation and fine particulate Matter Air Pollution in three study populations: KORA F3, KORA F4, and the normative aging study. Environ Health Perspect. 2016;124(7):983–90.
Xu X, Yavar Z, Verdin M, Ying Z, Mihai G, Kampfrath T et al. Effect of early particulate air pollution exposure on obesity in mice: role of p47phox. Arteriosclerosis, thrombosis, and vascular biology. 2010;30(12):2518–27.
Dye JA, Costa DL, Kodavanti UP. Executive Summary: variation in susceptibility to ozone-induced health effects in rodent models of cardiometabolic disease. Inhalation Toxicol. 2015;27(Suppl 1):105–15.
Wang T, Han Y, Li H, Fang Y, Liang P, Wang Y, et al. Fine particulate matter and vasoactive 20-hydroxyeicosatetraenoic acid: insights into the mechanisms of the prohypertensive effects of particulate air pollution. Sci Total Environ. 2022;806(Pt 3):151298.
Haberzettl P, Jin L, Riggs DW, Zhao J, O’Toole TE, Conklin DJ. Fine particulate matter air pollution and aortic perivascular adipose tissue: oxidative stress, leptin, and vascular dysfunction. Physiological Rep. 2021;9(15):e14980.
Lin H, Guo Y, Zheng Y, Di Q, Liu T, Xiao J, Long-Term Effects of Ambient PM(2.5) on Hypertension and Blood Pressure and Attributable Risk Among Older Chinese Adults., Hypertension et al. (Dallas, Tex: 1979). 2017;69(5):806 – 12.
Wensu Z, Wen C, Fenfen Z, Wenjuan W, Li L. The Association between Long-Term exposure to Particulate Matter and Incidence of Hypertension among Chinese Elderly: a retrospective cohort study. Front Cardiovasc Med. 2021;8:784800.
Acknowledgements
The authors would like to thank all the staff members who participated in this survey for all their work in the design, implementation, data collection, analysis, and reporting of this study. In particular, the authors would like to thank the China National Environmental Monitoring Center for providing open-source air quality data.
Funding
This study was supported by the China National Science and Technology Pillar Program (2011BAI11B01), Guangxi Key Laboratory of Precision Medicine in Cardio-Cerebrovascular Diseases Control and Prevention (22-035-18), Guangxi Clinical Research Center for Cardio-Cerebrovascular Diseases (AD17129014), National Natural Science Foundation of China (81860087, 81960082), Key R&D Program of Guangxi (Guike AB20297008), Guangxi Medical High-level Backbone Talents “139” Program (G201901006), and Clinical Research Climbing Program of the First Affiliated Hospital of Guangxi Medical University (YYZS2021003).
Author information
Authors and Affiliations
Contributions
YX, FH, ZY Z, and RJ H: conceptualization, visualization. YX, JL, XZ L and DZ L: investigation, data collection. YX, JS C, YL, YQ L: data verification, traceability and noise reduction. YX, JL, YN X, FH, ZY Z, and RJ H: data analysis, writing, original draft preparation, methodology, software, and reviewing. All authors contributed to the article and approved the submitted version.
Corresponding authors
Ethics declarations
Ethical approval and consent to participate
This study was conducted in strict accordance with the Declaration of Helsinki, and all participants provided written informed consent. All survey protocols were approved by the Ethics Committee of The First Affiliated Hospital of Guangxi Medical University (Guangxi, China) (approval number: 2012[KY-E-017]).
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Xue, Y., Li, J., Xu, YN. et al. Mediating effect of body fat percentage in the association between ambient particulate matter exposure and hypertension: a subset analysis of China hypertension survey. BMC Public Health 23, 1897 (2023). https://doi.org/10.1186/s12889-023-16815-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-023-16815-0