
Abstract
Background
Patients with type 2 diabetes Mellitus (T2DM) are more likely to suffer from a higher uric acid level in blood—hyperuricemia (HUA). There are no conclusive studies done to predict HUA among T2DM patients. Therefore, this study aims to explore the risk factors of HUA among T2DM patients and finally suggest a model to help with its prediction.
Method
In this retrospective research, all the date were collected between March 2017 and October 2019 in the Medical Laboratory Center of the First Affiliated Hospital of Xinjiang Medical University. The information included sociodemographic factors, blood routine index, thyroid function indicators and serum biochemical markers. The least absolute shrinkage and selection operator (LASSO) and multivariate binary logistic regression were performed to screen the risk factors of HUA among T2DM patients in blood tests, and the nomogram was used to perform and visualise the predictive model. The receiver operator characteristic (ROC) curve, internal validation, and clinical decision curve analysis (DCA) were applied to evaluate the prediction performance of the model.
Results
We total collected the clinical date of 841 T2DM patients, whose age vary from 19-86. In this study, the overall prevalence of HUA in T2DM patients was 12.6%. According to the result of LASSO-logistic regression analysis, sex, ethnicity, serum albumin (ALB), serum cystatin C (CysC), serum inorganic phosphorus (IPHOS), alkaline phosphatase (ALP), serum bicarbonate (CO2) and high-density lipoprotein (HDLC) were included in the HUA risk prediction model. The nomogram confirmed that the prediction model fits well (χ2 = 5.4952, P = 0.704) and the calibration curve indicates the model had a good calibration. ROC analysis indicates that the predictive model shows the best discrimination ability (AUC = 0.827; 95% CI: 0.78–0.874) whose specificity is 0.885, and sensitivity is 0.602.
Conclusion
Our study reveals that there were 8 variables that can be considered as independent risk factors for HUA among T2DM patients. In light of our findings, a predictive model was developed and clinical advice was given on its use.
Similar content being viewed by others


Background
Type 2 diabetes mellitus (T2DM) is a metabolic condition resulting from a combination of genetics, environmental factors, and dietary habits. The main symptoms of the condition are the inability to stabilise blood glucose levels and ineffective insulin secretion. The World Health Organization (WHO) has reported diabetes as the ninth leading cause of death in 2019 [1], with 1.5 million estimated deaths directly resulting from it, and the disease is likely to affect over 640 million adults by 2040 [2]. According to the International Diabetes Federation (IDF) report, the number of diabetes patients in China have been exceed 140 million currently [3]. Diabetes correlates with various diseases, such as thyroid dysfunction [4, 5], lipid metabolism disorder [6], purine metabolic disorder [7], cardiovascular disease [8], and cognitive function [9]. Long-term hyperglycemia leads to islet β-cells depletion and failure, ultimately resulting in hyperglycemia and metabolic decompensation [10].
Hyperuricemia (HUA) is a typical chronic metabolism illness brought about by purine metabolism disorder and serum uric acid (SUA) excretion disorder and it is a risk factor for diabetes, metabolic syndrome, obesity, high cholesterol, cardiovascular and kidney disease, [7, 11, 12]. According to a meta-analysis study [13], the prevalence of HUA was 16.4% in the Chinese population from 2000–2019. Epidemiological studies show that HUA is not only a key risk factor for gout, but also closely related to the diseases mentioned above as well as malignant tumors. As T2DM is a metabolic disorder, it often causes difficulty for patients to break down uric acid and leads to HUA, however the symptoms of HUA are not obvious, even more so among diabetic patients. There is a strong correlation between HUA and both diabetic peripheral neuropathy and diabetic microangiopathy [14]—resulting in nervous system and renal function damage, and increasing mortality among patients with diabetes.
T2DM as a risk factor for HUA has been poorly reported. There have been many studies on HUA risk prediction models, but most were developed on healthy populations. Eljaaly et al. [15] developed a logistic regression model that showed HUA was associated with hip circumference, total cholesterol, high-density lipoprotein, triglycerides, and serum creatinine. Huang et al. [16] constructed a nomogram prediction model for diabetic kidney disease. The predictive model was established to serve a clinical setting and so clear predictive ability, visualisation, and simple operation are necessary to ensure effective use. Thus, a clinically convenient and practical predictive model is imperative for early detection of HUA in patients with T2DM. In summation, the objective of our study was to investigate the potential risk factors associated with HUA in T2DM patients and develop an effective predictive model for clinical application.
Methods
Study population and definition
In this retrospective study, we collected clinical data from the Medical Laboratory Center of the First Affiliated Hospital of Xinjiang Medical University, China, between March 2017 and October 2019. Patients diagnosed with T2DM – as defined by the Chinese Diabetes Society [17] – had typical symptoms, including excessive thirst and appetite, polyuria, and blood glucose in a specific range (i.e., greater or equal to 11.1 mmol/L, a fasting blood glucose of greater or equal to 7.0 mmol/L, an oral glucose tolerance test where the blood glucose after 2 h was greater or equal to 11.1 mmol/L, or a HbA1c of greater or equal to 6.5%). In total 841 patients followed the screening process shown in Fig. 1. Diagnosing HUA was based on sound diagnostic criteria (i.e. SUA of greater or equal to 420 mmol/L and 360 mmol/L for male and female respectively) [18,19,20]. All tests were performed whilst the patients were hospitalised. The study was approved by the ethics committee of the First Affiliated Hospital of Xinjiang Medical University (No.: K2303-11), and written informed consent was obtained from all participants.

Flow chart of the research
The patients excluded were: (1) younger than 18 years old, (2) duplicated medical records, (3) effected by another type of diabetes, (4) not diagnosed with HUA but had transient elevated blood uric acid, (5) undergoing urate-lowering therapy or taking medications that affect blood uric acid levels, (6) suffering from a serious liver and kidney damage, (7) suffering from acute and chronic heart failure or heart failure; (8) suffering from infectious diseases, such as tuberculosis, AIDS, several type of hepatitis, etc., (9) suffering from severe diabetic complications.
According to the statistical analysis,the R package "epicalc" developed by Rodriguez [21] was used to calculate the sample size. The minimum sample size required was determined to be 169, considering the prevalence of HUA among T2DM patients in our research.
Data collection
The baseline characteristics, collected from medical records, included the following results: (1) sociodemographic markers—age, gender and ethnicity, (2) blood glucose monitoring, (3) blood cell content tests, (4) thyroid function tests; (5) blood lipid tests; (6) renal function tests; (7) liver function indicators and (8) serum ionic concentration index.
Statistical analysis
Statistical analysis and graph plotting were performed using SPSS 26.0 and R 4.1.3. Data are expressed as mean ± standard deviation, median (interquartile range, IQR) and numbers (percentage) for normal distribution quantitative variables, non-normal distribution quantitative variables and qualitative variables, respectively. The Student's t-test or the Wilcoxon rank-sum test was used to compare continuous data between two groups, while the chi-square test was used to compare categorical data between two groups. Given the strong collinearity among blood indicators in this study, the least absolute shrinkage and selection operator (LASSO) and multivariate logistic regression were used to screen characteristic variables. Then, we developed the nomogram according to the logistic regression. Receiver operating characteristic (ROC) curves and areas under the curve (AUC)—with 95% confidence intervals—were used to examine the predicting performance of the risk prediction model and each independent predictor for HUA. The decision curve analysis (DCA) was used to assess the maximum net benefit of the predictive model. The statistical difference was considered significant when the two-sided P-value was greater than 0.05.
Results
Baseline characteristics
A total of 618 eligible T2DM patients—410 males and 208 females—were included in this study, namely, 78 in the HUA group and 540 in the non-HUA group. In other words, the prevalence of hyperuricemia (HUA) among patients with type 2 diabetes is 12.6%. The mean ages of the non-HUA group and HUA group were (56.26 ± 12.17) and (57.46 ± 11.44) years, respectively. There were 17 (21.8%) well-controlled diabetic patients (i.e., with HbA1c less than 6.5%) in the non-HUA group, and 91 (16.7%) in the HUA group. The baseline characteristics of the participants were shown in Table 1. Participants with HUA were more likely to be female and different ethnic backgrounds contribute the different prevalence of HUA (P < 0.05). In addition, there were higher values of, TG, BUN, CREA, CysC, URIC, ALB, A/G, GGT and IPHOS in the HUA group compared to the non-HUA group (All P < 0.05), but lower values of HbA1c, GSP, MCH, APOA, HDLC, ALP, and CO2 (All P < 0.05). There was no significant difference in other indicators between HUA group and non-HUA group (P > 0.05).
Screening of HUA-related risk factors
As shown in Fig. 2, the variables were screened by LASSO regression and tenfold cross-validation, the λ was taken when the model error was the one standard error of the minimum (the one SE criteria), and nine indicators were finally screened, including sex, ethnicity, ALB, CysC, IPHOS, ALP, CO2, HDLC and TG. Then, these variables were incorporated into multivariate logistic regression analyses shown in Table 2. Sex, ethnicity, ALB, CysC, IPHOS, ALP, CO2 and HDLC were identified as independent risk factors for HUA in the T2DM patients.

Characteristic variables were screened using LASSO regression analysis. A LASSO coefficient profiles of the nine characteristic variables. A coefficient profile plot was produced against the log (lambda) sequence. B The selection of the best parameter (lambda) in the LASSO model uses tenfold cross-validation. The relationship curve between partial likelihood deviation (binomial deviation) and log (lambda) was plotted. Dotted vertical lines were drawn at the optimal values by using the minimum criteria and the one SE of the minimum criteria (the one SE criteria). Abbreviations: LASSO Least absolute shrinkage and selection operator, SE Standard error
The build and analysis of HUA risk prediction model
Based on the outcomes of LASSO-logistic regression results, the nomogram was created and shown in Fig. 3. The sum of the corresponding scores of each variable (including sex, ethnicity, ALB, CysC, IPHOS, ALP, CO2 and HDLC) was the individual risk score, which gave an estimated probability of HUA risk in T2DM patients. The Bootstrap method was used to test and verify the nomogram model giving a measure of internal validation, and the calibration curve (see Fig. 4) was drawn after the raw data was sampled 1,000 times. The Hosmer–Lemeshow goodness-of-fit test showed that the prediction model fits well (χ2 = 5.4952 and P = 0.704), which mean that there is no statistically significant difference between the risk prediction value and the actual observation value. The results showed that the model accurately predicts the risk of HUA in T2DM patients.

Nomogram for prediction HUA among T2DM patients. Abbreviations: HUA Hyperuricemia, ALB Serum albumin, CysC Serum cystatin C, IPHOS Serum inorganic phosphorus, ALP Alkaline phosphatase, HDLC High-density lipoprotein, CO2 Serum bicarbonate

The calibration plot for nomogram
The evaluation of the HUA risk prediction model in T2DM patients
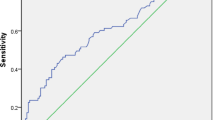
The ROC curves for identifying T2DM participants with HUA was shown in Table 3 and Fig. 5. IPHOS showed the best discrimination ability (AUC = 0.625; 95% CI: 0.557–0.693) among all 8 indicators (Delong's test all P < 0.05), including sex (AUC = 0.586), ethnicity (AUC = 0.87), ALB (AUC = 0.6), CysC (AUC = 0.593), IPHOS (AUC = 0.625), ALP (AUC = 0.588), HDLC (AUC = 0.625) and CO2 (AUC = 0.61). The AUC for the combination of the above 8 parameters, which gave a prediction for HUA among T2DM patients, is 0.827 (95% CI: 0.78–0.874, P < 0.001), specificity is 0.885, and sensitivity is 0.602. Collectively, its predictive performance was better than individual factors. Based on the result of DCA, the predictive model was also outperformed in comparison to individual indicators, see Fig. 6.

The ROC curve of the risk factor for predicting HUA in T2DM patients. Abbreviations: ROC Receiver operating characteristic, HUA Hyperuricemia, ALB Serum albumin, CysC Serum cystatin C, IPHOS Serum inorganic phosphorus, ALP Alkaline phosphatase, HDLC High-density lipoprotein, CO2 Serum bicarbonate

The DCA curve of the predictive model. Abbreviations: DCA Decision curve analysis, ALB Serum albumin, CysC Serum cystatin C, IPHOS Serum inorganic phosphorus, ALP Alkaline phosphatase, HDLC High-density lipoprotein, CO2 Serum bicarbonate
Discussion
Our result indicated the prevalence of HUA among patients with T2DM, identified independent risk factors associated with HUA, and established a HUA-related prediction model for T2DM patients in Urumqi city, China. The prevalence of HUA in our study population was 12.6%, which is lower than the reported prevalence among patients with diabetes (32%) [22]. To comprehensively assess the independent risk factors for HUA among T2DM patients, we conducted a thorough screening using demographic information, medical history, and laboratory test results from a cohort of 618 T2DM patients. Utilizing LASSO-logistic regression analysis, we identified several independent risk factors associated with HUA among T2DM patients, including sex, ethnicity, CysC, ALB, IPHOS, ALP, CO2, and HDLC.
Previous studies have verified estrogens have a uricosuric effect on the kidney to excrete SUA [23], which leads to the difference in the prevalence of HUA between males and females. Our research findings demonstrate that females with T2DM are more susceptible to HUA than their male counterparts, which aligned with the conclusions drawn in the study conducted by Eljaaly et al. [15]. Meanwhile, according to the reports and our result, it was indicated that different ethnic backgrounds ( e.g., ApoE E4, IL-8, IL-18 gene polymorphism) may contribute the different prevalence of HUA [24].
It is worthy to notice that serum cystatin C (CysC), serum albumin (ALB) and blood inorganic phosphorus (IPHOS) were significant risk factors for HUA among T2DM patients in blood indicators. CysC is an endogenous protease inhibitor in the cystatin superfamily, it contributes to intracellular protein breakdown [25]. Serum CysC plays a crucial role in reflecting renal function and SUA levels [26]. ALB is a significant human protein, maintains osmotic pressure, pH, and aids fatty acid transport [27]. Our study disclosed high serum ALB as a risk factor of HUA in T2DM patients. Chronic inflammation has a close relation with the concentrate of ALB [28]. T2DM patients exhibit an ALB increase, this possibly due to chronic inflammation [29]. To serum IPHOS, a cross-sectional study indicated that there is no substantial link between SUA and serum calcium/phosphorus levels [30]. While, in patients with primary hyperparathyroidism, a positive association between SUA and serum calcium/serum IPHOS concentration has been suggested [31]. Variability in serum IPHOS concentration, may influenced by a high phosphorus diet factors [32]. In our research findings, the impact of serum IPHOS and serum CysC on HUA is significant enough to warrant attention from clinical practitioners. Therefore, for T2DM patients, these two indicators can serve as important clinical monitoring parameters to prevent the occurrence of HUA and renal impairment.
In the current multivariate logistic regression analysis, high-density lipoprotein (HDLC), serum bicarbonate (CO2) and alkaline phosphatase (ALP) were emerged as protective factors for HUA in T2DM patients, and essential components for our prediction model. Prior studies have highlighted the independent predictive role of lower HDLC levels in HUA development [33, 34]. Lower HDLC levels to increased susceptibility to kidney impairment, thereby reducing uric acid excretion [35]. CO2 is a crucial factor in regulating body fluid acid–base and electrolyte balance, and low level of CO2 reflects impaired renal function to a certain extent [36]. ALP, involved in phosphorylation and cellular metabolism, correlates with asymptomatic HUA [29], implying roles in cell signaling, lipid metabolism, and uric acid modulation. Overall, we incorporate the above 8 indicators related to HUA into nomogram model.
A nomogram is a visual graph using distinct lines to predict clinical events. Our model's validity, discrimination, and application were verified. ROC analysis shows improved disease prediction (AUC = 0.827) and specificity (88.5%) vs. individual indicators. Goodness-of-fit and calibration plot confirm model accuracy. Huang et al. [16] reported BMI, HbA1c, eGFR, hyperlipidemia as DKD risk factors (AUC = 0.843). This nomogram for HUA influencing factors also showed clinical applicability. These similar studies highlight of nomograms in disease prediction. Visual models aid early HUA diagnosis and prevention in T2DM, which is crucial for resource-limited areas.
Limitations
The study developed a predictive model using 8 blood indicators, and the resulting nomogram showed promising predictive performance. However, the study has limitations. Firstly, due to its retrospective single-center design, there's potential for selection bias, which might affect the prediction model and experimental results with regional traits. Secondly, the patient sample size with HUA was insufficient for meaningful analysis. Thirdly, the study doesn't establish a causal relationship between influencing factors and HUA in T2DM patients. Thus, future research should involve prospective cohort or case–control studies to confirm our assumptions. Additionally, not considering anthropometric indicators in the analyses limits the scope of findings. Consequently, the conclusions drawn from our study warrant cautious interpretation.
Conclusion
This study supplements the evidence for the ability of each indicator to identify HUA among T2DM patients and provides theoretical support for early screening of diabetes complicated by HUA in the T2DM population. Our results have demonstrated that the proposed model achieved a higher value of AUC compared to previously models, indicating promising potential for early identification and diagnosis of HUA in T2DM patients. Regular monitoring of the relevant biomarkers included in the model can help reduce the incidence of HUA, thus mitigating the onset of associated comorbidities and improving the quality of life in diabetic patients.
Availability of data and materials
The database generated during the current study is not publicly available due to privacy restrictions. The data used to support the results of this study can be obtained from the corresponding authors as required. Please send specific suggestions for future cooperation to the corresponding authors.
References
Diabetes. https://www.who.int/news-room/fact-sheets/detail/diabetes (2023).
Lewandowicz A, Skowronek P, Maksymiuk-Kłos A, Piątkiewicz P. The giant geriatric syndromes are intensified by diabetic complications. Gerontol Geriatr Med. 2018;4:233372141881739.
Sun H, Saeedi P, Karuranga S, et al. lDF Diabetes Atlas: global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res Clin Pract. 2022;183: 109119.
Roa Dueñas OH, Van der Burgh AC, Ittermann T, Ligthart S, Ikram MA, Peeters R, et al. Thyroid function and the risk of prediabetes and type 2 diabetes. J Clin Endocrinol Metab. 2022;107(6):1789–98.
Chen RH, Chen HY, Man KM, Chen SJ, Chen W, Liu PL, et al. Thyroid diseases increased the risk of type 2 diabetes mellitus: a nation-wide cohort study. Medicine (Baltimore). 2019;98(20): e15631.
Wang Y, Yang LZ, Yang DG, Zhang QY, Deng ZN, Wang K, et al. MiR-21 antagomir improves insulin resistance and lipid metabolism disorder in streptozotocin-induced type 2 diabetes mellitus rats. Ann Palliat Med. 2020;9(2):394–404.
Li W, Wang Y, Ouyang S, Li M, Liu R, Zhang Y, et al. Association between serum uric acid level and carotid atherosclerosis and metabolic syndrome in patients with type 2 diabetes mellitus. Front Endocrinol (Lausanne). 2022;13: 890305.
Wang Z, Zhao H, Zhou Q. Analysis of risk factors of coronary heart disease and its correlation with inflammatory factors in patients with type 2 diabetes mellitus. BioMed Res Int. 2022;2022:1–9.
Milne NT, Bucks RS, Davis WA, Davis TME, Pierson R, Starkstein SE, et al. Hippocampal atrophy, asymmetry, and cognition in type 2 diabetes mellitus. Brain Behav. 2018;8(1): e00741.
van Baar ACG, Meiring S, Holleman F, Hopkins D, Mingrone G, Devière J, et al. Alternative treatments for type 2 diabetes and associated metabolic diseases: medical therapy or endoscopic duodenal mucosal remodelling? Gut. 2021;70(11):2196–204.
Yi F, Lan L, Jiang J, Peng L, Jin Y, Zhou X. The related factors of hyperuricemia in IgA nephropathy. Iran J Kidney Dis. 2021;15(4):256–62.
Liu L, Zhang X, Peng L, Ma N, Yang T, Nie C, et al. Hyperuricemia is related to the risk of cardiovascular diseases in ethnic Chinese elderly women. Glob Heart. 2022;17(1):12.
Chen T, Ding X, Tang W, Chen L, Mao D, Song L, et al. Association of self-reported snoring and hyperuricaemia: a large cross-sectional study in Chongqing, China. BMJ Open. 2022;12(4): e056143.
Arersa KK, Wondimnew T, Welde M, Husen TM. Prevalence and determinants of hyperuricemia in type 2 diabetes mellitus patients attending Jimma Medical Center, Southwestern Ethiopia, 2019. Diabetes Metab Syndr Obes. 2020;13:2059–67.
Eljaaly Z, Mujammami M, Nawaz SS, Rafiullah M, Siddiqui K. Risk predictors of high uric acid levels among patients with type-2 diabetes. Diabetes Metab Syndr Obes. 2021;14:4911–20.
Huang G, Li M, Mao Y, Li Y. Development and internal validation of a risk model for hyperuricemia in diabetic kidney disease patients. Front Public Health. 2022;10: 863064.
Chinese Diabetes Society. Chinese guidelines for the prevention and treatment of type 2 diabetes (2020 edition). Chin J Diabetes. 2021;13(4):315–409.
Endocrin Branch of Chinese Medical Association. Guidelines for diagnosis and treatment of hyperuricemia and gout in China (2019). Chin J Endocrinol Metab. 2020;36(1):1–13.
Nephrologist Branch of Chinese Medical Doctor Association. Practice Guidelines for the diagnosis and treatment of hyperuricemia in renal disease in China (2017 edition). Natl Med J China. 2017;97(25):1927–36.
Li Q, Li X, Wang J, Liu H, Kwong JS, Chen H, et al. Diagnosis and treatment for hyperuricemia and gout: a systematic review of clinical practice guidelines and consensus statements. BMJ Open. 2019;9(8): e026677.
Rodríguez del Águila M, González-Ramírez A. Sample size calculation. Allergol Immunopathol (Madr). 2014;42(5):485–92.
Wang J, Chen R-P, Lei L, et al. Prevalence and determinants of hyperuricemia in type 2 diabetes mellitus patients with central obesity in Guangdong Province in China[J]. Asia Pac J Clin Nutr. 2013;22(4):590–8.
Lin YK, Lin YP, Lee JT, Lin CS, Wu TJ, Tsai KZ, et al. Sex-specific association of hyperuricemia with cardiometabolic abnormalities in a military cohort: the CHIEF study. Medicine (Baltimore). 2020;99(12): e19535.
Liu F, Du GL, Song N, Ma YT, Li XM, Gao XM, et al. Hyperuricemia and its association with adiposity and dyslipidemia in Northwest China: results from cardiovascular risk survey in Xinjiang (CRS 2008–2012). Lipids Health Dis. 2020;19(1):58.
Yuan X, Han X, Jia C, Wang H, Yu B. Association of maternal serum uric acid and cystatin C levels in late pregnancy with adverse birth outcomes: an observational cohort study in China. Int J Women’s Health. 2022;14:213–23.
Ziegelasch N, Vogel M, Körner A, Koch E, Jurkutat A, Ceglarek U, et al. Cystatin C relates to metabolism in healthy, pubertal adolescents. Pediatr Nephrol. 2022;37(2):423–32.
Cao J, Qiu W, Yu Y, Li N, Wu H, Chen Z. The association between serum albumin and depression in chronic liver disease may differ by liver histology. BMC Psychiatry. 2022;22(1):5.
Lee YB, Jun JE, Lee SE, Ahn J, Kim G, Jee JH, et al. Utility of serum albumin for predicting incident metabolic syndrome according to hyperuricemia. Diabetes Metab J. 2018;42(6):529.
Kunutsor SK, Khan H, Laukkanen JA. Serum albumin concentration and incident type 2 diabetes risk: new findings from a population-based cohort study. Diabetologia. 2015;58(5):961–7.
Karimi F, Dabbaghmanesh MH, Omrani GR. Association between serum uric acid and bone health in adolescents. Osteoporos Int. 2019;30(10):2057–64.
Valdemarsson S, Lindblom P, Bergenfelz A. Metabolic abnormalities related to cardiovascular risk in primary hyperparathyroidism: effects of surgical treatment. J Intern Med. 1998;244(3):241–9.
Yoon CY, Park JT, Jhee JH, Noh J, Kee YK, Seo C, et al. High dietary phosphorus density is a risk factor for incident chronic kidney disease development in diabetic subjects: a community-based prospective cohort study. Am J Clin Nutr. 2017;106(1):311–21.
Qu X, Zheng L, Zu B, Jia B, Lin W. Prevalence and clinical predictors of hyperuricemia in Chinese bariatric surgery patients. Obes Surg. 2022;32(5):1508–15.
Lee MJ, Khang AR, Kang YH, Yun MS, Yi D. Synergistic interaction between hyperuricemia and abdominal obesity as a risk factor for metabolic syndrome components in Korean population. Diabetes Metab J. 2022;46(5):756–66.
Kawachi K, Kataoka H, Manabe S, Mochizuki T, Nitta K. Low HDL cholesterol as a predictor of chronic kidney disease progression: a cross-classification approach and matched cohort analysis. Heart Vessels. 2019;34(9):1440–55.
Brown DD, Roem J, Ng DK, Reidy KJ, Kumar J, Abramowitz MK, et al. Low serum bicarbonate and CKD progression in children. Clin J Am Soc Nephrol. 2020;15(6):755–65.
Acknowledgements
We thank the patients who participated in this survey for their valuable information and the medical service personnel who assisted in collecting the data.
Funding
This work was supported by Tianshan Cedar Plan of Science and Technology Department of Xinjiang Uygur Autonomous Region (granted number: 2019XS03) and Xinjiang Uygur Autonomous Region “14th Five-Year” Key Discipline of the Autonomous Region (High Plateau)—Public Health and Preventive Medicine.
Author information
Authors and Affiliations
Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
We confirm that all experimental protocols were approved and all methods were conducted in accordance with relevant guidelines and regulations by the Medical Laboratory Center of the First Affiliated Hospital of Xinjiang Medical University. This study was approved by the Ethics Committee of Medical Laboratory Center of the First Affiliated Hospital of Xinjiang Medical University (No.: K2303-11). We declare that informed consent was obtained from all participants.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Abudureyimu, P., Pang, Y., Huang, L. et al. A predictive model for hyperuricemia among type 2 diabetes mellitus patients in Urumqi, China. BMC Public Health 23, 1740 (2023). https://doi.org/10.1186/s12889-023-16669-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-023-16669-6